Embed Size (px)
Citation preview

8/19/2019 A Randomized Controlled Study of the Efficacy of Misoprostol
http://slidepdf.com/reader/full/a-randomized-controlled-study-of-the-efficacy-of-misoprostol 1/6
A randomized controlled study of the efficacy of misoprostol andhyaluronic acid in preventing adhesion formation after gynecologicalsurgery: a rat uterine horn model
Cihan Kaya a,*, Nurten Sever b, Huseyin Cengiz c, Sukru Yıldız c, Murat Ekin c, Levent Yasar c
a Van O zalp State Hospital, Clinic of Obstetrics and Gynecology, Turkeyb Bakirkoy Dr Sadi Konuk Training and Research Hospital, Department of Pathology, Turkeyc Bakirkoy Dr Sadi Konuk Training and Research Hospital, Department of Obstetrics and Gynecology, Turkey
1. Introduction
Postoperative intra-abdominal adhesions occur in 50–95% of women who undergo gynecological surgery [1]. The developmentof peritoneal adhesions following abdominal and pelvic surgery
leads to clinical problems, including intestinal obstruction,infertility, and chronic pelvic pain [2]. Adhesions remain a
potential problem for future surgical procedures, increasing healthexpenses and hospital readmission rates, and reducing the quality
of life of the patient [3]. There are several described causes of adhesions, such as mechanical trauma, ischemia caused by suturesor electrocautery, presence of foreign bodies, tissue desiccation,
and infection [4]. Furthermore, during peritoneal healing followingsurgery, the increase in peritoneal fluid, cytokines, proteins and
fibrin formation can promote adhesion formation [5,6].Currently, there are various methods of preventing adhesion
formation such as the use of barrier materials, non-steroid anti-
inflammatory drugs, calcium channel blockers, corticosteroids,vitamin E, antihistamines, metformin, melatonin, progesterone,
estrogen, gonadotrophin-releasing hormone (GnRH)-agonists andantagonists, anticoagulants, fibrinolytic agents, and antibiotics [7–
10].Hyalobarrier1 gel is a highly viscous gel derived from
hyaluronan, obtained through an auto-crosslinking process, andused as an adhesion prevention agent in a variety of surgical
procedures [11–13]. Hyalobarrier1 gel can reduce the incidenceand severity of postoperative adhesions in cases of severe uterinedamage caused by laparotomy or laparoscopic myomectomies[14,15]. The gel can also be easily applied during laparoscopic and
hysteroscopic procedures.
European Journal of Obstetrics & Gynecology and Reproductive Biology 176 (2014) 44–49
A R T I C L E I N F O
Article history:
Received 7 December 2013
Received in revised form 3 February 2014
Accepted 14 February 2014
Keywords:
Surgical adhesions
Hyaluronic acid
Misoprostol
PGE1
TGF b1
A B S T R A C T
Objective: To investigate the effect of misoprostol in the reduction of adhesion formation aftergynecological surgery.Study design: A double blind, randomized controlled experimental study was designed. Twenty-onefemale Wistar Hannover rats were divided into three groups as control, misoprostol and Hyalobarrier1
groups. A uterine horn adhesion model was created. After anesthesia induction, 1.5–2 cm injuries were
made to the each uterine horn by cautery. The control group received no special medications except for
the standard surgical procedure. The misoprostol group received 10 mcg/kg misoprostol in addition tothe standard surgical procedure, and the Hyalobarrier1 group received 1 cm3 ready-for-useHyalobarrier1 gel intraperitoneally in addition to the standard surgical procedure. After 14 days from
the first surgical procedure, adhesion scores were evaluated.Results: The extent ( p < 0.001), severity ( p < 0.001), degree ( p < 0.001) and total adhesion score( p < 0.001) values of the control group were statistically higher than the values of misoprostol andHyalobarrier1 groups. The inflammation score value of misoprostol group was statistically lower than
control and Hyalobarrier1 groups ( p < 0.001).Conclusion: In this study, we have found a newtherapeuticpotentialof misoprostol that maybe useful in
preventing pelvic adhesion and reducing inflammation scores. 2014 Elsevier Ireland Ltd. All rights reserved.
* Corresponding author at: Van Ozalp State Hospital, Clinic of Obstetrics and
Gynecology, Cumhuriyet Mh., No. 3 Merkez Ozalp, Van, Turkey.Tel.: +90 212 414 73 72.
E-mail address: [email protected] (C. Kaya).
Contents lists available at ScienceDirect
European Journal of Obstetrics & Gynecology andReproductive Biology
j o u r n a l h o m e p a g e : w w w . e l s e v i e r . c o m / l o c a t e / e j o g r b
http://dx.doi.org/10.1016/j.ejogrb.2014.02.033
0301-2115/ 2014 Elsevier Ireland Ltd. All rights reserved.

8/19/2019 A Randomized Controlled Study of the Efficacy of Misoprostol
http://slidepdf.com/reader/full/a-randomized-controlled-study-of-the-efficacy-of-misoprostol 2/6
Misoprostol, a synthetic analog of prostaglandin E1, is used as
an anti-ulcer drug that increases gastric mucus secretion andreduces gastric acid secretion [16]. Misoprostol is also used off-label by obstetricians for the induction of first trimester abortion[17]. Misoprostol hasbeen shown to alter enzymaticprocessesthat
cause degradation and remodeling of collagen fibers [18].Nevertheless, no in vivo studies have demonstrated that miso-prostol can reduce adhesion formation. Misoprostol is commer-cially available as Cytotec1 (Ali Raif Ilac, Istanbul, Turkiye) in a
pharmaceutical complex with hydroxypropyl methylcellulose,microcrystalline cellulose, sodium starch glycolate, and hydroge-nated castor oil [19].
In this study, we aimed to investigate the effect of the
intraperitoneal use of misoprostol in the prevention of adhesionsby reducing collagen synthesis, which plays a major role in woundhealing and scar formation, compared with that of Hyalobarrier1
gel, which is known to prevent adhesions in clinical practice.
2. Materials and methods
The study was approved by the local ethical review board of the
Bagcilar Training and Research Hospital in Istanbul, Turkey, for theuse of laboratory animals, and was performed at the experimental
surgery training and education center of the same hospital(approval number: 2013–17).
2.1. Animal maintenance and treatment
Rats weighing approximately 180–260 g were housed under
the institutional review board’s guidelines for animal care using aday cycle of 14 h of light with free access to food and water. Apower analysis was performed to calculate the minimum sample
size required for the study (alpha error = 0.05 and 1-beta = 0.8) andat least 12 uterine horns were required for each study group. As10% of the animals are lost during the procedures, we included intotal 14 horns. The rats were randomly assigned to three study
groups, each consisting of seven rats, using computer-based
randomization. Twenty-one mature, nonpregnant, female WistarHannover rats (aged 8–10 weeks) were used as models for theexperimental induction of postoperative uterine horn adhesion, as
defined by Kelekci et al. [20]. Animals were anesthetized using50 mg/kg of 10% ketamine hydrochloride (Ketasol; Richter PharmaAG, Wels, Austria) intramuscularly(IM) and 5 mg/kg of 2% xylazine(Rompun; Bayer Health Care LCC, Kansas, KS) IM. Prior to the
operation, the abdominal skin was shaved and disinfected using10% povidone-iodine solution (Batticon; Adeka Laboratories,Istanbul, Turkey). A 3-cm midline incision was made, and theuterine horns were exposed. Seven standard lesions were inflicted
in the antimesenteric surfaces of each uterine horn using a 10 Wbipolar cautery (Bovie1, FL, USA). An area of 1.5 cm 1.5 cmbetween the two main vascular branches of the lower side wall at
the level of each uterine horn was cauterized to produce anopposing lesion. The first group of rats served as the control groupandreceived no special medication. The second group (misoprostolgroup) received 10 mcg/kg misoprostol intraperitoneally (IP) usinga diluted Cytotec1 200 mcg tablet (Ali Raif Ilac, Istanbul, Turkiye).
The third group (Hyalobarrier1 gel group) received 1 mL of ready-to-use Hyalobarrier1 gel (Fidia Advanced Biopolymers S.r.I AbanoTerme, Italy) IP. The abdominal incision was closed in two layerswith a 4-0 polyglycolic acid suture (VicrylTM; Johnson and Johnson
Medical Limited, Ethicon Limited, UK) for the peritoneum and 3-0polyglactin suture for the skin.
After the animals recovered from surgery, they were housedseparately under controlled temperatures of 22 2 8C and a 14 h
light cycle with food and water ad libitum. The surgery waslimited to
approximately 15 min for each rat to prevent tissue drying at room
temperature.All thesurgicalprocedures were performed by thesame
researchers.
2.2. Tissue sample collection and histopathology
Following the 14-day recovery period, the rats were sacrificedby cervical dislocation. The adhesion areas were evaluated andgraded macroscopically by two observers who were blinded to thestudy groups. The extent and severity of the adhesions were
evaluated using an established scoring system [21]. The extent of adhesion spread to the uterine horn defect was scored as follows:0, no uterine adhesion; 1, 1–25% involvement, 2, 26–50%involvement, 3, 51–75% involvement, and 4, 76–100% involve-
ment. Adhesions were further characterized on gross examinationaccording to the severity of attachment between the uterine hornsand other abdominal organs as follows: 0, no adhesion, 1, filmyavascular, 2, vascular or opaque, and 3, cohesive. The degree of
adhesion formation was evaluated and scored using the following;0, no adhesion; 1, the adhesion could be separated from the tissuewith gentle traction, 2, the adhesion could be separated from thetissue with moderate traction, 3, the adhesion could be separated
from the tissue by sharp dissection. The sum of the threeparameters was used as the total score for each group.
Tissue samples were obtained from all serosal surfaces whereadhesions had developed. One histologist evaluated all tissues and
was blinded to the origin of the samples. Tissues were graded forlevels of inflammation and fibrosis using previously publishedgrading scales. For histological analyses, the excised tissues werefixed in 10% buffered formalin solution for 24 h. After fixation, a
routine tissue-processing procedure was performed, and sampletissues were embedded in paraffin. Paraffin wax blocks were cutinto 4-mm thick sections. Prepared sections were then stained withhematoxylin and eosin, and levels of inflammation were scored as
follows: 0, no inflammation; 1, presence of giant cells, occasionallymphocytes, and plasma cells; 2, presence of giant cells, plasmacells, eosinophils, and neutrophils; and 3, presence of many
inflammatory cells and microabscesses. The level of fibrosis was
scored as follows: 0, no fibrosis; 1, minimal, loose; 2, moderate; 3,florid dense [22].
2.3. Immunohistochemistry
Slides were immunostained with 100mg of transforminggrowth factor beta-1 (TGF-b1) rat polyclonal antibody (Acris
Antibodies GmbH; Schillerstraße 5, D-32052 Herford, Germany).The sections were incubated at 65 8C for 1 h overnight.
Deparaffinization was performed using the following series of washes: two xylene washes (3 min each), two 100% ethanol rinses
(3 min each), and one wash each of 95% ethanol, 70% ethanol, 50%ethanol, 30% ethanol, and Tris-buffered saline with 0.05% Tween(TBST; 3 min each wash on a shaker).
For antigen retrieval, 500 mL of distilled water was added to apressure cooker. The slides were immersed in a staining dishcontaining the antigen retrieval solution and then placed in a de-cloaking chamber. Sodium citrate buffer (10 mM Sodium citrate,0.05% Tween 20, pH 6.0) was used as the antigen retrieval buffer.
The sections were boiled for approximately 10 min and cooled atroom temperature. The slides were then removed and rinsed inTBST.
For the staining procedure, the slides were washed with TBST
and covered with 3% hydrogen peroxide to inactivate theendogenous peroxidase. The slides were washed three times withTBST for 3 min each on a shaker and blocked with a universalprotein blocking solution for 1 h. The TGF-b1 rat antibody
(AP06350PU-N) was diluted to 1:50. The primary antibody was
applied to each section and incubated overnight in a humidified
C. Kaya et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 176 (2014) 44–49 45

8/19/2019 A Randomized Controlled Study of the Efficacy of Misoprostol
http://slidepdf.com/reader/full/a-randomized-controlled-study-of-the-efficacy-of-misoprostol 3/6
chamber at 4 8C. The slides were washed three times with TBST
(3 min each on a shaker). Secondary HRP-conjugated antibodydiluted in the blocking solution was applied to each section as perthe manufacturer’s recommendations and incubated for 30 min at
room temperature. The slides were washed three times with TBST
(5 min each on a shaker) and incubated with freshly prepared 3,30-diaminobenzidine substrate until the stain developed. The sectionswere rinsed with water and counterstained with hematoxylin.
Table 1
Comparison of clinical, histopathological and immunohystochemistry scores of the control, misoprostol and Hyalobarrier1 groups.
Parameters Control group Misoprostol group Hyalobarrier1 group p-Value
Number of uterine horns 14 14 14
Clinical adhesion score
Extent score 2.29 0.73 [2 (1–3)] 0.860.86 [1 (0–2)] 0.860.86 [1 (0–2)] 0.0001Severity score 2.29 0.73 [2 (1–3)] 0.860.86 [1 (0–2)] 0.860.86 [1 (0–2)] 0.0001
Degree score 2.14 0.86 [2 (1–3)] 0.860.86 [1 (0–2)] 0.860.86 [1 (0–2)] 0.0001
Total score 6.712.13 [7 (3–9)] 2.572.59 [3 (0–6)] 2.572.47 [3 (0–6)] 0.0001
Histopathological scoreInflammation 2 0 [2 (2–2)] 1.430.51 [1 (1–2)] 2.140.36 [2 (2–3)] 0.0001
Fibrosis 1.29 0.47 [1 (1–2)] 1.430.51 [1 (1–2)] 1.290.47 [1 (1–2)] 0.658
Immunohystochemistry
TGF b1 antibody 1 0.78 [1 (0–2)] 0.710.47 [1 (0–1)] 0.860.66 [1 (0–2)] 0.581
TGF b1, transforming growth factor beta 1.
[
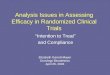
Fig. 1. Clinicaladhesion scoring.(a) No uterineadhesion, (b)1–25% involvement,filmy avascular, theadhesion could be separated fromtissuewith gentle traction, (c)26–50%
involvement,vascular and opaque, the adhesioncould be separated fromtissue withmoderate traction,and (d) 51–75% involvement,cohesive attachment of uterine hornto
each other or other abdominal organs, requiring sharp dissection.
C. Kaya et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 176 (2014) 44–4946

8/19/2019 A Randomized Controlled Study of the Efficacy of Misoprostol
http://slidepdf.com/reader/full/a-randomized-controlled-study-of-the-efficacy-of-misoprostol 4/6
Samples were then dehydrated by two washes with 100% ethanol
(3 min each) and two rinses with xylene (3 min each). The slideswere mounted with cover slips and all sections examined using alight microscope. Five randomly chosen fields of each horn wereexamined, and the number of positively stained cells among
100 cells was counted. A total of 500 cells were counted for eachhorn. The percentage of immunoreactive cells was recorded by anestablished scoring systemas follows: 0, negative; 1,<33% positivestaining; 2, 33–66% positive staining; 3, >66% positive staining
[23].
2.4. Statistical analysis
Statistical data analysis was performed using the NCSS 2007Statistical Software (Number Cruncher Statistical System; NCSSLLC, Kaysville, UT 84037, USA). Descriptive statistical methods(mean, standard deviation, min–max measurements) were used
for data analysis. The Kruskal–Wallis test was used to comparedifferences in scores between the groups and the Dunn test wasused to compare differences between subgroups. A p-value of
<0.05 was considered statistically significant.
3. Results
3.1. Macroscopic clinical adhesion scores
Total clinical adhesion formation scores were evaluated for thecontrol, misoprostol, and Hyalobarrier1 groups, and the scores
were 6.71 2.13, 2.57 2.59, and2.57 2.47 respectively (Table 1).
A statistically significant difference was found between the miso-
prostol and Hyalobarrier1 groupscomparedwith thecontrol group in
the total adhesion scores ( p = 0.0001), extent scores ( p = 0.0001), and
severity scores ( p = 0.0001). However, there was no significant
difference in these parameters between the misoprostol group and
the Hyalobarrier1 group. The scores for the degree of adhesion
formation were 2.14 0.86, 0.86 0.86, and 0.86 0.86 for the
control, misoprostol, and Hyalobarrier1 groups, respectively. A
statistically significant difference in these scores was noted between
themisoprostol andcontrol groups ( p = 0.002) and the Hyalobarrier1
and control groups ( p = 0.002), but there was no statistically
significant difference in this parameter between the misoprostol
and Hyalobarrier1 groups (Table 2 and Fig. 1A–D).
3.2. Microscopic histological features
The median histological inflammation scores were 2 0,
1.43 0.51, and 2.14 0.36 for the control, misoprostol, and
Hyalobarrier1 groups, respectively (Table 1). The inflammation score
of the misoprostol group was significantly lower than that of the
control and Hyalobarrier1 groups ( p = 0.0001) (Table 2). However,
there was no significant difference in the inflammation scores
between the control and Hyalobarrier1 groups(Fig.2A–D). There was
also no significant difference in the fibrosis score and immunohis-
topathological scoring with TGF-b1 (Fig. 3A and B) between the study
groups.
Table 2
Comparison of p values for clinical adhesion scores and inflammation scores of the
control, misoprostol and Hyalobarrier1 groups.
Dunn test Control group/
misoprostol
group
Control group/
Hyalobarrier1
group
Control group/
Hyalobarrier1
group
Extent score 0.0001 0.0001 0.999
Severity score 0.0001 0.0001 0.999
Degree score 0.002 0.002 0.999
Total score 0.0001 0.0001 0.999Inflammation 0.001 0.150 0.001
[
Fig. 2. Histopathologicalinflammation evaluation of adhered tissues. Hematoxylin and eosin 200. (a) Giant cellformation, (b) microabscesses formation, (c) minimal, loose
fibrosis, and (d) moderate fibrosis.
C. Kaya et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 176 (2014) 44–49 47

8/19/2019 A Randomized Controlled Study of the Efficacy of Misoprostol
http://slidepdf.com/reader/full/a-randomized-controlled-study-of-the-efficacy-of-misoprostol 5/6
4. Comment
Development of postoperative adhesions remains a majorhealthcare problem causing relaparotomy complications, extend-ed operation time, additional blood loss, and unexpected visceral
damage [24]. Adhesions occur after damage to the mesothelialcells on the serosal surface of tissues, followed by inflammation
with the release of cytokines, and the formation of a soft fibrin gelmatrix. If this softfibrin is not fractioned and fibrinolytic activity is
insufficient, dense fibrinous and vascular changes develop withintwo weeks [5]. To minimize this undesirable fibrin formation,several approaches have been suggested. These include minimiz-ing the tissue injury, removing the fibrin, and inhibiting the
proliferation of fibroblasts at the injured site [10]. A number of agents have been studied for this purpose, such as fibrinolyticagents to reduce the fibrinous mass, nonsteroidal anti-inflamma-tory drugs, corticosteroids, statins, metformin, methylene blue,
cyclooxygenase-2 inhibitors, PPARc and VEGF receptor inhibitors,anti-oxidants, aromatase inhibitors, GnRH-agonists, and humanamniotic membrane. There is, however, no optimal method for
adhesion prevention [5,10,20,25–29].
Hyaluronan (or hyaluronic acid) derivatives prevent adhesionsby reducing fibrin formation and promoting the production of peritoneal mesothelial cells [11]. Hyalobarrier1 is a reported
adhesion-preventing agent [15]. Furthermore, a systematic reviewand meta-analysis reported that the application of the auto-crosslinked hyaluronan gel significantly reduced the incidence of intraperitoneal adhesions after laparoscopic myomectomy and
incidence of intrauterine adhesions after hysteroscopy [11].Hyalobarrier1 gel is also useful in its simple, ready-to-use form.In a multicenter study, Hyalobarrier1 did not significantly prolongoperating time, and the mean application time of the product was
two minutes [30]. In ourinstitution, Hyalobarrier1 gel isused asanadhesion-preventing agent in routine surgical procedures.
Misoprostol, a drug that is commonly used by obstetricians for
the induction of labor and facilitation of cervical dilation beforeintrauterine procedures, alters the microstructural architectureand enzymatic processes of collagen [16]. In our study, we showedthat both misoprostol and Hyalobarrier1 significantly reduced theclinical adhesion score compared with that of the control group. To
the best of our knowledge, this is the first study evaluating theeffect of misoprostol on adhesion prevention. Fibrin formationfollowing the inflammatory process is believed to be the majorfactor in the development of surgical adhesions. This inflammatory
process begins after tissue damage and lasts throughout collagenfiber synthesis that enhances scar formation [10]. Although themechanism of action of misoprostol in reducing collagen fiberformation has not been completely described, we found that the
histopathological inflammation score of the misoprostol group
was significantly lower than that of the Hyalobarrier
1
and control
groups. We can speculate that misoprostol may prevent adhesion
by reducing the action of inflammatory cytokines involved in thefirst step of fibrin formation.
In our study, we also performed fibrosis scoring and TGF-b1 ratantibody immunohistochemistry scoring. TGF-b1 has a well-
described role in cell differentiation, in triggering angiogenesis,and as a fibroblast activator in the inflammatory response [31].
However, there was no significant difference found in the TGF-b1antibody immunohistochemistry scores between the control and
treatment groups. We postulate that, as a limitation of our study,the recovery period following the initial surgery was 14 days,which is the minimum stabilization time limit for collagensynthesis. Collagen band formation typically begins 3–5 days
following trauma and increases until stabilization at approximate-ly day 14 [32]. Therefore, assessments should be performed after14 days to provide more accurate immunohistochemistry results.
Most adhesion-preventing agents are administered locally in
daily surgical practice [30]. In our study, the preferred route of administration was IP because surgeons generally prefer applyingagents via small instruments to prevent adhesion during
minimally invasive surgical techniques. We used 10 mcg/kg of a
Cytotec1 tablet, as this was the described minimal dose of intraperitoneal misoprostol to produce its gastroprotective effect[33].
The limitations of our study are that the required dose of misoprostol was obtained by dissolving a Cytotec1 200 mcg tabletin distilled water and that the effects of the tablet components onadhesion prevention or formation are unknown. The optimal dose
and administration route of misoprostol are also unknown;therefore, pharmacokinetic studies should be performed on theuse of misoprostol in preventing pelvic adhesions. Moreover, thecellular and molecular interactions of misoprostol in this situation
need to be investigated further.
Conflicts of interest statement
The authors have no conflicts of interest to declare.
Acknowledgements
We are grateful to thank to Aysenur Turan for her technicalsupport and to Rana Konyalioglu for statistical analyses of the data.
References
[1] Hellebrekers BWJ, Trimbos-Kemper GCM, Blitterswijk VCA, Bakkum EA, Trim-bos JBMZ. Effects of five different barrier materials on postsurgical adhesionformation in the rat. Hum Reprod 2000;15:1358–63.
[2] Aritas Y, Akcan A, Erdogan AR, Akgun H, Saraymen R, Akyildiz H. Effects of
melatonin and phospholipid on adhesion formation and correlation with
[
Fig. 3. Histopathological TGFb1 antibodyevaluation of adhered tissues. (a) TGFb1 antibody400, 1–33% involvement and (b) TGFb1 antibody 400, 34–66% involvement.
C. Kaya et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 176 (2014) 44–4948

8/19/2019 A Randomized Controlled Study of the Efficacy of Misoprostol
http://slidepdf.com/reader/full/a-randomized-controlled-study-of-the-efficacy-of-misoprostol 6/6
vascular endothelial growth factor expression in rats. UlusTravmaAcil CerrahiDerg 2009;15:416–22.
[3] Kossi J, Salminen P, Rantala A, Laato M. Population based study of the surgicalworkload and economic impact of bowel obstruction caused by postoperativeadhesions. Br J Surg 2003;90:1441–4.
[4] Ferland R, Mulani D, Campbell PK. Evaluation of a sprayable polyethyleneglycol adhesion barrier in a porcine efficacy model. Hum Reprod2001;16:2718–23 .
[5] Moraloglu O, Isık H, Kılıc S, et al. Effect of bevacizumab on postoperativeadhesion formation in a rat uterine horn adhesion model and the correlationwith vascular endothelial growth factor and Ki-67 immunopositivity. Fertil
Steril 2011;95:2638–41.[6] Demirbag S, Cetinkursun S, Tasdemir U, Ozturk H, Pekcan M, Yesildaglar N.Comparison of hyaluronate/carboxymethylcellulose membrane and melato-nin for prevention of adhesion formation in a rat model. Hum Reprod2005;20:2021–4 .
[7] Wallwiener M, Brucker S, Hierlemann H, Brochhausen C, Solomayer E, Wall-wiener C. Innovative barriers for peritoneal adhesion prevention: liquid orsolid? A rat uterine horn model. Fertil Steril 2006;86(Suppl. 3):1266–76.
[8] Yeo Y, Highleya CB, Bellasa E, et al. In situ cross-linkable hyaluronic acidhydrogels prevent post-operative abdominal adhesions in a rabbit model.Biomaterials 2006;27:4698–705.
[9] Ahmad G, Duffy JMN, Farquhar C, et al. Barrier agents for adhesion preventionafter gynaecological surgery. Cochrane Database Syst Rev 2008;16:CD000475.
[10] Yilmaz B, Aksakal O, Gungor T, et al. Metformin and atorvastatin reduceadhesion formation in a rat uterine horn model. Reprod Biomed Online2009;18:436–42 .
[11] Mais V, Cirronis MG, Peiretti M, Ferrucci G, Cossu E, Melis GB. Efficacy of auto-crosslinked hyaluronan gel for adhesion prevention in laparoscopy and hys-teroscopy: a systematic review and meta-analysis of randomized controlled
trials. Eur J Obstet Gynecol Reprod Biol 2012;160:1–5.[12] De Iaco PA, Muzzupapa G, Bovicelli A, et al. Hyaluronan derivative gel
(Hyalobarrier gel) in intrauterine adhesion (IUA) prevention after operativehysteroscopy. Ellipse 2003;19:15–8.
[13] Pellicano M, Bramante S, Cirillo D, et al. Effectiveness of autocrosslinkedhyaluronic acid gel after laparoscopic myomectomy in infertile patients: aprospective, randomized, controlled study. Fertil Steril 2003;80:441–4.
[14] Acunzo G, Guida M, Pellicano M, et al. Effectiveness of autocross-linkedhyaluronic acid gel in the prevention of intrauterine adhesions after hystero-scopic adhesiolysis: a prospective,randomized, controlled study. Hum Reprod2003;18:1918–21.
[15] Pellicano M, Guida M, Bramante S, et al. Reproductive outcome after auto-crosslinked hyaluronic acid gel application in infertile patients who under-went laparoscopic myomectomy. Fertil Steril 2005;83:498–500.
[16] Cavallini ME, Andreollo NA, Metze K, Arau jo MR. Omeprazole and misoprostolforpreventinggastricmucosaeffects causedby indomethacinand celecoxib inrats. Acta Cir Bras 2006;21:168–76.
[17] Surbek DV, Fehr PM, Hosli I, Holzgreve W. Oral misoprostol for third stage of labor: a randomized placebo-controlled trial. Obstet Gynecol 1999;94:255–8.
[18] Shetty A, Danielian P, Templeton A. Sublingual misoprostol forthe inductionof laborat term. Am J Obstet Gynecol 2002;186:72–6.
[19] Jain JK, Mishell DR. A comparison of intravaginal misoprostol with prosta-glandin E2 for termination of second-trimester pregnancy. N Engl J Med1994;331:290–3.
[20] Kelekci S, Uygur D, Yilmaz B, Sut N, Yesildaglar N. Comparison of humanamniotic membrane and hyaluronate/carboxymethylcellulose membrane forprevention of adhesionformation in rats. ArchGynecol Obstet 2007;276:355–9.
[21] Leach RE, Burns JW, Dawe EJ, et al. Reduction of postsurgical adhesionformation in the rabbit uterine horn model with use of hyaluronate/carboxy-
methylcellulose gel. Fertil Steril 1998;69:415–8.[22] Hooker GD, Taylor BM, Driman DK. Prevention of adhesionformation withuseof sodium hyaluronate-based bioresorbable membrane in a rat model of ventral hernia repair with polypropylene mesh – a randomized, controlledstudy. Surgery 1999;125:211–6.
[23] Coppola D, Lu L, Fruehauf JP, et al. Analysis of p53, p21WAF1, and TGF- b1 inhuman ductal adenocarcinomaof thepancreas.Am J ClinPathol1998;110:16–23.
[24] Liakakos T, Thomakos N, Fine PM, Dervenis C, Young RL. Peritoneal adhesions:etiology, pathophysiology, and clinical significance. Recent advances in pre-vention and management. Dig Surg 2001;18:260–73.
[25] Nappi C, Di Spiezio Sardo A, Greco E, et al. Prevention of adhesions ingynaecological endoscopy. Hum Reprod Update 2007;13:379–94.
[26] Watson A, Vandekerckhove P, Lilford R. Liquid and fluid agents for preventingadhesions after surgery for subfertility. Cochrane Database Syst Rev2000;2:CD001298.
[27] Aksakal O, Yilmaz B, Gungor T, et al. A randomised controlled trial onmelatonin and rosiglitazone for prevention of adhesion formation in a ratuterine horn model. Arch Gynecol Obstet 2010;282:55–61.
[28] Kaya U, Oktem M, Zeyneloglu HB, Ozen O, Kuscu E. Impact of aromataseinhibitors on adhesion formation in a rat model. Fertil Steril 2007;87:934–9.
[29] Kalaycı MU, Eroglu HE, Kubilay D, et al. The effects of methylene blue onadhesion formation in a rat model of experimental peritonitis. Ulus TravmaAcil Cerrahi Derg 2011;17:205–9.
[30] Lundorff P, Donnez J, Korell M, Audebert AJM, Block K, diZerega GS. Clinicalevaluation of a viscoelastic gel for reduction of adhesions following gynae-cological surgery by laparoscopy in Europe. Hum Reprod 2005;20:514–20.
[31] Culhaci N, Sagol O, Karademir S, et al. Expression of transforming growthfactor-beta-1 and p27Kip1 in pancreatic adenocarcinomas: relation with cell-cycle-associated proteins and clinicopathologic characteristics. BMC Cancer2005;5:98.
[32] Keskin HL, Sirin YS, Keles H, Turgut O, Ide T, Avsar AF. The aromatase inhibitorletrozole reduces adhesion formation after intraperitoneal surgery in a ratuterine horn model. Eur J Obstet Gynecol Reprod Biol 2013;167:199–204.
[33] Chang FY, Chen TS, Lee SD, Doong ML, Wang PS. Misoprostol-inhibited ratgastric emptying is independent of gastric inhibitory polypeptide release.Pharmacology 1999;58:265–9.
C. Kaya et al. / European Journal of Obstetrics & Gynecology and Reproductive Biology 176 (2014) 44–49 49