Embed Size (px)
Citation preview
A RETROSPECTIVE REVIEW OF DENTAL IMPLANT SUPPORTED PROSTHESES
RESTORED IN A PROSTHODONTIC RESIDENCY PROGRAM IN THE UNITED
STATES OF AMERICA By
Kavitha P. Das, B.D.S., M.P.H., M.S.
Edited byJames M. Soberman, M.S., D.D.S., F.A.G.D, F.A.C.D
January 2011
SAHITYA BHAWAN PUBLISHERS & DISTRIBUTORS (P) LTD.
1
© Author
Printing and Publishing rights with the Publisher.No part of this book may be reproduced or copied in any form or by any means without the
written permission of the author and publisher. Breach of this condition is liable for legal action. The jurisdiction for all legal disputes shall be Agra only.
Book Code: 0071
“The reading of all good books is like a conversation with the finest men.”
Price :Rs.100.00
Note : Due care has been taken while editing and printing this book, neither the author nor the publisher of the book hold any responsibility for any mistake or error that may have inadvertently crept in and for the consequences of any action or decision taken on the basis of this book.
Published & Printed by
SAHITYA BHAWANPUBLISHERS & DISTRIBUTORS (P) LTD.34, Lajpat Kunj, Civil Lines, Agra-282 002 (U.P.)Mobile : 8810108090, E-mail : [email protected]
Visit us at: www.sahityabhawan.in.
2
Contents
Abstract…………………………………………………………………………..
Introduction………………………………………………………………………
Background………………………………………………………………………
Purpose…………………………………………………………………………...
Materials and Methods……………………………….…………………………..
Results…………………………………………………………………………….
Discussion………………………………………………………………………..
Conclusion………………………………………………………………………..
Appendix………………………………………………………………………….
References………………………………………………………………………..
3
Acknowledgements
I would like to thank the faculty, staff and colleagues who assisted in the completion
of the project
4

Abstract
Introduction
This report describes the outcomes of a retrospective chart review on dental
implant supported prostheses restored in the Department of Prosthodontics at
Columbia University College of Dental Medicine. The purpose of this review is to
evaluate the success rate of implants restored in a prosthodontic residency program
in a university setting, and assess post insertion visits and complications with
respect to the restored implants. Socio economic data, relevant medical and dental
information was collected and reviewed. For this retrospective study, the
prostheses were categorized as single implant crowns, implant supported fixed
partial dentures, complete fixed implant supported prostheses and complete
removable implant supported prostheses.
This report is phase I of a two phase study. Phase I includes a comprehensive chart
review.
Materials and Methods
All charts of patients treated in the Department of Prosthodontics from the year
2001 to 2006 were included in this study. A total of 101 charts were reviewed and
68 charts were narrowed down for the purpose of this study. Charts that did not
have information on the patient’s treatment plan were excluded from the 101 charts
reviewed.
5
Results
A total of three hundred and sixty implants were restored with an implant success
rate of 97.5%. More women were treated in the Department of Prosthodontics when
compared to men. The mean age of the patient was 61 years. The most frequently
restored dental implant was Biomet3I Osseotite, with implant single crowns
forming the largest group of prostheses restored. Hispanics and Whites formed the
most frequently treated groups of patients in this department, followed by Asians;
and self pay and Medicaid were the largest payment methods. Periodontal problems
followed by crowns on natural teeth were the most frequent dental history
recounted; hypertension followed by penicillin allergy were the most frequently
encountered medical complications; calcium supplements and multivitamins were
the medications listed most regularly; forty six percent stated that comprehensive
care and 30% stated the need for implant retained restoration as their chief
complaint. Panoramic radiographs were the most requested radiographs. The
average duration of treatment was 1.9 years and implant failure was the most
commonly seen implant related complication.
Limitations of the study
The major drawback of this study is the small sample size (68). A larger sample
would more accurately reveal the breakdown of various treatment options provided
to the patients.
6
Introduction
Osseointegrated dental implants have changed the approach to dental treatment.
The number of dental implants placed in the United States has increased, and it is
estimated that the field of implant dentistry will continue to grow by approximately
12% annually.1 The American Dental Association has reported the average survival
rates of multiple implant designs placed in various clinical situations as more than
90%.2 It has been estimated that more than 90% of surgical specialty dentists place
implants, 90% of prosthodontists restore implants, and 78% of general dentists
have used implants to support fixed and removable prosthesis compared to 65%
fifteen years ago. 3 The increased acceptance of dental implant treatment is
attributable to several factors, including patient’s expectations and acceptance,
endorsement by dentists and increased predictability of implant-supported
restorations.4,5
Background
In 1951, in Lund, Sweden, Dr. Branemark, an orthopedic surgeon discovered that it
was extremely difficult to recover bone-anchored titanium chambers that were
embedded in bone as a part of a vital microscopic animal and human study. The
titanium had seemingly bonded to living bone tissue. Dr. Branemark successfully
demonstrated that under carefully controlled conditions titanium could be
structurally integrated into living bone with a very high degree of predictability and,
7
without long-term soft tissue inflammation or ultimate fixture rejection. Dr.
Branemark named the phenomenon osseointegration. The first practical application
of osseointegration was the implantation of new titanium roots in an edentulous
patient in 1965. The discovery of use of titanium as the material of choice for
implantation was also a chance discovery. Dr. Emneus an orthopedic surgeon who
was studying various metals for hip-joint replacement introduced it to Dr.
Branemark. 6
More than forty years later, the field of dental implants has grown exponentially.7, 8
The vast majority of dental implants can be simply defined as a titanium screw that
is placed within the jawbone allowing a crown, fixed partial denture or complete
denture to be attached to it. Early implants used in the mid-twentieth century came
in a variety of shapes. These varied from implant frameworks that rested in direct
contact with the bone beneath the soft tissues, to blade shaped implants that were
placed within the alveolar bone. Most implants are commonly cylindrically shaped,
and are usually placed into a pre-prepared site within the maxillary or mandibular
bone.9
Purpose
Given the current trend in increased implant utilization by specialists and general
dentists, it is imperative that dental school curriculum in the United States includes
comprehensive training in implant dentistry. A few studies have been published on
the training provided in dental school settings. These studies have reported that the
implant survival of dental implants placed in a university setting is comparable to
8
implants placed by experienced clinicians 1,10 and that the implant success rate does
not vary depending on the implant system used. According to a study on pre
doctoral implant dentistry training in the United States published by Lim et al in
2008 11, 84 % of the schools reported that implant dentistry is part of the
curriculum, and 75% of the schools reported that the training provided was for an
average of 5.5 months.
Research has been carried out on the success or failure of different implant
supported prostheses, however, this has not been evaluated in university settings in
prosthodontic residency programs. Research needs to be carried out on implant
prostheses design and related factors in a prosthodontic residency setting.
The purpose of this report is to present the outcomes of phase I of a retrospective
study on dental implants restored in a prosthodontic residency in a university
setting in the United States. The first phase comprised of a chart review of patients
who had dental implants restored at the Department of Prosthodontics at Columbia
University College of Dental Medicine.
Materials and Methods
The study population consisted of patients treated at the Department of
Prosthodontics at Columbia University College of Dental Medicine from the year
2001 to 2006.
9
Phase I:
A chart review:
The chart review included a comprehensive overview of the study subjects
background, medical history, dental history, insurance type and implant prostheses
related information. Information on nineteen variables was collected.
Patients registered in the Department of Prosthodontics were identified using
billing codes used to delineate various procedures for prosthetic treatment. From
this master list, charts retained in the chart room were identified and selected based
on their availability in the chart room. Nineteen variables were identified as
relevant to the study and the data was entered into an excel spreadsheet.
Appendix 1 - list of variables collected from the chart review.
Phase II:
Clinical and radiographic evaluation of the implant supported prostheses:
The clinical evaluator measuring clinical parameters will fill out a questionnaire and
will assess different clinical parameters on prostheses and implant supported
prostheses success/failure will complete the questionnaire. This questionnaire will
address specific clinical variables related to the prosthesis and will include
radiographic evaluation of the prostheses as well as complications associated with
the prostheses.
Appendix 2 -lists details on the clinical variables to be included in the study.
10
A self-administered questionnaire on OHRQOL to be filled out by the study subject:
The use of a validated instrument strengthens a study .The OHRQOL will be
measured using the validated instrument, the Oral Health Impact Profile (OHIP).
The OHIP was developed with the aim of providing a comprehensive measure of
self-reported dysfunction, discomfort and disability attributed to oral conditions.
These impacts were intended to complement traditional oral indicators of clinical
disease. 12 The questionnaire will also collect data on each study member’s
occupation, education, income and related socio-demographic information. This
questionnaire will be administered to the patient.
Appendix 3- OHIP-14.
This report will enumerate the results of phase I- the chart review.
Results
A total of 101 charts were reviewed and 68 charts were narrowed down for the
purpose of this study. Charts that did not include treatment plan details were
excluded from the study.
Socio Demographic Variables:
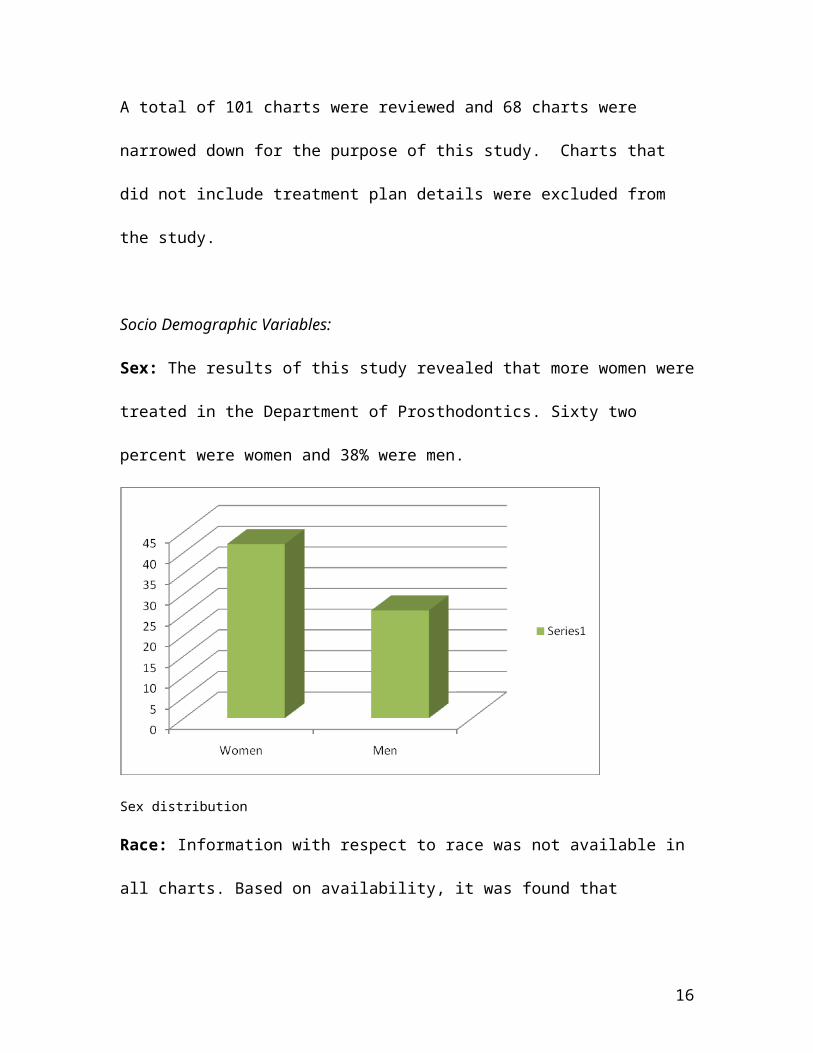
Sex: The results of this study revealed that more women were treated in the
Department of Prosthodontics. Sixty two percent were women and 38% were men.
11
Sex distribution
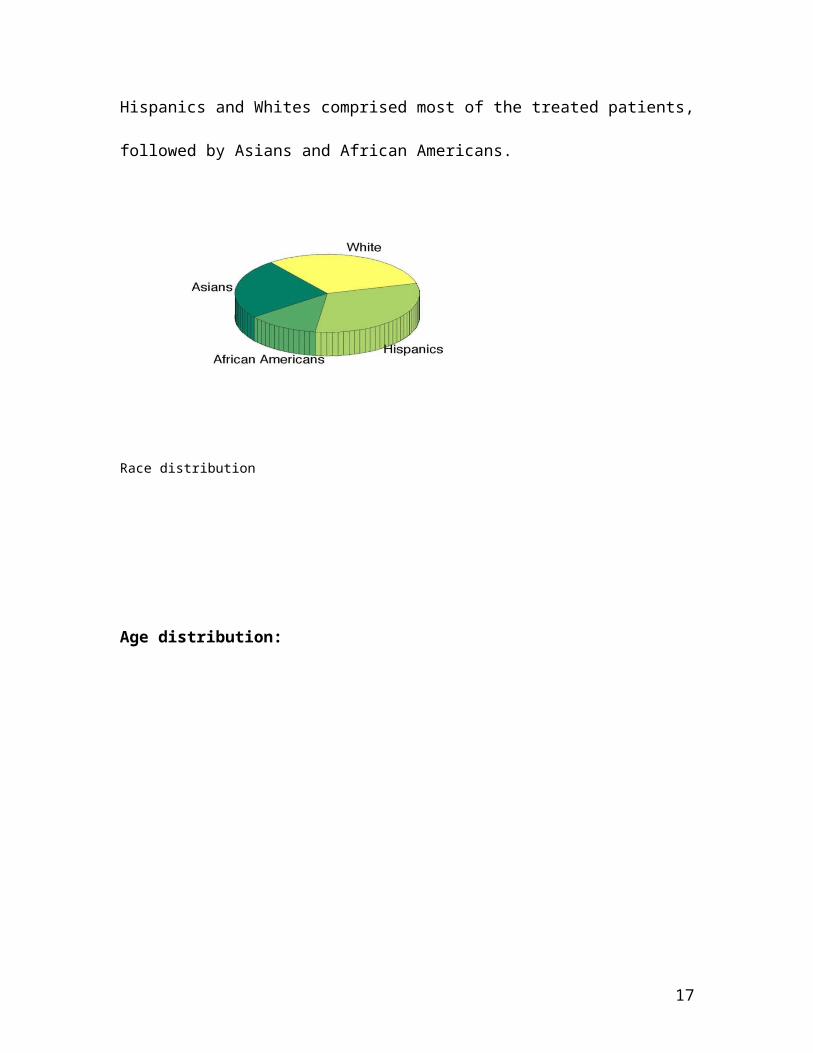
Race: Information with respect to race was not available in all charts. Based on
availability, it was found that Hispanics and Whites comprised most of the treated
patients, followed by Asians and African Americans.
Race distribution
12
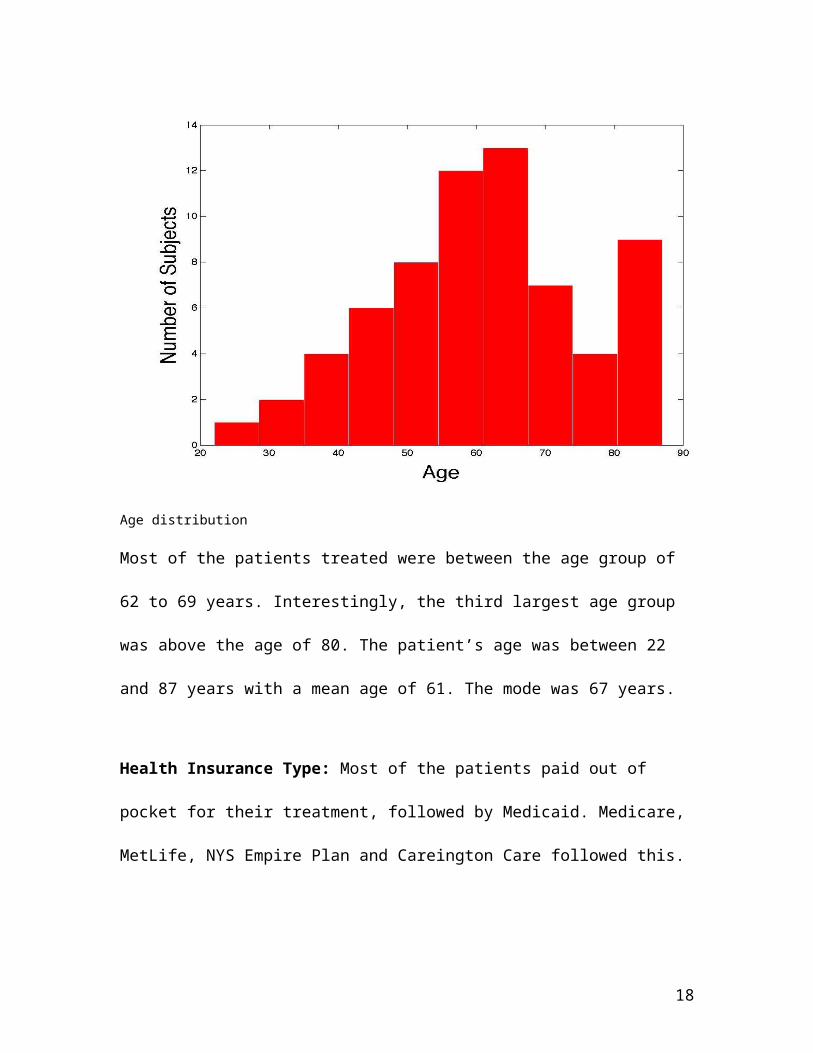
Age distribution:
Age distribution
Most of the patients treated were between the age group of 62 to 69 years.
Interestingly, the third largest age group was above the age of 80. The patient’s age
was between 22 and 87 years with a mean age of 61. The mode was 67 years.
Health Insurance Type: Most of the patients paid out of pocket for their treatment,
followed by Medicaid. Medicare, MetLife, NYS Empire Plan and Careington Care
followed this.
13
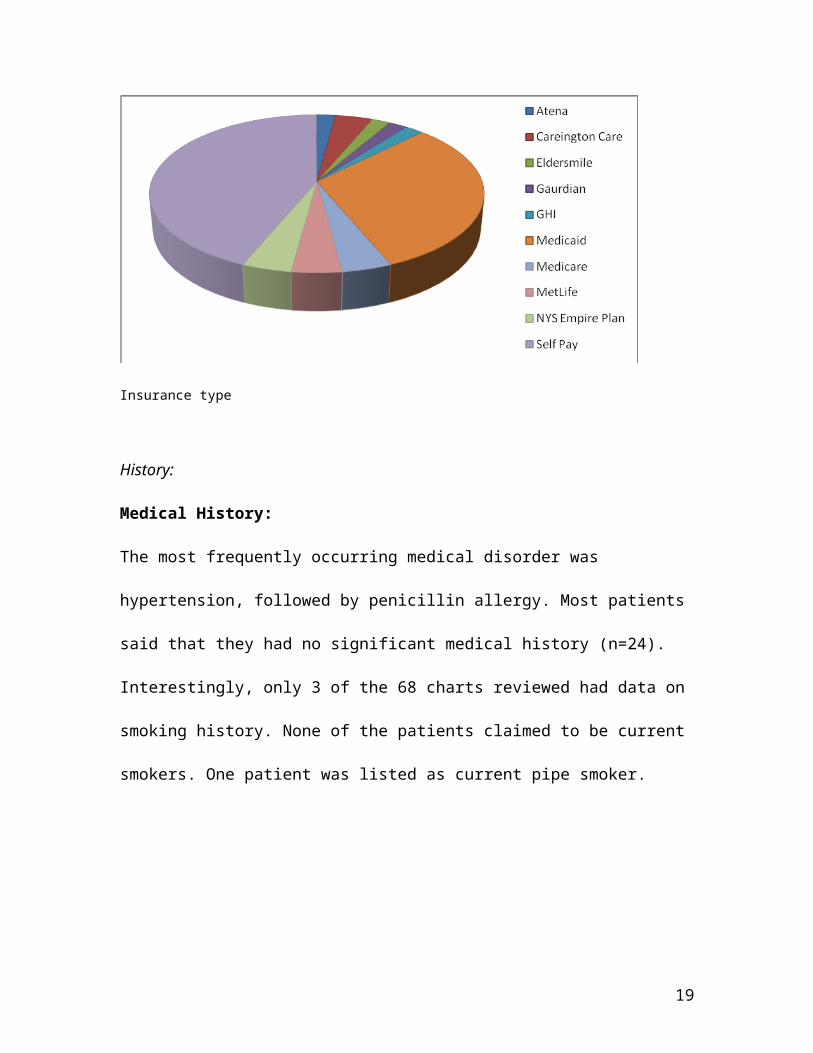
Insurance type
History:
Medical History:
The most frequently occurring medical disorder was hypertension, followed by
penicillin allergy. Most patients said that they had no significant medical history
(n=24). Interestingly, only 3 of the 68 charts reviewed had data on smoking history.
None of the patients claimed to be current smokers. One patient was listed as
current pipe smoker.
14
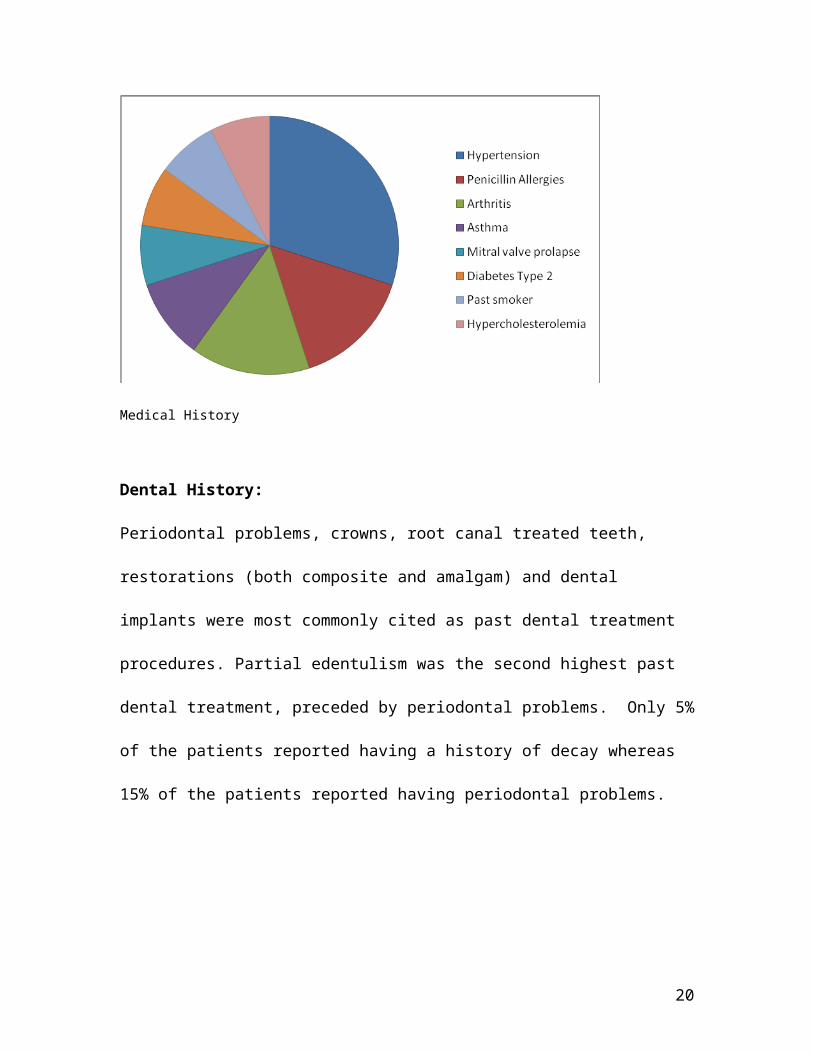
Medical History
Dental History:
Periodontal problems, crowns, root canal treated teeth, restorations (both
composite and amalgam) and dental implants were most commonly cited as past
dental treatment procedures. Partial edentulism was the second highest past dental
treatment, preceded by periodontal problems. Only 5% of the patients reported
having a history of decay whereas 15% of the patients reported having periodontal
problems.
15
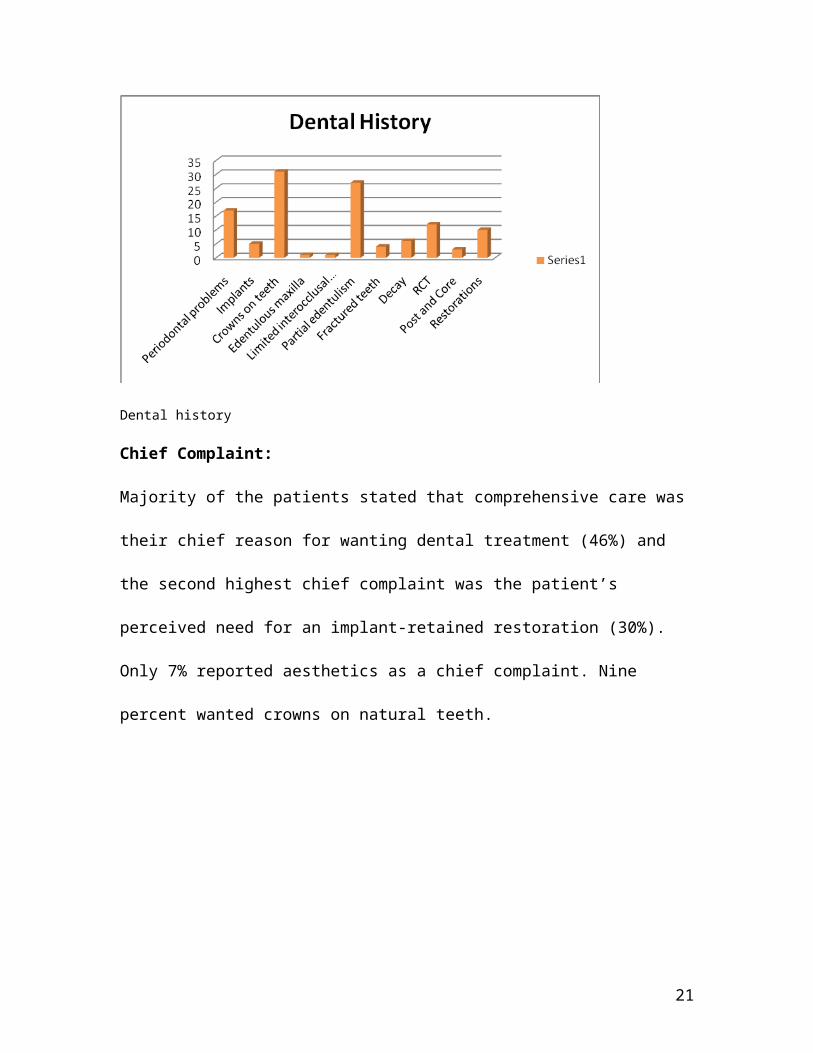
Dental history
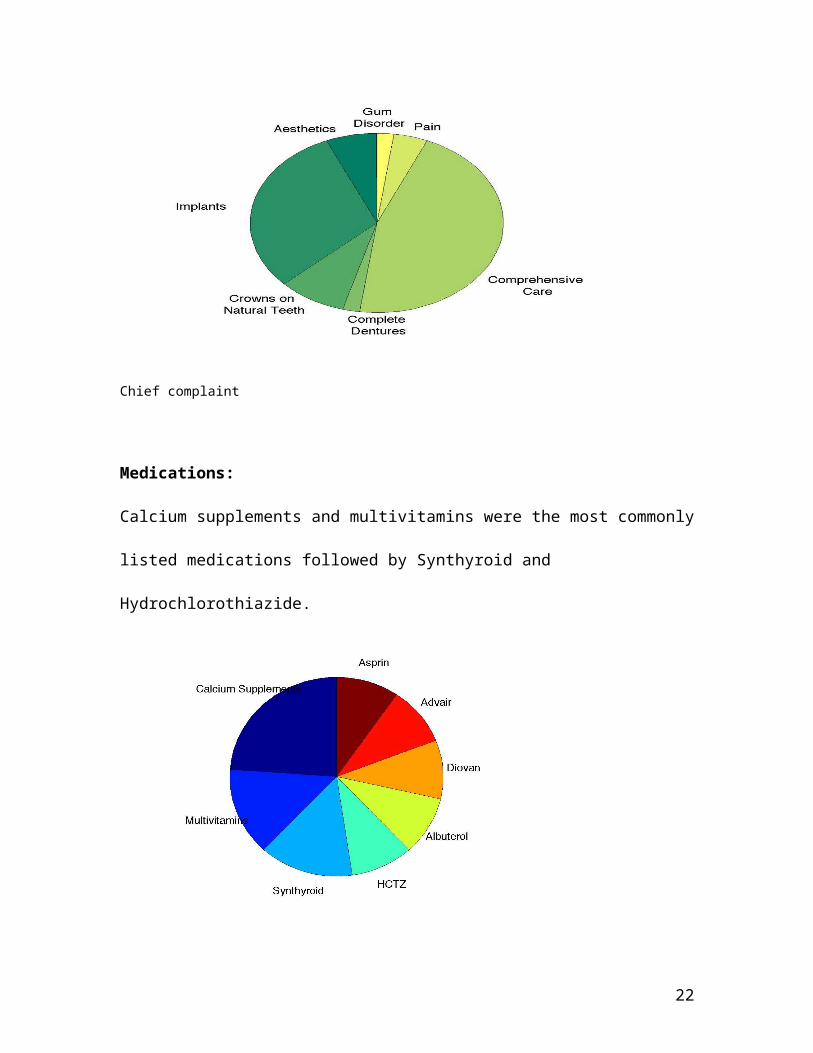
Chief Complaint:
Majority of the patients stated that comprehensive care was their chief reason for
wanting dental treatment (46%) and the second highest chief complaint was the
patient’s perceived need for an implant-retained restoration (30%). Only 7%
reported aesthetics as a chief complaint. Nine percent wanted crowns on natural
teeth.
Chief complaint
16
Medications:
Calcium supplements and multivitamins were the most commonly listed
medications followed by Synthyroid and Hydrochlorothiazide.
Medications
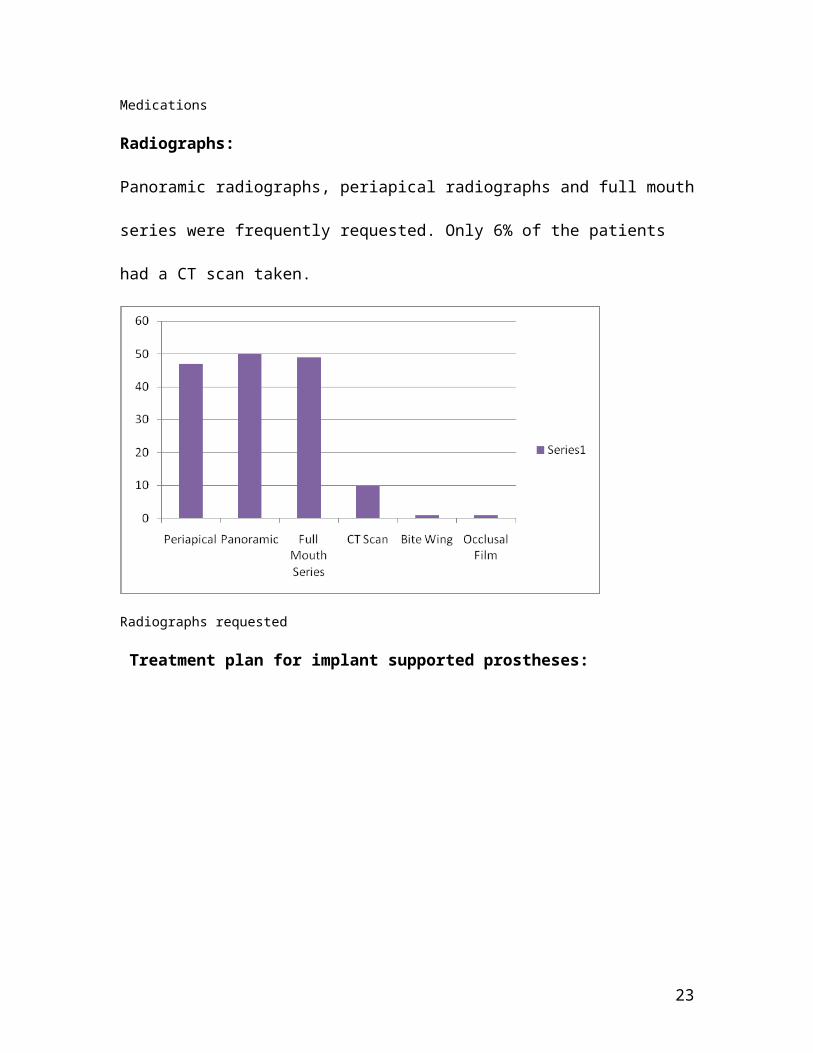
Radiographs:
Panoramic radiographs, periapical radiographs and full mouth series were
frequently requested. Only 6% of the patients had a CT scan taken.
17
Radiographs requested
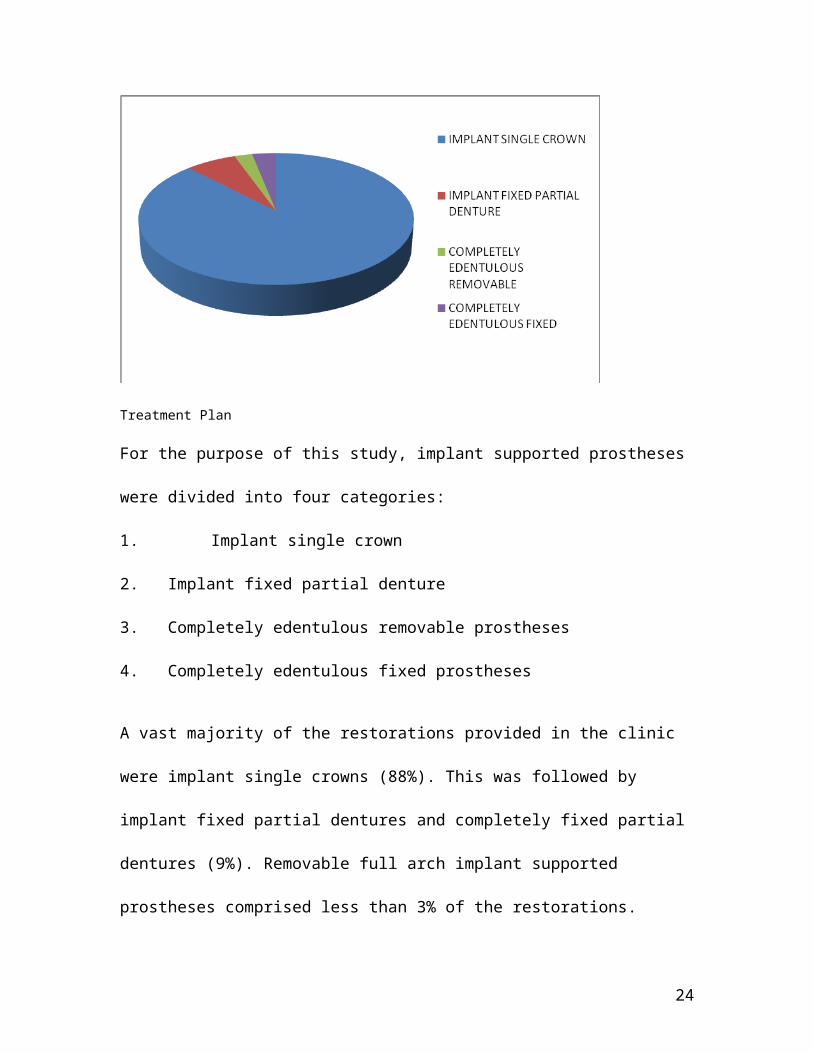
Treatment plan for implant supported prostheses:
Treatment Plan
For the purpose of this study, implant supported prostheses were divided into four
categories:
1. Implant single crown
2. Implant fixed partial denture
18
3. Completely edentulous removable prostheses
4. Completely edentulous fixed prostheses
A vast majority of the restorations provided in the clinic were implant single crowns
(88%). This was followed by implant fixed partial dentures and completely fixed
partial dentures (9%). Removable full arch implant supported prostheses
comprised less than 3% of the restorations.
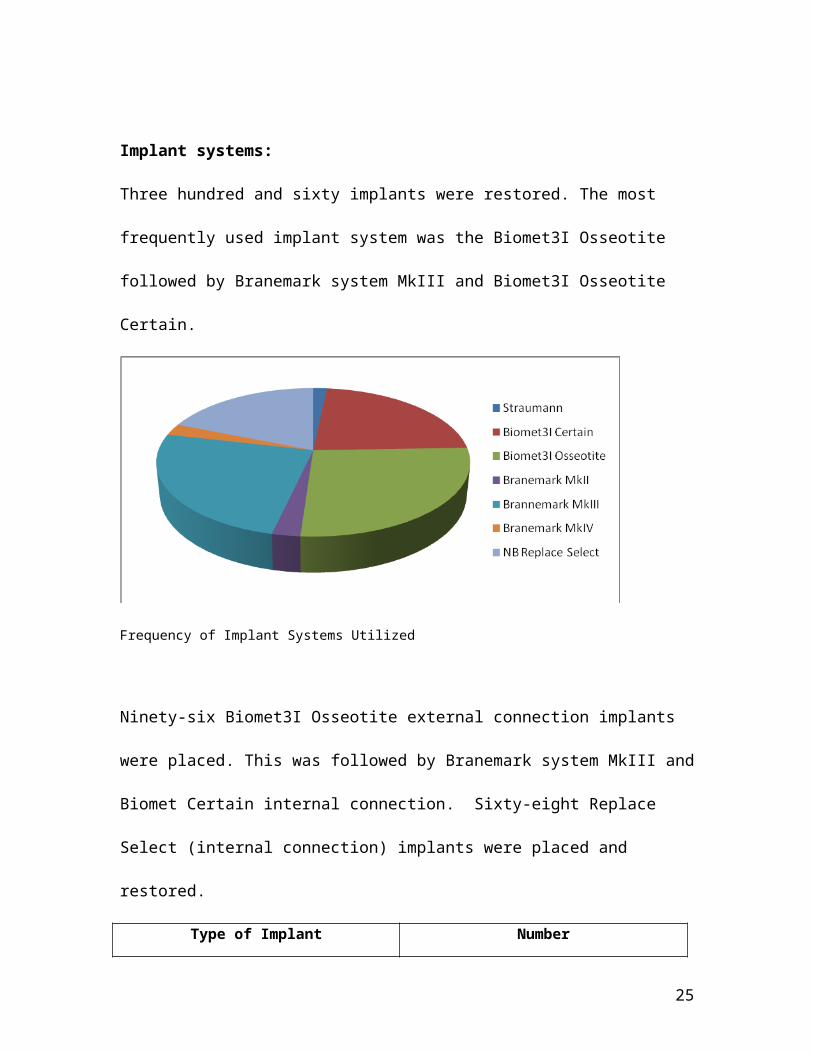
Implant systems:
Three hundred and sixty implants were restored. The most frequently used implant
system was the Biomet3I Osseotite followed by Branemark system MkIII and
Biomet3I Osseotite Certain.
Frequency of Implant Systems Utilized
Ninety-six Biomet3I Osseotite external connection implants were placed. This was
followed by Branemark system MkIII and Biomet Certain internal connection. Sixty-
eight Replace Select (internal connection) implants were placed and restored.
19
Type of Implant Number
Straumann6
Biomet3I Certain 82
Biomet3I Osseotite 96
Branemark MkII 9
Brannemark MkIII 90
Branemark MkIV9
Nobel Biocare Replace Select 68
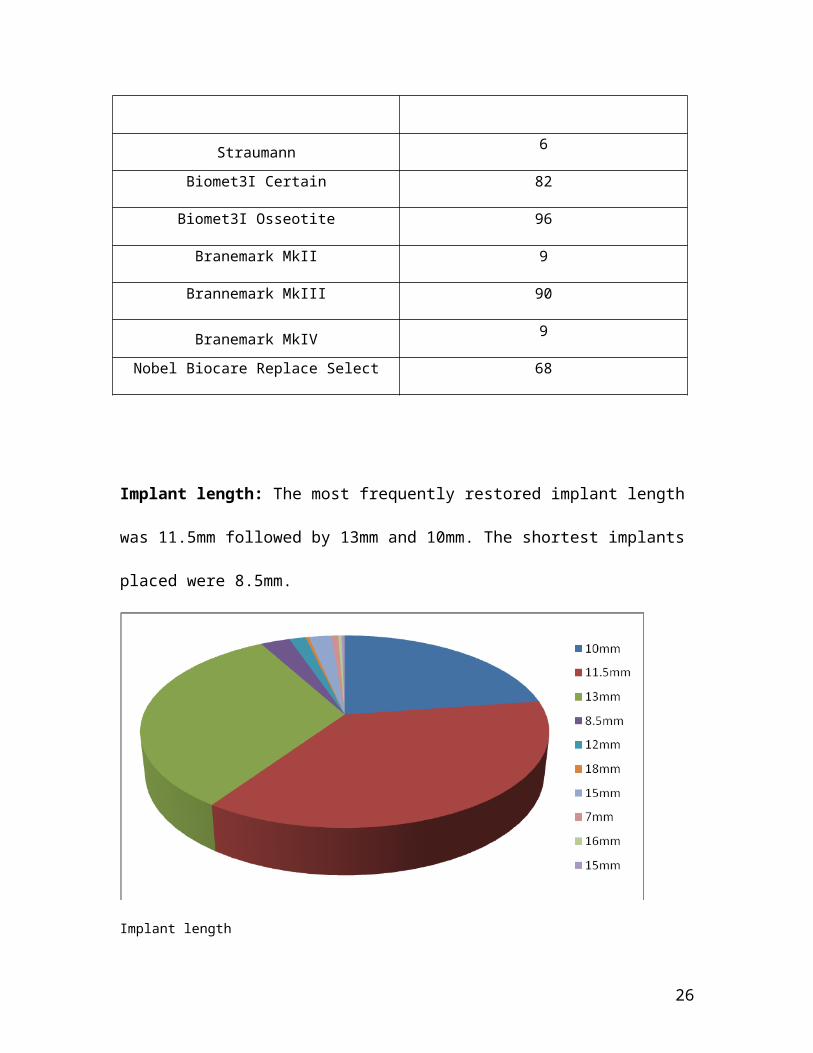
Implant length: The most frequently restored implant length was 11.5mm followed
by 13mm and 10mm. The shortest implants placed were 8.5mm.
Implant length
20
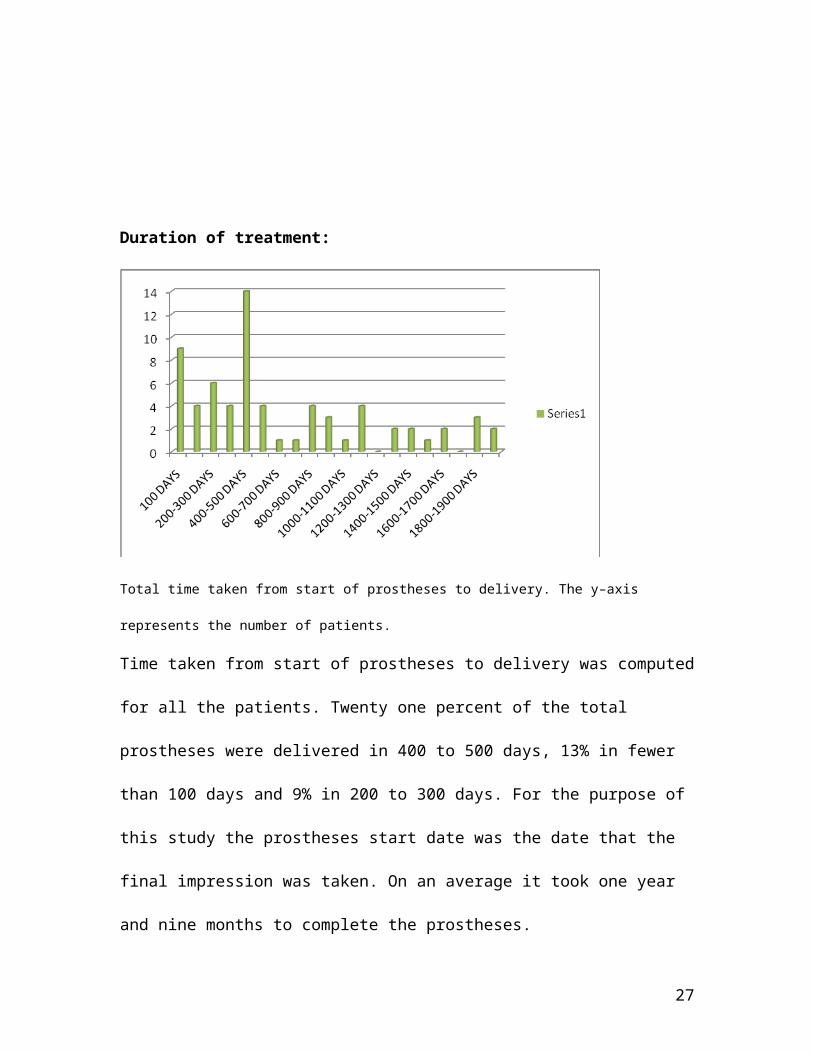
Duration of treatment:
Total time taken from start of prostheses to delivery. The y–axis represents the number of patients.
Time taken from start of prostheses to delivery was computed for all the patients.
Twenty one percent of the total prostheses were delivered in 400 to 500 days, 13%
in fewer than 100 days and 9% in 200 to 300 days. For the purpose of this study the
prostheses start date was the date that the final impression was taken. On an
average it took one year and nine months to complete the prostheses.
21
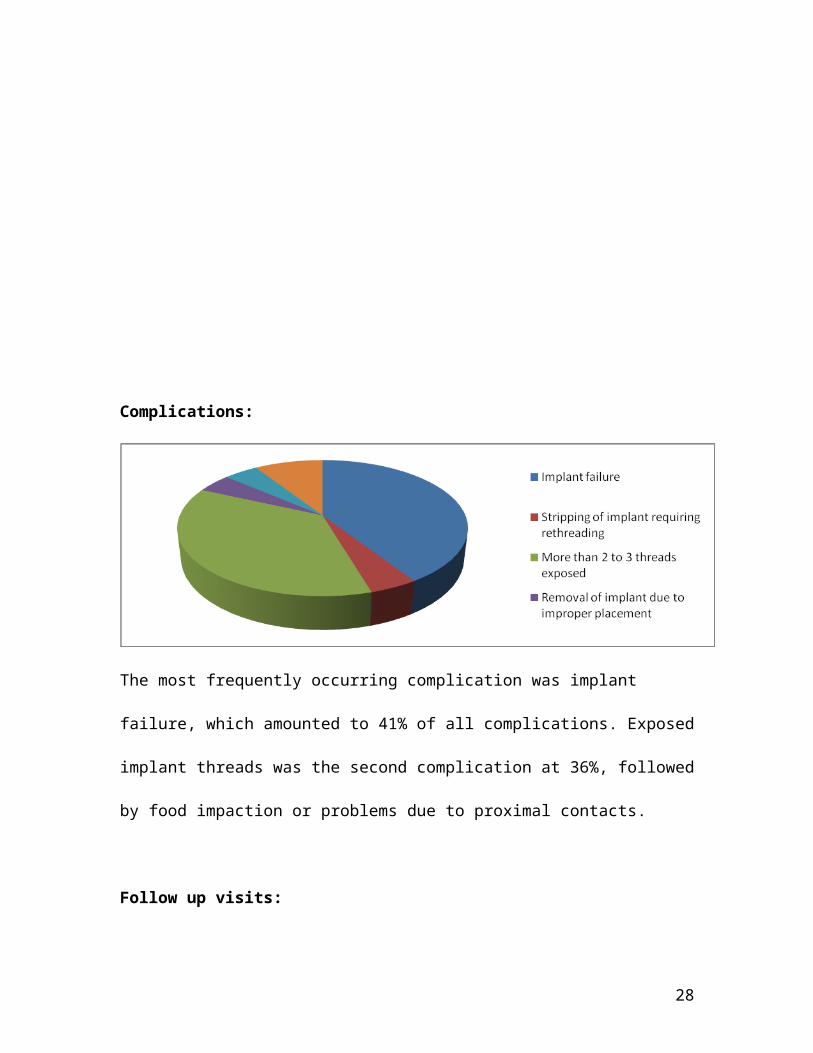
Complications:
The most frequently occurring complication was implant failure, which amounted to
41% of all complications. Exposed implant threads was the second complication at
36%, followed by food impaction or problems due to proximal contacts.
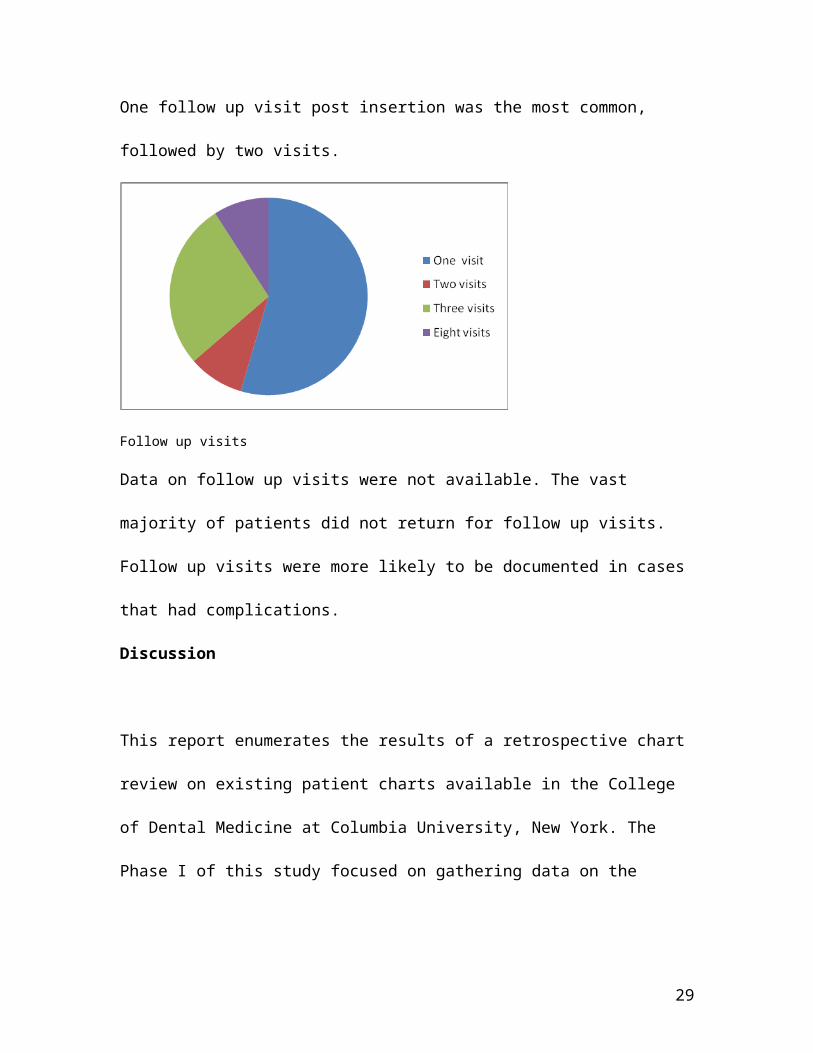
Follow up visits:
One follow up visit post insertion was the most common, followed by two visits.
Follow up visits
Data on follow up visits were not available. The vast majority of patients did not
return for follow up visits. Follow up visits were more likely to be documented in
cases that had complications.
22
Discussion
This report enumerates the results of a retrospective chart review on existing
patient charts available in the College of Dental Medicine at Columbia University,
New York. The Phase I of this study focused on gathering data on the patient’s
background, history, chief complaint, type of prostheses, implant type and duration
of treatment.
Awareness of dental implant treatment modalities has increased, and thus implant
treatments are more commonly accepted .For the majority of the population, the
clinical success of dental implant therapy has improved such that it has been
recognized as standard of care for certain prostheses types.13 Due to advancement
of technology and the current ease of accessibility to information, the general public
is able to research, visualize, and understand the advantages of dental implant
treatment. Improved chewing force and overall improved functionality of implant-
supported prostheses had been reported by Berg,14 Carlson et al15 and Lindquist.16
Ease of accessibility to information, more effective techniques and methodologies
that reflect a higher success rate is also the reason for increased acceptance of
dental implant supported prostheses. However, careful patient selection is needed
to ensure successful outcome. The patient needs to have an accurate assessment of
the procedures, the length of treatment time, risks and alternatives to implant
treatment. The trends in various new designs and methods are fast paced and
patients need to be informed of various options available to them.
23
Prostheses type: It must be noted that majority of the implants restored in the
Department of Prosthodontics were single crown implants. This chart review also
revealed that 88 porcelain fused to metal crowns were placed in the same
population. This is a lot less than the total number of implant supported single
crowns, which comprised 88% of all the implant, supported prostheses restored.
Lindh and Gunne, found in their meta analysis that implant survival was slightly
better for single crowns when compared with fixed implant supported prostheses.17
However, Weber and Sukotjo did not find higher success with implant single crowns
when compared to fixed splinted prostheses in a study published in 2007.18
Implant success: A total of three hundred and sixty implants were restored with an
implant success rate of 97.5%. According to Carl Misch, the term early implant
success is suggested for a span of 1 to 3 years, intermediate implant success for 3 to
7 years, and long-term success for more than 7 years. The implant success rate
should also include the associated prosthetic success or survival rate. Since this
study reviewed charts from 2001 to 2005, success can be categorized as
intermediate success of the implant.19 Information on the prostheses type will be
collected in the second phase of the study to determine the success and survival rate
of an implant supported prostheses. The type of abutment, the form of retention
(cement or screw retained) and the type of restorative material used will also be
evaluated for determining overall prosthetic success.
24
Implant type: The results on implant success rate obtained in this study are
comparable with data published on implant success in experienced clinicians and
residents in other surgical and general residency programs. In a retrospective study
published in 2004, on implant success in a general dentistry residency program,
authors Mohamed Maksoud and Clifford Starr state that the implant success rate
was 98.2% after a follow up of 6 months to 4 years.Error! Bookmark not defined. The study
population was 57% women and 43% men. The implant system evaluated in this
study were SteriOss (NobelBiocare, Branemark Novum ,Taperer-Lock (Zimmer
Dental), and ITI (Straumann). The success rate of implants placed in private practice
has been documented. In a study, which analyzed the success of 1003, implants
placed in 376 patients, the authors Lemmerman et al, state that the success rate was
approximately 95%. 20 Bahat demonstrated similar implant success rate in private
practice in another study where 660 Branemark implants were followed for 5 to 12
years.21 The success rate in the Bahat study was 93.4%. In the current retrospective
chart review, 62% were women and 38% were men. The implant systems restored
here were Straumann, Biomet 3I Certain, Biomet3I Osseotite, Branemark MkII,
Branemark MkIII and Branemark MkIV.
Implant length: The most frequently used length for dental implants restored in the
department were 11.5mm followed by 13mm and 10mm. This in accordance with
literature published by Jemt and Lekholm, 22 Naert et al; 23 Weng et al and
Herrmann et al, 24 which has favored the placement of longer implants to increase
25
implant survival rate. Babbush and Shimura study also demonstrated that longer
dental implants had a higher success rate.25 However, various authors have
reported good survival rates with shorter implants. Van Steenberghe et al, 26 Friberg
et al, 27 Jemt, 28 and Lekholm et al 29 have demonstrated that adequate survival of
implants can be obtained with the use of short implants. Some authors believe that
the use of implants over 12mm have higher chance of failure due to operator factors
such as longer drilling time, lesser ability of coolant to penetrate the osteotomy, or
inadvertent, increased drilling force to get a deeper osteotomy. xvii Buser et al, 30
Ellegaard et al, 31 Stellingsma et al 32 and Feldman et al, 33 reported that implant
length did not appear to significantly influence the implant survival rate . In this
retrospective chart review, 33% of the implants were 13mm long and 37% were
10mm long. The shortest implant restored in the Department of Prosthodontics was
8.5mm long. This accounted for 3% of all the implants restored. Seventy of the 360-
implant sites had bone augmentation.
Implant abutment interface: According to a literature review published in 2008,
author Theoharidou states that most invitro studies except one, have demonstrated
that internal connection implants are more mechanically stable than external
connection when restoring single implant crowns.34 Peirmatti et al, in their invitro
study have shown that external connection has better mechanical stability than
internal connection. Some authors prefer the use of internal connection implants for
sites where higher torque values are needed.35 However, research conducted in the
US market reveals that external connection implants are still more frequently used
26
than internal connection implants despite an increase in the sales of internal
connection implants in recent years. 35 Data collected from this retrospective study
shows that both internal and external connection implants were restored. Fifty
seven percent of the implants were external connection and 43% were internal
connection implants.
Radiographs: The most frequently requested radiographs were the panoramic
radiograph (32%) followed by full mouth series radiographs (31%) and periapical
radiographs (30%). Only 6 percent of the patients had CT scans requested. One
patient had a CT scan requested for Nobel guide surgery.
Complications: Implant failure requiring removal of the fixture was the most
frequently seen complication and amounted for 41% of all complication. Among the
failed implants, 33% of the failed implant sites had bone augmentation (Bioss).
Implant failure was seen more frequently in men (7) than in women (2). One
patient with implant failure was a pipe smoker. Thread exposure of more than two
to three threads due to bone resorption was the second most frequently seen
complication (36%). The other complications reported were stripping of the screw,
food impaction and incorrect placement of the implant.
Duration of treatment: For the purpose of this study the prostheses start date was
the date that the final impression was taken. On an average it took one year and 9
months to complete the prostheses. There is a paucity of literature available on the
27
average time taken to deliver prostheses in a Prosthodontic residency setting, so
comparison with another program is not possible. Factors that could account for
the length of procedure could be:
1) Treatment provided by residents in a residency program
2) Treatment is provided in a university setting requiring authorization of
procedures, and
3) Lack or delayed availability of prosthetic implant parts and materials
Health Insurance: The dental school at Columbia University accepts Medicaid and
self-payment for treatments rendered, which is reflected in the insurance plan
distribution among the patients. Forty four percent of the patients were self-pay
and Medicaid covered 31%. Despite the coverage extended for conversion of
complete dentures to implant supported removable prostheses, the percentage of
overdentures (2%) was lower than the percentage of fixed full arch prostheses
delivered (3%).
Age: It is estimated that New York City will see substantial increases in its elderly
population. The number of persons ages 65 and over is projected to rise 44.2
percent, from 938,000 in 2000 to 1.35 million in 2030. The average age of the
patient treated in the Prosthodontic department reflects this trend. The highest age
group treated in the department was between the ages of 60 to 70 years and the
third highest group was above the age of 80 years. To achieve predictable esthetic
and functional outcomes of implant treatment for geriatric patients, comprehensive
28
diagnosis and treatment planning is required. The patient’s medical and dental
history for bruxism, periodontal disease, tobacco use, uncontrolled diabetes mellitus
and metabolic diseases of bone need to be assessed and evaluated before implants
treatment.36
Medical History: In this study, the patient’s medical history listed hypertension,
arthritis and diabetes type 2 as some of the most common medical disorders.
Fiorellini et al and Klokkevold have stated that patients with Type 2 Diabetes are at
higher risk for failure of implants,37 particularly older patients.
Smoking history: This chart review also revealed that smoking habits of patients in
both adult and geriatric patient was not routinely documented. According to a
dental literature review conducted by Perry Klokkevold in 2007 using Medline,
Cochrane Collaboration and Embase databases, the author concluded that smoking
adversely affects the outcome of implant survival and success rate.38 Sanchez-Perz et
al and PK Moy et al, have reported elevated complications related to smoking after
controlling for age and other medical conditions;39,40 it is thus, important to assess
smoking history in the elderly.
The data from this study revealed no current cigarette smokers and one pipe
smoker.
Race: The breakdown of various groups according to race in the retrospective study
is in accordance with data on the race distribution in New York City. According to
29
projections from the U.S. Census Bureau, the New York City has the largest Asian
(Chinese) population of any city outside of Asia and the largest Puerto Rican
population anywhere in the world. The largest Dominican population outside of
Santo Domingo resides in New York City. 41 Forty three percent of the city’s
population is White. The largest groups of people treated in the department belong
to the Hispanic (31%), White (31%) or Asian (25%) background. African Americans
comprised 13% of this population. Although variations in implant success in
different ethnicities has not been observed, there are very few studies reporting on
race and implant success. One study, a retrospective multicenter cohort study on
two stage implants published in 2006, carried out in the South Korean population
states that there is no significant difference in implant success rate in the Korean
population and other published data on implant success.42
Utilization of health services: Utilization of health services varies by gender and age.
Some studies report that females are more likely to seek care than males.43, 44
However, other studies state that there is no variation in health seeking behavior in
males and females.45 Some published studies have stated that older men are more
likely to seek care. 46Mustard et al, state that expenditure for health is the same for
men and women. 47 The data gathered from this chart review shows that women are
more likely to seek dental treatment than men. The average age for women was 59
years and the average age for men was 65 years.
Missing data and lack of documentation: A large number of charts reviewed had
missing data or did not systematically document dental services rendered. Data on
30
socio economic variables, smoking behavior and race were not consistently
documented. However, data on implant type was included in all the 68 charts
reviewed. This could be due to the use of stickers provided by the manufacturer.
Using standardized forms to document prosthetic and surgical procedures might aid
the documentation process.
Conclusions
A hundred and one charts were reviewed and 68 charts were included in this study.
The following are the outcomes of the chart review:
1. The implant success rate is comparable to the general population and other
general and surgical residency programs.
2. Implant single crowns were the most frequently restored prostheses.
3. External connection implants with length 10mm and above were the most
frequently utilized implant.
4. Branemark implant system was the most frequently used implant.
5. The average time for completion of a prostheses was 1 year and nine months.
The results of this study will be strengthened by increasing the sample size and by
evaluating the implant-supported prostheses by clinical and radiographic
examinations.
31
Appendix 1CHART REVIEW SHEET
SES INFORMATIONSex DobRaceMedical historyMedicationsInsurance typeChief complaintDental historyRadiographsTreatment plan
IMPLANTS RELATED INFORMATIONDate implants placedType of implants placedBone augmentationOther relavent information wrt implantsComplications
PROSTHESESStart date of prosthetic treatmentDate deliveredNumber of post insertion visitsComplications associated with the prosthesesOther
32
Appendix 2Clinical Evaluation Questionnaire
Study number:
1) Is prosthesis mobility present? Yes No
2) Is there mobility of implants? Yes No
3) Is there any sign of localized infection around the implants or implant prosthesis?
a. Gingival irritation: Severe Moderate Minor
b. Suppuration present: Yes No
4) Is bone loss noted around the implants? Greater than 50% - Yes No
5) Oral hygiene status around implant prosthesis- Good Fair Poor
6) Is the patient satisfied with prosthesis mastication? Very satisfied Generally satisfied Dissatisfied
7) Is patient satisfied with esthetic outcome? Very satisfied Generally satisfied Dissatisfied
8) Is patient satisfied with phonetic outcome? Very satisfied Generally satisfied Dissatisfied
9) Were you satisfied with the time limit of treatment? Yes No
10)Are there any soft tissue complications around implants or prosthesis? Yes No
11)List prosthetic complications associated with the prostheses
33
Appendix 3Oral Health Impact Profile Questionnaire
Study number:Sex:Age:Occupation:Race:Insurance type:Education:Income:
Functional Limitations1. Have you had trouble pronouncing any words because of problems with your teeth, mouth, or dentures? (0.51)
2. Have you felt that your sense of taste has worsened because of problems with your teeth, mouth, or dentures? (0.49)
Physical Pain3. Have you had painful aching in your mouth? (0.34)
4. Have you found it uncomfortable to eat any foods because of problems with your teeth, mouth, or dentures? (0.66)
Psychological Discomfort5. Have you been self conscious because of your teeth, mouth, or dentures? (0.45)
6. Have you felt tense because of problems with your teeth, mouth, or dentures? (0.55)
Physical Disability7. Has your diet been unsatisfactory because of problems with your teeth, mouth, or dentures? (0.52)
34
8. Have you had to interrupt meals because of problems with your teeth, mouth, or dentures? (0.48)
Psychological Disability9. Have you found it difficult to relax because of problems with your teeth, mouth, or dentures? (0.60)
10. Have you been a bit embarrassed because of problems with your teeth, mouth, or dentures? (0.40)
Social Disability11. Have you been a bit irritable with other people because of problems with your teeth, mouth, or dentures? (0.62)
12. Have you had difficulty doing your usual jobs because of problems with your teeth, mouth, or dentures? (0.38)
Handicap13. Have you felt that life in general was less satisfying because of problems with your teeth, mouth, or dentures? (0.59)
14. Have you been totally unable to function because of problems with your teeth, mouth, or dentures? (0.41)
35
References
36
1 Millenium Research Group: US markets for dental implants 2001: Executive summary. Implant Dentistry 10:234, 2001
2 Stanford C, Rubenstein J. Dental endosseous implants—an update. ADA Council on Scientific Affairs. J Am Dent Assoc. 2004;135:92–95.
3 Carl Misch, Dental Implant prosthetics, 2005
4 Muller F, Wahl G, Fuhr K: Age-related satisfaction with complete dentures, desire for improvement and attitude to implant treatment. Gerodontology 11:7, 1994
5 Maico D. Melo, DMD, Grant McGann, DDS and George Obeid, DDS: Survey of Implant Training in Oral and Maxillofacial Surgery Residency Programs in the United States 2007 American Association of Oral and Maxillofacial Surgeons,J Oral Maxillofac Surg 65:2554-2558, 2007
6 Oosthuizen S J. Titanium: the innovators metal. Historical case studies tracing titanium process and product innovation. Advanced Metals Initiative Light Metals Conference 2010. http://researchspace.csir.co.za/dspace/bitstream/10204/4747/1/Oosthuizen3_2010.pdf 7 http://dentalimplants-usa.com/Treatment/implants/history.html
8 http://www.branemark.com/
9 http://www.nature.com/vital/journal/v6/n1/pdf/vital890.pdf
10Kohavi D, Azran G. Retrospective clinical review of dental implants placed in a university training program, Journal of Oral Implantology, vol xxx, no. 1, 2004
11 Lim MVC, Afsharzand Z, Rashedi B et al. Pre doctoral implant education in US dental schools. Journal of Prosthodontics 2005, Vol14, Issue 1, 46—56
12 Measuring oral health and quality of life: Published by: Department of Dental Ecology, School of Dentistry, University of North Carolina. September, 1997. Edited by Gary D. Slade
13 Fiene JS, Carlsson GE, Awad MA, et al. The McGill consensus statement on overdentures. Mandibular two – implant overdentures as the first choice standard of care for the edeuntulous mandible. Gerodontology. 2002 Jul;19(1):3-4.
14 Berg E. The influence of some anamnestic, demographic, and clinical variables on patient acceptance of new complete dentures. Acta Odontologica Scandinavica 1984; Vol 42, Issue 2,119–27.
15 Carlsson GE, Otterland A, Wennstrom A, Odont D. Patient factors in appreciation of complete dentures. The Journal of Prosthetic Dentistry 1967;17:322–8.
16 Lindquist LW, Carlsson GE, Hedegard B, Lundquist LW. Changes in bite force and chewing efficiency after denture treatment in edentulous patients with denture adaptationdifficulties. Journal of Oral Rehabilitation 1986;13:21–9.
17 Lindh T, Gunne J, Tillberg A, Molin MA. A meta analysis of implants in partial edentulism, Clinijcal Oral implant Res, 1998.9,80-90
18 Weber HP , Sukotjo C. Does the type of implant prosthesis affect the outcomes in a partially edentulous patient, International Journal of Oral and Maxillofacial Implants,2007, 22 (Suppl), 140 - 172
19 Misch CE, Perel ML, Wang HL, et al. Implant Success, Survival, and Failure: The International
Congress of Oral Implantologists (ICOI) Pisa Consensus Conference, The International Journal
of Oral Implantology, Volume 17(1), March 2008, pp 5-15
20Lemmerman KJ, Lemmerman NE. Osseointegrated Dental Implants in Private Practice: A Long-Term Case Series Study. J Periodontol 2005;76:310-319.
21 Bahat O. Branemark system implants in the posterior maxilla: Clinical study of 660 implants followed for 5 to 12 years. Int J Oral Maxillofac Implants. 2000;15:646-653.
22 Jemt T, Lekholm U. Implant treatment in edentulous maxillae: a 5-year follow-up report on patients with different degrees of jaw resorption. International Journal of Oral & Maxillofacial Implants, 1995, 10: 303–311
23 Naert I, Koutsikakis G, Quirynen M, et al. Biologic outcome of implant-supported restorations in the treatment of partial edentulism. Part I: a longitudinal clinical evaluation. Clinical Oral Implants Research, 2002, 13: 381–389
24 Herrmann I, Lekholm U, Holm S, et al. Evaluation of patient and implant characteristics as potential prognostic factors for oral implant failures. International Journal of Oral & Maxillofacial Implants, 2005, 20: 220–230
25 Babbush CA, Shimura M. Five-year statistical and clinical observations with the IMZ two-stage osteointegrated implant system. Int J Oral Maxillofac Implants 1993;8: 245-253
26 Van Steenberghe, D, Lekholm U, Bolender C, et al. The applicability of osseointegrated oral implants in the rehabilitation of partial edentulism: a prospective multicenter study on 558 fixtures. International Journal of Oral & Maxillofacial Implants, 1990; 5: 272–281.
27 Friberg B, Jemt T, Lekholm U. Early failure in 4641 consecutively placed Branemark dental implants: a study from stage 1 to the connection of completed prostheses. International Journal of Oral & Maxillofacial Implants, 1991; 6: 142–146.
28 Jemt, T. Failures and complications in 391 consecutively inserted fixed prostheses supported by Branemark implant in edentulous jaws: a study of treatment from the time of prosthesis placement to the first annual checkup. International Journal of Oral & Maxillofacial Implants 1991; 6: 270–276.
29 Lekholm U, Gunne J, Henry P. Survival of the Branemark implant in partially edentulous jaws: a 10-year prospective multicenter study. International Journal of Oral & Maxillofacial Implants, 1999; 14: 639–645.
30 Buser D, Mericske-Stern R, Bernard JP. Long-term evaluation of nonsubmerged ITI implants. Part 1: 8-year life table analysis of a prospective multicenter study with 2359 implants. Clinical Oral Implants Research; 1997; 8: 161–172.
31 Ellegaard B, Baelum V, Karring T. Implant therapy in periodontally compromised patients. Clinical Oral Implant Research, 1997; 8: 180– 188
32 Stellingsma K, Bouma J, Stegenga B. Satisfaction and psychosocial aspects of patients with an extremely resorbed mandible treated with implant-retained overdentures. Clinical Oral Implant Research, 2003; 14: 166–172
33 Feldman S, Boitel N, Weng D. Five-year survival distributions of short-length (10mm or less) machinedsurfaced and Osseotite implants. Clinical Implant Dentistry & Related Research, 2004; 6: 16–23.
34
Theoharidou A, Petridis HP, Tzannas K. Abutment Screw Loosening in Single-Implant Restorations: A Systematic Review. The International Journal of Oral & Maxillofacial Implants, July/August 2008; volume 23 , issue 4, 681 – 690.
35 Davi LR, Golin AL, Bernardes SR. In vitro integrity of implant external hexagon after application of surgical placement torque simulating implant locking. Oral Res. 2008 Apr-Jun;22(2):125-31
36 Beikler T, Flemmig TF. Implants in the medically compromised patient. Crit Rev Oral Biol Med 2003;14(4):305–16
37 Fiorellini JP, Nevins ML. Dental implant considerations in the diabetic patient. Periodontology 2000; 23:73–77
38 Klokkevold PK, Han TJ. How Do Smoking, Diabetes, and Periodontitis Affect Outcomes of Implant Treatment? The International Journal of Oral & Maxillofacial Implants, 2007; 22 (Suppl), 173- 202.
39 Sanchez-Perez A, Moya-Villaescusa MJ, Caffesse RG. Tobacco as a risk factor for survival of dental implants. J Periodontol 2007;78(2): 351–9
40 Moy PK, Medina D, Shetty V, Aghaloo TL. Dental implant failure rates and associated risk factors. Int J Oral Maxillofac Implants 2005;20(4):569–77
41http://www.nyc.gov/html/dcp/html/census/pop_facts.shtml
42 Ko SM , Lee JK, Eckert SE, Choi YG. Retrospective multicenter cohort study of the clinical performance of 2 Stage implants in South Korean population. International Journal of Oral and Maxillofacial Implants, 2006; 21; 785-788.
43 Husaini, B. A., Moore, S. T., & Cain, V. A. (1994). Psychiatric symptoms and help-seeing behavior among the elderly: An analysis of racial and gender differences. Journal of Gerontological Social Work, 21, 177–193
44 Neighbors HW, Howard CS. Sex differences in professional help seeking among adult black Americans. American Journal of Community Psychology, 1987;15, 403– 41
45 Ali F, Sami F, Rehman H, et al. Relation of gender education and health seeking behaviour of the general population regarding psychiatric illness. J Pak Med Assoc. 2006 Sep; 56(9): 421-2.
46 Ahmed SM, Adams AM, Chowdhury M, et al. Gender, socioeconomic development and health-seeking behaviour in Bangladesh. Social Science & Medicine, Volume 51, Issue 3, 1 August 2000, Pages 361-371
47 Mustard CA, Kaufert P, Kozyrskyj A, Mayer T. Sex Differences in the Use of Health Care Services, NEMJ, June 4, 1998; 338; 1678- 1683





























