Embed Size (px)
Citation preview
Seediscussions,stats,andauthorprofilesforthispublicationat:https://www.researchgate.net/publication/263207982
AReviewofLowerExtremityAssistiveRoboticExoskeletonsinRehabilitationTherapy
ArticleinCriticalReviewsinBiomedicalEngineering·January2013
DOI:10.1615/CritRevBiomedEng.2014010453·Source:PubMed
CITATIONS
34
READS
2,315
4authors:
Someoftheauthorsofthispublicationarealsoworkingontheserelatedprojects:
BionicDesignofSkeletalMuscle-likeVariableStiffnessActuatorViewproject
GongChen
NationalUniversityofSingapore
23PUBLICATIONS89CITATIONS
SEEPROFILE
ChowKhuenChan
NationalUniversityofSingapore
1PUBLICATION34CITATIONS
SEEPROFILE
ZhaoGuo
WuhanUniversity
25PUBLICATIONS109CITATIONS
SEEPROFILE
HaoyongYu
NationalUniversityofSingapore
137PUBLICATIONS888CITATIONS
SEEPROFILE
AllcontentfollowingthispagewasuploadedbyZhaoGuoon03October2014.
Theuserhasrequestedenhancementofthedownloadedfile.Allin-textreferencesunderlinedinblueareaddedtotheoriginaldocument
andarelinkedtopublicationsonResearchGate,lettingyouaccessandreadthemimmediately.
A Review on Lower Extremity Assistive Robotic
Exoskeleton in Rehabilitation Therapy
Gong Chen, Chow Khuen Chan, Zhao Guo, & Haoyong Yu*
Department of Biomedical Engineering, National University of Singapore, Singapore
*Address all correspondence to Haoyong Yu, Department of Biomedical Engineering, National
University of Singapore, 9 Engineering Drive 1, Singapore 117575 (Tel: +(65) 6601-1590; Fax: +(65)
6872-3069; E-mail: [email protected]).
ABSTRACT: The rapid advancement of robotics technology in recent years has pushed
the development of a distinctive field of robotic applications, namely robotic exoskeletons.
Due to the aging population, more people are suffering from neurological disorders such
as stroke, central nervous system disorder and spinal cord injury. As manual therapy
seems to be physically demanding for both treated patient and therapist, robotic
exoskeletons have been developed to increase the efficiency of the rehabilitation therapy.
Robotic exoskeletons are capable of providing more intensive patient training, better
quantitative feedback and improved functional outcomes for patients compared to manual
therapy. In this review, emphasize is placed on treadmill-based and over ground
exoskeletons for rehabilitation. Analyses of their mechanical designs, actuation systems
and the integrated control strategies are given priority as the interactions between these
components are crucial for the optimal performance of the rehabilitation robot. The review
also discusses the limitations of current exoskeletons and technical challenges faced in
exoskeleton development. A general perspective of the future development of more
effective robot exoskeletons, specifically real-time biological synergy-based exoskeletons,
could help promote brain plasticity among neurologically impaired patients, and allow
them to regain normal walking ability.
Keywords: Neuro-rehabilitation, robotics, exoskeleton, control strategies, rehabilitation
therapy, robotic rehabilitation, mechanical design, actuation system
ABBREVIATIONS: BWS, body weight support; CoP, center of pressure; DOF,
degree of freedom; EEG, electro-encephalograph; EMG, electromyography; FES,
functional electrical simulation; IMU, inertia measurement unit; PAM, pelvic assist
manipulator; POGO, pneumatically operated gait orthosis; SCI, spinal cord injuries; SEA,
series elastic actuator
1. Introduction
Computer technology has led to advancements in the development of lower extremities
robotic exoskeletons for rehabilitation therapy. There have also been an increasing number of new
exoskeletons which are designed to perform rehabilitation dedicated to certain patients. Hence, there
is no question that in future there will be an improvement in the medical rehabilitation therapy as it
seems no exact or proper medical cure for physiologically challenged subjects especially the paralytic,
neurologically damage [1] and spinal cord injured patients.
The designation of the lower limb robotic exoskeleton has been a complicated task as the
human walking is relatively complex, and rhythmic or likewise. The human walking involves the
coordination of brain, nerves and muscles whereby the lower and upper limb are systematically
controlled to generate the necessary force for locomotion. It is common knowledge that no two
individuals have identical walking styles. Diseases such as altered walking posture of the elderly,
reduction in walking ability caused by orthopedic disease (e.g. fracture or amputated limb), central
nervous system (CNS), and spinal cord disease or injury [1] make the rehabilitation process more
complicated and difficult to be treated either manually or with the assistance of devices. Therefore,
considerable number of factors needs to be taken care of in order to obtain a desirable design that
covers a wide range of DOFs in improving the mobility besides improving the neuroplasticity of the
patients [2-4]: severity of the impaired lower limb, mechanical design, actuation system, and control
strategy of the robotic exoskeleton.
One of the drawbacks of manual rehabilitation training, especially for the treadmill training, is
that it is not a very intensive training as the training time is limited to the personal trainer. With this
limitation of time, the gait pattern of the patient is not reproducible and thus the entire therapy is not
optimum. As for some severe SCI patients, the patient’s leg movements need to be assisted by at least
two therapists and in certain cases, a third therapist might even be needed to assist with the
stabilization of the pelvis movement. Moreover, the therapists will experience physical constraint and
ergonomically bad positions, in some circumstances [5]. With these physically demanding conditions,
the therapist will be exhausted and this further explains that manual rehabilitation training requires
great physical efforts [6-11].
Due to the difficulties in the manual rehabilitation therapy in correcting the ambulation of the
patients, robotic exoskeletons are suitable in taking over strenuous and repetitive task. The therapists
are then able to focus on more meaningful task such as interacting with patients, assessing the
outcome of the therapy, and intervene the training session if necessary. Optimal robotic training
programs can be designed according to the patient’s condition as this will improve the training quality
and motor recovery level [2-4]. Considerable studies have been reported to reveal the feasibility and
efficiency of the robotic exoskeletons [6-11], particularly on mechanical design point of view together
with its associated actuation system and control strategy.
The paper is organized as follows: Section 2 gives a description of the gait rehabilitation
devices that are currently available in the content of robotic rehabilitation exoskeleton. Section 3
presents the various types of gait rehabilitation exoskeletons including the treadmill-based gait
rehabilitation exoskeleton (Section 3.1) and exoskeleton for over ground gait training (Section 3.2). A
remarkable focus is given in the design consideration of the robotic exoskeleton in Section 4. Section
5 provides a description of the future challenge that can be a new paradigm shift in improving the
robotic exoskeleton technology.
2. Gait Rehabilitation Device
Robots can be designed to rehabilitate certain parts of the lower limb with different functions
and purposes. On the whole, the device can be classified into two groups: non-mobile robots and over
ground rehabilitation robots (Figure 1).
In the first group, immobile robots are devices that enable the users to receive gait training in
a fixed and confined area which include treadmill-based BWS system, treadmill-based exoskeleton,
BWS foot plate trainer and stationary device. Robotic gait rehabilitation trainer (RGR), an example of
treadmill-based based BWS system, offers the patient with the assistance of a BWS system but
unactuated joints [12]. Conversely, exoskeleton employs the treadmill-based mechanism with the
assistance of BWS system while the subject is walking on the treadmill. In this design, the BWS
system is required to maintain the balance while the exoskeleton is used to provide assistance to the
movements of the legs. The rehabilitation device, called as the treadmill-based exoskeleton, has been
widely used as this device has been implemented in Lokomat [13], ReoAmbulator [14], ALEX [15],
LOPES [16], University of Auckland system [17], POGO [18] and PAM [18]. The third gait
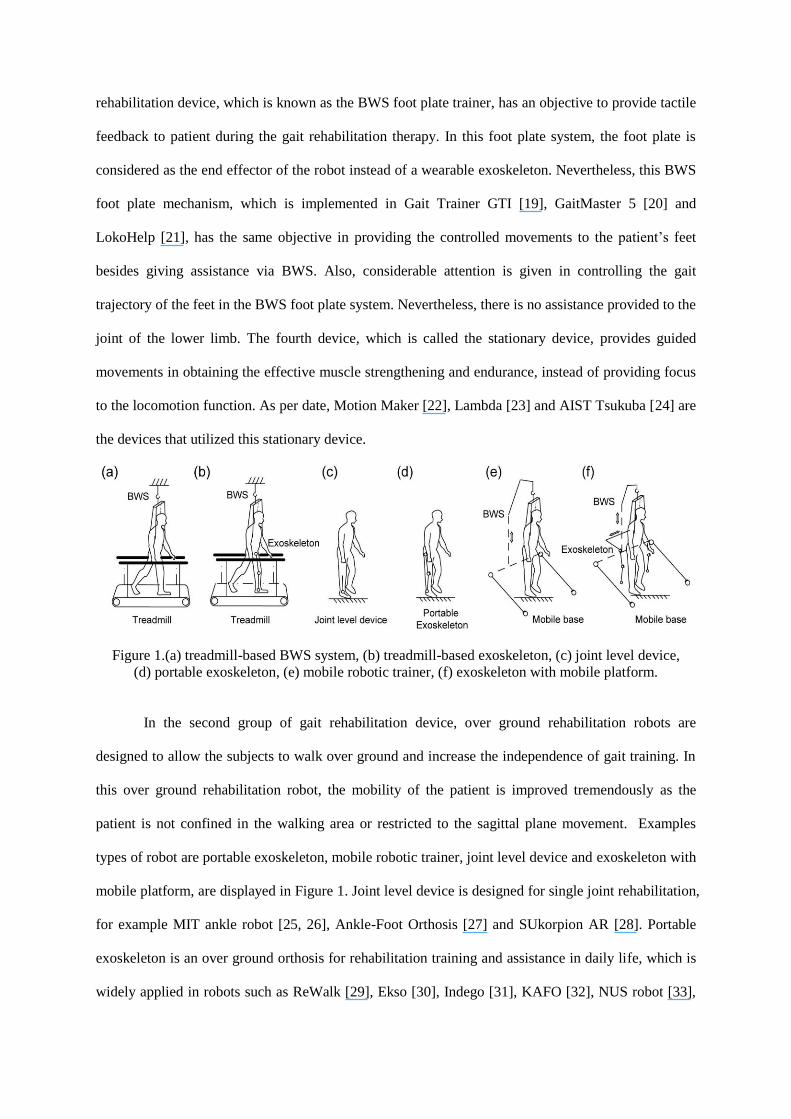
rehabilitation device, which is known as the BWS foot plate trainer, has an objective to provide tactile
feedback to patient during the gait rehabilitation therapy. In this foot plate system, the foot plate is
considered as the end effector of the robot instead of a wearable exoskeleton. Nevertheless, this BWS
foot plate mechanism, which is implemented in Gait Trainer GTI [19], GaitMaster 5 [20] and
LokoHelp [21], has the same objective in providing the controlled movements to the patient’s feet
besides giving assistance via BWS. Also, considerable attention is given in controlling the gait
trajectory of the feet in the BWS foot plate system. Nevertheless, there is no assistance provided to the
joint of the lower limb. The fourth device, which is called the stationary device, provides guided
movements in obtaining the effective muscle strengthening and endurance, instead of providing focus
to the locomotion function. As per date, Motion Maker [22], Lambda [23] and AIST Tsukuba [24] are
the devices that utilized this stationary device.
Figure 1.(a) treadmill-based BWS system, (b) treadmill-based exoskeleton, (c) joint level device,
(d) portable exoskeleton, (e) mobile robotic trainer, (f) exoskeleton with mobile platform.
In the second group of gait rehabilitation device, over ground rehabilitation robots are
designed to allow the subjects to walk over ground and increase the independence of gait training. In
this over ground rehabilitation robot, the mobility of the patient is improved tremendously as the
patient is not confined in the walking area or restricted to the sagittal plane movement. Examples
types of robot are portable exoskeleton, mobile robotic trainer, joint level device and exoskeleton with
mobile platform, are displayed in Figure 1. Joint level device is designed for single joint rehabilitation,
for example MIT ankle robot [25, 26], Ankle-Foot Orthosis [27] and SUkorpion AR [28]. Portable
exoskeleton is an over ground orthosis for rehabilitation training and assistance in daily life, which is
widely applied in robots such as ReWalk [29], Ekso [30], Indego [31], KAFO [32], NUS robot [33],
BLEEX [34-36], HAL[37-38] and PGO [39]. It provides assistive force to individual’s lower limb
joints or both legs and the user may require using crutches in maintaining the balance. Mobile robotic
trainer, on the other hand, provides both BWS and guidance in the patient’s motion especially on level
ground. The existing device that applies this concept is KineAssist [40]. Exoskeleton with mobile
platform is an exoskeleton system combining robotic mobile platform, a body weight support system
and a lower limb exoskeleton for over ground training. WalkTrainer [41], SUBAR [42], SJTU mobile
system [43] and NaTUre-gaits [44] are several examples of exoskeletons with such mechanisms.
3. Gait Rehabilitation Exoskeletons
Systems that are associated with the robotic gait rehabilitation exoskeleton are capable of
providing assistance and guidance to the joints of the human lower limbs. To ease the understanding
of the exoskeleton system, an in-depth explanation is provided for two types of gait rehabilitation
exoskeleton systems: treadmill-based exoskeleton and over ground exoskeleton. On the contrary,
exoskeletons which are designed for human performance augmentation or joint level robotic orthoses
are excluded.
3.1 Treadmill-based gait rehabilitation exoskeleton
Treadmill-based exoskeleton composed of a pair of powered leg orthoses, a BWS system and
a treadmill. This BWS treadmill training has proven to be effective for gait recovery by reducing the
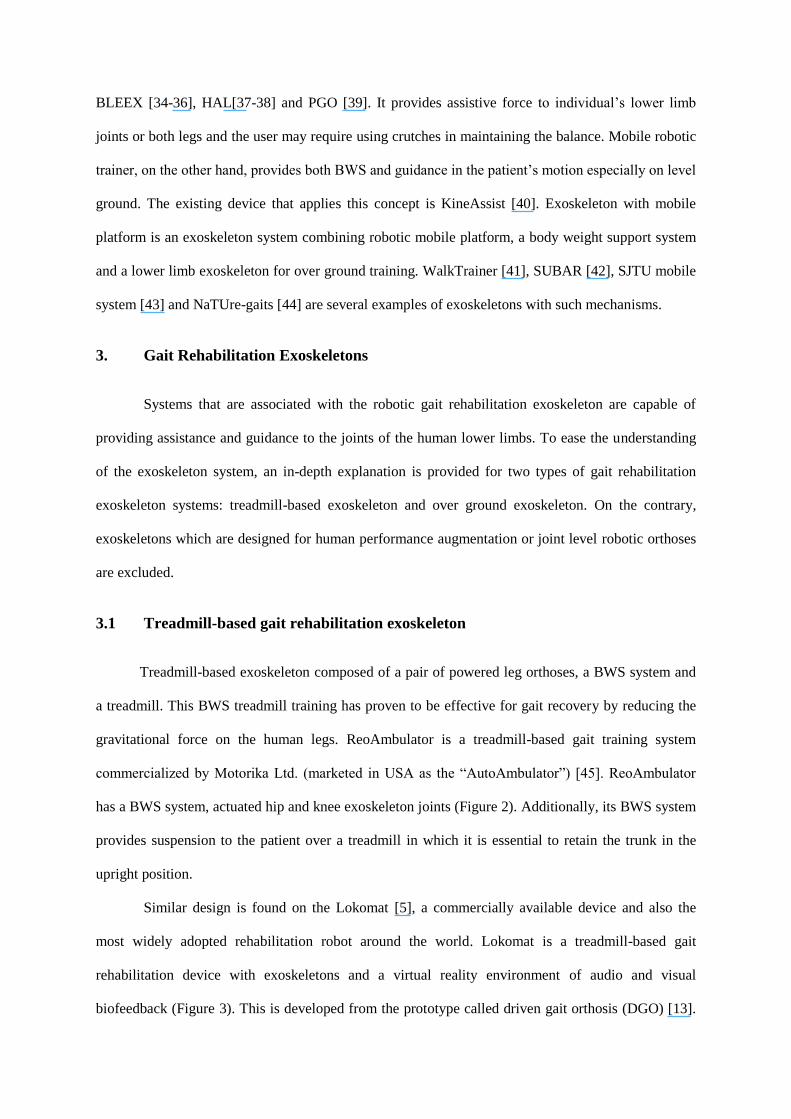
gravitational force on the human legs. ReoAmbulator is a treadmill-based gait training system
commercialized by Motorika Ltd. (marketed in USA as the “AutoAmbulator”) [45]. ReoAmbulator
has a BWS system, actuated hip and knee exoskeleton joints (Figure 2). Additionally, its BWS system
provides suspension to the patient over a treadmill in which it is essential to retain the trunk in the
upright position.
Similar design is found on the Lokomat [5], a commercially available device and also the
most widely adopted rehabilitation robot around the world. Lokomat is a treadmill-based gait
rehabilitation device with exoskeletons and a virtual reality environment of audio and visual
biofeedback (Figure 3). This is developed from the prototype called driven gait orthosis (DGO) [13].
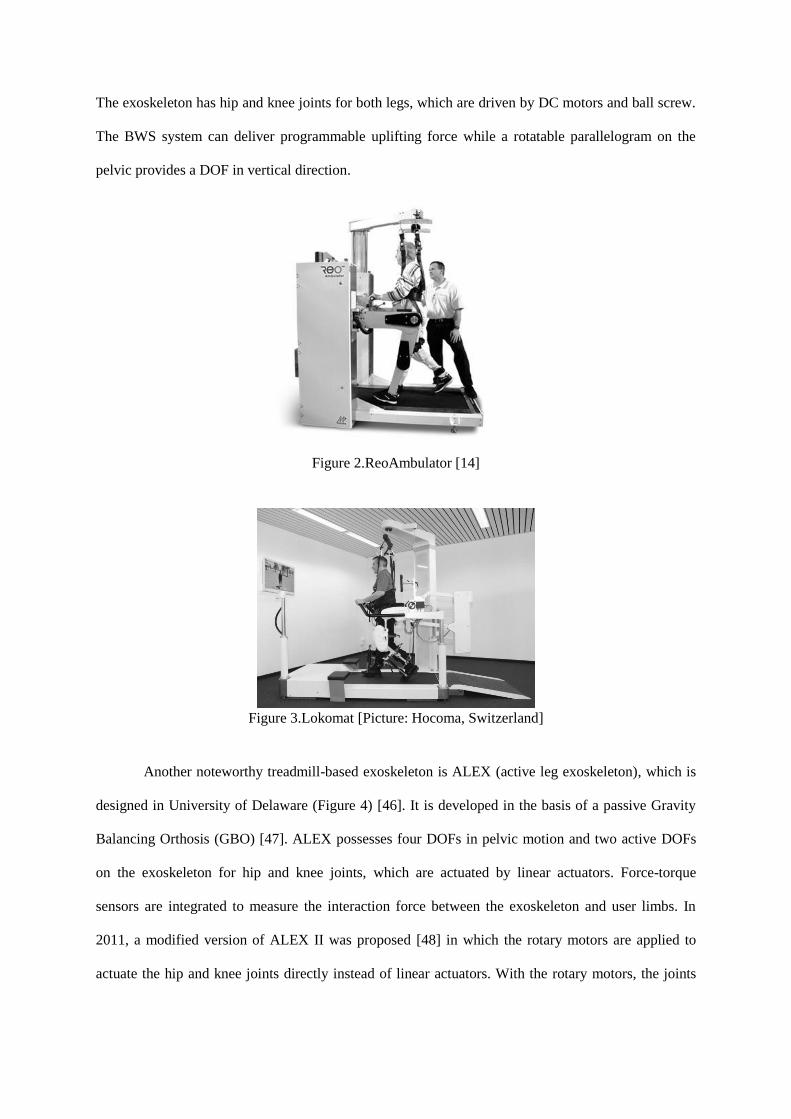
The exoskeleton has hip and knee joints for both legs, which are driven by DC motors and ball screw.
The BWS system can deliver programmable uplifting force while a rotatable parallelogram on the
pelvic provides a DOF in vertical direction.
Figure 2.ReoAmbulator [14]
Figure 3.Lokomat [Picture: Hocoma, Switzerland]
Another noteworthy treadmill-based exoskeleton is ALEX (active leg exoskeleton), which is
designed in University of Delaware (Figure 4) [46]. It is developed in the basis of a passive Gravity
Balancing Orthosis (GBO) [47]. ALEX possesses four DOFs in pelvic motion and two active DOFs
on the exoskeleton for hip and knee joints, which are actuated by linear actuators. Force-torque
sensors are integrated to measure the interaction force between the exoskeleton and user limbs. In
2011, a modified version of ALEX II was proposed [48] in which the rotary motors are applied to
actuate the hip and knee joints directly instead of linear actuators. With the rotary motors, the joints
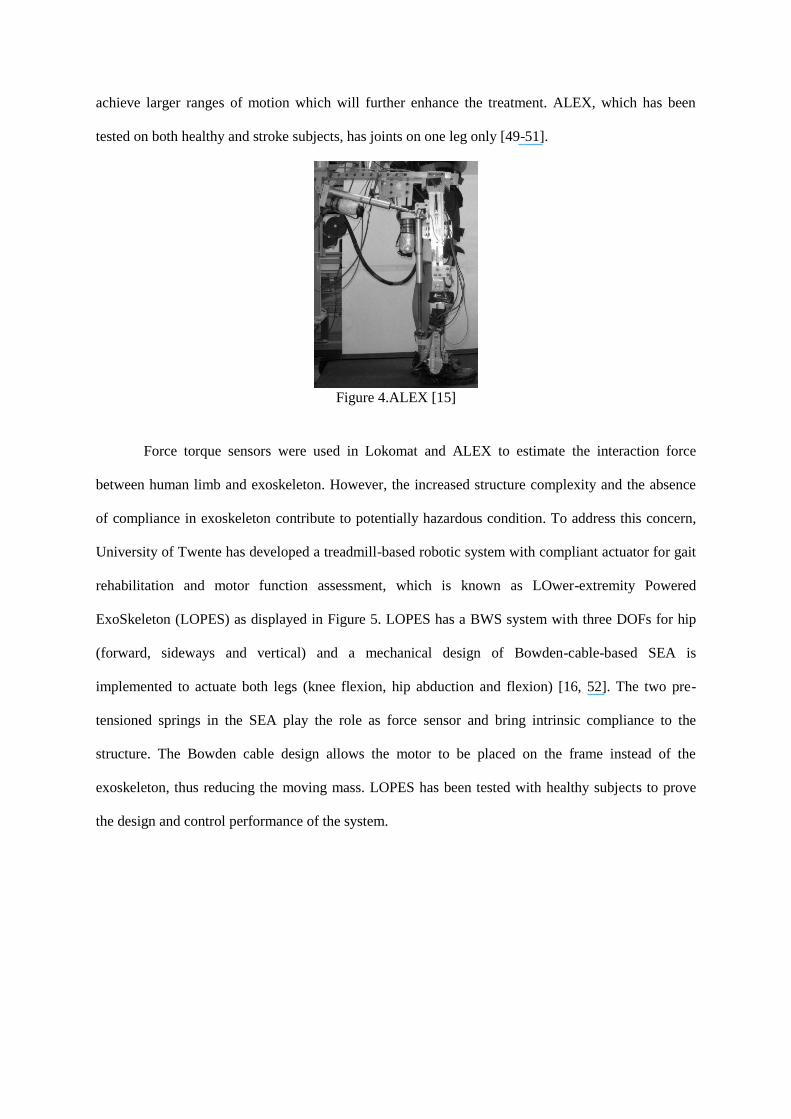
achieve larger ranges of motion which will further enhance the treatment. ALEX, which has been
tested on both healthy and stroke subjects, has joints on one leg only [49-51].
Figure 4.ALEX [15]
Force torque sensors were used in Lokomat and ALEX to estimate the interaction force
between human limb and exoskeleton. However, the increased structure complexity and the absence
of compliance in exoskeleton contribute to potentially hazardous condition. To address this concern,
University of Twente has developed a treadmill-based robotic system with compliant actuator for gait
rehabilitation and motor function assessment, which is known as LOwer-extremity Powered
ExoSkeleton (LOPES) as displayed in Figure 5. LOPES has a BWS system with three DOFs for hip
(forward, sideways and vertical) and a mechanical design of Bowden-cable-based SEA is
implemented to actuate both legs (knee flexion, hip abduction and flexion) [16, 52]. The two pre-
tensioned springs in the SEA play the role as force sensor and bring intrinsic compliance to the
structure. The Bowden cable design allows the motor to be placed on the frame instead of the
exoskeleton, thus reducing the moving mass. LOPES has been tested with healthy subjects to prove
the design and control performance of the system.

Figure 5.LOPES [16]
A research group from University of Auckland, New Zealand, proposed a robotic orthosis
powered by pneumatic artificial muscle actuators (Figure 6) [17]. This system is composed of an
exoskeleton for one leg only. PAM differs from SEA in working principles, but has the compliance
characteristics due to the fact that air is compressible. This orthosis has a BWS frame with two DOFs
on the waist namely lateral and vertical translations; while hip, knee rotations are actuated in the
sagittal plane. A single PAM can provide peak joint torque of 50Nm, which is sufficient for
rehabilitation. Impedance control was implemented with pneumatic muscle actuator. However, due to
the high nonlinearity effect of the pneumatic system, modeling and control become foremost concerns
in influencing the performance of the exoskeleton [53].
Figure 6.University of Auckland system [17]
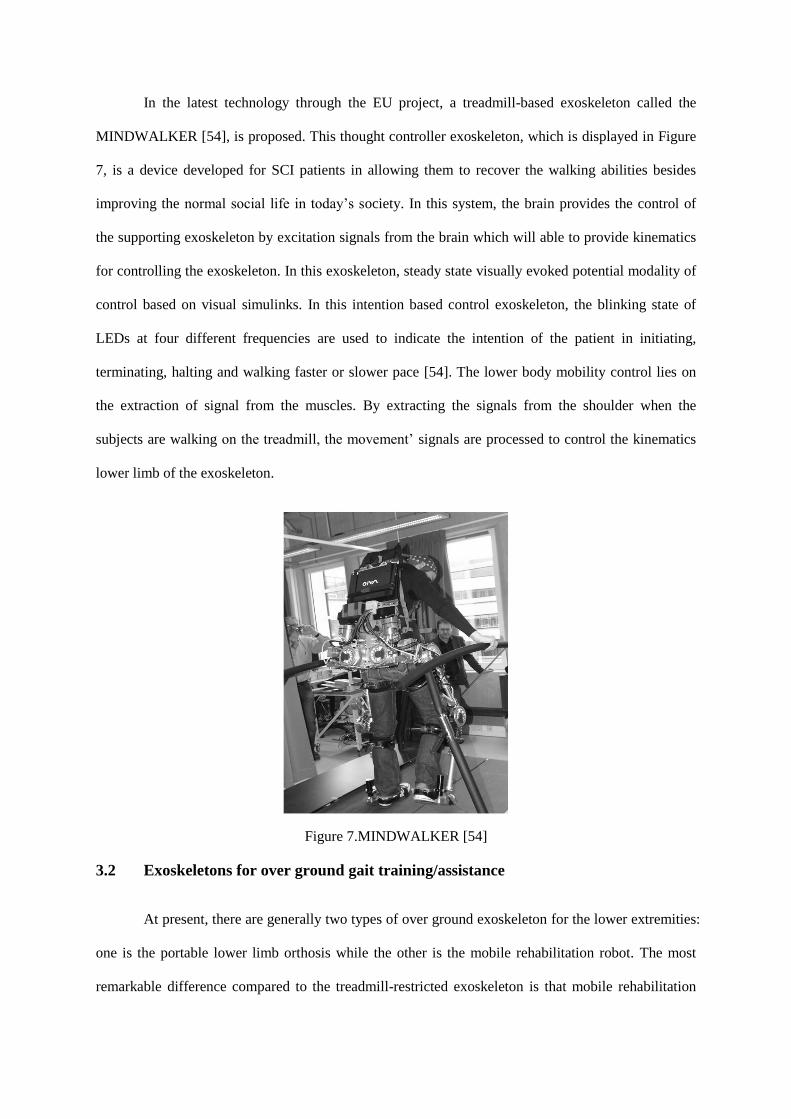
In the latest technology through the EU project, a treadmill-based exoskeleton called the
MINDWALKER [54], is proposed. This thought controller exoskeleton, which is displayed in Figure
7, is a device developed for SCI patients in allowing them to recover the walking abilities besides
improving the normal social life in today’s society. In this system, the brain provides the control of
the supporting exoskeleton by excitation signals from the brain which will able to provide kinematics
for controlling the exoskeleton. In this exoskeleton, steady state visually evoked potential modality of
control based on visual simulinks. In this intention based control exoskeleton, the blinking state of
LEDs at four different frequencies are used to indicate the intention of the patient in initiating,
terminating, halting and walking faster or slower pace [54]. The lower body mobility control lies on
the extraction of signal from the muscles. By extracting the signals from the shoulder when the
subjects are walking on the treadmill, the movement’ signals are processed to control the kinematics
lower limb of the exoskeleton.
Figure 7.MINDWALKER [54]
3.2 Exoskeletons for over ground gait training/assistance
At present, there are generally two types of over ground exoskeleton for the lower extremities:
one is the portable lower limb orthosis while the other is the mobile rehabilitation robot. The most
remarkable difference compared to the treadmill-restricted exoskeleton is that mobile rehabilitation
robot allows patients to regain natural gait training. With this relatively simple and small structure
exoskeleton, the patient will experience less visual impact. However, several important factors should
be taken into consideration during the designation of the exoskeletons. For instance, weight of the
device, balancing and power supply should be given priority so that the subject will not experience
additional burden and hazard during therapy.
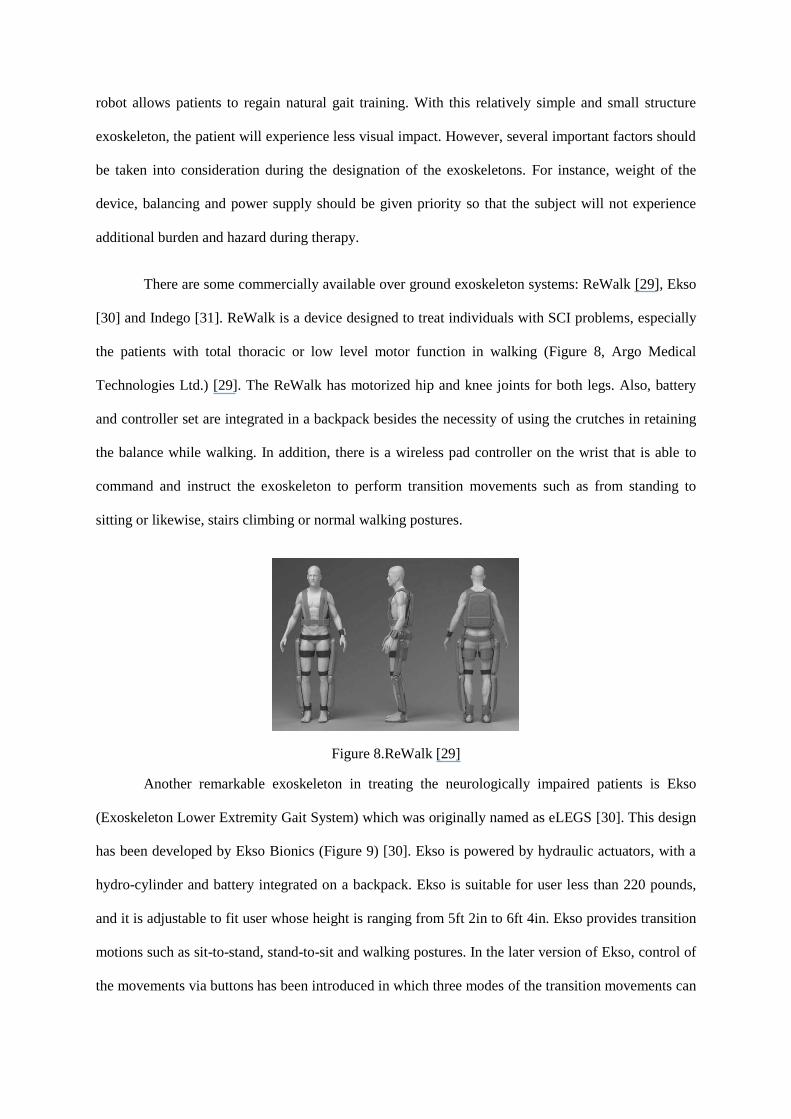
There are some commercially available over ground exoskeleton systems: ReWalk [29], Ekso
[30] and Indego [31]. ReWalk is a device designed to treat individuals with SCI problems, especially
the patients with total thoracic or low level motor function in walking (Figure 8, Argo Medical
Technologies Ltd.) [29]. The ReWalk has motorized hip and knee joints for both legs. Also, battery
and controller set are integrated in a backpack besides the necessity of using the crutches in retaining
the balance while walking. In addition, there is a wireless pad controller on the wrist that is able to
command and instruct the exoskeleton to perform transition movements such as from standing to
sitting or likewise, stairs climbing or normal walking postures.
Figure 8.ReWalk [29]
Another remarkable exoskeleton in treating the neurologically impaired patients is Ekso
(Exoskeleton Lower Extremity Gait System) which was originally named as eLEGS [30]. This design
has been developed by Ekso Bionics (Figure 9) [30]. Ekso is powered by hydraulic actuators, with a
hydro-cylinder and battery integrated on a backpack. Ekso is suitable for user less than 220 pounds,
and it is adjustable to fit user whose height is ranging from 5ft 2in to 6ft 4in. Ekso provides transition
motions such as sit-to-stand, stand-to-sit and walking postures. In the later version of Ekso, control of
the movements via buttons has been introduced in which three modes of the transition movements can
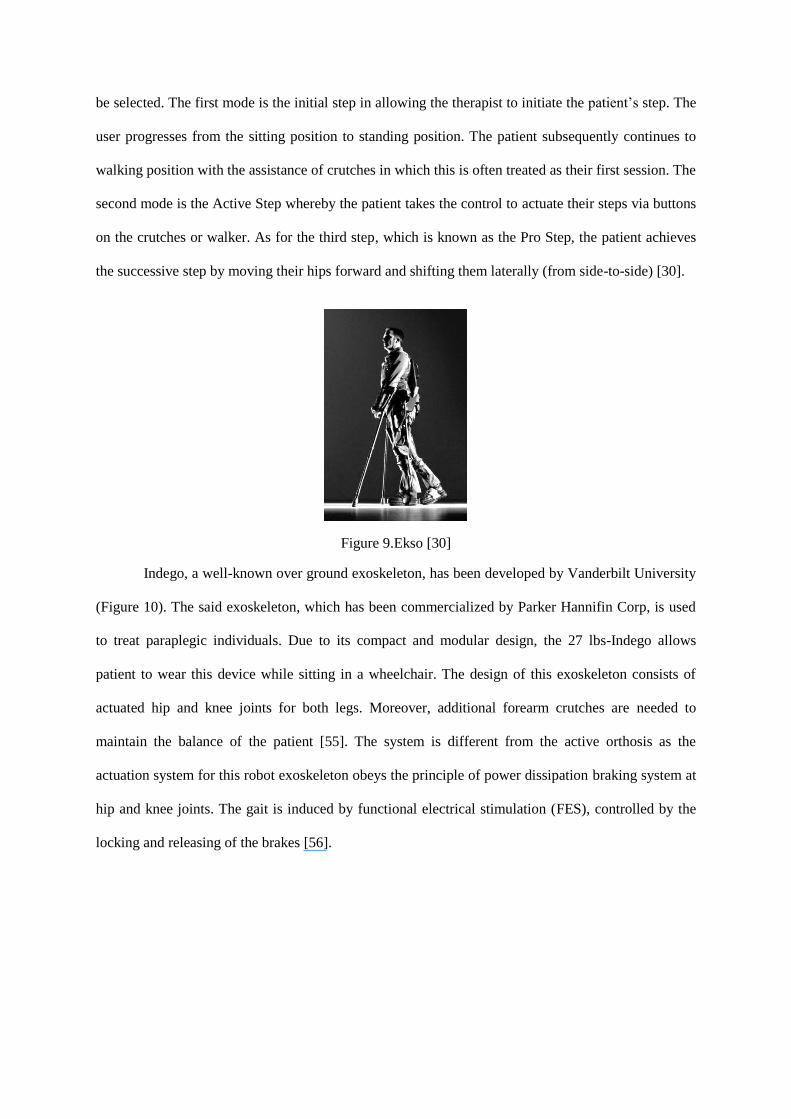
be selected. The first mode is the initial step in allowing the therapist to initiate the patient’s step. The
user progresses from the sitting position to standing position. The patient subsequently continues to
walking position with the assistance of crutches in which this is often treated as their first session. The
second mode is the Active Step whereby the patient takes the control to actuate their steps via buttons
on the crutches or walker. As for the third step, which is known as the Pro Step, the patient achieves
the successive step by moving their hips forward and shifting them laterally (from side-to-side) [30].
Figure 9.Ekso [30]
Indego, a well-known over ground exoskeleton, has been developed by Vanderbilt University
(Figure 10). The said exoskeleton, which has been commercialized by Parker Hannifin Corp, is used
to treat paraplegic individuals. Due to its compact and modular design, the 27 lbs-Indego allows
patient to wear this device while sitting in a wheelchair. The design of this exoskeleton consists of
actuated hip and knee joints for both legs. Moreover, additional forearm crutches are needed to
maintain the balance of the patient [55]. The system is different from the active orthosis as the
actuation system for this robot exoskeleton obeys the principle of power dissipation braking system at
hip and knee joints. The gait is induced by functional electrical stimulation (FES), controlled by the
locking and releasing of the brakes [56].
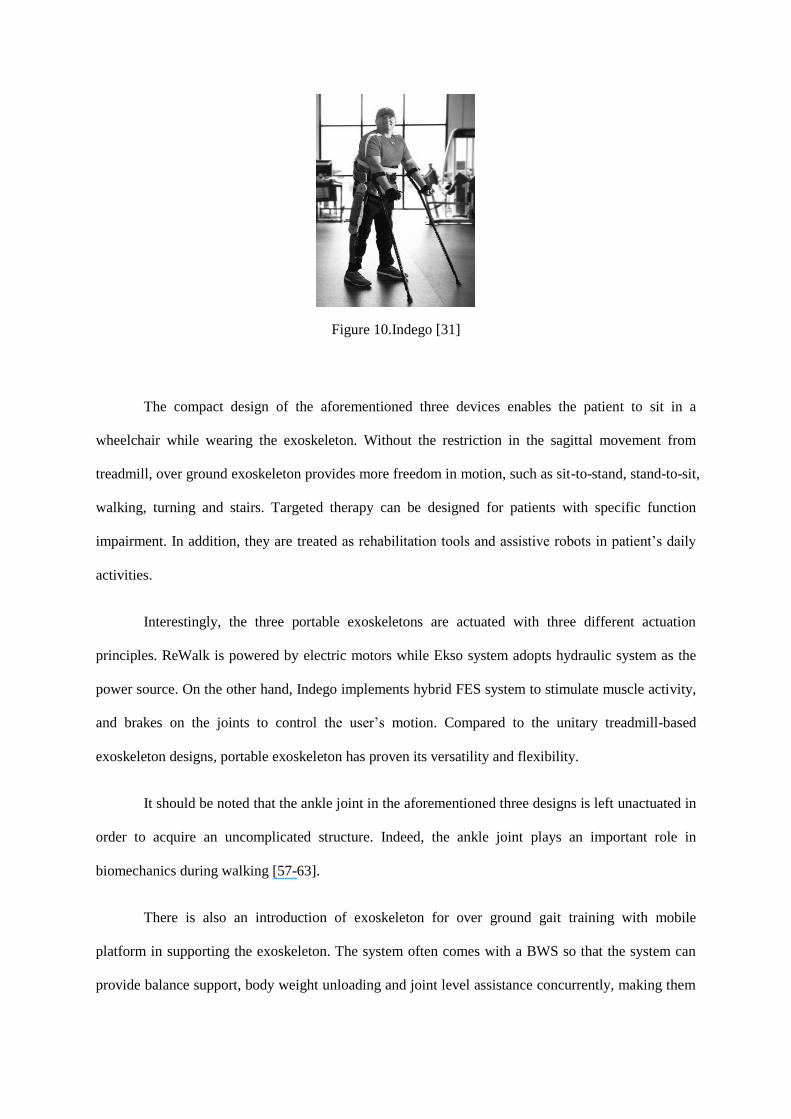
Figure 10.Indego [31]
The compact design of the aforementioned three devices enables the patient to sit in a
wheelchair while wearing the exoskeleton. Without the restriction in the sagittal movement from
treadmill, over ground exoskeleton provides more freedom in motion, such as sit-to-stand, stand-to-sit,
walking, turning and stairs. Targeted therapy can be designed for patients with specific function
impairment. In addition, they are treated as rehabilitation tools and assistive robots in patient’s daily
activities.
Interestingly, the three portable exoskeletons are actuated with three different actuation
principles. ReWalk is powered by electric motors while Ekso system adopts hydraulic system as the
power source. On the other hand, Indego implements hybrid FES system to stimulate muscle activity,
and brakes on the joints to control the user’s motion. Compared to the unitary treadmill-based
exoskeleton designs, portable exoskeleton has proven its versatility and flexibility.
It should be noted that the ankle joint in the aforementioned three designs is left unactuated in
order to acquire an uncomplicated structure. Indeed, the ankle joint plays an important role in
biomechanics during walking [57-63].
There is also an introduction of exoskeleton for over ground gait training with mobile
platform in supporting the exoskeleton. The system often comes with a BWS so that the system can
provide balance support, body weight unloading and joint level assistance concurrently, making them
suitable for rehabilitation for patients ranging from acute to chronic stages. Examples of robot
exoskeleton that utilize such systems are WalkTrainer [41], EXPOS, SJTU system [43] and NaTUre-
gaits.
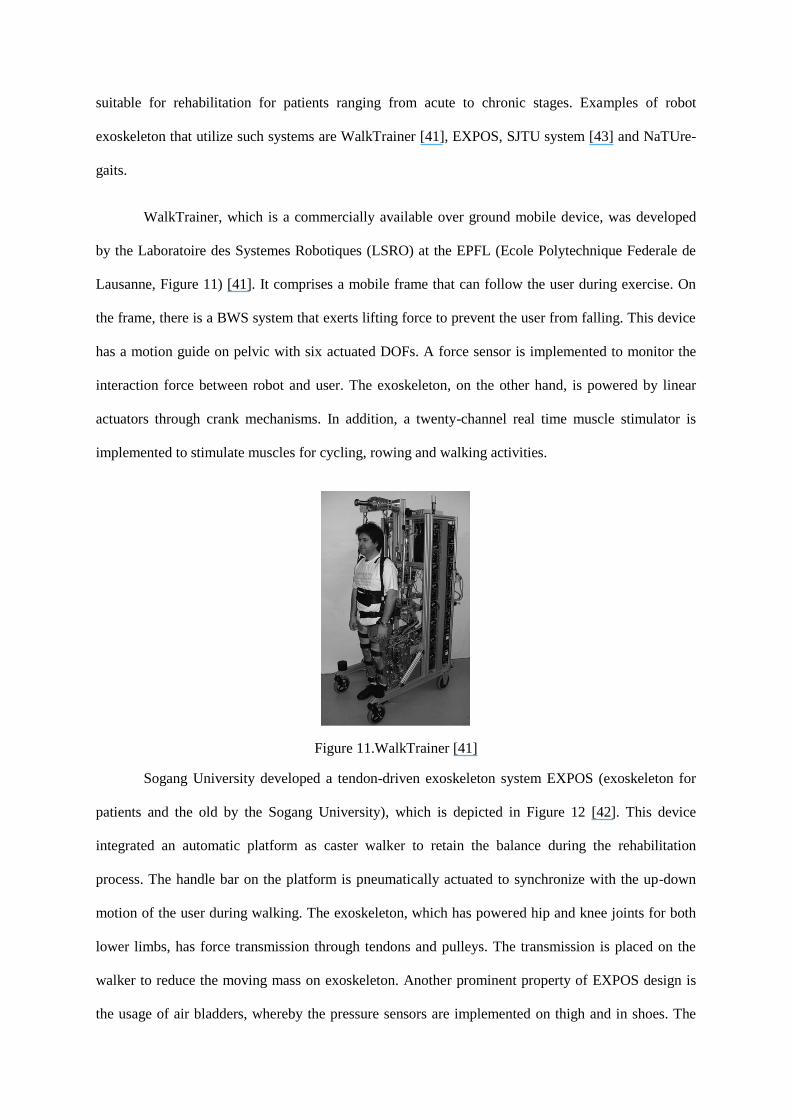
WalkTrainer, which is a commercially available over ground mobile device, was developed
by the Laboratoire des Systemes Robotiques (LSRO) at the EPFL (Ecole Polytechnique Federale de
Lausanne, Figure 11) [41]. It comprises a mobile frame that can follow the user during exercise. On
the frame, there is a BWS system that exerts lifting force to prevent the user from falling. This device
has a motion guide on pelvic with six actuated DOFs. A force sensor is implemented to monitor the
interaction force between robot and user. The exoskeleton, on the other hand, is powered by linear
actuators through crank mechanisms. In addition, a twenty-channel real time muscle stimulator is
implemented to stimulate muscles for cycling, rowing and walking activities.
Figure 11.WalkTrainer [41]
Sogang University developed a tendon-driven exoskeleton system EXPOS (exoskeleton for
patients and the old by the Sogang University), which is depicted in Figure 12 [42]. This device
integrated an automatic platform as caster walker to retain the balance during the rehabilitation
process. The handle bar on the platform is pneumatically actuated to synchronize with the up-down
motion of the user during walking. The exoskeleton, which has powered hip and knee joints for both
lower limbs, has force transmission through tendons and pulleys. The transmission is placed on the
walker to reduce the moving mass on exoskeleton. Another prominent property of EXPOS design is
the usage of air bladders, whereby the pressure sensors are implemented on thigh and in shoes. The
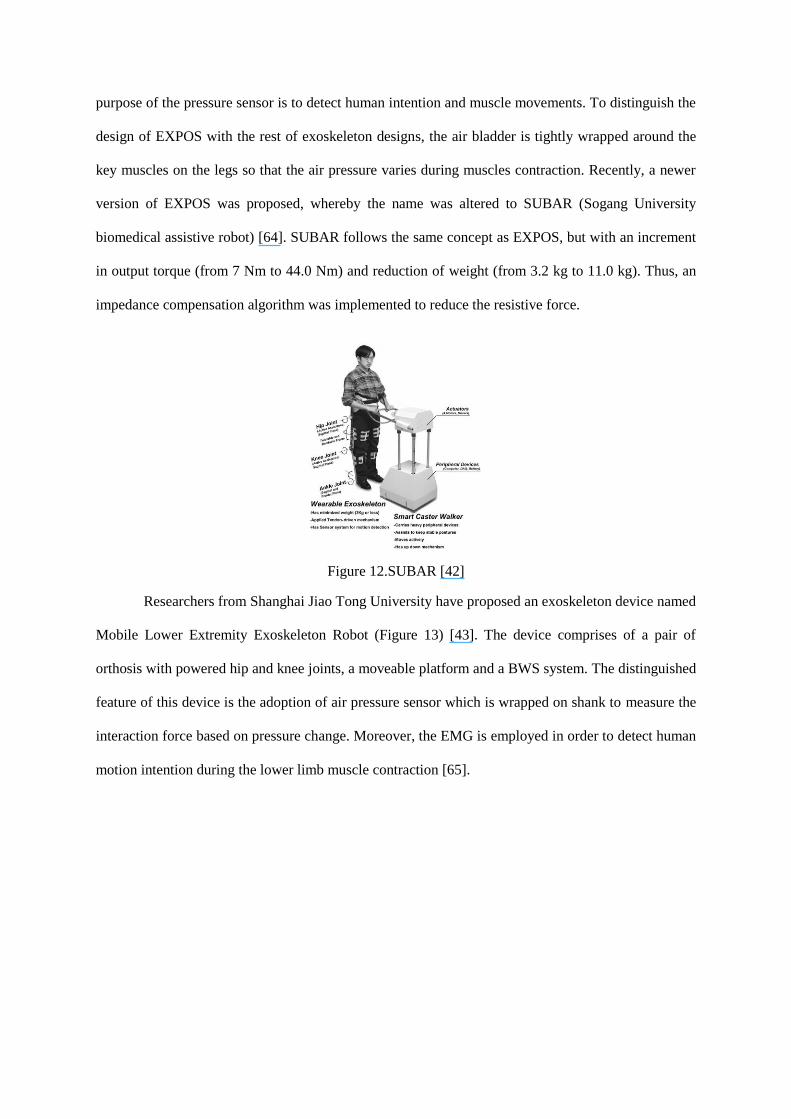
purpose of the pressure sensor is to detect human intention and muscle movements. To distinguish the
design of EXPOS with the rest of exoskeleton designs, the air bladder is tightly wrapped around the
key muscles on the legs so that the air pressure varies during muscles contraction. Recently, a newer
version of EXPOS was proposed, whereby the name was altered to SUBAR (Sogang University
biomedical assistive robot) [64]. SUBAR follows the same concept as EXPOS, but with an increment
in output torque (from 7 Nm to 44.0 Nm) and reduction of weight (from 3.2 kg to 11.0 kg). Thus, an
impedance compensation algorithm was implemented to reduce the resistive force.
Figure 12.SUBAR [42]
Researchers from Shanghai Jiao Tong University have proposed an exoskeleton device named
Mobile Lower Extremity Exoskeleton Robot (Figure 13) [43]. The device comprises of a pair of
orthosis with powered hip and knee joints, a moveable platform and a BWS system. The distinguished
feature of this device is the adoption of air pressure sensor which is wrapped on shank to measure the
interaction force based on pressure change. Moreover, the EMG is employed in order to detect human
motion intention during the lower limb muscle contraction [65].
Figure 13.SJTU mobile robot [43]
Nanyang Technological University (NTU) has introduced an over ground walking
rehabilitation device known as NaTUre-gaits (Natural and TUnable rehabilitation gait system). The
device consists of an exoskeleton with actuated hip-knee-ankle joints, BWS system and a mobile
platform [66]. One of the remarkable features of this device is that the system provides five actuated
DOFs on pelvic to assist in the pelvic movements. The advantage of this additional feature is to
promote motor recovery via repetition of therapy. In spite of the said features in which the mobility of
the patient is improved, these actuators however make the system relatively complicated and
cumbersome [67].
4. Discussion
The robotic exoskeletons can be viewed from three aspects: mechanical design, actuation
system and control strategy. Also, summary of the existing robotic rehabilitation exoskeletons and
the associated mechanical designs, actuation systems and control strategies are reviewed in the next
sections and tabulated in Table 1.
4.1 Mechanical design
Mechanical design plays an important role in determining the performance of gait
rehabilitation system as it affects the implementation of rehabilitation strategies. There are basically
two types of mechanical design which have been employed in many exoskeletons.
Exoskeleton of treadmill-based is considered as the conventional method of rehabilitation
exoskeleton mechanical design. By wearing the robotic exoskeleton, the patient is required to walk on
a treadmill during the rehabilitation treatment. In this design, the neurological impaired patient will be
able to perform a particular walking pattern without the direct assistance by the therapists. In another
words, there is no direct patient-therapist interaction compared to the physically demanding manual
therapy. The requirement of exorbitant force exerted on the patient will not be a major issue as the
robot arms are of lightweight and small. There is a claim that the treadmill bears the weight exerted by
the patient during the locomotion rehabilitation [68]. Notwithstanding the benefits mentioned, this
design is restricted to the flat plane ground walking. By employing this design, patients are only
allowed to move on the treadmill, in which the leg motion will be substantially limited to the sagittal
plane.
BWS system is widely adopted in treadmill-based exoskeletons, which provides uplifting
force to keep balance and provide suspension to the patient while walking on the treadmill. A
noteworthy exoskeleton that employs the aforementioned system is Lokomat. The suspension offers
an adjustable uplifting force to improve the gait pattern during training, and the support on pelvic
provides a freedom in vertical motion. Nonetheless, essential gait movements in pelvic, like rotating,
inclining and moving horizontally are inhibited [16]. In order to overcome the restrictions on pelvic,
LOPES group has enhanced its BWS system by providing three DOFs in pelvic motion: forward,
sideways and vertical. The vertical motion is unpowered but a spring mechanism is applied to
compensate gravity. The other DOFs are actuated by motors. The rotations, nevertheless, are still
constrained although the pelvic motion is improved with this configuration. The effort of reducing the
constraints tremendously seems to be not a perfect solution. To prevail over this problem, the
NaTUre-gaits device is invented whereby five powered assistance in pelvic movements are offered.
This device is superior in terms of comprising all significant during locomotion [69], but inferior in
terms of costing and conceptual design. It is discovered that the NaTU re-gaits device is a complex
and expensive; while its bulky design limits its optimal gait recovery. Thence, mobile walker seems to
be a solution to overcome this dilemma. The platform is used in providing some DOFs such as the
horizontal motion. The structure of BWS system is then simplified and adequate freedoms are
provided to promote natural gait motion.
In order to increase the mobility of the treated patients, the over ground exoskeleton design is
introduced. This portable exoskeleton provides more motion freedom compared to treadmill-based
exoskeleton in which patient can be treated and rehabilitated on stairs climbing and walking on flat
plane ground with different speeds and trajectory paths. This will be able to improve the brain
plasticity of the patient as the rehabilitation therapy for specific function is made possible. It is noted
that the over ground training is superior to the treadmill-based treatment [11, 68], and it is essential to
increase training independency among the patients.
In most of the exoskeletons designed till date, ankle joint is left unpowered. This is clearly
revealed in Lokomat, ReoAmbulator, LOPES, ALEX treadmill-based systems, ReWalk, Indego,
EXPOS over ground exoskeletons. The absence of actuated ankle joint brings the advantages of
simple structure and smaller moving mass on exoskeleton. In spite of that, ankle joint plays an
important role in biomechanics point of view [57-63]. The whole body weight is loaded on ankle joint
in a particular phase during walking and stairs. Absence of actuated ankle joint contributes to an
unnatural gait pattern. There are several exoskeletons with actuated ankle joint, such as WalkTrainer
and NaTUre-gaits that consist of complex mechanical structure with actuators attached to the mobile
platform. However, there seems to be a challenge in determining the method to achieve compactness
and effectiveness in ankle joint actuation. The key solution, however, lies in the actuator design of the
exoskeleton, which will be further explained in the next session.
4.2 Actuation system
The design of the actuation system is crucial for exoskeleton design as limitations in the
existing systems are due to the inefficient actuation system. Three types of actuators have been
utilized in exoskeleton systems: hydraulic, pneumatic actuator and electric motor. Hydraulic system,
which was adopted by Ekso, has the advantage of providing large output, but requires an additional
energy supply system. On the contrary, pneumatic artificial exoskeleton is known for its lightweight
and compliance. It appears that the nonlinear characteristic makes the pneumatically powered
exoskeleton difficult to be controlled. It is a fact that the hydraulic and pneumatic exoskeletons are not
portable as the actuators are usually bulky and difficult to be controlled. In order to overcome the
burdensome, electric motor is opted and used extensively in many existing designs. The usage of
electric motor produces the desired and controllable output with relatively fast and better response.
It must be borne in mind that the rehabilitation robots possess direct interaction with humans
physically. Thence, safety is a critical concern for human robot interaction. Conventional rigid
actuator is not inherently safe due to its high output impedance. Conversely, compliant actuator seems
to provide a better solution in which the famous ones are the pneumatic muscle actuator (PAM) and
series elastic actuator (SEA). PAM actuator, nonetheless, suffers a high nonlinearity effect which
leads to difficulty and inaccuracy in control system.
SEA actuator, on the other hand, places an elastic component between the power source and
output shaft. By measuring the deflection of the elastic component, the output force is then measured
based on Hooke’s law [70, 71]. LOPES uses a Bowden-cable-based SEA whereby two pre-tensioned
springs are adopted to drive the rotation of the joint. With this actuator, a desired torque is attained
besides the lightweight joint and incomplex structure. With the elastic component, SEA is back-driven
and intrinsically compliant. It works as a buffer between human limbs and exoskeleton which reduces
the impact of external shock to the subject. Furthermore, it is not necessary to apply force sensor and
this, of course, further simplifies the structure. However, SEA faces a dilemma of compliance and
force range, for which, a tradeoff has to be made. Softer component increases the force resolution but
reduces the compliance whereby the maximum output force is decreased. On the other hand, stiff
component yields larger range of output force, but extremely high stiffness will reduce the force
resolution. Recently, the NeuroRehabilitation Robotics research group from National University of
Singapore has recommended an approach by designing a novel linear SEA to overcome this limitation
[33, 72]. In this novel design, two springs with different stiffness ratio are placed in series; the softer
one enables the actuator to remain a low intrinsic compliance of the actuator, while the stiffer one
extends the range of output force. Experimental results have proven its excellent performance and
credibility in force tracking.
4.3 Control strategy
The main purpose of control strategy in the rehabilitation therapy is to engage the movement
sequences to assist in patient’s gait recovery. Different control strategies have been widely used in
the exoskeletons. Nonetheless, the discussion on control strategies in this paper is limited to pre-
defined trajectory based and intention based control strategies. The details of the mentioned control
strategies are presented in the following sections.
4.3.1 Trajectory based control strategy
In the early stage, exoskeletons move the patient’s limbs passively to follow a predefined gait
trajectory in rehabilitation therapies. However, the efficacy of this rehabilitation training is still
unknown due to the lack of human initiative [73]. Impedance control is then implemented in order to
engage human voluntary work in the rehabilitation treatment. This control provides assistive force
when human limb deviates from gait trajectory, in which restoring force that is proportional to the
deviation is provided [5, 16]. Clinical trials also affirmed that robot-applied resistance can improve
the performance of body-weight-supported treadmill training [74]. A number of control strategies
have been developed based on impedance control. This is clearly shown in LOPES exoskeleton as the
group proposed Virtual Mode Control whereby the selection of different gait functions is allowed [75].
On the other hand, ALEX used a force-field controller with visual guidance for gait rehabilitation [76].
The exoskeleton exerts both tangential and normal forces at the ankle joint with respect to the speed
of the reference trajectories. It should be borne in mind that assistive force varies with different
patients whereby this encourages them to have more engagement in the training process. Alexander et
al. developed a gait rehabilitation device, Lokomat, by constructing a path in space instead of gait
trajectory [77]. In this control strategy, the motion of the patient’s leg is constrained in both compliant
virtual tunnel and specific joint space. Thus, the guidance and assistance from the exoskeleton is
diminished besides interleaving effort and initiative from the patient.
Defining the gait trajectory reference for both passive and impedance control is a significant
issue to be taken into consideration. It is inaccurate to rely on a predefined gait pattern as reference
because every human has a unique gait pattern. Moreover, using fixed gait trajectories will prone to
the challenge in synchronization of desired gait cycle and subject’s gait phase. To prevail over this
problem, several approaches have been suggested: LOPES group proposed a method called CLME to
generate trajectories for the impaired leg with the motion of the healthy leg as reference [78]. ALEX
group also prepared a series of templates which are sorted according to the deviation from the
subject’s gait pattern to desired one [76]. By shifting the templates, the patient’s gait pattern is
improved when certain criterion is satisfied. To synchronize the reference and subject’s gait, Evryon
group has proposed an oscillator-based strategy [79]. Riener’s group has provided another approach in
allowing the subjects to adjust their pace initiatively by providing visual guide [77]. Adaptive
technique can also be applied to tune the trajectories in reducing or regulating the coordination
between human motion and exoskeleton assistance [80].
4.3.2 Intention based control strategy
A number of research groups have developed the control strategies of integrating the motion
intention of the subject (i.e. sit-to-stand, stand-to-sit, stairs climbing, walking in varying paces) in the
rehabilitation therapy.
Firstly, the physiological EMG and EEG signals are required to detect the intention of the
subjects. EMG is the mostly used technique in measuring muscle activity. Currently, there are several
exoskeletons that employ the EMG signal based assistance: HAL [37], KAFO [32] and NEUROExos
[81, 82]. However, it is plausible that noises in EMG signals increase the intricacy of muscle activity
evaluation [83-85]. Furthermore, EMG signals are very sensitive to the electrode placement,
disturbance from the neighboring muscles and skin properties (e.g. sweat on the skin) will further
make the detection unstable. Therefore, it is suggested that the EMG-based assistance should be tested
and calibrated for different patient in order to determine a better assistance.
In recent years, there has been much interest in introducing the EEG-based intention control
in treating the impaired lower limb [83]. The researchers of KAFO have revealed the potential of
high-density EEG to be implemented into the locomotors control [84]. The usage of EEG in providing
intention will be a challenge as the algorithm of the controller and the mapping limitation during
locomotion sources are no located in the brain cortex [86] and the relatively slow speed for real time
application [87]. Hence, the robustness and accuracy can be improved by fusing both the EEG and
EMG signals in providing assistance to the patient. With this combination technique, the EEG and
EMG signals are suitable in increasing the accuracy of features extraction [88, 89] and classification
which will improve the efficiency of the robot exoskeleton [90]. The mentioned fusion technique has
been employed by the MINDWALKER [54] in which further improvement can be suggested by
excluding the utilization of Brain Neural Computer Interface (BNCI). Hence, fusion of both EEG and
EMG is belief to be a new challenge in implementing human intention based control strategy.
Besides the physiological signals, human intention can be estimated from kinematics
information. Referring to Indego [55], changes of CoP on the ground are tracked to predict human
movements, such as sit-to-stand or stand-to-sit. Achievement via CoP is obtained but in-depth gait
patterns or biomechanics are required for better control. In order to achieve the gait patterns, inertia
measurement unit (IMU) can be implemented as a promising sensor. This can be noticed in [91],
whereby Peruzzi has estimated the stride length by double integrating the coordinate acceleration
components. With the increased number of IMUs, related gait pattern can be extracted [92] and the
motor abilities of human limbs are assessed [93, 94].
5. Conclusion
In this paper, an insight review has been conducted on the mechanical designs, actuation
systems and control strategies that are currently utilized in robot exoskeletons for rehabilitation
therapy. It should be borne in mind that rehabilitation related robotic exoskeletons are not only
designed to rehabilitate the lower limbs but also for the upper extremities. Nevertheless, significant
emphasis is given on the lower extremity rehabilitation in this review. As per date, there are several
types of exoskeletons which have their own advantages during rehabilitation therapy. Notably, our
discussion is constraint to the treadmill-based and over ground exoskeletons. On the contrary, a
detailed description of the compliance of both the mechanical design and actuation system to the
patients is offered: pneumatic-based, hydraulic-based and SEA actuator systems. Moreover, the
trajectory and intention based control strategies are given priority in this review.
Although research has been done extensively, the technology of robotic exoskeleton is
evolving rapidly. The question of the optimal effectiveness of the treadmill-based and over ground
exoskeleton is still remained open. It is predicted that the over ground exoskeleton has relatively high
potential in expanding its usage as it helps to increase the mobility of the patients, such as to perform
sit-to-stand, stand-to-sit and stairs climbing postures.
Through this study, it broadly reflects that the intention based control strategy is desired in the
next technological shift of robotic rehabilitation. With this new technology push, there is chance to
detect the human intention like gait cycles, stairs motion (both ascent and descent) and movements to
avoid obstacles based on the IMU system. Development of a control strategy by employing the fusion
of non-invasive human physiological signals, such as EMG and EEG, is worth being fully considered
in enhancing the rehabilitation treatment. With this relatively new intention based control strategy, the
rehabilitation outcome is desirable as this strategy engages more initiative from the patient.
Establishing the new concept of real-time control strategies and providing appropriate assistance to
the patients in a timely manner appear to be a new promising technology paradigm in yielding an
optimal rehabilitation therapy.
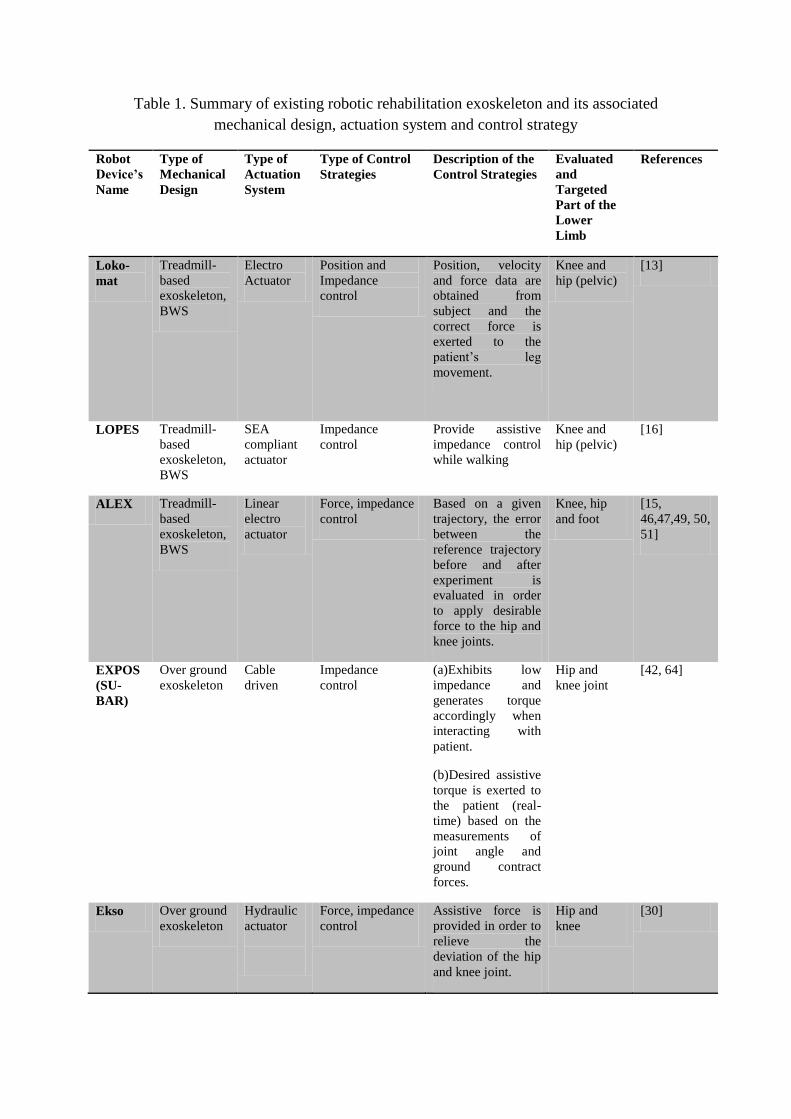
Table 1. Summary of existing robotic rehabilitation exoskeleton and its associated
mechanical design, actuation system and control strategy
Robot
Device’s
Name
Type of
Mechanical
Design
Type of
Actuation
System
Type of Control
Strategies
Description of the
Control Strategies
Evaluated
and
Targeted
Part of the
Lower
Limb
References
Loko-
mat
Treadmill-
based
exoskeleton,
BWS
Electro
Actuator
Position and
Impedance
control
Position, velocity
and force data are
obtained from
subject and the
correct force is
exerted to the
patient’s leg
movement.
Knee and
hip (pelvic)
[13]
LOPES Treadmill-
based
exoskeleton,
BWS
SEA
compliant
actuator
Impedance
control
Provide assistive
impedance control
while walking
Knee and
hip (pelvic)
[16]
ALEX Treadmill-
based
exoskeleton,
BWS
Linear
electro
actuator
Force, impedance
control
Based on a given
trajectory, the error
between the
reference trajectory
before and after
experiment is
evaluated in order
to apply desirable
force to the hip and
knee joints.
Knee, hip
and foot
[15,
46,47,49, 50,
51]
EXPOS
(SU-
BAR)
Over ground
exoskeleton
Cable
driven
Impedance
control
(a)Exhibits low
impedance and
generates torque
accordingly when
interacting with
patient.
(b)Desired assistive
torque is exerted to
the patient (real-
time) based on the
measurements of
joint angle and
ground contract
forces.
Hip and
knee joint
[42, 64]
Ekso Over ground
exoskeleton
Hydraulic
actuator
Force, impedance
control
Assistive force is
provided in order to
relieve the
deviation of the hip
and knee joint.
Hip and
knee
[30]
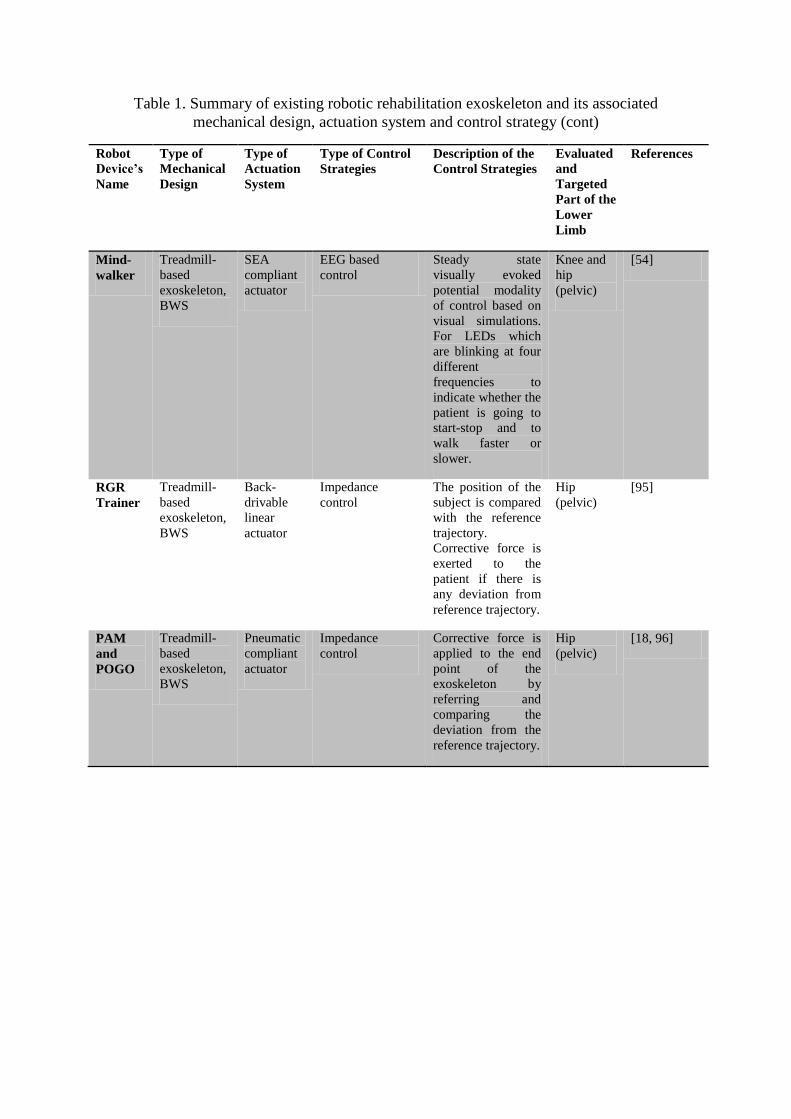
Table 1. Summary of existing robotic rehabilitation exoskeleton and its associated
mechanical design, actuation system and control strategy (cont)
Robot
Device’s
Name
Type of
Mechanical
Design
Type of
Actuation
System
Type of Control
Strategies
Description of the
Control Strategies
Evaluated
and
Targeted
Part of the
Lower
Limb
References
Mind-
walker
Treadmill-
based
exoskeleton,
BWS
SEA
compliant
actuator
EEG based
control
Steady state
visually evoked
potential modality
of control based on
visual simulations.
For LEDs which
are blinking at four
different
frequencies to
indicate whether the
patient is going to
start-stop and to
walk faster or
slower.
Knee and
hip
(pelvic)
[54]
RGR
Trainer
Treadmill-
based
exoskeleton,
BWS
Back-
drivable
linear
actuator
Impedance
control
The position of the
subject is compared
with the reference
trajectory.
Corrective force is
exerted to the
patient if there is
any deviation from
reference trajectory.
Hip
(pelvic)
[95]
PAM
and
POGO
Treadmill-
based
exoskeleton,
BWS
Pneumatic
compliant
actuator
Impedance
control
Corrective force is
applied to the end
point of the
exoskeleton by
referring and
comparing the
deviation from the
reference trajectory.
Hip
(pelvic)
[18, 96]
References
1. Anderson KD. Targeting recovery: Priorities of the spinal cord-injured population. J
Neurotraum. 2004;21(10):1371-83.
2. Reinkensmeyer DJ, Emken JL, Cramer SC. Robotics, motor learning, and neurologic
recovery. Annu Rev Biomed Eng. 2004;6:497-525.
3. Behmran AL, Harkema SJ. Locomotor training after human spinal cord injury: A series of
case studies. Phys Ther. 2000;80(7):688-700.
4. Calautti C, Baron JC. Functional neuroimaging studies of motor recovery after stroke in
adults: a review. Stroke. 2003;34(6):1553-66.
5. Riener R, Lunenburger L, Jezernik S, Anderschitz M, Colombo G, Dietz V. Patient-
cooperative strategies for robot-aided treadmill training: First experimental results. IEEE T Neur Sys
Reh. 2005;13(3):380-94.
6. Wirz M, Zemon DH, Rupp R, Scheel A, Colombo G, Dietz V, et al. Effectiveness of
automated locomotor training in patients with chronic incomplete spinal cord injury: A multicenter
trial. Arch Phys Med Rehab. 2005;86(4):672-80.
7. Coenen P, van Werven G, van Nunen MPM, Van Dieen JH, Gerrits KHL, Janssen TWJ.
Robot-Assisted Walking Vs Overground Walking in Stroke Patients: An Evaluation of Muscle
Activity. J Rehabil Med. 2012;44(4):331-7.
8. Laufer Y, Dickstein R, Chefez Y, Marcovitz E. The effect of treadmill training on the
ambulation of stroke survivors in the early stages of rehabilitation: A randomized study. J Rehabil Res
Dev. 2001;38(1):69-78.
9. Krebs HI, Hogan N. Therapeutic robotics: A technology push. P IEEE. 2006;94(9):1727-38.
10. Magagnin V, Bo I, Turiel M, Fornari M, Caiani EG, Porta A. Effects of robot-driven gait
orthosis treadmill training on the autonomic response in rehabilitation-responsive stroke and cervical
spondylotic myelopathy patients. Gait&Posture. 2010;32(2):199-204.
11. Van den Brand R, Heutschi J, Barraud Q, DiGiovanna J, Bartholdi K, Huerlimann M, et al.
Restoring Voluntary Control of Locomotion after Paralyzing Spinal Cord Injury. Science.
2012;336(6085):1182-5.
12. Pietrusinski M, Cajigas I, Mizikacioglu Y, Goldsmith M, Bonato P, Mavroidis C, Gait
Rehabilitation therapy using robot generated force fields applied at the pelvis. Proceedings of the
IEEE Haptics Symposium, (HAPTICS'10), 2010 March 25-26, Waltham, Mass, USA, 2010. p. 401-7.
13. Colombo G, Joerg M, Schreier R, Dietz V. Treadmill training of paraplegic patients using a
robotic orthosis. J Rehabil Res Dev. 2000;37(6):693-700.
14. Motorika. (2004). Retrieved 1 September, 2013, from
http://www.motorika.com/?categoryId=91202
15. Kao PC, Srivastava S, Agrawal SK, Scholz JP. Effect of robotic performance-based error-
augmentation versus error-reduction training on the gait of healthy individuals. Gait Posture.
2013;37(1):113-20.
16. Veneman JF, Kruidhof R, Hekman EEG, Ekkelenkamp R, Van Asseldonk EHF, van der
Kooij H. Design and evaluation of the LOPES exoskeleton robot for interactive gait rehabilitation.
IEEE T Neur Sys Reh. 2007;15(3):379-86.
17. Hussain S, Xie SQ, Jamwal PK, Parsons J. An intrinsically compliant robotic orthosis for
treadmill training. Med Eng Phys. 2012;34(10):1448-53.
18. Reinkensmeyer DJ, Aoyagi D, Emken JL, Galvez JA, Ichinose W, Kerdanyan G, et al. Tools
for understanding and optimizing robotic gait training. J Rehabil Res Dev. 2006;43(5):657-70.
19. Hesse S, Uhlenbrock D. A mechanized gait trainer for restoration of gait. J Rehabil Res Dev.
2000;37(6):701-8.
20. Yano H, Tamefusa S, Tanaka N, Saitou H, Iwata H, editors. Gait rehabilitation system for
stair climbing and descending. Proceedings of the IEEE Haptics Symposium, (HAPTICS), 2010
March 25-26, Waltham, Mass, USA, 2010. p. 393 - 400.
21. Freivogel S, Mehrholz J, Husak-Sotomayor T, Schmalohr D. Gait training with the newly
developed'LokoHelp'-system is feasible for non-ambulatory patients after stroke, spinal cord and brain
injury. A feasibility study. Brain Injury. 2008;22(7-8):625-32.
22. Schmitt C, Métrailler P, Al-Khodairy A, Brodard R, Fournier J, Bouri M, et al., The Motion
Maker™: a Rehabilitation System Combining an Orthosis with Closed-Loop Electrical Muscle
Stimulation. Proceedings of the 8th Vienna International Workshop in Functional Electrical
Stimulation, Vienna, Austria, 2004.
23. Bouri M, Le Gall B, Clavel R . A new concept of parallel robot for rehabilitation and fitness:
the Lambda. Proceedings of the IEEE International Conference on Robotics and
Biomimetics,(ROBIO), 2009 Dec 19-23,Guilin, China, 2009. p.2503-8.
24. Homma K, Fukuda O, Sugawara J, Nagata Y, Usuba M. A wire-driven leg rehabilitation
system: development of a 4-DOF experimental system. Proceedings of the International Conference
on Advanced Intelligent Mechatronics, (IEEE/ASME), 2003 July 2, Piscataway, NJ, USA, p.908-13.
25. Roy A, Krebs HI, Williams DJ, Bever CT, Forrester LW, Macko RM, et al. Robot-Aided
Neurorehabilitation: A Novel Robot for Ankle Rehabilitation. IEEE T Robot. 2009;25(3):569-82.
26. Blaya JA, Herr H. Adaptive control of a variable-impedance ankle-foot orthosis to assist
drop-foot gait. IEEE T Neur Sys Reh. 2004;12(1):24-31.
27. Ferris DP, Czerniecki JM, Hannaford B. An ankle-foot orthosis powered by artificial
pneumatic muscles. J Appl Biomech. 2005;21(2):189-97.
28. Satici AC, Erdogan A, Patoglu V. Design of a reconfigurable ankle rehabilitation robot and its
use for the estimation of the ankle impedance. Proceedings of the IEEE International Conference on
Rehabilitation Robotics, (ICORR), 2009 June 23-26. Kyoto, Japan, 2009. p. 257-64.
29. Zeilig G, Weingarden H, Zwecker M, Dudkiewicz I, Bloch A, Esquenazi A. Safety and
tolerance of the ReWalk (TM) exoskeleton suit for ambulation by people with complete spinal cord
injury: A pilot study. J Spinal Cord Med. 2012;35(2):96-101.
30. Ekso Bionics. (2012). Retrieved 2 September, 2013, from http://www.eksobionics.com/ekso
31. Indego Powering People Forward. (2012). Retrieved 1 September, 2013, from
http://www.parker.com/literature/Exoskeleton/Parker%20Indego%20Brochure.pdf
32. Sawicki GS, Ferris DP. A pneumatically powered knee-ankle-foot orthosis (KAFO) with
myoelectric activation and inhibition. J Neuroeng Rehabil. 2009;6:23
33. Yu H, Cruz MS, Chen G, Huang S, Zhu C, Chew E, et al. Mechanical Design of a Portable
Knee-Ankle-Foot Robot. Proceedings of IEEE International Conference on Robotics and Automation
(ICRA) 2013 may 6-10, Karlsruhe, Germany, 2013. p.2175-80.
34. Ghan J, Steger R, Kazerooni H. Control and system identification for the Berkeley lower
extremity exoskeleton (BLEEX). Adv Robotics. 2006;20(9):989-1014.
35. Zoss A, Kazerooni H. Architecture and hydraulics of a lower extremity exoskeleton.
Proceedings of the ASME Dynamic Systems and Control Division, 2005 Nov 5-11, Orlando, USA,
2005, p.1447-55.
36. Kazerooni H, Steger R, Huang LH. Hybrid control of the Berkeley Lower Extremity
Exoskeleton (BLEEX). Int J Robot Res. 2006;25(5-6):561-73.
37. Kawamoto H, Sankai Y. Comfortable power assist control method for walking aid by HAL-3.
Proceedings of IEEE International Conference on Systems, Man and Cybernetics, 2002 Oct 6-9, p.6.
38. Kawamoto H, Lee S, Kanbe S, Sankai Y, editors. Power assist method for HAL-3 using
EMG-based feedback controller. Proceedings of IEEE International Conference on Systems, Man and
Cybernetics,2003 Oct 5-8. P.1648-53.
39. Ruthenberg BJ, Wasylewski NA, Beard JE. An experimental device for investigating the
force and power requirements of a powered gait orthosis. J Rehabil Res Dev. 1997;34:203-14.
40. Patton J, Brown DA, Peshkin M, Santos-Munne JJ, Makhlin A, Lewis E, et al. KineAssist:
Design and development of a robotic overground gait and balance therapy device. Top Stroke Rehabil.
2008;15(2):131-9.
41. Stauffer Y, Allemand Y, Bouri M, Fournier J, Clavel R, Metrailler P, et al. The
WalkTrainer—a new generation of walking reeducation device combining orthoses and muscle
stimulation. IEEE T Neur Sys Reh. 2009;17(1):38-45.
42. Kong KC, Jeon D. Design and control of an exoskeleton for the elderly and patients. IEEE-
Asme TMech. 2006; 11(4): p.428-32.
43. Guo Z, Fan Y, Zhang J, Yu H, Yin Y. A new 4m model-based human-machine interface for
lower extremity exoskeleton robot. 5th international conference in Intelligent Robotics and
Applications (ICIRA), 2012, Oct 3-5, Montreal, 2012. p.545-54.
44. Luu TP, Lim H, Qu X, Low K. Pelvic motion assistance of NaTUre-gaits with adaptive body
weight support. 8th Asian Control Conference (ASCC), 2011 May 15-18, Kaohsiung, 2011, p.950-5.
45. G. R. West. Powered gait orhtosis and method of utilizing same. patent 6689075. 2004.
46. Banala SK, Agrawal SK, Scholz JP. Active Leg Exoskeleton (ALEX) for gait rehabilitation
of motor-impaired patients. Proceedings of the IEEE 10th International Conference on Rehabilitation
Robotics (ICORR); 2007 Jun 13-15; Noordwijk aan Zee, The Netherlands. 2007. p.401-7.
47. Agrawal SK, Banala SK, Fattah A, Sangwan V, Krishnamoorthy V, Scholz JR, et al.
Assessment of motion of a swing leg and gait rehabilitation with a gravity balancing exoskeleton.
IEEE T Neur Sys Reh. 2007;15(3):410-20.
48. Winfree KN, Stegall P, Agrawal SK. Design of a Minimally Constraining, Passively
Supported Gait Training Exoskeleton: ALEX II. Proceedings of the 2011 IEEE International
Conference on Rehabilitation Robotics (ICORR); 2011 Jun 29-Jul 1; Zurich, Switzerland. 2011. p.1-6.
49. Kim SH, Banala SK, Brackbill EA, Agrawal SK, Krishnamoorthy V, Scholz JP. Robot-
assisted modifications of gait in healthy individuals. Exp Brain Res. 2010;202(4):809-24.
50. Zanotto D, Rosati G, Avanzini F, Stegall P, Agrawal SK. Robot-assisted gait training with
complementary auditory feedback: results on short-term motor adaptation. Proceedings of the 4th
IEEE RAS & EMBS International Conference on Biomedical Robotics and Biomechatronics
(BioRob), 2012 June 24-27; Rome, Italy. 2012. p.1388-93.
51. Stegall P, Winfree KN, Agrawal SK. Degrees-of-Freedom of a Robotic Exoskeleton and
Human Adaptation to New Gait Templates. Proceedings of the 11th IEEE International Conference
on Robotics and Automation (ICRA); 2012 May 14-18; Saint Paul, MN. 2012. p.4986-4991.
52. Veneman JF, Ekkelenkamp R, Kruidhof R, van der Helm FCT, van der Kooij H. A series
elastic- and Bowden-cable-based actuation system for use as torque actuator in exoskeleton-type
robots. Int J Robot Res. 2006;25(3):261-81.
53. Hussain S, Xie SQ, Jamwal PK. Robust Nonlinear Control of an Intrinsically Compliant
Robotic Gait Training Orthosis. IEEE T Syst, Man, Cybern. 2013;43(3):655-65.
54. Mind controlled orthosis and VR training environment for walk empowering
(MINDWALKER). Retrieved 1 October, 2013, from https://www.mindwalker-project.eu/
55. Quintero HA, Farris RJ, Hartigan C, Clesson I, Goldfarb M. A Powered Lower Limb Orthosis
for Providing Legged Mobility in Paraplegic Individuals. Top Spinal Cord Inj Rehabil.
2011;17(1):25-33.
56. Turk R, Obreza P. Functional Electrical-Stimulation as an Orthotic Means for the
Rehabilitation of Paraplegic Patients. Paraplegia. 1985;23(6):344-8.
57. Winter DA, Sienko SE. Biomechanics of below-knee amputee gait. J Biomech.
1988;21(5):361-7.
58. Prilutsky BI, Petrova LN, Raitsin LM. Comparison of mechanical energy expenditure of joint
moments and muscle forces during human locomotion. J Biomech. 1996;29(4):405-15.
59. Nagano A, Ishige Y, Fukashiro S. Comparison of new approaches to estimate mechanical
output of individual joints in vertical jumps. J Biomech. 1998;31(10):951-5.
60. Nadeau S, McFadyen BJ, Malouin F. Frontal and sagittal plane analyses of the stair climbing
task in healthy adults aged over 40 years: what are the challenges compared to level walking? Clin
Biomech. 2003;18(10):950-9.
61. DeVita P, Torry M, Glover KL, Speroni DL. A functional knee brace alters joint torque and
power patterns during walking and running. J Biomech. 1996;29(5):583-8.
62. Riener R, Rabuffetti M, Frigo C. Joint powers in stair climbing at different slopes.
Proceedings of the IEEE International Conference on Engineering in Medicine and Biology; 1999 Oct
13-16; Atlanta, GA. 1999. p. 530.
63. Jacobs R, Bobbert MF, van Ingen Schenau GJ. Mechanical output from individual muscles
during explosive leg extensions: the role of biarticular muscles. J Biomech. 1996;29(4):513-23.
64. Carse B, Meadows B, Bowers R, Rowe P. Affordable clinical gait analysis: An assessment of
the marker tracking accuracy of a new low-cost optical 3D motion analysis system. Physiotherapy.
2013. In Press.
65. Yin YH, Fan YJ, Xu LD. EMG and EPP-Integrated Human–Machine Interface Between the
Paralyzed and Rehabilitation Exoskeleton. IEEE T Inf Technol Biomed. 2012;16(4):542-9.
66. Wang P, Low KH, Tow A. Synchronized Walking Coordination for Impact-less Footpad
Contact of an Overground Gait Rehabilitation System: NaTUre-gaits. Proceedings of the IEEE
International Conference on Rehabilitation Robotics (ICORR), 2011 June 29 -July 1, Zurich,
2011.p.1-6.
67. Wang P, Low KH, Tow A, Lim PH. Initial System Evaluation of an Overground
Rehabilitation Gait Training Robot (NaTUre-gaits). Adv Robotics. 2011;25(15):1927-48.
68. Lee SJ, Hidler J. Biomechanics of overground vs. treadmill walking in healthy individuals. J
Appl Physiol. 2008;104(3):747-55.
69. Lim HB, Luu TP, Hoon KH, Qu XD, Tow A, Low KH. Study of Body Weight Shifting on
Robotic Assisted Gait Rehabilitation with NaTUre-gaits. Proceedings of the 2011 IEEE/RSJ
International Conference on Intelligent Robots and Systems (IROS); 2011 Sep 25-30; San Francisco,
CA. 2011. p. 4923-8.
70. Pratt GA, Williamson MM. Series elastic actuators. Proceedings of the 1995 IEEE/RSJ
International Conference on Intelligent Robots and Systems 'Human Robot Interaction and
Cooperative Robots'; 1995 Aug 5-9; Pittsburgh, PA. 1995.p. 200-5.
71. Williamson MM. Series elastic actuators. 1995.
72. Yu H, Huang S, Chen G, Toh S-L, Cruz MS, Ghorbel Y, et al. Design and analysis of a novel
compact compliant actuator with variable impedance. Proceedings of the 2012 IEEE International
Conference on Robotics and Biomimetics (ROBIO); 2012 Dec 11-14; Guangzhou, China. 2012. p.
1188-93.
73. Lotze M, Braun C, Birbaumer N, Anders S, Cohen LG. Motor learning elicited by voluntary
drive. Brain. 2003;126:866-72.
74. Lam T, Pauhl K, Krassioukov A, Eng JJ. Using robot-applied resistance to augment body-
weight–supported treadmill training in an individual with incomplete spinal cord injury. Phys Ther.
2011;91(1):143-51.
75. Ekkelenkamp R, Veneman J, van der Kooij H. LOPES: Selective control of gait functions
during the gait rehabilitation of CVA patients. Proceedings of the 9th International Conference on
Rehabilitation Robotics; 2005 Jun 28-Jul 1; Chicago, Illinois. 2005. p.361-4.
76. Banala SK, Kim SH, Agrawal SK, Scholz JP. Robot Assisted Gait Training With Active Leg
Exoskeleton (ALEX). IEEE T Neur Sys Reh. 2009;17(1):2-8.
77. Duschau-Wicke A, von Zitzewitz J, Caprez A, Lunenburger L, Riener R. Path Control: A
Method for Patient-Cooperative Robot-Aided Gait Rehabilitation. IEEE T Neur Sys Reh.
2010;18(1):38-48.
78. Vallery H, van Asseldonk EHF, Buss M, van der Kooij H. Reference Trajectory Generation
for Rehabilitation Robots: Complementary Limb Motion Estimation. IEEE T Neur Sys Reh.
2009;17(1):23-30.
79. Ronsse R, Lenzi T, Vitiello N, Koopman B, van Asseldonk E, De Rossi SMM, et al.
Oscillator-based assistance of cyclical movements: model-based and model-free approaches. Med
Biol Eng Comput. 2011;49(10):1173-85.
80. Jezernik S, Colombo G, Morari M. Automatic gait-pattern adaptation algorithms for
rehabilitation with a 4-DOF robotic orthosis. IEEE T Robotic Autom. 2004;20(3):574-82.
81. Lenzi T, De Rossi SMM, Vitiello N, Carrozza MC. Intention-Based EMG Control for
Powered Exoskeletons. IEEE T Bio-Med Eng. 2012;59(8):2180-90.
82. Cain SM, Gordon KE, Ferris DP. Locomotor adaptation to a powered ankle-foot orthosis
depends on control method. J Neuroeng Rehabil. 2007;4(1):48.
83. Cheron G, Duvinage M, De Saedeleer C, Castermans T, Bengoetxea A, Petieau M, et al.
From Spinal Central Pattern Generators to Cortical Network: Integrated BCI for Walking
Rehabilitation. Neural Plast 2012.
84. Gwin JT, Gramann K, Makeig S, Ferris DP. Electrocortical activity is coupled to gait cycle
phase during treadmill walking. Neuroimage. 2011;54(2):1289-96.
85. Gwin JT, Gramann K, Makeig S, Ferris DP. Removal of Movement Artifact From High-
Density EEG Recorded During Walking and Running. J Neurophysiol. 2010;103(6):3526-34.
86. Petersen TH, Willerslev-Olsen M, Conway BA, Nielsen JB. The motor cortex drives the
muscles during walking in human subjects. J Physiol. 2012; 590(10): 2443-52
87. Gwin JT, Ferris DP. An EEG-based study of discrere isometric and isotonic human lower
limb muscle contractions. J. Neuroeng. Rehabil, 2012; 9(35):1-13
88. Athanasiou A, Lithari C, Kalogianni K, Klados M A, and Bamidis P D. Source Detection and
functional connectivity of the Sensorimotor Cortex during actual and Imaginary Limb Movement: A
preliminary Study on the Implementation of eCoonectome in Motor Imagery Protocols. Advances in
Human-Computer Interaction, 2012, 10.
89. Gramann K, Gwin JT, Ferris DP, Oie K, Jung TP, Lin CT, Liao LD, Makeig S. Cognition in
action: imaging brain/body dynamics in mobile humans. Rev. Neurosci. 2011, 22(6), 593-608.
90. Gwin JT, Gramann K, Makeig S, Ferris DP. Electrocortical activity is coupled to gait cycle
phase during treadmill walking. Neuroimage. 2011 Jan 15;54(2):1289-96.
91. Peruzzi A, Della Croce U, Cereatti A. Estimation of stride length in level walking using an
inertial measurement unit attached to the foot: A validation of the zero velocity assumption during
stance. J Biomech. 2011;44(10):1991-4.
92. Beravs T, Rebersek P, Novak D, Podobnik J, Munih M. Development and validation of a
wearable inertial measurement system for use with lower limb exoskeletons. Proceedings of the 11th
IEEE-RAS International Conference on Humanoid Robots (Humanoids); 2011 Oct 26–28; Bled,
Slovenia. 2011. p. 212-7.
93. Hester T, Hughes R, Sherrill DM, Knorr B, Akay M, Stein J, et al. Using wearable sensors to
measure motor abilities following stroke. Proceedings of the International Workshop on Wearable and
Implantable Body Sensor Networks; 2006 Apr 3–5; Cambridge, MA. p. 5-8.
94. Patel S, Lorincz K, Hughes R, Huggins N, Growdon J, Standaert D, et al. Monitoring motor
fluctuations in patients with Parkinson's disease using wearable sensors. IEEE T Inf Technol Biomed.
2009;13(6):864-73.
95. Pietrusinski M D, The robotic gait rehabilitation trainer Mechanical Engineering Dissertations.
2012.
96. Marchal-Crespo L and Reinkensmeyer D J. Review of control strategies for robotic
movement training after neurologic injury. J. Neuroeng. Rehabil. 2009; 6:20.
View publication statsView publication stats





























