Embed Size (px)
Citation preview

International Hepatology
A revolution in HCV treatment with direct-acting antivirals:From non-response to eradication
Tarik Asselah⇑
Hepatology Department, AP-HP, University Paris Diderot 7 and INSERM U773, CRB3, Beaujon Hospital, Clichy, France
COMMENTARY ON:Preliminary study of two antiviral agents for hepatitis C geno-type 1. Lok AS, Gardiner DF, Lawitz E, Martorell C, Everson GT,Ghalib R, Reindollar R, Rustgi V, McPhee F, Wind-Rotolo M,Persson A, Zhu K, Dimitrova DI, Eley T, Guo T, Grasela DM, Pas-quinelli C. N Engl J Med 2012 January 19;366(3):216–24. Copy-rigth (2012). Abstract reprinted with permission from theMassachusetts Medical Society.
http://www.ncbi.nlm.nih.gov/pubmed/22256805
Abstract: Background: Patients with chronic hepatitis C virus(HCV) infection who have not had a response to therapy with pegin-terferon and ribavirin may benefit from the addition of multipledirect-acting antiviral agents to their treatment regimen.Methods: This open-label, phase 2a study included an exploratorycohort of 21 patients with chronic HCV genotype 1 infection whohad not had a response to previous therapy (i.e., had not had P2log(10) decline in HCV RNA after P12 weeks of treatment withpeginterferon and ribavirin). We randomly assigned patients toreceive the NS5A replication complex inhibitor daclatasvir (60 mgonce daily) and the NS3 protease inhibitor asunaprevir (600 mgtwice daily) alone (group A, 11 patients) or in combination withpeginterferon alfa-2a and ribavirin (group B, 10 patients) for24 weeks. The primary end point was the percentage of patients witha sustained virologic response 12 weeks after the end of the treat-ment period.Results: A total of 4 patients in group A (36%; 2 of 9 with HCV geno-type 1a and 2 of 2 with genotype 1b) had a sustained virologicresponse at 12 weeks after treatment and also at 24 weeks aftertreatment. Six patients (all with HCV genotype 1a) had viral break-through while receiving therapy, and resistance mutations to bothantiviral agents were found in all cases; 1 patient had a viralresponse at the end of treatment but had a relapse after the treat-ment period. All 10 patients in group B had a sustained virologicresponse at 12 weeks after treatment, and 9 had a sustained virologicresponse at 24 weeks after treatment. Diarrhea was the most
Journal of Hepatology 20
Keywords: Interferon free regimen; NS5A inhibitors; Null response; Proteaseinhibitors; Immune response; Genotype 1.Received 10 March 2012; received in revised form 16 March 2012; accepted 18 March2012⇑ Tel.: +33 (0)140875579.E-mail address: [email protected]: HCV, hepatitis C virus; PegIFN, peginterferon alfa; RBV, ribavirin;SVR, sustained virologic response; DAAs, direct-acting antivirals.
common adverse event in both groups. Six patients had transient ele-vations of alanine aminotransferase levels to more than three timesthe upper limit of the normal range.Conclusions: This preliminary study involving patients with HCVgenotype 1 infection who had not had a response to prior therapyshowed that a sustained virologic response can be achieved withtwo direct-acting antiviral agents only. In addition, a high rate ofsustained virologic response was achieved when the two direct-act-ing antiviral agents were combined with peginterferon alfa-2a andribavirin. (Funded by Bristol-Myers Squibb; ClinicalTrials.gov num-ber, NCT01012895.).
� 2012 European Association for the Study of the Liver. Publishedby Elsevier B.V. All rights reserved.
Approximately 170 million people are infected with hepatitisC virus (HCV) worldwide. Treatment of genotype 1 naïve chronichepatitis C with peginterferon alfa (PegIFN) and ribavirin (RBV)for 48 weeks results in sustained virologic response (SVR) inapproximately 40% of patients. Retreatment of previous non-responders to PegIFN/RBV therapy with triple therapy, a proteaseinhibitor (telaprevir or boceprevir), PegIFN/RBV, results in an SVRin less than 30% of cases [1,2]. Direct-acting antivirals (DAAs)with different viral targets, including NS3 protease inhibitors,nucleoside/nucleotide analogues and non-nucleoside inhibitorsof the RNA-dependent RNA polymerase, and NS5A inhibitorsare under development [3]. Gane and colleagues found that acombination of two DDAs can suppress HCV RNA in genotype 1non-responder patients but the treatment with the DAAs combi-nation was limited to 13 days and was followed immediately bytreatment with PegIFN/RBV, thus preventing the assessment ofSVR with DAAs alone [4]. Studies of DAAs combinations in thegenotype 1 non-responder population are warranted.
Recently, Lok et al., in a preliminary study including patientswith HCV genotype 1 infection who were non-responders to priortherapy, showed that an SVR could be achieved with two DAAs[5].
Daclatasvir (BMS-790052) is a first-in-class, highly selectiveHCV NS5A replication complex inhibitor with picomolar potencyin vitro [6]. NS5A is a membrane-associated phosphoprotein pres-ent in basally phosphorylated (p56) and hyperphosphorylated(p58) forms. It was previously reported that only p58-defectivemutants could be complemented in trans, and NS5A is involvedin HCV virion production, suggesting that different forms ofNS5A exert multiple functions at various stages of the viral life
12 vol. 57 j 455–457

Group A: Daclastavir + AsunaprevirGroup B: Daclastavir + Asunaprevir + PegIFNα/RBV
0
20
40
60
80
100
SVR
(%)
n =Wk4 Wk12 Wk24
EOT SVR
64
11
7
60
10
6
46
11
5
90
10
9
46
11
5
100
10
10
36
11
4
90*
10
9
Group A
Group B
Week
QOLLDOLL
Post-treatment
0 1 2 3 4 6 8 10 12 16 20 1
2
3
4
5
6
7
24
Follow-up Daclatasvir + Asunaprevir +
HC
V R
NA
(log 10
IU/m
l)
4 12 24
QOLLLLOD
Follow-up Daclatasvir + Asunaprevir + PegIFNα/RBV
1
2
3
4
5
6
7
HC
V R
NA
(log 10
IU/m
l)
Week Post-treatment
0 1 2 3 4 6 8 10 12 16 20 24 4 12 24
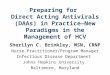
Fig. 1. Virologic response. (Group A) Four patients (36%) had an SVR at 12 weeksafter the end of the treatment period, and all four also had an SVR at week 24 aftertreatment. Six patients (all with HCV genotype 1a) had a viral breakthrough whilereceiving therapy; 1 patient had a viral response at the end of treatment butrelapsed after the treatment period. (Group B) (1) 10/10 patients had undetect-able HCV RNA by week 6 of therapy with no viral breakthrough; (2) 10/10patients achieved SVR12 and 9/10 achieved SVR24; (3) 1 patient <LLOQ at week 24post-treatment was undetectable on retesting, 1 and 3 months later. Adaptedfrom [5], with permission from the Massachusetts Medical Society.
International Hepatology
cycle. The N terminus of NS5A (domain I) has been crystallized inalternative dimeric forms and contains both zinc- and RNA-bind-ing domains, properties that have been demonstrated in vitro.Daclatasvir is active at picomolar concentrations in vitro towardsreplicons expressing a broad range of HCV genotypes and acts inan additive to synergistic way with interferon and other smallmolecule antiviral compounds [6,7]. The resistance profile ofBMS-790052 reveals that inhibitor sensitivity maps to the N ter-minus of domain 1 of NS5A [6–8]. In addition, it has been demon-strated that NS5A inhibitors could block hyperphosphorylation ofNS5A, which is believed to play an essential role in the viral lifecycle.Asunaprevir (BMS-650032) is a highly active HCV NS3 prote-ase inhibitor. NS3 serine protease is located at the N-terminalregion of NS3. The NS3 serine protease domain associates withthe NS4A co-factor to cleave four specific sites. This enzymehas been extensively characterized at the biochemical level andits structure is known [9]. The serine protease activity of NS3 isan attractive target for new drugs that could effectively blockviral replication. Protease inhibitors have high anti-viral efficacyand usually a low genetic barrier. The genetic barrier to resis-tance is defined as the number of amino acid substitutionsrequired to confer full resistance to a drug. The genetic barrierto protease inhibitors and NS5A inhibitors is usually low.
Both daclatasvir and asunaprevir produce marked declines inHCV RNA levels in patients with HCV genotype 1 infection [10,11]and administration of the two drugs in combination did not pro-duce a clinically meaningful pharmacokinetic interaction [12].
In the study reported by Lok et al., patients with HCV genotype1 infection, with no response to previous treatment with PegIFN/RBV, were randomly assigned to receive daclatasvir (60 mg oncedaily) and asunaprevir (600 mg twice daily) alone (group A, 11patients) or in combination with PegIFNa-2a and RBV (group B,10 patients) for 24 weeks [5]. A total of 4 patients in group A(36%; 2 of 9 with HCV genotype 1a and 2 of 2 with genotype1b) had an SVR 12 weeks after treatment and also 24 weeks aftertreatment (Fig. 1). Six patients (all with HCV genotype 1a) had aviral breakthrough while receiving therapy, and resistance muta-tions to both antiviral agents were found in all cases; 1 patienthad a viral response at the end of treatment but relapsed afterthe treatment period.
Viral variants in the NS5A domain included Q30R, L31M/V,and Y93C/N; variants in the NS3 protease domain includedR155K and D168A/E/T/V/Y. The patient with a viral relapse hada pre-existing NS3 protease resistance variant, R155K, at baselineand at the time of viral relapse, whereas the NS5A resistance var-iant Q30E was only detected at relapse. Although there were only2 patients with HCV genotype 1b infection in group A, the obser-vation that both of the patients had an SVR with two direct-act-ing antiviral agents alone may reflect a higher resistance barrierfor this combination of drugs in patients with HCV genotype 1binfection than in those with HCV genotype 1a infection. The highfrequency of resistance seen in patients with HCV genotype 1ainfection who were treated with DAAs alone suggests that studiesof DAAs combinations without PegIFN/RBV in patients with HCVgenotype 1a infection should proceed carefully. In group B, theinclusion of Peg IFN/RBV with daclatasvir and asunaprevir pro-vided sufficient antiviral activity to suppress the emergence ofresistance. All 10 patients in group B had an SVR 12 weeks aftertreatment, and 9 had an SVR 24 weeks after treatment.
456 Journal of Hepatology 201
It should be noticed that among the 14 patients who had anSVR 12 weeks after treatment, a HCV RNA level of less than25 IU/ml was detected in 1 patient 24 weeks after treatmentand in 2 other patients 48 weeks after treatment. All 3 patientshad undetectable HCV RNA on re-testing. These data indicate thatlate relapse is unlikely to occur in patients who have an SVR with
2 vol. 57 j 455–457

JOURNAL OF HEPATOLOGY
the DAAs combination, 12 weeks after treatment as previouslyestablished with PegIFN/RBV treatment [13].The most common adverse events were diarrhea, fatigue,headache, and nausea. Most adverse events were mild to moder-ate. There were no deaths, serious adverse events, or discontinu-ations of study treatment due to adverse events. Diarrhea was themost common adverse event in both groups. Six patients hadtransient elevation of alanine aminotransferase levels to morethan three times the upper limit of the normal range.
Finally, Lok et al. reported interesting results with daclatasvirand asunaprevir combination in HCV genotype 1 non-respondersto previous treatment with PegIFN plus ribavirin [5]. Similarly,Chayama et al. reported impressive results in a pilot study ofcombination therapy with asunaprevir and daclatasvir in 10 Jap-anese patients with HCV genotype 1b infection and who had notresponded to previous therapy with PegIFN/RBV: nine patientsachieved an SVR [14]. Several studies of DAA combinations areongoing with different HCV targets: [3,5,14,15]. Preliminaryresults of DAA combinations show increased antiviral efficacy,reduced resistance and a good safety profile. It is important tonote that some of these drugs have pan-genotypic activity. Thisrapid progress strongly suggests that in the near future, IFN-freeshort duration DAA combinations will make HCV the first chronicviral infection to be eradicated worldwide.
Conflict of interest
Tarik Asselah is a speaker and investigator for BMS, Boehring-Ingelheim, Tibotec, Janssen, Gilead, Roche and MSD.
References
[1] Zeuzem S, Andreone P, Pol S, et al. Telaprevir for retreatment of HCVinfection. N Engl J Med 2011;364:2417–2428.
Journal of Hepatology 201
[2] Bacon BR, Gordon SC, Lawitz E, et al. Boceprevir for previously treatedchronic HCV genotype 1 infection. N Engl J Med 2011;364:1207–1217.
[3] Asselah T, Marcellin P. Direct acting antivirals for the treatment of chronichepatitis C: one pill a day for tomorrow. Liver Int 2012;32:88–102.
[4] Gane E, Roberts S, Stedman C, et al. Oral combination therapy with anucleoside polymerase inhibitor (RG7128) and danoprevir for chronichepatitis C genotype 1 infection (INFORM-1): a randomised, double-blind,placebo-controlled, dose-escalation trial. Lancet 2010;376:1467–1475.
[5] Lok AS, Gardiner DF, Lawitz E, et al. Preliminary study of two antiviral agentsfor hepatitis C genotype 1. N Engl J Med 2012;366:216–224.
[6] Gao M, Nettles RE, Belema M, et al. Chemical genetics strategy identifies anHCV NS5A inhibitor with a potent clinical effect. Nature 2010;465:96–100.
[7] Asselah T. NS5A inhibitors: a new breakthrough for the treatment of chronichepatitis C. J Hepatol 2011;54:1069–1072.
[8] Fridell RA, Wang C, Sun JH, et al. Genotypic and phenotypic analysis ofvariants resistant to hepatitis C virus nonstructural protein 5A replicationcomplex inhibitor BMS-790052 in humans: in vitro and in vivo correlations.Hepatology 2011;54:1924–1935.
[9] Kim JL, Morgenstern KA, Lin C, et al. Crystal structure of the hepatitis C virusNS3 protease domain complexed with a synthetic NS4A cofactor peptide.Cell 1996;87:343–355.
[10] Nettles RE, Gao M, Bifano M, et al. Multiple ascending dose study of BMS-790052, a nonstructural protein 5A replication complex inhibitor, in patientsinfected with hepatitis C virus genotype 1. Hepatology 2011;54:1956–1965.
[11] Pasquinelli C, Eley T, Villegas C, et al. Safety, tolerability, pharmacokineticsand antiviral activity following single- and multiple-dose administration ofBMS-650032, a novel HCV NS3 inhibitor, in subjects with chronic genotype 1HCV infection. Hepatology 2009;50:411A, abstract.
[12] Bifano M, Sevinsky H, Bedford BR, et al. Co-administration of BMS-790052and BMS-650032 does not result in a clinically meaningful pharmacokineticinteraction in healthy subjects. Hepatology 2010;52:719A, abstract.
[13] Martinot-Peignoux M, Stern C, Maylin S, Ripault MP, Boyer N, Leclere L, et al.Twelve weeks posttreatment follow-up is as relevant as 24 weeks todetermine the sustained virologic response in patients with hepatitis Cvirus receiving pegylated interferon and ribavirin. Hepatology 2010;51:1122–1126.
[14] Chayama K, Takahashi S, Toyota J, et al. Dual therapy with the nonstructuralprotein 5A inhibitor, daclatasvir, and the nonstructural protein 3 proteaseinhibitor, asunaprevir, in hepatitis C virus genotype 1b-infected nullresponders. Hepatology 2012;55:742–748.
[15] Zeuzem S, Asselah T, Angus P, et al. Efficacy of the protease inhibitorBI201335, polymerase inhibitor BI 207127, and ribavirin in patients withchronic HCV infection. Gastroenterology 2011;141:2047–2055.
2 vol. 57 j 455–457 457
















![[2015] hcv direct acting antivirals [da as] stumbling](https://img.pdfslide.net/doc/110x75/587a6c621a28ab8a2a8b6c4d/2015-hcv-direct-acting-antivirals-da-as-stumbling.jpg)











