Embed Size (px)
Citation preview

Continuing Education
A SimplifiedAesthetic Concept
Historical Review and Current Clinical Application
Authored by Douglas A. Terry, DDS and Karl F. Leinfelder, DDS, MS
Course Number: 105.1
Upon successful completion of this CE activity 1 CE credit hour may be awarded
A Peer-Reviewed CE Activity by
Opinions expressed by CE authors are their own and may not reflect those of Dentistry Today. Mention of
specific product names does not infer endorsement by Dentistry Today. Information contained in CE articles and
courses is not a substitute for sound clinical judgment and accepted standards of care. Participants are urged
to contact their state dental boards for continuing education requirements.
Dentistry Today is an ADA CERPRecognized Provider.
Approved PACE Program ProviderFAGD/MAGD Credit Approvaldoes not imply acceptanceby a state or provincial board ofdentistry or AGD endorsement.June 1, 2006 to May 31, 2009AGD Pace approval number: 309062

ABOUT THE AUTHORS
Dr. Terry received his DDS from theUniversity of Texas Health Science CenterDental Branch at Houston in 1978, wherehe is now an assistant professor of thedepartment of restorative dentistry andbiomaterials. He has published more than
230 articles on various topics in aesthetic dentistry innumerous languages and authored the textbook NaturalAesthetics with Composite Resin. He maintains a privatepractice in Houston emphasizing aesthetic and restorativedentistry. He can be reached at (281) 481-3483.
Dr. Leinfelder earned his doctor of dentalsurgery and master of science (dentalmaterials) degrees from MarquetteUniversity. After serving for 8 years on thefaculty at Marquette, he joined the facultyat the University of North Carolina School
of Dentistry, where he attained the rank of professor anddirector of biomaterials clinical research in the DentalResearch Center. In 1983, he joined the School of Dentistry atthe University of Alabama and held the Joseph Volker Chair.He also served as chairman of the department of biomaterials
until 1994. Presently he holds positions at both universities:adjunct professor at the University of North Carolina andprofessor emeritus at the University of Alabama. He is therecipient of the Dr. George Hollenbeck award (1995) as well asthe Norton N. Ross award for outstanding clinical research(1997), and the American College of ProsthodontistsDistinguished Lecturer Award (1998). He has served asassociate editor of the Journal of the American DentalAssociation. He can be reached at (919) 370-9168.
INTRODUCTION
To fully understand the current approach to treatment,a clinician should be familiar with approaches used in the past. The restorative dentist must consider advances in material science as part of a continuum. Theknowledgeable clinician will be prepared to incorporate newconcepts into an existing paradigm.
Traditionally, hybrid composite resin was used becauseof its strength and fracture resistance, whereas microfillresin was developed to attain not only improvedpolishability, but to maintain the durability of the polish.However, it was soon discovered that this process ofstratification, which used the attributes of both the hybridand the microfill to create an optimal restoration withenhanced mechanical properties, provided anotheradvantage: a variation in the shades and opacities of color.This created a 3-dimensional effect—the polychromaticeffect.1,2 By using an anatomic stratification with successivelayers of dentin and enamel, a more realistic depth of colorcould be achieved,3 as well as surface and opticalcharacteristics that mimic nature.4,5 Therefore, past clinicaland scientific efforts to create a more ideal restorativematerial for function and anatomical form resulted in thedevelopment of color within a restoration, not simply on the surface.
Advances in restorative materials continue to enhance thepractice of dentistry. Newer formulations of composite resinsystems have improved physical, mechanical, and opticalcharacteristics that are directly related to the filler particle size,distribution, orientation, and quantity. Prior to the introductionof the small-particle composite resin, it was often necessary tocombine hybrid and microfilled composites to achieve proper
Continuing Education
1
Recommendations for Fluoride Varnish Use in Caries Management
LEARNING OBJECTIVES:
After reading this article, the individual will learn:
• the historical progression of aesthetic techniques forcomposite resin restorations, and
• a simplified aesthetic stratification technique.
A Simplified AestheticConceptHistorical Review and CurrentClinical Application

aesthetics (ie, luster, color) and mechanical stability (ie, strength, wear resistance, fracture resistance) inadhesive restorations. Since the development of the small-particle composite resin, it appears that theseproperties have been incorporated into a single restorativematerial. Although polychromatic stratification techniquesare still necessary with this re-vised composite resinformulation, they are used only to attain natural aestheticsand color rather than to improve physical characteristics.
This article describes a simplified concept of utilizing anexisting stratification technique with a new biomaterial toimprove the clinical outcome.
NATURAL TOOTH AESTHETICS
The successful aesthetic reproduction of the naturaldentition in terms of color requires an understanding of theinterrelationship of optical properties and the morphology ofthe tooth. As light passes through the natural tooth, it isreflected, refracted, absorbed, or transmitted by themultilayered tooth structure that varies according to theoptical densities of the hydroxyapatite crystals, enamelrods, and dentinal tubules.6 In natural teeth, different colorsare distributed, and various optical characteristics areobserved through the enamel and dentin.2 Thispolychromatic effect manifests in different opticalcharacteristics. These characteristics must be properlyinterpreted so the clinician and technician can fabricateaesthetic restorations.7 The dentin and enamel havedramatically different optical properties, and the relativecontribution of each should be considered during shadedetermination and fabrication of an aesthetic restoration.
To describe tooth color and aesthetics appropriately, abroad definition has been given to color that is based uponanatomy, optical properties, and polychromaticity.8 Thisdefinition is based upon the relative contribution of dentinand enamel to the color of the natural dentition. The primaryoptical properties are defined as hue, chroma, and value.The dentin imparts all of the colors of a tooth (ie,determines hue and chroma),2 while the enamel acts as afiber-optic structure that conducts light to capture theunderlying color of the dentin (ie, is a determinant of
value).9 The secondary optical properties includetranslucency, opacity, opalescence, iridescence, surfacegloss, and fluorescence. These secondary propertiescontribute significantly to the total aesthetics of the tooth,and may be better explained in terms of tooth anatomy.
The degree of translucency or opacity is determined bythe physical nature and the thickness of enamel and dentin,as well as the amount of light that penetrates the tooth or restoration. Although both dentin and enamel aretranslucent in the natural dentition, the enamel layer isvirtually transparent and colorless.
Opalescence is primarily observed in enamel, and inteeth it has a light-scattering effect that is associated withthe diameter of the enamel rods.
Iridescence produces a rainbow effect within the objectbeing viewed. While colors change based upon alterationsin the viewing direction, location, and illumination of anobject, the manner in which these parameters changedepends upon the wavelengths of dispersion, interference,and diffraction of light.
Surface gloss affects the appearance and vitality ofteeth and aesthetic dental materials. The surfacemorphology of natural teeth influences the surface gloss.While macro- or micromorphologically roughened or coarsesurfaces lead to diffuse reflection, flat or smooth surfacesallow specular (mirror-like) reflection. This optical scatteringof light has an effect on color perception and translucencyof the tooth.
Fluorescence occurs when ultraviolet (UV) light rays areabsorbed and blue or white visible light is emitted. Due to theorganic composition of dentin, UV light rays penetrate theenamel and excite the dentin photosensitivity (ie, sensitivity tothe action of radiant energy, or the color response to light). Theemitted light enhances the brilliance and vitality of teeth. Bothdentin and enamel fluoresce, and the combination of thesestructures can enhance the whiteness or value of teeth.
With this more comprehensive interpretation of colorderived from an understanding of the interrelation of opticalproperties and tooth morphology, clinicians and manufacturerscan work toward development of restorative systems (ie,composite, porcelain) that are capable of reproducing naturaltooth color within a restoration.
Continuing Education
2
A Simplified Aesthetic Concept: Historical Review and Current Clinical Application

COMPOSITE AND COLOR
Since no single monochromatic composite resin canduplicate the color evident in the natural dentition, it isnecessary to select various colors for the artificial enameland the artificial dentin layers. Accordingly, to reconstruct thenatural polychromatic effect, the layers cannot be stratified inequal dimensions as is present in plexiglass, which isuniformly distributed in layers. Rather, an aestheticrestoration requires the irregular, undulated placement ofvariations of composite resin colors. This allows light passingthrough the natural tooth and the restoration to reflect,refract, absorb, and transmit according to the opticaldensities of the hydroxyapatite crystals, enamel rods,dentinal tubules, and restorative material. Ideally, this createsa restored tooth with a multicolored, natural appearance.
Because composite does not have hydroxyapatitecrystals, enamel rods, and dentinal tubules, the compositerestoration requires the clinician to develop an illusion ofthe way light is reflected, refracted, transmitted, andabsorbed by dentin and enamel microstructures.6
Recreating a natural anatomical surface requires asimilar orientation of enamel and dentin. Newerformulations of composite resins possess optical propertiesthat render the tooth polychromatic (Figure 1).
A variety of dentin shades and translucencies areavailable, and enamel shades that are highly translucent,fluorescent, and opalescent have been developed. Utilizingthese composites, it is now possible for the clinician tofabricate a durable, long-lasting restoration that isaesthetically indistinguishable from natural tooth structure.Exacting shade matching and localized characterization isentirely possible. However, with some composite systemsthe attainment of ultimate aesthetics is time consuming.Most composite systems have standard composite resinshade guides that are manufactured from unfilledmethacrylates and do not accurately represent the trueshade, translucency, or opacity of the final polymerizedrestorative material.10 Furthermore, the range of shades inthese standard shade guides is not consistent with naturaltooth color. In addition, many of the composite resins aresynchronized to the Vita Lumin Shade Guide, which wasdesigned for porcelain systems and not composite resinsystems. Further, many of these composite resin systems
do not correspond to the true Vita shades. Thesediscrepancies are one reason for inconsistent color matchingthat requires a trial-and-error method through the fabricationof multiple custom shade tabs from the actual restorativematerial. Also, the use of color modifiers and opaquing resinscan be required to modify and adjust composite color toattain all of the possible natural tooth colors.
A recently developed composite resin system (Amaris[VOCO]) may provide a solution to this problem. Thissystem provides a simplified method of combining dentincolor and enamel value in a way that mimics natural toothstructure and color. This concept was designed withconsideration of both enamel and dentin shading instead ofusing a single monochromatic composite resin color. Theidea that most of the color (ie, yellow, orange, and red)originates from the dentin is the key here, resulting ingrouping Vita shades of similar hue and chroma torealistically replicate the optical properties of the naturaltooth. The composite system has 6 base opaque dentinshades arranged according to increasing chroma. Threeenamel translucent shades provide value (ie, brightness tothe restoration) and the aforementioned secondary opticalproperties (ie, translucency, fluorescence, iridescence, andopalescence; Figure 2).
Continuing Education
3
A Simplified Aesthetic Concept: Historical Review and Current Clinical Application
Figure 1. Developingnatural tooth anatomywith composite resinrequires a similarorientation of artificialenamel and dentin.Newer formulations ofcomposite resinspossess many of thesecondary opticalproperties that rendera tooth polychromatic.
Figure 2. An identical03 opaque dentinshaded compositesubstrate (03 above)is overlayed with 3
different translucent enamel shaded composites: translucentdark (TD), translucent neutral (TN), and translucent light (TL).

In addition, 2 special shades are provided: a hightranslucent and an opaque, shaded flowable composite.The high translucent shaded composite can be used forincisal edges, enamel or incisal defects, and to achieve ahigh-gloss surface reflectivity, while the opaque shadedcomposite can be used for masking discolorations (ie,amalgam staining, or altered color transition that occurswhen endodontic access openings are made in ceramicrestorations). This concept provides 18 possible tooth colorcombinations synchronized to the Vita shade guide.Furthermore, this system’s shade guides are manufacturedfrom the actual composite resin material, and accuratelyrepresent the true shade, translucency, or opacity of thefinal polymerized restorative material. Therefore, the shadematching system provides optimal replication of dentalcomposite color. This synchronization allows the clinician tocompare the actual polymerized restorative material to thenatural tooth color for a more accurate aesthetic colormatching. This concept not only simplifies the replication ofthe optical properties of the natural tooth, but also providesconsistent and predictable results.
The following clinical examples describe the process bywhich anterior and posterior composite resin restorationscan be efficiently developed using the Amaris system.
DEVELOPING AESTHETIC RESTORATIONS USING ASIMPLIFIED PLACEMENT TECHNIQUE
Aesthetic restoration of the prepared tooth has beenthe subject of considerable discussion. A myriad oftechniques have been developed to avoid the limitation ofdepth of cure, reduce the effects of polymerizationshrinkage, improve marginal adaptation and seal,11-15
enhance aesthetics,16,17 and enhance clinical outcomes ofsuch procedures.18 The incremental stratificationtechniques include horizontal, vertical oblique, centripetal,3-sited light-cure, and centripetal build-up. These variousmethods are recommended according to the type anddimension of the cavity preparation.19 It is commonlybelieved that segmentally filling the preparation generatesthe least pull on the buccal and lingual cusps. Not allliterature agrees with that concept. Douglas and colleagues
demonstrated that bulk fill produced the least strain on theopposing cusps.20 Although stratification techniques allowthe clinician to develop aesthetic restorations, the use ofintricate multilayering with numerous shades of compositemay not be efficient, realistic, or practical for the moderndental practice. In an effort to simplify and improveefficiency and provide optimal aesthetics, Amaris, a newnanocomposite formulation, was designed and integratedwith the duo-shade modified placement technique forposterior and anterior composite restorations.
For posterior restorations (Figures 3 to 8), thetechnique involves use of one continuous increment (ie,tubular shaped) that is placed and adapted in an obliquelayer against the cavity wall. A truncated cone-shapedcomposite instrument (PKT-3A [Brasseler USA]) should beused. The increment is cured through the cusp, and thepulpal floor becomes part of the cavity wall. This approachreduces the ratio of cavity volume to area of cavity wall,which results in a substantial reduction
in the marginal contraction gap.21 A second elongatedincrement is adapted in the same oblique manner againstthe opposing cavity wall, and is then light-cured through thecusp. For small- to medium-sized occlusal and proximalcavity preparations, the internal dentin core requires 2incremental placements. A final enamel layer is filled to theocclusal margins.
At this point a round-tipped instrument such as thePKT-3A is used to remove any residual composite material.Procedurally, the composite condenser is pressed againstthe occlusal surface. Using finger pressure, the instrumenttraces the entire margin of the preparation. This techniquenot only eliminates all residual composite extended beyondthe preparation, but also fills any region that may have been
Continuing Education
4
A Simplified Aesthetic Concept: Historical Review and Current Clinical Application
Figure 3. Preoperativeocclusal view ofdefective amalgamrestorations withrecurrent caries on themaxillary first andsecond premolars.
under filled. Upon completion, the same burnishinginstrument can be used to develop the central fissure,buccal and lingual developmental grooves, and in-clineplanes. After light-curing, the rubber dam is removed andarticulating paper is employed to identify any prematurecontacts.
This same duo shade placement technique can be utilizedin direct anterior composite restorations (Figures 9 to 14).However, polymerization shrinkage stress generated duringfabrication of anterior composite restorations is less than for
posterior restorations, since the ratio of bonded to unbondedsurfaces is generally less for anterior restorations. Therefore,utilization of stratification techniques to minimize the effects ofshrinkage stress is a less important consideration.
A long-bladed interproximal carver is preferred forresin placement and adaptation, and a sable brush isused to smooth the surface. A curved instrument (TINL-R[Brasseler USA]) can be used to shape the lingualsurfaces of anterior restorations. For class III and IVcomposite resin restorations an opacious dentin
Continuing Education
5
A Simplified Aesthetic Concept: Historical Review and Current Clinical Application
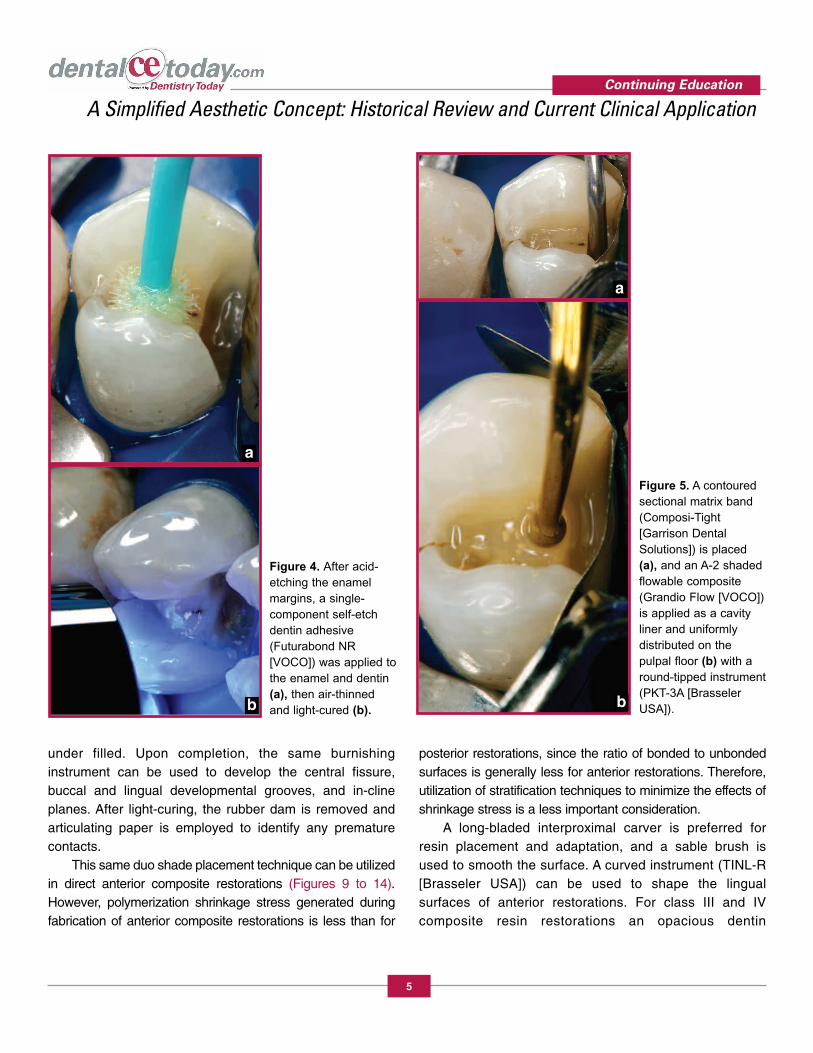
Figure 5. A contouredsectional matrix band(Composi-Tight[Garrison DentalSolutions]) is placed(a), and an A-2 shadedflowable composite(Grandio Flow [VOCO])is applied as a cavityliner and uniformlydistributed on thepulpal floor (b) with around-tipped instrument(PKT-3A [BrasselerUSA]).b
a
Figure 4. After acid-etching the enamelmargins, a single-component self-etchdentin adhesive(Futurabond NR[VOCO]) was applied tothe enamel and dentin(a), then air-thinnedand light-cured (b).
a
b
increment is placed as the internal core, and a secondenamel layer encapsulates this core. For class Vrestorations, this same placement procedure can beutilized with a translucent or opacious dentin core,depending upon the color of the dentin substrate. Fordeeper cervical restorations, placement of the dentin corein 2 sequential increments and utilizing a lower intensitylight power during the first 20 seconds of polymerizationmay result in an interval in which stress can be partly relieved by flow and elastic strain.22 The correlation
between the rate of conversion and the rate of shrinkagestress development requires a slower stiffnessdevelopment, which may result in overall stress reductionby allowing more yielding of the free surface of therestoration to the underlying contracting bulk.23 Theocclusal dentin segment (with a higher bond strength toenamel) is placed first, followed by the gingival segment.This approach reduces the potential for microgapformation at the gingival margin.
Creation of an aesthetic restoration depends on the
Continuing Education
6
A Simplified Aesthetic Concept: Historical Review and Current Clinical Application
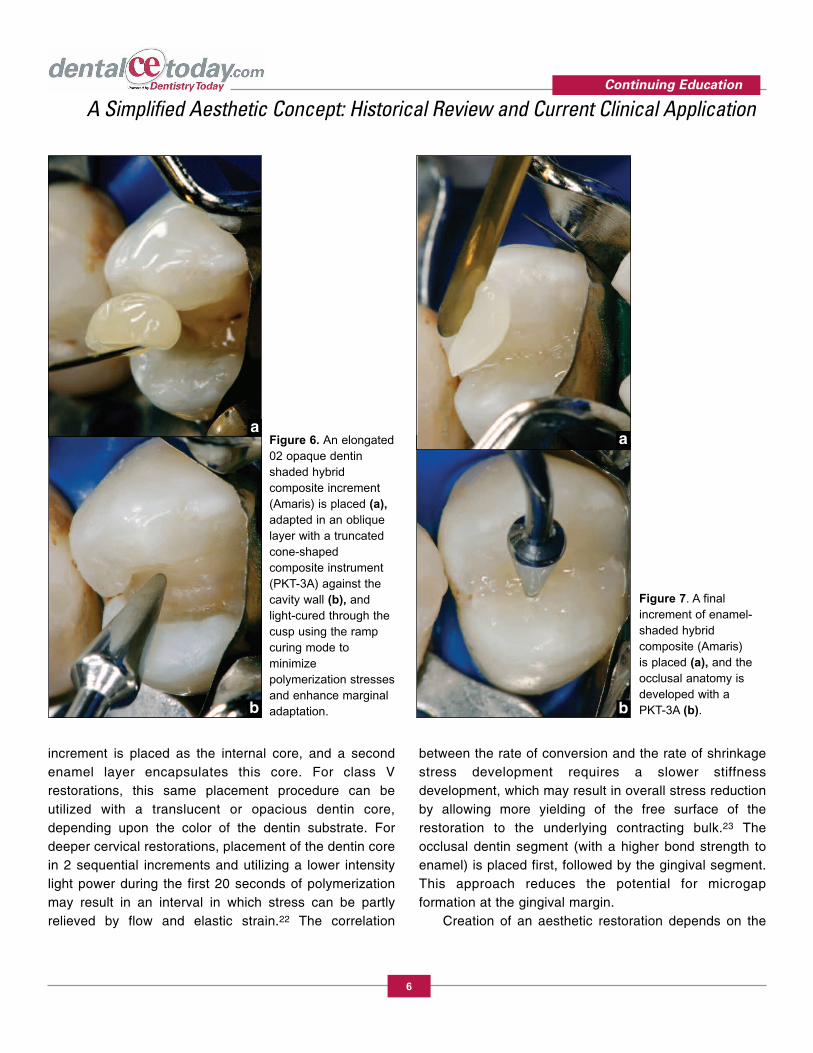
Figure 7. A finalincrement of enamel-shaded hybridcomposite (Amaris) is placed (a), and theocclusal anatomy isdeveloped with a PKT-3A (b).
Figure 6. An elongated02 opaque dentinshaded hybridcomposite increment(Amaris) is placed (a),adapted in an obliquelayer with a truncatedcone-shapedcomposite instrument(PKT-3A) against thecavity wall (b), andlight-cured through thecusp using the rampcuring mode tominimizepolymerization stressesand enhance marginaladaptation.
a
b
a
b

Continuing Education
7
A Simplified Aesthetic Concept: Historical Review and Current Clinical Application
Figure 12. Anincrement of 03 shadedhybrid composite(Amaris) is applied asan opaque dentin coreand light-cured for 40seconds from the facialusing the ramp curingmode to minimizepolymerization stressesand enhance marginaladaptation.
Figure 13. A final darktranslucent shadedenamel layer (DT) isapplied (a), sculptedand smoothed with asable brush (b), andpost-cured for 60seconds.
Figure 8. Thecompleted compositeresin restorations using the duo shadetechnique reflect theharmonious integrationof anatomical form and color.
Figure 9. Preoperativelingual view of adefective compositerestoration withdiscoloration andrecurrent caries on amandibular lateralincisor.
Figure 10. Therestorative shade isdetermined by colorphotographiccomparison to thenatural tooth structure.
Figure 11. After theenamel cavosurface isacid-etched, a single-component self-etchadhesive (FuturabondNR) is applied, air-thinned, and light-cured.
b
a

clinician’s understanding and interpretation of color and itsrelationship to the morphology of the tooth. The anatomy ofthe tooth should guide the clinician in developing the correctform and color. For optimal color matching of proximalcomposite restorations, consideration should be given to thesurrounding environment. Composite resin, enamel, anddentin cause considerable light scattering, which producesinternal diffusion of light and allows the composite restorationto blend with the tooth. This “chameleon effect” occurs asdiffused light enters from the surrounding tooth, and whenemitted from the restoration will alter its color by absorbingcolor from the tooth. This color alteration depends on thescattering and absorption coefficients, which can produce anappropriate color match.24 The composite resin systemdiscussed offers clinicians a more accurate and realisticrepresentation of natural tooth color combinations. The duoshade technique creates high-diffusion layers that allowoptimal light transmission within the restoration, providing amore realistic depth of color, as well as a natural appearingtooth surface.
CONCLUSION
Composite resin technology continues to improve thepractice of dentistry. Technological advances allow the clinicianto attain more predictable and aesthetic results. Clinical trialswill be required to determine the long-term results ofrestorations created with this new resin formulation. Theclinical examples provided in this article demonstrate the abilityof this nanoparticle hybrid formulation to simulate the opticalproperties of the natural dentition.
Continuing Education
8
A Simplified Aesthetic Concept: Historical Review and Current Clinical Application
Figure 14. Thepostoperative resultachieved with thissimplified 2-layernanocomposite systemreveals the naturalintegration ofcomposite resin withtooth structure.
Continuing Education
9
A Simplified Aesthetic Concept: Historical Review and Current Clinical Application
REFERENCES
1. Kovarik RE, Ergle JW. Fracture toughness of posteriorcomposite resins fabricated by incremental layering. J Prosthet Dent. 1993; 69:557-560.
2. Rinn LA. Applied theory of color. In: The PolychromaticLayering Technique: A Practical Manual for Ceramics &Acrylic Resins. Chicago, IL: Quintessence Publishing;1990:21-30.
3. Larson TD. Techniques for achieving realistic colordistribution in large composite resin restorations. J Am Dent Assoc. 1986;112:669-672.
4. Dietschi D. Free-hand composite resin restorations: a key to anterior aesthetics. Pract Periodontics Aesthet Dent.1995;7:15-25.
5. Donly KJ, Browning R. Class IV preparation design formicrofilled and macrofilled composite resin. Pediatr Dent.1992;14:34-36.
6. Winter R. Visualizing the natural dentition. J Esthet Dent. 1993;5:102-117.
7. Exner HV. Predictability of color matching and thepossibilities for enhancement of ceramic laminate veneers. J Prosthet Dent. 1991;65: 619-622.
8. Terry DA, Geller W, Tric O, et al. Anatomical form definescolor: function, form, and aesthetics. Pract Proced AesthetDent. 2002;14:59-67.
9. Fahl N Jr, Denehy GE, Jackson RD. Protocol for predictablerestoration of anterior teeth with composite resins. Pract Periodontics Aesthet Dent. 1995;7:13-21.
10. Baratieri LN. Esthetic Principles [in Portuguese]. Sao Paulo,Brazil: Quintessence Publishing; 1998:48.
11. Dietschi D, De Siebenthal G, Neveu-Rosenstand L, et al.Influence of the restorative technique and new adhesives onthe dentin marginal seal and adaptation of resin compositeClass II restorations: an in vitro evaluation. Quin-tessenceInt. 1995;26:717-727.
12. Lutz F, Kull M. The development of posterior toothcomposite system, in-vitro investigation. SSO SchweizMonatsschr Zahnheilkd. 1980; 90:455-483.
13. Eick JD, Welch FH. Polymerization shrinkage of posteriorcomposite resins and its possible influence on postoperativesensitivity. Quintessence Int. 1986;17:103-111.
14. Koenigsberg S, Fuks A, Grajower R. The effect of threefilling techniques on marginal leakage around Class IIcomposite resin restorations in vitro. Quintessence Int.1989;20:117-121.
15. Tjan AH, Bergh BH, Lidner C. Effect of various incrementaltechniques on the marginal adaptation of class II compositeresin restorations. J Prosthet Dent. 1992;67:62-66.
16. Tjan AH, Glancy JF. Effects of four lubricants used duringincremental insertion of two types of visible light-activatedcomposites. J Prosthet Dent. 1988;60:189-194.
17. Kovarik RE, Ergle JW. Fracture toughness of posteriorcomposite resins fabricated by incremental layering. J Prosthet Dent. 1993;69:557-560.
18. Davidson CL, Feilzer AJ. Polymerization shrinkage andpolymerization shrinkage stress in polymer-basedrestoratives. J Dent. 1997;25:435-440.
19. Terry DA. Adhesive preparation designs. In: Terry DA.Natural Aesthetics With Composite Resin. Mahwah, NJ:Montage Media; 2004:21-37.
20. Versluis A, Douglas WH, Cross M, et al. Does anincremental filling technique reduce polymerizationshrinkage stresses? J Dent Res. 1996; 75:871-878.
21. Hansen EK. Effect of cavity depth and application techniqueon marginal adaptation of resins in dental cavities. J Dent Res. 1986;65:1319-1321.
22. Dennison JB, Yaman P, Seir R, et al. Effect of variable lightintensity on composite shrinkage. J Prosthet Dent.2000;84:499-505.
23. Feilzer AJ, Dooren LH, de Gee AJ, et al. Influence of lightintensity on polymerization shrinkage and integrity ofrestoration-cavity interface. Eur J Oral Sci. 1995;103:322-326.
24. Hall NR, Kafalias MC. Composite colour matching: thedevelopment and evaluation of a restorative colour matchingsystem. Aust Prosthodont J. 1991;5:47-52.

POST EXAMINATION INFORMATION
To receive continuing education credit for participation inthis educational activity you must complete the programpost examination and receive a score of 70% or better.
Traditional Completion Option:
You may fax or mail your answers with payment to Dentistry Today(see Traditional Completion Information on following page). Allinformation requested must be provided in order to process theprogram for credit. Be sure to complete your “Payment”, “PersonalCertification Information”, “Answers” and “Evaluation” forms, Yourexam will be graded within 72 hours of receipt.. Upon successfulcompletion of the post-exam (70% or higher), a “letter ofcompletion” will be mailed to the address provided.
Online Completion Option:
Use this page to review the questions and mark your answers.Return to dentalCEtoday.com and signin. If you have notpreviously purchased the program select it from the “OnlineCourses” listing and complete the online purchase process. Oncepurchased the program will be added to your User History pagewhere a Take Exam link will be provided directly across from theprogram title. Select the Take Exam link, complete all the programquestions and Submit your answers. An immediate grade reportwill be provided. Upon receiving a passing grade complete theonline evaluation form. Upon submitting the form your Letter OfCompletion will be provided immediately for printing.
General Program Information:
Online users may login to dentalCEtoday.com anytime in thefuture to access previously purchased programs and view or print“letters of completion” and results.
POST EXAMINATION QUESTIONS
1. A variation in shades and opacities of color thatcreates the illusion of depth is called the____.
a. translucent effect
b. polychromatic effect
c. opaque effect
d. hybrid effect
2. Traditionally, hybrid composite resin was used for its ____.
a. polishability
b. durability of polish
c. strength and fracture resistance
d. both a and b
3. The combination of aesthetics and mechanicalstability in a single composite resin material ispossible due to the development of ____.
a. hybrid composites
b. microfill composites
c. small-particle composites
d. large-particle composites
4. A primary optical property is ___.
a. hue
b. chroma
c. value
d. all of the above
5. A secondary optical property is ___.
a. chroma
b. surface gloss
c. iridescence
d. both b and c
6. Both dentin and enamel are translucent in naturalteeth. The enamel layer is opaque and imparts allof the colors of a tooth.
a. The first sentence is true and the second sentence is false.
b. The first sentence is false and the second sentence is true.
c. Both sentences are true.
d. Both sentences are false.
7. Which property produces a rainbow effect withinthe object being viewed?
a. surface gloss
b. fluorescence
c. opalescence
d. iridescence
8. Both enamel and dentin fluoresce. Thecombination of these structures can enhance thewhiteness or value of teeth.
a. The first sentence is true and the second sentence is false.
b. The first sentence is false and the second sentence is true.
c. Both sentences are true.
d. Both sentences are false.
Continuing Education
10
A Simplified Aesthetic Concept: Historical Review and Current Clinical Application

PROGRAM COMPLETION INFORMATION
If you wish to purchase and complete this activitytraditionally (mail or fax) rather than Online, you mustprovide the information requested below. Please be sure toselect your answers carefully and complete the evaluationinformation. To receive credit you must answer at least sixof the eight questions correctly.
Complete online at: www.dentalcetoday.com
TRADITIONAL COMPLETION INFORMATION:Mail or Fax this completed form with payment to:
Dentistry TodayDepartment of Continuing Education100 Passaic AvenueFairfield, NJ 07004
Fax: 973-882-3662
PAYMENT & CREDIT INFORMATION:
Examination Fee: $20.00 Credit Hours: 1.0
Note: There is a $10 surcharge to process a check drawn on any bank other than a US bank. Should you have additionalquestions, please contact us at (973) 882-4700.
o I have enclosed a check or money order.
o I am using a credit card.
My Credit Card information is provided below.
o American Express o Visa o MC o Discover
Please provide the following (please print clearly):
Exact Name on Credit Card
Credit Card # Expiration Date
Signature
PROGRAM EVAUATION FORM
Please complete the following activity evaluation questions.
Rating Scale: Excellent = 5 and Poor = 0
Course objectives were achieved.
Content was useful and benefited your clinical practice.
Review questions were clear and relevant to the editorial.
Illustrations and photographs were clear and relevant.
Written presentation was informative and concise.
How much time did you spend reading the activity & completing the test?
Continuing Education
A Simplified Aesthetic Concept: Historical Review and Current Clinical Application
ANSWER FORM: COURSE #: 105.1
Please check the correct box for each question below.
1. o a o b o c o d 5. o a o b o c o d
2. o a o b o c o d 6. o a o b o c o d
3. o a o b o c o d 7. o a o b o c o d
4. o a o b o c o d 8. o a o b o c o d
PERSONAL CERTIFICATION INFORMATION:
Last Name (PLEASE PRINT CLEARLY OR TYPE)
First Name
Profession / Credentials License Number
Street Address
Suite or Apartment Number
City State Zip Code
Daytime Telephone Number With Area Code
Fax Number With Area Code
E-mail Address
/
Dentistry Today is an ADA CERPRecognized Provider.
Approved PACE Program ProviderFAGD/MAGD Credit Approvaldoes not imply acceptanceby a state or provincial board ofdentistry or AGD endorsement.June 1, 2006 to May 31, 2009AGD Pace approval number: 309062