Embed Size (px)
Citation preview

CLINICAL RESEARCH STUDIES
A single-center experience in open andendovascular treatment of hemodynamicallyunstable and stable patients with rupturedabdominal aortic aneurysmsGioacchino Coppi, MD, Roberto Silingardi, MD, Stefano Gennai, MD, Giuseppe Saitta, MD, andAnna Vittoria Ciardullo, MD, Modena, Italy
Objective: To retrospectively compare a single center’s immediate and mid-term outcomes of ruptured abdominal aorticaneurysm open and endovascular repair (EVAR) for two patient groups—hemodynamically stable and unstablepatients—in the same time period.Methods: Patients presenting at our center with confirmed rupture of an abdominal aortic aneurysm between December1999 and April 2006 were considered according to an intention-to-treat model with EVAR. Patients with symptomaticor acute (but not ruptured) AAAs were not included in this study. Thirty-three patients underwent EVAR, and 91underwent open repair. Seventy-two patients (EVAR, 45%; open, 63%) were classified as hemodynamically unstable atarrival, and 52 were classified as stable (EVAR, 55%; open, 37%). Ninety-seven percent of EVAR procedures commencedunder local anesthesia, and 100% of open repairs occurred with general anesthesia. Overall successful graft deployment,30-day mortality, overall reintervention rate, and complications were the study primary end points.Results: Overall successful graft deployment for EVAR was 91%; for open repair, it was 96%. Overall 30-day mortality forEVAR was 30% (unstable, 53%; stable, 11%), and the rate was 46% for open repair (unstable, 61%; stable, 21%). TheEVAR postoperative reintervention rate (within 30 days) was 15% (unstable, 20%; stable, 11%), and for open repair it was10% (unstable, 9%; stable, 15%). We recorded a 27% severe complication rate for EVAR patients (unstable, 40%; stable,17%), and for patients treated with open repair, it was 33% (unstable, 35%; stable, 29%). Our overall EVAR eligibility ratewas 52%, and our overall EVAR treatment rate was 27%.Conclusions: Our study’s overall results for EVAR remain encouraging when compared with those of conventional repair,
but large randomized trials are required to confirm the efficacy of the procedure. (J Vasc Surg 2006;44:1140-7.)The overall mortality rate for patients undergoing con-ventional repair of ruptured abdominal aortic aneurysms(rAAA) is up to 50%.1-5 Despite a documented gradualdecrease in this mortality rate in a 50-year meta-analysis,1 itis generally accepted that there has been no consistentimprovement in the number of operative deaths associatedwith rAAA in the last few decades.6 Conventional repair hasinherent limitations, including general anesthesia and lap-arotomy.3,7-11 The advantages of endovascular repair(EVAR) include the avoidance of both general anesthesiaand laparotomy, thus improving the physiological stress ofthe procedure for the patient.12-22 EVAR itself also carrieswith it an inherent limitation: a delay of treatment due to
From the Department of Vascular Surgery, Policlinico Hospital of Modenaand University of Studies of Modena and Reggio Emilia.
Competition of interest: none.Reprint requests: Gioacchino Coppi, MD, Department of Surgery, Opera-
tive Unit of Vascular Surgery, Policlinico of Modena, via del Pozzo, 71,41100 Modena, Italy (email: [email protected]).
0741-5214/$32.00Copyright © 2006 by The Society for Vascular Surgery.
doi:10.1016/j.jvs.2006.08.0701140
necessary preoperative imaging. However, recent studiesassessing the delay from patient arrival to death in nonsur-gical groups conclude that it is safe to assess the majority ofrAAA for EVAR.23,24
Improvements in mortality and morbidity associatedwith EVAR with respect to conventional repair have beenshown in some recent studies. However, these studies ofteninclude symptomatic, nonruptured aneurysms togetherwith truly ruptured aneurysms, and most include a mix ofstable and unstable patients.13,17,18,20,25-30 We present ourstudy as a comparison of the efficacy of EVAR comparedwith open repair for stable and unstable patients treated forrAAA in our center in the same study period.
METHODS
A total of 124 consecutive patients presented at ourhospital during the study period (December 1999 to April2006) with rAAA. Patients with acute or symptomatic butintact aneurysms shown at computed tomography (CT)were excluded. The exclusion criteria guidelines in our
center for EVAR are based on anatomic parameters: prox-
JOURNAL OF VASCULAR SURGERYVolume 44, Number 6 Coppi et al 1141
imal neck length less than 10 mm, proximal neck diametergreater than 32 mm, and external iliac artery diameter lessthan 7 mm and severe bilateral iliac artery disease. Thirty-three of the 124 patients were treated with EVAR. Thirty-one of the 91 surgically treated patients would have beenanatomically suitable for EVAR but were treated with openrepair at the beginning of our experience: 6 patients due toyoung age (initially considered a criteria of exclusion) and25 patients due to unavailability of adequately trained staffand endovascular supplies. Our overall EVAR eligibilityrate was 52% (64/124), and our overall EVAR treatmentrate was 27% (33/124). The outcomes measured includedimmediate technical success (successful deployment of thegraft with complete sealing of the aneurysm), conversion,immediate mortality (within 24 hours) and 30-day mortal-ity, complications, reinterventions, mortality during pa-tient follow-up, and intensive care unit (ICU) and hospitalstay.
We compared different rates in study outcomes be-tween the groups by means of logistic regression analysis.The level of significance was P � .05. Stata for Windows(release 7.0) (StataCorp LP; College Station, Tex) statisti-cal software package was used.
The patient demographic data are displayed in Table I.These patients were categorized into two subgroups forcomparative analysis according to their presentation at thehospital as being hemodynamically unstable (defined asunconscious and/or with a systolic blood pressure �80mm Hg after fluid resuscitation) or hemodynamically stable(conscious and/or with a systolic blood pressure �80 mmHg, with or without fluid resuscitation). Nineteen (58%) ofthe EVAR patients were preoperatively classified as unfit forsurgical treatment because of advanced age and comorbidi-ties.
All patients were assisted by a vascular surgeon and ananesthesiologist from their presentation at the emergencydepartment through to the operating room. Permissivehypotension was practiced with prudent fluid resuscitationto keep systolic blood pressure around 80 mm Hg, to avoida recommencement of or increase in bleeding. Eighty-fourpercent (EVAR, 88%; open, 83%) of patients were assessedby contrast-enhanced spiral CT 5-mm slices of the abdo-men. Rupture with CT was defined as extravasation ofblood surrounding the aneurysm, as evident by the scan. In4 EVAR cases (12%) rupture was confirmed by intraopera-tive angiography and intravascular ultrasonography (IVUS)and in 16 open cases (18%) rupture was confirmed in theoperating room. During the CT scanning, the operatingroom was prepared to further reduce delay.
The patients’ anatomic suitability for emergency EVARwas also determined at CT. Five EVAR and 12 open caseswere transferred from other hospitals with previously per-formed CT scans (delivered via a Dicon (Dicon; Kyonggi-do, Korea) intranet system for evaluation during patienttransportation). The maximum time taken to execute theCT was between 5 and 7 minutes (total time delay of 15-20minutes). The diameter and length of the aneurysms were
evaluated directly by the vascular surgeon from the screen.Open repair was performed in the traditional fashion, asdescribed in literature,31-33 with supraceliac clamping in100% of the unstable patients and in 73% of the stablepatients. All grafts used in the study were commerciallyavailable, supplied by Bard Inc (Murray Hill, New Jersey)and Boston Scientific (Watertown, Mass).
Four of the 15 EVAR hemodynamically unstable pa-tients followed a different course. These patients presentedunconscious with severe hypotension (40-50 mm Hg) andwere transferred directly to the operating room withoutCT. Intraoperative angiography and IVUS allowed confir-mation of the rupture and evaluation of EVAR suitability.In these four patients, a prototype occlusion balloon, in-serted from the contralateral femoral artery, was success-fully used. This device, developed in collaboration withEdwards Lifesciences (Irvine, Calif), is similar to a cali-brated catheter of 14F with a double channel (for ballooninflation and execution of intraoperative angiography).Once the balloon was inflated in the suprarenal aorta, animmediate increase in blood pressure was observed in allfour patients. The endograft was then successfully posi-tioned, and the occlusion balloon was deflated and with-drawn.
All EVAR procedures were performed in a dedicated
Table I. Summary of patient demographics,comorbidities, and preoperative aneurysm anatomicfeatures
Variable EVAR Open
Median age, y (range) 81 (65-99) 77 (53-92)Sex (M/F) 28/5 74/17Unstable 15 57Stable 18 34ASA class
III 49% 52%IV 19% 28%V 32% 20%
ComorbiditiesDiabetes 18% 11%Smoker 24% 54%Hypertension 87% 73%Hyperlipidemia 33% 35%Cardiac disease 69% 55%Carotid disease 3% 5%Renal disease 6% 15%Respiratory disease 69% 30%Previous laparotomy 25% 8%Obesity 40% 30%
Patient unfit for AAA open repair 19 (64%) —Patient unfit for general
anesthesia13 (43%) —
AAA maximum diameter (mm),median (range)
70 (43-100) 75 (60-100)
Neck diameter (mm),median (range)
23 (20-30) 27 (24-30)
Neck length (mm),median (range)
26 (14-40) 13 (0-28)
EVAR, Endovascular aneurysm repair; ASA, American Society of Anesthe-siologists; AAA, abdominal aortic aneurysm repair.
vascular operating room equipped with mobile C-arm

t.
JOURNAL OF VASCULAR SURGERYDecember 20061142 Coppi et al
(OEC 9800; GE Medical System, Salt Lake City, Utah),IVUS (Volcano s5; Volcano Corporation; Rancho Cor-dova, Calif), and ecoduplex scanner (Esaote AU 5; SocrateMedical Srl, Cesano Boscone, Milan, Italy). Our EVARteam includes two vascular surgeons (at least one endovas-cular expert), an anesthesiologist, an endovascular-trainedoperating room nurse, and a radiologic technician.
Ninety-seven percent of the EVAR procedures com-menced under local anesthesia (1% lidocaine) accompaniedwhen required with intravenous sedation for pain relief andpatient immobility. Arterial access was obtained throughsurgical exposure of both femoral arteries, except in onecase (Powerlink bifurcated endograft; Endologix Inc, Ir-vine, Calif), for which it was obtained through the exposureof the right artery and percutaneous access through the leftfemoral artery. Intraoperative angiography was performedmanually through a 7F or 8F 45-cm introducer sheath(Cordis; Cordis Corp; Hialeah, Fla) inserted from thefemoral artery contralateral to the side chosen for thedeployment of the endograft. A 9F 55-cm introducersheath (Cordis; Cordis Corp; Hialeah, Fla) was used whenIVUS was performed. With angiography, the exact posi-tions of the renal arteries and the aortic bifurcation weredetermined and marked directly by the vascular surgeon onthe C-arm screen.
After the insertion of a super-stiff guidewire (Am-
Table II. Operative details
Variable
ProductZenithTalentPowerlinkExcluderEndologixHemashield GoldBardTotal
Imaging AssessmentCT
StableUnstable
Intraoperative IVUS/angiography (without preoperative CT)StableUnstable
Procedural time, min, median (range)Duration skin to skinAUIBifurcatedTube
AnesthesiaLocalLocal to generalEpiduralGeneral
Volume of contrast agent, mL, median (range)
EVAR, Endovascular aneurysm repair; Bif, bifurcated endograft; AUI, aorintravascular ultrasonography.*Four patients died during the intervention, before deployment of the graf
platz or Backup Meyer; Boston Scientific), the endograft
was deployed. The aortouni-iliac device (AUI) coupledwith a femorofemoral bypass was the preferred techniquein rAAA (73%). Completion angiography confirmed ad-equate proximal and distal fixation and identified anyendoleak. In the case of an AUI procedure, a contralat-eral plug was inserted, and the procedure was completedwith a crossover femorofemoral bypass with a polytetra-fluoroethylene graft. Most patients undergoing this pro-cedure were converted to general anesthesia, but in sevenpatients the entire procedure was completed with localanesthesia. When required, postdilation was executedwith a compliant balloon (Reliant; Medtronic, WorldMedical Manufacturing Corp, Sunrise, Fla).
All of the endografts used in the study were commer-cially available: Talent (Medtronic Vascular, Santa Rosa,Calif), Excluder (W. L. Gore and Associates, Flagstaff,Ariz), Zenith (Cook, Bloomington, Ind), and Powerlink.The endografts were chosen according to the aneurysms’anatomic characteristics.
From the end of 2003, Cook has supplied our centerwith a specialized emergency kit of AUI Zenith endograftswith proximal diameters of 24, 28, and 32 mm; a distaldiameter of 12 mm; and a fixed 122-mm length. Whennecessary, the AUI graft can be lengthened with commer-cially available distal extensions.
The EVAR follow-up scheme consisted of routine CT
EVAR Open
13 (1 Bif, 12 AUI) —12 (1 Bif, 11 AUI) —
3 (1 Bif, 1 AUI, 1 Tube) —4 (4 Bif) —1 (1 Tube) —
— 77 (63 Tube, 14 Bif)10 (9 Tube, 1 Bif)
33 87*
18 (100%) 34 (100%)11 (73%) 41 (72%)
0 04 (27%) 0
133 (60-510) 178 (60-600)139 (60-510) —111 (60-180) 247 (100-600)
60 171 (60-360)
11 (45%) 019 (52%) 01 (3%) 0
0 91 (100%)201 (20-600) —
iliac endograft; Tube, Tube endograft; CT, computed tomography; IVUS,
touni-before discharge, at 3 and 12 months, and annually there-

JOURNAL OF VASCULAR SURGERYVolume 44, Number 6 Coppi et al 1143
after. Ecoduplex scanning was performed at 1 and 6months and annually thereafter. Plain radiographs wereperformed before discharge, at 6 months, and annuallythereafter. Open follow-up consisted of an ecoduplex scanat 1 month and the second and fifth years.
RESULTS
Operative data are displayed in Table II. The proce-dural details illustrate less invasiveness by the EVAR proce-dure, with a reduced overall procedure duration and in-creased use of local anesthesia. The EVAR study results arepresented in Table III. The four perioperative deaths werecaused by intractable hypovolemic shock. Within the first24 hours, three further deaths occurred: two from multipleorgan failure and one from bowel infarction. A furtherpatient died 12 days after the procedure from multipleorgan failure. Both immediate and 30-day mortality werestatistically significant between the two groups (P � .01).
Three patients were immediately converted to opensurgery. One conversion was due to the technical inabilityto successfully insert the AUI Talent endograft in a tortu-ous anatomy. A second conversion was performed becausethe device could not be attached to the short neck (AUITalent). Furthermore, a proximal cuff could not be insertedto correct this error because of the bending of the endograftin the aneurysmal sac, thus impeding its passage. An aorto-bifemoral bypass was performed in both cases. Both ofthese patients died during surgery as a result of intractablehypovolemic shock. The final immediate conversion wasalso performed because an AUI Talent endograft could notbe attached to the short, proximal neck; this resulted in a
Table III. Results of endovascular treatment
Variable Overal
No. patients in study 33Immediate conversion 9% (3/33)Successful graft deployment 91% (30/33)Immediate mortality (within 24 h) 27% (9/33)30-d mortality 30% (10/33)Conversion at a distance 3% (1/30)Overall reintervention rate 23% (7 in 6 pPostoperative reintervention (within 30 d) 15% (5/33)Secondary intervention 6% (2/33)Severe systemic complications 27% (9/33)
MOF (fatal) 3Bowel infarction (fatal) 1ACS 1*Acute renal failure (dialysis) 1*Stroke 1Severe respiratory insufficiency 1†
Gastrointestinal bleeding 1†
ICU stayNo. patients 14Average, h (range) 64
Hospital stay, d, median (range) 13 (1-30)
NS, Not statistically significant; MOF, multiple organ failure; ACS, abdomi*Same patient.†Same patient.
proximal endoleak that remained despite an attempted
correction. A surgical aortoaortic interposition was thenperformed successfully.
Of the 26 patients who survived successful endovascu-lar treatment, 14 (54%) were transferred to the ICU. Therewere five (17%) incidents of postoperative systemic compli-cations in three patients which were not associated withfatal outcomes. One patient developed abdominal com-partment syndrome and underwent drainage of the hema-toma by an extraperitoneal approach through a left iliacfossa cutdown. This situation was complicated further withacute renal failure necessitating dialysis, although the com-pletion angiography showed patency of both renal arteries.One patient had a stroke, and another patient experiencedrespiratory insufficiency accompanied by gastrointestinalbleeding and was treated with medication only.
We experienced five (17%) postoperative reinterven-tions. One patient developed a complete thrombosis of theAUI Talent endograft which was treated with an extra-anatomic axillobifemoral bypass. One patient developed athrombosis of the crossover and a type III endoleak be-tween the two segments of the AUI Talent endograft. Thispatient was treated with an additional segment of en-dograft, and the crossover was redone. A third patientdeveloped a type I proximal endoleak (AUI Zenith), whichwas considered unsuitable for correction by the addition ofa proximal cuff because of the shortness of the aneurysmalneck. Therefore, through a small abdominal incision, aDacron band (DuPont, Wilmington, Del) was successfullyplaced around the proximal neck to reduce the diameterand obtain complete sealing. Another patient developed atype I distal endoleak (AUI Zenith) because of an incom-
Unstable Stable P value
15 182 1 NS
87% (13/15) 94% (17/18) NS46% (7/15) 11% (2/18) �.0153% (8/15) 11% (2/18) �.01
1 —s) 20% (3/15) 17% (3/18) NS
20% (3/15) 11% (2/18) NS11% (2/18) —
40% (6/15) 17% (3/18) NS3 —
1 —1* —1* —1 —
1† —1† —
7 6 NS107 (10-280) 25 (4-48) �.0115 (7-24) 9 (1-30) �.01
mpartment syndrome; ICU, intensive care unit.
l
atient
nal co
plete sealing by the plug. A larger plug was inserted to
nal co
, mulfor op
JOURNAL OF VASCULAR SURGERYDecember 20061144 Coppi et al
correct the endoleak. The final patient had a type I proximalendoleak (AUI Talent), which was treated with a 25-mmballoon dilation of the proximal neck attachment, with areduction, but not the complete exclusion, of the aneu-rysm. Given the modest entity of the endoleak, the hemo-dynamic stability, and the stability of the dimension of thehematoma at the postoperative CT, the patient was main-tained under observation.
Two secondary interventions were necessary during thefollow-up period. At 1 year, a new type I distal endoleak wassuccessfully treated with a distal extension. At 6 months,the patient who had previously been unsuccessfully treatedwith a balloon dilation in the postoperative period wasconverted after a further unsuccessful attempt at endovas-cular correction with a proximal cuff extension. Our overallincidence of endoleak was 17% (5/30), and 4 of the 5occurrences were primary endoleaks.
At a mean follow-up of 27.5 months (range, 30-1456days), we have recorded five patient deaths. Two patients
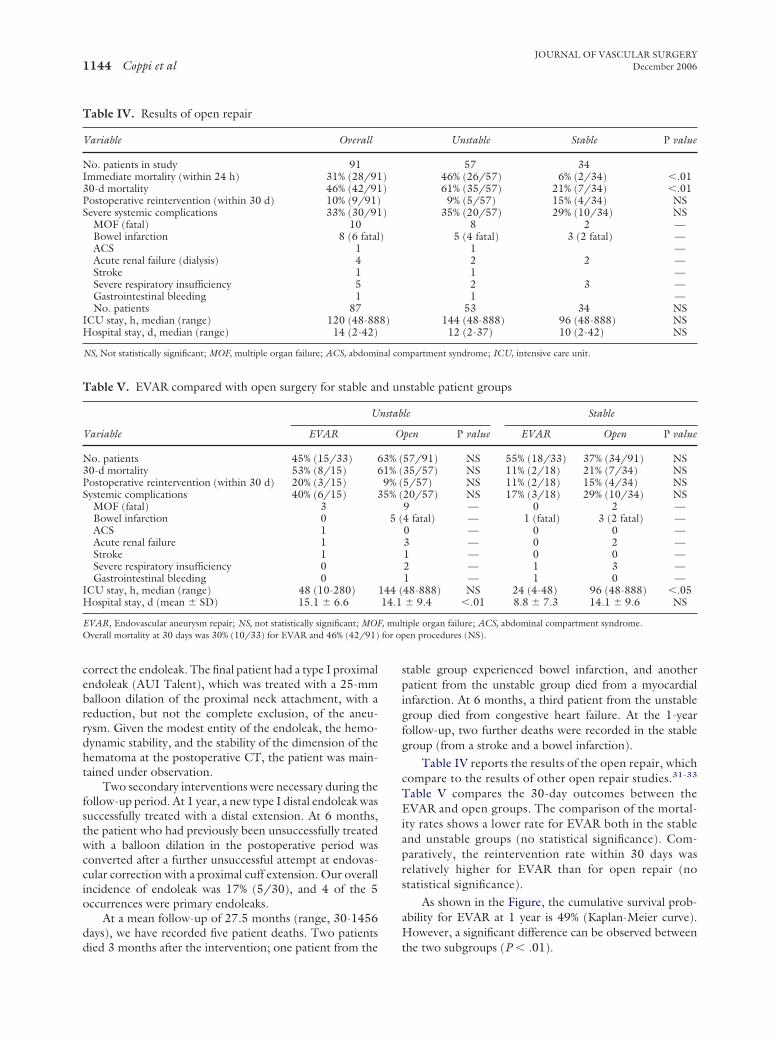
Table IV. Results of open repair
Variable Overall
No. patients in study 91Immediate mortality (within 24 h) 31% (28/9130-d mortality 46% (42/91Postoperative reintervention (within 30 d) 10% (9/91)Severe systemic complications 33% (30/91
MOF (fatal) 10Bowel infarction 8 (6 fatalACS 1Acute renal failure (dialysis) 4Stroke 1Severe respiratory insufficiency 5Gastrointestinal bleeding 1No. patients 87
ICU stay, h, median (range) 120 (48-88Hospital stay, d, median (range) 14 (2-42)
NS, Not statistically significant; MOF, multiple organ failure; ACS, abdomi
Table V. EVAR compared with open surgery for stable an
Variable
U
EVAR
No. patients 45% (15/33) 630-d mortality 53% (8/15) 6Postoperative reintervention (within 30 d) 20% (3/15)Systemic complications 40% (6/15) 3
MOF (fatal) 3Bowel infarction 0ACS 1Acute renal failure 1Stroke 1Severe respiratory insufficiency 0Gastrointestinal bleeding 0
ICU stay, h, median (range) 48 (10-280)Hospital stay, d (mean � SD) 15.1 � 6.6
EVAR, Endovascular aneurysm repair; NS, not statistically significant; MOFOverall mortality at 30 days was 30% (10/33) for EVAR and 46% (42/91)
died 3 months after the intervention; one patient from the
stable group experienced bowel infarction, and anotherpatient from the unstable group died from a myocardialinfarction. At 6 months, a third patient from the unstablegroup died from congestive heart failure. At the 1-yearfollow-up, two further deaths were recorded in the stablegroup (from a stroke and a bowel infarction).
Table IV reports the results of the open repair, whichcompare to the results of other open repair studies.31-33
Table V compares the 30-day outcomes between theEVAR and open groups. The comparison of the mortal-ity rates shows a lower rate for EVAR both in the stableand unstable groups (no statistical significance). Com-paratively, the reintervention rate within 30 days wasrelatively higher for EVAR than for open repair (nostatistical significance).
As shown in the Figure, the cumulative survival prob-ability for EVAR at 1 year is 49% (Kaplan-Meier curve).However, a significant difference can be observed between
Unstable Stable P value
57 3446% (26/57) 6% (2/34) �.0161% (35/57) 21% (7/34) �.01
9% (5/57) 15% (4/34) NS35% (20/57) 29% (10/34) NS
8 2 —5 (4 fatal) 3 (2 fatal) —
1 —2 2 —1 —2 3 —1 —
53 34 NS144 (48-888) 96 (48-888) NS12 (2-37) 10 (2-42) NS
mpartment syndrome; ICU, intensive care unit.
stable patient groups
le Stable
pen P value EVAR Open P value
57/91) NS 55% (18/33) 37% (34/91) NS35/57) NS 11% (2/18) 21% (7/34) NS5/57) NS 11% (2/18) 15% (4/34) NS20/57) NS 17% (3/18) 29% (10/34) NS9 — 0 2 —4 fatal) — 1 (fatal) 3 (2 fatal) —0 — 0 0 —3 — 0 2 —1 — 0 0 —2 — 1 3 —1 — 1 0 —48-888) NS 24 (4-48) 96 (48-888) �.05� 9.4 �.01 8.8 � 7.3 14.1 � 9.6 NS
tiple organ failure; ACS, abdominal compartment syndrome.en procedures (NS).
))
)
)
8)
d un
nstab
O
3% (1% (9% (5% (
5 (
144 (14.1
the two subgroups (P � .01).

JOURNAL OF VASCULAR SURGERYVolume 44, Number 6 Coppi et al 1145
DISCUSSION
Both open repair and EVAR for rAAA in the literaturehave results that are difficult to interpret because oftenpatients with symptomatic but not ruptured aneurysms areincluded, and the hemodynamic situations are not consid-ered in relation to the outcome (Table VI). In our study, weincluded only patients with evidenced rupture. They weredivided into two groups based on their hemodynamiccondition in the period from arrival to intervention. Thisclassification of the two patient groups was developed todiscern whether there was a difference in terms of outcome.The definition of patients’ hemodynamic stability was dif-ficult. The main criterion we chose, as is common in otherstudies, was the blood pressure at observation. We used acutoff of 80 mm Hg. It is clear that the arterial pressurecannot alone be sufficient to give a true indication of thegravity of the individual patient’s condition, which oftenalso depends on the amount of bleeding and the patient’sgeneral condition before rupture of the aneurysm. Thevarying definitions render a comparison of the variousstudies difficult. Thus, a development of a consensus be-tween experts is required to establish which patients willbenefit from EVAR in comparison to open repair andwhether, in some situations, abstention is indeed betterthan surgical or endovascular treatment.34
A crucial point to consider when treating with EVAR isthe time delay linked to the necessary CT scan, particularlyin hemodynamically unstable patients. In our center, the
Fig. Cumulative survival after endovascular repair of rcurve).
time delay for a CT scan has been reduced to approximately
15 to 20 minutes, in line with other specialized cen-ters.16,29,35 In reality, the survival of patients arriving alivein the hospital with rAAA is longer than one usually be-lieves. Lloyd et al23 reported a survival longer than 2 hoursin 87.5% of untreated rAAA patients and a median timefrom the beginning of symptoms to death of more than 16hours. Furthermore, Walker et al36 reported a mean timeinterval between admission and death of 8 hours. In ourexperience, four EVAR patients who presented in a state ofshock (with blood pressure �50 mm Hg) underwent asimple ecoduplex scan and were then transported immedi-ately to the operating room without CT. However, exceptfor extreme and selected cases, the CT scan remains ourfirst-choice imaging assessment for rAAA because it offers asure diagnosis of rupture, showing the periaortic hema-toma; it supplies vital information about the arterial ac-cesses and the aneurysmatic morphology and, hence, per-mits rapid evaluation of endovascular feasibility.
In these same four EVAR patients, we used a proto-type occlusion balloon, which proved extremely useful.In general, the aortic occlusion balloon represents atheoretical advantage because it mimics surgical clamp-ing and immediately slows the hemorrhage. However,dedicated occlusion balloons are not available on themarket, and the use of nondedicated balloons is prob-lematic, primarily because of balloon instability and di-ameter, the flexibility of the catheters, and problemslinked to executing angiography appropriately.37 For all
ed abdominal aortic aneurysms (Kaplan-Meier survival
upturof these issues, we believe that, today, the rapid deploy-

werecified.
JOURNAL OF VASCULAR SURGERYDecember 20061146 Coppi et al
ment of the endograft is preferable,4,14,27 with the ex-ception of gravely unstable patients.37
In EVAR treatment, we developed a preference for theAUI endograft (used in 73% of cases) given its simple andrapid deployment and greater anatomic adaptability. Ourpreference is not supported on the whole by other studies,which collectively have a mean use of AUI of 46.2% (TableVI).
EVAR has a higher reintervention rate than open repair(Table V). This could be attributed to the great dimensionsand difficult anatomies of these patients selected for EVAR,especially in terms of tortuosity and shortness of the aneu-rysmatic neck, and the necessary rapidity of the procedure.
The principal studies of EVAR for rAAA (Table VI)report a mean mortality rate of 21% (varying from 9.5% to45%), which is significantly lower than the historical mor-tality rates associated with surgery.31-33 However, there arevery few published experiences of EVAR for rAAA, andthese also have limited patient numbers (few studies have�25 patients). Furthermore, the mean percentage of pa-tients treated who are hemodynamically unstable and,therefore, at higher risk is infrequently specified, but ourliterature review shows it to be 32%.4,14-16,18,19,21,25-30
Although the combined mortality rates of 30% forEVAR and 46% for the surgically treated group (Table V)are not statistically significant, these results encourage us tocontinue our intention to treat with EVAR at our institu-tion. However, our limited experience is not evidence thatEVAR should be considered the first-choice treatment forrAAA. Whether EVAR should be considered a preferable
Table VI. Series of emergency endovascular repair of rAA
Study (location) Period No. P
Ohki, Veith, and associates(Montefiore)25,26
1994-1999 20
Hinchliffe (Nottingham)14 1994-2000 20 Scharrer-Pamler (Ulm)18 1995-2001 24 Resch (Malmo)19 1997-2002 21 van Heerzeele (Ghent)21 1997-2002 9 Hechelhammer (Zurich)27† 1997-2003 37 Lachat (Zurich) 16† 1998-2001 21 Gerassimidis (Thessaloniki)4 1998-2004 23 Yilmaz (Eindhoven)15‡ 1999-2001 24 (17Alsac (Créteil)28 2001-2004 17 Larzon (Sweden) 29 2001-2004 15 Peppelenbosch (Belgium/Netherlands)30 2001-2004 35 Lee (Florida) 31§ 2002-2004 13 Total/average 279
rAAA, Ruptured abdominal aortic aneurysm; AUI, aortouni-iliac endografcombination of different, unspecified grafts.*Thirty-day mortality is given where possible.†Same partial patient cohort; the Hechelhammer series was a more recent a‡The Eindhoven study also contained symptomatic and acute patients with§Unspecified percentage of hemodynamically unstable patients; no patients�The Florida study was not included, in which unstable patients were unspe
option for stable or unstable patients remains unknown.
Our experience shows a greater advantage for EVAR instable patients in terms of mortality, morbidity, and ICUstay, and this is quite surprising given that it would havebeen logical to hypothesize that the patients in the mostcritical condition (unstable) would be those who wouldbenefit most from a less invasive approach.
An explanation of the similar mortality for EVAR andopen treatment in the unstable group could be that thegrave condition of the patient at presentation is the deter-mining factor for survival, rather than the type of interven-tion chosen. The relatively higher mortality rate for thestable open group when compared with the stable EVARgroup could be explained by the fact that the high invasive-ness of the surgical treatment could precipitate the patientsfrom a stable condition to an unstable one, thereby wors-ening their chances of survival.
The improvements of the diagnostic/therapeuticcourse and of the availability of materials seem to havepositively conditioned the results, but further improve-ments seem possible, such as dedicated kits that render theprocedure more rapid and simple. Certainly, randomizedtrials are mandatory to establish the real efficacy of EVARfor rAAA.
The authors thank Johanna Chester, who helped coor-dinate the data collection, analysis, and writing of thearticle.
AUTHOR CONTRIBUTIONS
Conception and design: GC, RS, SG
ts Endograft typeUnstablepatients Mortality*
AUI, 17 homemade; Tube, 3 5 (25%) 2 (10%)
AUI 4 (20%) 9 (45%)AUI, 1; Bif, 19; Tube, 4 4 (17%) 5 (21%)AUI, 12; Bif, 9 5 (24%) 4 (19%)AUI, 5; Bif, 3; Tube, 1 5 (56%) 2 (22%)Bif, 35; Tube, 2 8 (22%) 4 (10.9%)Bif, 20; Tube, 1 3 (14%) 2 (9.5%)AUI, 10; Bif, 14 9 (36%) 9 (39%)
red) AUI 12 (50%) 4 (24%)AUI, 8; Bif, 8; iliac ext, 1 0 4 (23%)Bif, 13; comb, 2 11 (73%) 2 (13%)AUI, 32; Bif, 3 20 (57%) 8 (23%)Bif Unspecified 3 (23%)AUI, 129 (46%); Bif, 137
(49%); Tube, 11 (4%);comb, 2 (1%)
86 (32%)� 58 (21%)
e, Tube endograft; Bif, bifurcated endograft; iliac ext, iliac extension; comb,
ger study.pture.excluded on the basis of hemodynamic instability.
As
atien
ruptu
t; Tub
nd larout ru
Analysis and interpretation: GC, RS, SG, AVC

JOURNAL OF VASCULAR SURGERYVolume 44, Number 6 Coppi et al 1147
Data collection: SG, GSWriting the article: GC, RS, SGCritical revision of the article: GC, RS, SG, GS, AVCFinal approval of the article: GC, RS, SGStatistical analysis: SG, AVCOverall responsibility: GC
See Invited Commentary, page 1361
REFERENCES
1. Bown MJ, Sutton AJ, Bell PR, Sayers RD. A meta-analysis of 50 years ofruptured abdominal aortic aneurysm repair. Br J Surg 2002;89:714-30.
2. Lee AW, Hirneise CM, Tayyarah M, Huber TS, Seeger JM. Impact ofendovascular repair on early outcomes of ruptured abdominal aorticaneurysms. J Vasc Surg 2004;40:211-5.
3. Hinchliffe RJ, Braithwaite BD, Hopkinson BR. The endovascular man-agement of ruptured abdominal aortic aneurysm. Eur J Vasc EndovascSurg 2003;25:191-201.
4. Gerassimidis TS, Papazoglou KO, Kamparoudis AG, Konstantinidis K,Karkos CD, Karamanos D, et al. Endovascular management of rupturedabdominal aortic aneurysms: 6-year experience from a Greek centre. JVasc Surg 2005;42:615-22.
5. Noel AA, Gloviczki P, Cherry KJ, Bower TC, Pannetton JM, Mozes GI,et al. Ruptured abdominal aortic aneurysms: the excessive mortality rateof conventional repair. J Vasc Surg 2001;34:41-6.
6. Heller JA, Weinberg A, Arons R. Two decades of abdominal aorticaneurysm repair: have we made any progress? J Vasc Surg 2000;32:1091-101.
7. Buth J, van Merrewijk CJ, Harris PL, Hop WCJ, Riambau V, LaheijRJF. Outcome of endovascular abdominal aortic repair in patients withconditions considered unfit for open procedure. A report on theEUROSTAR experience. J Vasc Surg 2002;35:211-21.
8. Boyle JR, Thompson MM. Endovascular abdominal aortic aneurysmrepair is less invasive, now we must prove its efficacy. J Endovasc Ther2003;10:16-9.
9. Boyle JR, Goodall S, Thompson MM, Bell P, Thompson M. Endovas-cular AAA repair attenuates the inflammatory and renal responsesassociated with conventional surgery. J Endovasc Ther 2000;7:369-71.
10. Verhoeven EL, Prins TR, van den Dungen JJ, Tielliu IFJ, Hulsebos RG,van Schilfgaarde R. Endovascular repair of acute AAAs under localanesthesia with bifurcated endografts: a feasibility study. J EndovascTher 2002;9:729-35.
11. Kapma M-R, Verhoeven ELG, Tielliu IFJ, Zeebregts CJAM, Prins TR,Ven der Heij B, et al. Endovascular treatment of acute abdominal aorticaneurysm with bifurcated stentgraft. Eur J Vasc Endovasc Surg 2005;29:510-5.
12. Ohki T, Veith F. Endovascular grafts and other image-guided catheter-based adjuncts to improve the treatment of ruptured aortoiliac aneu-rysms. Ann Surg 2002;232:466-79.
13. Veith F, Ohki T. Endovascular approaches to ruptured infrarenal aor-toiliac. J Cardiovasc Surg 2002;43:369-78.
14. Hinchliffe RJ, Yusuf SW, Maceriewicz JA, MacSweeney STR, WenhamPW, Hopkinson BR. Endovascular repair of ruptured abdominal aorticaneurysm—a challenge to open repair? Results from a single centreexperience in 20 patients. Eur J Vasc Endovasc Surg 2001;22:528-35.
15. Yilmaz N, Peppelenbosh N, Cuypers PW, Tielbeek AV, Duijm LEM,Buth J. Emergency treatment of symptomatic or ruptured abdominalaortic aneurysms: the role of endovascular repair. J Endovasc Ther2002;9:449-57.
16. Lachat ML, Pfammatter T, Witzke HJ. Endovascular repair with bifur-cated stent-graft under local anaesthesia to improve outcome of rup-tured aortoiliac aneurysms. Eur J Vasc Endovasc Surg 2002;23:528-36.
17. Orend KH, Kotsis T, Scharrer-Pamler R, Kapfer X, Liewald F, Gorich J,et al. Endovascular repair of aortic rupture due to trauma and aneurysm.
Eur J Vasc Endovasc Surg 2002;23:61-7.18. Scharrer-Pamler R, Kotsis T, Kapfer X, Gorich J, Sunder-Plassmann L.Endovascular stent-graft repair of ruptured aortic aneurysms. J Endo-vasc Ther 2003;10:447-52.
19. Resch T, Malina M, Lindblad B, Dias NV, Sonesson B, Ivancev K.Endovascular repair of ruptured abdominal aortic aneurysms. J Endo-vasc Ther 2003;10:440-6.
20. Lombardi JV, Fairman RM, Golden MJ, Carpenter JP, Mitchell M,Barker C, et al. The utility of commercially available endografts in thetreatment of contained ruptured abdominal aortic aneurysms withhemodynamic stability. J Vasc Surg 2004;40:154-60.
21. van Heerzeele I, Vermassen F, Durieux C, Randon C, De Roose J.Endovascular repair of aortic rupture. Eur J Vasc Endovasc Surg 2003;26:311-6.
22. van Sambeek M, van Dijk LC, Hendriks JM, van Grotel M, Kuiper JW,Pattynama PMT, et al. Endovascular versus conventional open repair ofacute abdominal aortic aneurysm. Feasibility and preliminary results. JEndovasc Ther 2002;9:443-8.
23. Lloyd GM, Bown MK, Norwood MG, Fishwick G, Bell PRF, SayersRD. Feasibility of preoperative computer tomography in patients withruptured abdominal aortic aneurysm: a time-to-death study in patientswithout operation. J Vasc Surg 2004;39:788-91.
24. Boyle JR, Gibbs PJ, Kruger J, Shearman CP, Raptis S, Phillips MJ.Existing delays following the presentation of ruptured abdominal aorticaneurysm allow sufficient time to assess patients for endovascular repair.Eur J Vasc Endovasc Surg 2005;29:505-9.
25. Ohki T, Veith FJ, Sanchez LA, Cyamon J, Lipsitz EC, Wain RA, et al.Endovascular graft repair of ruptured aortoiliac aneurysms. J Am CollSurg 1999;189:102-12
26. Hechelhammer L, Lachat ML, Wildermuth S, Bettex D, Mayer D,Pfammatter T. Midterm outcome of endovascular repair of rupturedabdominal aortic aneurysms. J Vasc Surg 2005;41:752-7.
27. Alsac J-M, Desgranges P, Kobeiter H, Becquemin J-P. Emergencyendovascular repair for ruptured abdominal aortic aneurysms: feasibilityand comparison of early results with conventional repair. Eur J VascEndovasc Surg 2005;30:632-9.
28. Larzon T, Lindgren R, Norgren L. Endovascular treatment of rupturedabdominal aortic aneurysms: a shift in paradigm? J Endovasc Ther2005;12:548-55.
29. Peppelenbosch N, Cuypers PWM, Vahl AC, Vermassen F, Buth J.Emergency endovascular treatment for ruptured abdominal aortic an-eurysm and the risk of spinal cord ischemia. J Vasc Surg 2005;42:608-14.
30. Lee AW, Huber TS, Hirneise CM, Berceli SA. Eligibility rates ofruptured and symptomatic AAA for endovascular repair. J EndovascTher 2002;9:436-42.
31. Rutledge R, Oller DW, Meyer AA, Johnson GJ Jr. A statewide, popu-lation-based time-series analysis of the outcome of ruptured abdominalaortic aneurysm. Ann Surg 1996;223:492-502.
32. Dueck AD, Kucey DS, Johnston KW, Alter D, Laupacis A. Survival afterruptured abdominal aortic aneurysm: effect of patient, surgeon, andhospital factors. Vasc Surg 2004;39:1253-60.
33. Harris JR, Forbes TL, Steiner SH, Lawlor DK, Derose G, Harris KA.Risk-adjusted analysis of early mortality after ruptured abdominal aorticaneurysm repair. J Vasc Surg 2005;42:387-91.
34. Boyle JR, Gibbs PJ, King D, Shearman CP, Raptis S, Phillips MJ. Predict-ing outcome in ruptured abdominal aortic aneurysm; a prospective study of100 consecutive cases. Eur J Vasc Endovasc Surg 2003;26:607-11.
35. Peppelenbosch N, Yilmaz N, van Marrewijk C, Buth J, Cuypers P,Duijm L, et al. Emergency treatment of acute symptomatic or rupturedabdominal aortic aneurysm. Outcome of a prospective intent-to-treatby EVAR protocol. Eur J Vasc Endovasc Surg 2003;26:303-10.
36. Walker EM, Hopkison BR, Makin GS. Unoperated abdominal aorticaneurysm: presentation and natural history. Ann R Coll Surg Engl1983;65:311-3.
37. Malina M, Veith F, Ivancev K, Sonesson B. Balloon occlusion of theaorta during endovascular repair of ruptured abdominal aortic aneu-rysm. J Endovasc Ther 2005;12:556-9.
Submitted Jun 14, 2006; accepted Aug 26, 2006.