Embed Size (px)
Citation preview
PRACTICAL THERAPEUTICS
A 'Stages of Change' Approach toHelping Patients Change BehaviorGRETCHEN L. ZIMMERMAN. PSY.D.. tlVNTHlA G. OLSEN. M.D.. and MICHAEL E BOSWORTH. D.O.
State l'nivcrsit\' School ofMedicine, Dayton, Ohio
Helping patients change behavior is an important role for family physicians. Change inter-ventions are especially useful in addressing lifestyle modification for disease prevention,long-term disease management and addictions. The concepts of "patient noncompliance"and motivation often focus on patient failure. Understanding patient readiness to makechange, appreciating barriers to change and helping patients anticipate relapse can improvepatient satisfaction and lower physician frustration during the change process. In this arti-cle, we review the Transtheoretical Model of Change, also known as the Stages of Changemodel, and discuss its application to the family practice setting. The Readiness to ChangeRuler and the Agenda-Setting Chart are two simple tools that can be used in the office topromote discussion. (Am Fam Physician 2000;61:1409-16.)
Members of variousmedical facultiesdevelop articles for"Practical Therapeu-tics. " This article is onein a series coordinatedby the Department ofFamily Medicine atWright State UniversitySchool of Medicine,Dayton, Ohio. Guesteditors of this seriesare Cynthia G. Olsen,M.D., and GordonS.Walbroehl, M.D.
One role of family physicians isto assist patients in under-standing their health and tohelp them make the changesnecessary for health improve-
ment. Exercise programs, stress managementtechniques and dietary restrictions representsome common interventions that requirepatient motivation. A change in patientlifestyle is necessary for successful manage-ment of long-term illness, and relapse canoften be attributed to lapses in healthy behav-ior hy the patient. Patients easily understandlifestyle modifications (i.e., "1 need to reducethe fat in my diet in order to control myweight.") but consistent, life-long behaviorchanges are difficult.
Much has been written about success andfailure rates in helping patients change, aboutbarriers to change and about the role ofphysicians in improving patient outcomes.Recommendations for physicians helpingpatients to change have ranged from the "justdo it" approach to suggesting extended officevisits, often incorporating behavior modifica-tion, record-keeping suggestions and follow-up telephone calls.' ' Repeatedly educatingthe patient is not always successful and canbecome frustrating for the physician andpatient. Furthermore, promising patients animproved outcome does not guarantee theirmotivation for long-term change. Patients
may view physicians who use a confronta-tional approach as being critical rather thansupportive. Relapse during any treatmentprogram is sometimes viewed as a failure bythe patient and the physician. A feeling of fail-ure, especially when repeated, may causepatients to give up and avoid contact withtheir physician or avoid treatment altogether.After physicians invest time and energy inpromoting change, patients who fail are oftenlabeled "noncompliant" or "unmotivated."Labeling a patient in this way places responsi-bility for failure on the patient's character andignores the complexity of the behaviorchange process.
Lessons Learned from Smokingand Alcohol Cessation
Research into smoking cessation and alco-hol abuse has advanced our understanding ofthe change process, giving us new directionsfor health promotion. Current views depictpatients as being in a process of change; whenphysicians choose a mode of intervention,"one size doesn't fit all."''-̂ Two importantdevelopments include the Stages of Changemodel' and motivational interviewing strate-gies.*" The developers of the Stages of Changemodel used factor and cluster analytic meth-ods in retrospective, prospective and cross-sec-tional studies of the ways people quit smoking.The model has been validated and applied to a
MARCH 1,2000 / VOLUME 61,NUMBFR 5 AMERICAN FAMILY PHYSICIAN 1409
Behavior change Is rarely a discrete, single event; the patientmoves gradually from being uninterested (precontemplationstage) to considering a change (contemplation stage) todeciding and preparing to make a change.
variety of behaviors that include smoking ces-sation, exercise behavior, contraceptive use anddietary behavior."'" Simple and effective"stage-based" approaches derived from theStages of Change modeP demonstrate wide-spread utility.""'" In addition, brief counselingsessions (lasting five to 15 minutes) have beenas effeaive as longer visits.'̂ "*
Understanding ChangePhysicians should remember that behavior
change is rarely a discrete, single event. Physi-cians sometimes see patients who, afterexperiencing a medical crisis and beingadvised to change the contributing behavior,readily comply. More often, physiciansencounter patients who seem unable orunwilling to change. During the past decade,behavior change has come to be understoodas a process of identifiable stages through
The Authors
GRETCHEN L. ZIMMERMAN. PSY.D.. is an assistant professor in the Department ofFamily Medicine at Wnght State University School of Medicine, Dayton, Ohio. She isalso a faculty member in the Dayton Community Family Practice Residency Program.She received a doctorate in psychology at Wright State University School of Profes-sional Psychology in Dayton.
CYNTHIA G. OLSEN, M.D., is a professor and executive vice-chair in the Departmentof Family Medicine, Wright State University School of Medicine, where she obtainedher medical degree. She completed a family practice residency at Good Samaritan Hos-pital in Dayton.
MICHAEL F BOSWORTH, DO., is an associate professor in the Department of FamilyMedicine, Wnght State University School of Medicine, and residency director of theDayton Community Family Practice Residency. A graduate of the College of Osteo-pathlc Medicine and Surgery, Des Moines, he completed a family practice residency atWright Patterson Air Force Base in Dayton.
Address correspondence to Gretchen L Zimmerman, PsyD. Dayton Community Fam-ily Practice Residency Program, 2345 Philadelphia Dr, Dayton, OH 45406- Reprints arenot available from the authors.
which patients pass. Physicians can enhancethose stages by taking specific action. Under-standing this process provides physicianswith additional tools to assist patients, whoare often as discouraged as their physicianswith their lack of change.
The Stages of Change model** shows that,for most persons, a change in behavior occursgradually, with the patient moving from beinguninterested, unaware or unwilling to make achange (precontemplation), to considering achange (contemplation), to deciding andpreparing to make a change. Genuine, deter-mined action is then taken and, over time,attempts to maintain the new behavior occur.Relapses are almost inevitable and becomepart of the process of working toward life-long change.
PRECONTEMPLATION STAGE
During the precontemplation stage, pa-tients do not even consider changing. Smokerswho are "in denial" may not see that the adviceapplies to them personally. Patients with highcholesterol levels may feel "immune" to thehealth problems that strike others. Obesepatients may have tried unsuccessfully somany times to lose weight that they have sim-ply given up.
CONTEMPLATION STAGE
During the contemplation stage, patientsare ambivalent about changing. Giving up anenjoyed behavior causes them to feel a senseof loss despite the perceived gain. During thisstage, patients assess barriers (e.g., time,expense, hassle, fear, "I know I need to, doc,but...") as well as tbe benefits of change.
PREPARATION STAGE
During the preparation stage, patients pre-pare to make a specific change. They mayexperiment with small changes as their deter-mination to change increases. For example,sampling low-fat foods may be an experimen-tation with or a move toward greater dietarymodification. Switching to a different brand
1410 AMiiRiCAN FAMILY PHYSICIAN VOLUME 61, NUMBER 5 / MARCH 1,2000
Changing Behavior
of cigarettes or decreasing their drinking sig-nals that they have decided a change is needed.
A a i O N STAGE
The action stage is the one that most physi-cians are eager to see their patients reach. Manyfailed New Year's resolutions provide evidencethat if the prior stages have been glossed over,action itself is often not enough. Any actiontaken by patients should be praised because itdemonstrates the desire for lifestyle change.
MAINTENANCE AND RELAPSE PREVENTION
Maintenance and relapse preventioninvolve incorporating the new behavior "overthe long haul." Discouragement over occa-sional "slips" may halt the change process andresult in the patient giving up. However, mostpatients find themselves "recycling" throughthe stages of change several times before thechange becomes truly established.
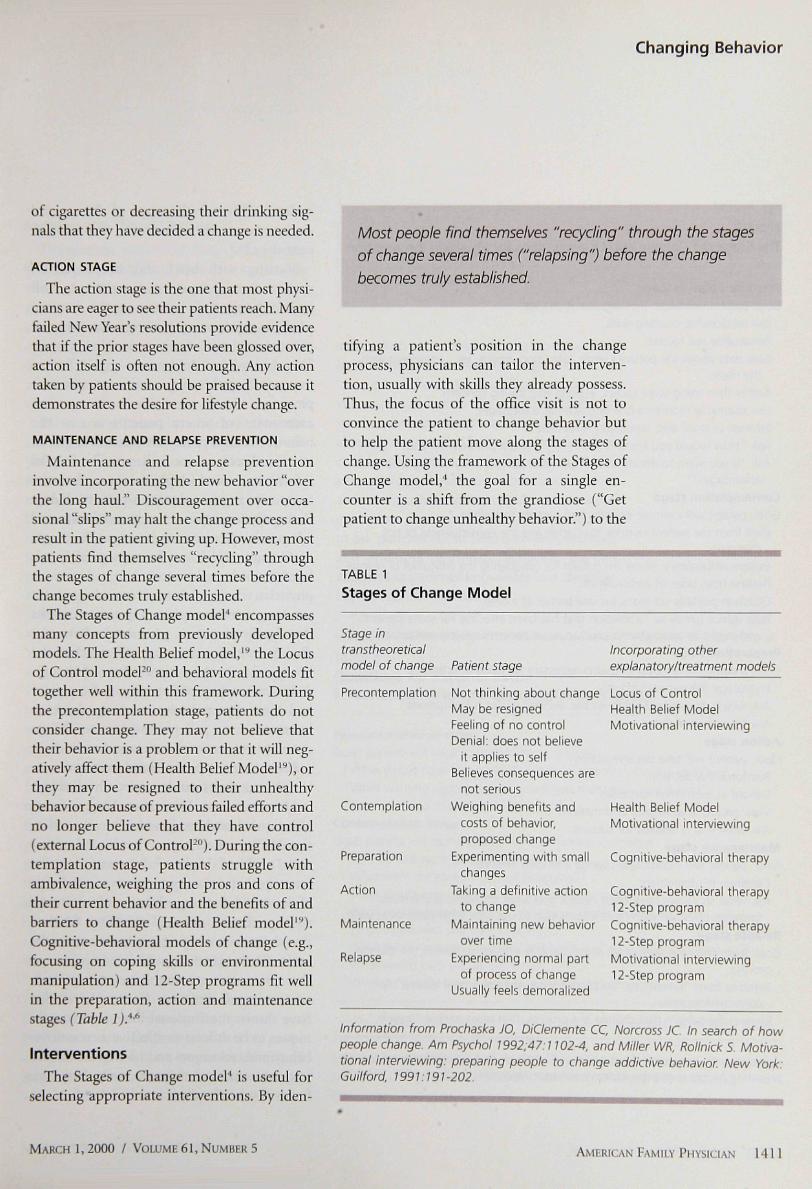
The Stages of Change model' encompassesmany concepts from previously developedmodels. The Health Belief model,'** the Locusof Control modeP*̂ ' and behavioral models fittogether well within this framework. Duringthe precontemplation stage, patients do notconsider change. They may not believe thattheir behavior is a problem or that it will neg-atively affect them (Health Belief Model'"*), orthey may be resigned to their unhealthybehavior because of previous failed efforts andno longer believe that they have control(external Locus of Control-* )̂. During the con-templation stage, patients struggle withambivalence, weighing the pros and cons oftheir current behavior and the benefits of andbarriers to change (Health Belief model'* )̂.Cognitive-behavioral models of change (e.g.,focusing on coping skills or environmentalmanipulation) and 12-Step programs fit wellin the preparation, action and maintenancestages (Table /).•*•*
InterventionsThe Stages of Change model' is useful for
selecting appropriate interventions. By iden-
Most people find themselves "recycling" through the stages
of change several times ("relapsing") before the change
becomes truly established.
tif/ing a patient's position in the changeprocess, physicians can tailor the interven-tion, usually with skills they already possess.Thus, the focus of the office visit is not toconvince the patient to change behavior butto help the patient move along the stages ofchange. Using the framework of the Stages ofChange model,"' the goal for a single en-counter is a shift from the grandiose ("Getpatient to change unhealthy behavior.") to the
TABLE 1
Stages of Change Model
Stage intranstheoreticalmodel of change Patient stage
Incorporating otherexplanatory/treatment models
Precontemplation
Contemplation
Preparation
Action
Maintenance
Relapse
Not thinking about changeMay be resignedFeeling of no controlDenial: does not believe
it applies to selfBelieves consequences are
not seriousWeighing benefits and
costs of behavior,proposed change
Experimenting with smallchanges
Taking a definitive actionto change
Maintaining new behaviorover time
Experiencing normal partof process of change
Usually feels demoralized
Locus of ControlHealth Belief ModelMotivational interviewing
Health Belief ModelMotivational interviewing
Cognitive-behavioral therapy
Cognitive-behavioral therapy12-Step programCognitive-behavioral therapy12-Step programMotivational interviewing12-Step program
Information from Prochaska JO. DiClemente CC, Norcross JC In search of howpeople change. Am Psychol 1992,47:1102-4, and Miller WR, Rotlnick S. Motiva-tional interviewing: preparing people to change addictive behavior New York-Guilford, 199 V.I 91-202.
MARCH 1,2000 / VOLUME 61, NUMBER 5 AMERICAN FAMILY PHYSICIAN 141
TABLE 2
The Stages of Change and Opportunities for Physician Intervention
Precontemplation stage
Goal, patient will begin thinking about change.
Use relationship-building skills.
Personalize risk factors.
Give data about the patient's vitals, laboratory results, etc., compared withthe norm.
Rather than using scare tactics, express your caring concern.
Use teachable moments (the symptom as a message).
Educate in small bits, repeatedly, over time.
Ask "How would you know if your was a problem for you?"
Ask "If you were to decide to change, what do you imagine might be some
advantages'^"
Contemplation stageGoal: patient will examine benefits and barners to change.
Elicit from the patient reasons to change and the consequences of notchanging.
Explore ambivalence; praise the patient for considering the difficulties of change.
Restate both sides of ambivalence-
Question possible solutions for one barrier at a time.
Pose advice gently as "a solution that has been effective for some patients
and might be adaptable to you" to avoid patient's natural resistance.
Preparation stageGoal: patient will discover elements necessary for decisive action.
Encourage the patient's efforts.
Ask which strategies the patient has decided on for risk situations.
Ask for a change date.
Action stageGoal: patient will take decisive action.
Reinforce the decision.
Delight in even small successes.
View problems as helpful information.
Ask what else is needed for success.
Maintenance stageGoal: patient will incorporate change into daily lifestyle.
Continue reinforcement.
Ask what strategies have been helpful and what situations problematic(provides physician with more information to use with other patients as well).
Relapse stageGoal: learn from the temporary success and re-engage patient in the change
process.Reframe from "failure" to "successful for a while plus new lessons" for
continued success.Remind the patient that change is a process, that most people "recycle."
Adapted with permission from Miller WR, Rollnick S. Motivational interviewing:preparing people to change addictive behavior New York: Guilford, 1991:191-202.
realistic ("Identify the stage of change andengage patient in a process to move to thenext stage.").''
Starting with brief and simple advicemakes sense because some patients willindeed change their behavior at the directiveol their physician. (This step also preventsprecontemplators from rationalizing that,"My doctor never told me to quit."). Ratherthan viewing this step as the intervention,physicians should view this as the openingassessment of where patients are in thebehavior change process. A patient's responseto this direct advice will provide helpfulinformation on which physicians can base thenext step in the physician-patient dialog.Rather than continue merely to educate andadmonish, interventions based on the Stagesof Change model"* can be appropriately tai-lored to each patient to enhance success. Aphysician who provides concrete advice aboutsmoking cessation when a patient remarksthat family members who smoke have notdied from lung cancer, has not matched theintervention to the patient's stage of change.A few minutes spent listening to the patientand then appropriately matching physicianintervention to patient readiness to changecan improve communication and outcome.
Patients at the precontemplation and con-templation stages can be especially challeng-ing for physicians. Motivational interviewingtechniques have been found to be most effec-tive. Miller and colleagues-' replicated studieswith "problem drinkers," demonstrating thatan empathetic therapist style was predictiveof decreased drinking while a confrontationalstyle predicted increased drinking. Motiva-tional interviewing incorporates empathyand reflective listening with key questions sothat physicians are simultaneously patient-centered and directive. Controlled studieshave shown motivational interviewing tech-niques to be at least as effective as cognitive-behavioral techniques and 12-step facilitationinterventions, and they are easily adaptablefor use by famiiy physicians."""
1412 AMERICAN FAMILY PHYSICIAN VOLUME 61, NUMBER 5 / MARCH 1,2000
Changing Behavior
an •rTniTTfiTTVr'rm-T
Helping the 'Stuck' PatientThe goal for patients at the precontempla-
tion stage is to begin to think about changinga behavior. The task for physicians is to empa-thetically engage patients in contemplatingchange (Table 2)." During this stage, patientsappear argumentative, hopeless or in "denial,"and the natural tendency is for physicians totry to "convince" them, which usually engen-ders resistance.
Patient resistance is evidence that thephysician has moved too far ahead of thepatient in the change process, and a shift backto empathy and thought-provoking questionsis required. Physicians can engage patients inthe contemplation process by developing andmaintaining a positive relationship, personal-izing risk factors and posing questions thatprovoke thoughts about patient risk factorsand the perceived "bottom line."
The wording of questions and the patient'sstyle of "not thinking about changing" arealso important. As precontemplators respondto questions, rather than jumping in and pro-viding advice or appearing judgmental, thetask for physicians is to reflect with empathy,instill hope and gently point out discrepan-cies between goals and statements. Askingargumentative patients, "Do you want to diefrom this?" may be perceived as a threat andcan elicit more resistance and hostility. Onthe other hand, asking patients, "How willyou know that its time to quit?" allowspatients to be their "own expert" and can helpthem begin a thought process that extendsbeyond the examination room. Well-phrasedquestions will leave patients pondering theanswers that are right for them and will movethem along the process of change (Table 3)."
It is not unusual for some patients to spendyears in the contemplation stage, whichphysicians can easily recognize by their "yes,but" statements. Empathy, validation, praiseand encouragement are necessary during allstages but especially when patients strugglewith ambivalence and doubt their ability to
Patients in the precontemplative stage appear to be argumen-
tative, hopeless or in "denial," and the natural tendency is to
try to "convince" them, which usually engenders resistance.
accomplish the change. Physicians may findstatements such as the following to be useful:"Yes, it is difficult. W^at difficult things haveyou accomplished in the past?" or "I've seenyou handle some tough stuff, I know you'll beable to conquer this." A successRil approachcalls for physicians to ask patients about pos-sible strategies to overcome barriers and thenarrive at a commitment to pursue one strat-egy before the next visit. It is also productiveto ask patients about their previous methodsand attempts to change behavior. Barriersand gaps in patients' knowledge can then sur-face for further discussion.
TABLE 3
Questions for Patients in thePrecontemplation and Contemplation Stages*
Precontemplation stage
Goal: patient will begin thinking about change.
"What would have to happen for you to know that this is a problem?"
"What warning signs would let you know that this is a problem?"
"Have you tried to change in the past?"
Contemplation stage
Goal: patient will examine benefits and barriers to change.
"Why do you want to change at this time?"
"What were the reasons for not changing?"
"What would keep you from changing at this time?"
"What are the barriers today that keep you from change?"
"What might help you with that aspect?"
"What things (people, programs and behaviors) have helped in the past?"
"What would help you at this time?"
"What do you think you need to learn about changing?"
*—The change can be applied to any desirable behavior (e.g., smoking or drink-ing cessation, losing weight, exercise).
Information from Miller WR, Rollnick S. Motivational interviewing: preparingpeople to change addictive behavior. New York: Guilford, 1991:191-202.
MARCH 1,2000 / VOLUME 61, NUMBER 5 AMERICAN FAMILY PHYSICIAN 1413
When patients experiment with changing abehavior (preparation stage) such as cuttingdown on smoking or starting to exercise, theyare shifting into more decisive action. Physi-cians should encourage them to address thebarriers to full-fledged action. While continu-ing to explore patient ambivalence, strategiesshould shiff from motivational to behavioralskills. During the action and maintenancestages, physicians should continue to askabout successes and difficulties—and be gen-erous with praise and admiration.
Relapse from Changed BehaviorRelapse is common during lifestyle changes.
Physicians can help by explaining to patientsthat even though a relapse has occurred, theyhave learned something new about themselvesand about the process of changing behavior.For example, patients who previously stoppedsmoking may have learned that it is best toavoid smoke-filled environments. Patientswith diabetes who are on a restricted diet maylearn that they can be successful in adhering tothe diet if they order from a menu rather thanchoose the all-you-can-eat buffet. Focusing onthe successful part of the plan ("You did it forsix days; what made that work?") shifts thefocus from failure, promotes problem solvingand offers encouragement. The goal here is tosupport patients and re-engage their efforts inthe change process. They should be left with asense of realistic goals to prevent discourage-ment, and their positive steps toward behaviorchange should be acknowledged.-"*
Additional ToolsTwo techniques useful in the primary care
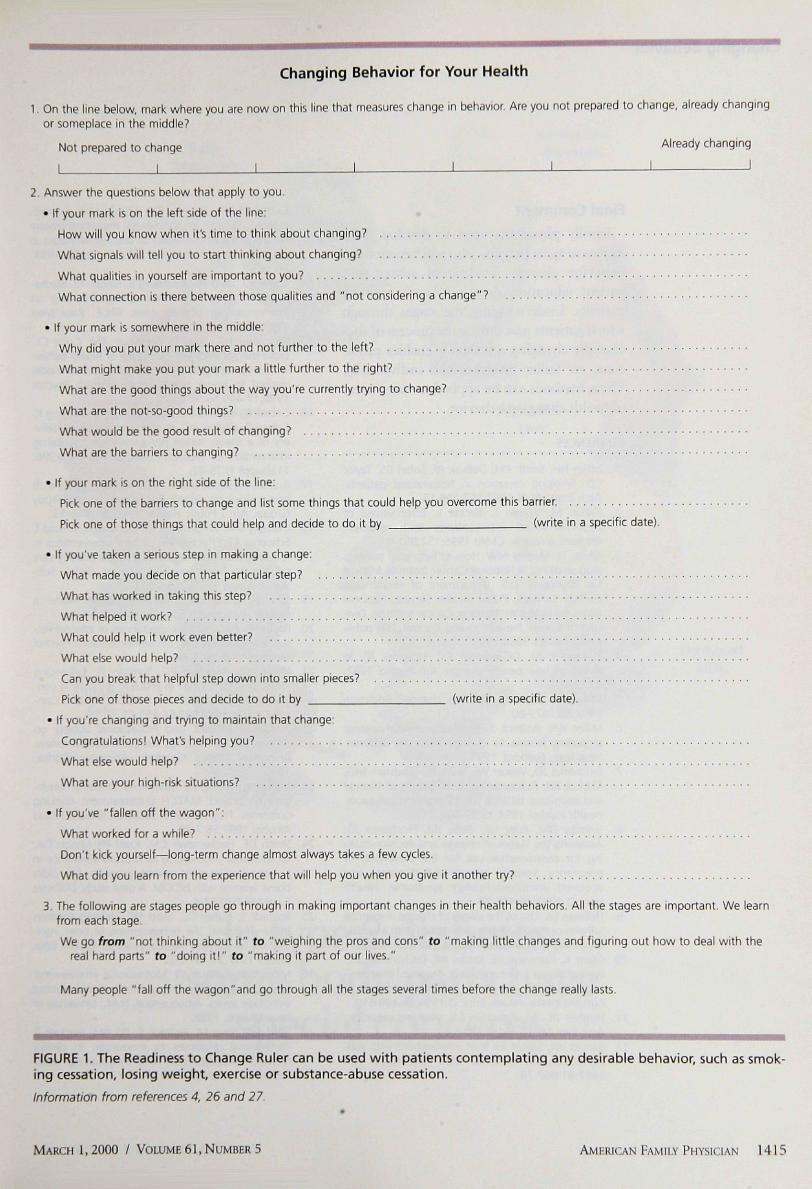
setting are the Readiness lo Change Ruler andthe Agenda-Setting Chart.^^'" The Readinessto Change Ruler, which is incorporated inFigure l^^-^^ is a simple, straight line drawnon a paper that represents a continuum fromthe left "not prepared to change" to the right"ready to change." Patients are asked to markon the line their current position in thechange process. Physicians should then ques-
tion patients about why they did not place themark further to the left (which elicits motiva-tional statements) and what it would take tomove the line further to the right (which elic-its perceived barriers). Physicians can askpatients for suggestions about ways to over-come an identified barrier and actions thatmight be taken before the next visit.
The Agenda-Setting Chart is useful whenmultiple lifestyle changes are recommended forlong-term disease management (e.g., diabetesor prevention of heart disease). The physiciandraws multiple circles on a paper, filling inbehavior changes that have been shown to affectthe disease in question and adding a few blankcircles. For example, "lose weight," "stop smok-ing" and "exercise" may each occupy a circle—all of them representing behavior changes thatare known to reduce the risk of heart disease.The physician begins the patient session with,"Let's spend a few minutes talking about someof the ways we can work together to improveyour health. In the circles are some factors wecan tackle to improve your health. Are thereother factors that you know woLild be impor-tant to address that we shoLild add to the blankcircles?" Discussion then revolves aroLind thepatient's priority area and identifies a goal thatmight be achievable before the next office visit.
Involving OthersWhile no research is available tbat uses the
Stages of Change model"" in teaching familieshow to intervene with their loved one'shealth-risk behavior, training about thismodel may help family members view the sit-uation differently.
Physicians can enlist the help of other healthcare professionals (e.g., nutritionists, nurses,mental health personnel) to reinforce the mes-sage that a change in behavior is needed and toprovide additional education and skill infor-mation to the patient. Referral can also reducesome patient care burden for physicians.Physicians should document the content andoutcome of patient conversations, includingspecific tasks and plans for follow-up.
1414 AMERICAN FAMILY PHYSICIAN VOLUME 61, NUMBER 5 / MARCH 1,2000
Changing Behavior for Your Health
1. On the line below, mark where you are now on this line that measures change in behavior. Are you not prepared to change, already changingor someplace in the middle?
Not prepared to change already changing
I \ I \ \ \ J 1
2. Answer the questions below that apply to you.
• If your mark Is on the left side of the line:
How will you know when it's time to think about changing?
What signals will tell you to start thinking about changing?
What qualities in yourself are important to you?
What connection is there between those qualities and "not considering a change"?
• If your mark is somewhere in the middle:
Why did you put your mark there and not further to the left?
What might make you put your mark a little further to the right?
What are the good things about the way you're currently trying to change?
What are the not-so-good things?
What vi/ould be the good result of changing?
What are the barriers to changing?
• If your mark is on the right side of the line:
Pick one of the barriers to change and list some things that could help you overcome this barrier.
Pick one of those things that could help and decide to do it by (write in a specific date).
• If you've taken a serious step in making a change:
What made you decide on that particular step?
What has worked in taking this step?
What helped it work?
What could help it v̂ /ork even better?
What else would help?
Can you break that helpful step down into smaller pieces?
Pick one of those pieces and decide to do it by {write in a specific date).
• If you're changing and trying to maintain that change:
Congratulations! What's helping you?
What else would help?
What are your high-risk situations?
• If you've "fallen off the wagon":
What worked for a while?
Don't kick yourself—long-term change almost always takes a few cycles.
What did you learn from the experience that will help you when you give it another try?
3. The following are stages people go through in making important changes in their health behaviors. Al! the stages are important. We learnfrom each stage.
We go from "not thinking about it" to "weighing the pros and cons" to "making little changes and figuring out how to deal with thereal hard parts" to "doing it!" to "making it part of our lives,"
Many people "fall off the wagon"and go through all the stages several times before the change really lasts.
FIGURE 1. The Readiness to Change Ruler can be used with patients contemplating any desirable behavior, such as smok-ing cessation, losing weight, exercise or substance-abuse cessation.
Information from references 4, 26 and 27.
MARCH 1,2000 / VOLUME 61, NUMBER 5 AMFRICAN FAMILY PHYSICIAN 1415
Changing Behavior
Final CommentFamily physicians need to develop tech-
niques to assist patients who will benefit frombehavior change. Traditional advice andpatient education does not work with allpatients. Understanding the stages throughwhich patients pass during the process of suc-cessfully changing a behavior enables physi-cians to tailor interventions individually.These methods can be applied to many areasof health changing behavior.
REFERENCES
1. Miller NH, Smith PM, DeBusk RF, Sobel DS, TaylorCB. Smoking cessation in hospitalized patients.Arch Intern Med 1997;157;409-15.
2. Kahan M, Wilson L, Becker L. Effectiveness ofphysician-based interventions with problemdrinkers: a review CMAJ 1995;1S2:851-9.
3. Glynn TJ, Manley MW. How to help your patientsstop smoking: a National Cancer Institute Manualfor Physicians. U.S. Department of Health andHuman Services, Public Health Service, NationalInstitutes of Health, National Cancer Institute, Divi-sion of Cancer Prevention and Control. NIH publi-cation no. 95-3064; 1995.
4. Prochaska JO, DiClemente CC, Norcross JC. Insearch of how people change. Am Psychol 1992;47:1102-4.
5 Miller WR What really drives change? Addiction1993;88:1479-80,
6. Miller WR, Rollnick S. Motivational interviewing:prepanng people to change addictive behavior.New York: Guilford, 1991.
7. Prochaska JO, Veticer WF, Rossi JS, Goldstein MG,Marcus BH, Rakowski W, et al. Stages of changeand decisional balance for 12 problem behaviors.Health Psychol 1994;13:39-46.
8. Grimley DM, Riley GE, Bellis JM, Prochaska JO.Assessing the stages of change and decision-mak-ing for contraceptive use for the prevention ofpregnancy, sexually transmitted diseases, andacquired immunodeficiency syndrome. HealthEducQ 1993;29 455-70.
9. Hellman EA Use of the stages of change in exerciseadherence model among older adults witb a cardiacdiagnosis J Cardiopulm Rehabil 1997;17:145-55,
10 Glanz K, Patterson RE, Kristal AR, DiClemente CC,Heimendinger J, Linnan L, et al Stages of change inadopting healthy diets: fat, fiber, and correlates ofnutrient intake. Health Educ Q 1994;21:499-519.
11. Hughes JR An algorithm for smoking cessation.Arch Fam Med 1994;3:280-5.
12. Barnes HN, Samet JH. Bnef interventions with sub-stance-abusing patients. Med Clin North Am1997;81:867-79.
13. Campbell MK, DeVellis BM, Strecher VJ, Ammer-man AS, DeVellis RF, Sandier RS. Improving dietarybehavior: the effectiveness of tailored messages inprimary care settings. Am J Public Health 1994;84:783-7.
14. Calfas KJ, Sallis JF, Oldenburg B, French M. Media-tors of change in physical activity following anintervention in primary care: PACE. Prev Med1997;26:297-304.
15. Weinstein ND, Lyon JE, Sandman PM, Cuite CL.Experimental evidence for stages of health behav-ior change: the precaution adoption process modelapplied to home radon testing. Health Psychol1998;17:445-53.
16- Cabrai RJ, Galavotti C, Gargiullo PM, Armstrong K,Cohen A, Gielen AC, et al. Para professional deliv-ery of a theory based HIV prevention counselinginten/ention for women. Public Health Rep 1996:ilKsuppI 1):75-82.
17. A cross-national trial of brief interventions withheavy drinkers. WHO Brief Intervention StudyGroup. Am J Public Health 1996;86:948-55.
18. Oliansky DM, Wildenhaus KJ, Manlove K. Arnold T,Schoener EP Effectiveness of brief interventions inreducing substance use among at-risk primary carepatients in three community-based clinics. Sub-stance Abuse 1997,18:95-103.
19. Janz NK, Becker MH. The Health Belief Model: adecade later. Health EducQ 1984; 11:1-47,
20 Rotter JB. Generalized expectancies of internal ver-sus external control of reinforcement. PsycholMonogr 1966;80:1-28.
21. Miller WR, Benefield RG, Tonigan JS. Enhancingmotivation for change in problem drinking: a con-trolled comparison of two therapist styles. J Con-sult Clin Psychol 1993;61:455-61.
22. Australian Medical and Professional Society onAlcohol and Other Drugs. Drug and alcohol review,Abingdon, United Kingdom: Abingdon Carfax,1996.
23. Matching alcoholism treatments to client hetero-geneity: project MATCH posttreatment drinkingoutcomes. Project Match Research Group. J StudAlcohol 1997;58:7-29.
24. Smith DE, Heckemeyer CM. Kratt PP, Mason DA.Motivational interviewing to improve adherence toa behavioral weight-control program for olderobese women with NIDDM. A pilot study DiabetesCare 1997;20:52-4
25. Rollnick S, Butler CC, Stott NC. Helping smokersmake decisions: the enhancement of brief inter-vention for general medical practice. Patient EducCouns 1997,31:191-203.
26. Miller WR, Rollnick W. Motivational interviewing:preparing people to change Professional trainingvideotape series, Albuquerque, NM.: University ofNew Mexico, 1998.
27. Stott NC, Rees M. Rollnick S, Pill RM, Hackett RProfessional responses to innovation in clinicalmethod: diabetes care and negotiating skills.Patient Educ Couns 1996;29:67-73.
1416 AMERICAN FAMILY PHYSICIAN VOLUME 61, NUMBER 5 / MARCH 1,2000





![Interventions before consultations for helping patients address … · 2012-12-12 · [Intervention Review] Interventions before consultations for helping patients address their information](https://img.pdfslide.net/doc/110x75/5ec57221f5ea872f585b6e4f/interventions-before-consultations-for-helping-patients-address-2012-12-12-intervention.jpg)
























