Embed Size (px)
Citation preview

A Synergistic Approach to Improving Outcomes for Homeless Mentally Ill Remand
Prisoners
Dr. Damian Smith, Ms. Orla Reynolds and Mr Philip Hickey
National Forensic Mental Health Service
and Cloverhill Prison, Dublin
Quality Network for Prison Mental Health Services
Special Interest Day, RCPsych
14th March 2017

Introduction

Transinstitutionalisation

Transinstitutionalisation

Homeless Mentally Ill Prisoners
• Homeless individuals with MMI and SUDs are over-represented in prison populations.
• Recidivism (Greenberg 2008)
• Mortality (Geddes 2011)

Difficulty Accessing Healthcare - Why?
Acutely Unwell
IntoxicatedHard to
find
“I know him, its just the drugs... And hes a PD”
“Always out of it”“I told you... Its just the drugs”
“No address”“Not our catchment area”
INVISIBLE

Ireland’s Homeless Crisis

Sentenced vs. Remand

Cloverhill Prison Inreach and Court liaison Service (PICLS)

Homeless Mentally Ill Prisoners – An Unmet Need?
• Prevalence of Homelessness among those seen by PICLS?
• How do the characteristics of homeless and non-homeless mentally ill prisoners differ?
• 3 year observational study with longitudinal data collection– 1st Jan 2012 to 31st Dec 2014
• Sources of Referral

Prevalence of Homelessness
• 35.0% (n=298) of all committals (n=1110, 902 individuals) seen by PICLS were homeless.
• This map displays the HSE regions of origin for non-homeless detainees seen (n=604)
• The population of a fictional “homeless region” surpassed each of the HSE regions (n=298).
298

Comparison of Homeless vs. Non-
Homeless
• Z-test statistic was used to test for differences in distribution of the variables between homeless and non-homeless subgroups
• X2* was used for binary outcome variables.

An unmet need was identified
• 35% of all referrals to PICLS over a 3 year period were homeless.
• These individuals had significantly increased levels of psychosis and comparable rates of substance misuse.
• Most were charged with Non-Violent Offences

Homeless Mentally Ill Prisoners
• Homeless individuals with MMI and SUDs are over-represented in prison populations.
• Recidivism (Greenberg 2008)
• Mortality (Geddes 2011)

Improving Outcomes for Homeless Mentally Ill Prisoners
• A “housing first” approach:recidivism hospitalisation (Srebnik 2013)
• This model targets homeless individuals with complex needs and provides them with supported accommodation ‘FIRST’, without the usual prerequisites of sobriety and stable mental health. (Tsemberis 2004)

A Synergistic Approach to Improving Outcomes for Homeless mentally Ill Remand Prisoners
HSW

Aims and Objectives
• To identify and support homeless mentally ill prisoners by:
– Improving their access to accommodation and by arranging appropriate mental health care
• In addition we aimed to measure:
i. Prevalence of homelessness ii. Homeless status of individuals seen by the HSW at time of receptioniii. Housing outcomes iv. Mental health outcomes v. Proportion of individuals registered with their local housing authority before
and after the introduction of the HSW

Method

Method
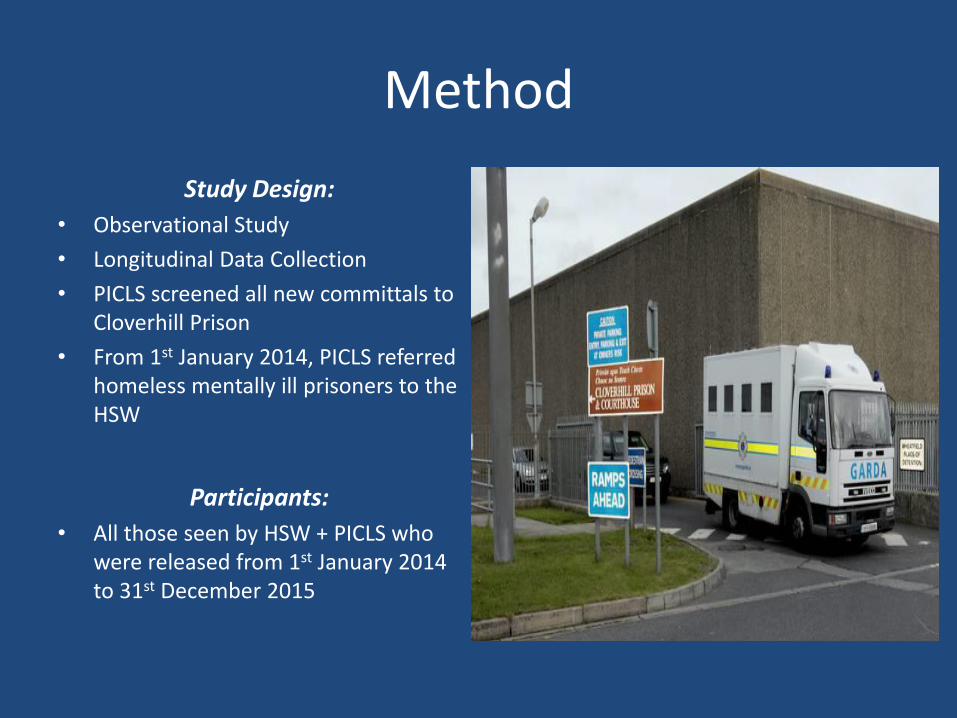
Setting:•Cloverhill Prison
•Closed, Medium Security, Male
•Capacity = 433
•60% of Ireland’s Remands
•Small number of sentenced prisoners
Method
Study Design:
• Observational Study
• Longitudinal Data Collection
• PICLS screened all new committals to Cloverhill Prison
• From 1st January 2014, PICLS referred homeless mentally ill prisoners to the HSW
Participants:
• All those seen by HSW + PICLS who were released from 1st January 2014 to 31st December 2015

Method
Variables:• Demographics
• Clinical
• Number of committals
• Homeless Status on Reception and at time of release
• Housing and Mental Health Outcomes
Statistical Analysis:• The z-test statistic was used to test
for differences between groups

The PICLS Team

Housing Support Worker (HSW)
• Identification
• Support, Advice and Advocacy
• Liaison with local authorities and housing support agencies to arrange for accommodation and support upon release
• Liaison with Community Mental Health Teams
• Court attendance
• Time-limited period of post-release support


Results

Results – Prevalence of Homelessness
Two Years Pre-HSW – 749 committals seen
– 293 were homeless (n=236 individuals)
– 39% (95% CI 35.7 – 42.7)
Two Years with HSW– 769 committals seen
– 248 were homeless (n=191 individuals)
– 32%, (95% CI 29.0 – 35.6)
No significant difference in the proportion of homeless individuals seen between the two time periods (p=0.15).
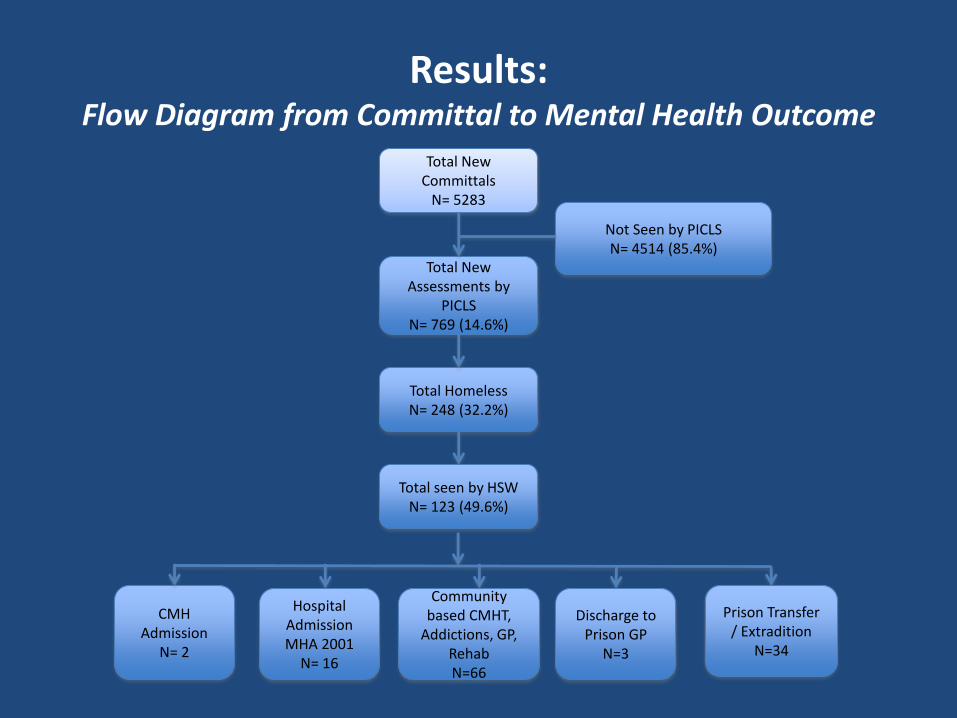
Results: Flow Diagram from Committal to Mental Health Outcome
Total New Committals
N= 5283
Total New Assessments by
PICLSN= 769 (14.6%)
Total HomelessN= 248 (32.2%)
CMH Admission
N= 2
Not Seen by PICLSN= 4514 (85.4%)
Hospital Admission MHA 2001
N= 16
Community based CMHT,
Addictions, GP, RehabN=66
Discharge to Prison GP
N=3
Prison Transfer / Extradition
N=34
Total seen by HSWN= 123 (49.6%)

Results
• HSW met with 123 separate committal episodes (n=90 individuals)
• 303 face-to-face meetings (mean 2.5, SD 2.1)
• All those seen:
1. Received a Homeless Service Information booklet,
2. Registered with the homeless Central Placement Service (CPS)
3. Offered assistance in applying for a medical card.
Results – Registration with Housing Authority
• 25 individuals (28%) were newly registered with their local housing authority
• of registration from 38% (n=34) to 66% (n=59), by the end of 2015 (p<0.001)
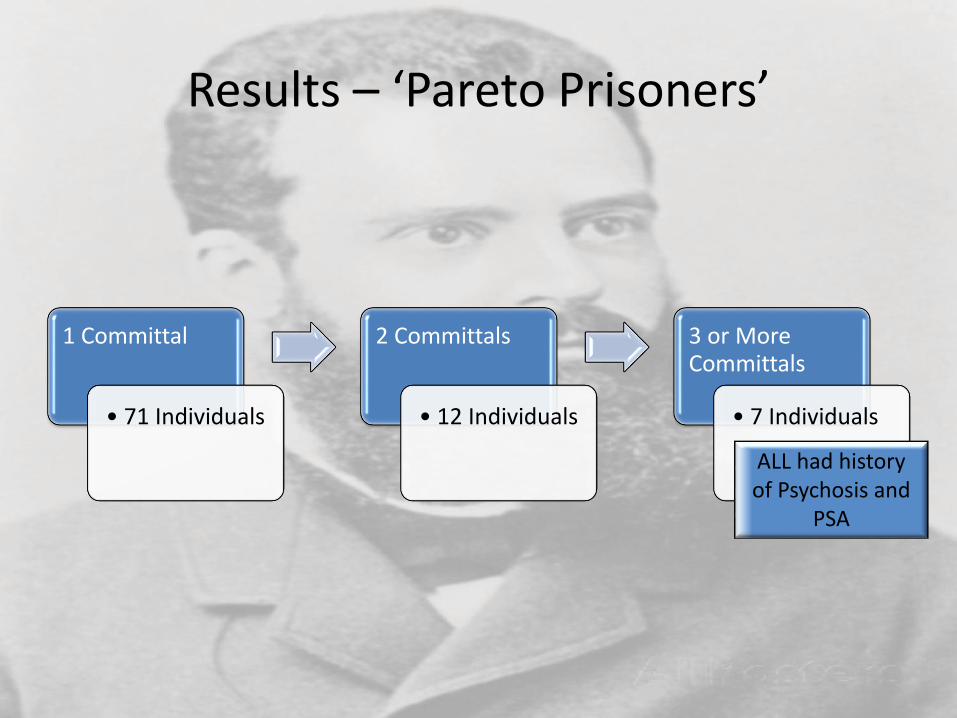
Results – ‘Pareto Prisoners’
1 Committal
• 71 Individuals
2 Committals
• 12 Individuals
3 or More Committals
• 7 Individuals
ALL had history of Psychosis and
PSA

Homeless Status at Time of Reception(n=123, 90 individuals)
Categories defined by the DRHE (Dublin Regional Homeless Executive)

Results – Rough Sleeping
30.1% (n=37) of new committals seen by the HSW were sleeping rough at the time of reception

Results - Accommodation at Time of Reception vs. Time of Release
(n=73, 56 Individuals)
28
18
1
7
14
7
0
9
6
26
20
12
0
5
10
15
20
25
30
RoughSleeping EmergencyAccom.-One-NightOnly
ShortTermHostel MediumTermSupportedHostel
Returnedtolivewithfamily/
Friend
SecureTenancy/ownhome/rental/Long
TermSupportedHostel
HousingatTimeofCommi al HousingatTimeofRelease
**
ns
ns

Results – Housing Outcomes
• The remaining 50 committal episodes resulted in the following outcomes:
– Transfer to CMH (n=2)
– Transfer to AMHS Hospital (n=16)
– Transfer to another prison (n=31)
– Extradition (n=1).

Mental Health Outcomes Following Input from PICLS and HSW (n=123)
2
16
66
3
34
0
10
20
30
40
50
60
70
CMHAdmission AMHS-HospitalAdmission
CommunitybasedOPD/GP/Addic on
Psychiatry/Rehab
DischargetoPrisonGP PrisonTransferandreferraltoReceivingPrisonInreachMHS

Results - Mortality
Tragically 2% (n=3) of those seen died following release within the two year
period

Conclusions:Making the Invisible: Visible
• Homelessness is prevalent among Mentally Ill remand Prisoners.
• These individuals have high rates of psychosis and PSA.
• Housing outcomes were improved following input from the HSW including:
– Improvement in housing status– Increased levels of registration with local housing authorities

‘A Day in the Life of the Invisible’
Case 1: ‘Entrenched Rough Sleeper’
• You are Mr Smith, a 41yo, single man
• You were released from court this afternoon after the Judge gave you time served (4 weeks) for 2 public order offences.
• You have been homeless for 12-13 years
• You prefer to sleep rough because the hostels are full of messers and junkies
• Your doctors tell you have Schizophrenia but you don’t believe this to be the case; its just a bit of confusion
• You aim to celebrate your release with a few cans of beer... It never did you any harm before now.... And sure it’s a Friday!

Case 2: ‘Long Term Homeless’
• You are Mr Hickey, a 25yo man
• You were released from court earlier today on a suspended sentence.
• You have to meet with your probation officer.
• You have been homeless for the past two years.
• You were staying in a hostel before prison but you’re unsure if you can go back to it
• You’ve been barred from many hostels previously because you don’t pay your rent and the staff think you’re trouble
• You’ve been told you have schizophrenia but you rarely go to appointments because they always give out to your drug use
• You were drug-free in prison and would like some support to stay drug-free in the community.

Case 3: ‘First time Homeless’
• You are Mr Reynolds, a 30yo man
• You were charged with breach of a barring order and unexpectedly released on bail this morning
• You only have 20 euro in your pocket
• You can’t return to your parent’s house or you’ll be arrested
• Your doctor’s told you that you’re “delusional” and that you might be “a risk” to your dad if you go back on the drink
• You think that's a load of rubbish, but you think you should follow their advice and attend the Psych Apt just in case they breach your bail

DISCUSSION

Discussion
• Homeless mentally ill prisoners present a challenge to services due to their complex needs.
• This can result in a cycle of relapse and recidivism.
• Although an inappropriate setting to provide healthcare, could a remand prison be viewed as an opportunity to engage this (hard to find, difficult to engage, vulnerable group) with much needed mental health and housing supports?
• In an environment where they can be:
i. found ii. are sober iii. are on medicationiv. have access to advocates

An Opportunity to Engage?
On Medication
SoberFound
VISIBLE

Discussion
• Urgent need for:1. Prison Inreach social work and HSW input in other prisons?
2. Community based step down unit aimed at providing rehabilitation and community reintegration?
• B-HOP Network – Interagency Think Tank
• Future Research:1. Level of engagement?
2. Improvements in Functioning and Quality of Life?
3. Pareto Patients?

AcknowledgementsDr Conor O’Neill
Mr Martin Caddow
Mr Fergal Duffy
Mr Philip Hickey
Ms Donna Madill
Dr Fintan Byrne
Dr Jamie Walsh
Dr Mark Joynt
Dr Tom Cronin
Dr Zetti Azvee
Prof Harry Kennedy
Mr Larry Keevans
Gov Ronan Maher
Gov Chris McCormack

Thank you!
Contact details: