Embed Size (px)
Citation preview

REVIEW
A systematic review and meta-analysis of social cognitivetheory-based physical activity and/or nutrition behavior changeinterventions for cancer survivors
Fiona G. Stacey & Erica L. James & Kathy Chapman &
Kerry S. Courneya & David R. Lubans
Received: 10 July 2014 /Accepted: 11 November 2014 /Published online: 29 November 2014# The Author(s) 2014. This article is published with open access at Springerlink.com
AbstractPurpose Little is known about how to improve and createsustainable lifestyle behaviors of cancer survivors. Interven-tions based on social cognitive theory (SCT) have shownpromise. This review examined the effect of SCT-based phys-ical activity and nutrition interventions that target cancersurvivors and identified factors associated with their efficacy.Methods A systematic search of seven databases identifiedrandomized controlled trials that (i) targeted adult cancersurvivors (any point from diagnosis); (ii) reported a primaryoutcome of physical activity, diet, or weight management; and(iii) included an SCT-based intervention targeting physicalactivity or diet. Qualitative synthesis and meta-analysis wereconducted. Theoretical constructs and intervention
characteristics were examined to identify factors associatedwith intervention efficacy.Results Eighteen studies (reported in 33 publications) metreview inclusion criteria. Meta-analysis (n=12) revealed asignificant intervention effect for physical activity (standard-ized mean difference (SMD)=0.33; P<0.01). Most studies(six out of eight) that targeted dietary change reported signif-icant improvements in at least one aspect of diet quality. NoSCT constructs were associated with intervention effects.There were no consistent trends relating to intervention deliv-ery method or whether the intervention targeted single ormultiple behaviors.Conclusions SCT-based interventions demonstrate promise inimproving physical activity and diet behavior in cancer survi-vors, using a range of intervention delivery modes. Furtherwork is required to understand how and why these interven-tions offer promise for improving behavior.Implications for Cancer Survivors SCT-based interventionstargeting diet or physical activity are safe and result in mean-ingful changes to diet and physical activity behavior that canresult in health improvements.
Keywords Cancer . Physical activity . Nutrition . Systematicreview . Social cognitive theory
Background
Due to population growth and aging and improved cancerdetection and treatment, the number of cancer survivors isincreasing [1, 2]. Many cancer survivors experience sideeffects from treatment and are at risk for secondary cancersand other chronic diseases such as cardiovascular disease anddiabetes [3]. Several systematic reviews and meta-analyseshave synthesized the findings of physical activity (PA) inter-ventions in cancer survivors [4–9]. These reviews concluded
F. G. Stacey (*) : E. L. JamesSchool ofMedicine and Public Health, University of Newcastle, W4,HMRI Building, Callaghan, NSW 2308, Australiae-mail: [email protected]
F. G. Stacey : E. L. JamesHunter Medical Research Institute, Callaghan, NSW, Australia
F. G. Stacey : E. L. JamesPriority Research Centre for Health Behavior, University ofNewcastle, Callaghan, NSW, Australia
F. G. Stacey : E. L. James :D. R. LubansPriority Research Centre in Physical Activity and Nutrition,University of Newcastle, Callaghan, NSW, Australia
K. ChapmanCancer Council New South Wales, Woolloomooloo, NSW, Australia
K. S. CourneyaFaculty of Physical Education and Recreation, University of Alberta,Edmonton, Alberta, Canada
D. R. LubansSchool of Education, University of Newcastle, Callaghan, NSW,Australia
J Cancer Surviv (2015) 9:305–338DOI 10.1007/s11764-014-0413-z

that being physically active improved fitness, strength, bodycomposition, fatigue, anxiety, depression, self-esteem, physicalfunction, bone health, and quality of life [5, 6, 8, 9] and reducedrisk of cancer recurrence and mortality among survivors ofbreast, bowel, prostate, and ovarian cancer [9, 10]. Dietaryinterventions report improved physical functioning [11, 12]and weight loss [13], lower levels of depression [12], and areduction in new cancer events [13]. Diet and PA also play arole in energy balance andweight management, an independentpredictor of cancer risk, and risk of recurrence and mortality[14] and contribute to the development of other chronic dis-eases, like diabetes and cardiovascular disease [15–17]. Forthese reasons, guidelines recommend PA (both aerobic andresistance), healthy diet, and healthy weight management forimproving the health and well-being [8, 9, 14, 18–21] of cancersurvivors across all phases of the cancer continuum [22]. Whileweight management is not a lifestyle behavior, it is the keytarget of lifestyle behavior strategies. Despite the potentialimpact of behavior on improved health outcomes, cancer sur-vivors’ compliance with health recommendations remains lessthan optimal and is similar to the general population [23–25].
Effective diet and PA interventions have the potential toimprove cancer survivors’ health, but little is known about whatinterventions work best. Interventions based on behavioraltheory are reported to be more effective than atheoretical ap-proaches [26, 27]. Theory-based research provides a frame-work for the development and evaluation of interventions[28] and facilitates understanding of the factors that mediatebehavior change and the reasons why the intervention workedor failed [29, 30]. Social cognitive theory (SCT) is one prom-ising theory for use in behavior change interventions [31],particularly as it provides a framework for understanding whypeople make andmaintain health behaviors. The key constructsof SCT include the following: (1) knowledge of health risks andbenefits; (2) perceived self-efficacy that a person can controltheir own health habits; (3) the expected costs and benefits oroutcome expectations; (4) health goals, both proximal anddistal intentions to engage in the behavior; (5) perceived facil-itators and social support; and (6) barriers to making changes[31]. In 2004, Bandura reported a framework that specified thekey determinants and the interplay between the key constructs(known as “reciprocal determinism”). Knowledge of healthrisks and benefits sets the scene for possible behavior change;however, it is not enough to prompt behavior change alone[31]. Self-efficacy influences outcome expectations and bar-riers/facilitators, and all constructs influence goals [31]. Allconstructs influence behavior and motivation and are influ-enced by the environment [31]. Self-efficacy is the centralconstruct in SCT because it influences behavior directly,through belief in their ability to apply skills effectively indifficult situations, and indirectly, through influence on goals,outcome expectations, and barriers and facilitators [31, 32].Self-efficacy is a major influence on motivation by determining
the goals people set for themselves, the strength of commitmentto them, and the outcomes they expect for their efforts [32].Self-efficacy allows the individual to gain knowledge anddevelop skills, and as self-efficacy increases, people expectpositive outcomes, overcome barriers, and show motivationand commitment to goals [32]. SCT constructs explain 40–71 % of the variance in PA behavior in adults [33–37] andhave been shown to explain dietary behavior in adults,explaining 14–35, 22–53, and 36–61 % of the variance in fat,fiber, and fruit and vegetable intake [37, 38]. SCT also offersprinciples on how to motivate people to make positive behaviorchange [31]. Previous meta-analysis of health outcomes trialswith cancer survivors concluded that SCT-based interventionsresulted in improvements in global affect, depression, socialoutcomes, objective physical outcomes, and specific quality oflife outcomes [39]. However, little is known about whetherinterventions based on SCT can positively impact on PA anddiet behaviors, and what constructs and intervention character-istics are associated with increased behavior change.
There are currently no systematic reviews including multi-ple cancer types that synthesize both PA and diet behaviorchange interventions. While there is significant evidencesupporting the impact of diet and PA behavior on healthoutcomes, there is a need to move to interventions that testhow to motivate cancer survivors to make positive sustainablebehavior change. Current evidence suggests that cancer sur-vivors do not maintain PA behavior after participating in asupervised PA intervention [40, 41]. This review examined PAand diet behavior change interventions based on SCT incancer survivors with mixed diagnoses both during and aftercompletion of cancer treatment [42].
Aim
This systematic review and meta-analysis aimed to (1) syn-thesize randomized controlled trials (RCTs) evaluating theefficacy of SCT-based behavior change interventions on PAand/or diet behaviors for cancer survivors of mixed diagnosesand (2) identify successful strategies for behavior change thatcan be used to guide intervention development. Of importancefor a reviewwith this aim is the definition of what constitutes abehavior change trial. We have used the reference defined byCourneya [43], that is, trials where the primary outcome isbehavior (as opposed to a health outcomes trial where theprimary outcome is quality of life, fatigue, etc.).
Method
Search strategy
The review was guided by the PRISMA statement [44].Studies were identified by structured database search from
306 J Cancer Surviv (2015) 9:305–338

inception until September 2014, in PsycINFO, CINAHL,Cochrane Central Register of Controlled Trials, Embase,Medline, SportDiscus, and Web of Science using the follow-ing search strings:
1. (Cancer survivor) or (cancer patient) or cancer.2. Nutrition or diet or food or fruit or vegetable.3. (Physical activity) or exercise or weight or aerobic or
(strength training) or (resistance training) or walking.4. (Social cognitive theory) or (social cognitive) or (social
learning theory) or (behavio#r change theor*). Stringswere made up of 1+(2 or 3) +4.
A sample search strategy is listed in the Appendix 1.Searches were limited to English language articles and thosethat targeted humans. Study titles were screened for eligibilityby a single reviewer (FS). Full text of the remaining titles wasobtained and screened in hierarchical order with studies ex-cluded at the first reason for exclusion (FS).
1. Participants: adults aged 18 years or older, diagnosed withany cancer (at any point from diagnosis)
2. Outcomes: primary outcome of PA or diet or body weight(loss, or maintenance)
3. Intervention:
(a) Any intervention designed to influence any type ofPA or diet quality
(b) Based on Bandura’s SCT [31], or explicitly de-scribed and referenced any SCT component (suchas “self-efficacy”)
4. Comparator: any parallel control group5. Study design: RCTs
Data extraction
Data extraction was conducted by one author (FS), and theextracted data was independently checked by a second author(EJ, DL, or KC). Disagreements were resolved by consensus.Data extraction forms were developed, piloted with one trial,and amended (FS). The following data were extracted: studypopulation and eligibility, behavior change outcomes andfollow-up periods, intervention characteristics, and how thetheory constructs were operationalized and assessed. Whereauthors indicated a trial protocol number, the protocol wasretrieved, but no other attempt was made to obtain unpub-lished trial information.
Synthesis of results
Separate meta-analyses were planned for PA and dietary out-comes. However, due to heterogeneity in dietary outcomes,
meta-analyses were conducted only for studies that reportedthe effect of the intervention on total PA using RevManversion 5.1 [45]. As recommended by the Cochrane Collabo-ration, posttest means and their standard deviations were usedin the analysis. Intention-to-treat data was extracted frompapers. When studies compared multiple treatment groupswith a single control group (n=2), the sample size of thecontrol group was divided to avoid double counting. All datawere considered continuous, but as PA was measured usingvarious methods, we report the standardized mean difference(SMD) and their 95 % confidence intervals. Statistical hetero-geneity was examined using chi-squared and the I2 index tests.A guide to the interpretation of heterogeneity based on the I2
index is as follows: 0–40 % might not be important; 30–60 %may represent moderate heterogeneity; 50–90 % may repre-sent substantial heterogeneity; and 75–100 % considerableheterogeneity [46].
Subgroup analyses comparing the number of behaviorstargeted (multiple behaviors compared to one only), cancertype, and number of theoretical constructs operationalized(self-efficacy compared to multiple theoretical constructs)were planned. However, the limited number of studies andheterogeneity of included trials did not allow for subgroupanalyses.
Risk of bias
Risk of bias was assessed using the McMaster Quality As-sessment Tool [47], with a score of “strong,” “moderate,” or“weak” methodological quality assigned to each of six sec-tions (1. selection bias; 2. study design; 3. confounders; 4.blinding; 5. data collection methods; 6. withdrawals and drop-outs). A global rating was made based on the ratings fromeach of the six sections. As recommended, papers with no“weak” ratings were “strong” methodological quality; thosewith one “weak” rating were “moderate”; and those with twoor more “weak” ratings were “weak” [47]. Risk of bias wasundertaken by two independent reviewers (FS and EJ, or DL,or KC), with disagreements resolved by consensus (FS andEJ).
Results
Study selection
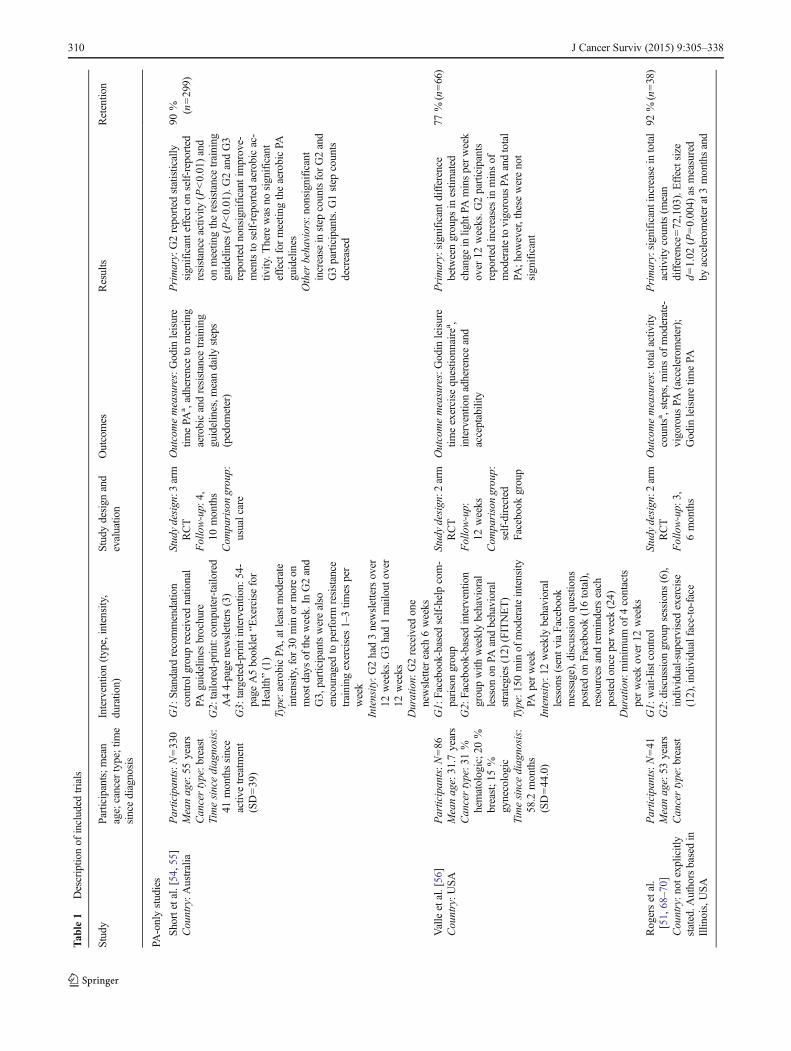
Figure 1 shows the flow of studies through the review processand the reasons for exclusion. Database searches resulted in2020 potentially relevant titles. The full text of 110 articleswas assessed for eligibility, and 18 studies (reported in 33publications) met inclusion for the review (Table 1). Studieswere grouped and reported by intervention topic: PA only (ten
J Cancer Surviv (2015) 9:305–338 307

trials), diet only (one trial), or multiple health behavior (PAand diet) (seven trials).
Risk of bias assessment
There was initially 75 % agreement between authors on thestudy assessment criteria and full consensus was achievedafter discussion. Risk of bias results are reported in Table 2.Of the ten PA-only studies, five were classified as strongmethodological quality [48–52], three as moderate [53–56],and two as weak [57, 58]. The diet-only trial was classified asmoderate [59]. In the sevenmultiple behavior studies, one wasclassified as strong [60], four were moderate [61–65], and two
weak [66, 67]. Three trials were excluded from the meta-analysis [57, 58, 67] due to being weak.
The most common areas with a high risk of bias wereselection bias, confounders, and blinding. Eleven studies[53, 54, 56–58, 61–67] were rated as weak in selection biascategory with less than 60 % of potentially eligible partici-pants recruited. Two studies [59, 66] were rated as weak as thecontrol of confounders was not described. No studies receiveda strong rating for blinding as (understandably given they arebehavior change trials), all participants were aware of theresearch question, and if the outcome assessor was also awareof the intervention status of participants, studies were rated asweak methodological quality [57, 58, 67].
Fig. 1 PRISMA flow diagram
308 J Cancer Surviv (2015) 9:305–338

Physical activity trials
There were ten trials that targeted PA alone [48–54, 56–58].
Participants
Ten PA trials reported a total of 960 participants (range36–330). Six trials targeted breast cancer survivors [48,50–52, 54, 58, 68–72], one targeted colorectal cancersurvivors [53], one targeted both breast and bowel can-cer survivors [49], and two included cancers of mixeddiagnoses [56, 57]. Mean time since diagnosis was3.1 years (range 0.9–4.9 years) [50, 51, 53, 54,56–58]. Time since diagnosis was not reported in twostudies [49, 52]; however, one trial reported participantswere scheduled to begin chemotherapy [52]. All othertrial participants had completed active cancer treatment(excluding hormone treatment). In five studies, onlycancer survivors who were inactive or insufficientlyactive were eligible to participate [48–50, 57, 58]. Threetrials used a wait-list control group design [48, 51, 58],three had attention control groups [50, 56, 57], andthree had usual care control groups [49, 52, 54]. Onetrial used an attention control design, with the controlgroup offered a limited intervention (written materialsonly) at the end of the study [53].
Intervention characteristics
One intervention was delivered by email [48], one de-livered by mail [54, 55], and one delivered usingFacebook [56], and all others used a combination ofdelivery formats, including telephone [49, 50, 52, 53,57, 58], mail [50, 53], and face-to-face counseling[51–53, 57, 58]. The majority were home-based, withonly one intervention reporting supervised PA sessions[51]. Three were walking interventions [51, 52, 58], andfour had PA goals that were based on duration [49, 54,56, 57] and/or moderate intensity [50, 53, 54, 56, 57].One targeted resistance training [54].
Interventions were commonly 12 weeks in duration [48,50, 51, 53, 54, 56, 58] and ranged from 6 [52] to 18 weeks[57]. The average number of intervention contacts was 15, andranged from 1 [54] to 52 [56]. Intervention adherence washigh, ranging from 94 % compliance with home exercise logs[58] to 99 % of total contacts completed [51]. Telephonecounseling adherence was also high with a median of 9 (of11) calls completed [49] and a mean of 11 (of 12) callscompleted [50, 53]. The intervention delivered usingFacebook reported lower adherence, with 81% of interventionparticipants who reported receiving ten or more messagesfrom Facebook, and 49 % had made two or more Facebookposts [56].
Outcome assessment
Two trials used an objective measure (accelerometer) to assessPA behavior change [50, 51]. All others relied on self-reportmeasures [48, 49, 52–54, 56–58] or used an objective measurein a subsample only [58]. Effect sizes for PA behavior changewere reported in four studies (d=0.55–1.93) [51, 53, 54, 57].Three home-based walking interventions reported significantimprovements postintervention (6–12 weeks) to total PA (d=1.02; P=0.004) [51] and walking [52, 58]. Three moderateintensity interventions reported significant postinterventionincreases in PA (d=0.55; P<0.05) (d=1.93; P=0.02) [50,53, 57], and two reported nonsignificant increases to aerobicand moderate-vigorous PA [54, 56]. One trial that targetedresistance training reported significant improvements and thatthe odds of meeting the resistance training guidelines hadincreased by 3.38 in the tailored intervention group [54].
Of the four trials that reported follow-up assessments of6 months or longer [51, 53, 57, 68], only two reported behav-ior change 3 months after intervention completion [53, 68].One trial reported that accelerometer-assessed behavior wasmaintained [68], and one reported that there were significantpostintervention changes that were not maintained at 6 and12 month follow-ups [53]. Study retention was high, with amean retention rate of 86 % (range 71 % [57] to 95 % [50,53]). One trial [52] reported adverse events involving twoparticipants that experienced anemia, shortness of breath,and dizziness. Participants in this trial were undergoing activetreatment at the time of intervention.
Meta-analysis of SCT intervention effects on physical activity
Meta-analysis was conducted with 12 trials, which reportedPA outcomes [48–54, 56–58, 60, 63–65] in Fig. 2. Six trialswere not included in the meta-analysis [57–59, 61, 66, 67].Reasons for exclusion were as follows: diet-only study [59];did not report adequate information from the modified PArecall [61]; and did not report duration of PA [66]; or had ahigh risk of bias [57, 58, 67].
Two trials consisted of three study arms, which comparedtwo PA interventions to a standard recommendation control[54, 55], and a PA intervention to a PA and diet intervention,compared to an attention control group [60]. The results foreach intervention compared to the control group are reportedseparately in the meta-analysis. Results were pooled to estab-lish the effects of interventions on total PA at interventioncompletion. As there was moderate heterogeneity amonginterventions (χ2=22.71, df=13 [P=0.05]; I2=43 %), therandom effects models were used. The impact of interventionson PA immediately postintervention was significant (SMD=0.33 [0.23, 0.44], Z=6.34 [P<0.00001]) (Fig. 2). Sensitivityanalysis was undertaken that compared this analysis to a meta-analysis which included the three trials with high risk of bias
J Cancer Surviv (2015) 9:305–338 309
Tab
le1
Descriptio
nof
included
trials
Study
Participants;m
ean
age;cancer
type;tim
esincediagnosis
Interventio
n(type,intensity,
duratio
n)Studydesign
and
evaluatio
nOutcomes
Results
Retentio
n
PA-onlystudies
Shortetal.[54,55]
Country:A
ustralia
Participants:N
=330
Meanage:55
years
Cancertype:b
reast
Timesincediagnosis:
41monthssince
activ
etreatm
ent
(SD=39)
G1:
Standard
recommendatio
ncontrolg
roup
received
natio
nal
PAguidelines
brochure
G2:tailo
red-print:computer-tailo
red
A44-page
newsletters(3)
G3:
targeted-print
interventio
n:54-
page
A5booklet“Exercisefor
Health
”(1)
Type:aerobicPA
,atleastmoderate
intensity,for
30min
ormoreon
mostdaysof
theweek.In
G2and
G3,participantswerealso
encouraged
toperform
resistance
training
exercises1–3tim
esper
week
Intensity:G
2had3newslettersover
12weeks.G
3had1mailout
over
12weeks
Duration:
G2received
one
newslettereach
6weeks
Studydesign:3
arm
RCT
Follow-up:
4,10
months
Com
parisongroup:
usualcare
Outcomemeasures:Godin
leisure
timePA
a ,adherenceto
meetin
gaerobicandresistance
training
guidelines,m
eandaily
steps
(pedom
eter)
Primary:G2reported
statistically
significanteffecto
nself-reported
resistance
activ
ity(P<0.01)and
onmeetin
gtheresistance
training
guidelines
(P<0.01).G2andG3
reported
nonsignificant
improve-
mentsto
self-reportedaerobicac-
tivity.T
here
was
nosignificant
effectformeetin
gtheaerobicPA
guidelines
Other
behaviors:nonsignificant
increase
instep
countsforG2and
G3participants.G
1step
counts
decreased
90% (n=299)
Valleetal.[56]
Country:U
SA
Participants:N
=86
Meanage:31.7
years
Cancertype:3
1%
hematologic;2
0%
breast;1
5%
gynecologic
Timesincediagnosis:
58.2
months
(SD=44.0)
G1:
Facebook-based
self-helpcom-
parisongroup
G2:
Facebook-based
interventio
ngroupwith
weeklybehavioral
lesson
onPA
andbehavioral
strategies
(12)
(FITNET)
Type:150
minof
moderateintensity
PAperweek
Intensity:1
2weeklybehavioral
lessons(sentv
iaFacebook
message),discussion
questio
nsposted
onFacebook(16total),
resourcesandreminderseach
posted
once
perweek(24)
Duration:
minim
umof
4contacts
perweekover
12weeks
Studydesign:2
arm
RCT
Follow-up:
12weeks
Com
parisongroup:
self-directed
group
Outcomemeasures:Godin
leisure
timeexercise
questio
nnairea ,
interventio
nadherenceand
acceptability
Primary:significantd
ifference
betweengroups
inestim
ated
change
inlig
htPA
minsperweek
over
12weeks.G
2participants
reported
increasesin
minsof
moderatetovigorous
PAandtotal
PA;h
owever,these
werenot
significant
77%
(n=66)
Rogersetal.
[51,68–70]
Country:n
otexplicitly
stated.A
uthorsbasedin
Illin
ois,USA
Participants:N
=41
Meanage:53
years
Cancertype:b
reast
G1:
wait-listcontrol
G2:
discussion
groupsessions
(6),
individual-supervisedexercise
(12),individualface-to-face
Studydesign:2
arm
RCT
Follow-up:
3,6months
Outcomemeasures:totalactivity
countsa ,steps,minsof
moderate-
vigorous
PA(accelerom
eter);
Godin
leisuretim
ePA
Primary:significantincreaseintotal
activ
itycounts(m
ean
difference=72,103).Effectsize
d=1.02
(P=0.004)
asmeasured
byaccelerometerat3monthsand
92%
(n=38)
310 J Cancer Surviv (2015) 9:305–338

Tab
le1
(contin
ued)
Study
Participants;m
ean
age;cancer
type;tim
esincediagnosis
Interventio
n(type,intensity,
duratio
n)Studydesign
and
evaluatio
nOutcomes
Results
Retentio
n
Timesincediagnosis:
34monthssince
surgery(0.7–134)
counselin
g(3),transitio
nto
home-basedprogram
Type:m
oderateintensity
with
the
aim
ofbuild
ingup
to150min
ofmoderatewalking
perweek
Intensity:21sessions
over3months
Duration:
multip
leexposure
(minim
umweekly)
Com
parisongroup:
wait-listcontrol
remainedsignificantat6
months
(meandifference=61,651;
P=0.06)
Other
behaviors:significantincrease
inmoderateandvigorous
minutes
(d=0.57;d
=0.54
(P=0.09)).
Nonsignificantincreasein
self-
reported
moderateandvigorous
activ
ity(d=0.16;P
=0.63)
Pinto
etal.[50,71];
Rabin
etal.[72]
Country:n
otexplicitly
stated.A
uthorsbasedin
Rhode
Island,U
SA
Participants:N
=86
Meanage:53
years
Cancertype:early
stagebreastcancer
Timesincediagnosis:
1.74
years(SD
1.49)
G1:
contactcontrol,w
eeklyphone
callandcancer
survivorship
writtensheets
G2:
weeklytelephonecounselin
g(12)
andcustom
ized
written
feedback
(4),homeexercise
logs,
pedometer
Type:m
oderateintensity
PA(55–
65%
ofmaxim
umheartrate)
walking
gradually
build
ingup
togoalof30
minofaccumulated
PAperdayon
atleast5
days
per
week
Intensity:16contactsover3months
Duration:
multip
leexposure
(minim
umweekly)
Studydesign:2
arm
RCT
Follow-up:
12weeks,
6months,
9months
Com
parisongroup:
attentioncontrol
Outcomemeasures:7dayPA
recalla,1
mile
walktesta ,
accelerometera ,percentage
ofbody
fat(skinfold
thickness)a ,
body
massindexa
Primary:significantincreaseinmins
ofPA
,and
1mile
walktest
(P<0.001).S
ignificant
between
groupdifferenceswereevident
fortotalm
insof
PAon
7dayPA
recall(P<0.001),higherweekly
minsof
moderateintensity
PA(P<0.001),highertotalenergy
expenditu
re(P<0.001)
at12
weeks
Nodifference
inbody
massindexor
percentage
ofbody
fat
Other
behaviors
95%
(n=82)
Bennettetal.[57]
Country:n
otexplicitly
stated.F
irstauthor
basedin
New
Zealand;
co-authorsbasedin
Portland,U
SA
Participants:N
=56
Meanage:
interventio
n56
years;control
60years
Cancertype:any
Timesincediagnosis:
4.8years(SD3.0)
interventio
n
G1:
contactcontrol
G2:
singleface-to-face
counselin
g(30min)with
3follo
w-uptele-
phonecalls
(20min
percall),pe-
dometer
Type:p
hysicalactivity
aim
toreach
30min
ofmoderateintensity
PAon
mostd
aysof
week
Intensity:4
contactsover
18weeks
Duration:multip
leexposure(atleast
2weeks
apart)
Studydesign:2
arm
RCT
Follow-up:
3,6months
Com
parisongroup:
attentioncontrol
Outcomemeasures:Com
munity
Health
yActivities
Model
Program
forSeniors(CHAMPS
)(caloricexpenditu
reperweekin
kilocalories
perweek)
a
Primary:significantincreasein
PAat6months(d=0.55;P
<0.05)
with
adifference
inPA
increase
over
timeof
1159
kcalperweek
betweenthetwogroups
Other
behaviors
Interventio
n.71.4
%(n=20);
control,
92.9
%(n=26)
Matthew
setal.2007
[58]
Country:U
SA
Participants:N
=36
Meanage:
interventio
n51
years;control
57years
G1:
wait-listcontrol
G2:
face-to-face
behavioral
counselin
g(1)andtelephone
counselin
g(5)
Type:w
alking
(moderateintensity
)build
ingfrom
20to
30min
per
session,3tim
esperweekto
30–
Studydesign:2
arm
RCT
Follow-up:
6,12
weeks
Com
parisongroup:
wait-listcontrol
Outcomemeasures:Com
munity
Health
yActivities
Model
Program
forSeniors(CHAMPS
)(energyexpenditu
reMET-hper
week)
a ,accelerometer(subsample
only),21-item
diethabits
Primary:significantincreaseinself-
reported
walking
(P=0.01),MET-
hperweek(P=0.01)with
differ-
ence
of10.2
MET-hperweekof
walking
at12
weeks
betweenthe
groups
Not
reported
J Cancer Surviv (2015) 9:305–338 311

Tab
le1
(contin
ued)
Study
Participants;m
ean
age;cancer
type;tim
esincediagnosis
Interventio
n(type,intensity,
duratio
n)Studydesign
and
evaluatio
nOutcomes
Results
Retentio
n
Cancertype:
postmenopausal
breast
Timesincediagnosis:
0.9years(range
0.7–1)
interventio
n
40min
persession,5tim
esper
week
Intensity:6
sessions
over
12weeks
Duration:decreasing
frequencyover
12weeks.F
ace-to-facecounsel-
ing(30min).Telephonecounsel-
ing(10–15
min
percall)
questio
nnaire,19-item
fruitand
vegetablescreener
Other
behaviors:Nosignificant
changesto
fruitand
vegetable
consum
ptionandoveralld
ietary
habitsandno
significantchanges
werenoted,although
thedatawas
notshown
Ligibeletal.[49]
Country:U
SA
Participants:N
=121
Meanage:54
years
Cancertype:b
reast,
colonor
rectal
cancer
Timesincediagnosis:
notreported
G1:
usualcare,offeredone
consultatio
nwith
exercise
trainer
G2:
semistructuredtelephone
counselin
gandparticipant
workbook
Type:p
hysicalactivity
Intensity:1
0–11
semistructured
telephonecalls
(30–45
min
each)
over
16weeks
Duration:decreasing
frequencyover
16weeks
Studydesign:2
arm
RCT
Follow-up:
16weeks
Com
parisongroup:
usualcare
Outcomemeasures:7dayPA
recall
interview(changein
minutes
ofweeklyPA
)a
Primary:nonsignificant
increase
inphysicalactiv
ityminutes
per
weekby
40min
(P=0.13),and
MET-hperw
eekby
2h(P=0.23)
Other
behaviors
Interventio
n,79
%(n=48);
control,
85%
(n=51)
Wangetal.[52]
Country:T
aiwan
Participants:N
=72
Meanage:50
years
Cancertype:n
ewly
diagnosedbreast,
scheduledto
start
chem
otherapy
Timesincediagnosis:
Firstmeetin
gis
24hpriorto
participantsurgery
G1:
usualcare
G2:
weeklytelephonecalland
weeklyindividualface-to-face
meetin
gs(heartratemonito
r,pe-
dometer,exercisediary,androle
modelstory)
Type:h
ome-basedwalking
program
oflowto
moderateintensity
from
40to60
%,3
to5tim
esperw
eek,
atleast3
0min
persessionor
the
accumulationof
30min
perses-
sion
Intensity:1
2telephoneandface-to-
face
contactsover
6weeks
Duration:
2sessions
perweek
Studydesign:2
arm
RCT
Follow-up:
24h
priorto
day1of
chem
otherapy,
thedayof
chem
otherapy
mid-cycle,
6weeks
Com
parisongroup:
usualcare
Outcomemeasures:exercise
behavior
(Godin
leisuretim
equestio
nnaire)a
Primary:significantincreases
inphysicalactiv
ityatallfollow-up
timepointsfortheinterventio
ngroup(allP<0.05).The
differ-
ence
betweenthegroups
was
62.7,58.2,and38.8
min
atthe
second,third,and
fourth
follo
w-
up(P<0.001)
Other
behaviors
Interventio
n,86
%(n=30);
control,
86%
(n=32)
Pinto
etal.[53]
Country:U
SA
Participants:N
=46
Meanage:57
years
Cancertype:colon
orrectalcancer
Timesincediagnosis:
3.1years(SD1.6)
(intervention)
G1:
contactcontrol
groupoffered
writtenmaterialatstudy
completion
G2:
oneface-to-face
appointm
ent,
oneweeklytelephonecall(12),
weeklyPA
andcancer
survivor-
shiptip
sheet(12),feedback
letter
summarizingprogress
(4),pe-
dometer
Studydesign:2
arm
RCT
Follow-up:
3,6,
12months
Com
parisongroup:
contactcontrol,
offeredwritten
materialsat
study
completion
Outcomemeasures:7dayPA
recall
(self-reported
PA)a,C
ommunity
Health
yActivities
Model
Program
forSeniors(CHAMPS
),accelerometer
Primary:Significant
increase
inPA
at3monthsin
interventio
n(d=1.93)(P=0.02),butincreases
werenotm
aintainedat6and
12month
follo
w-ups.T
here
was
asignificantd
ifferencebetween
groups
at3monthsby
117min/
week(P<0.05)butn
otat6or
12months
Other
behaviors
Interventio
n,95
%(n=19);
control,
88%
(n=23)
312 J Cancer Surviv (2015) 9:305–338

Tab
le1
(contin
ued)
Study
Participants;m
ean
age;cancer
type;tim
esincediagnosis
Interventio
n(type,intensity,
duratio
n)Studydesign
and
evaluatio
nOutcomes
Results
Retentio
n
Type:m
oderateintensity
home-
basedPA
with
goalto
perform
moderateintensity
activ
ityaero-
bicactiv
ities
at64–76%
ofesti-
mated
maxim
umheartrate
Intensity:29contactsover12
weeks
Duration:
2contactsperweek
minim
umHatchettetal.[48]
Country:n
otexplicitly
reported.L
eadauthor:
Mississippi,U
SA
Participants:N
=85
Meanage:not
reported
Cancertype:b
reast
cancer
Timesincediagnosis:
44%
between0
and20
months;
27%
between21
and40
months;
19%
between41
and70
months
G1:
wait-listcontrol
G2:em
ailm
essages(8),accesstoan
e-counselor(experienced
exercise
physiologist)
Type:p
hysicalactivity
(emails
focusedon
changing
SCT
constructs)
Intensity:total8em
ailm
essages,
weeklyfor5weeks,then
fortnightly
fornext
6weeks
Duration:
once
perweek(5
weeks),
then
fortnightly
for6weeks
fora
totalof8
messagesover12
weeks
Studydesign:2
arm
RCT
Follow-up:
6,12
weeks
Com
parisongroup:
wait-listcontrol
Outcomemeasures:7dayPA
recalla
Primary:At12weeks,for
totaldays
ofexercise,therewas
asignificant
difference
betweenthegroups
(P<0.001)
with
theinterventio
nreporting2.05
moredays
ofexercise
comparedto
thecontrol
group(P<0.001)
Other
behaviors
Interventio
n,88.4
%(n=38);
control,
85.7
%(n=36)
Dieto
nly
Parsonsetal.[59]
Country:U
SA
Participants:N
=43
Meanage:64
years
Cancertype:p
rostate
Timesincediagnosis:
notreported—
receivingonly
activ
esurveillance
astreatm
ent
G1:
standard
care
control
G2:
telephonecounselin
gType:d
iet(7servings/day
vegeta-
bles;2
servings/day
wholegrains,
1serving/daybeans/legumes)
Intensity:totalof
13sessions
Duration:
13structured
telephone
counselin
gsessions
over
6months.Calld
urationof
25–
50min
Studydesign:2
arm
RCT
Follow-up:
6months
Com
parisongroup:
usualcare
Outcomemeasures:24
hdietary
recalla,blood
samples
(plasm
acarotenoid
concentration)
a
Primary:To
talvegetableandtomato
productintakesignificantly
increasedin
theinterventio
n(P<0.05).Nosignificantchanges
infruit,wholegrain,beans,gram
sof
fiberperday,or
fatintake
Other
behaviors
96.7
%(n=42)
Multip
lebehavior
studies
Dem
ark-Wahnefried
etal.S
TRENGTH
trial[60]
Country:U
SA
Participants:n
=90
Meanage:
41.8
years
Cancertype:
prem
enopausal
breast
Timesincediagnosis:
notreported,
interventionoccurs
duringchem
otherapy
G1:
attentioncontrol(calcium-rich
diet)
G2:
calcium-richdietandexercise
(telephone
counselin
gcontacts
(14),exerciseequipm
ent,heart
ratemonito
r,workbook,video-
tape)
G3:
calcium-richdietandexercise
andhigh
fruitand
vegetable,low-
Studydesign:3
arm
RCT
Follow-up:
3,6months
Com
parisongroup:
attentioncontrol
Outcomemeasures:%
body
fat
(wholebody
DXAscans)a ,144-
item
diethistoryquestio
nnaire,
LongitudinalS
tudy
PhysicalAc-
tivity
Questionnaire
(MET-h/
week),accelerom
eter
(kcal/d
ay)
Primary:Consistentincreases
forall
measuresof
adiposity
were
observed
overtim
eandam
ongall
groups.G
3hadsignificantly
lower
scores
for%
ofbody
fat
(minus
thetrunk)
(P<0.05)
Other
behaviors:no
significant
changesin
physicalactiv
ityover
timeor
betweenstudyarms
91.2
%(n=82)
J Cancer Surviv (2015) 9:305–338 313

Tab
le1
(contin
ued)
Study
Participants;m
ean
age;cancer
type;tim
esincediagnosis
Interventio
n(type,intensity,
duratio
n)Studydesign
and
evaluatio
nOutcomes
Results
Retentio
n
fatd
iet(resourcesprovided
toG2
+encouraged
tomaintainhigh
fruitand
vegetable,low-fatdietto
reduce
energy
density
ofthediet).
Goallevelsof
<20
%of
energy
from
fat,and>5servings
fruitand
vegetables
perday
Type:d
iet(high
fruitand
vegetable,
lowfat)andexercise
(aerobicand
strength
training)(aerobic
exercise
>3tim
es/week,
strength
training
everyotherday)
Intensity:m
ultip
lecontacts(atleast
fortnightly
)Duration:
14telephonecounselin
gcontacts(10–30
min)over
6months
There
wereno
differencesin
energy
intake
amongstudyarms.
How
ever,G
3exhibitedhigher
fruitand
vegetableintakes(by1.7
serves)andlower
fatintakes
(reductio
nof
5.2%
calories
from
fat)at6months
Cam
pbelletal.[61];
Reedy
etal.[111];
Koetal.[112]
Country:U
SA
Participants:N
=922
(n=266colorectal
cancer
survivors)
Meanage:66.5
years
Cancertype:
colorectalcancer
Timesincediagnosis:
7.6%:lessthan
1year
ago;
29%:
1–2yearsago;
57%:2
–5years
ago
G1:
generichealth
education(2
mailin
gs)andtailo
red-print
newsletters(4)afterfollo
w-up
completed
G2:
4tailo
red-printn
ewsletters
G3:
4telephonecalls
(20min
duratio
n)G4:
4tailo
red-printn
ewsletters+4
telephonecalls
(20min
duratio
n)Type:d
iet,physicalactiv
ity,
colorectalcancer
screening
Intensity:m
ultip
leexposure
(less
than
monthly)
Duration:
1year
Studydesign:4
arm
RCT.
2×2
design—
stratifiedby
colorectalcancer
and
noncolorectal
cancer
status
Follow-up:
6,12
months
Com
parisongroup:
usualcarewith
tailo
red
newslettersat
study
completion
Outcomemeasures:modifiedBlock
Food
FrequencyQuestionnaire
(36item)a,2-item
fruitand
vege-
tablescreeningquestio
nsa ,modi-
fied
7dayPA
recall(m
oderateto
vigorous
PAscore)
Primary:There
wereno
significant
changesin
fruitand
vegetable
consum
ptionin
colorectalcancer
survivors,usingtheFo
odFrequencyQuestionnaire.T
here
was
anonsignificant
increase
inG2interventio
nby
ameanof
1.0
serves/day
Using
the2-item
screeningques-
tions,all3interventio
ngroups
show
edstatistically
significant
increasesam
ongcolorectalcancer
survivors
Other
behaviors:Nosignificant
change
onphysicalactiv
ity,and
participantsin
all4
groups
were
less
activ
eatfollo
w-upcompared
tobaselin
e
79.7
%(n=735)
from
total
sample
Von
Gruenigen
etal.
[65,73]
Country:U
SA
Participants:N
=45
Meanage:55
years
Cancertype:
endometrialcancer
Timesincediagnosis:
20.6
months
median
(intervention)
G1:
standard
care
G2:
face-to-face
groupsessions,
telephone,or
writtennewsletters
Type:w
eightloss,PA
,eating
behaviors
Intensity:w
eeklycontact
Duration:
totalo
f21
sessions
offace-to-face
(11),telephone
(5),
Studydesign:2
arm
RCT
Follow-up:
3,6,
12months
Com
parisongroup:
usualcare
Outcomemeasures:weightchange
(kilo
gram
s)—measureda,PA
usingLeisure
ScoreIndexof
the
Godin
leisuretim
eexercise
questio
nnaire
(frequency
per
weekon
Leisure
Score
Indexfor
mild
,moderate,strenuousPA
),3dayfood
record
(vitamin
Cand
Primary:The
meandifference
inweightchangebetweenthetwo
groups
was
−4.9
kg(P=0.018)
at12
months.The
controlgroup
did
notd
emonstrateanysignificant
changesin
weightfrom
baselin
e.Meanweightchangeexpressedas
apercentage
from
baselin
eto
Interventio
n,78
%(n=18);
control,
90%
(n=20)
314 J Cancer Surviv (2015) 9:305–338

Tab
le1
(contin
ued)
Study
Participants;m
ean
age;cancer
type;tim
esincediagnosis
Interventio
n(type,intensity,
duratio
n)Studydesign
and
evaluatio
nOutcomes
Results
Retentio
n
writtennewsletters(5)over
6months
folateas
markerof
fruitand
vegetableintake,kilo
calories)
12monthswas
−3.1
%in
the
interventio
ncomparedto
1.0%
inthecontrolg
roup
(mean
difference
−4.1
%,P
=0.020)
Other
behaviors:At1
2months,
therewas
asignificantd
ifference
inLeisure
Score
Indexbetween
groups
(meangroupdifference
17.8,P
=0.002)
Therewereno
significantchanges
indiet.T
heinterventio
ngrouphada
lower
energy
intake
(kilo
calories)
butw
asnotstatistically
signifi-
cant
from
thecontrolg
roup
Von
Gruenigen
etal.
[67]
Country:U
SA
Participants:N
=75
Meanage:58.0
years
Cancertype:
endometrialcancer
Timesincediagnosis:
20.7
months
G1:
standard
care
G2:
face-to-face
groupsessions,in-
dividualphysiciancounselin
g,newsletters,telephone,and
contactw
ithregistered
dietician.
Receivedpedometer,heartrate
monito
r,hand
andankleweights
Type:w
eightloss,PA
,resistance
exercises,dietquality
Intensity:w
eekly(10),then
biweekly(6)groupsessions.
Physiciancounselin
gat3,6,and
12months
Duration:
minim
umof
19contacts
for12
months
Studydesign:2
arm
RCT
Follow-up:
3,6,
12months
Com
parisongroup:
standard
care
received
one
inform
ation
brochure
Outcomemeasures:measured
weightaandheight,w
aist
circum
ference,hipcircum
ference,
Godin
leisuretim
eexercise
questio
nnaire,2
×24
hdietary
recalls,pedom
eter
step
counts
Primary:significantd
ifferences
for
weightchangefrom
baselin
eto3,
6,and12
months(P<0.001).
Mean(95%
CI)difference
betweengroups
at6monthswas
−4.4
kg[−5.3,−3
.5],P<0.001
andat12
monthswas
−4.6
kg[−5.8,−3
.5],P<0.001.Mean
percentw
eightchangein
the
interventio
nwas
−4.1
%as
comparedto−0
.8%
incontrolsat
6monthsand−3
.0%
and+
1.4%
at12
months
Other
behaviors:mean(95%
CI)
difference
inchange
at6months
was
100min
perweek[6,94],
P=0.038andat12
monthswas
89min
perweek[14,163],
P=0.020.Meanchange
inpedometer
step
countsfrom
baselin
eto
6monthswas
2353
intheinterventio
ngroupversus
−9.4stepsperdayin
theusual
care
group(differenceof
[95%
CI]of
2362
(494,4230);
P=0.015)
Meandifference
inchange
intotal
fruitand
vegetableintake
was
0.91
servings
perday(P<0.001)
78.7
%(n=59).
Interven-
tion,
85.4
%(n=35);
control,
70.6
%(n=24)
J Cancer Surviv (2015) 9:305–338 315

Tab
le1
(contin
ued)
Study
Participants;m
ean
age;cancer
type;tim
esincediagnosis
Interventio
n(type,intensity,
duratio
n)Studydesign
and
evaluatio
nOutcomes
Results
Retentio
n
at6monthsand0.92
(P<0.001)
at12
months.Meandifference
inchange
inkilocalories
between
groups
was
−228.8,−
217.8,and
−187.2
kcalat3,6,and
12months(P<0.001)
Dem
ark-Wahnefried
etal.[62];Dem
ark-
Wahnefriedetal.[63];
Mosheretal.[78];
Wilk
insonetal.[113];
Christy
etal.[74].—
FRESHST
ART
Country:U
SA
Participants:N
=543
Meanage:57
years
Cancertype:b
reast,
prostate
Timesincediagnosis:
3.83
months(SD
2.74)
G1:
attentioncontrol
G2:
tailo
red-printn
ewslettersand
workbook
Type:d
ietand
physicalactiv
ityIntensity:initialw
orkbookand(6)
tailo
rednewslettersevery7–
9weeks
for10
months
Duration:
totalo
f7contactsfor
10months
Studydesign:2
arm
RCT
Follow-up:
1year,
2years
Com
parisongroup:
attentioncontrol
Outcomemeasures:numberof
goal
behaviorspracticed
(percentage
adoptinggoalbehavior
inatleast
2areas)a ,7dayPA
recall,
diet
historyquestio
nnaire,D
iet
QualityIndexmeanscore
Primary:both
armssignificantly
improved
theirlifestylebehaviors
(P<0.05).Significant
difference
betweengroups
inpracticeof
2or
moregoalbehaviors(P<0.0001)
(16%
greaterin
interventio
nparticipants)
Other
behaviors:significant
differencesbetweengroups
inexercise
minutes
perweek
(P=0.02)(+20
min/week
interventio
n),fruitandvegetables
perday(P=0.01)(+0.5servings
interventio
n),totalfat(P<0.0001)
(−2.3%
interventio
n),saturated
fat(P<0.0001)(−1.0%)
Interventio
n,93.4
%(n=253);
control,
97.8
%(n=266)
Djuricetal.[64]
Country:U
SA
Participants:N
=40
Meanage:52
years
Cancertype:b
reast
Timesincediagnosis:
notreported
although
either
scheduledforor
startin
gchem
otherapy
inthenext
2weeks
G1:
controlg
roup
received
written
dietandphysicalactiv
itymaterialsandpedometer(sam
eas
G2),and
bimonthly
study
newsletters
G2:writtendietandphysicalactiv
itymaterials,pedom
eter,telephone
counselin
g(byadieticiantrained
inmotivationalinterview
ing)
Type:h
ighfruitand
vegetable,low-
fatd
iet,weightcontrol,30min
perdayof
moderate-to-vigorous
PAIntensity:m
ultip
lecontacts(atleast
monthly)
Duration:
totalo
f19
calls,w
ritten
materials,and
pedometer,over
12months
Studydesign:2
arm
RCT
Follow-up:
6,12
months
Com
parisongroup:
attentioncontrol
with
written
materialsand
pedometer
(sam
eas
the
interventio
ngroup)
Outcomemeasures:measured
weightand
body
fata,19-item
fruitand
vegetablescreener,17-
item
percentage
ofenergy
from
fat,24
hdietrecall,
Wom
en’s
Health
Initiativevalid
ated
PAquestio
nnaire
Primary:thepercentage
ofbody
fat
increasedby
1.2%
inthecontrol
groupanddecreasedby
0.07
%in
theinterventio
ngroup.Weight
decreasedby
0.8kg
at12
months
Other
behaviors:To
talp
hysical
activ
ityincreasedto
ameanof
364min
perweekandmoderate/
vigorous
activ
ityincreasedto
ameanof
315min
perweekat
12months,slightly
belowthe
targetof
350min
perweekof
moderate/vigorous
activ
ity.F
orfruitand
vegetableintakesfrom
unannouncedrecalls,the
number
ofservings/day
increasedonly
inthetelephonearm,and
themean
reported
intake
at12
monthswas
justabovetheminim
uminter-
ventiongoalof7servings
perd
ay,
notcountingpotatoes.T
here
was
Interventio
n.65
%(n=13);
control.
85%
(n=17)
316 J Cancer Surviv (2015) 9:305–338

Tab
le1
(contin
ued)
Study
Participants;m
ean
age;cancer
type;tim
esincediagnosis
Interventio
n(type,intensity,
duratio
n)Studydesign
and
evaluatio
nOutcomes
Results
Retentio
n
asignificantincreasein
fruitand
vegetableservings
by3.1serves
from
baselin
eto
12months
Djuricetal.[66]
Country:U
SA
Participants:N
=48
Meanage:mean:
51.7
years
Cancertype:b
reast
Timesincediagnosis:
notreported—
although
needed
tohave
been
diagnosedwith
inthepast4years
G1:
standard
care
G2:
weightw
atchers(freecoupons
toattend
each
week)
(52)
G3:
telephonecounselin
gby
dietician(24calls),andmailed
writtenmaterial(12)
G4:
weightw
atchersfree
coupons
(52),dietician-deliv
ered
tele-
phonecounselin
g(24),m
ailed
writtenmaterial(12)
Type:w
eightlossgoal(10%
baselin
eweighto
ver6months)
bydecreasing
energy
andfat
intake,and
30–45min
moderate
activ
itymostd
aysof
theweek
Intensity:m
ultip
lecontacts
(minim
ummonthly)
Duration:To
talcontactsvaried
from
36(G
3),52(G
2),88(G
4),in
12month
interventio
n
Studydesign:4
arm
RCT
Follow-up:
3,6,
12months
Com
parisongroup:
usualcare
Outcomemeasures:weighta,3
day
food
record,physicalactivity
logs
(self-reported
intentional
exercise)
Primary:significantd
ifferencein
weightlossat12
monthsfor
participantsin
G3(m
ean8kg
loss)andG4(m
ean9.4kg
loss).
Therewas
anonsignificantlossof
2.5kg
inG2,andan
increase
of0.85
kgin
G1(control
group)
Other
behaviors:nonsignificant
decreasesin
energy
intake
(kilo
calories
perday)
ineach
ofthethreeinterventio
ngroups
(by
447–616kcalperday),and
nonsignificant
decrease
infat
intake
(%of
energy
from
fat)in
the3interventio
ngroups
(by2–
11%)at12
months.The
control
groupenergy
intake
remainedthe
same(decreaseof
126kcalper
day),and
increasedfatintake(by
7%)
There
was
nodifference
inweight
loss
betweenwom
enwho
self-
reported
intentionalexercise(be-
yond
daily
activ
ities),andthose
who
reported
nointentionalac-
tivities
ineach
studygroup
81.3
%(n=39)
Ggroup
aDenotes
prim
aryoutcom
e
J Cancer Surviv (2015) 9:305–338 317

[57, 58, 67]. There was no change to the impact of interven-tions on total PA (SMD=0.34 [0.24, 0.44]). However, therewas an increase in heterogeneity (χ2=30.31, df=16 [P=0.02];I2=47 %).
Diet-only trial
One trial reported dietary outcomes only [59]. The trialtargeted men receiving active surveillance for prostate cancer,with a dietary counseling intervention delivered by telephoneover 6 months. Men completed self-report measures andprovided blood samples for objective assessment of caroten-oid intake at completion of the intervention. Retention ratewas 97 %, with significant increases to vegetable consump-tion. There was no change to fruit, whole grains, beans, or fatconsumption [59].
Multiple behavior trials
Seven studies focused on multiple behaviors (PA and diet)[60, 61, 63–66].
Participants
A total of 1107 participants were randomized (range 40–543).Three studies recruited newly diagnosed patients [60, 62–64],and patients were diagnosed with breast [60, 62–64, 66],prostate [62, 63], colorectal [61], or endometrial [65, 67, 73]cancer. Only three trials reported time since diagnosis, whichvaried from a mean of 3.8 months [63], to a mean of20.6 months [65, 67]. In two trials, participants were sched-uled to start chemotherapy [60, 64]. Three trials were aimedexclusively at overweight or obese breast [66] or endometrialcancer survivors [65, 67], with the aim of achieving weightloss through changing PA and diet behaviors. Two trialsreported PA [66] or PA and diet [64] outcomes for the purposeof intervention adherence.
Three trials had a usual care control group [65–67], and oneused a usual care comparison group with tailored newslettersat study completion [61]. Two had attention control groups[60, 63], and one used attention control with the same writtenmaterials and pedometer as the intervention group [64].
Intervention characteristics
All of the interventions were home-based and did not includeany supervised PA. All trials targeted both PA and diet behav-iors. Four of these targeted weight loss [60, 64–67], or pre-vention of weight gain [60, 64–66], through changing PA anddiet behaviors [60, 64–66]. Four trials were aimed at increas-ing fruit and vegetables and reducing fat [60, 61, 63, 65, 67],one targeted only energy and fat [66], two included bothaerobic and strength activity [60, 67], two targeted moderate
or moderate-to-vigorous PA [64, 66], and the remaining threetargeted PA [61, 63, 65].
Interventions were delivered using telephone counseling[60, 61, 64–67], written materials [60–62, 64, 65, 67], or faceto face [65–67]. Most trials used multiple delivery modes,with one that used tailored newsletters [63]. Interventionduration was 6 months [60, 65], 9 months [61], 10 months[62], or 12 months [64, 66, 67]. The average number ofcontacts was 27 (ranging from 4 [61] to 88 [66]). Studiesreported high adherence with all intervention componentsranging from 73 to 100 %, with no difference between deliv-ery modes.
Outcome assessment
Objectively assessed weight or body fat was reported as theprimary outcome in five studies [60, 64–67]. All trialsassessed diet using a range of self-reported measures [60,61, 63–67]. Only one trial used an objective measure of PA(accelerometer) [60], and the remaining trials assessed PA byself-report only [61, 62, 64–67].
Follow-up periods were 6 months in one study [60],12 months [61, 64–67], or 2 years [62]. However, only twostudies reported follow-up beyond postintervention time point[63, 65]. At 12 months, one trial reported significant differ-ences in PA levels, with no difference in diet [65]. After 2 yearsof follow-up, both study groups hadmaintained increased fruitand vegetable consumption, decreased saturated fat, and im-proved overall diet quality [74]. The mean retention rate was84 % (range 75 % [64] to 96 %[63]). No adverse events werereported in two studies [60, 61, 63, 64]. In two studies thatreported adverse events, 10–13% (n=4; n=74) [63, 64] of thetotal sample reported serious adverse events that led towithdrawal.
Five of the seven studies [60, 61, 63, 64, 67] reportedsignificant improvements in one or more aspects of diet qual-ity, as assessed by self-report, over the medium to long term(6 months to 2 years). The remaining two studies reportednonsignificant decreases in energy [65, 66] and fat intake inthe intervention groups [66]. Inconsistent improvements infruit and vegetable consumption were reported using a two-item screening question; however, these improvements werenot found when using the comprehensive Food FrequencyQuestionnaire results [61]. At 6 months, significant improve-ments were reported for vegetables [60], fruit [60], combinedfruit and vegetables [67], and decreased fat [60]; however,there was no change for energy [60]. At 12months, significantimprovements were reported for fruit and vegetables, by amean of 0.5 [63], 0.9 [67] to 3.1 serves per day [64]. Therewas also a significant reduction by 2.3 % in the proportion ofenergy from fat [63], which is supported by similar reductionsin other trials [64–66]. There were two trials that reported noeffect on PA at 3, 6, or 12 months [60, 61]. At 12 months, four
318 J Cancer Surviv (2015) 9:305–338

trials reported improvements in PA, ranging from 20 min perweek (P=0.02) [63] to 89 min per week [67] to 117 min perweek [64], and a difference of 17.8 (P=0.002) on the LeisureScore Index [65].
Theoretical framework
Recent development of behavior change taxonomies [28, 75,76] has encouraged consistent reporting of behavior changetechniques. We have mapped the SCT constructs to identifythe behavior change techniques that align with each construct,using the taxonomy designed to change PA and eating behav-iors [75] in Table 3.
Self-efficacy was the most commonly assessed construct[48–50, 52, 55–57], with four PA studies that assessed otherSCTconstructs [48, 51, 53, 55] (Table 4). Two studies [52, 57]reported that the study was based on Bandura’s self-efficacytheory, and the only construct operationalized was self-effica-cy. Four PA interventions that used telephone or face-to-facecounseling reported that the counseling principles were basedon SCT [49, 51, 53, 58]. Five studies reported that the studywas based on SCT and the transtheoretical model (TTM), orelements of TTM, such as stages of change [50, 53, 57, 61,
62]. Stage of change was assessed in four studies [50, 51, 53,57] with reference to both the TTM and social cognitivetheories. However, one trial assessed stage of change, despitenot providing any reference to TTM or rationale for why stageof change was assessed [51]. Most studies reported using goalsetting [48, 51–54, 56–58, 77]; however, few specificallyreported action plans [54] or review of goals [56–58]. Themost common strategy to increase self-efficacy was to providea pedometer [49, 50, 52, 53, 56, 57] and/or a log sheet for self-monitoring of PA behavior [49–53]. Social support or socialcomparison was the most common outcome expectancytargeted [48, 51, 54, 56, 58], and two trials reported strategiestargeting environment [51, 54] or relapse prevention [49, 53].Five trials incorporated identification and discussion of bar-riers and how to overcome them [50, 51, 53, 57, 58], but onlyone prompted a focus on past successful strategies [49].
In PA-only trials, improvements in self-efficacy were asso-ciated with increased PA in three studies [49, 50, 52]. Moder-ation analyses identified that intervention participants withhigh self-efficacy increased their PA levels faster over the6 month assessment period compared to intervention partici-pants with low self-efficacy [57]. Mediation analyses identi-fied that improvements in barrier interference and barrier self-
Table 2 Risk of bias (assessed using McMaster Quality Assessment Tool) [47]
Study (a)Selectionbias
(b)Studydesign
(c)Confounders
(d)Blinding
(e) Data collectionmethod
(f)Withdrawalsand dropouts
Globalrating
PA-only studies
Short et al. [54, 55] Weak Strong Strong Moderate Strong Strong Moderate
Valle et al. [56] Weak Strong Strong Moderate Strong Moderate Moderate
Rogers et al. [51, 68] Moderate Strong Moderate Moderate Strong Strong Strong
Pinto et al. [50, 71, 72] Moderate Strong Strong Moderate Strong Strong Strong
Bennett et al. [57] Weak Strong Strong Weak Strong Moderate Weak
Matthews et al. [58] Weak Strong Strong Weak Moderate Weak Weak
Ligibel et al. [49] Moderate Strong Strong Moderate Strong Moderate Strong
Wang et al. [52] Moderate Strong Strong Moderate Strong Strong Strong
Pinto et al. [53] Weak Strong Strong Moderate Strong Strong Moderate
Hatchett et al. [48] Moderate Strong Strong Moderate Strong Strong Strong
Diet only
Parsons et al. [59] Moderate Strong Weak Moderate Strong Strong Moderate
Multiple behavior studies
Demark-Wahnefried et al.—STRENGTH [60]
Strong Strong Strong Moderate Strong Strong Strong
Campbell et al. [61] Weak Strong Strong Moderate Strong Strong Moderate
Von Gruenigen et al. [65, 73] Weak Strong Strong Moderate Strong Moderate Moderate
Von Gruenigen et al. [67] Weak Strong Strong Weak Strong Moderate Weak
Demark-Wahnefried et al.—FRESH START[62, 63, 78]
Weak Strong Strong Moderate Strong Strong Moderate
Djuric et al. [64] Weak Strong Strong Moderate Strong Moderate Moderate
Djuric et al. [66] Weak Strong Weak Moderate Strong Strong Weak
J Cancer Surviv (2015) 9:305–338 319

efficacymediated 39 and 19% of the intervention effect on PAmaintenance 3 months after the intervention [70]. There wereno significant changes in decisional balance pros, cons, orexperiential processes of change [71, 72], or task self-efficacy,social support, outcome expectations, or fear of exercise [70].Two trials assessed but did not report results for self-regula-tion, outcome expectancy values, exercise self-efficacy, exer-cise role identity, behavioral capability, or social support [48,
54, 55]. Intervention effects on stage of change results weremixed, with one trial that reported a medium-to-large effect[51], one reported significant postintervention improvementsthat declined over subsequent follow-ups [53], and one re-ported no effect on stage of change [71].
The diet-only trial reported that the telephone counselingprotocol “used strategies adopted from SCT”; however, nofurther detail was provided [59]. In multiple behavior studies,
Fig. 2 Meta-analysis examiningthe effects of SCT-based inter-ventions on physical activity im-mediately postintervention
Table 3 SCT constructs mappedto behavior change techniquesusing the CALO-RE taxonomy[75]
SCT construct Behavior change techniquenumber
Behavior change technique description
Knowledge 1 Provide information on consequences of behavior ingeneral
2 Provide information on consequences of behavior to theindividual
Self-efficacy 16 Prompt self-monitoring of behavior
17 Prompt self-monitoring of behavioral outcome
21 Provide instruction on how to perform the behavior
22 Model/demonstrate the behavior
26 Prompt practice
27 Use of follow-up prompts
Goals 5 Goal setting (behavior)
6 Goal setting (outcome)
7 Action planning
10 Prompt review of behavioral goals
11 Prompt review of outcome goals
Outcomeexpectations
16 Prompt self-monitoring of behavior
17 Prompt self-monitoring of behavioral outcome
23 Teach to use prompts/cues
24 Environmental restructuring
28 Facilitate social comparison
29 Plan social support/social change
31 Prompt anticipated regret
35 Relapse prevention/coping planning
Facilitators/impediments
8 Barrier identification/problem solving
18 Prompting focus on past success
29 Plan social support/social change
320 J Cancer Surviv (2015) 9:305–338

Tab
le4
Socialcognitive
theory
constructsoperationalized
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
PA-onlytrials
Shortetal.
[54,55]
One
interventiongroup(G
2)received
computer-tailo
red
newslettersbasedon
SCT
G3(targeted-print)interventio
nreceived
aTheoryof
Planned
Behavior-basedbooklet(previ-
ouslyevaluated)
Knowledgeof
PAguidelines,
beneficialoutcom
esof
PA,action
planning,feedbackon
PAperformance,socialsupport,role
modeling,physicalenvironm
ent
G2:tailored-printnew
sletters(n=3)
tai-
loredusinginform
ationfrom
individ-
ualassessm
entsatbaseline,and“up-
datecards”
assessingPA
andgoal
setting
behavior
overthelastmonth.
New
sletter1strategies
wereadvice
formeetingthePA
guidelines
for
cancersurvivors,inform
ationabout
thebeneficialoutcomesofPA
,advice
onexercising
safely,and
actionplan-
ning.N
ewsletter2strategies
were
expertadvice
from
abehaviorchange
expert,feedback
onPA
performance,
atestimonial,advice
onenhancing
socialsupport,andactionplanning.
New
sletter3containedexpertadvice
from
anexercise
physiologist,feed-
back
onPA
performance,tipson
changing
thePA
environm
ent,infor-
mationon
gainingfurthersupport,
andactionplanning
Outcomeexpectations
(11items);
outcom
eexpectancies
(1item);task
self-efficacy(7
items);b
arrier
self-
efficacy
(17items);b
ehavioralca-
pability(6
items);socialsupport
(15items);p
erceived
built
environ-
ment(7items);self-regulatio
n(12
items);actionplanning
(4items)
Not
reported
Valleetal.[56]
SCTwith
focuson
strategies
toenhanceself-efficacy,
behavioralcapability,self-
monito
ring,and
socialsupport
Socialsupport,problem
solving,self-
monito
ring,m
aintaining
PA,goal
setting,personalized
feedback
FITNETinterventio
ngoalwas
tomeet
PArecommendatio
nforcancer
survivors(150
min
moderate
intensity
PA/week).B
ehavioral
capabilitywas
operationalized
throughlin
ksto
publicly
available
websitesrelatedtoPA
and/orcancer
survivorship,12weeklyFacebook
messageswith
expanded
behavioral
lessonson
PAtopics
andbehavioral
strategies;self-efficacy
was
opera-
tionalized
bypedometer
which
provides
feedback
ondaily
walk-
ing,websitewith
weeklygoalset-
tingandchartsprovidingfeedback
onperformance
relativ
eto
weekly
exercise
goal,previousweeks
and
overallinterventiongoal;self-
monito
ring
was
operationalized
with
apedometer
tomonito
rsteps,
websitewith
diaryto
record
walk-
ingstepsandPA
type,duration,and
intensity
;and
socialsupportw
asoperationalized
throughthe
Facebookgroupwith
moderated
Nonereported
J Cancer Surviv (2015) 9:305–338 321

Tab
le4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
discussion
prom
ptsto
encourage
support,lin
ks,and
weeklyre-
minders
Rogersetal.
[51,68–70]
SCTself-efficacy,em
otional
coping,reciprocaldeterminism,
perceivedbarriers,outcome
expectations,behavioral
capability,goalsetting,
environm
ent,observational
learning,and
self-control
Socialsupport,exercise
barriers,self-
efficacy,goalsetting,environm
ent,
self-m
onito
ring,barrier
self-
efficacy,taskself-efficacy,barrier
interference,outcomeexpectations,
value(outcomeim
portance),
enjoym
ent,fear
ofexercise,role
model,exercisepartner
Participantsattended
6discussion
groupsessions
with
aclinical
psychologistwho
encouraged
socialsupport,provided
breast
cancer
survivor
exercise
role
models,andcoveredthefollo
wing
topics:journaling,tim
emanagem
ent,stress
managem
ent,
dealingwith
exercise
barriers,and
behavior
modification.The
specific
SCTconstructsaddressedby
the
groupsessions
included
self-
efficacy,emotionalcoping,
reciprocaldeterm
inism,perceived
barriers,outcomeexpectations,
behavioralcapability,goalsetting,
environm
ent,observational
observationallearning,andself-
control.Participantsalso
attended
12individualsupervised
exercise
and3individual“face-to-face”
updatecounselingsessions
with
anexercise
specialistthattapered
toa
home-basedprogram
bytheendof
theinterventio
n.The
specificSC
Tconstructsaddressedby
theindi-
vidualsessions
included
self-effi-
cacy,outcomeexpectations,behav-
ioralcapability,perceived
barriers,
andgoalsetting
with
self-m
onito
r-ing.To
furtherenhanceself-m
oni-
toring,participantswereencour-
aged
to“convert”theminutes
spent
inPA
recorded
ontheirweeklyex-
ercise
logs
into
“miles”
(i.e.,
1min
=2miles),w
hich
were
graphedon
amap
PAstageof
change
(5items);b
arrier
self-efficacy(9
items);taskself-
efficacy
(4items);b
arrier
interfer-
ence
(21items);socialsupport(4
items),positive
expectations
(14
items);n
egativeoutcom
eexpecta-
tions
(3items);fearof
exercise
(1item);PA
enjoym
ent(1item);ex-
ercise
rolemodels(3
items);exer-
cise
partner(1
item)
Medium-to-largeeffectsize
increase
was
notedforstageof
change
(meandifference=0.95;9
5%
CI=
0.75–1.83;
d=0.71;P
=0.034).
Com
paredwith
usualcare,the
interventio
ngroupreported
lower
barriersinterference
(mean
difference=−7
.8;P
=0.04)and
greaterPA
enjoym
ent(mean
difference=0.7;
P=0.06).
Statistically
nonsignificant
small-
to-m
edium
positiv
eeffectsize
in-
creaseswerenotedforbarrierself-
efficacy,fam
ilysocialsupport,and
totalsocialsupport,w
hilepositive
outcom
eexpectations,negative
outcom
eexpectations,and
negative
outcom
evalues
demonstrated
small-to-m
edium
negativ
eeffect
size
changesfortheintervention
comparedto
theusualcaregroup.
Littleto
nochange
was
notedfor
task
self-efficacy,friend
socialsup-
port,importance
ofpositiv
eout-
comes,fearof
exercise,exercise
partner,androlemodels
Mediatio
n:Barriersinterference
mediated39
%(P=0.004)
ofthe
interventio
neffecton
PA3months
postinterventio
n.PA
enjoym
ent
was
nota
significantm
ediator.
Reducingbarriersto
PApartially
explainedinterventio
neffect
Pintoetal.[50,
71,72]
Interventio
nbasedon
transtheoreticalmodel(TTM)
andSC
T.Pintoetal.2005[50]
statethatinterventio
nisbased
onTTM
only
TTM:counselingtailo
redto
participant’s
stageof
readinessto
change,S
CT:self-efficacy,goals,
PAbarriers
EachPA
participantreceivedin-person
instructions
onhowto
exercise
ata
moderateintensity
level,howto
monito
rheartrate,andhowto
warm
upbefore
exercise
andcool
downafterexercise.T
heywere
givenhomelogs
tomonitorPA
Decisionalb
alance
pros
andcons
(16
items),exerciseself-efficacy(5
items),stage
ofmotivationalreadi-
ness
forPA
(4items)
Nosignificantchanges
indecisional
balancepros,decisionalb
alance
cons,orstageof
change.B
aseline
self-efficacywas
asignificantp
osi-
tivepredictorof
meanminutes
ofweeklyexercise
(B=79.46min;
P=0.004),m
eanpedometer
steps
322 J Cancer Surviv (2015) 9:305–338

Tab
le4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
participationandapedometer.E
ach
participantreceivedaweeklytele-
phonecallover
12weeks
from
re-
search
staffto
monitorPA
partici-
patio
n,identifyrelevant
health
problems,problem
solveanybar-
riersto
PA,and
reinforcepartici-
pantsfortheirefforts.Finally,a
feedback
lettersummarizingthe
participant’s
progress
(e.g.,number
ofPA
sessions,average
durationof
each
session,andtheparticipant’s
barriersto
PAandsuggestions
toovercomethem
)was
sent
tothe
patient
atweeks
2,4,8,and12.A
ttheweeklycalls,subjectsreported
onthePA
recorded
onhomelogs,
andthey
received
feedback
perweek(B=2636.9steps;
P=0.0006)
Bennettetal.
[57]
TTM
andperceivedself-efficacy
from
SCT
Self-efficacy,goals
Duringtheinitialcounselingsession,
theparticipantw
asencouraged
toidentifybarriersto
engaging
inregularexercise,and
thePA
counselorandtheparticipant
workedtogethertodevelopideasto
overcomebarriers.A
goalof
30min
ofmoderateintensity
plannedPA
onmostd
aysof
the
week,butsom
eparticipantsstarted
with
moremodestg
oals.E
ach
interventionparticipantreceiveda
pedometer
andwas
show
nhowto
useitas
amotivator
forwalking
exercise,but
participantswerenot
required
towalkifthey
preferred
anotherform
ofmoderateintensity
exercise.T
elephone
calls
were
plannedto
lastabout2
0min,and
theconversatio
nincluded
motivationalstrategiesdirected
atsolvingproblems,offering
encouragem
ent,andreform
ulating
goals,ifneeded
Self-efficacyforregularPA
(6items);
stageof
change
forexercise
(6items:baselineonly)
Self-efficacywas
tested
asamoderator
ofinterventioneffects.Individuals
with
high
self-efficacyin
theinter-
ventionincreasedPA
levelsfaster
over
6monthsthan
lowself-
efficacy
individualsin
theinter-
ventiongroup.In
thecontrolgroup,
self-efficacyhadno
impacton
PAlevels(B=121.35;P
<0.05)
Matthew
setal.
[58]
Structured
behavioralcounseling
grounded
inSC
T(using
semistructuredscript)
Goals,PAenjoym
ent,positiv
ereinforcem
ent,self-rew
ard,
personalmotivation,barriers,
problem
solving,socialsupport,
The
initialcounselingsession
emphasized
goalsetting
andPA
safety.S
ubsequentcounselingcalls
weredesigned
tomonitor
None
J Cancer Surviv (2015) 9:305–338 323

Tab
le4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
goalreview
,self-efficacy,self-
monito
ring
participantsafetyandenhance
adherencethroughstructured
behavioralcounselin
gthatwas
grounded
inSC
T.Asemistructured
scriptwas
used
bythecounselorsin
each
ofthecalls
toinitiate
discussion
with
participantsabout
theirexperience
inmeetin
g(ornot)
theirw
alking
goalsthatwereagreed
upon
attheprevious
intervention
contact.Taking
theircues
from
the
inform
ationprovided
bythe
participantsin
theseconversatio
ns,
thestaffthen
delivered
appropriate
interventio
nmessages.When
participantsmettheirgoals,
individualized
positive
reinforcem
entw
asprovided
inthe
form
ofadiscussion
ofenjoym
ent
associated
with
beingactiv
eand
relevantself-rew
ards.D
iscussionof
personalmotivations
thathelped
theindividualmeettheirwalking
goalswas
also
emphasized.In
contrast,iftheparticipantd
idnot
meettheirwalking
goals,the
conversatio
nnaturally
ledto
the
barriersparticipantsexperiencedin
theperiod,and
thecounselor
initiated
aconversatio
nabout
problem
solvingstrategies
that
might
help
overcomeanticipated
barriersin
thecomingweek(s).
Whenappropriate,participants
wereencouraged
toelicitsocial
supportfrom
theirfamily
and
friendsthatmight
help
them
meet
theirgoals(e.g.,awalking
partner,
helpwith
othertim
ecommitm
ents).
Callswereendedwith
arecapofthe
conversatio
n(bythecounselor)that
included
areview
oftheagreed
upon
goalforthenext
week(s),a
review
ofthebehavioralissues
that
werediscussedduring
thecall(e.g.,
positivereinforcem
entsor
barriers/
problemsolving),and
anindicatio
n
324 J Cancer Surviv (2015) 9:305–338

Tab
le4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
ofwhenthenext
counselin
gcall
would
occur
Ligibeletal.
[49]
SCTandclient-centered
counseling
Goalsettin
g,self-efficacy,self-
monito
ring
Initialcalls
focusedon
goalsetting
and
performanceassessmentsoastobuild
self-efficacyforexercise
behaviors,
whilelatercallsconcentratedupon
the
adequacy
ofplansforrelapsepre-
vention.Eachcallreview
edperfor-
mance
onthebehaviorspreviously
discussedandencouraged
thepartici-
panttokeep
usingself-regulatory
skillstoachievechange.T
hetele-
phonecalls
weresupplementedby
aParticipantWorkbook,which
includ-
edadditionalinformationregarding
theimportanceof
exercise
incancer
populations,guidelines
forexercise
safety,and
journalpages
totrack
weeklyexercise.Participantswere
provided
with
apedometer.Instruc-
tions
forusingthepedometerwere
included
intheParticipantWorkbook
andwerereview
edduringthefirst
counselingsession.Participantswere
askedtorecord
thenumberof
mi-
nutesof
exercise
they
performed
and
stepsthey
completed
each
dayin
journals,w
hich
werereview
edduring
thetelephonecounselingcalls
Self-efficacy(5
items)
Interventio
nparticipantsreported
trends
towardim
provem
entin
exercise
self-efficacy(0.1±1.2vs
−0.3(±
0.8)
(P=0.06),as
compared
with
controls
Wangetal.
[52]
Bandura’sself-efficacytheory
Self-efficacy
Discuss
program
with
wom
enand
maketheirow
nweeklywalking
goalforexercise;encourage
wom
ento
documentw
eekly
walking
logs
sothey
canseetheir
ownprogress
during
theprogram;
storytelling/rolemodelstoryin
booklet;theresearcher
will
make
weeklyphonecalls
tounderstand
wom
en’sfeelings,the
effects,and
thecountereffectsof
exercise,and
will
praise
wom
en’sperformance
andencouragewom
ento
keep
progressingintheprogramfortheir
personalgoals;self-m
onitoring
with
theheartratering
andpedom-
eter
during
exercise;introduce
the
walking
program
with
written
Exerciseself-efficacyscale(18items)
Subjectsin
theexercise
grouphad
significantly
betterexercise
self-
efficacy
than
thoseintheusualcare
groupover
theinterventionperiod.
Atb
aseline,theinterventio
ngroup
was+13.5pointshigher,and
attim
e4,thedifference
hadincreasedto
+31.3(P<0.001)
J Cancer Surviv (2015) 9:305–338 325

Tab
le4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
materialand
verbalexplanationby
theresearcher
includingwarm
up,
cool
down,andprogressivelyin-
creasing
intensity,frequency,and
durationover
time
Pintoetal.[53]
Transtheoreticalmodelandthe
SCT
Self-efficacy,outcom
eexpectations,
stim
ulus
control,reinforcem
ent
managem
ent,self-m
onito
ring,
goals,planning
Participantsreceived
in-personin-
structions
onhowto
exercise
ata
moderateintensity
level,howto
monito
rheartrate,andhowto
warm
upbefore
exercise
andcool
downafterexercise.T
heywere
givenhomelogs
tomonitorPA
participationandapedometer.E
ach
participantreceivedaweeklycall
over
12weeks
from
research
staff
tomonito
rPA
participation,identi-
fyrelevant
health
problems,prob-
lem
solveanybarriersto
PA,and
reinforceparticipantsfortheiref-
forts.Activity
counselin
gwas
basedon
thetranstheoreticalmodel
andthesocialcognitive
theory
and
tailo
redto
each
participant’s
moti-
vationalreadiness.T
hecounseling
focusedon
strengtheningself-
efficacy
forexercise,onsetting
re-
alistic
outcom
eexpectations,and
ontraining
participantsin
using
behavioralprocessesof
change
such
asstim
ulus
controland
rein-
forcem
entm
anagem
entand
inusingtechniques
such
asself-
monitoring
ofexercise
behavior,
setting
exercise
goals,andplanning
forexercise.A
fter
the12
week
program
was
completed,m
onthly
phonecalls
wereprovided
for
3monthsto
reinforceprogress,
identifylapses
from
PA,and
re-
coverfrom
anylapses
thatmay
have
occurred.F
inally,a
feedback
lettersummarizingparticipants’
progress
was
sent
atweeks
2,4,8,
and12
Stageof
motivationalreadinessforPA
(5items)
The
interventionproduced
strong
effectson
participants’m
otivational
readinessat3months(O
R=5.26,
95%
CI=
1.32–20.93;P
=0.018)
thatwereattenuated
at6months
(OR=3.81,95%
CI=
0.90–16.71;
P=0.070)
andweakenedfurtherat
12months(O
R=1.89,95%
CI=
0.52–6.86;
P=0.335)
Hatchettetal.
[48]
SCT
Self-efficacy,goalsetting,anticipated
resultof
exercise,tim
eThe
e-counseloroffered
adviceregarding
exercise
andPA
.The
researchersbe-
lievedthatifaparticipantwereasked
SCTvariables:self-regulation(20
items);o
utcomeexpectancy
values
(19items);exerciseself-efficacy
Not
reported
326 J Cancer Surviv (2015) 9:305–338

Tab
le4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
managem
ent,self-m
onito
ring,
barriers,relapse
preventio
ntoofferinformationregardingherb
e-havior
duringtheintervention,she
wouldbe
morelikelytoengage
inthe
desiredbehavior.T
hetopics
ofeach
emailareas
follows:week1:goal
setting,anticipated
resultof
exercise;
week2:goalsetting,timemanage-
ment,self-monitoring;week3:self-
monitoring,descriptionof
anexercis-
er,overcom
ingbarriers;w
eek4:self-
monitoring,barrierstoexercise;w
eek
5:self-monitoring,overcomingbar-
riers,describetheanticipated
out-
comes
ofexercise;w
eek7:goalset-
ting,self-monitoring,tim
emanage-
ment,relapseprevention;week9:
overcomingbarriers,goalsetting,
self-monitoring,tim
emanagem
ent,
relapseprevention;week11:proper-
tiesof
anexerciser,results
ofcancer
(14items);exerciseroleidentity(9
items)
Diet-only
trials
Parsonsetal.
[59]
Strategies
adoptedfrom
SCT
Not
described
The
principlestrategy
toprom
otedietary
change
intheinterventionarm
was
atelephonecounselingprotocolwith
individualized,directassistance
tailoredtoeach
participant.T
hetelephonecounselingprotocol
followed
astepwise,phased
approach
thatused
strategies
adoptedfrom
SCT.Motivationalinterview
ing
techniques
wereused
tohelp
participantsassumeandmaintain
responsibilityfortheirbehavioral
change.N
ootherdetails
reported
Not
reported
Multiplebehavior
trials
Dem
ark-
Wahnefried
etal.—
STRENGTH
[60]
SCT(key
conceptsof
prom
oting
self-efficacyandbehavioral
monito
ring)
Self-efficacy,behavioralmonito
ring
Writtenandverbalinstructionbased
onSC
T(key
conceptsof
prom
oting
self-efficacyandbehavioralmoni-
toring)(a
workbookandtelephone
counselin
g).N
ootherdetails
re-
ported
Confidence(self-efficacy)in
making
changesin
theirdietaryor
exercise
practices
(didnotspecify
numberof
items)
Not
reported
Cam
pbelletal.
[61,111,
112]
TTM andSC
TStages
ofchange,socialsupport,
barriersto
change,knowledge,role
models,self-efficacy
G2received
tailo
red-
printexpert
feedback
driven
bybaselin
edata.
G3received
motivational
interviewingtelephonecalls
that
encouraged
participantsto
over-
comeam
bivalenceandidentify
Self-efficacy—
eatin
gfruitand
vegetables,and
engaging
inPA
(2items).S
ocialsupportforhealthy
eatingandexercise
(4items).
Perceivedbarriersto
behavior
Mediatio
n:Nonemediateddietary
change.H
igherself-efficacywas
associated
with
greaterfruitand
vegetableconsum
ptionatboth
baselineandfollo
w-up,butincrease
inself-efficacydidnotp
redict
J Cancer Surviv (2015) 9:305–338 327

Tab
le4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
theirow
nstrategies
forchange.G
4received
both
thetailored-print
feedback
andmotivational
interviewingtelephonecalls
change
(6items),knowledgeof
recommendatio
ns(1
item)
greaterchange
infruitand
vegeta-
bleconsum
ption
There
wereno
interventioneffectsfor
colorectalcancer
survivors
Von Gruenigen
etal.[65,73]
SCT
Establishshort-term
goals,build
self-
efficacy,reinforcement,individual
progresstowardgoals,em
phasison
long-term
change,patient
feedback
The
protocol
follo
wed
astepwise,
phased
approach
usingstrategies
outlinedby
SCT,indicatingthatthe
optim
alinterventio
nforamajor
behavior
change
should
focuson
establishing
short-term
goals,and
enablingtheperson
tobuild
self-
efficacy.P
articipantswere
contactedby
theresearch
dietician
byphoneor
newslettereveryweek
thatthegroupdidnotm
eet.Ph
one
calls
werestructured
incontentand
included
reinforcem
entand
discus-
sion
regardingtheprevious
week’s
topic.Participantswerealso
given
feedback
onindividualprogress
to-
wardPA
andnutrition
goals.
New
slettertopics
included
thefol-
lowing:
holid
ayrecipes,reinforce-
mento
fnutrition
goals,waysto
increase
PAandstep
count,restau-
rant
menumakeovers,and
eatin
gon
therun
Self-efficacyusingtheWeight
EfficacyLife-Style(W
EL)ques-
tionnaire
(20items).S
elf-efficacy
specificto
eatin
gbehaviorsin
five
situationalfactors:n
egativeem
o-tio
ns,foodavailability,socialpres-
sure,physicald
iscomfort,and
pos-
itive
activ
ities
Significantd
ifferencein
“social
pressure”subscale(P=0.03).
Increase
inself-efficacyrelatedto
negativeem
otions
(P<0.01),food
availability(P=0.03),andphysical
discom
fort(P=0.01)in
those
wom
enwho
lostweightd
uringthe
year.A
t12months,self-efficacy
scores
remainedhigh
(6months
afterinterventio
nhadconcluded).
Morbidlyobesepatientshadsig-
nificantly
decreasedself-efficacy
whenfeelingphysicaldiscom
fort
anddecreasedtotalself-efficacy
score.Therewas
asignificanteffect
forself-efficacyrelatedto
social
pressure
andrestraintimproved.
Forself-efficacyrelatedto
negativ
eem
otions,there
was
ameanin-
crease
of8.9in
wom
enwho
lost
weightv
ersus0.6in
thosewhose
weightw
asstableor
who
had
gained
weight
Von Gruenigen
etal.[67]
SCTwith
afocuson
establishing
short-term
goals,enablingthe
person
tobuild
self-efficacy
The
interventionfollowed
astepwise,
phased
approach
with
afocuson
establishing
short-term
goals,en-
ablin
gtheperson
tobuild
self-effi-
cacy
Individualexpertphysiciancounseling,
individualgoalsetting,goal
reinforcem
entinnewsletters,social
supportand
eatinginsocialsituations,
planning
mealsandgrocery
shopping,how
toread
food
labels,
pedometersprovided
feedback
and
reinforcem
entofPA
goals.
Increm
entalgoals(for
months1–2,
months5–6),m
odelingof
resistance
exercise.T
heinterventionfocusedon
theadoptionof
lifelongchanges
ratherthan
caloric
restriction.
Educationandskilldevelopm
entto
increasePA
andPA
self-efficacywere
included
usingaguidepreviously
developedforbreastcancersurvivors.
Patientswereencouraged
toaddac-
tivitiesthatthey
enjoyedortobegina
walking
programor
otherexercise
Not
reported
328 J Cancer Surviv (2015) 9:305–338

Tab
le4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
activity.L
ong-term
changesinevery-
dayactivities
(for
exam
ple,climbing
stairsinsteadof
taking
elevators)and
moderateaerobicactivity
wereem
-phasized.Participantsweregivenpe-
dometerstoprovideimmediatefeed-
back
andreinforcem
enttopatients
andtoprovideobjectiveassessment
ofPA
.Patientsweregiven3lbhand
andadjustableankleweightsand
instructed
intheproperform
and
procedureforperformingresistance
exercises.Heartratemonitorswere
provided
tofacilitatemonitoringof
targetheartrategoals.Physician
counselingvisits(conducted
bythe
PI)at3,6,and
12monthsfocusedon
nutritionandPA
goalsforSU
CCEED
participantsinordertoaugm
entthe
groupsessions
andprovideindividu-
alized
attention
Dem
ark-
Wahnefried
etal.—
FRESH
START[62,
63,78]
SCT:cuesto
action,self-efficacy,
skill
developm
ent,goals,goal
reinforcem
ent.Messageswere
custom
ized
tostages
ofchange
(TTM)
Benchmarkbehavior,goal,behavior
logs,behavioralcues,tailo
redto
stages
ofchange,goal,testim
onial,
overcomingbarriers,benefits,
progress
togoal
The
FRESH
STARTinterventionwas
basedon
theSC
Tthatem
phasizes
confidence
buildingandskills
developm
ent;thetranstheoretical
modelalso
was
used
tofram
emessageson
participants’stageof
readinesstomotivatebehavior
change.Participantsareencouraged
tosetsmallincrementalgoals,w
hich,
whenachieved,arereinforced
tobuild
self-efficacy.To
build
upon
self-
efficacyincrem
entally,participants
areassisted
inmakingchangesinone
behavioraldomainatatim
e.Partici-
pantsarefirstassigned
thebehavior
with
thehighestself-efficacyscore,
andbehaviorswith
lowerscores
are
presentedsubsequently(with
thepre-
misethatafterthe
participantachieves
successfulbehaviorchange
inthefirst
area,heor
shecangeneralizethis
successtothenexthealthdomain).In
situations
whereself-efficacyscores
areequalfor
thetwobehaviors,the
mostadvancedstageofreadinesswill
dictatethefirstdomaintargeted.For
Self-efficacy(PAanddiet)(3
items),
stageof
readiness(range
3–12
items,dependingon
responses),
socialsupport(11
items),barriers
(37items)
The
interventionwas
notsignificantly
associated
with
self-efficacyfor
exercise;how
ever,therewas
apos-
itive
correlationobtained
between
self-efficacyforexercise
andtotal
minutes
perweekof
exercise
atfollow-up
Mediatio
n:Resultssupportthe
hypothesisthatchangesin
self-
efficacy
forfatrestrictionandeatin
gmorefruitand
vegetables
partially
mediatetheeffectsof
theinterven-
tionon
dietquality
(37.7%
vari-
ance,P
<0.001).F
urthermore,
change
inself-efficacyforfatre-
strictionpartially
mediatedthein-
terventio
n’seffectson
thepercent-
ageof
kilocalories
from
fat(30.1
%variance,P
<0.001),and
change
inself-efficacyforfruitand
vegetable
consum
ptionpartially
mediatedthe
interventio
n’seffectson
daily
serv-
ings
offruitand
vegetables
J Cancer Surviv (2015) 9:305–338 329

Tab
le4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
participantsreporting
3deficientbe-
havioralareas,theinitialintervention
materialstargetthebehavior
associat-
edwith
thehighestself-efficacyscore,
andthesecond
behavioralarea
isse-
lected
atrandom
.Intheinitialmail-
ing,participantsreceiveapersonal-
ized
workbookthatincludes
thefirst
unitmaterials,and
asecond
install-
mentofworkbookmaterialsarrives
midway
throughtheintervention.For
each
unit,thefirstpage
isafeedback
form
inwhich
theparticipant’sbe-
havior
iscomparedwith
goalbehav-
ior,andencouragem
entisprovided
toachievethegoal.E
achinstallmentof
theworkbookincludes
personalized
behavior
record
logs
thatcorrespond
tothecontentareas
tohelppartici-
pantstrack
behavior
(toprom
ote
change
andimproveself-reporting
accuracy).In
addition,each
install-
mentoftheworkbookincludes
items
thatserveas
behavioralcues
[i.e.,a
pany
theexercise
unit].N
ewsletters
are4pagesof
colorfulgraphics
and
textthatincludethefollowingcom-
ponents:(1)apersonalized
greeting
tailoredtostageof
readiness;(2)a
goalstatem
entthatreflectsengage-
mentingoalsetting
behavior;(3)
atestimonialtailoredon
age,race,and
cancercoping
style;(4)an
advice
columnthatprovides
guidance
for
overcomingbarriers—tailoredtoa
subject’s
reportedbarriers;(5)
a“Fun
Facts”
section—
untailored;(6)a
benefitssectionthatisuntailoredand
emphasizes
thebenefitsof
practicing
goalbehavior;(7)astatus
sectionthat
features
agraphdepictingthepartici-
pant’sprogressinrelationtogoaland
accompanyingtailoredmessages[i.e.,
achievem
entofgoal(praise),progress
towardgoal(praiseandencourage-
ment),no
progress(encouragement),
330 J Cancer Surviv (2015) 9:305–338
pedometerandTherabands®
accom-

Tab
le4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
ortheabsenceof
data(encourage-
menttosubm
itupdateddata)]
Djuricetal.
[64]
SCT—thetelephonecounseling
approach
blendedmotivational
interviewing(M
I)with
SCT
Goals,self-monito
ring,self-efficacy
The
telephonecounselingapproach
blendedMIwith
SCT.Theyalso
received
pedometers,adaily
food
and
exercise
log,andexam
plemenus
atindividuallyappropriatecalorie
levels.
The
counselingplan
was
forthe
dieticiantocontactsubjectsw
eeklyfor
thefirsttwocalls,biweeklyforthe
next5months,andmonthlyforthe
last6months,foratotalof19
calls.
The
self-monitoringlogs
were
review
edduringthecalls.T
hecounselingapproach
combinedprin-
ciples
ofSC
TandMI.Subjectswere
involved
inderivingtheirow
nshort-
term
goalsandevaluatingtheirprog-
resstowardgoals.To
build
self-effi-
cacy,any
positivechangeson
theself-
monitoringsheetswereidentifiedand
praised
Self-efficacy(6items),self-confidence
formaintaining
ahealthylifestyle
(6items)
Not
reported
Djuricetal.
[66]
SCT
Self-m
onitoring,goalsettin
g,self-
efficacy,considerationof
body
image,socialsupport,removing
roadblocks,positive
thinking,
dealingwith
high-risksituations
andslips,andcueelim
ination
G3(individualized
arm):Monthly
writteninform
ationwas
prepared
onvarious
weightlosstopics
(environm
entalcontrol,servingsize
control,exercise,m
otivation,goal
setting,holiday
eating,seasonal
foods)andeitherpresentedtothe
wom
enatthemonthlymeetingor
mailedtotheirhomes.Pedom
eters
wereprovided
forself-monitoringand
goalsetting.Itw
asrequestedthatex-
ercise
anddietarylogs
bekeptdaily,
andthesewerereview
edtogetherwith
each
subject.Contactswereby
phone
orinperson,and
food
andexercise
recordsweremailedtothedietician
beforethescheduledcontact.The
counselingsessionvariedinlength
dependingon
individualneeds.The
dieticianfirstverifiedwhetheror
not
theparticipantwas
meetingbehavior
change
goalssetintheprevious
week.
Ifnot,theproblem
was
delineated,
andthedieticianhelped
thesubject
devise
aplan
thatwouldbe
used
to
Nonereported
Not
reported
J Cancer Surviv (2015) 9:305–338 331

one did not report how SCT constructs were operationalized[60]. All other trials reported goal setting, self-monitoring,building self-efficacy (for PA and diet) [60–63, 67], or diet[65, 73], or for maintaining a healthy lifestyle [64], overcom-ing barriers, and social support [61–66, 73]. Goal setting [48,63–67] and review of goals [63–66] were commonly opera-tionalized. Self-monitoring was commonly operationalizedthrough providing a pedometer [63, 64, 66, 67] or log sheet[63, 64, 66]. Few trials reported how they operationalizedoutcome expectations, with only three that reported socialsupport [63, 66, 67], one that included environment [66],and one that reported relapse prevention [48]. Four studiesincluded identification of barriers and how to overcome them[48, 61, 63, 66]. Self-efficacy did not appear to be related toPA behavior change [60, 63]. Improvements to diet qualitywere partially mediated by changes in self-efficacy for fatrestriction and eating more fruit and vegetables [62, 63, 78].Only the social pressure subscale of self-efficacy was signif-icantly related to eating behaviors (P=0.03) [65, 73]. Twotrials reported that self-efficacy was not associated with dietchanges [60] or fruit and vegetable consumption [61]. Socialsupport for healthy eating, perceived barriers to behaviorchange, and knowledge of recommendations were assessed,but none mediated fruit and vegetable consumption [61].
Discussion
Overview of findings
The aims of this review were to synthesize the existing liter-ature relating to PA and diet interventions based on SCT thattarget cancer survivors and to identify successful strategies toassist cancer survivors in making positive PA and diet behav-ior change. This review supports the efficacy of SCT-basedinterventions in changing PA and diet behavior in cancersurvivors. Our effect size of 0.33 for PA interventions can bedefined as a small-to-medium effect [79] and is similar toother meta-analyses [5, 80, 81] that reported effect sizes of0.32–0.38 for PA interventions (including cancer survivorsboth during and after treatment). Our positive results for PAbehavior mirror the results reported in two recent reviewsexamining PA behavior change in breast cancer survivorsand also found that trials were mostly PA only, few includedobjective measures, and few reported postintervention main-tenance [82, 83]. While evidence has been building to supportthe effects of PA and diet behavior on health outcomes, thereremains a need to focus on behavior change trials to under-stand how to promote sustainable healthy behaviors.
Our findings that the majority of included trials reportedstatistically significant improvements to at least one aspect ofdiet quality and weight loss are supported by other reviewsT
able4
(contin
ued)
Study
Theoreticalbasis
SCTconstructsoperationalized
How
constructswereoperationalized
Constructsmeasured(no.of
items)
Results
circum
venttheproblem.T
hetech-
niques
taughtincluded
goalsetting,
menuplanning,self-efficacy,self-
monitoring,considerationof
body
image,socialsupport,socialeating,
removingroadblocks,positive
think-
ing,dealingwith
high-risksituations
andslips,andcueelimination
G4(com
prehensive
arm):Subjects
received
theindividualized
counselingdescribed
aboveandwere
askedtoattend
weeklyweight
watchersmeetings
usingfree
coupons
332 J Cancer Surviv (2015) 9:305–338

with the general adult population [80, 81]. Due to considerableheterogeneity in the dietary outcomes assessed, it was notpossible to conduct a meta-analysis, although self-reportedimprovements to diet quality were evident in six of eightstudies. The two trials that did not find improvements todietary quality had a primary aim of decreasing weight, ratherthan behavior change [65, 66]. More evidence is requiredfrom behavior change trials that have an emphasis on dietarychange rather than weight.
The limited number of trials and the heterogeneity ofincluded studies in this review prevented any formal subgroupanalyses in our review. The effect appeared strongest for PA-only interventions compared to multiple behavior interven-tions; however, this should be interpreted with caution as PA-only interventions included smaller sample sizes and shorterfollow-up periods. A review of single compared to multiplebehavior interventions in older adults also reported that PAeffects appeared strongest in single behavior change interven-tions. However, there were inadequate multiple health behav-ior change interventions to compare to [84]. Similar reviews[80, 81] examined intervention setting, duration, person de-livering the intervention, delivery mode, age of target group,and intervention effectiveness and found that only increasedcontact frequency was associated with increased PA and dietbehavior change [80].
Social cognitive theory
Few trials conducted mediation analyses or reported changes intheoretical constructs. In those that did report the impact ofinterventions on theoretical constructs, results were inconsis-tent. Self-efficacy was the only construct that appeared to beassociated with positive behavior change for both PA and diet[52, 57, 61–63, 65, 73]; however, mediation analyses in twotrials identified that theoretical constructs only partially medi-ated the intervention effects [62, 63, 70]. Other reviews exam-ining individual SCT constructs have concluded positive out-come expectations, and intentions are associated with behaviorchange [85, 86]. Self-efficacy and goal setting were commonlyoperationalized, but there was limited reporting of how otherconstructs were operationalized as part of the intervention.Recent reviews identified that self-efficacy, self-monitoring ofbehavior, prompting intention formation, planning, specificgoal setting and review, and feedback on performance wereassociated with increased effectiveness in PA and diet behaviorchange [80, 81, 87]. However, given the crossover betweentheoretical constructs and behavior change techniques, the pos-itive results for SCT-based trials in this review may be a resultof the individual behavior change techniques employed, such asself-regulatory behaviors, rather than the theoretical constructs.
Recent reviews have questioned the value of theory indeveloping and evaluating interventions, with two recent be-havior change reviews concluding that interventions based on
theory were no more effective than atheoretical interventions[80, 88] and another two reviews that supported the efficacy oftheory-based interventions [89, 90]. The conflicting resultsmay be due, at least in part, to the inadequate description ofhow theory is implemented and evaluated in interventions andalso due to the overlap with specific behavior change tech-niques, which have been associated with interventioneffectiveness.
There were differences in the risk of bias assessment. Themajority of PA-only studies received a strong global rating(n=5), and multiple behavior trials received a moderate globalrating (n=5). Trials received a weak global rating becausefewer than 60 % of potentially eligible participants agreed totake part before randomization, which is used as an estimate ofthe external validity of the study [47, 91], and because both theoutcome assessor and study participants were aware of theresearch question [47]. Unlike in clinical trials where partici-pants are unaware of their exposure status, behavior changetrials present significant problems with blinding and recruit-ment as participants are expected to actively engage with theintervention. Self-selection bias is a likely issue in behaviorchange trials.
Strengths and weaknesses of review methods
Although this is a comprehensive review of the publishedliterature, there are some limitations that should be noted.Search results were screened for eligibility by only one re-viewer, despite recommendations that this step is conductedby two independent reviewers [92]. This review comprehen-sively searched a number of databases; however, it made noattempt to search for non-English publications or unpublishedliterature. Potentially eligible study protocols were obtained;however, no attempt was made to contact trial authors toobtain unpublished results of these studies [93–95]. The re-view included a broad definition of cancer survivors, includ-ing those both during and after completion of active treatment.While this increases the breadth of evidence, it likely contrib-uted to the heterogeneity of the included studies.
There are a number of SCT-based health outcomes trials,including the WINS [96–98] and WHEL [99, 100] trials,Active for Life trial [101], and RENEW trial [102, 103], thatinitially met criteria for inclusion in the review [104]. How-ever, the study team agreed not to include these trials asbehavior changewas either not reported [101, 104] or reportedas a secondary outcome only [96, 99, 102]. Due to the hetero-geneity of these trials and the inconsistency in reportingbehavior change outcomes, these trials were not included inthe review. The definition of SCT-based intervention wasrelatively broad and not limited by how well SCT was de-scribed or operationalized in the intervention. Studies neededto explicitly state that the intervention was based on SCT,which may or may not have included other theories, and was
J Cancer Surviv (2015) 9:305–338 333

dependent on the author description of the trial. Recent pub-lications have detailed a checklist for evaluating the extent towhich an intervention is theory-based [105], whichwill enablegreater clarity in the role of theory in the development of anintervention. There was one trial where it was unclear if thestudy was based on a theoretical framework. One paper [50]had been screened and judged not eligible due to notreporting that the trial was based on SCT. However,subsequent eligible and included trial papers [71, 72]reported that the intervention was based on SCT, andtherefore, this trial was included in the review. It maybe that due to publication size restrictions, authors havelimited space to fully describe intervention development.Alternatively, theoretical frameworks may be appliedpost hoc to an intervention. With journals requiringadherence to CONSORT [91], this is likely to improvethe consistent and transparent reporting of RCTs.
Limitations of the included trials
Studies demonstrated moderate heterogeneity, although mostinterventions included breast cancer patients and were con-ducted with patients after completion of active treatment. Thislimits the generalizability of findings to males, to survivors ofother cancer types, and to patients undergoing active treat-ment. Most studies involved small sample sizes and only fourtrials reported a sample size greater than 100 [49, 54, 61, 63].Only three of the trials included in this review focused onpromoting resistance training [54, 60, 67], despite a recentreview and meta-analysis that concluded resistance traininghas benefits on body composition and muscle strength incancer patients during and after cancer treatment [106].Meta-analysis used objectively assessed data, where available[51, 60]; however, the majority of data was self-reported. PAand diet outcomes were predominantly based on self-reportdata, while weight was frequently measured or objectivelyassessed [59–62, 64–66]. Participants were not blinded tointervention aims in any trials, so there may be inherentdifferences between those participants recruited for PA-onlyinterventions, compared to participants interested in diet,weight control, or multiple behavior interventions.
Future research
This review supports the efficacy of SCT-based interventionsin changing PA and diet behavior in cancer survivors. Whileinterventions reported a theoretical basis, these constructswere often inadequately operationalized or reported and rarelymeasured or tested [89, 107, 108]. Despite a large body ofcross-sectional data [33–38] linking SCT constructs with dietand PA behavior, there remains a need to test whether changesin these constructs predict behavior change in interventions.
Comparison between health theories would also be a usefulgap to address.
Development of the taxonomy assessing the extent towhich interventions are theory-based and use of behaviorchange techniques [81, 105] will contribute evidence to helpresearchers understand the intervention components that areessential to behavior change. Whether these are related tospecific theoretical constructs, or to behavior change tech-niques, such as self-regulatory techniques, requires furtherresearch. Research assessing whether single or multiple healthbehavior interventions have the greatest benefit to improve PAand diet behaviors is required.
There is a large evidence base supporting the efficacy of PAinterventions, and these are predominantly based on breastcancer patients, using short-term, self-reported outcomes. Fu-ture studies need to consider how to translate this research intoongoing support and programs to assist cancer survivors toincrease and maintain PA levels. Further work should alsoinclude trials which focus on resistance training, as there arespecific guidelines for cancer survivors to undertake resis-tance training. The field of dietary interventions is much lessdeveloped, with interventions demonstrating that cancer sur-vivors are willing and able to make improvements to diet [13,63, 80, 99, 102]. As diet quality is comprised of a complex setof behaviors, there is a need to examine the co-occurrence ofchanges in different aspects of diet [109]. Future studieswould benefit from considering the impact of behavior changefrom a healthy lifestyle perspective, such as considering com-pliance with World Cancer Research Fund guidelines [14].
Implications
Despite the limitations of this review, it appears that SCT-based interventions demonstrate promise for improving thePA and diet behaviors of cancer survivors. Interventions usinga range of delivery modes all demonstrated significant PAimprovements, with a small-to-medium effect size, after arelatively short intervention period (12 weeks). Diet and mul-tiple behavior component interventions tended to have ahigher number of intervention contacts and greater interven-tion duration (6 months). However, the increased contact timedid not appear to be related to the magnitude of change. Hightrial retention across both single and multiple behavior changetrials may be related to the low burden of predominantlyunsupervised interventions or that cancer survivors are moti-vated to improve their PA and diet behaviors. Unfortunately,there was little evidence to guide researchers in helping cancersurvivors to maintain health behaviors after completion ofinterventions, and this has been noted previously [83, 110].Improved description and reporting of intervention contentand the way in which theory-based interventions use theoryto guide the trial and intervention components remain neces-sary to understand what factors are driving the results of
334 J Cancer Surviv (2015) 9:305–338

theory-based interventions. Given the recent mixed findingson the efficacy of theory-based interventions, a greater under-standing of how theory is operationalized is necessary tounderstand what factors contribute to the success of interven-tions. Further evidence on theory-based trials is required tounderstand the crossover between theory-based constructs andbehavior change techniques and understand the impact of eachon improving health behaviors. Research expanding the rig-orous implementation and reporting of behavior change tech-niques is likely to improve understanding of the workingmechanisms that underpin how and why an interventionworks or does not work.
Conclusions
SCT-based interventions appear effective in improving PAand diet behaviors. No specific intervention characteristicsor theoretical constructs were associated with effectiveness.Future SCT-based interventions should describe the extent towhich theoretical or behavior change constructs are imple-mented and evaluated, in order to identify the successfulcomponents of SCT-based interventions.
Conflict of interest The authors have no potential financial or personalconflicts of interest to disclose in relation to this work.
Appendix 1: Medline search
1. cancer survivor*.mp.2. Survivors/3. cancer*.mp.4. exp Cancer/5. 3 or 46. 2 and 57. cancer patient*.mp.8. patient*.mp.9. exp Patients/
10. 8 or 911. 5 and 1012. 1 or 6 or 7 or 1113. exp Nutrition Surveys/ or exp Nutrition Policy/ or exp
Nutrition Assessment/ or exp Nutrition Therapy/14. Diet, Cariogenic/ or Diet Surveys/ or Diet, Carbohy-
drate-Restricted/ or Diet Therapy/ or Diet, Atherogenic/or Diet/ or Diet, Sodium-Restricted/ or Diet, Gluten-Free/ or Diet, Reducing/ or Diet, Fat-Restricted/ or Ke-togenic Diet/ or Diet Fads/ or Diet, Macrobiotic/ or Diet,Protein-Restricted/ or Diet, Vegetarian/ or Diet,Mediterranean/ or Diabetic Diet/ or Diet Records/
15. Food Habits/ or exp Food/ or Health Food/ or FoodPreferences/
16. 13 or 14 or 1517. physical activity.mp. or Motor Activity/18. exercise therapy/ or muscle stretching exercises/ or re-
sistance training/ or strength training19. Exercise/20. weight.mp.21. aerobic.mp. or Physical Exertion/22. running/ or swimming/ or walking/23. 17 or 18 or 19 or 20 or 21 or 2224. 16 or 2325. Health Behavior/ or Self Efficacy/ or social cognitive
theory.mp. or Psychological Theory/ or Social Support/26. social cognitive.mp.27. Motivation/ or Health Education/ or Health Promotion/
or social learning theory.mp.28. 25 or 26 or 2729. 12 and 24 and 28
Open Access This article is distributed under the terms of the CreativeCommons Attribution License which permits any use, distribution, andreproduction in any medium, provided the original author(s) and thesource are credited.
References
1. Campo RA, Rowland JH, Irwin ML, Nathan PC, Gritz ER, KinneyAY. Cancer prevention after cancer: changing the paradigm—areport from the American Society of Preventive Oncology. CancerEpidemiol Biomarkers Prev. 2011;20:2317–24.
2. Jemal A, Bray F, Center MM, Ferlay J, Ward E, Forman D. Globalcancer statistics. CA Cancer J Clin. 2011;61:69–90.
3. Carmack CL, Basen-Engquist K, Gritz ER. Survivors at higher riskfor adverse late outcomes due to psychosocial and behavioral riskfactors. Cancer Epidemiol Biomarkers Prev. 2011;20:2068–77.
4. Cramp F, Daniel J. Exercise for the management of cancer-relatedfatigue in adults (review). Cochrane Database of SystematicReviews. 2008;CD006145.
5. Speck RR, Courneya KS, Masse LC, Duval S, Schmitz KH. Anupdate of controlled physical activity trials in cancer survivors: asystematic review and meta-analysis. J Cancer Surviv. 2010;4:87–100.
6. Ferrer RA, Huedo-Medina TB, Johnson BT, Ryan S, Pescatello LS.Exercise interventions for cancer survivors: a meta-analysis ofquality of life outcomes. Ann Behav Med. 2011;41:32–47.
7. McNeely ML, Campbell KL, Rowe BH, Klassen TP, Mackey JR,Courneya KS. Effects of exercise on breast cancer patients andsurvivors: a systematic review and meta-analysis. Can Med AssocJ. 2006;175:34–41.
8. Schmitz KH, Courneya KS, Matthews C, Demark-Wahnefried W,Galvao DA, Pinto BM, et al. American College of Sports Medicineroundtable on exercise guidelines for cancer survivors. Med SciSport Exerc. 2010;42:1409–26.
9. Rock CL, Doyle C, Demark-Wahnefried W, Meyerhardt J,Courneya KS, Schwartz AL, et al. Nutrition and physical activity
J Cancer Surviv (2015) 9:305–338 335

guidelines for cancer survivors. CA Cancer J Clin. 2012;62:242–74.
10. Ballard-Barbash R, Friedenreich CM, Courneya KS, Siddiqi SM,McTiernan A, Alfano CM. Physical activity, biomarkers, and dis-ease outcomes in cancer survivors: a systematic review. J NatlCancer Inst. 2012;104:1–26.
11. Demark-Wahnefried W, Clipp EC, Morey MC, Pieper C, Sloane R,Snyder DC, et al. Lifestyle intervention development study toimprove physical function in older adults with cancer: outcomesfrom Project LEAD. J Clin Oncol. 2006;24:3465–73.
12. Scheier MF, Helgeson VS, Schulz R, Colvin S, Berga S, BridgesMW, et al. Interventions to enhance physical and psychologicalfunctioning among younger women who are ending nonhormonaladjuvant treatment for early-stage breast cancer. J Clin Oncol.2005;23:4298–311.
13. Chlebowski R. Lifestyle change including dietary fat reduction andbreast cancer outcome. J Nutr. 2007;137:233S–5S.
14. World Cancer Research Fund/American Institute for CancerResearch. Food, nutrition, physical activity, and the prevention ofcancer: a global perspective. Washington: AICR; 2007.
15. Psaltopoulou T, Ilias I, Alevizaki M. The role of diet and lifestyle inprimary, secondary, and tertiary diabetes prevention: a review ofmeta-analyses. Rev Diabet Stud. 2010;7:26–35.
16. Hussain A, Claussen B, Ramachandran A, Williams R. Preventionof type 2 diabetes: a review. Diabetes Res Clin Pract. 2007;76:317–26.
17. Artinian NT, Fletcher GF, Mozaffarian D, Kris-Etherton P, VanHorn L, Lichtenstein AH, et al. Interventions to promote physicalactivity and dietary lifestyle changes for cardiovascular risk factorreduction in adults: a scientific statement from the American HeartAssociation. Circulation. 2010;122:406–41.
18. Robien K, Demark-Wahnefried W, Rock CL. Evidence-based nu-trition guidelines for cancer survivors: current guidelines, knowl-edge gaps, and future research directions. J Am Diet Assoc.2011;111:368–75.
19. Hayes SC, Spence RR, Galvão DA, Newton RU. Australian asso-ciation for exercise and sport science position stand: optimisingcancer outcomes through exercise. J Sci Med Sport. 2009;12:428–34.
20. Campbell A, Stevinson C, Crank H. The BASES expert statementon exercise and cancer survivorship. J Sports Sci. 2012;30:949–52.
21. Cancer Council Australia. Position statement on benefits of healthydiet and physical activity for cancer survivors. 2013 Available from:www.cancer.org.au/content /pdf/CancerControlPolicy/PositionStatements/PSbenefitshealthydietcancersurvivorsJUN06.pdf. Accessed 11 Aug 2013.
22. Courneya KS, Friedenreich CM. Physical activity and cancer con-trol. Semin Oncol Nurs. 2007;23:242–52.
23. Bellizzi KM, Rowland JH, Jeffery DD, McNeel T. Healthbehaviors of cancer survivors: examining opportunities forcancer control intervention. J Clin Oncol. 2005;23:8884–93.
24. Eakin EG, Youlden DR, Baade PD, Lawler SP, Reeves MM,Heyworth JS, et al. Health behaviors of cancer survivors: data froman Australian population-based survey. Cancer Causes Control.2007;18:881–94.
25. Blanchard CM,CourneyaKS, Stein K. Cancer survivors’ adherenceto lifestyle behavior recommendations and associations with health-related quality of life: results from the American Cancer Society’sSCS-II. J Clin Oncol. 2008;26:2198–204.
26. Glanz K, Bishop DB. The role of behavioral science theory indevelopment and implementation of public health interventions.Annu Rev Public Health. 2010;31:399–418.
27. Noar SM, Benac CN, Harris MS. Does tailoring matter? Meta-analytic review of tailored print health behavior change interven-tions. Psychol Bull. 2007;133:673–93.
28. Abraham C, Michie S. A taxonomy of behavior change techniquesused in interventions. Health Psychol. 2008;27:379–87.
29. Nigg CR, Allegrante JP, Ory M. Theory-comparison and multiple-behavior research: common themes advancing health behavior re-search. Health Educ Res. 2002;17:670–9.
30. Lubans DR, Foster C, Biddle SJH. A review of mediators ofbehavior in interventions to promote physical activity among chil-dren and adolescents. Prev Med. 2008;47:463–70.
31. Bandura A. Health promotion by social cognitive means. HealthEduc Behav. 2004;31:143–64.
32. Bandura A. Health promotion from the perspective of social cogni-tive theory. Psychol Health. 1998;13:623–49.
33. White S, Wojcicki T, McAuley E. Social cognitive influences onphysical activity behavior in middle-aged and older adults. GerontolPsychol Sci Soc Sci. 2011;67B:18–26.
34. Phillips S, McAuley E. Social cognitive influences on physicalactivity participation in long-term breast cancer survivors.Psychooncology. 2012;22:783–91.
35. Rovniak LS, Anderson ES, Winett RA, Stephens RS. Socialcognitive determinants of physical activity in young adults: aprospective structural equation analysis. Ann Behav Med.2002;24:149–56.
36. Ayotte B, Margrett J, Hicks-Patrick J. Physical activity in middle-aged and young-old adults: the roles of self-efficacy, barriers, out-come expectancies, self-regulatory behaviors and social support. JHealth Psychol. 2010;15:173–85.
37. Anderson-Bill ES, Winett RA, Wojcik JR. Social cognitive deter-minants of nutrition and physical activity among web-health usersenrolling in an online intervention: the influence of social support,self-efficacy, outcome expectations, and self-regulation. J MedInternet Res. 2011;13:e28.
38. Anderson E, Winett RA, Wojcik JR. Self-regulation, self-efficacy,outcome expectations, and social support: social cognitive theoryand nutrition behavior. Ann Behav Med. 2007;34:304–12.
39. Graves KD. Social cognitive theory and cancer patients’ quality oflife: a meta-analysis of psychosocial intervention components.Health Psychol. 2003;22:210–9.
40. Courneya KS, Segal RJ, Mackey JR, Gelmon K, Reid RD,Friedenreich CM, et al. Effects of aerobic and resistance exercisein breast cancer patients receiving adjuvant chemotherapy: a multi-center randomized controlled trial. J Clin Oncol. 2007;25:4396–404.
41. Courneya KS, Sellar CM, Stevinson C, McNeely ML, Peddle CJ,Friedenreich CM, et al. Randomized controlled trial of the effects ofaerobic exercise on physical functioning and quality of life inlymphoma patients. J Clin Oncol. 2009;27:4605–12.
42. Rowland JH, Hewitt M, Ganz PA. Cancer survivorship: a newchallenge in delivering quality cancer care. J Clin Oncol. 2006;24:5101–4.
43. Courneya KS. Efficacy, effectiveness, and behavior change trials inexercise research. Int J Behav Nutr Phys. 2010;7:81.
44. Liberati A, Altman DG, Tetzlaff J, Mulrow C, Gotzsche PC,Ioannidis JPA, et al. The PRISMA statement for reportingsystematic reviews and meta-analyses of studies that evaluatehealthcare interventions: explanation and elaboration. BMJ.2009;339.
45. Review Manager (RevMan). The Cochrane Collaboration,Copenhagen, Denmark. 2011.
46. Deeks JJ, Higgins JPT, AltmanDG. Analysing data and undertakingmeta-analyses. In: Higgins JPT, Green S, editors. Cochrane hand-book for systematic reviews of interventions. Chichester: Wiley;2008.
47. Thomas BH, Ciliska D, Dobbins M, Micucci S. A process forsystematically reviewing the literature: providing the research evi-dence for public health nursing interventions. Worldviews EvidBased Nurs. 2004;1:176–84.
336 J Cancer Surviv (2015) 9:305–338

48. Hatchett A, Hallam J, Ford M. Evaluation of a social cognitivetheory-based email intervention designed to influence the physicalactivity of survivors of breast cancer. Psychooncology. 2012;22:829–36.
49. Ligibel JA, Meyerhardt J, Pierce JP, Najita J, Shockro L, CampbellN, et al. Impact of a telephone-based physical activity interventionupon exercise behaviors and fitness in cancer survivors enrolled in acooperative group setting. Breast Cancer Res Treat. 2011;132:205–13.
50. Pinto BM. Home-based physical activity intervention for breastcancer patients. J Clin Oncol. 2005;23:3577–87.
51. Rogers L, Hopkins-Price P, Vicari S, Pamenter R, Courneya K,Markwell S, et al. A randomized trial to increase physical activityin breast cancer survivors. Med Sci Sports Exerc. 2009;41:935–46.
52. WangY-J, BoehmkeM,WuY-WB, Dickerson SS, Fisher N. Effectsof a 6-week walking program on Taiwanese women newly diag-nosed with early-stage breast cancer. Cancer Nurs. 2011;34:E1–E13.
53. Pinto BM, Papandonatos GD, Goldstein MG, Marcus BH, FarrellN. Home-based physical activity intervention for colorectal cancersurvivors. Psychooncology. 2013;22:54–64.
54. Short CE, James EL, Girgis A, D’Souza MI, Plotnikoff RC. Mainoutcomes of the Move More for Life trial: a randomised controlledtrial examining the effects of tailored-print and targeted-print mate-rials for promoting physical activity among post-treatment breastcancer survivors. Psychooncology. 2014.
55. Short CE, James EL, Girgis A, Mcelduff P, Plotnikoff RC. Movemore for life: the protocol for a randomised efficacy trial of atailored-print physical activity intervention for post-treatment breastcancer survivors. BMC Cancer. 2012;12:172.
56. Valle CG, Tate DF, Mayer DK, Allicock M, Cai J. A randomizedtrial of a Facebook-based physical activity intervention for youngadult cancer survivors. J Cancer Surviv. 2013;7:355–68.
57. Bennett JA, Lyons KS, Winters-Stone K, Nail LM, Scherer J.Motivational interviewing to increase physical activity in long-term cancer survivors: a randomized controlled trial. Nurs Res.2007;56:18–27.
58. Matthews CE, Wilcox S, Hanby CL, Der Ananian C, Heiney SP,Gebretsadik T, et al. Evaluation of a 12-week home-based walkingintervention for breast cancer survivors. Support Care Cancer.2007;15:203–11.
59. Parsons JK, Newman VA, Mohler JL, Pierce JP, Flatt S, Marshall J.Dietary modification in patients with prostate cancer on activesurveillance: a randomized, multicentre feasibility study. BJU Int.2008;101:1227–31.
60. Demark-WahnefriedW, Case LD, Blackwell K,Marcom PK, KrausW, Aziz N, et al. Results of a diet/exercise feasibility trial to preventadverse body composition change in breast cancer patients onadjuvant chemotherapy. Clin Breast Cancer. 2008;8:70–9.
61. Campbell MK, Carr C, Devellis B, Switzer B, Biddle A,Amamoo MA, et al. A randomized trial of tailoring andmotivational interviewing to promote fruit and vegetableconsumption for cancer prevention and control. Ann BehavMed. 2009;38:71–85.
62. Demark-Wahnefried W, Clipp E, McBride C, Lobach D, Lipkus I,Peterson B, et al. Design of FRESH START: a randomized trial ofexercise and diet among cancer survivors. Med Sci Sports Exerc.2003;35:415–24.
63. Demark-Wahnefried W, Clipp EC, Lipkus IM, Lobach D, SnyderDC, Sloane R, et al. Main outcomes of the FRESH START trial: asequentially tailored, diet and exercise mailed print interventionamong breast and prostate cancer survivors. J Clin Oncol.2007;25:2709–18.
64. Djuric Z, Ellsworth JS, Weldon AL, Ren J, Richardson CR,Resnicow K, et al. A diet and exercise intervention during chemo-therapy for breast cancer. Open Obes J. 2011;3:87–97.
65. von Gruenigen VE, Courneya KS, Gibbons HE, Kavanagh MB,Waggoner SE, Lerner E. Feasibility and effectiveness of a lifestyleintervention program in obese endometrial cancer patients: a ran-domized trial. Gynecol Oncol. 2008;109:19–26.
66. Djuric Z, DiLaura NM, Jenkins I, Darga L, Jen CK-L, MoodD, et al. Combining weight-loss counseling with the weightwatchers plan for obese breast cancer survivors. Obes Res.2002;10:657–65.
67. von Gruenigen V, Frasure H, Kavanagh MB, Janata J, Waggoner S,Rose P, et al. Survivors of uterine cancer empowered by exerciseand healthy diet (SUCCEED): a randomized controlled trial.Gynecol Oncol. 2012;125:699–704.
68. Rogers L, Hopkins Price P, Vicari S, Markwell S, Pamenter R,Courneya K, et al. Physical activity and health outcomes threemonths after completing a physical activity behavior change inter-vention: persistent and delayed effects. Cancer EpidemiolBiomarkers Prev. 2009;18:1410–8.
69. Rogers L, Vicari S, Courneya K. Lessons learned in the trenches:facilitating exercise adherence among breast cancer survivors in agroup setting. Cancer Nurs. 2010;33:E10–7.
70. Rogers LQ, Markwell S, Hopkins-Price P, Vicari S, Courneya K,Hoelzer K, et al. Reduced barriers mediated physical activity main-tenance among breast cancer survivors. J Sport Exerc Psychol.2011;33:235–54.
71. Pinto BM, Rabin C, Dunsiger S. Home-based exercise amongcancer survivors: adherence and its predictors. Psychooncology.2009;18:369–76.
72. Rabin CS, Pinto BM, Trunzo JJ, Frierson GM, Bucknam LM.Physical activity among breast cancer survivors: regular exercisersvs participants in a physical activity intervention. Psychooncology.2006;15:344–54.
73. von Gruenigen V, Gibbons H, Kavanagh M, Janata J, Lerner E,Courneya K. A randomized trial of a lifestyle intervention in obeseendometrial cancer survivors: quality of life outcomes and media-tors of behavior change. Health Qual Life Outcomes. 2009;7:17.
74. Christy SM, Mosher CE, Sloane R, Snyder DC, Lobach DF,Demark-Wahnefried W. Long-term dietary outcomes of theFRESH START intervention for breast and prostate cancer survi-vors. J Am Diet Assoc. 2011;111:1844–51.
75. Michie S, Ashford S, Sniehotta FF, Dombrowski SU, Bishop A,French DP. A refined taxonomy of behaviour change techniques tohelp people change their physical activity and healthy eating behav-iours: the CALO-RE taxonomy. Psychol Health. 2011;26:1479–98.
76. Michie S, Richardson M, Johnston M, Abraham C, Francis J,Hardeman W, et al. The behavior change technique taxono-my (v1) of 93 hierarchically clustered techniques: buildingan international consensus for the reporting of behaviorchange interventions. Ann Behav Med. 2013;46:81–95.
77. Norris JM, Culos-Reed SN, Carlson LE, Aldous SH. Utilizing theTPB for understanding yoga participation in cancer survivors. JSport Exerc Psychol. 2007;29:S194-S.
78. Mosher CE, Fuemmeler BF, Sloane R, Kraus WE, LobachDF, Snyder DC, et al. Change in self-efficacy partially me-diates the effects of the FRESH START intervention oncancer survivors’ dietary outcomes. Psychooncology.2008;17:1014–23.
79. Cohen J. Statistical power analysis for the behavioral sciences. 2nded. New Jersey: Lawrence Erlbaum Associates; 1988.
80. Greaves CJ, Sheppard KE, Abraham C, Hardeman W, Roden M,Evans PH, et al. Systematic review of reviews of interventioncomponents associated with increased effectiveness in dietary andphysical activity interventions. BMC Public Health. 2011;11:119.
81. Michie S, Abraham C, Whittingham C, McAteer J, Gupta S.Effective techniques in healthy eating and physical activityinterventions: a meta-regression. Health Psychol. 2009;28:690–701.
J Cancer Surviv (2015) 9:305–338 337

82. Short CE, James EL, Stacey F, Plotnikoff RC. A qualitative synthe-sis of trials promoting physical activity behaviour change amongpost-treatment breast cancer survivors. J Cancer Surviv. 2013.
83. Spark LC, Reeves MM, Fjeldsoe BS, Eakin EG. Physical activityand/or dietary interventions in breast cancer survivors: a systematicreview of the maintenance of outcomes. J Cancer Surviv. 2013.
84. Nigg CR, Long CR. A systematic review of single health behaviorchange interventions vs. multiple health behavior change interven-tions among older adults. TBM. 2012;2:163–79.
85. Webb TL, Sheeran P. Does changing behavioral intentions engenderbehavior change? A meta-analysis of the experimental evidence.Psychol Bull. 2006;132:249–68.
86. Williams DM, Anderson ES, Winett RA. A review of the outcomeexpectancy construct in physical activity research. Ann BehavMed.2005;29:70–9.
87. Anderson ES, Winett RA, Wojcik JR, Williams DM. Social cogni-tive mediators of change in a group randomized nutrition andphysical activity intervention: social support, self-efficacy, outcomeexpectations and self-regulation in the guide-to-health trial. J HealthPsychol. 2010;15:21–32.
88. Prestwich A, Sniehotta FF, Whittington C, Dombrowski SU,Rogers L, Michie S. Does theory influence the effectiveness ofhealth behavior interventions? Meta-analysis. Health Psychol.2013;33:465–74.
89. Avery KNL, Donovan JL, Horwood J, Lane JA. Behavior theory fordietary interventions for cancer prevention: a systematic review ofutilization and effectiveness in creating behavior change. CancerCauses Control. 2013;24:409–20.
90. Broekhuizen K, Kroeze W, Poppel MNM, Oenema A, Brug J. Asystematic review of randomized controlled trials on the effective-ness of computer-tailored physical activity and dietary behaviorpromotion programs: an update. Ann BehavMed. 2012;44:259–86.
91. Moher D, Hopewell S, Schulz KF, Montori V, Gotzsche PC,Devereaux PJ, et al. CONSORT 2010 explanation and elaboration:updated guidelines for reporting parallel group randomised trials.BMJ. 2010;340:c869.
92. Higgins JPT, Green S. Cochrane handbook for systematic reviewsof interventions version 5.1.0 [updated March 2011]: The CochraneCollaboration; 2011. Available from: www.cochrane-handbook.org.
93. Livingston PM, Salmon J, Courneya KS, Gaskin CJ, Craike M,Botti M, et al. Efficacy of a referral and physical activity programfor survivors of prostate cancer [ENGAGE]: rationale and designfor a cluster randomised controlled trial. BMCCancer. 2011;11:237.
94. Rogers LQ, McAuley E, Anton PM, Courneya KS, Vicari S,Hopkins-Price P, et al. Better exercise adherence after treatmentfor cancer (BEAT Cancer) study: rationale, design, and methods.Contemp Clin Trials. 2012;33:124–37.
95. James EL, Stacey F, Chapman K, Lubans DR, Asprey G, SundquistK, et al. Exercise and nutrition routine improving cancer health(ENRICH): the protocol for a randomized efficacy trial of a nutritionand physical activity program for adult cancer survivors and carers.BMC Public Health. 2011;11:236.
96. Blackburn GL, Wang KA. Dietary fat reduction and breast canceroutcome: results from the Women’s Intervention Nutrition Study(WINS). Am J Clin Nutr. 2007;86(suppl):878S–81S.
97. Chlebowski RT, Blackburn GL, Thomson CA, Nixon DW, ShapiroA, Hoy MK, et al. Dietary fat reduction and breast cancer outcome:interim efficacy results from the Women’s Intervention NutritionStudy. J Natl Cancer Inst. 2006;98:1767–76.
98. Hoy MK, Winters BL, Chlebowski RT, Papoutsakis C, Shapiro A,LubinMP, et al. Implementing a low-fat eating plan in theWomen’sIntervention Nutrition Study. J Am Diet Assoc. 2009;109:688–96.
99. Pierce JP, Natarajan L, Caan BJ, Parker BA, Greenberg RE, FlattSW, et al. Influence of a diet very high in vegetables, fruit, and fiberand low in fat on prognosis following treatment for breast cancer:TheWomen’s Healthy Eating and Living (WHEL) randomized trial.J Am Med Assoc. 2007;298:289–98.
100. Pierce JP, Natarajan L, Sun S, Al-Delaimy W, Flatt SW, Kealey S,et al. Increases in plasma carotenoid concentrations in response to amajor dietary change in the Women’s Healthy Eating and Livingstudy. Cancer Epidemiol Biomarkers Prev. 2006;15:1886–92.
101. Carmack Taylor CL, Demoor C, Smith MA, Dunn AL, Basen-Engquist K, Nielsen I, et al. Active for Life After Cancer: a ran-domized trial examining a lifestyle physical activity program forprostate cancer patients. Psychooncology. 2006;15:847–62.
102. Morey MC, Snyder DC, Sloane R, Cohen HJ, Peterson B, HartmanTJ, et al. Effects of home-based diet and exercise on functionaloutcomes among older, overweight long-term cancer survivors:RENEW: a randomized controlled trial. J Am Med Assoc.2009;301:1883–9.
103. Snyder DC, Morey MC, Sloane R, Stull V, Cohen HJ, Peterson B,et al. Reach out to Enhance Wellness in Older Cancer Survivors(RENEW): design, methods and recruitment challenges of a home-based exercise and diet intervention to improve physical functionamong long-term survivors of breast, prostate, and colorectal cancer.Psychooncology. 2009;18:429–39.
104. Twiss JJ,WaltmanNL, Berg K, Ott CD, Gross GJ, Lindsey AM. Anexercise intervention for breast cancer survivors with bone loss. JNurs Scholarsh. 2009;41:20–7.
105. Michie S, Prestwich A. Are interventions theory-based?Development of a theory coding scheme. Health Psychol.2010;29:1–8.
106. Strasser B, Steindorf K, Wiskemann J, Ulrich CM. Impact ofresistance training in cancer survivors: a meta-analysis. Med SciSports Exerc. 2013;45:2080–90.
107. Hutchison AJ, Breckon JD, Johnston LH. Physical activity behaviorchange interventions based on the transtheoretical model: a system-atic review. Health Educ Behav. 2008;36:829–45.
108. Painter JE, Borba CPC, Hynes M, Mays D, Glanz K. The use oftheory in health behavior research from 2000 to 2005: a systematicreview. Ann Behav Med. 2008;35:358–62.
109. Lawler SP, Winkler E, Reeves MM, Owen N, Graves N, Eakin EG.Multiple health behavior changes and co-variation in a telephonecounseling trial. Ann Behav Med. 2010;39:250–7.
110. White SM, McAuley E, Estabrooks PA, Courneya KS. Translatingphysical activity interventions for breast cancer survivors into prac-tice: an evaluation of randomized controlled trials. Ann BehavMed.2009;37:10–9.
111. Reedy J, Haines PS, Campbell MK. The influence of health behav-ior clusters on dietary change. Prev Med. 2005;41:268–75.
112. Ko LK, Campbell MK, LewisMA, Earp J, DeVellis B.Mediators offruit and vegetable consumption among colorectal cancer survivors.J Cancer Surviv. 2010;4:149–58.
113. Wilkinson AV, Barrera SL, McBride CM, Snyder DC, Sloane R,Meneses KM, et al. Extant health behaviors and uptake of standard-ized vs tailored health messages among cancer survivors enrolled inthe FRESH START trial: a comparison of fighting-spirits vs fatal-ists. Psychooncology. 2012;21:108–13.
338 J Cancer Surviv (2015) 9:305–338





























