Embed Size (px)
Citation preview
A Three-Week Intensive Pediatric Physical Therapy Plan of Care for a Child with Spastic Quadriplegia Cerebral Palsy: A Case Report
Brandie Schmierer, DPT student; Kirsten Buchanan, PhD, PT, ATC University of New England, Department of Physical Therapy, Portland, Maine
The benefits of physical therapy (PT) on gross motor function and general strength in children with spastic quadriplegia cerebral palsy (CP) are well documented.1, 2, 3, 4
There have been no firm conclusions that have determined the optimal duration and intensity of PT interventions for patients with spastic quadriplegia CP.5
The purpose of this case report was to investigate an intensive course of PT for 3 hours a day, 5 days a week, for 3 weeks in a pediatric patient with spastic quadriplegia CP.
CP occurs as a result of a brain injury associated with birth. Worldwide the prevalence of CP was 1.5 to 3.0 per 1,000 live births in
2009.6
Previous research demonstrated that PT intervention in children with CP improved gross motor function and strength, decreased the assistance required for mobility, and decreased step length differences.3,7
Current research supports a high frequency schedule of PT, however, the optimal intensity and duration of PT has not been determined.5
2 year old female with infantile spastic quadriplegia CP, Gross Motor Function Classification System (GMFCS) level V.
The patient had a history of seizures and gastroesophageal disease. The patient received Botox injections to bilateral pectoral and
hamstring musculature a month prior to treatment. Her primary impairments were decreased muscle strength and
endurance and abnormal muscle tone leading to a lack of independent age appropriate ambulation and gross motor skills.
PBWSTT: Partial Body Weight Supported Treadmill Training
Modified Ashworth Scale: 2 for all major joints in all extremities Full passive range of motion at all extremities
UEs: upper extremities; LEs: Lower extremities
As a result of a 3 week intensive PT session, improvements were noted in gross motor function and strength in a 2 year old with spastic quadriplegia CP.
The dynamic systems theory provides a rationale for use of task-specific, highly repetitious activities for the patient to be an active participant in motor learning.
Future research should continue to investigate the ideal treatment interval and intensity necessary for optimal PT outcomes.
1. Damiano DL, Abel MF. Functional outcomes of strength training in spastic cerebral palsy. Arch Phys Med Rehabil. 1998;79(2):119-25. PubMed PMID: 9473991.
2. Blundell SW, Shepherd RB, Dean CM, Adams RD, Cahill BM. Functional strength training in cerebral palsy: a pilot study of a group circuit training class for children aged 4-8 years. Clin Rehabil. 2003;17(1):48-57. PubMed PMID: 12617379.
3. Begnoche DM, Pitetti KH. Effects of traditional treatment and partial body weight treadmill training on the motor skills of children with spastic cerebral palsy. A pilot study. Pediatr Phys Ther. 2007;19(1):11-9. PubMed PMID: 17304093.
4. Curtis DJ, Butler P, Saavedra S, Bencke J, Kallemose T, Sonne-Holm S, Woollacott M. The central role of trunk control in the gross motor function of children with cerebral palsy: a retrospective cross-sectional study. Dev Med Child Neurol. 2015;57(4):351-7. doi: 10.1111/dmcn.12641.
5. Størvold GV, Jahnsen R. Intensive motor skills training program combining group and individual sessions for children with cerebral palsy. Pediatr Phys Ther. 2010;22(2):150-9. doi: 10.1097/PEP.0b013e3181dbe379.
6. Arneson CL, Durkin MS, Benedict RE, Kirby RS, Yeargin-Allsopp M, Van Naarden Braun K, Doernberg NS. Prevalence of cerebral palsy: Autism and Developmental Disabilities Monitoring Network, three sites, United States, 2004. Disabil Health J. 2009;2(1):45-8. doi: 10.1016/j.dhjo.2008.08.001.
7. Sorsdahl AB, Moe-Nilssen R, Kaale HK, Rieber J, Strand LI. Change in basic motor abilities, quality of movement and everyday activities following intensive, goal-directed, activity-focused physiotherapy in a group setting for children with cerebral palsy. BMC Pediatr. 2010;10:26. doi: 10.1186/1471-2431-10-26.
None
Kirsten Buchanan, PhD, PT, ATC Danielle Guerin, DPT
Interventions Week One – Three
Manual Therapy
PROM to all major joints at all extremities into flexion and extension.
• PROM for torso rotation.
Motor Function Training
Rolling Prone press up onto
forearms Prone to quadruped
transitions Quadruped holds Taylor sitting Anterior propped sitting Straddle sit over peanut
90/90 sitting on bench with reaching Sit to stand from low bench Supported standing Lateral protective extension Ambulation and supported standing in
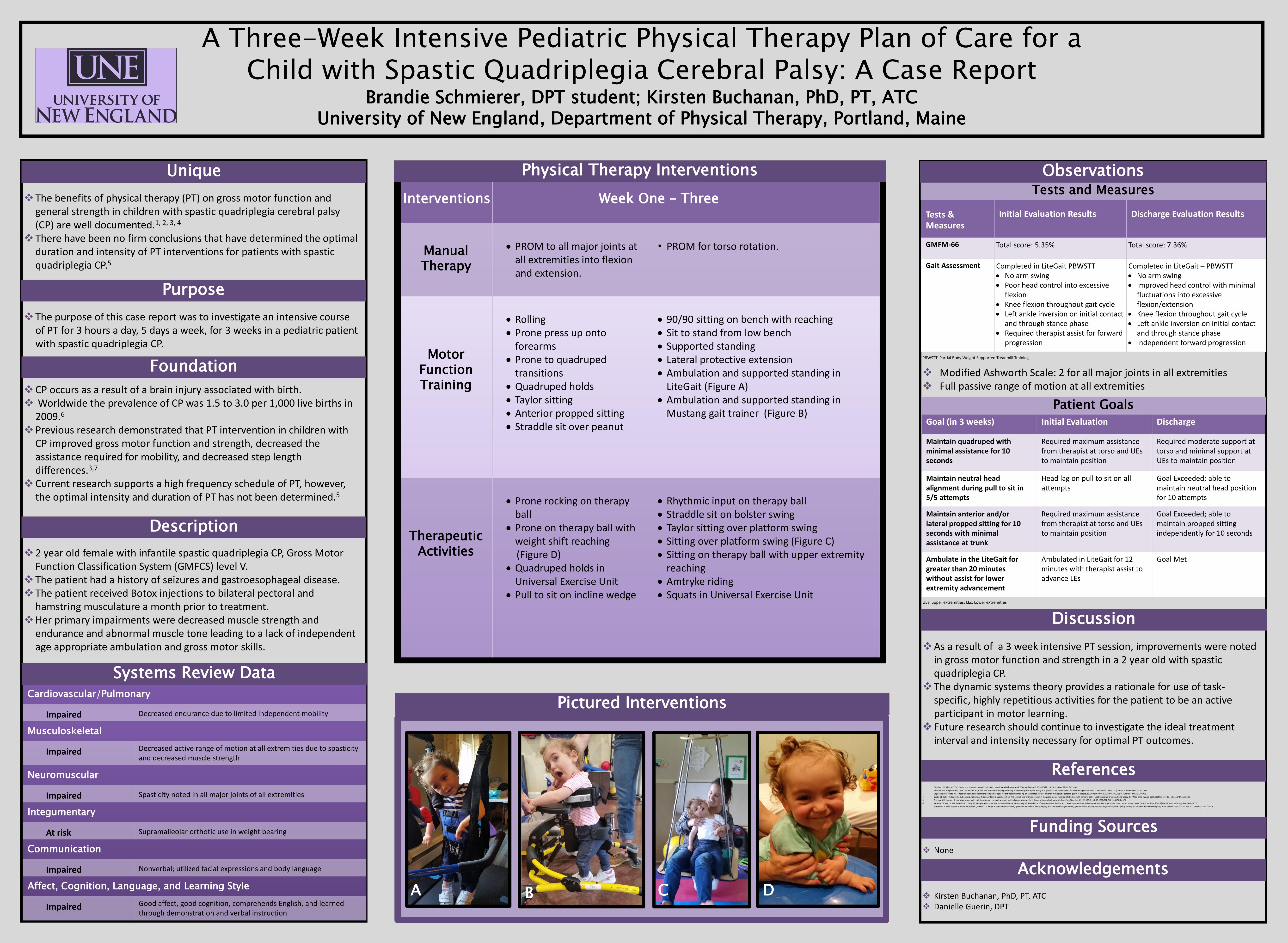
LiteGait (Figure A) Ambulation and supported standing in
Mustang gait trainer (Figure B)
Therapeutic Activities
Prone rocking on therapy ball
Prone on therapy ball with weight shift reaching
(Figure D) Quadruped holds in
Universal Exercise Unit Pull to sit on incline wedge
Rhythmic input on therapy ball Straddle sit on bolster swing Taylor sitting over platform swing Sitting over platform swing (Figure C) Sitting on therapy ball with upper extremity
reaching Amtryke riding Squats in Universal Exercise Unit
Goal (in 3 weeks) Initial Evaluation Discharge
Maintain quadruped with minimal assistance for 10 seconds
Required maximum assistance from therapist at torso and UEs to maintain position
Required moderate support at torso and minimal support at UEs to maintain position
Maintain neutral head alignment during pull to sit in 5/5 attempts
Head lag on pull to sit on all attempts
Goal Exceeded; able to maintain neutral head position for 10 attempts
Maintain anterior and/or lateral propped sitting for 10 seconds with minimal assistance at trunk
Required maximum assistance from therapist at torso and UEs to maintain position
Goal Exceeded; able to maintain propped sitting independently for 10 seconds
Ambulate in the LiteGait for greater than 20 minutes without assist for lower extremity advancement
Ambulated in LiteGait for 12 minutes with therapist assist to advance LEs
Goal Met
Tests & Measures
Initial Evaluation Results Discharge Evaluation Results
GMFM-66 Total score: 5.35% Total score: 7.36%
Gait Assessment Completed in LiteGait PBWSTT No arm swing Poor head control into excessive
flexion Knee flexion throughout gait cycle Left ankle inversion on initial contact
and through stance phase Required therapist assist for forward
progression
Completed in LiteGait – PBWSTT No arm swing Improved head control with minimal
fluctuations into excessive flexion/extension
Knee flexion throughout gait cycle Left ankle inversion on initial contact
and through stance phase Independent forward progression
Physical Therapy Interventions
Cardiovascular/Pulmonary
Impaired Decreased endurance due to limited independent mobility
Musculoskeletal
Impaired Decreased active range of motion at all extremities due to spasticity and decreased muscle strength
Neuromuscular
Impaired Spasticity noted in all major joints of all extremities
Integumentary
At risk Supramalleolar orthotic use in weight bearing
Communication
Impaired Nonverbal; utilized facial expressions and body language
Affect, Cognition, Language, and Learning Style
Impaired Good affect, good cognition, comprehends English, and learned through demonstration and verbal instruction
Systems Review Data
Tests and Measures
Pictured Interventions
Patient Goals
Unique
Purpose
Foundation
Description
Observations
Discussion
References
Funding Sources
Acknowledgements
A D B C