Embed Size (px)
Citation preview

87 (2006) 100–108www.elsevier.com/locate/schres
Schizophrenia Research
A volumetric MRI and magnetization transfer imaging follow-upstudy of patients with first-episode schizophrenia
Gary Price a,⁎, Mara Cercignani a, Manjinder S. Bagary a, Thomas R.E. Barnes b,Gareth J. Barker c, Eileen M. Joyce a, Maria A. Ron a
a Department of Neuroinflammation, Institute of Neurology, University College London, Queen Square, London, WC1N 3BG, UKb Imperial College Faculty of Medicine, Charing Cross Campus, London, UK
c King's College London, Institute of Psychiatry, Department of Clinical Neuroscience, Centre for Neuroimaging Sciences, London, UK
Received 2 February 2006; received in revised form 17 May 2006; accepted 9 June 2006Available online 14 July 2006
Abstract
Conventional MRI studies have not provided definitive evidence of progressive loss of brain volume in the early stages ofschizophrenia, although more subtle changes may have gone undetected. We have looked for such subtle changes using volumetricMRI and magnetization transfer imaging (MTI), an advanced MRI technique sensitive to subtle neuropathological abnormalities.Magnetization transfer images and high-resolution volumetric T1-weighted images were acquired from 16 patients with first-episode schizophrenia at the start of the study and 3.7years later. A group of 12 healthy controls were also scanned on twooccasions. Images were processed using a voxel-based approach that allows whole-brain analysis. There was a group differencewith a significant volume loss in the patients' white matter adjacent to the lateral ventricles in the right and left temporal lobes, inmedial temporal gyrus, and in the white matter in and around the right middle frontal gyrus. No cortical differences were detectedbetween the groups using MTI or volumetric MRI. The absence of any time-by-group interaction suggests that these abnormalitiesdo not progress in the early stages of the disease. The results of the study need to be interpreted in the light of the small sample sizeand of the limitations of current image analysis methods.© 2006 Elsevier B.V. All rights reserved.
Keywords: First-episode schizophrenia; Follow-up; Volumetric MRI; Magnetization transfer imaging; Voxel-based morphometry
1. Introduction
The most consistent finding in magnetic resonanceimaging (MRI) studies in schizophrenia is a reduction inbrain volume (Lawrie and Abukmeil, 1998; Shenton etal., 2001) and enlargement of lateral ventricles (Shenton
⁎ Corresponding author. Tel.: +44 207 837 3611x4170; fax: +44 207278 5616.
E-mail address: [email protected] (G. Price).
0920-9964/$ - see front matter © 2006 Elsevier B.V. All rights reserved.doi:10.1016/j.schres.2006.06.019
et al., 2001). However, the time course of these andother brain changes is debatable. It has also been shownthat certain brain MRI abnormalities are already evidentby the first episode of illness (Gur et al., 2000; Panteliset al., 2003) and may be present in unaffected relatives(McDonald et al., 2004). Recent studies using magne-tization transfer imaging (MTI), an MRI techniquesensitive to subtle neuropathological changes, havereported diffuse cortical abnormalities in people withchronic schizophrenia (Foong et al., 2001) and focalabnormalities in the medial prefrontal cortex, insula, and

101G. Price et al. / Schizophrenia Research 87 (2006) 100–108
fasciculus uncinatus in first-episode patients in theabsence of detectable atrophy (Bagary et al., 2003).
The histological abnormalities that underlie theseimaging changes are subtle. Decreases in neuronal sizein hippocampus and neocortex with reduced dendriticarborisation and synaptic abnormalities (Blennow et al.,1996), together with reduction in the number ofoligodendrocytes, have been described (Uranova et al.,2004). These abnormalities may be genetically deter-mined (see Harrison and Weinberger, 2005, for areview), and may represent the structural basis of thefunctional “disconnectivity” that may explain thesymptoms and cognitive impairment of schizophrenia(Harrison and Eastwood, 2001).
The natural history of the neuropathology ofschizophrenia is still unclear. Longitudinal imagingstudies have not provided clear evidence of progression(see Shenton et al., 2001 for a review). However, theapparent clinical deterioration of some patients overtime and reports suggesting progressive volumetric loss(Woods et al., 1990; DeLisi et al., 1995; Rapoport et al.,1999; Ho et al., 2003) have rekindled interest in thenotion of neurodegeneration as an alternative to a non-progressive neurodevelopmental pathology, even ifneuropathological studies have so far failed to supportsuch an hypothesis (Arnold et al., 1998; Purohit et al.,1998; Falke et al., 2000).
Here we present data from a volumetric MRI andMTI follow-up study of first-episode schizophreniapatients. MTI is based on the interaction betweenprotons bound to macromolecular structures (e.g.myelin and cell membranes) and free protons in tissuewater (Wolff and Balaban, 1989). If the bound protons(which are invisible to conventional MRI) arepreferentially saturated using an off-resonance radio-frequency pulse, this saturation is transferred to thefree pool by cross-relaxation and chemical exchange,resulting in decreased signal from the MR-visible freewater. The amount of signal loss, measured inpercentage units, is the magnetization transfer ratio(MTR) which is highly reproducible in normalsubjects rescanned at intervals (Barker et al., 1996).MTR depends on the density of macromolecules in agiven tissue and pathological processes that damagethe macromolecular structure will result in MTRreductions. We used voxel-based morphometry(VBM) (Ashburner and Friston, 2000; Good et al.,2001) to analyze the T1-weighted data sets and asimilar voxel-based method for the MTR data sets.VBM is an automated method that avoids operatorbias and yields information about the whole brainwithout an a priori selection of possibly abnormal
brain regions. It has recently been applied to the studyof brain abnormalities in schizophrenia and otherpsychiatric disorders (Kubicki et al., 2002; Moorheadet al., 2004).
2. Methods
2.1. Subjects
The subjects participating in this follow-up study hadtaken part in a previously reported cross sectional studyof first-episode schizophrenia (Bagary et al., 2003). Thepatients were initially recruited and scanned within1month of their first presentation to psychiatric serviceswith a first-episode of psychosis with the diagnosis ofschizophrenia according to DSM-IV criteria subse-quently being confirmed in all patients. The meaninterval between the initial and the follow-up examina-tion was 3.7years. Of the 30 patients who were part ofthe original study, 12 were not available for follow-up: 3had moved away and could not be contacted, 8 refusedto participate, and one had died. Eighteen patientsagreed to undergo scanning but two could not toleratethe procedure. This resulted in a final group of 16patients (12 males and 4 females), with a mean age of26.3years at baseline (range 16–45) and 29.9years(range 19–49) at follow-up. All participants werereviewed by experienced clinicians (EJ and TREB)after recruitment. Patients' symptoms were alsoassessed with the Scales for the Assessment of PositiveSymptoms (SAPS) (Andreasen, 1981) and NegativeSymptoms (SANS) (Andreasen, 1983). Scores forpositive, disorganisation and negative syndromes ofschizophrenia (Liddle and Barnes, 1990) were calcu-lated for each patient by summing the SAPS and SANSglobal sub-scale scores relevant to each factor. Anti-psychotic medication being taken at the time of bothscans was recorded.
Thirty healthy volunteers had taken part in theoriginal study (Bagary et al., 2003) and 12 returned forfollow-up (4 males and 8 females); their mean ages were31.6years at baseline (range 21–48years) and 36yearsat follow-up (range 26–50years). The mean intervalbetween scans was 4.4years. The criteria for exclusionfor patients and controls were a history of head injury,neurological or systemic illness, a history of substanceabuse during the study, or alcohol intake above 210g/week during the study period. Controls with a history ofpsychiatric illness were also excluded. The study wasapproved by the relevant research Ethics Committeesand written informed consent was obtained from allsubjects.

102 G. Price et al. / Schizophrenia Research 87 (2006) 100–108
2.2. MRI
MRI scans for all subjects were obtained using astandard quadrature head coil on a GE Signa 1.5 Teslascanner (General Electric, Milwaukee, WI), whichunderwent regular quality-control checks. The sameMRI scanner and an identical scanning protocol to thatused in the original study (Bagary et al., 2003) wereused at follow-up. A preliminary sagittal localizing scanwas acquired, which was also used to check headposition for the follow-up scan. High-resolution coronalvolumetric images were acquired using a 3-dimensionalinversion-recovery prepared T1-weighted spoiled gra-dient recalled (SPGR) echo sequence generating 124contiguous, 1.5-mm coronal slices (echo time [TE]4.2ms, repetition time [TR] 15ms, inversion time [TI]450ms, field of view [FOV] 24cm2, 256×192 matrix,flip angle 20°). The 1×1.2×1.5-mm voxel size atacquisition was determined by scan time constraints,and images were automatically reconstructed by thescanner at a 1×1×1.5 mm voxel size.
Axial magnetization transfer (MT) images wereacquired using a dual spin-echo-based MT sequence(TE 30/80ms, TR 1720ms, 28 contiguous 5-mm axialslices, 256×128 pixel image matrix, 24cm2 FOV) withand without a saturation pulse (16ms, 23.2μT Hammingappodized 3-lobe sinc pulse applied 1KHz from waterresonance). The 1×2×5 mm voxel size was againdetermined by scan time constraints, and the scannerautomatically reconstructed the images at a 1×1×5 mmvoxel size. The MT sequence (Barker et al., 1996)generates proton-density and T2-weighted images alongwith MT-weighted images. These images are allinherently registered to each other, and to the calculatedMTR image created from proton-density and MT-weighted images.
2.3. Image processing
Data were processed on a Sun workstation (SunMicrosystems, Santa Clara, CA). First MTR maps werecalculated on a pixel-by-pixel basis from the formula:MTR={[Mo−Ms]/Mo}×100, where Ms and Mo aremean signal intensities with and without the saturationpulse, respectively. MTR is not calculated in voxelswhere values in source images are below a thresholddetermined by the mean background noise level. Weused the 30-ms (first) echo for MT calculation becausethe resulting map has higher signal-to-noise ratio thanthat from the 80-ms echo. For our spin-echo sequence,typical MTR values were approximately 40pu (percen-tage units) for white matter, 35pu for subcortical grey
matter, 32pu for cortical grey matter, and 2pu(demonstrating the minimal direct saturation effects)for CSF.
The following steps of the processing wereperformed using SPM2 (Wellcome Department ofCognitive Neurology, London, UK) in MATLAB(MathWorks, Natick, MA) (Fig. 1). First, the proton-density weighted scans from the MT sequences atbaseline and at follow-up were each coregistered to thecorresponding SPGR volume, using normalized mutualinformation as the cost function (Studholme et al.,1996). The SPGR volume at follow-up was thencoregistered to the SPGR volume at baseline, and thetransformation determined was applied to the follow-up MTR scan. At this stage all images were in thespace of the baseline SPGR volume. The SPGRvolumes were then segmented to produce images ofthe grey matter ‘shell’, both at baseline and follow-up(Ashburner and Friston, 2000). An average of thebaseline and follow-up grey matter shells was thennormalized to the SPM grey matter template, and thetransformation thus determined was applied to thecoregistered SPGR and MTR images. This approachwas chosen, instead of normalizing each time pointseparately, in order to preserve small changes thatmight have occurred over the follow-up period. Finally,the normalized SPGRs were then segmented toproduce images of grey matter and white mattervolume in normalized space.
2.4. Smoothing
To improve signal-to-noise ratio, the segmented greymatter and white matter images were smoothed using a6-mm full-width-half-maximum (FWHM) Gaussianfilter. This procedure also allows for anatomicalvariability between subjects and has the effect ofnormalizing the distribution of the error terms in thedata. After smoothing, the individual voxel intensitybecomes the locally weighted average of grey matterdensity (Ashburner and Friston, 2000). Smoothingensures the validity of inferences based on parametrictests according to the central limit theorem (Salmond etal., 2002) and sensitizes the analysis to features of a sizedetermined by the smoothing kernel width (the ‘matchedfilter theorem’). Thus the size of the kernel can have asignificant effect on the results of the analysis (asdemonstrated, albeit for a different type of data, byJones et al., 2005). We selected a priori a smallsmoothing kernel (6mm) to match the expected smallextent of changes taking place during the follow-upperiod (see Shenton et al., 2001). A similar smoothing

Fig. 1. Image processing steps using SPM2. GM, grey matter; MTR, magnetic transfer ratio; PD, Proton Density; PDW, Proton Density Weighted;WM, white matter.
103G. Price et al. / Schizophrenia Research 87 (2006) 100–108
procedure using 6-mm FWHM was performed on theMTR images.
Since we were interested in estimating groupdifferences over time, as well as differences betweengroups at baseline, for each image type (MTR, whitematter and grey matter maps) we computed a ‘sum’ anda ‘difference’ image between the normalized andsmoothed image at follow-up and the normalized andsmoothed image at baseline. As this step was performedfor each subject, this gave a total of 28 ‘difference’images and 28 ‘summed’ images for each grey matter,white matter and MTR image set. These combinedimages were used for the statistical comparison asexplained below.
2.5. Statistical analysis
Statistical comparisons of both grey and white mattervolumes, and of MTR maps, were performed usingSPM2, which is based upon the general linear model andthe theory of Gaussian random fields (Friston et al.,1994). Two ANCOVAmodels were used to compare the‘difference’ and the ‘sum’ images between patients andcontrols:
(1) The ‘difference’ images were used to assess themain effect of time, by means of the T contrast
[1, 1], as well as the group-by-time interaction, bymeans of the T contrast [1, −1].
(2) The ‘sum’ images were used to assess the groupeffect, by means of the T contrast [1, −1].
This type of analysis, recommended as a way ofimplementing a repeated-measure ANCOVA in SPM(http://www.jiscmail.ac.uk/lists/spm.htm), also pre-vents the differences already present at baselinebetween patients and controls from masking subse-quent changes.
In both comparisons we accounted for age, sex andscan interval for each subject as nuisance variables. Thechoice of age and sex as nuisance variables was basedon previous studies demonstrating regional anatomicaldifferences in normal subjects related to these variables(Xu et al., 2000; Good et al., 2001).
3. Results
There were no significant differences in age betweenthe patient and control groups (t(26)=0.076). However,there were significant differences in gender, with moremales in the patient group (χ2(1)=0.027) (Table 1).When patients in the current study were compared withthose from the original study who were not available forfollow-up, there were no baseline differences in age (t

Table 1Demographic data of follow-up patients and controls
Demographic data Patients (n=16) Controls (n=12)
Age at baseline[mean (range)]
26.3 (16–45) years 31.6 (21–48) years
Age at follow-up[mean (range)]
29.9 (19–49) years 36 (26–50) years
Males:females 3:1 1:2⁎NART IQ (mean±range)at baseline
100.3 (75–121) 110.9 (93–126)
Mean follow-up period(range in days)
1329days 1606days3.64years 4.4years(709–1801) (1198–1877)
⁎NART, National Adult Reading Test (Nelson, 1982), an estimate ofpremorbid IQ.
104 G. Price et al. / Schizophrenia Research 87 (2006) 100–108
(28)=−0.52), gender ratio (χ2(1)=0.05), premorbid IQ(t(27)=−0.79),ordurationofuntreatedpsychosis (t(28)=−0.79). An assessment of baseline symptoms scoresrevealed that there were no significant differences innegative symptoms (t(28)=0.382), positive symptoms(t(28)=0.167) or disorganization symptoms (t(28)=0.053) between these two patient groups. One yearfrom the onset of the study, quantitative clinical datawere available in 10 of the 14 patients who failed toparticipate in the follow-up imaging study and in all 16who participated. Comparisons between the two groupsof patients revealed no significant differences on thescores for negative symptoms (t(24)=0.426), positivesymptoms (t(24)=0.827) and disorganization symp-toms (t(24)=0.075). These comparisons suggest thatthe subgroup that took part in the follow-up imagingstudy is representative of the original sample, at least inthe early stages of the disease. Unfortunately, at 3-yearfollow-up, quantitative clinical data were available foronly 3 of the 14 patients who did not take part in thefollow-up imaging study.
The clinical outcome of the patients reported in thisstudy was variable. Eight had been continuouslysymptomatic in the intervening period despite medica-tion, four had relapsed at least once or exhibited mildresidual symptoms and were receiving medication, andthe remaining four had been in full remission andmedication-free throughout. When first scanned, 7 ofthese patients were receiving first-generation (typical)and 9 second-generation (atypical) antipsychotics. Ofthe 12 patients who were taking medication on bothoccasions, 8 had remained on the same type ofantipsychotic (3 on first-generation and 5 on second-generation antipsychotics), and 4 had switched to adifferent type of drug (3 from first to second-generationantipsychotics). No gross structural brain abnormalitieswere reported at follow-up in any of the subjects when
the MRI images were visually inspected by anexperienced neuroradiologist.
3.1. Longitudinal changes in MTR and brain volume(time effect)
When patients and controls were considered as asingle group, there were no significant changes betweenbaseline and follow-up in MTR, white matter and greymatter volumes.
3.2. Comparisons of MTR and brain volumes betweenpatients and controls (group effect)
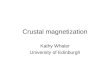
When the ‘sum’ images (initial and follow-up scans)of patients and controls were compared, there were nosignificant between-group differences in MTR or greymatter volume that survived corrections for multiplecomparisons. On the other hand, there were significantvolume losses (p<0.05) in the patients in the whitematter adjacent to the lateral ventricles in the right andleft temporal lobes, in medial temporal gyrus, and in thewhite matter in and around the right middle frontalgyrus, and this finding survived the false discovery rate(FDR) correction for multiple comparisons (Fig. 2).
3.3. Comparisons of change in MTR and brain volumesover time between patients and controls (group-by-timeinteraction)
There were no significant differences between thegroups in the magnitude of changes in MTR, white orgrey matter volumes during the follow-up period,suggesting that the changes in these parameters (i.e.white matter volume) were already present at baseline inthe patient group and did not change over time.
4. Discussion
In this small follow-up study of patients with first-episode schizophrenia using both conventional andadvanced MRI techniques, we found no evidence tosuggest a progression of brain abnormalities in theearly stages of the disease. Volumetric losses in whitematter were present in patients with schizophreniaearly in the disease, mostly in an area adjacent to thelateral ventricles and in and around the right middlefontal gyrus, areas that have previously been impli-cated in the illness (Shenton et al., 2001). Our findingsare in keeping with those of other studies showingreductions in white matter volume (Hulshoff Pol et al.,2004; Antonova et al., 2005), and in particular with

Fig. 2. SPM map of white matter reductions in patients vs. controls at baseline.
105G. Price et al. / Schizophrenia Research 87 (2006) 100–108
those of voxel based morphometric studies reportingwhite matter volume loss in frontal regions (Paillere-Martinot et al., 2001) and in areas adjacent to the leftfrontal and temporal cortex (Spalletta et al., 2003). Ourfindings are also in keeping with one of the mostrobust MRI findings in schizophrenia research, namelyventricular enlargement (Shenton et al., 2001; DeLisi
et al., 1997; Rapoport et al., 1997; Lieberman et al.,2001), which is likely to be related to a reduction ofwhite matter adjacent to the ventricles (Christensen etal., 2004).
In our original first-episode study (Bagary et al.,2003) MTI proved a valuable tool to detect grey matterabnormalities at baseline in a larger group of patients

106 G. Price et al. / Schizophrenia Research 87 (2006) 100–108
that included those reported here. The sample attrition atfollow-up is likely to explain our failure to detect suchabnormalities here, although the image analysis meth-odology used in this longitudinal study may also havecontributed to our negative findings.
The lack of evidence for progressive brain abnorm-alities in our study echoes the findings of others in theearly stages of the disease (Puri et al., 2001; Dickey etal., 2004; DeLisi and Hoff, 2005) and may be related tothe characteristics of our sample, as previous follow-upstudies have suggested that the evolution of brainabnormalities detected during the first episode isvariable and to some extent related to clinical outcomeand treatment, and that progressive changes, if present,may occur at different times and affect some brainareas preferentially. The results of these studies,including our own, have to be considered in the lightof their limitations, among which the small samplesizes and methodological variability are paramount.DeLisi and collaborators, following a group of patientsover a 10-year period, did not detect changes inventricular, hippocampal or temporal lobe volume inthe first 5years of the study, although ventricularenlargement occurred in the subsequent 5years in thosewith a poor clinical outcome (DeLisi et al., 1992, 1995,1997, 2004). Others (Nair et al., 1997) have describedearly ventricular enlargement with later stabilization.Lieberman et al. (2001), in a 6-year follow-up study,also described progressive ventricular enlargement inrelation to the course of illness, while cortical andhippocampal volumes remained unchanged. Severalstudies (Keshavan et al., 1998; Lieberman et al., 2001,2005; Chakos et al., 2005) have suggested thatantipsychotic drugs, in particular the second-generationdrugs, may prevent some of these changes. More recentstudies have also reported decreased frontal whitematter (Ho et al., 2003) in the early stages of theillness, and other studies have revealed progressivegrey matter changes (Mathalon et al., 2001; Shenton etal., 2001; Pantelis et al., 2003). A series of relatedstudies of childhood-onset schizophrenia (Thompson etal., 2001; Gogtay et al., 2004; Whitworth et al., 2005;Vidal et al., 2006) have found severe cortical volumeloss in this subgroup of patients with a particularly badprognosis.
Differences in image analysis are also important inexplaining the conflicting results of different follow-upstudies. We used a voxel-based method, because it hasthe advantage of exploring the whole brain, without anya priori hypothesis on the location of abnormalities, butthere are shortcomings to this method that limited itssensitivity to small changes. In particular, individual
anatomical variability (Rajkowska and Goldman-Rakic,1995), difficulty of coregistration (Ashburner andFriston, 2001; Bookstein, 2001) and overstringentstatistical corrections for multiple comparisons (Worsleyet al., 1996) which have all been discussed by others. Inthis context it is also important to mention that thechoice of the size of the smoothing kernel (6mm in ourcase), dictated by the magnitude of the expectedchanges, determines in turn the sensitivity of the methodand, therefore, our results should be interpreted asshowing lack of evidence for longitudinal changes of aspatial extent comparable to the size of our smoothingkernel, while more subtle changes would have goneundetected. We cannot exclude the possibility that theuse of a different smoothing kernel, or a less stringentanalysis (e.g. region of interest methodology), mighthave led to a different result.
Aside from these methodological considerations,there are other potential shortcomings of this study,such as the small sample size and the imperfectmatching between patients and controls. Both of theseproblems resulted from the difficulty in tracing some ofthe subjects from the original study (Bagary et al.,2003). The small sample size has prevented us fromexploring whether brain abnormalities evolve differ-ently in patients exposed to different types of neurolep-tics or with different clinical outcome. However, the sizeof our sample does not differ greatly from that of manyfollow-up studies (Chakos et al., 1994; DeGreef et al.,1991; Jacobsen et al., 1998; Keshavan et al., 1998; Nairet al., 1997; Rapoport et al., 1997, 1999; Kasai et al.,2003) and we have, as far as possible, controlled for thedifferences in age and gender between the groups bystatistical means.
Finally, our study does not rule out the possibilitythat progressive brain abnormalities may occur at a laterstage in the disease in relation to poor clinical outcomeor cognitive impairment, and a longer follow-up studyof a larger sample of patients will be required to answerthese questions.
Acknowledgements
This study was supported by a programme grant fromthe Wellcome Trust.
We are grateful to Professor David Miller and othermembers of the NMR Unit, Clare Foster for herassistance and Dr. Dan Altmann for his statisticaladvice. We thank all the subjects who participated in thisstudy and the consultants of West London and SouthWest London and St George's Mental Health NHSTrusts.

107G. Price et al. / Schizophrenia Research 87 (2006) 100–108
References
Andreasen, N.C., 1981. Scale for the Assessment of NegativeSymptoms (SANS). University of Iowa, Iowa City, IA.
Andreasen, N.C., 1983. Scale for the Assessment of PositiveSymptoms (SAPS). University of Iowa, Iowa City, IA.
Antonova, E., Kumari, V., Morris, R., Halari, R., Anilkumar, A.,Mehrotra, R., Sharma, T., 2005. The relationship of structuralalterations to cognitive deficits in schizophrenia: a voxel-basedmorphometry study. Biol. Psychiatry 15;58 (6), 457–467.
Arnold, S.E., Trojanowski, J.Q., Gur, R.E., Blackwell, P., Han, L.Y.,Choi, C., 1998. Absence of neurodegeneration and neural injury inthe cerebral cortex in a sample of elderly patients withschizophrenia. Arch. Gen. Psychiatry 55, 225–232.
Ashburner, J., Friston, K.J., 2000. Voxel based morphometry—themethods. Neuroimage 11, 805–821.
Ashburner, J., Friston, K.J., 2001. Why voxel-based morphometryshould be used. Neuroimage 14 (6), 1238–1243.
Bagary,M.S., Symms,M.R., Barker, G.J., Mutsatsa, S.H., Joyce, E.M.,Ron, M.A., 2003. Grey and white matter brain abnormalities infirst-episode schizophrenia inferred from magnetization transferimaging. Arch. Gen. Psychiatry 60, 779–788.
Barker, G.J., Tofts, P.S., Gass, A., 1996. An interleaved sequence foraccurate and reproducible clinical measurement of magnetizationtransfer ratio. Magn. Reson. Imaging 14, 403–411.
Blennow, K., Davidsson, P., Gottfries, C.-G., Ekman, R., Heilig, M.,1996. Synaptic degeneration in thalamus in schizophrenia [letter].Lancet 348, 692–693.
Bookstein, F.L., 2001. “Voxel-based morphometry” should not be usedwith imperfectly registered images. Neuroimage 14 (6),1454–1462.
Chakos, M.H., Lieberman, J.A., Bilder, R.M., Borenstein, M.,Lerner, G., Bogerts, B., Wu, H., Kinon, B., Ashtari, M., 1994.Increase in caudate nuclei volumes of first-episode schizophrenicpatients taking antipsychotic drugs. Am. J. Psychiatry 151,1430–1436.
Chakos, M.H., Schobel, S.A., Gu, H., Gerig, G., Bradford, D., Charles,C., et al., 2005. Duration of illness and treatment effects onhippocampal volume in male patients with schizophrenia. Br. J.Psychiatry 186, 26–31.
Christensen, J., Holcomb, J., Garver, D.L., 2004. State-related changesin cerebral white matter may underlie psychosis exacerbation.Psychiatry Res. 15;130 (1), 71–78.
DeGreef, G., Ashtari, M., Wu, H.W., Borenstein, M., Geisler, S.,Lieberman, J., 1991. Follow up MRI study in first episodeschizophrenia. Schizophr. Res. 5, 204–206.
DeLisi, L.E., Hoff, A.L., 2005. Failure to find progressive temporallobe volume decreases 10years subsequent to a first episode ofschizophrenia. Psychiatry Res. 138, 265–268.
DeLisi, L.E., Stritzke, P., Riordan, H., Holan, V., Boccio, A., Kushner,M., McClelland, J., Van Eyl, O., Anand, A., 1992. The timing ofbrain morphological changes in schizophrenia and their relation-ship to clinical outcome. Biol. Psychiatry 31, 241–254.
DeLisi, L.E., Tew, W., Xie, S., Hoff, A.L., Sakuma, M., Kushner, M.,et al., 1995. A prospective follow-up study of brain morphologyand cognition in first-episode schizophrenic patients: preliminaryfindings. Biol. Psychiatry 38, 349–360.
DeLisi, L.E., Sakuma, M., Tew, W., Kushner, M., Hoff, A.L.,Grimson, R., 1997. Schizophrenia as a chronic active brainprocess: a study of progressive brain structural change subsequentto the onset of schizophrenia. Psychiatry Res. 74, 129–140.
DeLisi, L.E., Sakuma, M., Maurizio, A.M., Relja, M., Hoff, A.L.,2004. Cerebral ventricular change over the first 10 years after theonset of schizophrenia. Psychiatry Res. 130, 57–70.
Dickey, C.C., Salisbury, D.F., Nagy, A.I., Hirayasu, Y., Lee, C.U.,McCarley, R.W., Shenton, M.E., 2004. Follow-up MRI study ofprefrontal volumes in first-episode psychotic patients. Schizophr.Res. 71, 349–351.
Falke, E., Han, L.Y., Arnold, S.E., 2000. Absence of neurodegenera-tion in the thalamus and caudate of elderly patients withschizophrenia. Psychiatry Res. 93, 103–110.
Foong, J., Symms, M.R., Barker, G.J., Maier, M., Woermann, F.G.,Miller, D.H., et al., 2001. Neuropathological abnormalities inschizophrenia: evidence from magnetization transfer imaging.Brain 124, 882–892.
Friston, K.J., Worsley, K., Frackowiak, R.S., Maziotta, J.C., Evans,A.C., 1994. Assessing the significance of focal activation usingtheir spatial extent. Hum. Brain Mapp. 1, 210–220.
Gogtay, N., Sporn, A., Clasen, L.S., Nugent III, T.F., Greenstein, D.,Nicolson, R., Giedd, J.N., Lenane, M., Gochman, P., Evans, A.,Rapoport, J.L., 2004. Comparison of progressive cortical graymatter loss in childhood-onset schizophrenia with that in child-hood-onset atypical psychoses. Arch. Gen. Psychiatry 61, 17–22.
Good, C.D., Johnsrude, I.S., Ashburner, J., Henson, R.N., Friston, K.J.,Frackowiak, R.S., 2001. A voxel-based morphometric study ofageing in 465 normal adult human brains. Neuroimage 14, 21–36.
Gur, R.E., Turetsky, B.I., Cowell, P.E., Finkelman, C., Maany, V.,Grossman, R.I., et al., 2000. Temporolimbic volume reductions inschizophrenia. Arch. Gen. Psychiatry 57, 769–775.
Harrison, P.J., Eastwood, S.L., 2001. Neuropathological studies ofsynaptic connectivity in the hippocampal formation in schizo-phrenia. Hippocampus 11, 508–519.
Harrison, P.J., Weinberger, D.R., 2005. Schizophrenia genes, geneexpression, and neuropathology: on the matter of their conver-gence. Mol. Psychiatry 10, 40–68.
Ho, B.C., Andreasen, N.C., Nopoulos, P., Arndt, S., Magnotta, V.,Flaum, M., 2003. Progressive structural brain abnormalities andtheir relationship to clinical outcome a longitudinal magneticresonance imaging study early in schizophrenia. Arch. Gen.Psychiatry 60, 585–594.
Hulshoff Pol, H.E., Brans, R.G., van Haren, N.E., Schnack, H.G.,Langen, M., Baare, W.F., van Oel, C.J., Kahn, R.S., 2004. Grayand white matter volume abnormalities in monozygotic and same-gender dizygotic twins discordant for schizophrenia. Biol.Psychiatry 15;55 (2), 126–130.
Jacobsen, L.K., Giedd, J., Castellanos, F.X., Vaituzis, A.C., Hambur-ger, S.D., Kumra, S., et al., 1998. Progressive reduction oftemporal lobe structures in childhood-onset schizophrenia. Am. J.Psychiatry 155, 678–685.
Jones, D.K., Symms, M.R., Cercignani, M., Howard, R.J., 2005. Theeffect of filter size on VBM analyses of DT-MRI data. Neuroimage26, 546–554.
Kasai, K., Shenton, M.E., Salisbury, D.F., Hirayasu, Y., Onitsuka, T.,Spencer, M.H., et al., 2003. Progressive decrease of left Heschlgyrus and planum temporale grey matter volume in first-episodeschizophrenia: a longitudinal magnetic resonance imaging study.Arch. Gen. Psychiatry 60, 766–775.
Keshavan, M.S., Haas, G.L., Kahn, C.E., Aguilar, E., Dick, E.L.,Schooler, N.R., Sweeney, J.A., Pettegrew, J.W., 1998. Superiortemporal gyrus and the course of early schizophrenia: progressive,static, or reversible? J. Psychiatr. Res. 32, 161–167.
Kubicki, M., Shenton, M.E., Salisbury, D.F., Hirayasu, Y., Kasai, K.,Kikinis, R., et al., 2002. Voxel-based morphometric analysis of

108 G. Price et al. / Schizophrenia Research 87 (2006) 100–108
grey matter in first episode schizophrenia. Neuroimage 17,1711–1719.
Lawrie, S.M., Abukmeil, S.S., 1998. Brain abnormality in schizo-phrenia. A systematic and quantitative review of volumetricmagnetic resonance imaging studies. Br. J. Psychiatry 172,110–120.
Liddle, P.F., Barnes, T.R., 1990. Syndromes of chronic schizophrenia.Br. J. Psychiatry 157, 558–561.
Lieberman, J., Chakos, M., Wu, Hu, Alvir, J., Hoffman, E., Robinson,D., et al., 2001. Longitudinal study of brain morphology in firstepisode schizophrenia. Biol. Psychiatry 49, 487–499.
Lieberman, J.A., Tollefson, G.D., Charles, C., Zipursky, R., Sharma,T., Kahn, R.S., et al., 2005. Antipsychotic drug effects on brainmorphology in first-episode psychosis. Arch. Gen. Psychiatry 62,361–370.
Mathalon, D.H., Sullivan, E.V., Lim, K.O., Pfefferbaum, A., 2001.Progressive brain volume changes and the clinical course ofschizophrenia in men: a longitudinal magnetic resonance imagingstudy. Arch. Gen. Psychiatry 58, 148–157.
McDonald, C., Bullmore, E.T., Sham, P.C., Chitnis, X., Wickham, H.,Bramon, E., et al., 2004. Association of genetic risks forschizophrenia and bipolar disorder with specific and genericbrain structural endophenotypes. Arch. Gen. Psychiatry 61,974–984.
Moorhead, T.W., Job, D.E., Whalley, H.C., Sanderson, T.L.,Johnstone, E.C., Lawrie, S.M., 2004. Voxel-based morphometryof comorbid schizophrenia and learning disability: analyses innormalized and native spaces using parametric and nonparametricstatistical methods. Neuroimage 22, 188–202.
Nair, T.R., Christensen, J.D., Kingsbury, S.J., Kumar, N.G., Terry,W.M., Garver, D.L., 1997. Progression of cerebroventricularenlargement and the subtyping of schizophrenia. PsychiatryRes. 74, 141–150.
Nelson, H.E., 1982. The National Adult Reading Test. NFER-NelsonPublishing, Windsor, Berks, UK.
Pantelis, C., Velakoulis, D., McGorry, P.D., Wood, S.J., Suckling, J.,Phillips, L.J., et al., 2003. Neuroanatomical abnormalities beforeand after onset of psychosis: a cross-sectional and longitudinalMRI comparison. Lancet 361, 281–288.
Paillere-Martinot, M., Caclin, A., Artiges, E., Poline, J.B., Joliot, M.,Mallet, L., Recasens, C., Attar-Levy, D., Martinot, J.L., 2001.Cerebral gray and white matter reductions and clinical correlates inpatients with early onset schizophrenia. Schizophr. Res. 30;50 (1-2), 19–26.
Puri, B.K., Hutton, S.B., Saeed, N., Oatridge, A., Hajnal, J.V., Duncan,L., et al., 2001. A serial longitudinal quantitative MRI study ofcerebral changes in first-episode schizophrenia using imagesegmentation and subvoxel registration. Psychiatry Res. 106,141–150.
Purohit, D.P., Perl, D.P., Haroutunian, V., Powchik, P., Davidson, M.,Davis, K.L., 1998. Alzheimer disease and related neurodegenera-tive diseases in elderly patients with schizophrenia: a postmortemneuropathologic study of 100 cases. Arch. Gen. Psychiatry 55,205–211.
Rajkowska, G., Goldman-Rakic, P.S., 1995. Cytoarchitectonic defini-tion of prefrontal areas in the normal human cortex: II. Variabilityin locations of areas 9 and 46 and relationship to the TalairachCoordinate System. Cereb. Cortex 5 (4), 323–337.
Rapoport, J.L., Giedd, J., Kumra, S., Jacobsen, L., Smith, A., Lee, P.,Nelson, J., Hamburger, S., 1997. Childhood-onset schizophrenia.Progressive ventricular change during adolescence. Arch. Gen.Psychiatry 54, 897–903.
Rapoport, J.L., Giedd, J.N., Blumenthal, J., Hamburger, S., Jeffries,N., Fernandez, T., et al., 1999. Progressive cortical change duringadolescence in childhood-onset schizophrenia. A longitudinalmagnetic resonance imaging study. Arch. Gen. Psychiatry 56,649–654.
Salmond, C.H., Ashburner, J., Vargha-Khadem, F., Connelly, A.,Gadian, D.G., Friston, K.J., 2002. Distributional assumptions invoxel-based morphometry. Neuroimage 17 (2), 1027–1030.
Shenton, M.E., Dickey, C.C., Frumin, M., McCarley, R.W., 2001. Areview of MRI findings in schizophrenia. Schizophr. Res. 49,1–52.
Spalletta, G., Tomaiuolo, F., Marino, V., Bonaviri, G., Trequattrini, A.,Caltagirone, C., 2003. Chronic schizophrenia as a brain mis-connection syndrome: a white matter voxel-based morphometrystudy. Schizophr. Res. 1;64 (1), 15–23.
Studholme, C., Hill, D.L.G., Hawkes, D.J., 1996. Automated three-dimensional registration of magnetic resonance and positronemission tomography brain images by multiresolution optimiza-tion of voxel similarity measures. Med. Phys. 24, 25–35.
Thompson, P.M., Vidal, C., Giedd, J.N., Gochman, P., Blumenthal, J.,Nicolson, R., et al., 2001. Mapping adolescent brain changereveals dynamic wave of accelerated gray matter loss in very early-onset schizophrenia. Proc. Natl. Acad. Sci. U. S. A. 98,11650–11655.
Uranova, N.A., Vostrikov, V.M., Orlovskaya, D.D., Rachmanova, V.I.,2004. Oligodendroglial density in the prefrontal cortex inschizophrenia and mood disorders: a study from the StanleyNeuropathology Consortium. Schizophr. Res. 67, 269–275.
Vidal, C.N., Rapoport, J.L., Hayashi, K.M., Geaga, J.A., Sui, Y.,McLemore, L.E., Alaghband, Y., Giedd, J.N., Gochman, P.,Blumenthal, J., et al., 2006. Dynamically spreading frontal andcingulate deficits mapped in adolescents with schizophrenia. Arch.Gen. Psychiatry 63, 25–34.
Whitworth, A.B., Kemmler, G., Honeder, M., Kremser, C., Felber,S., Hausmann, A., Walch, T., Wanko, C., Weiss, E.M.,Stuppaeck, C.H., Fleischhacker, W.W., 2005. Longitudinalvolumetric MRI study in first-and multiple-episode maleschizophrenia patients. Psychiatry Res. 140, 225–237.
Wolff, S.D., Balaban, R.S., 1989. Magnetization transfer contrast(MTC) and tissue water proton relaxation in vivo. Magn. Reson.Med. 10, 135–144.
Woods, B.T., Yurgelun-Todd, D., Benes, F.M., Frankenburg, F.R.,Pope Jr., H.G., McSparren, J., 1990. Progressive ventricularenlargement in schizophrenia: comparison to bipolar affectivedisorder and correlation with clinical course. Biol. Psychiatry 27,341–352.
Worsley, K.J., Marrett, S., Neelin, P., Vandal, A.C., Friston, K.J.,Evans, A.C., 1996. A unified statistical approach for determiningsignificant signals in images of cerebral activation. Hum. BrainMapp. 4 (1), 58–73.
Xu, J., Kobayashi, S., Yamaguchi, S., Iijima, K., Okada, K.,Yamashita, K., 2000, Jan. Related Articles, 2000; Gender effectson age-related changes in brain structure. AJNR Am. J.Neuroradiol. 21 (1), 112–118.