Embed Size (px)
Citation preview

This OSLI RetIna supplement is produced by SLACK Incorporated and sponsored as an educational service by Alimera Sciences.
May 2016Volume 46 • Number 10
Cited iN MEDLINE
Supplement toHealio.com/OSLIRetina

May 2016 · Vol. 46, No. 10 (Suppl) S3
SLACK IncorporatedChief Content Officer
Joan-Marie Stiglich, ELS
EDItOrIaLSenior Editorial Director
David W. MullinExecutive EditorCara Dickinson
Operations ManagerCheryl McKeown
SpECIaL SErvICESSenior vice president, Special Services
Andrea L. Gaymon, M.Ed.Operations Manager, Special Services
Laura Stefano, MA, ELSMedical Copy Editor, Special Services
Norma Hanna project Editor, Special Services
Nick Andrews
SaLESvice president, Sales and Marketing,
Surgical SpecialtiesPatrick Duffey
Global Sales Director, Eye Care GroupScott Wright
Senior account Manager, Eye Care GroupJenna Gentile
Director, Sales administration and Support
Carolyn BoernerSales administrator
Wanda Granatorecruitment/Classified Sales representative
Tara KosmowskyCirculation Manager
John Kainreprints/Eprints
Licensing Opportunities: Wright’s Media 877-652-5295
DESIGNCreative Director
Thomas Cavallaro
The Wyanoke Grouppresident
Peter N. Slack Chief Operating Officer
John C. CarterExecutive vice president
Richard N. Roash Chief Financial Officer
Darrell Blood Senior vice president
Denise MealeyChief technology Officer
Linda Baker
Ophthalmic Surgery, laSerS & imaging retina® (ISSN-2325-8160, Canadian BN-12978 0466 RT) is published 10 times per year by SLACK Incorporated®, and is an official publication of ARVO/ISIE. Publication Office: SLACK Incorporated®, 6900 Grove Road, Thorofare, NJ 08086-9447. Telephone (856) 848-1000. Printed in the USA. Periodicals Class Postage Paid at Thorofare, NJ 08086 and at additional mailing offices.
Contents copyrighted by SLACK Incorporated®, 2016. All rights reserved. Permission requests to copy or reuse material published herein should be addressed to [email protected]. All requests to reprint or use material published herein should be addressed to Reprints/Eprints, Licensing Opportunities: Wright’s Media at 877-652-5295. Authorization to photocopy items for internal or personal use, or the internal or personal use of specific clients, is granted by SLACK Incorporated®, provided the fee of $.25 per page per copy is paid directly to Copyright Clearance, 222 Rosewood Drive, Danvers, MA 01923. This consent does not extend to other kinds of copying, such as for general distribution, resale, advertising and promotional purposes, or for creating new collective works.
Subscription rates in the U.S. and possessions: Individuals: One year—$194.00. Institutional: One year—$583.00. Residents and fellows: $97.00 for one year (a letter of certification indicating residency of the subscriber is required). Canada add 5% GST, all other countries add $52.00 per year. All subscriptions, without exception, will start with the first issue published after the order is received. Single copies and back issues, when available, are $86.00. Payment must accompany order. Subscription requests should be addressed to the publisher.
Change of Address: Notice should be sent to the publisher six weeks in advance of effective date. Include old and new addresses with zip codes. The publisher cannot accept responsibility for undelivered copies. Duplicate copies will not be sent to replace ones undelivered through failure to notify the publisher of change of address. POSTMASTER: Send Form 3547 to Ophthalmic Surgery, laSerS & imaging retina®, SLACK Incorporated®, 6900 Grove Road, Thorofare, NJ 08086-9447.
Articles are intended for informational purposes only and should not be used as the basis of patient treatment. All opinions expressed by authors and quoted sources are their own and do not necessarily reflect the opinions of the editors, publisher, or editorial boards of SLACK Incorporated®. The acceptance of advertising in no way implies endorsement by the editors, publisher, or editorial boards of SLACK Incorpo-rated®. See website for print and web advertising policy.
Readers with queries about the Journal's policies on error correction, version control, journal of record, ancillary material, or archiving should contact [email protected]. The Journal staff have no financial relationships to disclose. Financial disclosures for the Editor and members of the Editorial Board are on file with the editorial office.
Indexed in: MEDLINE/PubMed, ProQuest, EMCare, EMBASE, Science Citation Index, Current Contents/Clinical Medicine, BioEngineering Abstracts, CAB Abstracts, and SCOPUS.
Editorial Board
Carmen A. Puliafito, MDEditor-in-ChiefDean, Keck School of MedicineUniversity of Southern CaliforniaLos Angeles, CA
Darius M. Moshfeghi, MDDeputy EditorByers Eye InstituteStanford University School of MedicineMenlo Park, CA
Jay S. Duker, MDAssociate EditorNew England Eye CenterTufts University School of MedicineBoston, MA
Joel S. Schuman, MDAssociate EditorImagingUPMC Eye CenterUniversity of Pittsburgh School of MedicinePittsburgh, PA
Editorial Office Tufts Medical Center800 Washington StreetBoston, MA 02111Phone: (617) 636-9033
Managing EditorAlan Ball
Sophie Bakri, MDMayo ClinicRochester, MN
Francesco Bandello, MDUniversity Vita Salute Hospital San Raffaele Milan, Italy
Audina Berrocal, MDBascom Palmer Eye InstituteUniversity of Miami School of MedicineMiami, FL
Susanne Binder, MDRudolph Foundation ClinicVienna, Austria
Gabriel Coscas, MDHospital of CreteilCreteil, France
Donald J. D’Amico, MDWeill Cornell Medical CollegeNew York, NY
Diana Do, MDStanley M. Truhlsen Eye InstituteUniversity of Nebraska Medical CenterOmaha, NE
Pravin U. Dugel, MDRetinal Consultants of Arizona Retinal Research InstitutePhoenix, AZ
Dean Eliott, MDMassachusetts Eye & Ear InfirmaryHarvard Medical SchoolBoston, MA
Howard F. Fine, MDRobert Wood Johnson University HospitalNew Brunswick, NJ
Harry W. Flynn Jr., MDBascom Palmer Eye Institute University of Miami School of MedicineMiami, FL
Thomas R. Friberg, MDUPMC Eye CenterUniversity of Pittsburgh School of MedicinePittsburgh, PA
James G. Fujimoto, PhDMassachusetts Institute of TechnologyCambridge, MA
Alain Gaudric, MDHopital LaribosièreParis, France
Evangelos S. Gragoudas, MDMassachusetts Eye & Ear InfirmaryHarvard Medical SchoolBoston, MA
Seenu Hariprasad, MDPritzker School of MedicineUniversity of Chicago Chicago, IL
Alon Harris, PhDIndiana University School of MedicineIndianapolis, IN
Tarek Hassan, MDOakland University William Beaumont School of MedicineRoyal Oak, MI
Allen C. Ho, MDWills Eye InstituteThomas Jefferson UniversityPhiladelphia, PA
David Huang, MD, PhDCasey Eye InstituteOregon Health Sciences UniversityPortland, OR
Shuliang Jiao, PhDDepartment of Biomedical EngineeringFlorida International UniversityMiami, FL
Peter K. Kaiser, MDCole Eye InstituteCleveland Clinic Cleveland, OH
Judy E. Kim, MDMedical College of WisconsinMilwaukee, WI
Shoji Kishi, MD, PhDGunma University School of MedicineMaebashi, Japan
Szilárd Kiss, MDWeill Cornell Medical CollegeNew York, NY
John W. Kitchens, MDRetina Associates of KentuckyLexington, KY
Theodore Leng, MDByers Eye instituteStanford University School of MedicinePalo Alto, CA
Martin A. Mainster, PhD, MDUniversity of Kansas Medical CenterKansas City, KS
Andrew A. Moshfeghi, MDKeck School of Medicine University of Southern CaliforniaLos Angeles, CA
Quan Dong Nguyen, MDStanley M. Truhlsen Eye InstituteUniversity of Nebraska Medical CenterOmaha, NE
Joan M. O’Brien, MDScheie Eye InstituteUniversity of PennsylvaniaPhiladelphia, PA
Gholam A. Peyman, MDUniversity of Arizona College of MedicinePhoenix, AZ
Carl D. Regillo, MDWills Eye InstituteThomas Jefferson UniversityPhiladelphia, PA
Richard B. Rosen, MDNew York Medical CollegeNew York, NY
Philip J. Rosenfeld, MD, PhDBascom Palmer Eye Institute University of Miami School of MedicineMiami, FL
Stephen R. Russell, MDUniversity of IowaIowa City, IA
SriniVas R. Sadda, MDKeck School of MedicineUniversity of Southern CaliforniaLos Angeles, CA
David Sarraf, MDJules Stein Eye InstituteLos Angeles, CA
Ingrid U. Scott, MD, MPHPenn State College of Medicine Hershey, PA
Gaurav K. Shah, MDWashington University School of Medicine St. Louis, MO
Lawrence J. Singerman, MDCase Western Reserve UniversityCleveland, OH

S4 Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina May 2016 · Vol. 46, No. 10 (Suppl) S5
abStraCt: .
P..
Carmen A. Puliafito, MD, MBAEditor-in-Chief
OSLI RetIna
Improving Outcomes for Patients With Diabetic Macular Edema
Introduction
MODEratOr
Stephen Michels, MD, is founder and director of Retina Health Center in Fort Myers, Florida, and consulting associate in the department of ophthalmology at Duke University School of Medicine in Durham, North Carolina. dr. eaton received a modest honoraria from SLACK Inc. for his contribution to this supplement.
Edoardo Midena, MD, serves as General Secretary for the European Board of Ophthalmology and is Chair of the Ophthalmology Department at University Hospital in Padova, Italy. Dr. Midena recieved a modest honoraria from SLACK Inc. for his contribution to this supplement.
Johnathan Kitchens, MD, is ophthalmolgist and vitreoretinal surgeon with Retina Associates of Kentucky in Lexington. president-elect of the Kentucky Academy of Eye Physicians and Surgeons. Dr. Prenner received a modest honoraria from SLACK Inc. for his contribution to this supplement.
Jonathan prenner, MD is Board Certified in Ophthalmology and is associate clinical professor in the department of Ophthalmology at Rutgers Robert Wood Johnson Medical School. Dr. Prenner received a modest honoraria from SLACK Inc. for his contribution to this supplement.
Carl regillo, MD,
is Director of the Retina Service at Wills Eye Hospital in Philadelphia. He is a fellow of the American College of Surgeons and an active member of the American Academy of Ophthalmology. Dr. Regillo received a modest honoraria from SLACK Inc. for his contribution to this supplement.
Elias reichel, MD, is vice chair for research and education in the department of ophthalmology at the New england Eye Center in MA, and he is a professor of ophthalmology at Tufts University School of Medicine. Dr. Reichel received a modest honoraria from SLACK Inc. for his contribution to this supplement.
FaCULty
peter Kaiser, MD, is the Founding Dirextor of the Digital Optical Coherence Tomography Reading Center for the Cole Eye Institute. He is also a staff memeber at the Cole Eye Institute at the main campus in Cleveland. Dr. Kaiers recieved a modest honoraria from SLACK Inc. for his contricution to this supplement.
dOi Number
Diabetic macular edema (DME) results from diabetic retinopathy (DR) which causes more cases of blindness among working-age adults than all other causes and often goes unno-ticed until patients present with vision loss which makes early detection difficult. Along with factors such as thickness, quantity and visual acuity (VA), the location (of the edema) greatly influences treatment decisions. DME that is center involving, that is to say, edema that threatens the fovea thereby threatening VA, is center -involving DME (ci-DME). DME occurring safely away from the fovea is non-center-involving DME (nci-DME). The Early Treatment of Diabetic Retinopathy Study (ETDRS) coined the term, “clinically significant macular edema” (CSME) to refer to DME that required treatment or affected VA. Since the development and widespread use of optical coherence tomography (OCT), finding DME before a patient experiences vision loss became possible even if that DME was center involving. Once OCT began identifying DME before it affected VA, the term “CSME” became confusing because DME could be center involving without being clinically significant. Thus, classifying DME as center involving and non-center involving clarifies a patient’s circumstances, and in turn guides ophthalmologists toward the best disease management path. Vascular Endothelial Growth Factor (VEGF) plays a key role in DME progression; therapies that act by inhibiting VEGF production improve visual acuity in patients with DME. Two anti-VEGF therapies have been approved for the treatment of DME: ranibizumab and aflibercept. Bevacizumab, which is approvedfor the treatment of certain types of cancer1, is occasionally used off-label to treat DME. Anti-VEGF therapy can stop vision loss and improve VA. Anti-VEGF therapy is one of five treatments available to oph-thalmologists throughout the course of DME progression, a list which includes: modified grid laser therapy, anti-VEGF injections, steroid injections or implants, panretinal photocoagulation (PRP) therapy, and pars plana vitrecomy surgery. DME treatment combination options fuel the need for new data and discussion2; specifically, regarding how the different treatment options interact with one another. Beginning with the diagnosis of diabetes, this discussion will focus on the treatment of DME and aims to provide clinical opinions about treatment protocol sur-rounding intravitreal anti-VEGF therapy.

S6 Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina May 2016 · Vol. 46, No. 10 (Suppl) S7
2 diabetics9. The impacts of diabetes to eye care specialists bring particular caution because so much about the early stages of the effect of diabetes on eye care are unknown. Even more concerning is the fact that almost a third of patients with diabetes are undiagnosed10. Caring for these patients is costing society over $200 billion each year11. We as physicians have a lot of work ahead of us to improve the statistics.
PREPARING FOR TREATMENT
Kaiser: Moderate non-proliferative retinopa-thy follows mild non-proliferative retinopathy. Blood vessels responsible for the nourishment of the retina may swell and lose their ability to transport blood12. When patients present with moderate non-proliferative retinopathy, what kinds of tests or exams are important for the first visit?
Michels: Fundus photos, angiography and OCT are all instrumental for the development of DR treatment paths. I add ultra widefield fluoresce-in angiography. It seems as if interest in wide-field angiography is on the rise but we still have a lot to learn about how to best use widefield effectively. Information provided by the fluores-cein angiography, however, contextualizes each patient’s individual circumstances thus guiding her/his best treatment path.
Kitchens: Ultra widefield angiography is ab-solutely essential in patients with moderate or worse non-proliferative retinopathy. So many times in the past, I’ve underestimated the level of retinopathy on my clinical examination. The ultra widefield system, in these cases, will often show areas of non-perfusion or even occult neovascularization of the retina which was not visible on routine exam. Conversely, if a pa-tient looks really good on their ultra widefield angiogram, I will have the confidence to bring them back in 6 to 12 months even if they have significant looking retinopathy. I think this rela-
tively new diagnostic entity really modifies how we think about the DRS and ETDRS studies.
Michels: DME is a disease that presents with systemic inflammation. The disease may re-spond to anti-inflammatory treatment such as steroids with increasing effectiveness through-out treatment even though the inflammation is continuous.
Kaiser: Intraretinal microvascular abnormality (IrMA) is one of three qualifiers laid out in the ETDRS “4-2-1” rule. The “4-2-1” rule refers to three different circumstances that indicate severe non-proliferative diabetic retinopathy (NPDR). Twenty or more hemorrhages in 4 quadrants and/or venous beading (VB) in 2 quadrants and/or IrMA in 1 quadrant indicate severe NPDR13. The classification system and diagnostic recommendations are simple to understand and are easy to compare. The 4-2-1 rule still makes sense today14. I use widefield photos often in my practice where I find that Nonprofusion shows up more often and in larger amounts than I would have guessed. This is most surprising to see in patients whom I thought had no DR. When this happens to a patient I had been seeing annually, I’ll carefully consider seeing that patient a little more fre-quently. Patients who present with ischemia that eventually turns into inflammation has been a recent topic of discussion where treatment may need to be altered. Is the level of inflamma-tion affected in any way by whether or not the patient has chronic retinopathy?
Regillo: I routinely perform spectral domain optical coherance tomography (SDOCT) and fundus photography at the first encounter for such a patient. In many cases, I also perform fluorescein angiography, either traditional fun-dus camera-based photography with peripheral sweeps or widefield angiography. I am part of a large retina practice with multiple offices, and widefield imaging equipment is not available in
SCREENING AND FOLLOW UP
Peter Kaiser, MD: Diabetes affects over three hundred million people world-wide and if rates continue it will be the seventh leading cause of death on Earth3. Diabetes results in DR for nearly 80 percent of patients with diabetes who have had diabetes for ten years or longer. Al-most all patients with type 1 diabetes have DR and more than 60 percent of patients with type 2 diabetes are affected. How does diabetes lead to both DR and eventually DME and what role does vascular endothelial growth factor play in the process?
Jonathan Prenner, MD: Information from our peer-reviewed literature and the Centers for Disease Control and Prevention (CDC) illus-trates the shocking increase in the incidence of diabetes in the western world. Approximately 25% of the 29 million adults who have diabetes are not currently diagnosed. In 2005-2008 4.2 million (28.5%) of patients with diabetes over age 40 had diabetic retinopathy, and 655,000 (4.4%) had advanced diabetic retinopathy, including proliferative diabetic retinopathy (PDR). Only 50-75% of Americans with diabe-tes receive annual dilated eye exams, and nearly one in three cases of DME goes undiagnosed. Undiagnosed DME is problematic and requires continued attention.
Elias Reichel, MD: The exact way in which diabetes leads to DR and DME is still being researched4. A breakdown of the vascular in-ner blood- retinal barrier causes leakage from microaneurysms and/or leakage from capil-lary walls which leads to DME. It is also clear that long-term increased glucose levels lead to both DR and DME. Increased glucose, in turn, increases hypoxia5. Hypoxia results in ischemia and at some VEGF plays a role. The different interactions between the physiological factors make the process complex.
Carl Regillo, MD: Upregulation of VEGF promotes an influx of inflammatory cells and associated cytokines. A vicious cycle ensues with further breakdown of retinal blood vessel walls promoting additional leakage and isch-emia which, in turn, further increases VEGF and inflammatory cytokine production6
Edoardo Midena, MD: European telemedicine screening systems which allow patients to be easily examined and screened any time are nec-essary. This system benefits both patients and doctors because the screening centers provide imaging equipment and staff qualified to oper-ate that equipment [which is] inaccessible to some ophthalmologists and thus add[s] depth to a patient’s status. Telemedicine takes screening out of the hands of ophthalmologist practitio-ners which allows more time to focus on treat-ment7.
Reichel: I want to see patients newly diagnosed with diabetes. I want to counsel their primary care physician to recommend annual exams looking for DR. I want an updated hemoglo-bin A1C (A1C) reading. Though this approach is arguably conservative, I believe early and consistent follow up are important. The ground-breaking Early Treatment Diabetic Retinopathy Study (ETDRS) emphasized the importance of regular screening8. ETDRS also highlighted the need for early detection and early treatment due to the asymptomatic nature of DR.
Johnathan Kitchens, MD: I find it shock-ing that 10% of the American population has diabetes, the vast majority of whom have type
“Telemedicine. . .allows more time to focus on treatment.” —EDORARDO MIDENA, MD

S8 Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina May 2016 · Vol. 46, No. 10 (Suppl) S9
option of many as the first line of treatment. Focal grid laser therapy presents with some troublesome side effects i.e., distorted or discol-ored peripheral vision and problems with night vision22. Once circinate exudates outside the fovea show up on a patient’s OCT and he/she presents with intraretinal fluid approaching the fovea, meaning the patient presents with notice-able nci-DME, is laser treatment the logical next step?
Prenner: Typically, stimulating the retinal pig-ment epithelium (RPE) helps reabsorb diffuse areas of fluid. These treatments are distinct and very different. The first works well when there are a few very leaky microaneurysms which can be directly treated and closed without affecting the foveal avascular zone (FAZ). The second type is a little more nebulous as it can lead to diffuse areas of RPE loss if performed too ag-gressively. In these cases, I’ll usually reserve grid laser for patients that are less responsive to intravitreal therapies. I will always start with sub threshold laser in these cases and I find that pattern laser is very helpful. The DRCRnet protocol I study did show that patients treated with prompt laser did not have the same visual improvements as those with deferred laser.
Michels: The biggest question revolves around laser treatment. I believe there are other op-
tions even at this stage of nci-DME. I think it is worth watching the patient. If the patient shows the disease is progressing and intraretinal fluid continues to approach the fovea, attractive treat-ments exist outside of laser treatments. I think laser treatment, even though some do not prefer
the term laser, is a destructive treatment and I can say I would not want it done to my own retina. Newer laser technologies are likely less destructive, but their effectiveness should first be evaluated in prospective, controlled clini-cal trials, before a general recommendation is given.
Prenner: Focal laser remains an excellent option in certain cases, and has the obvious advantage of being non-invasive. In addition, laser may allow for sustained and prolonged therapeutic benefit without the need for frequent retreatment. I am building my personal experi-ence with Micropulse laser. I also continue to treat focal areas of nci-DME particularly when circinate lipid is present, with standard-ETDRS style focal laser. I no longer perform grid laser without the Micropulse laser.
Regillo: Once the patient begins to present with ci-DEM, I still prefer to watch the patient. The patient’s other eye and the level of the retinopa-thy may influence the decision at that point. If a patient presents with ci-DME and is at risk of proliferative diabetic retinopathy or, experienc-es any measurable VA loss (20/32 and 20/50 on Snellen and ETDRS scales, respectively.) from DME, treatment is triggered and I begin with anti-VEGF injections.
TREATING WITH ANTI-VEGF
Kaiser: Anti-VEGF injection therapy is the most popular form of treatment for DME23 and “Aflibercept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema” otherwise known as Protocol T, published in the summer of 2015 by The New England Journal of Medicine, con-tained significant information and protocol as it pertains to DME treatment and which anti-VEGF therapies work in which circumstances. However, when to begin anti-VEGF treatment and which treatment regimen to follow remains one of the most prominent clinical questions
all of our offices. It should be said that I do not feel handicapped or limited from a diagnostic standpoint in offices without widefield imaging. Imaging helps to quantify the level of retinopa-thy and guide both intensity of follow-up and type of treatment. Things I look for include the number of intraretinal hemorrhages in each quadrant, the status of venous beading or dilation, the presence or absence of IrMA and neovascularization and the degree and location of retinal capillary nonperfusion and macular thickening/edema Our group has OCTA in our main office and, as Elias pointed out, its use is primarily investigational, but clinically it can be helpful to detect central macular ischemia in a relatively quickly and noninvasively manner.
Kaiser: Some patients respond quite slowly to the anti-VEGF injections. Whether or not a particular patient will respond to anti-VEGF therapy becomes apparent quickly. Patients typically maintain the same relative response to any further anti-VEGF therapies15. The best indicator of responsiveness to anti-VEGF treat-ment is a dry macula. Protocol T showed 70% of maculae fell below the pre-defined thresh-old16. That means that throughout the many injections in the course of a year 30% were not dry. That dry macula ought to be weighed equally with vision improvement because they are both important indicators as to whether or not treatment is working. Drying the macula can improve patient status. There are different ways of modulating inflammation but steroids may be the most impactful17.
Reichel: VEGF does not always need to be elevated in the vitreous or the aqueous for the patient to present with DME. This implies
possible systemic issues at play causing the DME. Those issues may or may not be related to systemic inflammation but in these patients it is not up-regulated VEGF causing the inflam-mation. Some recent data shows interleukin-8 (IL-8) to be much higher in patients who do not respond to anti-VEGF injections18. If a patient does not respond to anti-VEGF and if there are no signs of up-regulated VEGF, steroids clearly make sense.
Midena: Ischemia is not the only cause of VEGF up-regulation in patients with hypergly-cemia. In fact, VEGF-A is not the only member of the cytokine family up-regulating; tumor necrosis factor-a (TNF-a) and interleukin-6 (IL-6) also up-regulate19. Cytokines in patients with diabetes show in a very expressive way even if retinopathy is not yet present. Early inflammatory phenomena modulate treatment and encourage the use of steroids; but, the inflammation will be a long-standing issue. As many as three injections ought to be enough to determine whether the patient is an anti-VEGF responder or non-responder. As many as 40% of patients with DR do not respond to anti-VEGF therapy. I argue that those 40% are likely the population who present with high inflammatory components which remain unaffected by the anti-VEGF. Most of the published studies on anti-VEGF treatment, including some seminal studies published by the Diabetic Retinopa-thy Clinical Research Network (DRCR), have shown that about 40% of the treated popula-tion doesn’t adequately respond to the initial anti-VEGF treatment and that the next step is to switch drugs20.
MODIFIED FOCAL GRID LASER THER-APY
Kaiser: Photocoagulation laser treatment provided the first real treatment for DME over 30 years ago21. Recent advancements made in anti-VEGF therapy have made it the preferred
“Attractive treatments exist outside of laser treatments.” — sTEPHAN MICHELs, MD
“There are different ways of modulateing inflammation but steroids may be the most impactful.” — PETER kAIsER, MD

S10 Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina April 2016 · Vol. 46, No. 10 (Suppl) S11
personalized kind of treatment like treat-and-extend include possible financial benefit for the patient and decreased wear on the eye being treated. Both RISE and RIDE, as well as VIVID and VISTA studies, showed that arterial throm-boembolic events (ATE) were considerably higher in patients who underwent continuing in-jections over time. Given the risks and benefits to anti-VEGF treatment what kind of protocol or method do you use to administer anti-VEGF injections?
Michels: Because of patient compliance I favor treat-and-extend. Patients being treated with the treat-and-extend method are continuously treated and under my watch. DME is a chronic disease and patients with diabetes tend to pres-ent compliance issues. It is important to help educate patients about the risks of foregoing treatment and to show them that the disease is chronic and it needs to be approached that way. I might suspend treatment if the patient goes a year or more without ci-DME recurring. Currently nobody can completely exclude a systemic risk of intravitreal anti-VEGF therapy,
but if there is one, it has to be very low27.
Regillo: Anti-VEGF treatment burden is typi-cally greatest in the first year of therapy. Pro-tocols I and T, which utilized a PRN-like style of treatment, showed a mean number of anti-VEGF injections to be in the range of eight to 10 in the first year. By years 2 or 3 in Protocol I, the mean dropped to less than half that amount, and it was not uncommon for patients to not need further treatment or at least very few injec-tions going forward28,29.
Midena: I am fully convinced that loading phase treatment is essential. Loading phases allow me to follow up with a personalized treat-ment. Randomized trials, case records and pub-lished records, show an increase in visual func-tion and decrease in thickness on the OCT30. I use the loading phase to identify whether or not the treatment is working for the patient. De-pending on the drug, the loading phase varies between three injections and six. The results that a loading phase provides also involve the retina which only provides more information about the efficacy of the treatment and detailed information about the patient.
Regillo: The shortcoming of the treat-and-extend approach in this setting is not knowing which patient can come off treatment. I treat more like what was done in Protocol I and Pro-tocol T – PRN (pro re nata or as needed) style. I administer injections monthly at first until the macula is dry. Once the macula is dry, I watch and closely monitor for recurrence and then treat accordingly as needed.
Reichel: Practically speaking, looking at trials (such as RISE, RIDE, VIVID, VISTA, Protocol T,) it generally took five or six injections to get to the plateau in OCT or the increased plateau on VA. It is exceptional to think that just an injection or two adequately manages significant ci-DME. That is not normal. In the first year of treatment, I argue that erring on the side of overtreatment is better than undertreatment.
Kaiser: It is exceptional to think that one or two injections over a few months adequately manages significant ci-DME. A treatment-intensive timeframe will get the edema down which will help the patient. Getting in front of the disease is the key and that lies with treat-ing early. Recently, an approach being labeled “Observe-and-Plan” has been drawing atten-tion. This approach aims to maximize efficiency without overtreating. The observe-and-plan
surrounding DME. When will you begin treat-ment with anti-VEGF injections?
Regillo: Anti-VEGF injections are clearly the correct move once a patient presents with vi-sion loss from ci-DME. Until the Protocol T results were published, the differences between respective anti-VEGF therapies was purely anecdotal. Protocol T did show some differ-ence in the efficacy of these drugs, though. The anti-VEGFs in Protocol T did not dif-ferentiate themselves when the patient had milder degrees of visual acuity loss (ETDRS Snellen equivalent of 20/32-20/40) coupled with smaller amounts of edema. The results were the same regardless of which anti-VEGF was used24. When there was worse presenting visual acuity or more severe degrees of central retinal thickness, some differences in efficacy then became apparent with aflibercept being the most effective and bevacizumab the least effective.
Prenner: We now well recognize the common-ly seen disconnect between the retinal anatomy on exam and imaging tests, and associated vi-sual function. I generally will not treat patients who are very well seeing initially, but will fol-low closely for a short period of time and try to help the patient recognize signs of clinical damage on imaging tests. OCT is quite valu-able in this regard. I also ask patients to moni-tor themselves for compromise of their visual function in daily life. In cases with significant vision loss and OCT thickening, Protocol T suggests that aflibercept is the preferred thera-peutic option. Protocol T also suggests that any of the three anti-VEGF agents are appro-priate in eyes that are relatively well seeing. I tend to follow these guidelines generated from the DRCRnet in clinical practice.
Kitchens: I find this proposition to be perhaps the most controversial and thought provoking surrounding DME. A difficult decision must be
made when asymptomatic patients present with both good visual acuity and nci-DME. My current modus operandi leaves that decision up to the patient. I make perfectly clear, how-ever, that deferring injections leads directly to frequent follow-ups. Fortunately, the DRCRnet is looking at this question with the protocol v study which is evaluating patients with ci-
DME and very good vision25.
Reichel: For me, vision loss is the key symp-tom before treatment. Presently, any of the three anti-VEGF therapy options are accept-able. OCT results play a role in choosing which anti-VEGF to use because Protocol T and supplemental materials show that patients who presented with 400 microns of thickness tended to do better with aflibercept26. Afliber-cept’s advantage was not clinically noticeable when patients presented with mild macula thickness or mild VA loss (between 20/32 and 20/40 Snellen chart results) at the time of initial treatment. However, patients who presented with advanced thickness, visible on the OCT, or showed a worse Snellen chart VA than 20/40 responded to aflibercept more than ranibizumab and bevacizumab respectively.
ADMINISTERING ANTI-VEGF THERA-PY
Kaiser: Data is still needed to recommend an injection administering protocol for anti-VEGF therapy. The treat-and-extend approach, where anti-VEGF is administered monthly until the macula is dry and injection date intervals are extended with each visit, has been rising in popularity recently. Reasons to follow a
“. . .patients who presented with 400 microns of thickness tended to do better with aflibercept.” — ELIAs REICHEL, MD
“Anti-VEGF treatment burden is typically greatest in the first year of therapy.” — CARL REGILLO, MD

S12 Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina April 2016 · Vol. 46, No. 10 (Suppl) S13
effective anti-VEGF treatment. I found that aflibercept showed supremacy in the following categories: overall visual acuity, visual acuity in patients 20/50 or worse, OCT improvements, rescue laser therapy, number of re-treatments needed, etc. Additionally, if the patient is failing to respond, I want to consider steroids as soon as possible.
COMBINATION THERAPY
Kaiser: Three good steroid options exist in the United States—two are FDA approved (dexa-methasone and fluocinolone implants) and one is off-label (triamcinolone.) When usV-ing triamcinolone, I inject a 2 mg dose which gives me a good effect and typically lasts about 3 months or so. The FDA approved the dexa-methasone implant for DME over a year ago and I find that it provides an effect that averages about 4 months, sometimes a bit longer in the setting of DME. The final steroid option is the
fluocinolone implant. It is an option for patients who respond well to the shorter acting steroids and don’t have secondary significant intraocular pressure elevation. Furthermore, it is very long lasting, and its continuous effect may also slow the progression of DR like anti-VEGF drugs. Once other treatment options are exhausted, Proliferative Diabetic Retinopathy (PDR) may require vitrectomy. All surgery poses risks to
patients and removing vitreous gel has a major impact on the eye and can cause cataract and retinal detachment along with endophthlamitis. However, when this procedure is necessary, how does that affect your treatment plan for a patient? How does the state of DME affect your treatment plan?
Regillo: I have never been convinced that using PRP for a patient with peripheral non-perfusion had a significant impact on DME. I have tried scatter laser to areas of peripheral nonperfusion for the purpose of reducing macular edema in both DR and retinal vein occlusions and did
method has seen success in the treatment of wet age-related macular degeneration (AMD).
Prenner: I generally manage patients with a treat-and-extend approach when treating wet AMD, as the consequences of under treatment can be devastating. I tend to treat with serial monthly injections in DME until the retinal anatomy mostly normalizes. Subsequently, I switch to a PRN treatment approach in many patients, as there is little downside risk to most recurrences of DME. Often, this change to a re-duced treatment burden is patient driven in the younger, less compliant population of patients who have DME compared to those with wet AMD.
SWITCHING TO AFLIBERCEPT
Kaiser: Protocol T revealed different suc-cess rates in the respective anti-VEGFs. For a minimum of one focal grid laser treatment in the course of the study: aflibercept 37%; beva-cizumab 56%; ranibizumab 46%31.Protocol T clearly showed that aflibercept improved VA and reduced edema under certain circumstances including a worse initial VA and a macula more than 400 microns thick. At which point in a patient’s treatment plan does switching anti-VEGFs make sense and is that anti-VEGF aflibercept?
Midena: Switching to aflibercept is the correct move when treatment reaches plateau. If the most recent OCT shows no change and the pa-tient begins experiencing VA issues, aflibercept makes the most sense. Patients with DME have systemic endothelial issues resulting from dia-betes. The easiest way to measure those issues may be by checking the progenitor endothelial cells in the blood. It is important to remember that DME is a chronic disorder. Despite its chronicity, this disorder is self-limiting. The decreased need for injections is evidence for the limiting nature of the condition.
Regillo: Patient progress indicates whether or not a switch is the right course of action. As long as the OCT shows improvement in thick-ness or the VA is improving, I stay the course of treatment. However, should a patient undergo four to six monthly treatments without signifi-cant improvement in either parameter, I would look to make a change. If I started with beva-cizumab or ranibizumab, I would first switch to aflibercept. If already on aflibercept, I will consider switching to a steroid. Steroids work well to treat inflammation-related disorders of the eye, and that includes DME. For nearly fif-teen years now, we have known that DME and associated decreased visual acuity improve after intravitreal steroid injections.32 Long-acting intravitreal steroid exposure may also decrease DR progression33.
Prenner: If I do not see sufficient anatomic im-provement on OCT after treatment with beva-cizumab, I will change anti-VEGF agents and treat with aflibercept. After multiple additional injections, if an acceptable clinical response is not achieved, I will add a regional depot steroid to the treatment regimen, typically utilizing Ozurdex. In these difficult cases, continued anti-VEGF therapy may be required while the steroid is active. I have recently had encourag-ing results with Iluvein, and look forward to gaining more experience with this novel tech-nology in challenging eyes with DME.
Kitchens: I start with aflibercept because I want to make sure I am treating with the most effec-tive anti-VEGF therapy. My interpretation of Protocol T is that aflibercept is the most
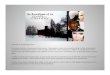
Figure 1. Mean Change in visual acuity over timev
Shown are the changes in visual acuity overall (Panel A) and according to baseline visual acuity (Panel B). In Panel B, solid lines indicate baseline visual acuity of 20/50 or worse, and dashed lines indicate baseline visual acuity of 20/32 to 20/40. Outlying values were truncated to 3 Sd from the mean. the number of eyes assessed at each 4-week interval ranged from 195 to 224 in the aflibercept group, 188 to 218 in the bevacizumab group, and 188 to 218 in the ranibizumab group (see Fig. S2 in the Supplementary Appendix for the exact number assessed at each 4-week interval). I bars indicate 95% confidence intervals.
Reprinted from The New England Journal of Medicine, volume 372, pages 1193-1203, Aflibercept, Bevacizumab, Ranibizumab for Diabetic Macular Edema.
“My interpretation. . . is that aflibercept is the most effective anti-VEGF treatment.” — JOHvNATHAN kITCHENs, MD

S14 Ophthalmic Surgery, Lasers & Imaging Retina | Healio.com/OSLIRetina April 2016 · Vol. 46, No. 10 (Suppl) S15
rEFErENCES
1. Adhi, M., Duker, J. S. Optical Coherence Tomography – Cur-rent and Future Applications. Current Opinion In Ophthalmology. 2013;24(3):213-221.
2. Diabetes Basics. American Diabetes Association Web site. http://www.diabetes.org/diabetes-basics/statistics/ Accessed February 1, 2016
3. Brown, D. M. Long-term Outcomes of Ranibizumab. Ophthalmol-ogy, 2013 Oct;120(10):2013-22. doi: 10.1016
4. C Ehlken1, S. J. Switch of anti-VEGF agents is an option for non-responders in the treatment of AMD. Eye. 2014 May;28(5):538-45. doi: 10.1038.
5. J. Cai, M. Bouton. The pathogenesis of diabetic retinopathy: old con-cepts and new questions. Eye 2002 May;16(3):242-60
6. Dabir, S. S. (2014). Differential systemic gene expression profile in pa-tients with diabetic macular edema: Responders versus nonresponders to standard treatment. Indian Journal of Ophthalmology.2014 Jan; 62(1): 66–73. doi: 10.4103/0301-4738.126186
7. Desouza, C. V., Shivaswamy, Vijay. Pioglitazone in the Treatment of Type 2 Diabetes: Safety and Efficacy Review. Clin Med Insights En-docrinol Diabetes. 2010; 3: 43–51.Published online 2010 Aug 3. d Diabetes.
8. Intravitreal Ranibizumab or Triamcinolone Acetonide in Combina-tion with Laser Photocoagulation for Diabetic Macular Edema. Dia-betic Retinopathy Clinical Research Network Public Web site. http://drcrnet.jaeb.org/Studies.aspx?RecID=146. Accessed December, 2015.
9. Writing Committee for the Diabetic Retinopathy Clinical Research Network. Panretinal Photocoagulation vs Intravitreous Ranibizumab for Proliferative Diabetic RetinopathyA Randomized Clinical Trial. JAMA. 2015;314(20):2137-2146. doi:10.1001/
10. Fileta JB, S. I. Meta-analysis of infectious endophthalmitis after in-travitreal injection of anti-vascular endothelial growth factor agents. OSLI-Retina, 2014 Mar-Apr;45(2):143-9. doi: 10.3928/23258160-20140306-08
11. Hanharta, J., Chowersa, I. Evaluation of the Response to Ranibizum-ab Therapy following Bevacizumab Treatment Failure in Eyes with Diabetic Macular Edema. Case Reports In Ophthalmology, 2015 Feb 10;6(1):44-50. doi: 10.1159/000375230.
12. Jr, R. E. Diabetic Macular Edema Associated With Glitozone Use. Retina, 2006 May-Jun;26(5):562-70.
13. Lihteh Wu, P. F.-L.-B. Classification of Diabetic Retinopathy and Dia-betic Macular Edema. World Journal of Diabetes, 2013 Dec 15; 4(6): 290–294.doi: 10.4239/wjd.v4.i6.290.
14. Triantafylla, Magdalini Massa, Horace F. Ranibizumab for the treat-ment of degenerative ocular conditions. Clinical Ophthalmology, 2014; 2014:8 Pages 1187-98 doi:http://dx.doi.org/10.2147/OPTH.S40350.
15. The DR Disease Severity Scale. Medscape Web stie. http://www.med-scape.org/viewarticle/459913_3. Accessed December, 2015.
16. National Eye Institute. Treatment techniques and clinical guidelines for photocoagulation of diabetic macular edema. Early Treatment Diabetic Retinopathy Study Report Number 2. Early Treatment Diabetic Retinopathy Study Research Group. Ophthalmology. 1987 Jul;94(7):761-74.
17. Facts About Diabetic Eye Disease. National Institute of Health Web site. https://nei.nih.gov/health/diabetic/retinopathy. Accessed January, 2016.
18. Nguyen, Q.. Ranibizumab for diabetic macular edema: results from 2 phase III randomized trials: RISE and RIDE. Ophtalmology, 2012 Apr;119(4):789-801. doi: 10.1016.
19. PA, C. Long-term benefit of sustained-delivery fluocinolone aceton-ide vitreous inserts for diabetic macular edema. Opthalmology, 2011 Apr;118(4):626-635.e2. doi: 10.1016.
20. Semeraro, F. Diabetic Retinopathy: Vascular and Inflamma-tory Disease. Journal of Diabetes Research. (2015), http://dx.doi.org/10.1155/2015/582060 .
21. Treatment for CI-DME in Eyes With Very Good VA Study (Proto-col V). Diabetic Retinopathy Clinical Research Network Web site. https://clinicaltrials.gov/ct2/show/NCT01909791. Study verified No-vember, 2015 by Diabetic Retinoptahty Clinical Research Network.
22. The Diabetic Retinopathy Clinical Research Netowrk Consortium.
Randomized Trial Evaluating Ranibizumab Plus Prompt or Deferred Laser or Triamcinolone Plus Prompt Laser for Diabetic Macular Ede-ma. Ophthalmology, 2010 Jun;117(6):1064-1077.e35. doi: 10.1016.
23. The Diabetic Retinopathy Clinical Research Network. (2015). Afliber-cept, Bevacizumab, or Ranibizumab for Diabetic Macular Edema. The New England Journal of Medicine, 1193-1203.
24. Moja L, Lucenteforte E, Kwag KH, Bertele V, Campomori A, Chakra-varthy U, D’Amico R, Dickersin K, Kodjikian L, Lindsley K, Loke Y, Maguire M, Martin DF, Mugelli A, Mühlbauer B, Püntmann I, Reeves B, Rogers C, Schmucker C, Subramanian ML, Virgili G.Cochrane Database Syst Rev. 2014 Sep 15;9:CD011230.
25. Thomas A. Ciulla, M. (2003). Diabetic Retinopathy and Diabetic Macular Edema. Diabetes Care, 2643-2664.
26. Thompson-Reid, P., & Ernst, K. L. (2010). The Diabetes Prevention and Control Programs In the United States and Public Health Law and Policy. In D. W. K.M. Venkat Narayan, Diabetes Public Health: From Data To Policy (p. 499). Oxford University Press.
27. Vujosevic S1, M. E. Retinal layers changes in human preclinical and early clinical diabetic retinopathy support early retinal neu-ronal and Müller cells alterations. Journal of Diabetes Research. 2013;2013:905058. doi: 10.1155/2013/905058.
28. W. Zhang, H. Liu, M. Al-Shabrawey, R.W. Caldwell and R.B. Caldwell. Inflammation and diabetic retinal microvascular complica-tions. J. Cardiovasc Dis (2011) 2(2): 96-103.
29. Wenick, A. S., Bressler, N. M. Diabetic Macular Edema: Current and Emerging Therapies. Middle East Africa Journal of Ophtalmology, 2012 Jan-Mar; 19(1): 4–12. doi: 10.4103/0974-9233.92110.
30. 10 Facts About Diabetes. World Health Organization Web site. http://www.who.int/features/factfiles/diabetes/facts/en/. Accessed Decem-ber, 2015.
39. Casparis H, Wolfensberger TJ, Becker M, Eich G, Graf N, Ambresin A, Mantel I, Michels S. Incidence of presumed endophthalmitis after intravitreal injection performed in the operating room: a retrospec-tive multicenter study. Retina. 2014 Jan;34(1):12-7. doi: 10.1097/IAE.0b013e31829f74b0
not see significant benefit and published data to date appear to support the lack of effect. Fur-thermore, non-perfusion can be a moving target in DR especially if the eye is also receiving an-ti-VEGF therapy. Because regular anti-VEGF injections in the setting of DR can reduce the level of DR, the area of non-perfusion could change in a positive way.
Kitchens: I do think that PRP may affect the pharmacokinetics of future injections. To me, the most important aspect of injections in patients requiring surgery is to ensure that they have received an anti-VEGF medication preop-eratively. This seems to reduce the risk of post-operative vitreous hemorrhage and may reduce rates of intraoperative complications.
Michels: In our setting I reassure patients that endophthalmitis is extremely rare with anti-VEGF treatment34. OSLI Retina reported the instances to be below 200 for over 350,000 patients35. Retinal detachment and lens damage are rare with rates as low as 1 in 20,000. When risks are that low, I can confidently assure my patients of their safety.
Midena: In my experience, adverse effects from anti-VEGF injection procedures are purely anecdotal and unpredictable. The biggest con-cern about systemic safety does not have to do with what we know now but what might still be discovered. We know when laser therapy started and was approved. We know studies backed safety and efficacy of laser therapy at the time. However, some 20 years later, we saw patients with scarring. In patients with diabetes, nerve fiber thinning can be seen even before retinopa-thy can be seen and we know that nerve fiber thinning has been associated with anti-VEGF36. I consider what might happen to a patient who was treated for DME with anti-VEGF injections ten years or more after his/her last injection.
Prenner: I am always concerned about en-dophthalmitis despite the low incidence rate,
particularly in well seeing eyes. While endo-phthalmitis is fortunately rare in modern prac-tice, the outcomes of these infections are often
devastating. My general impression is that all three anti-VEGF agents may carry a low associ-ated risk of systemic adverse events, although we are limited in prospective evidence concern-ing this issue. In addition, studies that demon-strate a safety imbalance between anti-VEGF agents do not exist, as registration trials of these agents were not powered to demonstrate a safety difference.
Kaiser: I think we have some great studies in anti-VEGF head-to-head but we have very little anti-VEGF with steroids and other treatments, including things we have mentioned like vit-rectomy. I think DRCR ought to be looking at this situation. We need better guidance regard-ing the relationship between multiple treatment paths. We need to know when steroids should be added and whether or not we should con-tinue with anti-VEGF therapy thereafter. I do not want to be doing a disservice to the patient. I think that it is important that the ophthalmolo-gist community, particularly involved with DME, understand that diabetes does not always have a consistent VEGF or anti-VEGF protocol. There are a lot of pathways involved that are well outside even the VEGF pathway.
“Studies that demonstrate a safety imbalance between anti-VEGF agents do no exist.” — JONATHAN PRENNER, MD

Delivering the best in health care information and education worldwide
6900 Grove Road, Thorofare, NJ 08086 UsA
phone: 856-848-1000 • Healio.com/OSLIRetina
This OSLI RetIna supplement is produced by SLACK Incorporated and
sponsored as an educational service by Alimera Sciences.