Embed Size (px)
Citation preview

ABLondon 27/1/2005
Andreas BaumbachBristol Heart Institute
Bristol Royal Infirmary

AB
Revascularisation in ACS
ICTUS
MERLIN
REACT
4mins
4mins
4mins
Tony’s Comments15mins

AB
ICTUS
Comparison of an early invasive with a selective invasive strategy
in pts presenting with Trop positive ACS

ESC München 2004
ESC Hotline-II
Robbert J de Winter MD PhD FESC
Academic Medical CenterDepartment of Cardiology
University of Amsterdam
No financial interests to disclose

ESC München 2004
Design
Inclusion criteria
• Anginal symptoms at rest < 24 hours
• Troponin T concentration 0.03 ng/L
• And one of the following:
Documented history of coronary artery disease
Ischemic changes on the ECG
ST-segment depression 0.05 mV
Transient ST‑segment elevation
T-wave changes 0.2 mV in two contiguous leads

ESC München 2004
NSTE-ACSTrop T pos Death, MI, or ACS
Abciximab during all PCI procedures
Selective invasive
Early invasive
AspirinEnoxaparinClopidogrel
Statins
CAG Medical Rx
PCI / CABG
Medical Rx
CAG / PCI / CABG
ETT
Chest pain
- 24 hrs
Random.
0 hrs
Refractory angina
-
+
24-48 hrs
1 year
Design
Study design
ESC München 2004
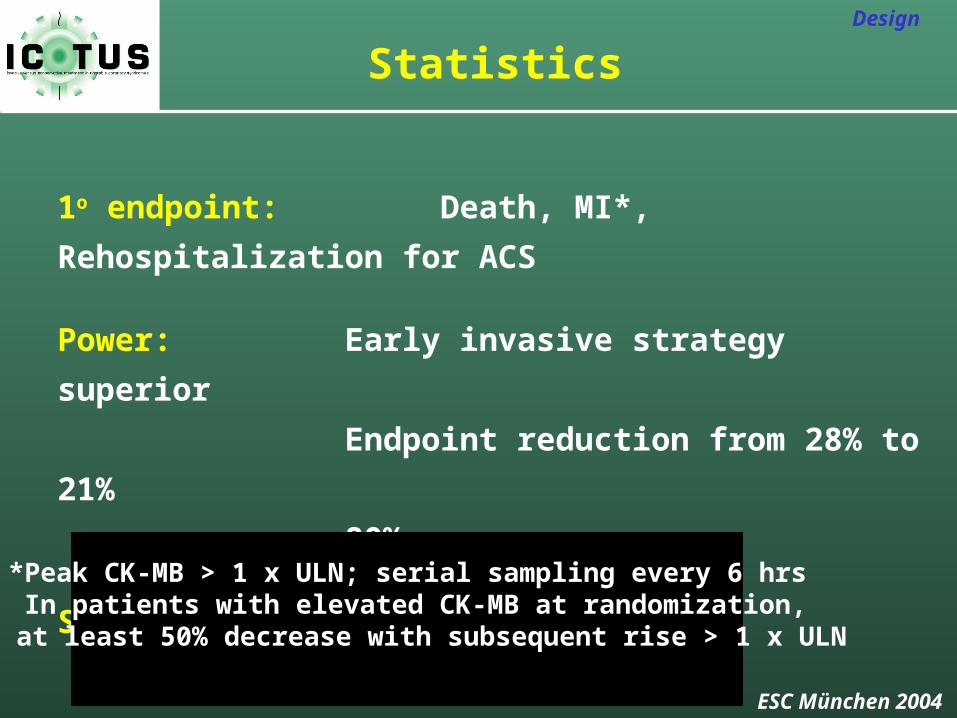
1o endpoint: Death, MI*, Rehospitalization for ACS
Power: Early invasive strategy superior
Endpoint reduction from 28% to 21%
80% power
Sample size: 2 x 600 patients
Design
Statistics
*Peak CK-MB > 1 x ULN; serial sampling every 6 hrs In patients with elevated CK-MB at randomization,
at least 50% decrease with subsequent rise > 1 x ULN

ESC München 2004
Results
Results
• 42 participating Dutch centers, 12 intervention centers
• 1201 patients randomized between July 2001- August 2003
Early invasive: 604 patients
Selective invasive: 597 patients
• One year follow-up (August 20th 2004), 98% complete

ESC München 2004
100 200 300
20%
40%
60%
80%
100%
73%
47%
Early invasive
Selective invasive
Time (days)
Results
Revascularization over time
Early invasive: 97% CAGSelective invasive: 67% CAG
Highest Angio/Revascularisation Rate

ESC München 2004
10%
20%
30%
100 200 300
Early invasive
Selective invasive
Death, MI, Rehospitalization for ACS
21.7%
20.4%
Results
Relative Risk: 1.0695% CI: 0.85 – 1.32
P = 0.59
Time (days)

ESC München 2004
Events at one year
Death
New or recurrent MI
Rehosp. for ACS
Primary endpoint
P-value
0.86
0.006
0.017
0.59
2.2
14.6
7.0
21.7
Earlyinvasive
(%)
2.0
9.4
10.9
20.4
Selectiveinvasive
(%)
Results
1.07
1.55
0.63
1.06
RelativeRisk
No difference in Angina
AB
Conclusion1. An early invasive strategy was not
superior to a selective invasive strategy for NSTE-ACS
2. Use of active risk stratification, and liberal use of coronary angiography is a good treatment option
3. The treadmill is back !

AB
MERLIN
Comparison of Rescue angioplasty for failed thrombolysis with a
conservative strategy

MERLIN
Mark de Belder
The James Cook University Hospital
Middlesbrough
Is rescue angioplasty worth it?

MERLINMETHODS
Inclusion Criteria
• STEMI and evidence of “failure to reperfuse” • Presentation to hospital within 10 hours of
symptoms • “Failure to reperfuse” at 60 min ECG:
Failure of the ST segment elevation in the worst lead to have resolved by 50%
Endpoints• Primary end point:
30 day all cause mortality
• Secondary endpoints: i) 30 day composite of death, reinfarction, stroke, heart failure, unplanned revascularisation ii) Left ventricular function at 30 days assessed by the RWMI.iii) Further analysis at 6, 12, 24, 36 months

MERLIN Results: 30 days
0
10
20
30
40
50%
Primary endpoint Composite secondary endpoint
Rescue N:154 Conservative N:153
p=0.7
p=0.02
0
5
10
15
20
25
30%
Dea
th
ReM
I
Str
oke
Unp
lann
ed
reva
sc CCF
P=0.7
P=0.3
P=0.03
P=0.0004
P=0.3
11.1
1.3
0
2
4
6
8
10
12
%
Rescue Conservative
Transfusions
Sutton AGC, Campbell PG, Graham R et al. JACC 2004;44:287-96
9.8 11

MERLINResults in the elderly
0
5
10
15
20
25
%
<56 56-65 66-75 >75
MERLIN: 30 day deaths
ConsRescue

30 day Kaplan-Meier survival curve
0 10 20 300
25
50
75
100
%
Days
Conservative
Rescue
p=0.7

30 day Kaplan-Meier event free survival curve
0 10 20 300
25
50
75
100
Days
%
p=0.02Conservative
Rescue

MERLIN – 1yr event free survival
p=0.005
0 100 200 300 400 0
25
50
75
100
Days
Conservative Rescue

0 100 200 300 400 0
25
50
75
100
Days
Conservative Rescue
MERLIN – 1yr survival

AB
Conclusion1. No early mortality benefit
2. Less urgent revascularisations
3. At 1 yr there is no mortality benefit for a strategy of rescue angioplasty
based on the 60 mins ECG

AB
REACT
Comparison of Rescue angioplasty, repeat thrombolysis and
conservative treatment for failed thrombolysis

Steering CommitteeSteering CommitteeSteering CommitteeSteering Committee
A.H.Gershlick (PI) A.H.Gershlick (PI) M de Belder M de Belder H H Swanton Swanton
R.Wilcox R.Wilcox K Abrams K Abrams
David de BonoDavid de Bono
A.H.Gershlick (PI) A.H.Gershlick (PI) M de Belder M de Belder H H Swanton Swanton
R.Wilcox R.Wilcox K Abrams K Abrams
David de BonoDavid de Bono
Data & Safety Data & Safety Data & Safety Data & Safety
End Point CommitteeEnd Point CommitteeEnd Point CommitteeEnd Point Committee
Kim FoxKim Fox
J. BirkheadJ. Birkhead
M. Bland M. Bland
Kim FoxKim Fox
J. BirkheadJ. Birkhead
M. Bland M. Bland J.HamptonJ.Hampton
S DaviesS Davies
J.HamptonJ.Hampton
S DaviesS Davies
Trial Co-Ordinators/ MonitorsTrial Co-Ordinators/ Monitors Sarah HughesSarah Hughes
Amanda Stephens-LloydAmanda Stephens-LloydIndependent StatisticianIndependent Statistician
Suzanne Stevens/ Alan Skene Suzanne Stevens/ Alan Skene
Trial Co-Ordinators/ MonitorsTrial Co-Ordinators/ Monitors Sarah HughesSarah Hughes
Amanda Stephens-LloydAmanda Stephens-LloydIndependent StatisticianIndependent Statistician
Suzanne Stevens/ Alan Skene Suzanne Stevens/ Alan Skene
Dr N UrenDr N Uren
Dr A de BelderDr A de Belder
Dr J DavisDr J Davis
Dr M PittDr M Pitt
Dr F AlamgirDr F Alamgir
Dr A BanningDr A Banning
Dr A BaumbachDr A Baumbach
Dr MF ShiuDr MF Shiu
Dr B VallanceDr B Vallance
Dr P SchofieldDr P Schofield
Dr K DawkinsDr K Dawkins
Prof P WeissbergProf P Weissberg
Dr R HendersonDr R Henderson
Dr E LeathamDr E Leatham
Dr M MalekianDr M Malekian
Dr M Millar-CraigDr M Millar-Craig
Dr S RedwoodDr S Redwood
Dr S OdemuyiwaDr S Odemuyiwa
Dr P WalkerDr P Walker
Dr E LeeDr E Lee
Dr K OldroydDr K Oldroyd
Dr D O'NeillDr D O'Neill
Dr N CurzenDr N Curzen
Dr S HoodDr S Hood
Dr D HackettDr D Hackett
Dr C LawsonDr C Lawson
Dr H SwantonDr H Swanton
Dr R FoaleDr R Foale
Dr W PennyDr W Penny
Dr D SmithDr D SmithDr I SquireDr I Squire
Dr I HudsonDr I HudsonDr M.NorellDr M.Norell
All Investigators

REACT (REscue Angioplasty v Conservative treatment or repeat Thrombolysis)
ECGECG 90 min90 min post (any) thrombolyticpost (any) thrombolytic
ST < 50 % resolution (with or without pain) CONSENT & RANDOMISE
(IF PCI possible within 12hrs of CP)
Conservative 2 nd thrombolytic Coronary Angio 24 iv heparin Acelerated tPA or +/- PCI Reteplase
P. End point: 6/12 ~death/re-infarction/CVA / severe HF
REACT (REscue Angioplasty v Conservative treatment or repeat Thrombolysis)
ECGECG 90 min90 min post (any) thrombolyticpost (any) thrombolytic
ST < 50 % resolution (with or without pain) CONSENT & RANDOMISE
(IF PCI possible within 12hrs of CP)
Conservative 2 nd thrombolytic Coronary Angio 24 iv heparin Acelerated tPA or +/- PCI Reteplase
P. End point: 6/12 ~death/re-infarction/CVA / severe HF

n=427
R -LYSIS (n=142)
CONS (n=141)
R-PCI (n=144)
Overall
AgeAge 61.3 (10.3) y 61.0 (10.7) y 61.1 (11.9) y
Anterior infarct 38.0% 46.8% 42.7% 42.5%42.5%
FIRST LYTICFIRST LYTIC
rPA 30.3% 19.9% 29.2% 26.5%
SK 57.7% 62.4% 58.3% 59.5%59.5%TNK 1.4% 3.5% 2.1% 2.3%
tPA 10.6% 14.2% 10.4% 11.7%
Stents 68.5%
GP IIb/IIIa 43.4%
RESULTS RESULTS

Primary composite endpoint:Death and non-fatal re-AMI, CVA , Severe HFPrimary composite endpoint:Death and non-fatal re-AMI, CVA , Severe HF
p= 0.78 p= 0.78
p = 0.0009 p = 0.0009
p = 0.002 p = 0.002
6 Months RESULTS
Gr AN=142
R-LYSIS
Gr AN=142
R-LYSIS
Gr BN=141
Conservative
Gr BN=141
Conservative
Gr CN=144
R-PCI
Gr CN=144
R-PCI
44
(31.0%)44
(31.0%)42
(29.8%)42
(29.8%)22
(15.3%)22
(15.3%)

Rank log p=0.004
R-PCI 84.6% (ci 78.7%-90.5%)
R-Lysis 68.7% (ci 61.1%-76.4%)
Conserv 70.1% (ci 62.5%-77.7%)
RESULTS 6 months RESULTS 6 months

p=0.13
R-PCI 93.8% (ci 89.8%-97.7%)
R-Lysis 87.3% (ci 81.9%-92.8%)
Conserv 87.2% (ci 81.7%-92.7%)
Mortality at 6 months
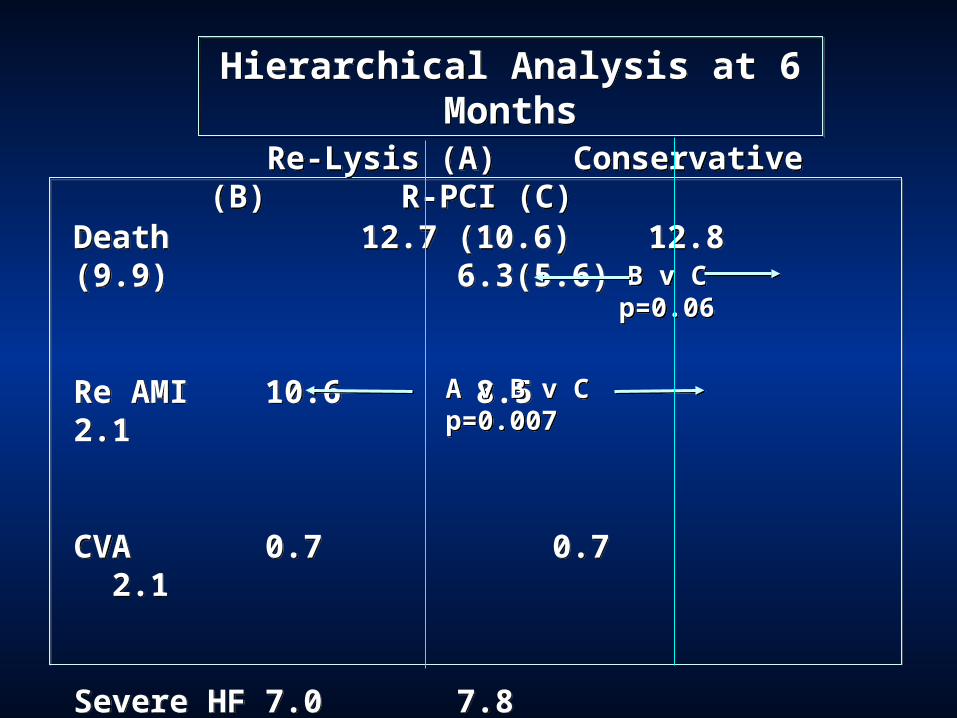
Hierarchical Analysis at 6 MonthsHierarchical Analysis at 6 Months
Death 12.7 (10.6) 12.8 (9.9) 6.3(5.6)
Re AMI 10.6 8.5 2.1
CVA 0.7 0.7 2.1
Severe HF 7.0 7.8 4.9
Death 12.7 (10.6) 12.8 (9.9) 6.3(5.6)
Re AMI 10.6 8.5 2.1
CVA 0.7 0.7 2.1
Severe HF 7.0 7.8 4.9
Re-Lysis (A) Conservative (B) R-PCI (C) Re-Lysis (A) Conservative (B) R-PCI (C)
B v C p=0.06
B v C p=0.06
A v B v C p=0.007
A v B v C p=0.007

MAJOR MINOR
( > 3g/dl) ( 2g/dl -3 g/dl)
MAJOR MINOR
( > 3g/dl) ( 2g/dl -3 g/dl)
5
15
20
10
OVERT Bld No OVERT Bld OVERT Bld No OVERT Bld OVERT Bld No OVERT Bld OVERT Bld No OVERT Bld
4.9
2.1
18.7
3.5
8.58.4
22/27
(82%) sheath
22/27
(82%) sheath
%%
<0.0003
Bleeding Outcomes Bleeding Outcomes
9/9
(100%) sheath
9/9
(100%) sheath
15.5
6.2
3.53.5
15.6
10.4
ns
Lysis C RPCI Lysis C RPCI Lysis C RPCI Lysis C RPCI
Fatal Bleeding complicationsRescue: 0
Conservative: 3Repeat Thrombolysis: 5

AB
Conclusion
1. REACT shows a clear benefit of rescue angioplasty for failed thrombolysis
2. Comparison with MERLIN will be important
3. Forget Re-thrombolysis !




















![[John Chadwick, Lydia Baumbach] the Mycenaean Greece](https://img.pdfslide.net/doc/110x75/55cf8569550346484b8db41e/john-chadwick-lydia-baumbach-the-mycenaean-greece.jpg)