Embed Size (px)
Citation preview

Medical Respite for Individuals Experiencing
Homelessness
A Review for London, Ontario
Dr. Abe Oudshoorn

AuthorAbe Oudshoorn, RN, PhDAssistant ProfessorSchool of NursingWestern UniversityN6A [email protected] x86042
April 2013

Table of Contents
1 Background 1
2 Defining the Target Population 4
3 Understanding the Need 8
4 Building the Model 10
5 Anticipated Outcomes 12
6 Finances: Considerations 13
7 Local Opportunities 14
8 References 15
Medical Respite for People Experiencing Homelessness iii

1 BackgroundThe health challenges faced by people experiencing homelessness are well documented in both scholarly and grey literature. This is supported anecdotally in London, Ontario, where those in both the health and social services have long expressed concerns that our current medical system is failing these individuals in some manner. This project started as a reflection that street level health outreach might fill some of the gaps, but pursuit of this direction led to a larger review of health services for those experiencing homelessness. The report from this review is available for download at http://www.abeoudshoorn.com/wp-content/uploads/2013/02/Health-Services-and-Homelessness-2011-FINAL.pdf. A summary of this work appears on the next page.
Subsequent to this review of health services, the working group looked specifically at the health needs of 19 individuals considered ‘hard to house’, and receiving intensive case management services through London CAReS. A summary of this review appears on page 3 of this report. At the same time as this process was unfolding, a group of service providers led by shelter and healthcare providers began to meet to address the particular gap of respite or infirmary care. There was a shared concern in the community that individuals experiencing homelessness were being discharged from hospital or long-term care without the adequate supports to meet their health needs. This was leading to poorer health outcomes as well as increased use of services, such as hospital readmissions or emergency room use. Healthcare providers shared frustrating anecdotes of individuals with wounds, new diagnoses, difficult to manage medications, or requiring physiotherapy ‘disappearing’ into the community, while shelter providers spoke of the high degree of health needs of individuals accessing their services that were beyond the expertise of staff.
Ultimately, this direction was considered worth pursuing, with a desire to find the most appropriate model and to make the services sustainable. The purpose of this report is to provide background information to assist in the development of a program that might meet the needs of individuals in London, Ontario. The term ‘respite’ is used throughout, rather than infirmary, although these have been used at times for similar and at times for different models.
1

Medical Respite for People Experiencing Homelessness 2

Medical Respite for People Experiencing Homelessness 3

2 Defining the Target PopulationA review of the resources presented in the background demonstrates that the health needs
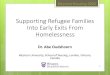
of people experiencing homelessness are extensive. There is room for improvement on mobile healthcare, communication/integration, quality of care provided, access to dental care, and access to appropriate primary care. As the graph below shows, these health needs are not unique to people who are absolutely homeless, but correlate inversely with income across all income quartiles:
Therefore, there is no end of opportunities to target health services to people most at risk of poor health outcomes. For the purpose of this project, we will look particularly at those who are experiencing homelessness, as this population is particularly susceptible to poor health outcomes. As stated by Oudshoorn (2011):
In spite of the variation in causes and experiences of homelessness, for all who experience it, homelessness is an experience that compromises one’s health (Crowe & Hardill, 1993; Hatton & Fisher, 1999). And, as suggested by the Ottawa Charter (World Health Organization, 1986), the health challenges that arise during homelessness have to do with more than physical illness, and include the social determinants of health (e.g. income and social status, social support networks, education and literacy, employment/working conditions, social environments, physical environments, personal health practices and coping skills, healthy child development, biology and genetic endowment, health services, gender, and culture; Public Health Agency of Canada, PHAC, 2003). For most individuals, homelessness is a transitional state rather than a
Medical Respite for People Experiencing Homelessness 4

permanent situation (Buck, Rochon, Davidson & McCurdy, 2004), and during this time much can occur that exacerbates existing health concerns, or creates new ones.
Understanding the health impacts of homelessness is somewhat complicated in that many of the conditions faced (such as mental illness, substance use and chronic health conditions) can be both causes of and results of homelessness (NHCHC, 2009), but the case of negative health impacts of homelessness is well established (Daiski, 2007). One study of homeless women found that 35% had been hospitalized in the past year, five times the rate of the national average (Lim, et al., 2002). Most striking in terms of the negative health effects of homelessness is the high mortality rates of homeless persons (Frankish, Hwang & Quantz, 2005; Levy & O’Connell, 2004), including youth (Klein, et al., 2000), with the life expectancy of homeless persons averaging 35-47 years (Podymow, Turnbull & Coyle, 2006). This coincides with findings from Denmark of age and sex standardised mortality ratios for homeless persons of 2.8 for men and 5.6 for women (Nordentoft & Wandall-Holm, 2003), and an average age of death for homeless persons in Germany of 44.5 years (Ishorst-Witte, Heinemann & Puschel, 2001).Statistics on acute and chronic conditions and homeless persons are striking. Street Health in Toronto, Canada found that 55% of homeless persons have a serious physical health condition, and 63% of these have more than one (Street Health, 2005). Kinzel, Flagg and Vredevoe (1991), in an ethnography of self-perceived health amongst homeless persons, found that 25% were currently experiencing hypertension. Burt and colleagues (1999), in a survey of homeless persons in 76 U.S. census areas found that 46% had chronic conditions and 26% had acute infectious conditions. These chronic conditions often occur very prematurely amongst homeless persons in comparison to housed persons (Daiski, 2007). Additionally, in Paris, France, Kovess and Mangin Lazarus (1999) found a lifetime incidence of 58% for psychiatric conditions and 34% for substance abuse amongst homeless persons. In Western nations, psychiatric conditions such as psychosis, major depression, personality disorders and addictions are higher amongst homeless persons than the general public (Fazel, Khosla, Doll & Geddes, 2008). These conditions can, in part, be caused by and exacerbated by the challenges that homeless persons face: taking medications as prescribed (Burt, et al., 1999), risk of injury (Ensign & Gittelsohn, 1998), lack of access to good hygiene (Gerberich, 2000), poor nutrition and exposure to the elements (Jackson & McSwane, 1992), social isolation (Kinzel, Flagg & Vredevoe, 1991), and exposure to physical and sexual violence (Levy & O’Connell, 2004). When asked about their health concerns, homeless men focused on broader health and safety needs and acute conditions, rather than chronic illnesses (Lafuente, 2003), an important consideration for the structuring of health care services for homeless persons. And, in the face of these myriad difficulties, studies have found that homeless persons still actively work to promote their health, but often in what would be considered unconventional ways (McCormack & MacIntosh, 2001; Rew, 2003). For example, Rew (2003) demonstrates how homeless youth may carry weapons as a means of self-preservation, or use dangerous means of transportation such as riding on the backs of buses in order to access free meals or shelters before they are closed.
Therefore, a strong relationship between homelessness and poor health is well established within the literature. The next challenge in addressing this population and health is how we define
Medical Respite for People Experiencing Homelessness 5

‘homelessness’. The image below is a summary of the recognized Canadian definition of homelessness:
Although this begins to define the focus of services, in terms of respite care this needs to be further defined. Not every person who is homeless and exiting hospital requires respite care. Similarly, respite services can include more than post-discharge care, including palliative care, medical detox, or pre/post-natal care for homeless women. Lastly, there is little value to the system by duplicating existing resources. Our current medical system already provides options for care including homecare, long-term care, advanced level of care, and health providers who
Medical Respite for People Experiencing Homelessness 6

visit social services. Therefore, we need to consider a very particular group of people experiencing homelessness with particular health needs which is:
1. Those who are well enough to be discharged from hospital but are too ill for shelter; or
2. Those who have behavioural or health concerns (such as addictions and mental illness) that have limited their options for healthcare and are too ill for shelter (ex. have been kicked out of long-term care); or
3. Those who have behavioural or health concerns who have left hospital against medical advice (AMA) and are too ill for shelter; and
4. Whose health needs could not be met with existing services.
These narrow definitions account for the above mentioned existing options, such as homecare nurses who will visit in the shelter, that still fail to meet the needs of some individuals experiencing homelessness. In particular, those most in need of alternatives are those considered ‘hard to serve’ within the existing modalities. These are primarily individuals with concurrent mental health and addiction challenges, often combined with negative coping/survival behaviours. Consider the following case:
This is the type of complexity that challenges existing modes and resources. If not well supported, these individuals end up consuming a massive amount of time and resources through interaction with social services, emergency services, police services, and acute care services. Without intensive support, you could anticipate John being admitted on a Form 1, and/or requiring a subsequent surgery up to and including amputation, and/or ending up in intensive care, and/or dying. You could change the case to have him female, addicted to alcohol, suffering from an acute respiratory condition, kicked out of long-term care, and showing up at a walk-in clinic, and the challenges would be much the same.
Medical Respite for People Experiencing Homelessness
John is a 39 year old male who has been moving between shelters for the past 2 years, but intermittently homeless over the past 13 years. John is a poly-substance user as well as having been diagnosed in the past with all of: depression, bi-polar disorder, and schizophrenia. John was assaulted 3 months ago, resulting in a compound fracture of his tibia. Following an open reduction internal fixation surgery, John has returned twice to hospital for both a wound infection and cellulitis. John left the hospital AMA yesterday after a confrontation with staff regarding suspected misappropriation of medication. Although connected with CCAC during his stay, he made no plan for an address subsequent to his impromptu exit, and shows up at crash beds. He has a large leg dressing, visibly oozing, has difficulty walking, but told staff he would simply take off if an ambulance was called. John needs to complete a course of antibiotics, he needs an x-ray to ensure the initial hardware is still in place, and he needs ongoing physiotherapy to assist him with ambulation.
7

3 Understanding the NeedAlthough the individuals described above have multiple healthcare challenges, is there a
need for medical respite as a component to address these challenges? Medical respite care for people experiencing homelessness is a well established service to:
Assist those particularly with active addictions in a high tolerance environment; Provide temporary housing until the medical need has passed; and Provide dignified palliative care for those with health and social complexities;
Research has demonstrated a number of positive outcomes from this service for both improved health outcomes and decreased use of hospital resources, particularly through decreased re-hospitalization.
Improved Outcomes
As medical respite programs are a relatively new service area, there is limited research available on the health outcomes if individuals using the services. Additionally, as the individuals accessing the services often have concurrent physical health, mental health, and addictions issues, service goals need to be realistic. In many cases the principles of palliative care are more appropriate than rehabilitative medicine. Lastly, as significant outcomes of decreased service use (as described below) have been demonstrated, there is little appetite for randomized trials as usual care holds little appeal. That said, health outcomes at a few American medical respite centres are available.
Gundlapalli and colleagues (2005) describe the services of Fourth Street Clinic in Salt Lake City, Utah, which provides a network of respite care crossing multiple models. Patients are triaged to either shelter-based care, motel-based care, care in supportive housing, or specialized long-term care. This model serves an average of 337 patients a year, and includes healthcare providers who are both mobile and on-site. Overall, the key finding of health outcomes is that all patients are discharged in relatively stable condition. Greysen and colleagues (2012), exploring discharge planning for people experiencing homelessness, highlight the integrated challenges of health and housing, and note that 42% of those who are homeless and avoid healthcare services do so based on a concern of being unable to obtain or maintain shelter. So, not only does lack of stable housing tenure lead to difficulty in following-up with individuals experiencing homelessness, it also leads to service avoidance. Medical respite offers an opportunity to bridge the shelter gap, leading to increased engagement in care.
Podymow and colleagues (2006) present the most thorough review of health outcomes in medical respite services found in the literature. They reviewed a 20-bed shelter-based respite centre in Ottawa, Ontario, over a 3 year period. The following outcomes were observed:
18.6% obtained a new family physician, 59.2% achieved medication adherence, 55% achieved appointment adherence.
A similar study in Amsterdam over 7 years found that only 5% of respite patients saw a worsening of their condition while in care (van Laere, de Wit & Klazinga, 2008). Although
Medical Respite for People Experiencing Homelessness 8

these numbers lack comparators, those with experience with individuals experiencing concurrent physical health, mental health, and addictions challenges in the context of homelessness will recognize these as very positive statistics.
Decreased Service Use
Far more data is available on system-level outcomes, in particular decreased use of emergency services and hospital re-admissions. Emergency service use by individuals experiencing homelessness is known to be a significant challenge for healthcare systems, both in terms of resource consumption, and in representing a less-than-optimal mode of primary care. Rates of emergency room use by people experiencing homelessness have been measured as high as 72 visits per 100 individuals per year, with a four times greater rate of re-visiting the emergency within three days than the general population (Ku, Scott, Kertesz & Pitts, 2010). This is paralleled by a finding of a 47.8% rate of re-visiting emergency within 28 days of discharge, in an Australian study (Moore, Gerdtz, Hepworth & Manias, 2010), and a rate of 40.8% of individuals making one or more visits per year in San Francisco (Kushel et al., 2002). Therefore, any alteration to rates of emergency room use will have significant positive impacts both for system costs and patient outcomes.
In the absence of respite services, supportive housing has been used to improve health outcomes. Case-managed supportive housing in Chicago led to an average reduction of 0.5 hospitalizations and 1.2 emergency department visits per year for homeless adults experiencing a chronic illness (Sadowski, Romina, VanderWeele & Buchanan, 2009). The same research team using a randomized controlled methodology demonstrated healthcare savings of $6,307 per person (Basu, Buchanan & Sadowski, 2012).
The best outcomes in terms of decreased service use have been demonstrated with full medical respite services. Ultimately, respite services lead to less time in hospital, whether it be calculated as overall days admitted or hospital readmissions. Kertesz and colleagues (2009) reviewed hospital records in Boston over a period of three years and found that a 90-bed respite program led to a 50% decrease in odds of readmission compared to discharge to shelter or own care. This also represented lower odds of readmission than discharge to long-term care. The authors hypothesized that the mean cost savings of $1,935 per patient would cover the additional cost of respite services over-and-above long-term care, though did not cost it against shelter or affordable housing. A review of challenges of discharge planning for individuals experiencing homelessness recommended formalizing relationships between hospitals and medical respite centres due to decreased rates of readmission at a cost of less than 10% of acute care bed (Fader & Phillips, 2012).
Researchers from Chicago demonstrated decreased overall days in hospital due to medical respite care (Buchanan, Doblin, Sai & Garcia, 2006). In a three year retrospective review, use of a 60-bed respite home resulted in 4.7 fewer hospital days per year compared with a control group (those turned away due to unavailability of beds). This is significantly higher than the 0.5 days achieved by the supportive housing model reported above, and equates to a 58% reduction. Ultimately, those receiving respite care cost $706 less per day of care.
Medical Respite for People Experiencing Homelessness 9

4 Building the ModelA variety of models are available for respite care, including care that goes to where
people are housed (including motel, social housing, or private housing), care that is provided within a shelter, or a stand-alone facility. Within each of these modes there are a variety of service designs depending on resources available, and this will be explored further in section 7.
In the current context, respite care provided where people are housed does not appear to be a promising direction for a number of reasons. Most importantly, reflecting on the target population defined above, individuals with concurrent physical health, mental health, and addiction challenges face severe limitations to securing and maintaining housing tenure. There are already existing homecare services for those who are stable and stably housed, which function well to meet the needs of most patients. However, thinking of the target population, it is not surprising that research presented in the preceding section shows minimal benefit to mobile services. Patients not being present for appointments, refusing entry to healthcare providers, or coming into conflict with providers are known challenges of providing homecare in this context. That said, it is important to note that this does not preclude offering mobile primary care services for people experiencing homelessness with complex challenges, but in a scenario of acute distress or post-hospital discharge, missed appointments and unstable housing are exactly the challenges leading to poor outcomes. Mobile primary care and respite care can be delivered hand-in-hand, such as with Ottawa Inner City Health, but meet two different types of need.
Shelter-based care is a fairly common model of service across North America. This is an attractive model in that limited capital expense is required, other than possible conversion and installation of equipment (such as wall-mounted oxygen). However, shelter-based programs face a number of limitations:
Shelters have existing rules around substance use and behaviours, which often preclude the very individuals identified as the target population,
Those who are vulnerable due to their current health situation may be victimized by other shelter residents, or, conversely, individuals with significant concurrent challenges can have a negative impact on the environment of the shelter,
There is a temptation to create minimally-staffed programs in shelters that meet the needs of some, but not the target population,
Being a resident of a shelter versus a patient under the charge of a physician can lead to more tenuous residence due to differing philosophies,
There is a risk of disagreement around admissions.
All of these limitations are dependent on the context of the community, the availability of shelter space, the resources available, and the philosophies of shelter providers. That said, shelter-based systems are often considered ‘stepping stones’ to more ideal models but become permanent if resources for stand-alone services are not made available. Because of the limitations, these models don’t necessarily demonstrate the full cost effectiveness and health outcomes possible in medical respite. Additionally, if those with the most complex challenges are precluded from these models, the very pressures on systems that led to their creation may continue unabated.
Therefore, the ideal model for medical respite is a stand-alone facility, with full freedom to create a model of care for the target population. Advantages of a stand-alone facility include:
Medical Respite for People Experiencing Homelessness 10

The ability to create policies around substance use and challenging behaviours that adapt to the needs of those who may be both the most ill and the most addicted,
Full control of the lead physician or physician group to determine both admission and discharge of patients/residents,
Physical separation from individuals who may be harmful in the patient’s life, Freedom to determine length of stay based on medical need, including a stay of
indeterminate length for example in the case of palliative care, The ability to create the physical structure optimally designed for the type of care and the
type of patient being served.
Ultimately, the reality of the need is that addiction to drugs and/or alcohol is the primary issue that limits access of the target population to existing services. Individuals who are not recovery-ready but yet have severe health needs both need and deserve adequate care, but are not well served within existing services. The physician managing the care needs to have the freedom to practice within a harm reduction model, with discharge considering the individual’s health condition first.
The down-side of a stand-alone facility is obviously cost. This means both capital and operating expenses to be met. Stand-alone facilities will also face zoning requirements and may encounter resistance from neighbourhood residents depending on where they are sited. However, an optimal model will equate to optimal system cost-savings, potentially balancing the additional capital expenses. The final dynamic is financial impact on the patient. Any decrease in an OW or ODSP cheque caused by admission to the facility will provide a strong disincentive for the patient to remain until sufficient recovery has been achieved.
Medical Respite for People Experiencing Homelessness 11

5 Anticipated Outcomes To be justified, medical respite for people experiencing homelessness must provide better
outcomes than usual care. As presented in Section 3, the primary outcomes to be measured in delivering such a program are health outcomes for the patient, and cost benefits for the system.
Medical Respite for People Experiencing Homelessness
Health Outcomes
Key Outcomes Deemed healthy enough for discharge Discharge from facility to housing Dying with dignity
Additional Outcomes Patient’s perceived health and wellbeing Medication management (ex. appropriate antibiotic) Medication and treatment plan compliance Increased self-management of condition Reduced harm of substance use Receipt of a health card/drug card Relational engagement with healthcare team (onsite or offsite) Discharge from facility to shelter Other measures of improved health (ex. decreased viral load in case
of communicable diseases, increased ambulation, progression of wound healing, etc.
System Outcomes
Decreased use of 911 services Decreased use of emergency department Decreased readmission to hospital or long-term care Decreased days of stay in hospital or long-term care Decreased use of primary care services other than the patient’s
primary care physician/group or respite care provider
12

6 Finances: Considerations Full costing of medical respite services is beyond the scope of this report, and would be
part of a business plan once a community, model, and partners are determined. However, the following considerations are important when thinking of costing:
1) Both a shelter model and stand-alone facility model will require capital dollars, whether just for renovations or for full purchasing of land and building of the facility. Full consultation will be required with the healthcare team as scope of the services to be provided and the target population will both influence building design and cost (ex. space for a Hoyer Lift, ‘over bed’ built-in equipment).
2) Start-up equipment costs can be significant, so partnership with existing health services as beneficial both for sharing equipment and for purchasing at an optimal price.
3) The largest ongoing cost will be staffing. Therefore, optimizing use of existing staff such as primary care providers who work in the sector, homecare services, and other mobile providers is important for minimizing costs.
4) Staffing should include 24/7 nursing support, and will need to include access to a physician.
5) Staffing needs may increase unexpectedly in the situation of a patient becoming terminally ill.
6) Health provider students can supplement existing services, but should not be a core component due to the requirement of having adequate and appropriate supervision.
7) Ongoing equipment and supply cost considerations should include less common supplies such as harm reduction equipment, and pest extermination expenses.
8) Costs may not necessarily be less than equivalent acute care services, but should be justifiable based on factors such as shorter stays, less readmissions, and less likelihood of requiring critical care.
9) Cost justifications should account for real-world health system economics where freeing beds in an over-stretched system does not necessarily translate to true savings but rather decreases the waitlist for access to care.
10) Being managed by an existing organization will save time and costs involved with registering a new non-profit corporation.
11) Developing relationships with existing shelters, primary care providers, long-term care facilities, and acute care facilities will prevent empty beds.
The National Health Care for the Homeless Council – Respite Care Providers’ Network offers an essential planning tool:
Medical Respite for People Experiencing Homelessness
Medical Respite Program Development Workbook:
http://www.nhchc.org/wp-content/uploads/2011/09/WorkBook.pdf
13

7 Local Opportunities This final section explores the local context of London, Ontario and particular
opportunities to consider in establishing a medical respite program. This may be of interest to other readers in terms of reflecting on your own opportunities, but does only represent a particular moment in time in a particular city.
The ideal model as explored in this document and as considered by the working group in London is a small stand-alone facility of approximately 6-8 beds, offering an unlimited length of stay (until the resident is well enough to leave), accommodating individuals with concurrent physical health, mental health, and addictions challenges, and with access to 24 hour nursing care as well as one or more physicians and nurse practitioners. Housing post-discharge would be a primary consideration for all residents, and finding housing would begin upon admission. Equipment and supplies would be available to serve individuals with such conditions as complicated upper respiratory tract infections, skin infections, abscesses, new diagnoses of chronic disease (ex. diabetes), cancer being actively treated, wounds, fractures, or any other variety of conditions that become problematic in the context of homelessness and concurrent challenges. Length of stay could be short, to simply complete a course of medication for example, or long, such as to provide palliative care. Discharge to traditional forms of acute, secondary, or tertiary care would always be consider if individuals overcome the challenges that makes these modes problematic. For example, an individual successfully started on methadone maintenance therapy and obtaining an apartment through a housing worker might demonstrate improvements since admission that would make homecare sufficient to meet her medical needs.
London has a wealth of expertise than can be leveraged to minimize staffing costs. London InterCommunity Health Centre (LIHC) and the Centre of Hope Family Health Team are currently collaborating on providing healthcare to the exact population that would access this service. Although they do not have the space to provide the service at this time, they are both open to finding ways to leverage the expertise of their staff on the project. In particular, Dr. Jamie Harris from LIHC has a strong interest in this type of model, seeing the need for many patients over the years whom he serves as a family physician. John Gordon Home has a history of providing respite style care in the context of HIV/AIDS, and more recently Hepatitis C. Although they do not have the staff resources at this time to manage the program themselves, they have offered their expertise and experience to help develop the particulars of operations. The South West CCAC has engaged over the years in programs to try to provide service to those with a chaotic lifestyle. They have expressed interest in this model, as it would provide a home address to which their services could go to treat clients. Shelter providers, including Mission Services of London, the Unity Project, and the Salvation Army have expressed support of this model as their staff and services are often taxed by the target population, and they are very open to finding ways to meet the needs of these individuals. The Salvation Army is open to considering space within the Centre of Hope for the program, although at this point in time, this is not considered the optimal model. The behaviours and substance use challenges of the target population would possibly lead to discharge based on other policies than optimal health outcome. London CAReS has experience providing housing support to those facing the most barriers to housing. Their expertise is well aligned with finding and supporting post-discharge housing, and their staff likely have relationships with most of those who would use the program. Other partners are engaged with the project and will bring their own expertise. Still others are likely to come on as partners in the future.
Medical Respite for People Experiencing Homelessness 14

8 ReferencesBasu, A., Buchanan, D., Sadowski, L. (2012). Comparative cost analysis of housing and case management program for chronically ill homeless adults compared to usual care. Health Services Research, 47(1), 423-443.
Buchanan, D., Doblin, B., Sai, T., & Garcia, P. (2006). The effects of respite care for homeless patients: A cohort study. American Journal of Public Health, 96(7), 1278-1281.
Gundlapalli, A., Hanks, M., Stevens, S.M., Geroso, A.M., Viavant, C.R., McCall, Y., Lang, P., Bovos, M., Branscomb, N.T., & Ainsworth, A.D. (2005). It takes a village: A multidisciplinary model for the acute illness aftercare of individuals experiencing homelessness. Journal of Health Care for the Poor and Underserved, 16(2), 257-72.
Fader, H., Phillips, C. (2012). Frequent-user patients: reducing costs while making appropriate discharges. Journal of the Healthcare Financial Management Association, 66(3), 98-100.
Greysen, S.R., Allen, R., Lucas, G., Wang, E., Rosental, M. (2012). Understanding Transitions in Care from Hospital to Homeless Shelter: a Mixed-Methods, Community-Based Participatory Approach. American Journal of General Internal Medicine, 27(11), 1484-1491.
Haley, L. (2003). Respite care reduces hospitalization of homeless. Medical Post, 39(20), 8.
Kertesz, S.G., Posner, M.A., O’Connell, J.J., Swain, S., Mullins, A.N., Schwartz, M., & Ash, A.S. (2009). Post-hospital medical respite care and hospital readmission of homeless persons. Journal of Prevention and Intervention in the Community, 37(2), 129-42.
Ku, B., Scott, K., Kertesz, S., Pitts, S. (2010). Factors Associated with Use of Urban Emergency Departments by the U.S. Homeless Population. Public Health Rep, 125(3), 398–405.
Kushel, M.B., Perry, S., Bangsberg, D., Clark, R., Moss, A. (2002). Emergency department use among the homeless and marginally housed: Results from a community-based study. American Journal of Public Health, 92(5), 778-784.
Moore, G., Gerdtz, M., Hepworth, G., Manias, E. (2010). Homelessness: patterns of emergency department use and risk factors for re-presentation. Emergency Medicine Journal, 28(5), 422-427.
Moore, G., Gerdtz, M., Manias, E. (2007). Homelessness, health status and emergency department use: an integrated review of the literature. Australasian Emergency Nursing Journal, 10(4), 178-185.
Podymow, T., Turnbull, J., Tadic, V., & Muckle, W. (2006). Shelter-based convalescence for homeless adults. Canadian Journal of Public Health, 97(5), 379-83.
Medical Respite for People Experiencing Homelessness 15

Sadowski, L., Romina, K., VanderWeele, T., Buchanan D. (2009). Effect of a Housing and Case Management Program on Emergency Department Visits and Hospitalizations Among Chronically Ill Homeless Adults. The Journal of American Medical Association, 301(17), 1771-1778.
van Laere, I., de Wit, M., & Klazinga, N. (2009). Shelter-based convalescence for homeless adults in Amsterdam: A descriptive study. BMC Health Services Research, 9, doi:10.1186/1472-6963-9-208.
Medical Respite for People Experiencing Homelessness 16

















![The Experience of Homelessness: A Qualitative Study Using ... › 623947 › 1 › Zoe_Brown[1].pdf · Previous research concerning homelessness has mainly used quantitative methodology](https://img.pdfslide.net/doc/110x75/5f0c17027e708231d433b0f2/the-experience-of-homelessness-a-qualitative-study-using-a-623947-a-1-a.jpg)