-
7/29/2019 Abnormal Lfts Autumn 2005
1/59
Evaluation of Abnormal LiverFunction Tests
Dr Chris Hovell
Consultant Gastroenterologist
Dorset County Hospital
-
7/29/2019 Abnormal Lfts Autumn 2005
2/59
LFTs
Markers of hepatocellular damage
Cholestasis
Liver synthetic function
-
7/29/2019 Abnormal Lfts Autumn 2005
3/59
Markers of Hepatocellular damage
(Transaminases) AST- liver, heart skeletal muscle, kidneys,
brain, RBCs
In liver 20% activity is cytosolic and 80% mitochondrial
Clearance performed by sinusoidal cells, half-life 17hrs
ALTmore specific to liver, v.low concentrations inkidney and
skeletal muscles.
In liver totally cytosolic.
Half-life 47hrs
-
7/29/2019 Abnormal Lfts Autumn 2005
4/59
Gamma-GThepatocytes and biliary epithelial cells,pancreas, renal
tubules and intestine
Very sensitive but Non-specific
Raised in ANY liver discease hepatocellular or cholestatic
Usefulness limited Confirm hepatic source for a raised ALP
Alcohol
Isolated increase does not require any further evaluation,
suggest watch and rpt 3/12 only if other LFTs becomeabnormal
then investigate
-
7/29/2019 Abnormal Lfts Autumn 2005
5/59
Markers of Cholestasis
ALPliver and bone (placenta, kidneys, intestines orWCC)
Hepatic ALP present on surface of bile duct epithelia
andaccumulating bile salts increase its release from cell
surface. Takes time for induction of enzyme levels so may
not be first enzyme to rise and half-life is 1 week.
ALP isoenzymes, 5-NT or gamma GT may be necessary to
evaluate the origin of ALP
-
7/29/2019 Abnormal Lfts Autumn 2005
6/59
Bilirubin, Albumin and Prothrombin time
(INR)
Useful indicators of liver synthetic function
In primary care when associated with liver
disease abnormalities should raise concern
Thrombocytopaenia is a sensitive indicator
of liver fibrosis
-
7/29/2019 Abnormal Lfts Autumn 2005
7/59
Patterns of liver enzyme alteration
Hepatic vs cholestatic
Magnitude of enzyme alteration (ALT >10x vsminor
abnormalities)
Rate of change
Nature of the course of the abnormality (mildfluctuation vs
progressive increase)
-
7/29/2019 Abnormal Lfts Autumn 2005
8/59
Patterns of liver enzyme alteration
Acute hepatitistransaminase > 10x ULN
Cholestatic
Mild rise in ALT
-
7/29/2019 Abnormal Lfts Autumn 2005
9/59
Acute hepatitis (ALT>10xULN)
Viral
Ischaemic
Toxins
Autoimmune
Early phase of acute obstruction
-
7/29/2019 Abnormal Lfts Autumn 2005
10/59
Acute hepatitis (ALT>10xULN)
ViralHep A, B, C, E, CMV, EBV
ALT levels usually peak before jaundice appears.
Jaundice occurs in 70% Hep A, 35% acute Hep B,25% Hep C
Check for exposure
Check Hep A IgM, Hep B core IgM andHepBsAg, Hep C IgG or Hep C
RNA
-
7/29/2019 Abnormal Lfts Autumn 2005
11/59
Acute hepatitis (ALT>10xULN)
Ischaemic- sepsis, hypotension
?most common cause in-patients
Often extremely high >50x
Decrease rapidly
LDH raised 80%
Rarely jaundiced
-
7/29/2019 Abnormal Lfts Autumn 2005
12/59
Acute hepatitis (ALT>10xULN)
Toxins - paracetamol (up to 50% of all cases of
Acute Liver Failure)
Ecstasy ( 2nd most common cause in the young2 in 70%
-
7/29/2019 Abnormal Lfts Autumn 2005
13/59
Acute hepatitis (ALT>10xULN)
Autoimmune
Rarely presents with acute hepatitis
Usually jaundiced and progressive liver failure
Raised IgG and autoantibodies (anti-SM, -LKM, -
SLA)
Liver biopsy Steroids and azathioprine
-
7/29/2019 Abnormal Lfts Autumn 2005
14/59
Acute hepatitis (ALT>10xULN)
Early phase- extrahepatic obstruction/cholangitis
Usually have history of pain
USSdilated CBD ? ERCP or lap chole
-
7/29/2019 Abnormal Lfts Autumn 2005
15/59
Cholestasis
Isolated ALP 3rd trimester, adolescents
Boneexclude by raised GGT, 5-NT or
isoenzymes May suggest biliary obstruction, chronic liver
disease or hepatic mass/tumour
Liver USS/CT most important investigation-
dilated ducts Ca pancreas, CBD stones, cholangioca or liver
mets
-
7/29/2019 Abnormal Lfts Autumn 2005
16/59
Cholestasis non-dilated ducts
Cholestatic jaundiceDrugs- Antibiotics, Nsaids,Hormones,
ACEI
PBCanti- mitochondrial Ab, M2 fraction, IgM
PSCassociated with IBD 70%, p-ANCA,MRCP and liver biopsy
Chronic liver disease
Cholangiocarcinomabeware fluctuating levels
Primary or Metastatic cancer, lymphoma
Infiltrativesarcoid, inflammatory-PMR, IBD
Liver biopsy often required
-
7/29/2019 Abnormal Lfts Autumn 2005
17/59
Dear Dr Hepaticus,
I have just reviewed our patient database and have identified
420 patientswith persistently abnormal LFTs whoare otherwise well
and are not knownto have liver disease. When can yousee them?
Yours,
Dr G Practice
-
7/29/2019 Abnormal Lfts Autumn 2005
18/59
COMMON CAUSES OF
ABNORMAL LFTS IN THE UK
Transient mild abnormalities which
are simply impossible to explain
Drugseg Statins
Alcohol excess
Hepatitis C
Non-Alcoholic Fatty Liver Disease
(NAFLD)
-
7/29/2019 Abnormal Lfts Autumn 2005
19/59
-
7/29/2019 Abnormal Lfts Autumn 2005
20/59
Investigation of Abnormal LFTs -ALT/AST 2-5x normal
(100-200)
History and Examination
Discontinue hepatotoxic drugs
Continue statins but monitor LFTsmonthly
Lifestyle modification (lose wt, reduce
alcohol, diabetic control) Repeat LFTs at 1 month and 6
months
-
7/29/2019 Abnormal Lfts Autumn 2005
21/59
Investigation of Abnormal LFTs
- Raised ALT / AST
If still abnormal at 6 months:
Consider referral to secondary care
Hepatitis serology (B, C) Iron studiestransferrin saturation +
ferritin
Autoantibodies & immunoglobulins
Consider caeruloplasmin
Alpha-1- antitrypsin
Coeliac serology
TFTs, lipids/glucose
Consider liver biopsy esp if ALT > 100)
-
7/29/2019 Abnormal Lfts Autumn 2005
22/59
Hepatits C
Most asymptomatic; acute hepatitis withjaundice is uncommon
80% will have chronic / persistent infection.Of these,
10% will develop cirrhosis of the liver 10years after
infection
20-30% will develop cirrhosis of the liver 30years after
infection
5% will develop hepatocellular carcinoma(liver cancer) 20 years
after infection.
-
7/29/2019 Abnormal Lfts Autumn 2005
23/59
Hepatitis C: Factors associated
with progression of liver disease The genotype of the virus
-IB
Acquiring the infection at an older age
Alcohol misuse
Male gender
Co-infection with Hepatitis B or HIV
-
7/29/2019 Abnormal Lfts Autumn 2005
24/59
Treatment of Hepatitis C
Hep C RNA by PCRLiver biopsy for genotype I, treatment
isrecommended for patients with moderate to
severe hepatitisPeg-interferon given by sc injection 1/
week,Ribavirin bd dose
Patients with genotypes II and III are treated
with for 6 months. Response rate 70% Patients with genotypes I,
IV, V, and VI aretreated with interferon and ribavirin for
12months, if responsive on viral load at 3/12.Response rate
30%-40%.
-
7/29/2019 Abnormal Lfts Autumn 2005
25/59
Prevalence of Inherited Liver Diseases
Disease HomozygoteFrequency
GeneFrequency
HeterozygoteFrequency
Haemochromatosis 1:400 1:20 1:10
1AT Deficiency 1:1600 1:40 1:20
Cystic Fibrosis 1:2500 1:50 1:25
Wilson's Disease 1:30,000 1:170 1:85
Leggett et alBrit J. Haem. 1990
-
7/29/2019 Abnormal Lfts Autumn 2005
26/59
Genetics of
Haemochromatosis Autosomal recessive
Mutations in HFE gene (C282Y and H63D)
Cause increased intestinal absorption of Fe
C282Y/C282Y and C282Y/H63D are
responsible for 95% of genetic
haemochromatosis
-
7/29/2019 Abnormal Lfts Autumn 2005
27/59
-
7/29/2019 Abnormal Lfts Autumn 2005
28/59
Screening Strategy for Haemochromatosis(HFE Associated)
1.Perform transferrin saturation (or UIBC)2. If 45% - repeat
fasting
3. If still 45% - perform HFE testing
4. If C282Y +/+ or C282Y/H63D +/+:
- perform serum ferritin and LFT- if SF > 1000 and/or LFT
abnormal
- Liver biopsy essential
5. If C282Y +/- :
- Counsel re:Alcohol NASH
HCV PCT
6. Venesection and family screening
-
7/29/2019 Abnormal Lfts Autumn 2005
29/59
Liver biopsy Findings inAbnormal LFTs
Skelly et al:
354 Asymptomatic patients
Transaminases persistently 2X normal
No risk factors for liver disease Alcohol intake < 21
units/week
Viral and autoimmune markers negative
Iron studies normal
Skelly et al. J Hepatol 2001; 35: 195-294
-
7/29/2019 Abnormal Lfts Autumn 2005
30/59
Liver biopsy Findings in AbnormalLFTs Skelly et al. J Hepatol
2001
6% Normal
26% Fibrosis
6% Cirrhosis
34% NASH (11% of which had bridgingfibrosis and 8%
cirrhosis)
32% Simple Fatty Liver
18% Alteration in Management
3 Families entered into screeningprogrammes
Oth Li bi Fi di i
-
7/29/2019 Abnormal Lfts Autumn 2005
31/59
Other Liver biopsy Findings in
Abnormal LFTs Skelly et al. J Hepatol 2001
Cryptogenic hepatitis 9% Drug induced 7.6%
Alcoholic liver disease 2.8%
Autoimmune hepatitis 1.9%
PBC 1.4% PSC 1.1%
Granulomatous disease 1.75%
Haemochromatosis 1%
Amyloid 0.3% Glycogen storage disease 0.31%
-
7/29/2019 Abnormal Lfts Autumn 2005
32/59
LIVER BIOPSY FOR
-
7/29/2019 Abnormal Lfts Autumn 2005
33/59
LIVER BIOPSY FOR
SERONEGATIVE ALT < 2X
NORMAL N = 249, mean age 58, etoh < 25 units per
week, 9% diabetes, 24% BMI > 27
ALT 51-99 (over 6 m)
72% NAFLD
10% Normal histologically
Others: Granulomatous liver disease 4%, Autoimmune2.7%,
cryptogenic hepatitis 2.5%, ALD 1.4%,metobolic 2.1%, biliary
1.8%
Ryder et al BASL 2003
LIVER BIOPSY FOR
-
7/29/2019 Abnormal Lfts Autumn 2005
34/59
LIVER BIOPSY FOR
SERONEGATIVE ALT < 2X
NORMALOf those with NAFLD:
56% had simple steatosis
44% inflammation and/or fibrosis
Risk of Severe Fibrotic Disease associated with:
BMI >27 Gamma GT > 2x normal
Ryder et al BASL 2003
-
7/29/2019 Abnormal Lfts Autumn 2005
35/59
Ultrasound in Liver Disease
Detects Fatty Liver
Increased echogenicity may not bespecific for fat
Unable to detect Inflammation orcirrhosis (unless advanced)
Therefore unable to discriminate betweenNASH and simple fatty
liver or identifyother types of liver disease (which mayinclude
fatty change)
Liver biopsy is the only way to make anaccurate diagnosis
It may be worth treating fatty liver for 6months before
considering referral for
biopsy
Non Alcoholic Fatty Liver
-
7/29/2019 Abnormal Lfts Autumn 2005
36/59
Non-Alcoholic Fatty LiverDisease
-
7/29/2019 Abnormal Lfts Autumn 2005
37/59
Type 1 Fat alone
Type 2 Fat + inflammationType 3 Fat + ballooning
degeneration
Type 4 Fat + fibrosis and/or Mallory
bodies
Only types 3 and 4 have been definitively
shown to progress to advanced liver disease
and can be classified as NASH
The spectrum of
Nonalcoholic Fatty Liver Disease
-
7/29/2019 Abnormal Lfts Autumn 2005
38/59
NAFLD - Classification and Causes
PRIMARY
Increased insulin resistance syndrome
Diabetes mellitus (type II)
ObesityHyperlipidemia
-
7/29/2019 Abnormal Lfts Autumn 2005
39/59
NAFLD - Secondary CausesDrugs Surgical Procedures
Miscellaneous
Corticosteroids Gastroplexy Hepatitis CSynth oestrogens
Jejunoileal bypass Abetalipoproteinaemia
Amiodarone Extensive small bowel Weber-Christian
Perhexiline resection disease
Nifedipine Biliopancreatic diversion TPN with glucoseTamoxifen
Environmental toxins
Tetracycline S.bowel diverticulosis
Chloroquine Wilsons disease
Salicylates MalnutritionIBD
HIVinfection
-
7/29/2019 Abnormal Lfts Autumn 2005
40/59
Prevalence of NAFLD andNASH
No good data - histological diagnosis
Car Crash post mortem study - 24%
NAFL, 2.4% NASH - Hilden et al 1977 (n=503)
USS - 16.4- 23% NAFL (Italy, and Japan)
-
7/29/2019 Abnormal Lfts Autumn 2005
41/59
Prevalence of NAFLD / NASH
High risk groups Severely obese subjects - 25% incidence of
NASH at laparoscopy
Type 2 diabetes - 28-55% NAFL
Hyperlipidaemia - 20-90% NAFL
Approx 60% of NAFL occurs in females
Many patients are neither obese nor diabetic(Bacon et al 1994,
George et al 1998)
-
7/29/2019 Abnormal Lfts Autumn 2005
42/59
Obesity and Fatty liver
Prevalence increases with weight
Up to 80% of obese individuals
Up to 10-15% of normal subjects
Correspondingly, 15-20% of morbidly obesesubjects and 3% of
non-obese subjects have
NASH Increasing prevalence in children
AGA, Gastroenterology 2002
-
7/29/2019 Abnormal Lfts Autumn 2005
43/59
NAFLD - Clinical Features
Mostly an incidental finding inasymptomatic individuals
ALT 2-5x normal
AST:ALT < 1 except in severe injury
ALP, GGT 2-3x normal
-
7/29/2019 Abnormal Lfts Autumn 2005
44/59
NASH - Natural History
15-50% of NASH patients have fibrosis or
cirrhosis at index biopsy James and Day 1998
In Aetiological studies NASH is now the mostcommon cause of
cryptogenic cirrhosis Caldwellet al 1999, Poonwala et al 2000
In a 19 year follow up study, steatosis (alone)did not progess
histologically Teli et al 1995
-
7/29/2019 Abnormal Lfts Autumn 2005
45/59
.
3.4
0
21
28
0
5
10
15
20
25
30
1 2 3 4
NAFL Types
%
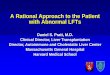
NASH - Natural History
10 year retrospective follow up study
n = 9811% Liver Related deaths in types 3 and 4
80% of those developing cirrhosis had fibrosis at index
biopsy
%Developing
Cirrhosis
Matteoni et al 1999
-
7/29/2019 Abnormal Lfts Autumn 2005
46/59
NASH-natural history
Steatosis only can progress to cirrhosis 1-2 % over
5-17yrs (Danish and Italian studies)
NASH + fibrosiscirrhosis 0% at 5yrs 12% at8ys
Prognosis in cirrhotics poor-30% developing liver-
related morbidity or mortality (liver failure +
HCC) over short period Adams et al Gastroenterology 2005
NASH - RISK FACTORS FOR
-
7/29/2019 Abnormal Lfts Autumn 2005
47/59
NASH RISK FACTORS FOR
FIBROSIS AND CIRRHOSIS
Independent risk factors in several studies: Age >45
ALT > 2x normal
AST/ALT ratio > 1
Obesity, particularly truncal
Type 2 diabetes
Insulin Resistance
Hyperlipdaemia (trigycerides > 1.7) Hypertension
Iron overload
NB: Studies are in selected groups; may not apply to all
patie
NASH Wh Sh ld H
-
7/29/2019 Abnormal Lfts Autumn 2005
48/59
NASH - Who Should Have a
Liver biopsy?To Identify Patients at Risk of Progression
restrict biopsy to patients
with some, if not all of:
ALT > 2x normal
AST > ALT At least moderate central obesity
NIDDM or Impaired glucose tolerance
Hypertension Hypertriglyceridaemia
Day, Gut 2002;50:5585-588
-
7/29/2019 Abnormal Lfts Autumn 2005
49/59
PATHOGENESIS OF NASHInsulin Resistance is the First Hit
NASH should be viewed as part of a
multifactorial disease
Commonly associated with syndrome X -85% in a retrospective
study (Wilner et al 2001)
Treatment strategies may be directed at
Insulin Resistance
NASH TREATMENT
-
7/29/2019 Abnormal Lfts Autumn 2005
50/59
NASH - TREATMENT
Steady Weight Loss - logical treatment Reduces fatty
infiltration
Improves LFTs
CAUTION - In some patients,
inflammation and fibrosis increaseespecially with rapid wt loss
(cf gastricand intestinal bypass)
Improved diabetic control - little histological
data
Exercise - patients with NAFLD have verypoor respiratory
quotients. LFTs and RQ
improve with exercise Elias 2001
-
7/29/2019 Abnormal Lfts Autumn 2005
51/59
NASHDRUG TREATMENT
No completed RCTs to date
CLOFIBRAT
No improvement in LFTs or histology over 1year in NASH (n=16)
Laurin et al 1996
Gemfobrozil
One randomized study, improved LFTs after 4weeks (n=46)
Basaranoglu et al 1999
-
7/29/2019 Abnormal Lfts Autumn 2005
52/59
NASH - Drug TREATMENT 2
Ursodeoxycholic Acid
3 open label studies (n = 24, 24, 31)
One randomised (vs diet alone)
Improvement in aminotransferases
12 month study demonstrated improvement in
steatosis but not other histological features RCT trial now
underway
* Laurin et al 1996, Guma et al 1997, Ceriani et al 1998
-
7/29/2019 Abnormal Lfts Autumn 2005
53/59
NASH - DRUG TREATMENT 3
ANTIOXIDANTS
Betaine (methionine)
Improved LFTs, steatosis and inflammation
n = 8, 12 months therapy, Abdelmalek et al 2000
N-Acetylcysteine Improved LFTs
n = 11, Gulbahar et al 2000
Vitamin E - Tocopherol
Improved LFTs over 4-10 months
n = 11, Lavine et al 2000
NASH DRUG TREATMENT
-
7/29/2019 Abnormal Lfts Autumn 2005
54/59
NASH - DRUG TREATMENT 4
Insulin Resistance
Metformin Improves sreatosis in ob/ob leptin deficient mouse
Decreased Transaminases in non-diabetic subjectswith NASH
compared with diet alone over 4m
Reduced liver volume
n = 20, Marchesini et al 2001
RCT planned by BASL
Troglitazone
Improved LFTs but no histological change n = 6, 4 months,
Caldwell et al 2001
-
7/29/2019 Abnormal Lfts Autumn 2005
55/59
Management of NAFLD
-
7/29/2019 Abnormal Lfts Autumn 2005
56/59
NAFLD CONCLUSIONS
NAFLD is common
A small proportion progress to cirrhosis
NASH is the commonest cause of cryptogeniccirrhosis
More information needed on prevalence,
pathogenesis and natural history RCTs urgently needed -
Metfomin,
antioxidants and UDCA
-
7/29/2019 Abnormal Lfts Autumn 2005
57/59
Abnormal LFTs - Conclusions
Many abnormal LFTs will return to normalspontaneously
An important minority of patients withabnormal LFTs will have
importantdiagnoses, including communicable andpotentially life
threatening diseases
Investigation requires clinical assessmentand should be timely
and pragmatic
GUIDELINES TO IX AND BX OF PATIENTS WITH ABNORMAL LFTs AND NO
CLEAR
-
7/29/2019 Abnormal Lfts Autumn 2005
58/59
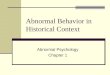
GUIDELINES TO IX AND BX OF PATIENTS WITH ABNORMAL LFTs AND NO
CLEAR
DIAGNOSIS AFTER ROUTINE TESTS: WITH EMPHASIS ON FATTY LIVER AND
NASH AS
UNDERLYING DIAGNOSIS
SCREEN FOR XS ALCOHOL CONSUMPTION
SCREEN FOR OCT/PD/RD DRUGS
INTERVENE AND REVIEW
INTERVENE AND REVIEW
SEROLOGICAL INVESTIGATIONS* NEGATIVEUSS NO SPECIFIC
DIAGNOSIS
NO CLEAR CLINICAL (e.g. FHx A1 disease/xanthelasma/Signs
CLD)
ASSOCIATIONS WITH LIVER DISEASE
RE-EVALUATE DIAGNOSIS
AND BIOPSY
ABNORMAL
CLINICAL SIGNS
PRESENT
NO CLINICAL SIGNS
PERSISTENT ABNORMAL
LFTs > 6/12
NO CLINICAL SIGNS
ALT >3x normal
High risk LFT profile
MEASURE:TG
Chol.
AST/ALT Ratio
TFTs
BP
Fasting Blood Sugar
Calculate BM1
CONFIRM
TREATMENTEFFECTIVE
LIFESTYLE MODIFICATION
LFTs NOT IMPROVED
RE-EVALUATE CLINICAL RISK
FACTORS
CONSIDER BIOPSY AND
FURTHER IMAGING
SEE GUIDANCE NOTES
LFTs IMPROVED
LFTs WORSEN OR BECOME
ABNORMALRETURN TO NORMAL OR IMPROVE
MONITOR EFFECTIVENESS
MONITOR
LFTs WORSEN OR BECOME
ABNORMAL
IF ABNORMALTREAT
-
7/29/2019 Abnormal Lfts Autumn 2005
59/59
GUIDANCE NOTES
PREDICTIVE OF PATHOLOGY
VS NORMAL:
ALT > 2 x NormalAST: ALT >1
Age > 50
Low Platelet Count
OTHER GROUPS WITH HIGH RISK
PATHOLOGY:
Raised Conjugated Bili with: ALTALK P
Consider: BX; MRCP; ERCP
Any abnormality of ALK P in addition to
abnormality ALT/AST
Consider BXPREDICTORS OF NASH AND FIBROSIS IN
PRESENCE OF NASH
ALT > 2 x Normal
AST > ALT
Moderate Central Obesity
BM1 > 28
NIDDM/Impaired GTT
BP
TGs.
SUGGESTED ROUTINE SEROLOGICAL INVESTIGATIONS:
Alpha 1 AT; HAV; HBV; HCV; AIP and Igs; Fe Studies and HFE
genotype; Caeruloplasmin; USS Fatty Change or Normal echo
only; Bilirubin and haemolysis studies if appropriate
- ANY ABNORMALITIES IN THESE PARAMETERS, RE-EVALUATE POTENTIAL
DIAGNOSIS AND CONSIDER BIOPSY
N.B. THESE NOTES/ALGORITHMS ARE FOR GUIDANCE ONLY. THIS IS A
MOVING FIELD AND DESPITE IMPROVEMENTS IN
SEROLOGICAL AND RADIOLOGICAL TECHNIQUES, THERE REMAIN SMALL
NUMBERS OF PATIENTS WHO HAVE SIGNIFICANT LIVER
DISEASE WITH ONLY MILDLY ABNORMAL LFTs. THE ALGORITHM IS NO
SUBSTITUTE FOR CAREFUL AND REPEATED CLINICAL
EVALUATION AND CLINICAL VIGILANCE