Embed Size (px)
Citation preview

DEPARTMENT Case Study—Acute and Specialty Care
Aborted Sudden CardiacDeath in a 14-Year-OldAthlete: The AnomalousCoronary Artery
Megan Trahan, MS, CPNP-AC, & Shari Simone, DNP, CPNP-ACSection EditorsKarin Reuter-Rice, PhD, CPNP-AC, FCCMCorresponding EditorDuke UniversityDurham, North Carolina
Terea Giannetta, DNP, RN, CPNPCalifornia State UniversityChildren’s Hospital Central CaliforniaFresno, California
Maureen A. Madden, MSN, RN, CPNP-AC, CCRN,FCCMRutgers Robert Wood Johnson Medical SchoolNew Brunswick, New JerseyBristol Myers Squibb Children’s HospitalNew Brunswick, New Jersey
Megan Trahan, Pediatric Critical Care Nurse Practitioner,
Department of Pediatrics, University of Maryland Medical Center,
Baltimore, MD.
Shari Simone, Senior NPClinical ProgramManager,Women’s andChildren’s Services, University of Maryland Medical Center,
Baltimore, MD.
Conflicts of interest: None to report.
Correspondence: Megan Trahan, MS, CPNP-AC, Department of
Pediatrics, University of Maryland Medical Center, 110 South
Paca St, 8th Floor, Baltimore, MD 21201; e-mail: [email protected].
J Pediatr Health Care. (2014) -, ---.
0891-5245/$36.00
Copyright Q 2014 by the National Association of Pediatric
Nurse Practitioners. Published by Elsevier Inc. All rights
reserved.
http://dx.doi.org/10.1016/j.pedhc.2014.02.001
www.jpedhc.org
KEY WORDSSudden cardiac death, anomalous coronary artery, athlete
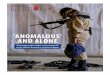
A 14-year old female athlete with no significant med-ical history was admitted to the pediatric intensive careunit (PICU) after sudden cardiac arrest while playingfield hockey. On the day of presentation, she experi-enced chest pain during a field hockey game andbecame unresponsive. Cardiopulmonary resuscitation(CPR) was performed by a bystander, and emergencymedical services was called. Upon evaluation by para-medics, the initial cardiac rhythmwas interpreted as tor-sades de pointes (Figure 1), and she successfullyconverted to normal sinus rhythm with defibrillationand administrationof intravenous lidocaine.Thepatientwas transported to a local emergency department,where she was intubated for respiratory distress andtransferred to the PICU. According to her family, in thepast few months the patient had reported chest painwith shortness of breath upon exertion, but it resolvedwith rest. Results of her last sports physicalwerenormal.
MEDICAL HISTORYThe patient was previously healthy. Her family historywas noncontributory; there were no unexplaineddeaths in the family or a history of collagen vasculardisorders or asthma. The patient was not taking anymedications, and the family denied a history of drug,alcohol, or substance abuse.
INITIAL PHYSICAL EXAMINATION ANDLABORATORY FINDINGSUponpresentation to the PICU, the following vital signswere obtained: temperature, 36.1�C; pulse, 100 beatsper minute; blood pressure, 130/80 mmHg; respiratory
-/- 2014 1
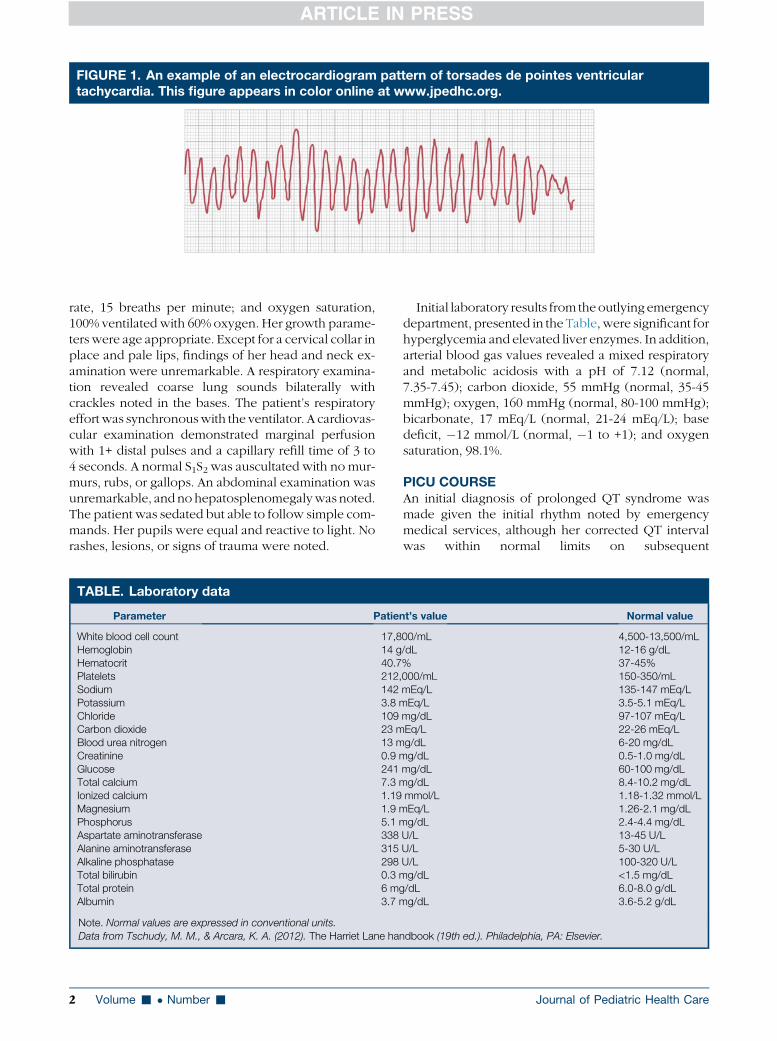
FIGURE 1. An example of an electrocardiogram pattern of torsades de pointes ventriculartachycardia. This figure appears in color online at www.jpedhc.org.
rate, 15 breaths per minute; and oxygen saturation,100% ventilated with 60% oxygen. Her growth parame-ters were age appropriate. Except for a cervical collar inplace and pale lips, findings of her head and neck ex-amination were unremarkable. A respiratory examina-tion revealed coarse lung sounds bilaterally withcrackles noted in the bases. The patient’s respiratoryeffortwas synchronouswith the ventilator. A cardiovas-cular examination demonstrated marginal perfusionwith 1+ distal pulses and a capillary refill time of 3 to4 seconds. A normal S1S2 was auscultated with no mur-murs, rubs, or gallops. An abdominal examination wasunremarkable, andno hepatosplenomegalywas noted.The patient was sedated but able to follow simple com-mands. Her pupils were equal and reactive to light. Norashes, lesions, or signs of trauma were noted.
TABLE. Laboratory data
Parameter Patie
White blood cell count 17,8Hemoglobin 14 gHematocrit 40.7Platelets 212,Sodium 142Potassium 3.8 mChloride 109Carbon dioxide 23 mBlood urea nitrogen 13 mCreatinine 0.9 mGlucose 241Total calcium 7.3 mIonized calcium 1.19Magnesium 1.9 mPhosphorus 5.1 mAspartate aminotransferase 338Alanine aminotransferase 315Alkaline phosphatase 298Total bilirubin 0.3 mTotal protein 6 mgAlbumin 3.7 m
Note. Normal values are expressed in conventional units.
Data from Tschudy, M. M., & Arcara, K. A. (2012). The Harriet Lane ha
2 Volume - � Number -
Initial laboratory results from theoutlying emergencydepartment, presented in the Table, were significant forhyperglycemia and elevated liver enzymes. In addition,arterial blood gas values revealed a mixed respiratoryand metabolic acidosis with a pH of 7.12 (normal,7.35-7.45); carbon dioxide, 55 mmHg (normal, 35-45mmHg); oxygen, 160 mmHg (normal, 80-100 mmHg);bicarbonate, 17 mEq/L (normal, 21-24 mEq/L); basedeficit, �12 mmol/L (normal, �1 to +1); and oxygensaturation, 98.1%.
PICU COURSEAn initial diagnosis of prolonged QT syndrome wasmade given the initial rhythm noted by emergencymedical services, although her corrected QT intervalwas within normal limits on subsequent
nt’s value Normal value
00/mL 4,500-13,500/mL/dL 12-16 g/dL% 37-45%000/mL 150-350/mLmEq/L 135-147 mEq/LEq/L 3.5-5.1 mEq/L
mg/dL 97-107 mEq/LEq/L 22-26 mEq/Lg/dL 6-20 mg/dLg/dL 0.5-1.0 mg/dL
mg/dL 60-100 mg/dLg/dL 8.4-10.2 mg/dLmmol/L 1.18-1.32 mmol/LEq/L 1.26-2.1 mg/dLg/dL 2.4-4.4 mg/dL
U/L 13-45 U/LU/L 5-30 U/LU/L 100-320 U/Lg/dL <1.5 mg/dL/dL 6.0-8.0 g/dLg/dL 3.6-5.2 g/dL
ndbook (19th ed.). Philadelphia, PA: Elsevier.
Journal of Pediatric Health Care

electrocardiograms (ECGs). The patient was scheduledto have surgery for an implantable cardioverter/defi-brillator (AICD). Continuing evaluation of the arrestincluded an echocardiogram, a cardiac magnetic reso-nance imaging (MRI) scan, and a gated cardiaccomputed tomography (CT) scan, although none wasdiagnostic of the origin of the coronary arteries as aresult of pulmonary hemorrhage from CPR.
The patient was extubated on hospital day three, andthe echocardiogram and gated cardiac CT scan wererepeated the day before the scheduled AICD surgery.On both repeat diagnostic tests, findings included an
www.jpedhc.org
anomalous left coronary artery arising from the rightcoronary sinus (Figure 2) with a short intramuralcourse, in which the coronary artery travels within theaortic wall and the ostium (orifice) has a slitlike appear-ance rather than the normal round appearance. TheAICD placement was cancelled, and the patient wastaken to the operating room for unroofing of the leftcoronary artery with reimplantation of the ostium intothe left coronary sinus (Figure 3). The patient had nomajor postoperative complications and is awaiting herscheduled 3-month follow up with a stress test, echo-cardiogram, and coronary CT scan.
CASE STUDY QUESTIONS
1. What is the differential diagnosis of sudden cardiac arrest in the healthy adolescent athlete?2. What is the pathophysiology of an anomalous coronary artery arising from the opposite sinus of Valsalva?3. What is the appropriate diagnostic workup for a suspected anomalous coronary artery?4. What is the current management strategy and expected outcomes for patients with an anomalous coronary
artery?5. What are some primary and secondary strategies for prevention of sudden cardiac death from anomalous
coronary arteries and other causes?
CASE STUDY ANSWERS
1. What is the differential diagnosis of sudden car-diac arrest in the healthy adolescent athlete?
The overwhelming majority of fatalities from suddencardiac arrest in a healthy athlete occur as a result of car-diovascular causes, mainly structural defects (Maron,Doerer, Haas, Tierney, &Mueller, 2009). The prevailingcause of sudden cardiac death in young athletes is hy-pertrophic cardiomyopathy and ‘‘possible hypertro-phic cardiomyopathy,’’ in which the heart has anoticeable increase inmasswithout the clinical featuresof hypertrophic cardiomyopathy. Other cardiovascularcauses include myocarditis, aortic aneurysms, arrhyth-mogenic right ventricle, Wolf-Parkinson-White disor-der, and long QT syndrome (Angelini, 2007; Berger,Kugler, Thomas & Friedberg, 2004).
Among noncardiovascular causes of sudden cardiacdeath, blunt chest trauma precipitating commotio cordisis the most common phenomenon. This phenomenonoccurs when a low-impact blow to the chest precipitatesa life-threatening dysrhythmia—usually ventricularfibrillation. Commotio cordis is most commonly seenin the sports of baseball, softball, hockey, and lacrosse(Maron, Gohman, Kyle, Estes, & Link, 2002).
2. What is the pathophysiology of an anomalouscoronary arising from the opposite sinus of Val-salva?
The second most common cause of sudden cardiacarrest after hypertrophic cardiomyopathy is aberrantcoronary arteries, with the anomalous left coronary
artery arising from the right sinus of Valsalva as theprimary lethal defect (Maron, 2003). Anomalous coro-nary artery from the opposite facing sinus of Valsalva(ACAOS) is a congenital heart defect in which a coro-nary artery arises from the opposite sinus and has ananomalous course (Angelini, Villason, Chan, & Diez,1999). The two most common forms of ACAOS areanomalous left coronary artery arising from the rightcoronary sinus and anomalous right coronary arteryarising from the left coronary sinus. Anomalous leftcoronary arteries are more commonly known to causesudden cardiac death than their counterpart (Eckart,Jones, Shry, Garrett, & Scoville, 2006). Of those, bothright and left, that cause sudden cardiac death, onlyapproximately 37% to 52% of the patients were symp-tomatic in the months prior to their death (Basso,Maron, Corrado, & Thiene, 2000; Mainwaring et al.,2011). Symptoms of anomalous coronary arteries area result of cardiac ischemia and include chest painand syncope (Mainwaring et al., 2011).Some controversy exists with regard to the cause of
ischemic symptoms in patients with anomalous coro-nary arteries. Initially, the common thought was thatboth the pulmonary artery and the aorta exerted pres-sure on the coronary artery in a hyperdynamic state(i.e., with exercise), causing poor perfusion to thedistal portion of the vessel. This idea has lost favor,because the pulmonary artery does not create enoughpressure, even during exercise, to create such an ef-fect. Other theories include a narrowed ostium, anacute angulation of the artery at the point of entry at
-/- 2014 3

FIGURE 2. Normal and anomalous left coronary artery from the right coronary cusp with intramuralcourse. L = left coronary cusp; P = posterior non-coronary cusp; PA = pulmonary artery; R = rightcoronary cusp. This figure appears in color online at www.jpedhc.org.
the aorta, or coronary spasm from endothelial damage(Kaushal et al., 2011). Current opinion purports thatthe most likely cause of ischemia and related symp-
FIGURE 3. Unroofing and reimplantation of the left ccoronary artery orifice and the anomalous left coronand an intramural segment of the left coronary.B, Thto create a neo-orifice in the left sinus. C, The left cposition. (Reprinted from Pediatric Clinics of NorthLitwin, S.B., Surgical therapy for sudden cardiac depermission from Elsevier.) This figure appears in co
4 Volume - � Number -
toms is the length of the anomalous artery that runstangential to and shares a commonwall with the aorta.The pressure of the aorta increases during exercise,
oronary artery. A, The normally positioned rightary artery orifice both arising from the right sinuse intramural segment of the coronary is unroofedoronary artery is reimplanted into a normalAmerica, 51, Jaquiss, R.D.B., Tweddell, J.S., &ath in children, 1394, Copyright (2004) withlor online at www.jpedhc.org.
Journal of Pediatric Health Care

Whereas thediagnosis ofACAOS has beenassociated withadverse outcomessuch as suddencardiac death, theprimary surgery torepair this defecthas very fewassociatedcomplications.
which compresses the coronary artery and limits coro-nary blood flow.
3. What is the appropriate diagnostic workup for asuspected anomalous coronary artery?
An anomalous coronary artery from the opposite si-nus of Valsalva can result in a diagnostic challenge, asevidenced by this case study. A simple ECG and stresstest are not sufficient and have been normal prior tosudden cardiac arrest in patients with ACAOS (Eckartet al., 2006). Current practice guidelines, includingthose from the American Heart Association (AHA;Bluemke et al., 2008), call for specific evaluation ofanomalous coronary artery with any incidence of sud-den cardiac death, life-threatening dysrhythmias, andischemic symptoms in the pediatric and young adultpopulation.
To date, several algorithms have been suggested forthe evaluation of anomalous coronary arteries,although none has been included in existing practiceguidelines. Angelini (2007) suggested that the evalua-tion should include an ECG, Holter monitor, and echo-cardiogram with Doppler. If the echocardiogramidentifies two normal coronary ostia, no further testingis required. If, however, the echocardiogram cannotdecipher two normal ostia, an MRI or CT scan is indi-cated. A diagnosed anomalous coronary artery also re-quires a baseline stress test.
Current opinions differ as to the optimal modality fordiagnosis of ACAOS if the echocardiogram cannotclearly delineate coronary artery origins. Although cor-onary angiographywas considered the gold standard inthe past, a gated cardiac CT scan has been shown toidentify coronary anatomy when angiography yieldedequivocal results (Datta et al., 2005). A cardiac CTscan, although efficient, requires use of intravenouscontrast material and radiation, although current tech-niques have considerably limited the radiation dose.For this reason, some authors strongly recommend cor-onary MRI/magnetic resonance angiography (MRA;Bluemke et al., 2008). However, coronaryMRA requiresa relatively stable patient and is liable to a certainamount of artifact (Arrigan, Killeen, Dodd, &Torreggiani, 2011). At this point, clinical judgment andpatient condition dictate which modality must be used.
4. What is the current management strategy and ex-pected outcomes for patients with an anomalouscoronary artery?
Several management options exist for the treatmentof ACAOS. Both nonsurgical and surgical options maybe considered, depending on which coronary arteryis anomalous, if there is an intramural course, and pre-senting symptoms (Mainwaring et al., 2011). Althoughseveral surgical options are available for a patientwith ACAOS, nonoperative management is now an op-
www.jpedhc.org
tion for patients with an anomalous right coronaryartery if certain criteria are met. A practice guidelinefrom the AHA states that anomalous left coronaryarteries must be operated on because of the risk of sud-den death, whereas with right coronary arteries, sur-gery is indicated if there is an intramural course, if theartery courses between the aorta and the pulmonary ar-tery, or if the patient has ischemic symptoms (Bluemkeet al., 2008). Practice guidelines from the American Col-lege of Cardiology also recommend that all patientswith unrepaired anomalous coronary arteries shouldbe totally restricted from participating in competitivesports (Graham et al., 2005).Many options are available to the pediatric cardio-
thoracic surgeon for operative repair of ACAOS;these options include unroofing of the intramuralsegment, in which the shared common wall betweenthe ACAOS and aorta is excised, reimplantation ofthe anomalous coronary artery, and coronary arterybypass grafting with use of the saphenous or internalmammary artery (Figure 3). Although an explanationof surgical options is beyond the scope of this paper,it should be noted that the two techniques mostfrequently utilized include unroofing and reimplan-tation. Individual anatomy plays a large role in theselection of the preferred surgical correction. Bypassgrafting has been deemed undesirable because ofgraft atrophy from competitive flow (Warnes et al.,2008).Whereas thediagnosis of ACAOShas been associated
with adverse outcomes such as sudden cardiac death,the primary surgery to repair this defect has very fewassociated complications. Authors of all but one study
found no complica-tions/minimal compli-cations or residualcoronary ischemia inthe corrected anoma-lous coronary arteryby unroofing of theintramural segment(Frommelt, Frommelt,Tweddell, & Jaquiss,2003; Romp et al.,2003). Authors of onestudy found noresidual symptoms,and 85% of patientswere unrestricted inactivities, with a 63%participation rate in sports at 5-year follow-up (Mainwaring et al., 2011).Authors of only one study found evidence of ischemiain 9 of 24 patients postoperatively, utilizing three stresstest modalities to evaluate for ischemia (Brothers et al.,2007). All of these patients were asymptomatic.Current practice guidelines for adults recommend a-/- 2014 5

3-month waiting period after a full surgical repairbefore return to sports if the patient is asymptomaticand has no evidence of ischemia (Warnes et al.,2008). To date, no studies have been performed toexamine the outcomes of a conservative approach toasymptomatic anomalous right coronary artery withno intramural course.
5. What are some primary and secondary strategiesfor prevention of sudden cardiac death fromanomalous coronary arteries and other causes?
Prevention of sudden cardiac death is at the crux of adebate involving appropriate athlete screening in theUnited States and internationally. The American Acad-emy of Pediatrics (AAP) released a policy statement in2012 regarding sudden cardiac arrest. Primary preven-tion of sudden cardiac arrest includes appropriate diag-nosis and treatment of the common causes responsiblefor the arrest. Primary prevention includes prepartici-pation sports physicals by the athlete’s primary carephysician with use of a formal screening tool inconjunction with a thorough cardiovascular examina-tion. The utility of a screening ECG in the preventionof sudden cardiac arrest is addressed in the policy state-ment. Although screening ECGs are endorsed by theEuropean Society of Cardiology and refuted by theAHA, the AAP (2012) does not take a stance, statingonly that the issue requires ‘‘more data and debate.’’
Secondary prevention of sudden cardiac arrest in-cludes early CPR combined with early defibrillation us-ing an automated external defibrillator. The AHA andthe AAP both advocate for emergency response pre-paredness and automated external defibrillator pro-grams in schools and sports facilities.
Anomalous coronary artery from the oppositesinus of Valsalva is a rare but serious congenital heartdefect. Presentation can be dramatic, frequently withsudden cardiac death, and diagnosis continues to bea challenge for practitioners, as evidenced by thecase presentation. Appropriate nonsurgical and surgi-cal management lead to a favorable prognosis withfew complications.
REFERENCESAmerican Academy of Pediatrics, Section on Cardiology and Cardiac
Surgery. (2012). Pediatric sudden cardiac arrest. Pediatrics,129, e1094.
Angelini, P. (2007). Coronary artery anomalies: An entity in search ofan identity. Circulation, 115, 1296-1305.
Angelini, P., Villason, S., Chan, A., & Diez, J. (1999). Normal and
anomalous coronary arteries in humans. Philadelphia, PA: Lip-pincott Williams & Wilkins.
Arrigan, M., Killeen, R., Dodd, J., & Torreggiani, W. (2011). Imagingspectrum of sudden athlete cardiac death. Clinical Radiology,66, 203-223.
6 Volume - � Number -
Basso, C.,Maron, B., Corrado, D., & Thiene, G. (2000). Clinical profileof congenital coronary artery anomalies with origin from thewrong aortic sinus leading to sudden death in young competi-tive athletes. Journal of the American College of Cardiology,
36(6), 1493-1501.Berger, S., Kugler, J. D., Thomas, J. A., & Friedberg, D. Z. (2004).
Sudden cardiac death in children and adolescents: Introduc-tion and overview. Pediatric Clinics of North America, 51(5),1201-1209.
Bluemke, D., Achenbach, S., Budoff, M., Gerber, T., Gersh, B., Hillis,D., . Woodard, P. K. (2008). Noninvasive coronary artery im-aging: Magnetic resonance angiography and multidetectorcomputed tomography angiography: A scientific statementfrom the American Heart Association Committee on Cardiovas-cular Imaging and Intervention of the Council on CardiovascularRadiology and Intervention, and the Councils on Clinical Cardi-ology and Cardiovascular Disease in the Young. Circulation,118(5), 586-606.
Brothers, J., McBride, M., Seliem, M., Marino, B., Tomlinson, R.,Pampaloni, M. H., . Paridon, S. M. (2007). Evaluation ofmyocardial ischemia after surgical repair of anomalous aorticorigin of a coronary artery in a series of pediatric patients. Jour-nal of the American College of Cardiology, 50, 2078-2082.
Datta, J., White, C., Gilkeson, R., Meyer, C., Kansal, S., Jani, M., .Read, K. (2005). Anomalous coronary arteries in adults: Depic-tion at multi-detector row CT angiography. Radiology, 235,812-818.
Eckart, R., Jones, S., Shry, E., Garrett, P., & Scoville, S. (2006). Sud-den death associated with anomalous coronary origin andobstructive coronary disease in the young. Cardiology in Re-
view, 14, 161-163.Frommelt, P., Frommelt, M., Tweddell, J., & Jaquiss, R. (2003). Pro-
spective echocardiographic diagnosis and surgical repair ofanomalous origin of a coronary artery from the opposite sinuswith an interarterial course. Journal of the American College of
Cardiology, 42, 148-154.Graham, T., Driscoll, D., Gersony, W., Newberger, J., Rocchini, A., &
Towbin, J. (2005). Task force 2: Congenital heart disease. Jour-nal of the American College of Cardiology, 45(8), 1326-1333.
Kaushal, S., Backer, C., Popescu, A.,Walker, B., Russell, H., Koenig,P., . Mavroudis, C. (2011). Intramural coronary length corre-lates with symptoms in patients with anomalous aortic originof the coronary artery.Annals of Thoracic Surgery, 92, 986-992.
Mainwaring, R., Reddy, M., Reinhartz, O., Petrossian, E., MacDon-ald, M., Nasirov, T., . Hanley, F. L. (2011). Anomalous aorticorigin of a coronary artery: Medium-term results after surgicalrepair in 50 patients. Annals of Thoracic Surgery, 92, 691-697.
Maron, B. (2003). Sudden death in young athletes. New England
Journal of Medicine, 349, 1064-1075.Maron, B., Gohman, T., Kyle, S., Estes, N., & Link, M. (2002). Clinical
profile and spectrum of commotio cordis. Journal of the Amer-
ican Medical Association, 287, 1142-1146.Maron, B., Doerer, J., Haas, T., Tierney, D., &Mueller, F. (2009). Sud-
den deaths in young competitive athletes: Analysis of 1866deaths in the United States, 1980-2006. Circulation, 119,1085-1092.
Romp, R., Herlong, J. R., Landolfo, C., Sanders, S., Miller, C., .Jaggers, J. (2003). Outcome of unroofing procedure for repairof anomalous aortic origin of left or right coronary artery. Annalsof Thoracic Surgery, 76, 589-596.
Warnes, C., Williams, R., Bashore, T., Child, J., Connolly, H., Dear-ani, J. A., . Yancy, C. W. (2008). ACC/AHA 2008 Guidelinesfor themanagement of adults with congenital heart disease.Cir-culation, 118, e714-e833.
Journal of Pediatric Health Care