Embed Size (px)
Citation preview

About Stoma Reversal
Freephone helpline: 0800 328 4257

About Stoma Reversal
Perhaps you are trying to decide whether to have a reversal…
Stomas are formed for a variety of medical reasons. Different people will have had different types of operations – how much and which part of the bowel has been removed will vary, some people have a loop stoma, others an end stoma.
Although we can’t provide the answer for individual cases…
We can give you information…
Oliver Shihab, Research Fellow at the Pelican Cancer Foundation, describes the different typesof stoma and the surgical techniques involved in their reversal from a surgeon’s point of view.
Shelley Biddles and Diana Wilson, who have many years experience as colorectal and stoma carenurses, consider the advantages and possible problems associated with a reversal and suggest asimple checklist to ensure you

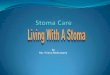
oesophagus
stomach
transverse colon
descending colon
sigmoid colon
rectumanus
ascending colon
small intestine or ileum
liver
large intestinegall bladder
The Digestion System
caecum

About Stoma Reversal
What you need to know about Stoma Reversal…
The main reasons that temporary stomas are formed are for cancer ofthe bowel, inflammatory bowel disease, diverticulitis (a condition wherepockets in the bowel wall become inflamed and infected) and injuries tothe bowel that mean it has to be rested, so that it may heal.
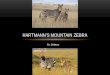
Stomas formed from the colon (large bowel) are called colostomies. Those formedfrom the ileum (small bowel) are called ileostomies. In each case they can be eithera loop or an end stoma. Please see diagrams opposite.

Illustrations reproduced courtesy of Coloplast
B
A
C
D
Loop Colostomy To form a loop colostomy a loop of large bowel is brought out usually inthe upper abdomen, and then opened andstitched to the skin. This gives two openings. The upper, or proximal, limb links up with thestomach and intestines higher up and producesstool, the other, distal, limb leads to the anusand only produces small amounts of mucus.
B
End Colostomy This is usually sited in the left side of the abdomen. With this type ofcolostomy the colon (large bowel) is severed andthe functioning end is brought to the skin. The distal end, which leads to the anus, is sealed and left inside the abdomen.
A
Loop Ileostomy A loop ileostomy is formedfrom a loop of ileum (small bowel). Today theyare more commonly used than the loopcolostomy, if a temporary diversion of bowelcontents is required, when a join in the bowel(e.g. after cancer surgery for the large bowel)needs to be rested and given time to heal.
C
End Ileostomy The end ileostomyis usually sited on the right side of the abdomen.It is more commonly reserved for those who havehad all or most of their colon removed, usuallydue to inflammatory bowel disease or multiplepolyps of the large bowel.
D

About Stoma Reversal
Loop or end stoma?Usually the temporary form of stoma is the loop ileostomy (or less frequently the transverse loopcolostomy). This is created when the bowel is obstructed, and needs to be relieved in anemergency or where another section further down the bowel has had to be removed.
Occasionally, however, there are situations in which an end colostomy will be created on atemporary basis, usually done as part of what is known as “Hartmann’s procedure”. In thisoperation an end colostomy is formed, and the remaining part of the bowel below this securelysealed and left in the abdomen. This is usually carried out for emergencies, such as a blockedbowel where there may have been perforation of the bowel or for complications of diverticulardisease, where there has been infection in the abdomen and it is not safe to join the bowel upimmediately.
Can it be joined up?Ideally as many people as possible will be joined up, but there may be several reasons why thesurgeon looking after you is reluctant to do so.
Firstly, to be operated on, no matter how minor the procedure, is never without risk so thedoctors must be happy that you are fit enough for another operation.
Secondly, the bowel and the anal sphincters that control the flow from the bowels need to beworking, so that incontinence will not develop as a result. To help in this assessment the surgeonis likely to perform a rectal examination, and possibly arrange some further tests of anal tone ifthere is any doubt.
Overall around 8% of those who have had a planned temporary stoma for cancer of the rectumend up keeping it as a permanent stoma.
How soon can it be joined up?It is understandable that people want their normal bowel function restored as quickly as possible,and there have been several studies that have looked at the best time to do so. After anyoperation on the abdomen, there is an inflammatory response to this insult, which results in theformation of adhesions. These adhesions are band-like structures, which are essentially scar tissue.If they are very dense they can cause considerable problems for the surgeon, as they can makesome parts of the bowel very hard to get to and operate on safely. These will be at their worstfor the surgeon in the weeks following an operation, so it is advised that surgery be postponeduntil at least nine weeks after the previous operation. This time allows the adhesions to settle,the patient to recover from the previous operation and any swelling within the abdomen orstoma site to fully resolve.

Joining it all upClosure of a loop colostomy or ileostomy is a relatively simple procedure, and in over 95% ofcases does not require any further incisions to be made in the abdomen. A small rim of skin iscut around the stoma (about 2mm), and the incision is deepened until the abdominal cavity isreached. Once this has happened the bowel and abdominal cavity are checked, to ensure there isnothing still attached to the bowel, and the bowel is then closed - either stitched by hand orstapled together.
Reversal of an end colostomy or ileostomy is more difficult, however, as one end of the bowelthat is to be rejoined is within the abdomen. This usually means that the surgeon will have toopen the abdomen via the old scar to be able to safely access the bowel. As a result of theincreased surgery, compared to the closure of a loop stoma, there will be a longer stay in hospitaland a greater recovery time before normal activities can be resumed.
There will be some centres that will offer to attempt to reverse an end colostomy laparoscopically(by keyhole surgery), but this is dependent on the training of the surgeon. Even if this isattempted it may be necessary to convert to the open operation, as the aforementionedadhesions can cause severe problems laparoscopically. That said, if this type of surgery is carriedout then it is likely there will be less post-operative pain and a shorter stay in hospital.
How long in hospital?This will depend on the type of operation: for the closure of a loop colostomy it will be aroundthree to five days and five to ten days for closure of an end colostomy. The surgeons lookingafter you will want to be sure that you can cope with your bowel movements once again, as it isfairly common to pass looser and more frequent stools than you may have been used topreviously. They will also want to ensure that the area where the anastomosis (join) was formedhas not narrowed (strictured) as a result of scarring, as this can lead to partial or full blockage ofthe bowel. If this is the case then it may be necessary to have the area stretched, which isnormally carried out using a colonoscope.
What about afterwards?When you get home, your return to normal activities will be determined by your physicalcondition before the operation and, again, on the type of operation that you have had. It couldbe at least ten weeks before you are able to lift heavy weights or fully use your abdominalmuscles. Driving will be allowed only when you can perform an emergency stop without anypain, or fear of pain.
Your diet may well require readjustment initially, as the time after the reversal can be similar tothe time the stoma was originally formed, with loose bowels and sudden urges to go. It is alsopossible that some people will have developed inflammation of the lower part of colon, whichcan occur if it is not used for some time. This can lead to loose stools, with some bleeding andmucus, but this usually settles down without need for treatment.

About Stoma Reversal
What can go wrong?In any surgery there are risks, but fortunately life-threatening complications are rare. As with anysurgery there will be those general complications that can result from undergoing any surgicalprocedure, which your surgeon will discuss with you before your operation.There are also those that are specific to the reversal of the stoma:
• Ileus - temporary paralysis of the bowel: Sometimes the bowel is slow to start working aftersurgery, particularly if it has been handled by the surgeon. Disturbances in the salt balance inyour body and some pain medications can also increase the risk of this occurring. If this happensthe bowel will need to be rested, which involves stopping food, and taking minimal water. Fluidgiven via a vein (a drip) is used to replace fluids, and you may need a tube down your nose toyour stomach (nasogastric tube) which decompresses the bowel, and helps it to start up again.
• Bowel obstruction: If there is a physical blockage or problems with adhesions causing ablockage another operation may be required. Fortunately this type of physical blockage is rareimmediately after an operation.
• Anastomotic leak - breakdown of the join in your bowel: If this is suspected you will bestarted on antibiotics, and it is likely that another operation will be required. However, this cantake a controlled form, whereby an abscess forms. If this is the case there may not be the needfor an operation, as it may be possible to control it with antibiotics and drainage under X-rayguidance.
• Urinary and sexual function may be affected temporarily but the risk of this being permanentis higher in surgery to reconnect an end colostomy, as the nerves controlling these functions liein this region.
Hopefully this has given a clearer picture of the types of temporary stoma used, and theprocesses involved in their closure. Before the operation the surgeon looking after you has a dutyto inform you about the potential risks involved. This is not designed to create doubt and fear,but rather to allow you to make a fully informed decision about your treatment. However, itshould not be forgotten that over 6,000 stoma reversals are carried out in England every year,and that the vast majority are successful.
Oliver Shihab MBBS MRCS (Eng)Research RegistrarThe Pelican Cancer Foundation

Readers’ Writes on Stoma Reversal…
Here are some extracts from letters published in the original article on Stoma Reversal,first featured in Issue 7 of Tidings Magazine 2007 (for more information about Tidings Magazine and the Colostomy Association please visit our website:www.colostomyassociation.org.uk).
Some letters mention the possible problems which our colorectal surgeon andspecialist nurses refer to in their articles. However, more than half told of successfulreversals. We would like to thank everyone who wrote to tell us of their experience of stoma reversal.
I am happy to be ableto tell you that myhusband, Antonio,
recently had a completelysuccessful reversal operation.Also we are hoping to moveover to Spain within the nextsix to eight weeks so we willnot require any furthermailings of Tidings.
Antonio was given a stoma inSeptember 2005. He went intohospital for repair of an analfissure and a colonoscopy. Afairly large polyp was found onthe bowel and removed.Unfortunately two days laterAntonio was re-admitted tohospital suffering fromperitonitis as his bowel hadbeen perforated when thepolyp was removed.
He was promised a reversal butbecause of his heart attack in1990 the surgeon was quitewary of performing such a bigoperation. However, after many
visits to the cardiologist andanaesthetist and various tests,it was decided he was fitenough for the operation andthis went ahead at the end ofNovember 2006. It took sixand a half hours as there weremany adhesions in theabdomen and the surgeondecided to give Antonio a loopileostomy to allow the colonto heal properly.
He recovered very well fromthis operation and theileostomy was closed on 16thMay, Antonio’s sixty-fifthbirthday!
Apart from suffering fromdiarrhoea for a couple of daysafter the loop stoma wasclosed, everything rapidlysettled down and he has nothad to take any medication.He is absolutely delighted withthe quality of his life. B.R.S. (Mrs)
I would personallyadvise against a
reversal operation.
I was diagnosed with bowelcancer in October 1996. I thenhad radiotherapy from 5th to9th December 1996. On the18th December, I had mybowel operation and mycolostomy was formed. I wascoping really well and feelingfine. Then on 15th May 1997,I had a reversal.That was when the troublestarted: my bottom was redraw and bleeding, I haddiarrhoea, then constipationand problems with sitting andwalking. No one seemed tounderstand. Then finally Iwent back into hospital tohave my colostomy reformedon the 15th May 1999. I wastold afterwards it was theradiotherapy that had damagedmy insides.

About Stoma Reversal
Since then, with help from mylocal stoma care nurses, I havenever looked back.Jenny
I was rushed intohospital in severe pain
on New Year’s Eve2002. They weren’t sure whatwas causing the pain, andoperated on New Year’s Day.Imagine my utter shock whenfour days later coming out ofintensive care I was told I hada colostomy. I found it veryhard to live with and wasoverjoyed when the surgeonsaid I could consider a reversalin six months time.
I was very afraid, as I had beenso ill with the first operation,but the thought of continuingas I was made me determinedto go ahead. When I saw thesurgeon regarding theoperation he explained thefailures that can occur and Iwas worried. My family didn’twant me to have the operationbut I was determined to gothrough with it whatever thecost. The operation was noteasy, but very successful andworth everything I wentthrough.
It is now five years since mytwo operations and I feelwonderful. I’m seventy-twobut feel more like thirty-two.You need to think carefullybefore you decide, but if youreally want a reversal my
advice is go ahead with it. Ithas certainly worked for meand, given the samecircumstances, I would do itover again. Believe me, it’sworth it. D.B. (Mrs)
I had a Hartmann'sprocedure done in
1997 after peritonitisfrom a ruptured bowel causedby diverticular disease. When Iawoke from anesthesia my firstquestion was: "Have I got abag?" My world appeared toend and I went back to sleep.However, with the kind andencouraging words from mystoma nurse I realized it wasn'tsuch a bad thing.
In fact I’ve opted to keep mystoma instead of having itreversed. My quality of life isso much better now thanpreviously when I frequentlyhad an urgent need to find atoilet. I wasn’t able to go tofunctions or travel withoutplanning the toilet stops. Infact now I can visit a toilet inmuch less time than someonewith natural functions, and,barring accidents, do so in MYtime, when it suits me.
I developed a large parastomalhernia and in June last yearhad surgery to repair it withmesh reinforcement. After along recovery period I am nowquite well and looking betterthan I have for years. So,
anyone having a colostomy, ifI can overcome the "horror" socan you. It really isn't so badafter all.Fiona
My husband’sproblems started
when he was sixty-seven with a little bleedingfrom his back passage. A smallpolyp was found in the wall ofthe bowel and it was decidedto operate before it grew anybigger. He had an anteriorresection and part of thesigmoid colon and rectum wasremoved and he was given anileostomy. They found somecancer had spread through thewall to the lymph nodes, DukeStage ‘C’, so he had a courseof chemotherapy. A CT scan inOctober 2005 showed thateverything was OK. We hadups and downs with theileostomy but on the wholebegan to manage quite well.My husband could still enjoyhis hobby of walking.
We tried to find out aboutreversals and went to thelibrary, even looked on theinternet - but nothing. InMarch 2006 he had asigmoidoscopy and everythingwas clear. So a date in Junewas arranged for the reversal –twenty-one months after theileostomy was formed. Afterthe reversal, my husbandsuffered from diarrhoea. Thenin September he needed an

emergency operation becauseof a blockage and a “transversecolostomy” was formed. Thistemporary loop colostomy hasbeen hard to deal with,because it is retracted and wehave to use paste to preventleakage.
The consultant does not knowwhy the reversal failed. Iwondered if it was the lengthof time before reversal but hesaid ‘no’. He offered to doanother reversal but myhusband doesn’t want to riskthe same thing happeningagain. He could have apermanent end colostomylower down but this is anothermajor op. The third option,which we have decided to goahead with, is to refashion thetransverse colostomy.
It has been a traumatic threeyears. We wish he had hisileostomy back but you can’tgo back in time. He wantedthe reversal to be back tonormal.R S. (Mrs)
In November 2005,without any symptoms
or warning, I becamevery seriously ill. Seven daysafter the initial pain, a CT scanshowed that a diverticularabscess had burst andperforated my bowel. I thenhad emergency life-savingsurgery which resulted inabout a foot of bowel being
removed and a Hartmann’sprocedure to form an endcolostomy. I remember saying:‘but I’m a swimmer!’ I wasassured that I would still beable to go swimming with acolostomy.
I was in hospital for nearly amonth, but I gradually made afull recovery and, yes, I did getback to swimming, also cyclingand walking. My consultantmentioned reversal when I sawher two months after mysurgery, but told me to thinkabout it and we would talkabout it again in six monthstime. I wrote to the ColostomyAssociation for informationand also read a lot of negativethings about it and heardstories from people whoregretted having the reversal.Someone did write a verypositive article about hisreversal in “Tidings”, so thathelped. I did feel reluctantabout going ahead with theoperation as I felt so well andwas coping very well with mystoma.
When I saw my consultant sixmonths later she spent a longtime talking it through withme and said that she felt sureall the negative things andproblems that were writtenabout would not apply in mycase. However, she did stressthat it was a major operationand told me all the things thatcould go wrong! Anyway, Idecided to go on the waiting
list which turned out to beseven months.I had my operation in Februarythis year. I am sixty-three yearsold and, as the consultant said,I was fit and well going intothis operation, so my recoverywould be much quicker thanmy previous emergencysurgery. The operation wasvery successful and I said‘Goodbye’ to my stoma afterhaving it for fifteen months. Iwas in hospital for eleven days.There were some days after theoperation when I didn’t feelwell and I felt a bit low, butonly a few.
I am really glad that I had thereversal operation and havemade a really good recovery.Everything is functioningnormally again. And, yes, I amback to swimming, cycling andwalking!J.W. (Mrs)

About Stoma Reversal
People with stomas can leadfull and active lives. However,for many, who have been toldthat their stoma is temporary,a stoma reversal cannot comequickly enough. Stoma closureis a very safe and successfulsurgical procedure for themajority of ostomates.Following a period ofrehabilitation, bowel actionreturns to normal or at leastan acceptable level offunction. However,unfortunately, for some thereality of stoma closure maynot be as problem-free as theywould have hoped.
In this article we intend todiscuss the issues which needto be taken into considerationand how they may affect post-operative recovery and bowelfunction, as well as passing onsome hints and tips that maybe useful following a reversal.We will focus on the two mostcommon types of stomareversal procedures i.e. loopstoma closure and reversal ofHartmann's procedure.
Undergoing anotheroperation! All stoma closure is performedas a planned operation andthis does minimise the risk ofpost-operative complications.The surgical team (includingthe anaesthetist) will assess allpossible risks before theoperation and put measures inplace to try and prevent anyproblems occurring.
Sometimes it can be quitenerve racking going for furthersurgery when the last occasionmay have been an emergencyor, for whatever reason, it maybe an unpleasant memory.
Loop stoma closureThis is considered a relativelystraightforward procedurecompared to the original stoma operationand therefore there is lesslikelihood of complicationsarising, although no surgery iswithout risks. It involvesfreeing up the stoma bycutting around where it joinsthe skin and rejoining the endsof the bowel, thus restoringbowel continuity. As this isperformed through the stomasite it does not usually requirethe abdomen to be re-opened.
Reversal ofHartmann'sprocedureThis is a major operation as itinvolves opening up theabdomen to reach the portionof bowel that was left inside.There are several aspects thatmust be considered:
• The surgeon will open thesame abdominal incision asbefore. The initial operationmay have been performed asan emergency and although,generally speaking, recoveryfrom any planned surgery isbetter nevertheless theconsequences of the procedurei.e. hospital stay and recoverywill be comparable with thatof the previous surgery.
• Undertaking surgery doesnot guarantee that the stomawill actually be reversed. If theremaining redundantcolon/rectum is too short tosuccessfully join the ends ofbowel together or if theviability of the redundantsection of bowel is suspect i.e.the blood supply is too poor toensure a healthy join, theattempt to reverse the stomawill be abandoned.
• It is possible that during thereversal operation a furtherstoma may need to be formed.If the remaining redundantbowel is very short or there areadhesions from previoussurgery making the re-joining

procedure difficult, it may benecessary to form anothertemporary loop stoma toprotect the new join. Thismeans another period of timeas an ostomate and then yetanother operation to completebowel continuity.
Recovery TimeInpatient hospital stay isgetting shorter and shorterwith enhanced recoveryprogrammes in place; stomareversals are even beingperformed as day-cases insome centres. However, formost it does mean a furtherstay in hospital. This can rangefrom one or two days for someprocedures to one or twoweeks, even when no post-operative complications haveoccurred.
A period of recovery is alsonecessary. This may vary froma couple of weeks with a loopstoma or laparoscopic(keyhole) reversal up to acouple of months after reversalwhere the abdominal muscleshave been cut again. Time offwork may be a concern forsome when contemplatingmore surgery.
Whilst hospital stay andrecovery are imprecise, themost variable aspect ofrehabilitation is the attainmentof acceptable bowel function.This may make getting back to“normality” unpredictable.
Function followingstoma closureIt will take time for bowelfunction to settle into somesort of pattern. This timeperiod will vary from person toperson as will the perceptionof what is a satisfactoryfunction. During the first fewweeks following stoma reversal,bowel function can be erratic.
The following are quitecommon at first: • Loose motions (which can
swing to constipation).
• Going to the toilet to passfaeces more frequently.
• Having some degree ofurgency when going to thetoilet.
• Difficulty determining windfrom motion.
• Sore skin around the backpassage(anus).
It is often difficult to predictexactly how problematic bowelfunction will be. It is notusually due to the type oftemporary stoma which wasformed but more likely due to:
1. The amount of colon and/orrectum removed.
2. Treatments and the healthof the remaining colonand/or rectum.
3. Other previous pelvic surgery
and/or any previous or co-existing pelvic disease.
4. The distance of the join inthe colon/rectum from theback passage.
5. Capability of anal sphincters.
6. Personal satisfaction.
Faeces enters the colon as aliquid and one of the mainfunctions of the colon is to re-absorb water back into thebody. When a significantsection of colon is removed,the natural consistency of thewaste matter will become moreliquid. This may result in morefrequent visits to the toilet andfor some may cause concernregarding control. Exerciseswhich build up and strengthenthe anal sphincter muscles mayprove helpful in preventingleakage of gas and stool fromthe back passage.
Treatments such aschemotherapy andradiotherapy to the pelvis candelay the return to acceptablebowel function. In some casesthe damage may makefunction more unpredictableand for some it may bepainful.
Previous pelvic disease orabdominal surgery may makestoma closure more difficultand may also affect long-termfunction.

About Stoma Reversal
The use of stapling guns forrejoining bowel has allowedthe surgeon to make a lowerjoin (anastomosis) in therectum reducing the necessityto remove the back passageand form a permanentcolostomy. However, this mayhave an impact on bowelfunction and control. Therectum acts as a reservoir or“holding area” for faeces andwhen a significant portion isremoved, coupled with a lowscar line close to the sphinctermuscles, the effect can bequite debilitating for some.This is commonly known asanterior resection syndromewhich is characterised by thefollowing symptoms:
• Increased frequency.
• Urgency and a feeling of theneed to defaecate.
• Fragmentation of the motion(a feeling of not havingcompleted passing faeces.)
• Inability to distinguish 'wind'from motion resulting insoiling or possibleincontinence.
This will settle down for mostbut can take quite asignificant time to do so.
Childbirth, age and trauma arejust some of the processes thatmay have a detrimental effecton sphincter control in general.If the initial surgery causes a
looser output or reduces the“holding” capacity, control ofbowel function can becomemore difficult. Pelvic floor andsphincter exercises to aidbowel control may help.
Advice following a reversalWhat is acceptable to one maybe intolerable to another.Some may expect bowelfunction to return exactly tohow this was prior to anydisease process and surgery.This will often be unrealisticand unachievable. Also, timeto heal must be taken intoconsideration.
MedicationAnti-diarrhoea medication,softeners, or bulking agentsmay be required to regulatebowel action and may help toimprove the consistency.
Dietary AdviceFollowing stoma closure it maytake time to get back to eatinga normal, healthy diet. Thedigestive system may be quiteupset and temperamental. Thiswill mean a “settling-in”period for both the stomachand the bowel. During thisperiod it is sensible to limitfoods which can irritate thegut for example:
• Acidic/citrus fruits e.g.
grapefruit, oranges,strawberries, grapes.
• Highly spiced foods e.g.curry, chilli con carne.
• Big fatty meals.
• Vegetables with a high“flatulence factor” i.e.cabbage, Brussel sprouts,onions.
• Large amounts of beer or lager.
Skin care When bowel movement isloose or if problems occur withsoiling in the area around theback passage, irritation orsoreness may occur. To preventskin excoriation, diligent skincare is essential. Washingthoroughly with warm waterand “patting” dry with a softcloth after each bowelmovement is necessary.Applying a protective creamwill help to minimise any skinproblems. However, if this isnot adequate contact yourstoma care nurse for specialistadvice.
Stoma Closure -Your choiceThere are an appreciablenumber of stomas where theintention was that they wouldbe temporary, where in fact areversal is not performed. This

may be due to the patient’spersonal decision or to advicegiven by the surgicalconsultant in charge.
You will hear stories frompatients who have hadproblems following a reversalor where stomas have had tobe reformed and there will bealways be those for whom theoutcome wasn't what theydesired. However, for themajority of people who havehad stoma reversal, this is avery worthwhile procedure,resulting in a very successfuloutcome. The surgical teamwill assess in depth yoursurgical complication risks, thepotential success of stomaclosure and the likelihood ofacceptable function beforeoffering you a reversal. Thesefacts must be outlined anddiscussed with you, prior tosurgery. This is called informedconsent.
Our article may have focusedsomewhat on the negativeside; however, our intention isto ensure that people areaware of all the implications of further surgery.
We would like all reversals tohave a successful outcome andhave therefore produced asimple checklist:
• Make sure you understandwhy your stoma was formedin the first place.
• Ask your consultant or nursespecialist to provide you withdetailed informationregarding the proposedsurgery and the realisticoutcome you can expect inrelation to hospital stay,length of recovery andexpected bowel function -both in the short-term andlong-term.
• Consider what your qualityof life is like with a stoma.
• Consider what your qualityof life would be like withouta stoma, taking into accountall the surgery and treatmentthat you have had.
• Speak to similar people whohave undergone theprocedure.
• Ask for a written summaryof your consultant’s plan.
We hope this helps to ensurethat you make the mostappropriate “informed”decision for yourself.
Article written for theColostomy Association by:-
Shelley Biddles RGN RMN Stoma Care 216 Education & Training Co-ordinatorNottingham Cancer Centre
Nottingham UniversityHospitals NHS Trust
Diana Wilson RGN RM Stoma Care 216Stoma Nurse SpecialistColoplast Ltd

2 London CourtEast StreetReading RG1 4QL
Tel: 0118 939 1537
Helpline: 0800 328 4257
E-mail:
Website:
www.colostomyassociation.org.uk
How to contact us...
We would like to take this opportunity to thank Oliver Shihab MBBS MRCS (Eng) ResearchRegistrar - The Pelican Foundation, Shelley Biddles RGN RMN Stoma Care 216, Education andTraining Co-ordinator, Nottingham Cancer Centre, Nottingham University Hospitals NHS Trustand Diana Wilson RGN RM Stoma Care 216 Stoma Nurse Specialist, Coloplast Ltd for their kind assistance in the production of this booklet.