Embed Size (px)
Citation preview

FAMILY MEDICINE CLERKSHIP HANDBOOKEffective 2018
Department of Family Medicine Undergraduate Medical Education University of Ottawa
Page 1
About the Authors:
Victoria Gerber, Miki Lackman and Tyler Letain, third year medical students (MD 2019) at the University of Ottawa updated the handbook for 2018-2019 academic year. The handbook was originally created in 2011 by Stephanie Ahken, a second year University of Ottawa medical student, as part of the Faculty of Medicine Undergraduate Summer Studentship program. The handbook has since served as a valuable resource for all clerkship students rotating through their core family medicine rotation!
We would also like to acknowledge previous medical students at the University of Ottawa for their contributions in updating this handbook. These include:
MD 2018: Brendan Sanders, Iuliia Povieriena, Lawrence Yau, Monica Gad, Nickan Motamedi, Omar Anjum, Sarah Buttle & Sean Patrick MD 2017: Katherine Li & Olivia Margie MD 2016: Sarina Scaffidi Argentina & Kimberly Reiter MD 2015: Kelly Frydrych MD 2014: Bonnie Tang
Please Note:We have made every effort to ensure that the information and references in this handbook are correct at the time of printing. However errors may be present and web based references may change. Please refer to the original references whenever possible in making decisions relating to patient care. For a comprehensive list of links to resources pertaining to all learning objectives, please visit the University of Ottawa, Department of Family Medicine Website (Undergraduate Medical Education).
This handbook is intended as a reference document to 3rd year medical students during their family medicine clerkship rotation. It outlines specific objectives and includes references to various resources such as best current practice guidelines as well as diagnostic and management algorithms on selected topics. Content of the handbook is based-on (but not exclusive to) the University of Ottawa Family Medicine clerkship learning objectives.
Page 2
Table of ContentsAbdominal Pain..........................................................................................................................6
Differential Diagnosis by Quadrant.......................................................................................6Red Flags................................................................................................................................6Irritable Bowel Syndrome......................................................................................................7
Alopecia...........................................................................................................................................8Asthma...........................................................................................................................................10
Diagnosis..............................................................................................................................10Triggers................................................................................................................................10Management.........................................................................................................................10Techniques...........................................................................................................................13Monitoring............................................................................................................................13
COPD.............................................................................................................................................14Targeted Screening...............................................................................................................14Assessment...........................................................................................................................14Management.........................................................................................................................15
Diabetes/Dysglycemia...................................................................................................................18Screening/Diagnosis.............................................................................................................18Diabetes Monitoring & Targets............................................................................................20
Gestational Diabetes......................................................................................................................22Screening and Diagnosis......................................................................................................22Management.........................................................................................................................23Referral.................................................................................................................................23Prognosis..............................................................................................................................23
Dizziness/Vertigo..........................................................................................................................24Approach to Dizziness.........................................................................................................24
Dyslipidemia..................................................................................................................................25Screening for Dyslipidemia..................................................................................................25Management of Dyslipidemia..............................................................................................25
Dyspepsia/GERD...........................................................................................................................26
Page 3
Gout...............................................................................................................................................30Headaches .....................................................................................................................................34
Primary Headaches..............................................................................................................34 Secondary Headaches...........................................................................................................35Red Flags..............................................................................................................................36
Hypertension .................................................................................................................................37Valid BP...............................................................................................................................37Treatment.............................................................................................................................40
Fibromyalgia..................................................................................................................................40Lower Back Pain............................................................................................................................41Acute Otitis Media.........................................................................................................................44Osteoarthritis .................................................................................................................................44Osteoporosis..................................................................................................................................46Pain................................................................................................................................................47
Neuropathic Pain..................................................................................................................47Nociceptive Pain..................................................................................................................47
Anxiety..........................................................................................................................................48Depression....................................................................................................................................50 Psychiatry......................................................................................................................................51Skin Conditions.............................................................................................................................52
Acne.....................................................................................................................................52Eczema (Atopic Dermatitis).................................................................................................52Actinic Keratosis (Solar Keratosis)......................................................................................54Basal Cell Cacinoma............................................................................................................54Squamous Cell Carcinoma...................................................................................................55
Red Eye..........................................................................................................................................55Red Flags for Urgent Ophthalmology Referral:...................................................................56
Problems in the Elderly.................................................................................................................58Elder Abuse...................................................................................................................................58Assessment & Management of Falls.............................................................................................59 Dementia.......................................................................................................................................62 Pseudodementia............................................................................................................................64
Page 4
Primary Care Pediatrics.................................................................................................................65Well Child Visits.......................................................................................................................65Infant Feeding and Nutrition.....................................................................................................66Pain Reduction Strategies for Immunizations:..........................................................................67
Health Promotion and Screening...................................................................................................68Periodic Health Examination....................................................................................................68
Breast Cancer Screening................................................................................................................69Cervical Cancer Screening............................................................................................................70Colorectal Cancer Screening.........................................................................................................72Skin Cancer Screening...................................................................................................................73Smoking Cessation Medications....................................................................................................74Smoking Cessation Flow Sheet.....................................................................................................76Contraception Options...................................................................................................................77Quick Reference Guide..................................................................................................................80Common Antibiotics......................................................................................................................80Common Antivirals.......................................................................................................................82Immunization Schedule.................................................................................................................83
Vaccine Contraindications...................................................................................................84Live Attenuated Vaccines:...................................................................................................84
Developmental Milestones............................................................................................................85Dermatology Glossary...................................................................................................................86Antenatal Care Timelines..............................................................................................................87
Page 5
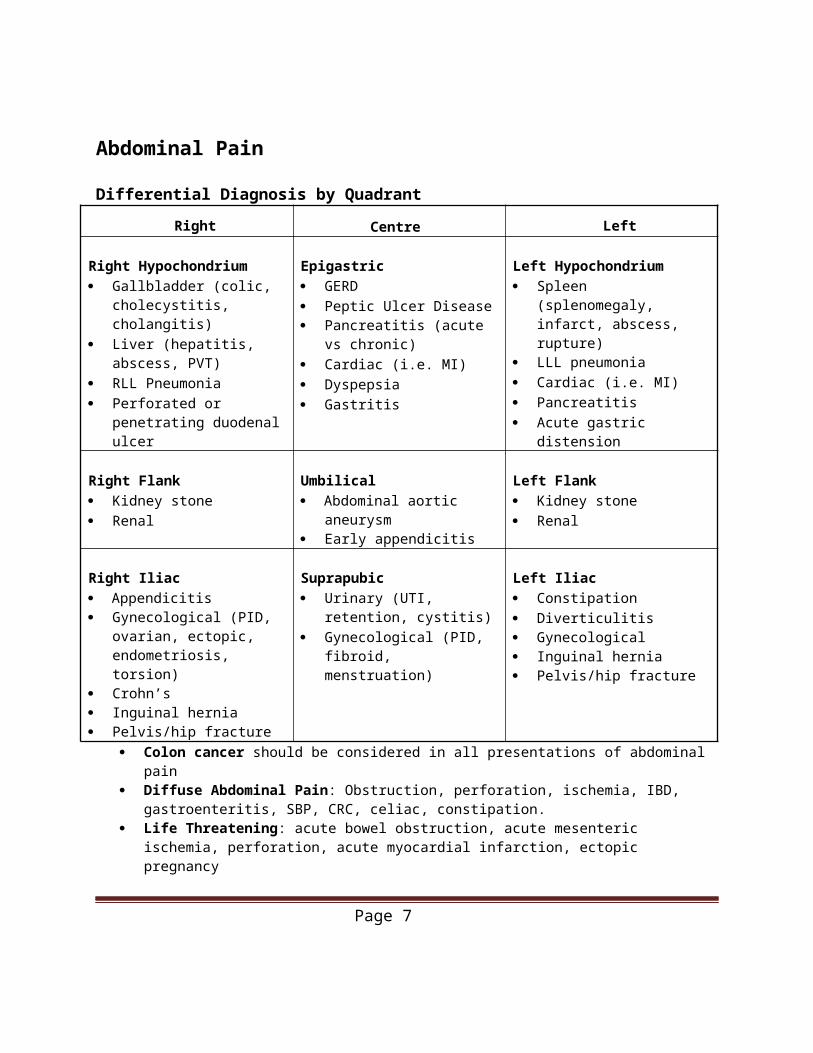
Abdominal Pain
Differential Diagnosis by Quadrant
Right Centre Left
Right Hypochondrium Gallbladder (colic,
cholecystitis, cholangitis) Liver (hepatitis, abscess, PVT) RLL Pneumonia Perforated or penetrating
duodenal ulcer
Epigastric GERD Peptic Ulcer Disease Pancreatitis (acute vs chronic) Cardiac (i.e. MI) Dyspepsia Gastritis
Left Hypochondrium Spleen (splenomegaly, infarct,
abscess, rupture) LLL pneumonia Cardiac (i.e. MI) Pancreatitis Acute gastric distension
Right Flank Kidney stone Renal
Umbilical Abdominal aortic aneurysm Early appendicitis
Left Flank Kidney stone Renal
Right Iliac Appendicitis Gynecological (PID,
ovarian, ectopic, endometriosis, torsion)
Crohn’s Inguinal hernia Pelvis/hip fracture
Suprapubic Urinary (UTI, retention,
cystitis) Gynecological (PID, fibroid,
menstruation)
Left Iliac Constipation Diverticulitis Gynecological Inguinal hernia Pelvis/hip fracture
Colon cancer should be considered in all presentations of abdominal pain Diffuse Abdominal Pain: Obstruction, perforation, ischemia, IBD, gastroenteritis, SBP, CRC, celiac,
constipation. Life Threatening: acute bowel obstruction, acute mesenteric ischemia, perforation, acute myocardial
infarction, ectopic pregnancy
Differential Diagnosis by QuadrantRed Flags
Acute onset Fever Nausea/vomiting Hematochezia Melena Anemia Weight loss >10lbs (unintentional) Change in bowel habits
Chest pain No improvement with current
management Family history of colon cancer or IBD Wakes from sleep Unstable vitals Peritonitis
Sources:Dash M, Arnold A. Guide to the Canadian Family Medicine Examination. New York, NY: McGraw-Hill Education; 2013.Charts. 8th ed. Saskatoon, SK: Saskatoon Heath Region; 2010; 43.Sam AH. Rapid Differential Diagnosis. Blackwell, 2003.
Page 6
Talley NJ, O’Connor S. Clinical Examination: A Systematic Guide to Physical Diagnosis. MacLennan and Petty. 3rd edition, 1998https://www.uptodate.com/contents/causes-of-abdominal-pain-in-adults
Irritable Bowel Syndrome
Rome IV Criteria Recurrent abdominal pain or discomfort at least 1 day/week in the last 3 months.
Associated with ≥2 of the following criteria: o Related to defecationo Onset associated with a change in stool frequencyo Onset associated with a change in stool form (appearance)
Investigations Typical history with no red flags, if red flags consider further imaging and an endoscopic
evaluation Obtain baseline labs (specific to patient’s symptoms) and begin treatment
o Diarrhea predominant: ESR, CBC, TTG (celiac), TSH, O&Po Constipation: CBC, TSH, lytes, Ca, X-ray o Abdo pain: LFTs and amylase
Treatment resistant: further imaging and scope
Management Education and strong therapeutic alliance Conservative
o Trial of soluble fiber (psyllium)o Increase fluid intakeo Dietary modifications (low FODMAP diet, exclusion of gas-producing foods,
decrease caffeine and alcohol intake)o Physical activity
Constipation prone patients with IBS: if fail fiber considero Begin with PEGo Consider Lubiprostone (chloride channel activator), or Linaclotide (guanylate
cyclase agonist) Diarrheaprone patients with IBS: begin with antidiarrheals such as Loperamide
o Consider Bile acid sequestrants (many side effects such as bloating, flatulence, abdominal discomfort and constipation)
Antispasmodic agents PRNo Dicetel (Pinaverium)o Bentyl (Dicyclomine)o Buscopan (Hyoscine)
Sources: Kolodziejak L, Schuster B, Reiger L, Jensen B. Irritable bowel syndrome (IBS). RxFiles Drug Comparison
Page 7
https://www.uptodate.com/contents/treatment-of-irritable-bowel-syndrome-in-adults?source=search_result&search=irritable%20bowel%20syndrome&selectedTitle=1~150#H5
Page 8
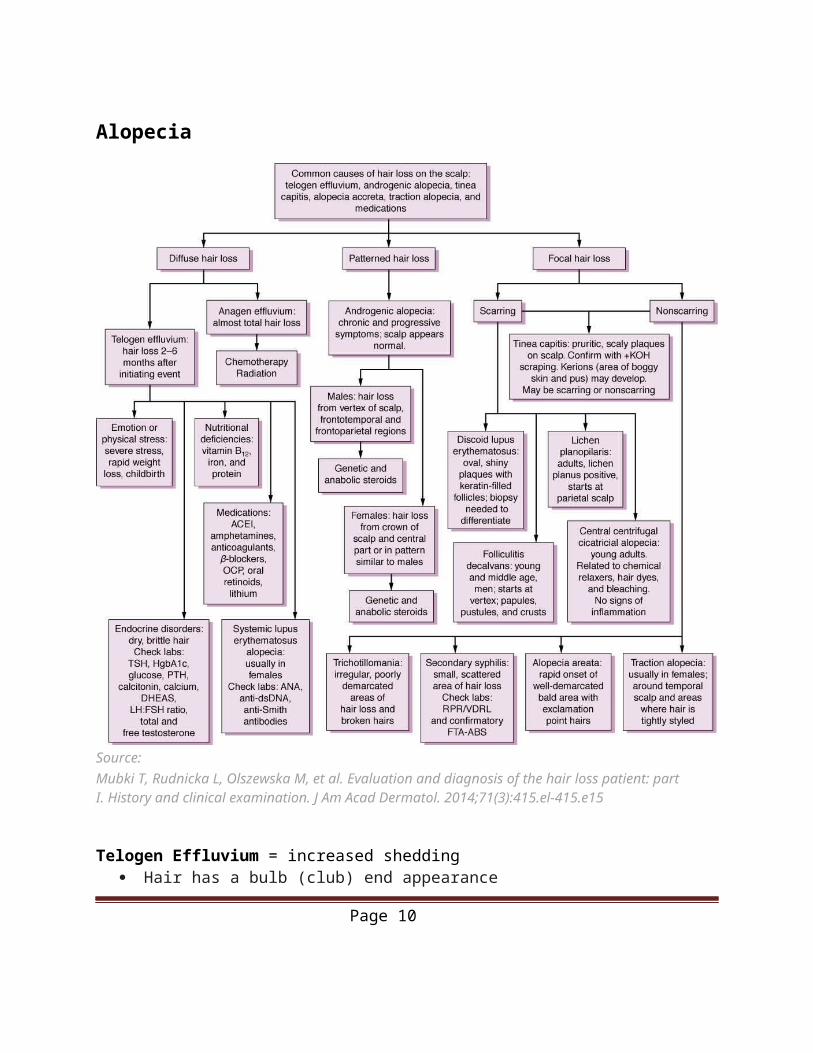
Alopecia
Source: Mubki T, Rudnicka L, Olszewska M, et al. Evaluation and diagnosis of the hair loss patient: part I. History and clinical examination. J Am Acad Dermatol. 2014;71(3):415.el-415.e15
Telogen Effluvium = increased shedding Hair has a bulb (club) end appearance Diffuse non scarring hair loss.
Anagen Effluvium = decreased growth of hair
Page 9
Hair is tapered or broken off with associated shedding. Chemotherapy is the major cause. Interruption in hair growth leading to acute (within 2 weeks) extensive hair loss
Androgenic Alopecia = male/female pattern hair loss Male-pattern hair loss Slow frontotemporal hair loss advancing to vertex and possibly
entire scalp (most common type of hair loss in men) Female-pattern hair loss Less pronounced hair thinning affected anterior scalp with
sparing of the occipital region Treatment:
o Rogaine (Minoxidil) – topical solution applied to the scalp for use in both sexes Hair growth stimulation secondary to vasodilation and increased
cutaneous blood flowo Propecia (Finasteride) – pill only recommended for use in men
Competitively inhibits type II- 5-alpha reductase resulting in decreased conversion of testosterone to dihydrotestosterone
o Others Sprinolactone (Aldactone) and Flutamide for women Euflex (Dutasteride) for men
Trichotillomania = compulsive hair pulling Individuals compulsively pull hair from the scalp or other regions Irregular shapes areas of hair loss with hair at different lengths
Alopecia Areata = autoimmune hair loss Autoimmune disorder resulting in total hair loss of the scalp, which can progress to involve
any body hair but can also include any body hair Hair loss presents as a round bald patch or generalized thinning leading to total hair loss Spontaneous regrowth can occur, but frequent recurrence precipitated by emotional stress Treatment:
o Intra-lesional or topical corticosteroids (Triamcinolone 2.5-5 mg/mL q4-6weeks for 6 months)
o Topical immunotherapy Most effective for extensive scalp involvement (Performed by
Dermatologists)
Traction Alopecia = acquired hair loss Resulting from prolonged or repetitive tension on the scalp of hair
Hair loss due to scalp conditions (e.g., tinea capitis, psoriasis, seborrheic dermatitis)
Sources: Alopecia – Canadian Dermatology Association [Internet]. Dermatology.ca. 2017 [cited 26 April 2017]. Available from: http://www.dermatology.ca/skin-hair-nails/hair/alopecia/#/Mounsey AL, Reed SW. Diagnosing and treating hair loss. American family physician. 2009 Aug
Page 10
15;80(4).Oakley A. Hair loss. DermNet New Zealand [Internet]. Dermnetnz.org. 2017 [cited 26 April 2017]. Available from: http://www.dermnetnz.org/topics/hair-loss/
Asthma
Clinical Features Wheezing, cough and dyspnea
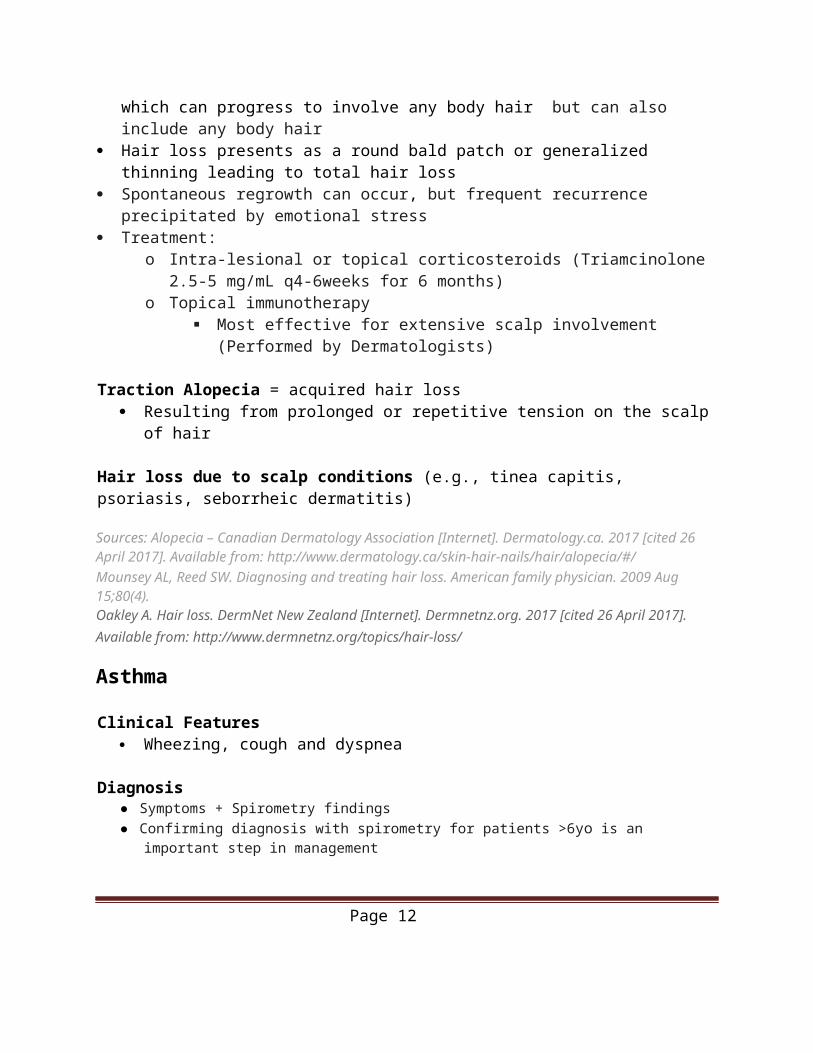
Diagnosis● Symptoms + Spirometry findings● Confirming diagnosis with spirometry for patients >6yo is an important step in management
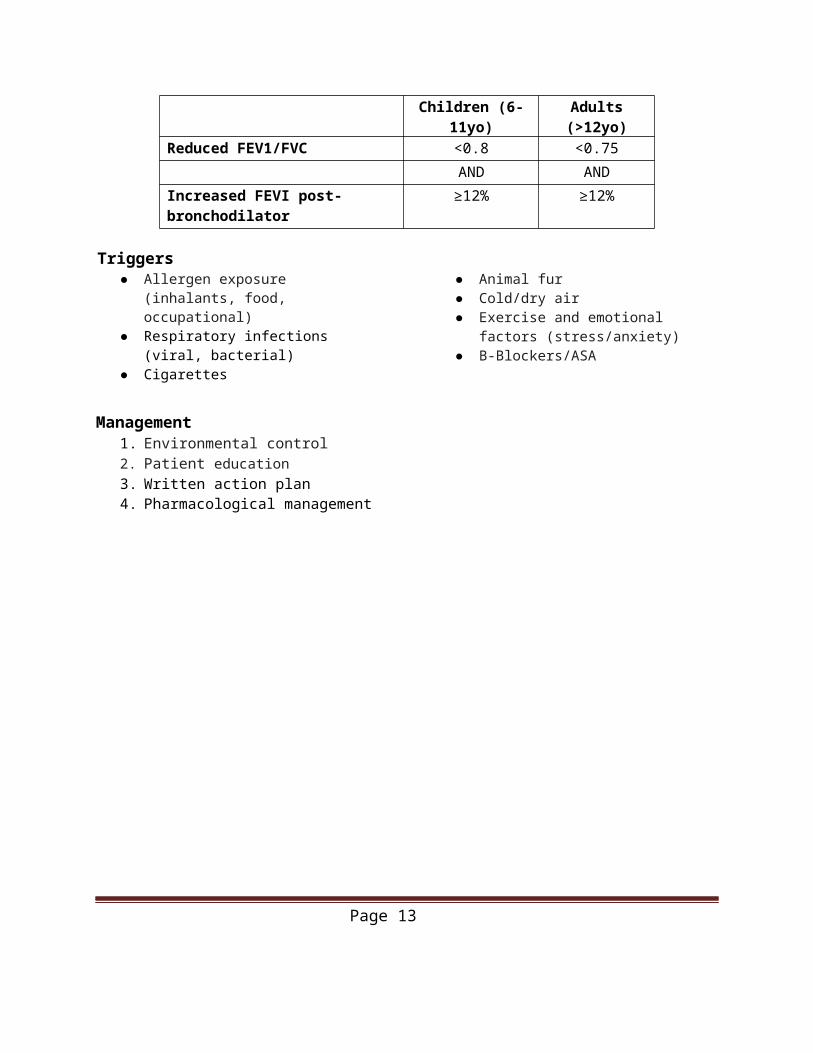
Children (6-11yo) Adults (>12yo)Reduced FEV1/FVC <0.8 <0.75
AND ANDIncreased FEVI post-bronchodilator ≥12% ≥12%
Triggers● Allergen exposure (inhalants, food,
occupational)● Respiratory infections (viral, bacterial)● Cigarettes ● Animal fur
● Cold/dry air● Exercise and emotional factors
(stress/anxiety)● B-Blockers/ASA
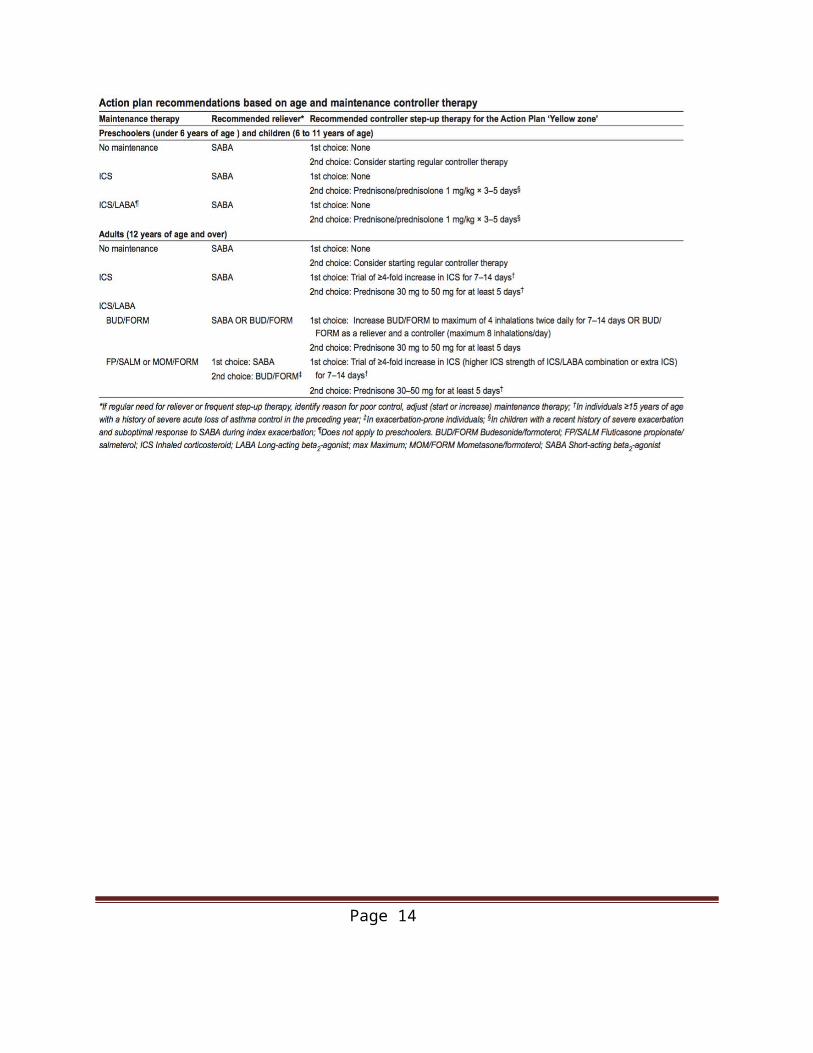
Management1. Environmental control2. Patient education3. Written action plan4. Pharmacological management
Page 11
Page 12
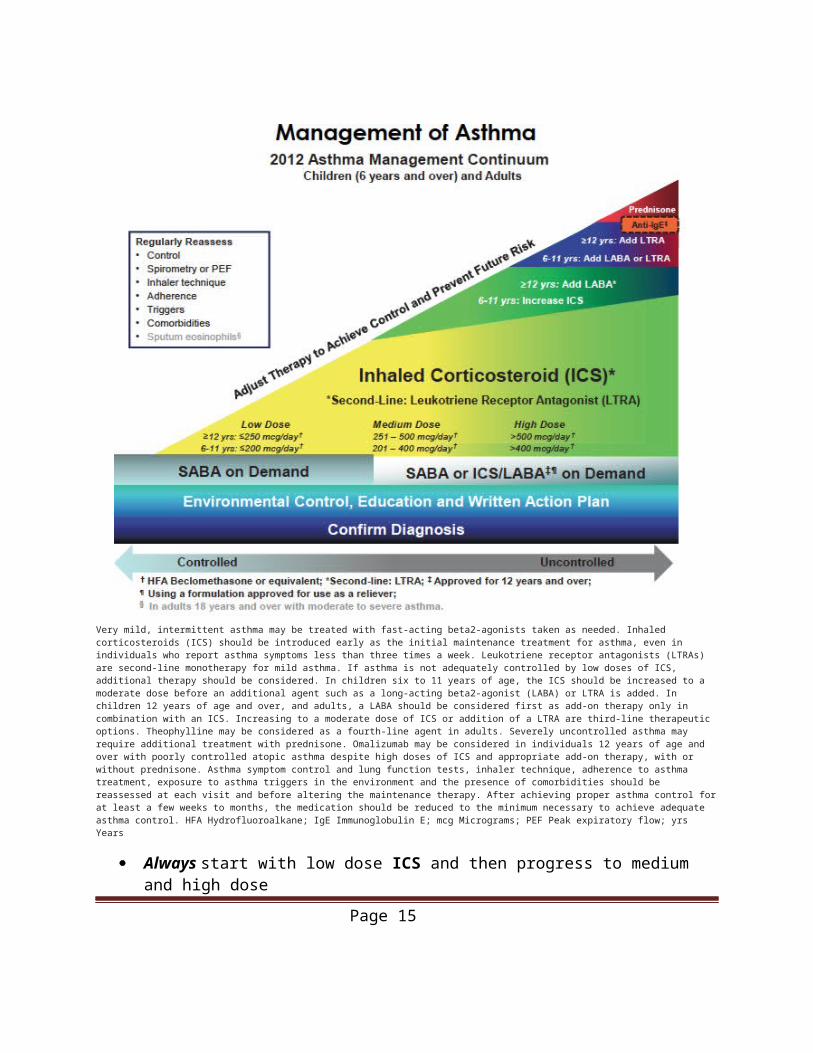
Very mild, intermittent asthma may be treated with fast-acting beta2-agonists taken as needed. Inhaled corticosteroids (ICS) should be introduced early as the initial maintenance treatment for asthma, even in individuals who report asthma symptoms less than three times a week. Leukotriene receptor antagonists (LTRAs) are second-line monotherapy for mild asthma. If asthma is not adequately controlled by low doses of ICS, additional therapy should be considered. In children six to 11 years of age, the ICS should be increased to a moderate dose before an additional agent such as a long-acting beta2-agonist (LABA) or LTRA is added. In children 12 years of age and over, and adults, a LABA should be considered first as add-on therapy only in combination with an ICS. Increasing to a moderate dose of ICS or addition of a LTRA are third-line therapeutic options. Theophylline may be considered as a fourth-line agent in adults. Severely uncontrolled asthma may require additional treatment with prednisone. Omalizumab may be considered in individuals 12 years of age and over with poorly controlled atopic asthma despite high doses of ICS and appropriate add-on therapy, with or without prednisone. Asthma symptom control and lung function tests, inhaler technique, adherence to asthma treatment, exposure to asthma triggers in the environment and the presence of comorbidities should be reassessed at each visit and before altering the maintenance therapy. After achieving proper asthma control for at least a few weeks to months, the medication should be reduced to the minimum necessary to achieve adequate asthma control. HFA Hydrofluoroalkane; IgE Immunoglobulin E; mcg Micrograms; PEF Peak expiratory flow; yrs Years
Always start with low dose ICS and then progress to medium and high dose Never give LABA as mono-therapy (ie. should always be given with ICS) Theophylline is reserved for near last-line Omalizumab can be given to those with atopic asthma and poor control despite high
dose ICS
Source: Canadian Thoracic Society 2012 guideline update: Diagnosis and management of asthma in preschoolers, children and adults (http://www.respiratoryguidelines.ca/sites/all/files/2012_cts_asthma_
Page 13
guideline.pdf). This information was originally published in Can Respir J 2012;19(2):127-164.
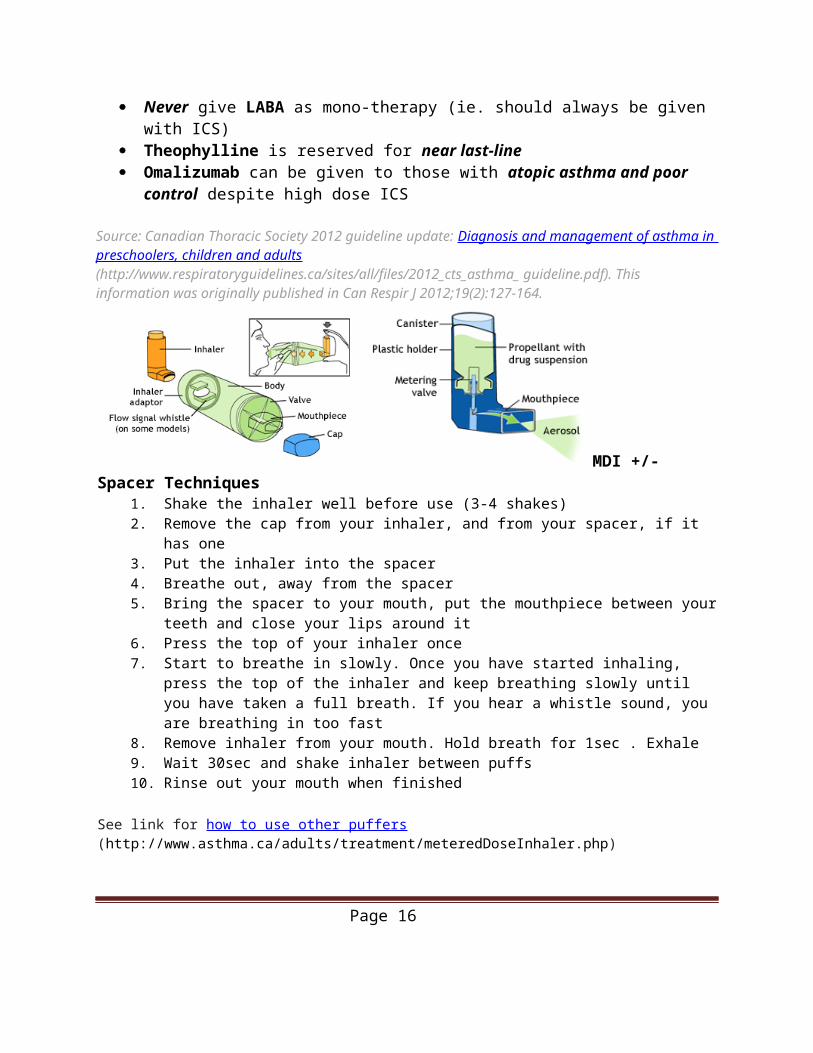
MDI +/- Spacer Techniques
1. Shake the inhaler well before use (3-4 shakes)2. Remove the cap from your inhaler, and from your spacer, if it has one3. Put the inhaler into the spacer4. Breathe out, away from the spacer5. Bring the spacer to your mouth, put the mouthpiece between your teeth and close your lips
around it6. Press the top of your inhaler once7. Start to breathe in slowly. Once you have started inhaling, press the top of the inhaler and
keep breathing slowly until you have taken a full breath. If you hear a whistle sound, you are breathing in too fast
8. Remove inhaler from your mouth. Hold breath for 1sec . Exhale9. Wait 30sec and shake inhaler between puffs10. Rinse out your mouth when finished
See link for how to use other puffers (http://www.asthma.ca/adults/treatment/meteredDoseInhaler.php)
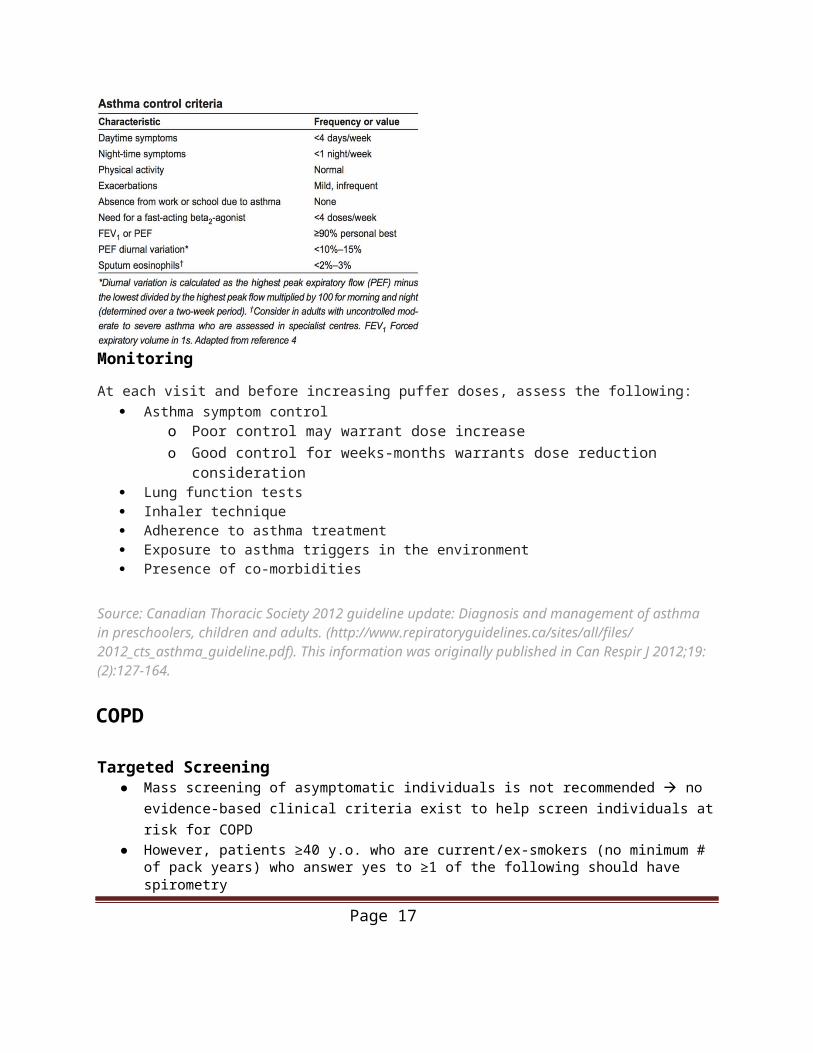
Monitoring
At each visit and before increasing puffer doses, assess the following: Asthma symptom control
Page 14
o Poor control may warrant dose increaseo Good control for weeks-months warrants dose reduction consideration
Lung function tests Inhaler technique Adherence to asthma treatment Exposure to asthma triggers in the environment Presence of co-morbidities
Source: Canadian Thoracic Society 2012 guideline update: Diagnosis and management of asthma in preschoolers, children and adults. (http://www.repiratoryguidelines.ca/sites/all/files/ 2012_cts_asthma_guideline.pdf). This information was originally published in Can Respir J 2012;19: (2):127-164.
COPD
Targeted Screening● Mass screening of asymptomatic individuals is not recommended no evidence-based clinical
criteria exist to help screen individuals at risk for COPD● However, patients ≥40 y.o. who are current/ex-smokers (no minimum # of pack years) who answer
yes to ≥1 of the following should have spirometryo Do you cough regularly?o Do you cough up phlegm regularly?o Do even simple chores make you short of breath?o Do you wheeze when you exert yourself, or at night?o Do you get frequent colds that persist longer than those of other people you know?
Triggers for a COPD Exacerbation Respiratory Infection (viral or bacterial) Stress Air pollution or changes in weather
Indications of a COPD Exacerbation Change in the amount or color of the sputum More short of breath than usual Possible changes in mood (feeling down or anxious) Low energy of tiredness
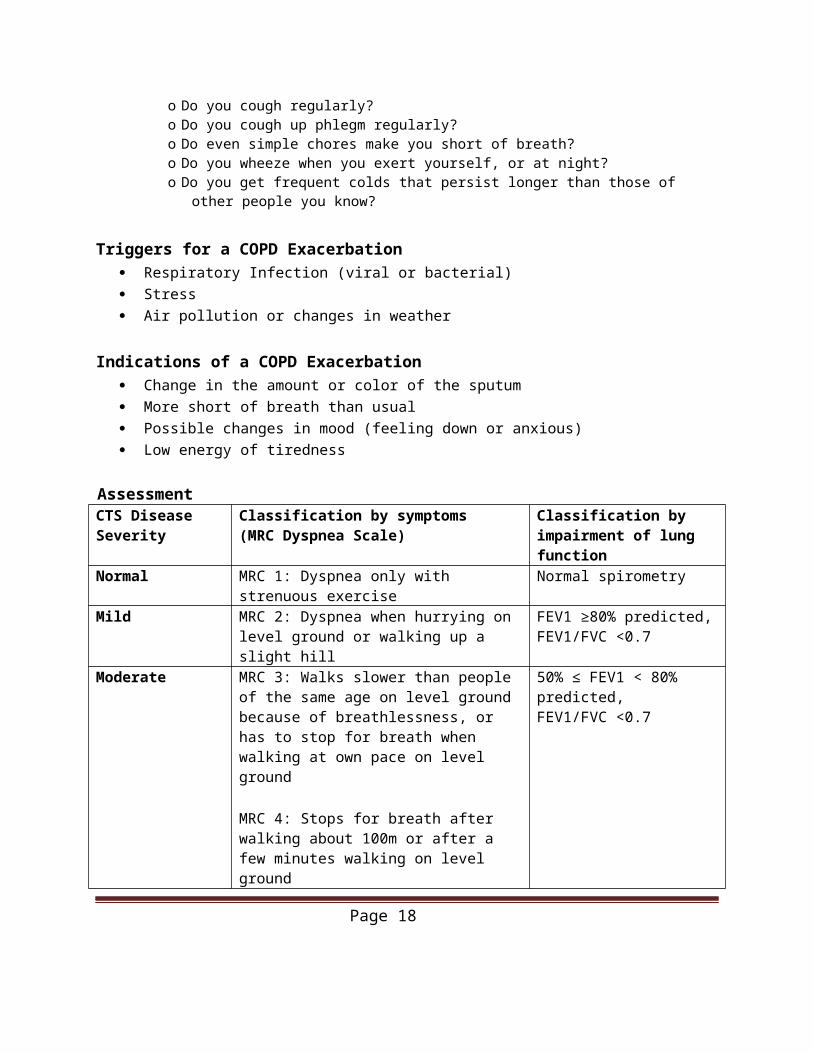
AssessmentCTS Disease Severity
Classification by symptoms (MRC Dyspnea Scale)
Classification by impairment of lung function
Normal MRC 1: Dyspnea only with strenuous exercise Normal spirometry
Mild MRC 2: Dyspnea when hurrying on level ground or walking up a slight hill
FEV1 ≥80% predicted,FEV1/FVC <0.7
Page 15
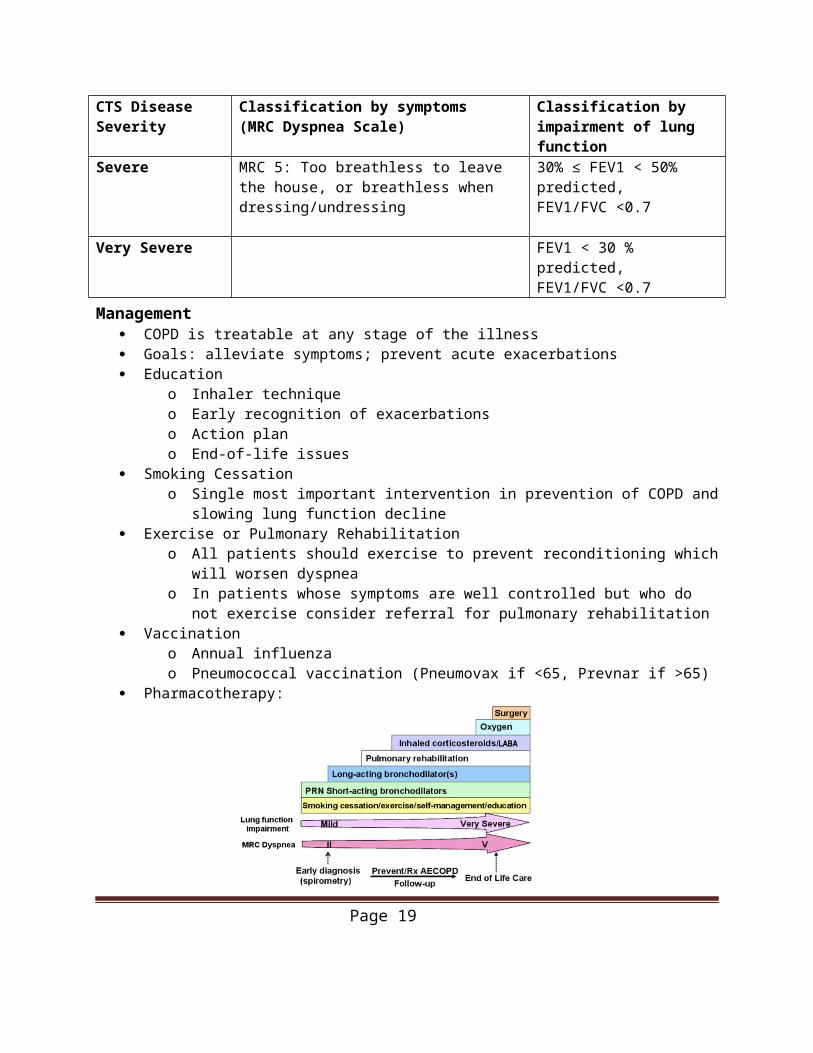
CTS Disease Severity
Classification by symptoms (MRC Dyspnea Scale)
Classification by impairment of lung function
Moderate MRC 3: Walks slower than people of the same age on level ground because of breathlessness, or has to stop for breath when walking at own pace on level ground
MRC 4: Stops for breath after walking about 100m or after a few minutes walking on level ground
50% ≤ FEV1 < 80% predicted,FEV1/FVC <0.7
Severe MRC 5: Too breathless to leave the house, or breathless when dressing/undressing
30% ≤ FEV1 < 50% predicted,FEV1/FVC <0.7
Very Severe FEV1 < 30 % predicted,FEV1/FVC <0.7
Management COPD is treatable at any stage of the illness Goals: alleviate symptoms; prevent acute exacerbations Education
o Inhaler techniqueo Early recognition of exacerbationso Action plano End-of-life issues
Smoking Cessationo Single most important intervention in prevention of COPD and slowing lung function
decline Exercise or Pulmonary Rehabilitation
o All patients should exercise to prevent reconditioning which will worsen dyspneao In patients whose symptoms are well controlled but who do not exercise consider referral
for pulmonary rehabilitation Vaccination
o Annual influenzao Pneumococcal vaccination (Pneumovax if <65, Prevnar if >65)
Pharmacotherapy:
Page 16
Indications for Home Oxygen Therapy● Severe hypoxemia (PaO2 ≤55mmHg or SaO2≤88%)● PaO2 <59mmHg + bilateral ankle edema or cor pulmonale (ECG) or Hct >55%
Source:s2013 CTS COPD Action Plan. Canadian Respiratory Guidelines [Internet]. Respiratoryguidelines.ca. 2017 [cited 27 April 2017]. Available from: http://www.respiratoryguidelines.ca/updated-cts-copd-action-planCTS recommendations for management of COPD 2008 – highlights for primary care (http://www. respiratoryguidelines.ca/sites/all/files/CTS_COPD_Highlights_2008.pdf). This information wasoriginally published in Can Respir J 2008; 15 (SupplA): 1A-8A.Criner G, Bourbeau J. 2014 CHEST-CTS Guideline: Prevention of Acute Exacerbation of Chronic Obstructive Pulmonary Disease. Presentation presented at; 2017.O’donnell DE, Aaron S, Bourbeau J, Hernandez P, Marciniuk DD, Balter M, Ford G, Gervais A, Goldstein R, Hodder R, Kaplan A. Canadian Thoracic Society recommendations for management of chronic obstructive pulmonary disease–2007 update. Canadian Respiratory Journal. 2007;14(Suppl B):5B-32B.Recommendations for the Management of Chronic Obstructive Pulmonary Disease 2008 Update [Internet]. 1st ed. Canadian Thoracic Society; 2008 [cited 27 April 2017]. Available from: http://www.respiratoryguidelines.ca/sites/all/files/2008_CTS_Slide_Kit_COPD.pdf
Page 17
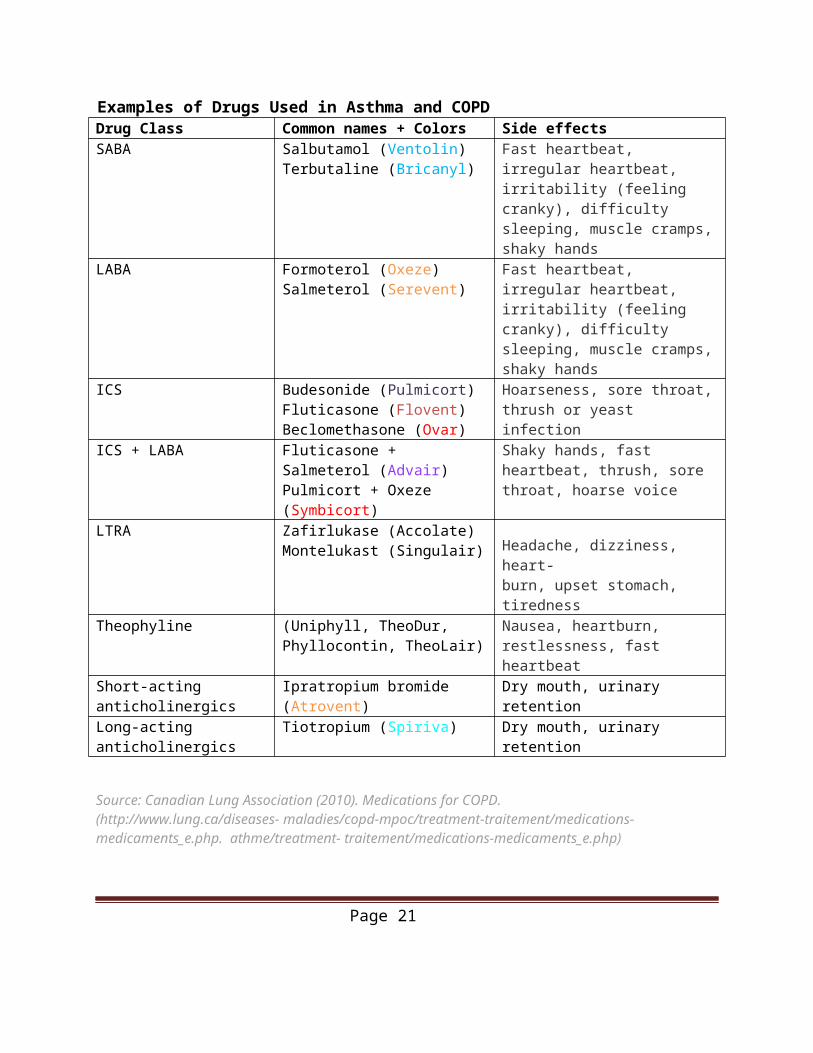
Examples of Drugs Used in Asthma and COPDDrug Class Common names + Colors Side effectsSABA Salbutamol (Ventolin)
Terbutaline (Bricanyl)Fast heartbeat, irregular heartbeat, irritability (feeling cranky), difficulty sleeping, muscle cramps, shaky hands
LABA Formoterol (Oxeze)Salmeterol (Serevent)
Fast heartbeat, irregular heartbeat, irritability (feeling cranky), difficulty sleeping, muscle cramps, shaky hands
ICS Budesonide (Pulmicort)Fluticasone (Flovent)Beclomethasone (Ovar)
Hoarseness, sore throat, thrush or yeast infection
ICS + LABA Fluticasone + Salmeterol (Advair)Pulmicort + Oxeze (Symbicort)
Shaky hands, fast heartbeat, thrush, sore throat, hoarse voice
LTRA Zafirlukase (Accolate)Montelukast (Singulair) Headache, dizziness, heart-
burn, upset stomach, tirednessTheophyline (Uniphyll, TheoDur, Phyllocontin,
TheoLair)Nausea, heartburn, restlessness, fast heartbeat
Short-acting anticholinergics Ipratropium bromide (Atrovent) Dry mouth, urinary retention
Long-acting anticholinergics Tiotropium (Spiriva) Dry mouth, urinary retention
Source: Canadian Lung Association (2010). Medications for COPD. (http://www.lung.ca/diseases- maladies/copd-mpoc/treatment-traitement/medications-medicaments_e.php. athme/treatment- traitement/medications-medicaments_e.php)
Page 18
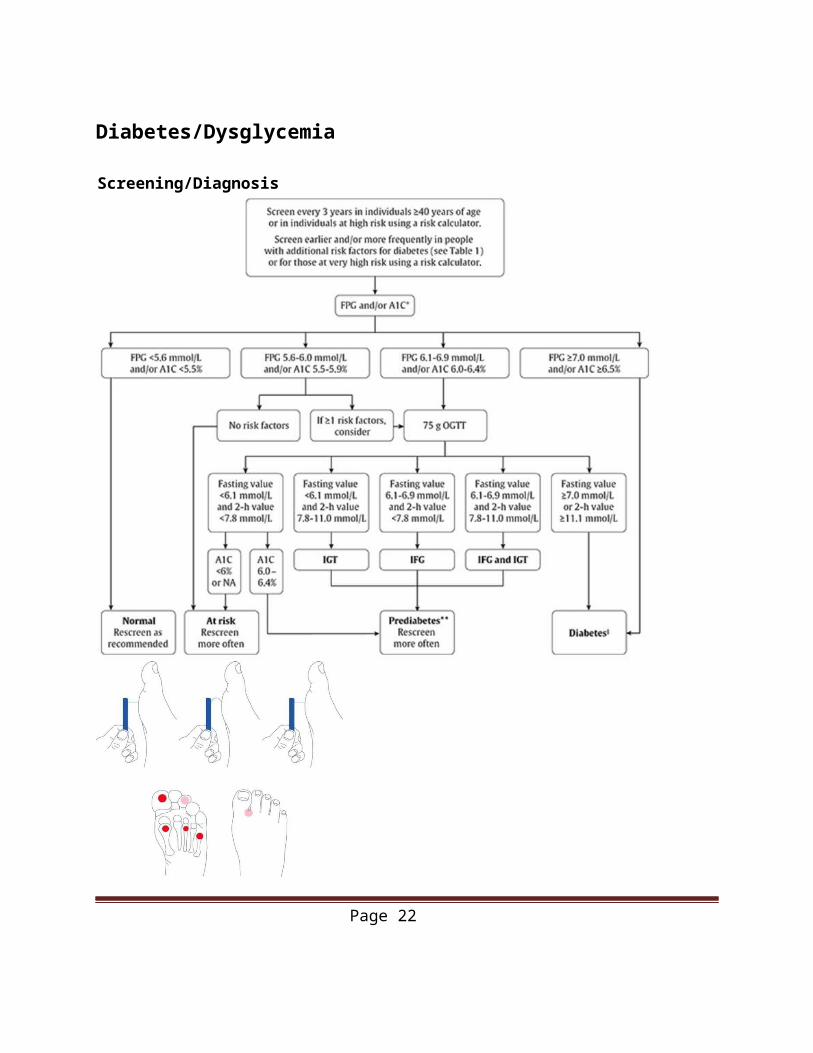
Diabetes/Dysglycemia
Screening/Diagnosis
10g Monofilament Test1. Demonstrate on patient’s forearm how the
Page 19

monofilament feels2. Instruct the patient to close their eyes and say “yes”
when they feel the filament applied3. Using a 10g monofilament and one smooth motion,
apply pressure until the filament bends and then release
4. Do this at four sites on the plantar surface of the patient’s foot (1st, 3rd, and 5th metatarsal heads and plantar surface of distal hallux)
Source:Screening [Internet]. Guidelines.diabetes.ca. 2017 [cited 27 April 2017]. Available from: http://guidelines.diabetes.ca/screeninganddiagnosis/screening
Page 20
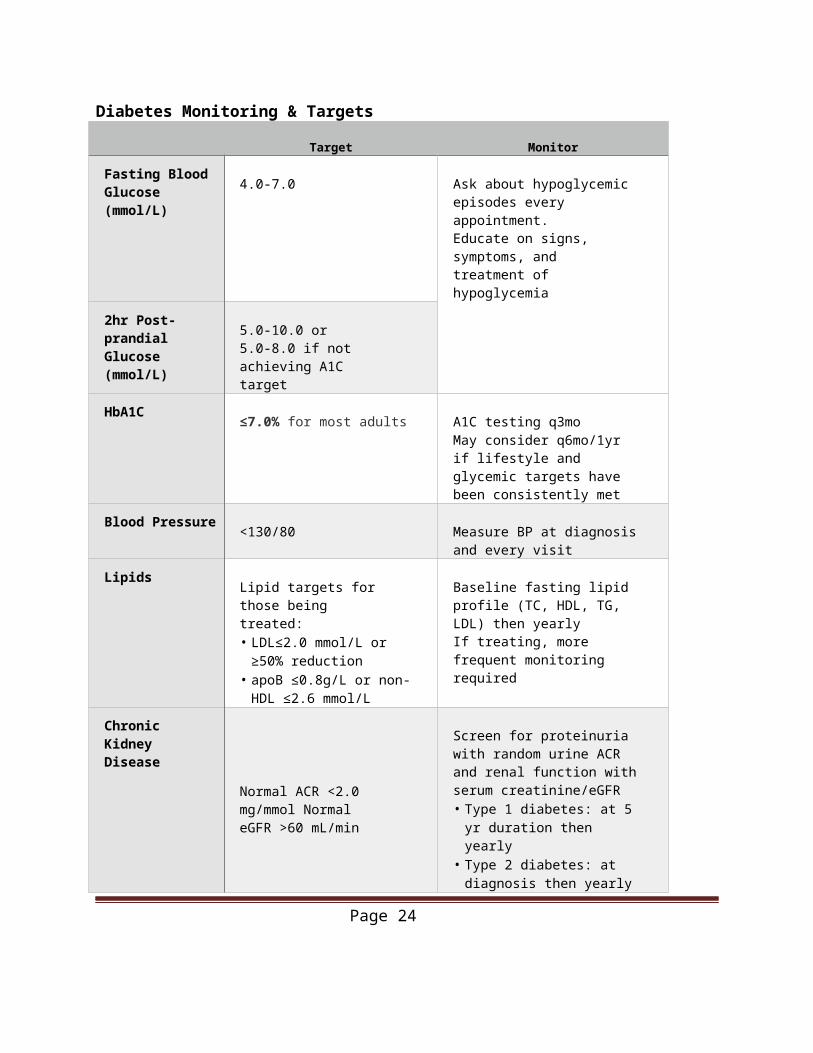
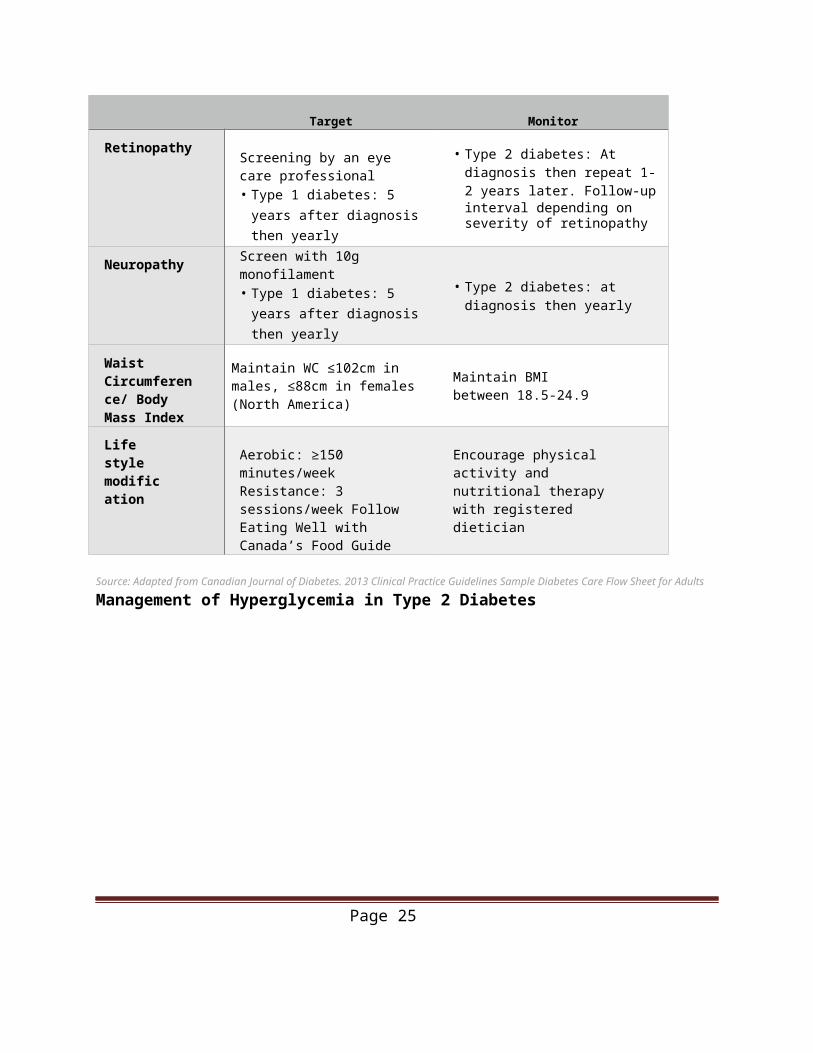
Diabetes Monitoring & Targets
Target Monitor
Fasting Blood Glucose (mmol/L) 4.0-7.0 Ask about hypoglycemic
episodes every appointment.Educate on signs, symptoms, and treatment of hypoglycemia
2hr Post-prandial Glucose (mmol/L) 5.0-10.0 or 5.0-8.0 if
not achieving A1C target
HbA1C ≤7.0% for most adults A1C testing q3moMay consider q6mo/1yr if lifestyle and glycemic targets have been consistently met
Blood Pressure <130/80 Measure BP at diagnosis and every visit
Lipids Lipid targets for those being treated:• LDL≤2.0 mmol/L or
≥50% reduction• apoB ≤0.8g/L or non-HDL
≤2.6 mmol/L
Baseline fasting lipid profile (TC, HDL, TG, LDL) then yearlyIf treating, more frequent monitoring required
Chronic Kidney Disease
Normal ACR <2.0 mg/mmol Normal eGFR >60 mL/min
Screen for proteinuria with random urine ACR and renal function with serum creatinine/eGFR• Type 1 diabetes: at 5 yr
duration then yearly• Type 2 diabetes: at diagnosis
then yearly
Retinopathy Screening by an eye care professional• Type 1 diabetes: 5 years after
diagnosis then yearly
• Type 2 diabetes: At diagnosis then repeat 1-2 years later. Follow-upinterval depending on severity of retinopathy
Neuropathy Screen with 10g monofilament• Type 1 diabetes: 5 years after
diagnosis then yearly
• Type 2 diabetes: at diagnosis then yearly
Waist Circumference/ Body Mass Index
Maintain WC ≤102cm in males, ≤88cm in females (North America)
Maintain BMI between 18.5-24.9
Page 21
Target Monitor
Life style modification
Aerobic: ≥150 minutes/week Resistance: 3 sessions/week Follow Eating Well with Canada’s Food Guide
Encourage physical activity and nutritional therapy with registered dietician
Source: Adapted from Canadian Journal of Diabetes. 2013 Clinical Practice Guidelines Sample Diabetes Care Flow Sheet for Adults
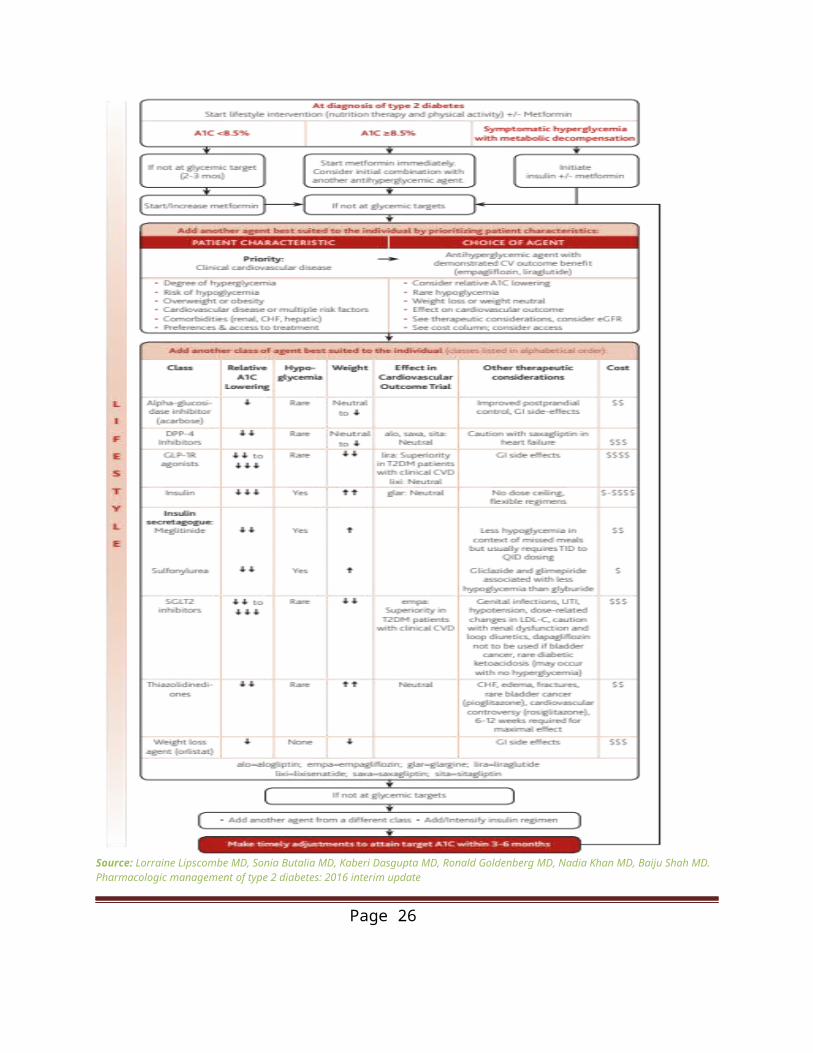
Management of Hyperglycemia in Type 2 Diabetes
Page 22
Source: Lorraine Lipscombe MD, Sonia Butalia MD, Kaberi Dasgupta MD, Ronald Goldenberg MD, Nadia Khan MD, Baiju Shah MD. Pharmacologic management of type 2 diabetes: 2016 interim update
Page 23
Gestational Diabetes
Risk Factors History of GDM or macrocosmic infant Family history of DM Current fetal macrosomia or polyhydramnios [Grade D recommendation] Age ≥35yo High risk population (Aboriginal, Hispanic, South Asian, Asian, African) BMI ≥30kg/m2 PCOS, acanthosis nigricans, metabolic syndrome Essential HTN or pregnancy-related HTN Corticosteroid use Multiple gestations Glycosuria at first prenatal visit
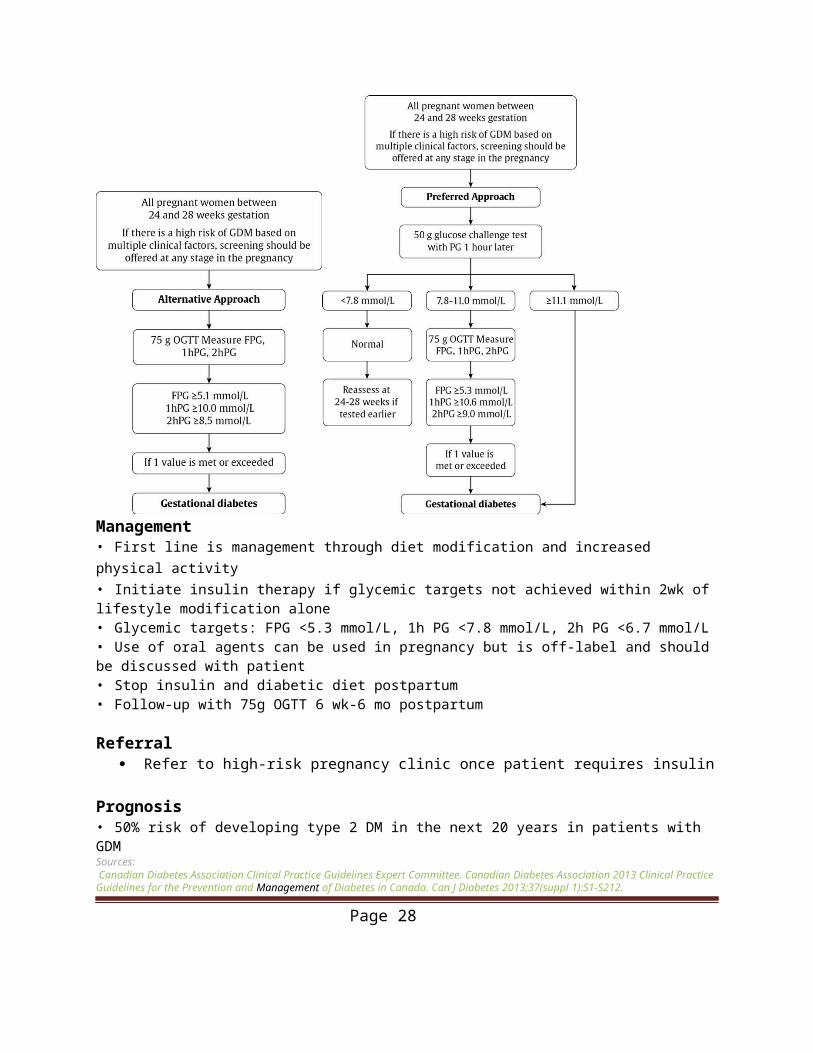
Screening and Diagnosis If patient has multiple clinical factors and is at high risk for GDM, screening should be offered at
any stage in pregnancy [Grade D recommendation] If screening is performed prior to the recommended 24-28 week window, the patient should be
rescreened during the recommended time Two step: 1hr glucose challenge test (GCT), if positive then 2hr GCT—Canadian Diabetes
Association recommendation One step: Only 2 hr GCT
Page 24
Management• First line is management through diet modification and increased physical activity• Initiate insulin therapy if glycemic targets not achieved within 2wk of lifestyle modification alone• Glycemic targets: FPG <5.3 mmol/L, 1h PG <7.8 mmol/L, 2h PG <6.7 mmol/L• Use of oral agents can be used in pregnancy but is off-label and should be discussed with patient• Stop insulin and diabetic diet postpartum• Follow-up with 75g OGTT 6 wk-6 mo postpartum
Referral Refer to high-risk pregnancy clinic once patient requires insulin
Prognosis• 50% risk of developing type 2 DM in the next 20 years in patients with GDMSources: Canadian Diabetes Association Clinical Practice Guidelines Expert Committee. Canadian Diabetes Association 2013 Clinical Practice Guidelines for the Prevention and Management of Diabetes in Canada. Can J Diabetes 2013;37(suppl 1):S1-S212. https://www.uptodate.com/contents/diabetes-mellitus-in-pregnancy-screening-and-diagnosis
Page 25
Dizziness/VertigoApproach to Dizziness
Source: Post, R.E., & Dickerson, L.M. (2010) Dizziness: A Diagnostic Approach. Am Fam Physician,
Page 26
82(4), 361-368. (http://www.aafp.org/afp/2010/0815/p361.html)
DyslipidemiaScreening for Dyslipidemia
Management of Dyslipidemia
Page 27
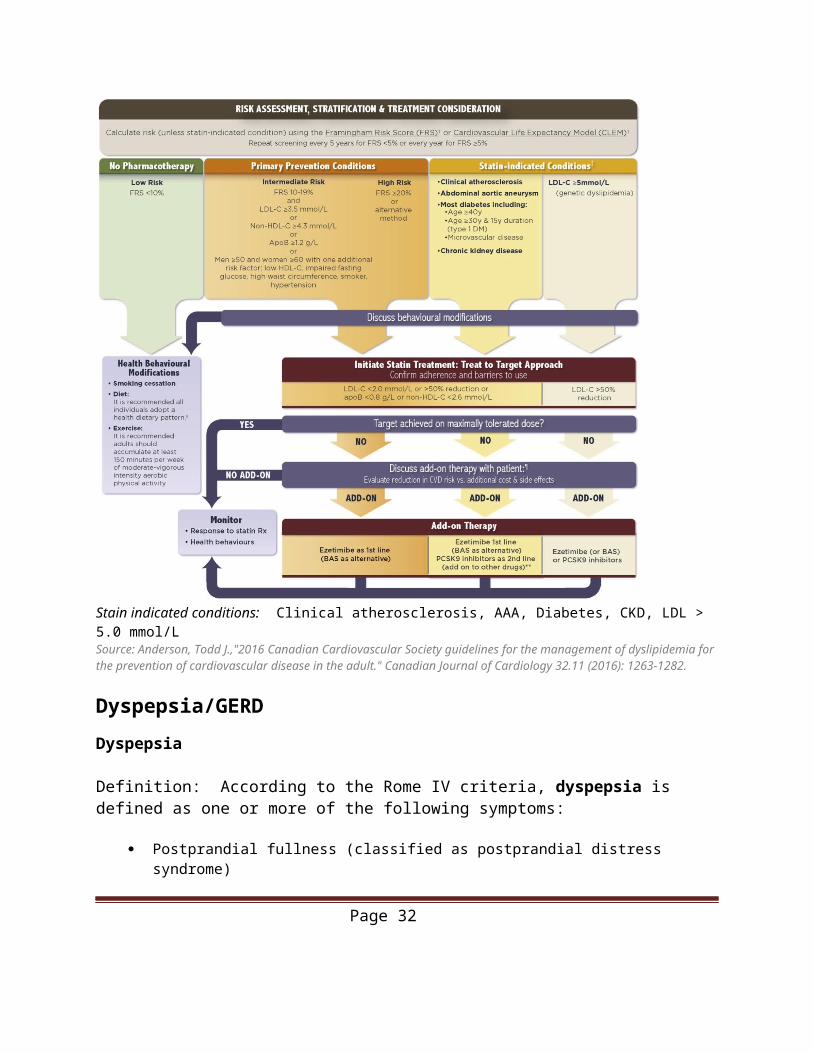
Stain indicated conditions: Clinical atherosclerosis, AAA, Diabetes, CKD, LDL > 5.0 mmol/LSource: Anderson, Todd J.,"2016 Canadian Cardiovascular Society guidelines for the management of dyslipidemia for the prevention of cardiovascular disease in the adult." Canadian Journal of Cardiology 32.11 (2016): 1263-1282.
Dyspepsia/GERDDyspepsia
Definition: According to the Rome IV criteria, dyspepsia is defined as one or more of the following symptoms:
Postprandial fullness (classified as postprandial distress syndrome) Early satiation (inability to finish a normal sized meal, also classified as postprandial distress
syndrome) Epigastric pain or burning (classified as epigastric pain syndrome)
Approximately 25 percent of patients with dyspepsia have an underlying organic cause. However, up to 75 percent of patients have functional (idiopathic or nonulcer) dyspepsia with no underlying cause on diagnostic evaluation.
Red Flags in dyspepsia: Age >55 with new onset dyspepsia Family history of upper GI cancer Progressive dysphagia Odynophagia Unexplained iron deficiency anemia Persistent vomiting Palpable mass or lymphadenopathy Jaundice
GERD
Gastroesophageal reflux disease (GERD) is a condition that develops when the reflux of stomach contents causes troublesome symptoms and/or complications. The diagnosis of GERD can be based upon clinical symptoms alone.
GERD is classified based on the appearance of the esophageal mucosa on upper endoscopy into the following:
Erosive esophagitis — Erosive esophagitis is characterized by endoscopically visible breaks in the distal esophageal mucosa with or without troublesome symptoms of GERD.
Nonerosive reflux disease — Nonerosive reflux disease or endoscopy negative reflux disease is characterized by the presence of troublesome symptoms of GERD without visible esophageal mucosal injury.
Page 28

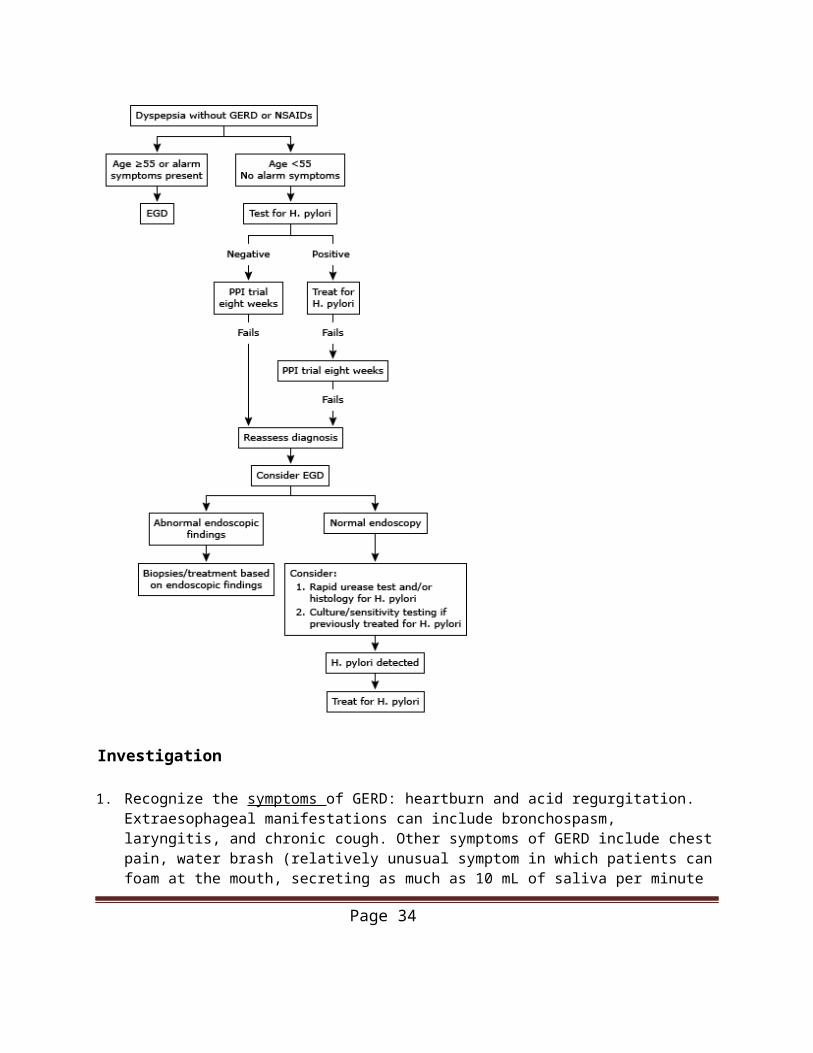
Investigation
1. Recognize the symptoms of GERD: heartburn and acid regurgitation. Extraesophageal manifestations can include bronchospasm, laryngitis, and chronic cough. Other symptoms of GERD include chest pain, water brash (relatively unusual symptom in which patients can foam at the mouth, secreting as much as 10 mL of saliva per minute in response to reflux), globus sensation, odynophagia, and nausea.
2. Look for alarm features: vomiting, evidence of GI blood loss, anemia, involuntary weight loss, dysphagia, or chest pain
Page 29

3. Endoscopic evaluation is not routinely done to diagnose GERD4. Use endoscopy to:
Investigate atypical or alarm features Detect Barrett’s esophagus Investigate dysphagia that has not resolved within 2-4 weeks of adequate twice daily PPI
therapy Determine severity of erosive esophagitis (look for erosions or mucosal breaks)
5. You do not need to test for H. pylori before starting treatment for typical GERD symptoms
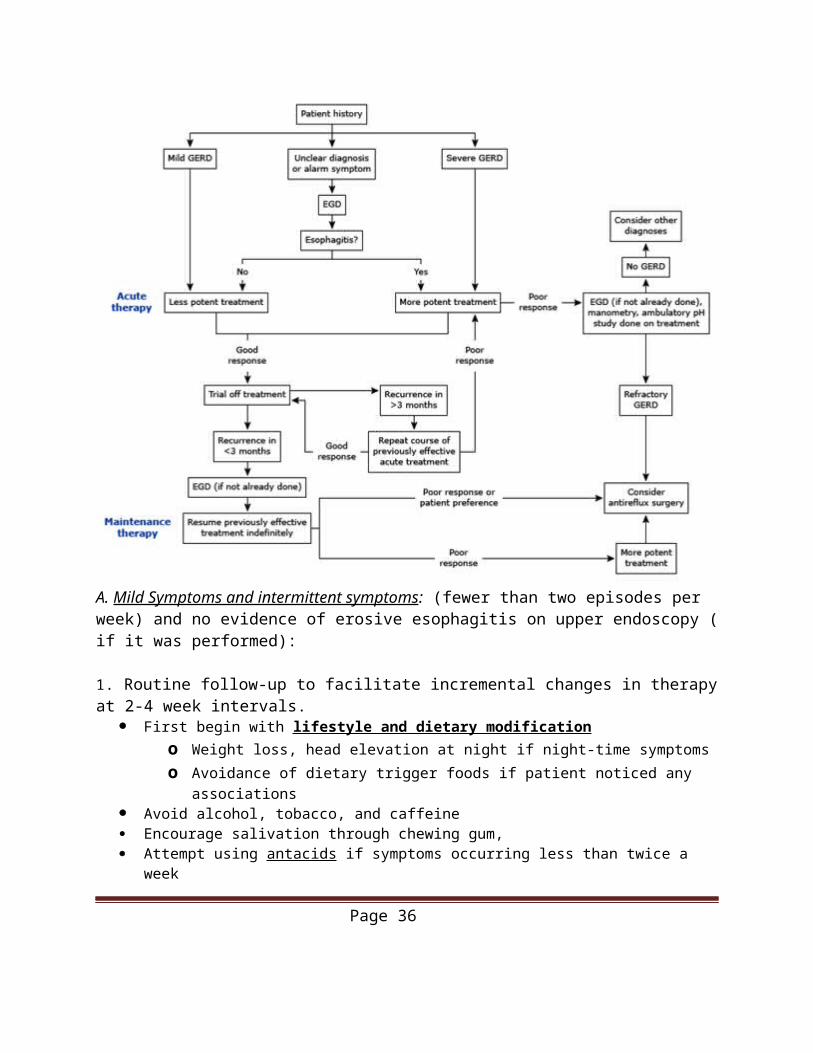
Treatment of GERD
A. Mild Symptoms and intermittent symptoms: (fewer than two episodes per week) and no evidence of erosive esophagitis on upper endoscopy ( if it was performed):
1. Routine follow-up to facilitate incremental changes in therapy at 2-4 week intervals. First begin with lifestyle and dietary modification
o Weight loss, head elevation at night if night-time symptomso Avoidance of dietary trigger foods if patient noticed any associations
Page 30
Avoid alcohol, tobacco, and caffeine Encourage salivation through chewing gum, Attempt using antacids if symptoms occurring less than twice a week Consider stating low-dose his t amine 2 receptor antagonists (H2RAs) PRN
2. If symptoms despite these measures. Increase the dose of H2RAs to standard dose, twice daily for a minimum of two weeks. If symptoms of GERD persist, discontinue H2RAs and initiate once-daily PPIs at a low
dose o Increase doses if required.o Once symptoms are controlled, treatment should be continued for at least eight
weeks.
B. Severe or frequent symptoms (two or more episodes per week, impact quality of life) or erosive esophagitis
1. Begin with standard-dose PPI once daily for 4-8 weeks in addition to lifestyle and dietary modification.
2. If symptoms improve decrease acid suppression to low-dose PPIs and then to H2RAs 3. Discontinue acid suppression in all asymptomatic patients with the exception of patients
with severe erosive esophagitis or Barrett's esophagus, in whom maintenance PPI therapy is suggested.
Diagnostic testing for H. pylori 1. Non invasive
Urea breath test, stool antigen assay, serology (IgG)2. Endoscopic
Biopsy urease testing, histology Treatment: H. pylori Eradication
1. Triple therapy for 7-14 d (Hp-Pac): PPI bid (e.g. lansoprazole 30mg bid) + amoxicillin 1g bid + clarithromycin 500mg bid
Less than 80% success rate due to Clarithromycin resistance 2. Quadruple therapy for 10-14 d: PPI bid + bismuth 525mg qid + tetracycline 500mg qid +
metronidazole 250mg qid First line therapy if resistance to clarithromycin or metronidazole is high, or in patients
with recent or repeated exposure to these drugs Levofloxacin can replace metronidazole or tetracycline
Sources:Ontario Guidelines Advisory Committee (2007). Gastroesophageal Reflux Disease (GERD) in Adults. Ref.#248 (http://www.gacguidelines.ca/site/GAC_Guidelines/assets/pdf/GERD05_Summary.pdf) Toronto Notes 2015 Gastroenterology G14https://www.uptodate.com/contents/approach-to-the-adult-with-dyspepsiahttps://www.uptodate.com/contents/medical-management-of-gastroesophageal-reflux-disease-in-adults
Page 31
https://www.uptodate.com/contents/clinical-manifestations-and-diagnosis-of-gastroesophageal-reflux-in-adults
GoutGout is defined as arthritis due to precipitation of monosodium urate crystals in the joint space.
Risk factors Body mass index Hypertension Diuretic use Coffee consumption Alcohol intake Sweetened beverage consumption Meat/seafood consumption Dairy product consumption Vitamin C intake
Diagnostic criteria Presence of characteristic urate crystals in the joint fluidOR Presence of a tophus proven to contain urate crystals by chemical means or polarized light microscopyOR Presence of 6 or more of the following clinical, laboratory, or radiologic findings:
o Asymmetric swelling within a joint on radiographyo Attack of monoarticular arthritiso Culture of joint fluid negative for microorganisms during attack of joint inflammationo Development of maximal inflammation within one dayo Hyperuricemiao Joint rednesso More than one attack of acute arthritiso Pain or redness in the first metatarsophalangeal jointo Subcortical cyst without erosions on radiographyo Suspected tophuso Unilateral attack involving first metatarsophalangeal jointo Unilateral attack involving tarsal joint
*Normal serum urate levels do not exclude the diagnosis of gout
TreatmentTreatment principles in Acute Gout:
1. Treatment of acute gout should commence within 24 hours of symptom onset to achieve rapid & complete resolution of symptoms
2. Medical Managementa. Mild - Moderate attack (few small joints or two large joints) includes monotherapy with:
i. NSAIDS (first-line treatment) orii. Colchicine or
iii. Corticosteroids
Page 32
b. Severe attack (many joints) include combination therapy with:i. Colchicine + NSAIDs
ii. Colchicine + Oral Corticosteroidsiii. Intra-articular steroids + all other modalities
*see further detailed management algorithm and medication recommendations below
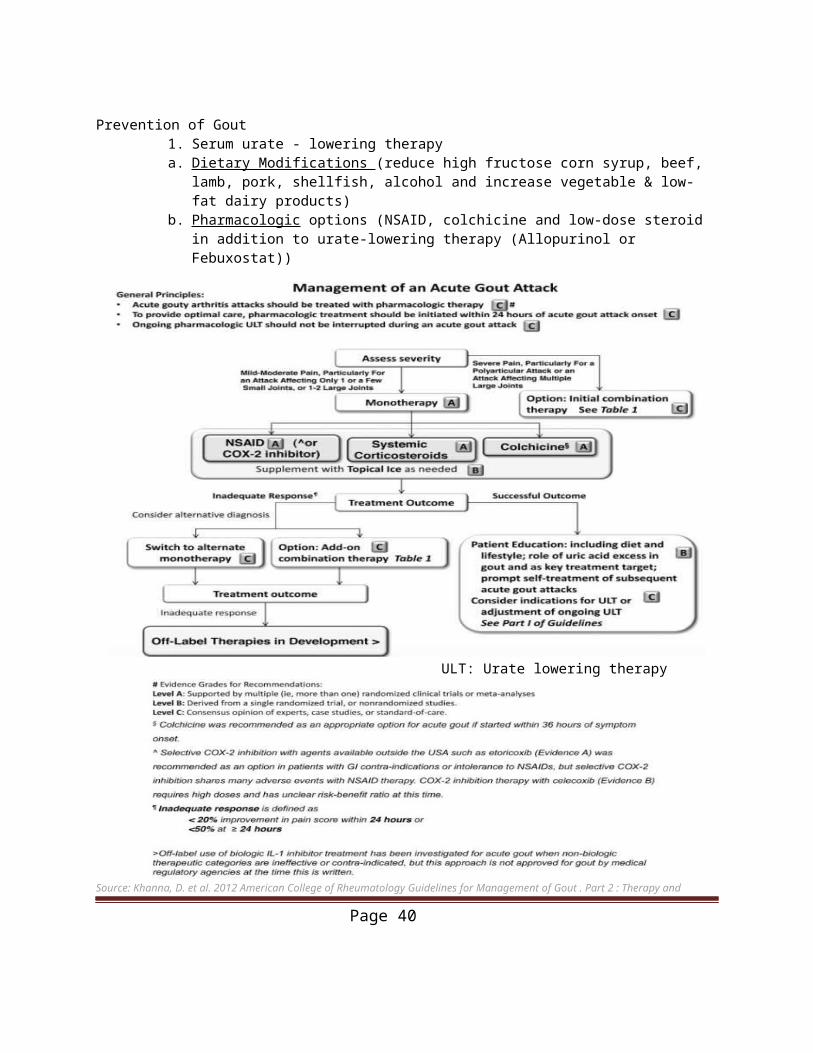
Prevention of Gout1. Serum urate - lowering therapya. Dietary Modifications (reduce high fructose corn syrup, beef, lamb, pork, shellfish, alcohol
and increase vegetable & low-fat dairy products) b. Pharmacologic options (NSAID, colchicine and low-dose steroid in addition to urate-
lowering therapy (Allopurinol or Febuxostat))
ULT: Urate lowering therapy
Page 33
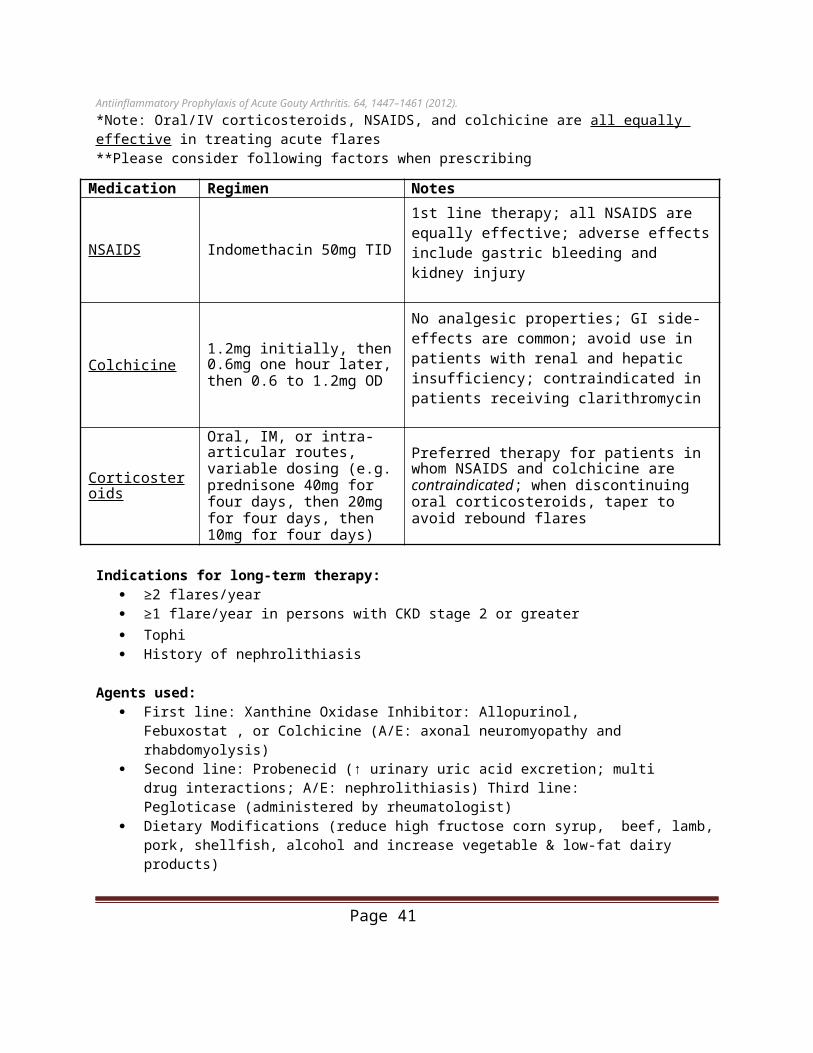
Source: Khanna, D. et al. 2012 American College of Rheumatology Guidelines for Management of Gout . Part 2 : Therapy and Antiinflammatory Prophylaxis of Acute Gouty Arthritis. 64, 1447–1461 (2012).*Note: Oral/IV corticosteroids, NSAIDS, and colchicine are all equally effective in treating acute flares**Please consider following factors when prescribing
Medication Regimen Notes
NSAIDS Indomethacin 50mg TID1st line therapy; all NSAIDS are equally effective; adverse effects include gastric bleeding and kidney injury
Colchicine1.2mg initially, then 0.6mg one hour later, then 0.6 to 1.2mg OD
No analgesic properties; GI side-effects are common; avoid use in patients with renal and hepatic insufficiency; contraindicated in patients receiving clarithromycin
Corticosteroids
Oral, IM, or intra-articular routes, variable dosing (e.g. prednisone 40mg for four days, then 20mg for four days, then 10mg for four days)
Preferred therapy for patients in whom NSAIDS and colchicine are contraindicated; when discontinuing oral corticosteroids, taper to avoid rebound flares
Indications for long-term therapy: ≥2 flares/year ≥1 flare/year in persons with CKD stage 2 or greater Tophi History of nephrolithiasis
Agents used: First line: Xanthine Oxidase Inhibitor: Allopurinol, Febuxostat , or Colchicine (A/E: axonal
neuromyopathy and rhabdomyolysis) Second line: Probenecid (↑ urinary uric acid excretion; multi drug interactions; A/E:
nephrolithiasis) Third line: Pegloticase (administered by rheumatologist) Dietary Modifications (reduce high fructose corn syrup, beef, lamb, pork, shellfish, alcohol and
increase vegetable & low-fat dairy products)
Duration of treatment:• No ongoing symptoms: continue for 3-6 months after a flare• Ongoing signs or symptoms (e.g., tophi on examination): continue indefinitely• Current evidence suggests there is uncertainty about the value of a treat-to-target strategy compared with a strategy of basing treatment intensity on minimizing symptoms.
*ULTs can be started during acute gout flares if used in conjunction with an NSAID and colchicine*Anti-inflammatory prophylaxis should not be continued for long periods without ULT because uric acid crystals continue to accumulate and damage the joint despite a lack of clinical signs/ symptoms.
Sources:Hainer, B. L., Matheson, E., Wilkes, R. T. & Carolina, S. Diagnosis, Treatment, and Prevention of Gout. (2014).Khanna, D. et al. 2012 American College of Rheumatology Guidelines for Management of Gout . Part 2 : Therapy and Antiinflammatory Prophylaxis of Acute Gouty Arthritis. 64, 1447–1461 (2012).Qaseem, Amir, Russell P. Harris, and Mary Ann Forciea. "Management of Acute and Recurrent Gout: A Clinical Practice Guideline From the
Page 34
American College of Physicians." Annals of Internal Medicine 166, no. 1 (2016): 58. doi:10.7326/m16-0570
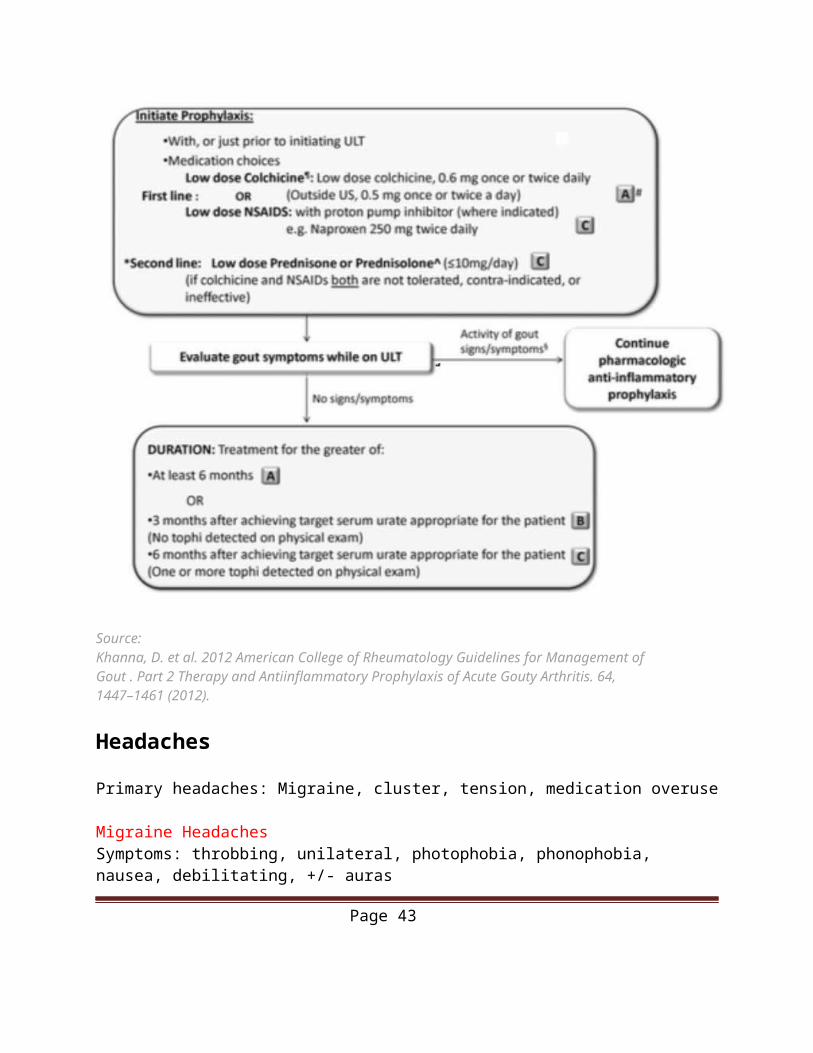
Anti-inflammatory Prophylaxis
Source:Khanna, D. et al. 2012 American College of Rheumatology Guidelines for Management of Gout . Part 2 Therapy and Antiinflammatory Prophylaxis of Acute Gouty Arthritis. 64, 1447–1461 (2012).
Headaches
Primary headaches: Migraine, cluster, tension, medication overuse
Migraine HeadachesSymptoms: throbbing, unilateral, photophobia, phonophobia, nausea, debilitating, +/- aurasTriggers: stress, physical activity, poor sleep, fatigue, EtOH, chocolate, cheese, MSG, aspartame, caffeine, nuts, nitrates
Page 35
Acute Treatment: NSAIDs = first line (ASA 1000mg q4h or Advil 200-800mg), triptans, ergotamines, prochlorperazine 5-10mg IM/IV +/- antiemetics (for nausea)Prevention: B-blockers = first line (propranolol 40-240mg/day), CCB (verapamil 240-320mg/day), anticonvulsants (topiramate 25-100mg/day), TCAs (amitriptyline 50-150mg/day)
Diagnostic criteria for migraine without aura: A. At least five attacks fulfilling criteria B through DB. Headache attacks lasting 4 to 72 hours (untreated or unsuccessfully treated)C. Headache has at least two of the following characteristics:
1. Unilateral location2. Pulsating quality3. Moderate or severe pain intensity4. Aggravation by or causing avoidance of routine physical activity (eg. Walking or
climbing stairs)D. During headache at least one of the following:
1. Nausea, vomiting or both2. Photophobia and phonophobia
E. Not better accounted for by another diagnosis
Diagnostic criteria for migraine with aura:A. At least two attacks fulfilling criterion B and CB. One or more of the following fully reversible aura symptoms
a. Visualb. Sensoryc. Speech and/or languaged. Motore. Brainstemf. Retinal
C. At least three of the following six characteristics a. At least one aura symptom spreads gradually over >5 minutesb. Two or more symptoms occur in successionc. Each individual symptom lasts 5-60 minutesd. At least one aura is unilaterale. At least one aura symptom is positivef. The aura is accompanied or followed within 60 minutes by headache
D. Not better accounted for by another diagnosis
Cluster HeadachesDiagnosis: episodes lasting 15-180 mins, frequency 8x/day to q2d, unilateral (orbital/temporal), autonomic ipsilateral sx (conjunctival injection, tearing, pseudo Horner’s syndrome)Triggers: often alcoholAcute Treatment: 100% O2 = first line (high flow >7L/min x10min), sumatriptan 6mg sc,
Page 36
lidocaine 1mL 4% intranasal, octreotide 100mcg scPrevention: prednisone 40-80mg x7d, then taper over 5 days (bridging prophylaxis), verapamil SR 120-360 mg/day= first line, lithium, methysergide, topiramate, melatonin, ergotamine
Tension HeadachesSymptoms: bilateral, fronto-occipital band-like pain, contracted neck/scalp musclesTriggers: stressful eventsAcute Treatment: rest and relaxation, NSAIDs or acetaminophenPrevention: physical activity, rest, biofeedback
Medication Overuse Headaches
Diagnosis: Episodic headache disorder, migraine or tension-type. Headache occurring on 15 or more days per month, developing as a consequence of regular overuse of acute or symptomatic headache medication for more than three months. Triggers: regular intake, for ≥10 days per month for >3 months, of ergotamines, triptans, opioids, or combination analgesics, or any combination of ergotamines, triptans, simple analgesics, nonsteroidal anti-inflammatory drugs (NSAID) and/or opioidsTreatment: Most experts regard withdrawal of the overused medication as the treatment of choice.
Secondary headaches: Extracranial: carotid or vertebral artery dissection, dental disorders, glaucoma, sinusitisIntracranial: brain tumor/mass, Chiari type I malformation, CSF leak with low-pressure headache, hemorrhage (intracerebral, subdural, subarachnoid), idiopathic intracranial hypertension, infections (meningitis, encephalitis, subdural empyema), obstructive hydrocephalus, vascular disordersSystemic disorders: hypertensive crisis, bacteremia, Giant cell arteritis, hypercapnea, hypoxiaDrugs and toxins: analgesia overdose, caffeine withdrawal, carbon monoxide, hormones (ie. estrogen), nitrates, PPIs
Page 37
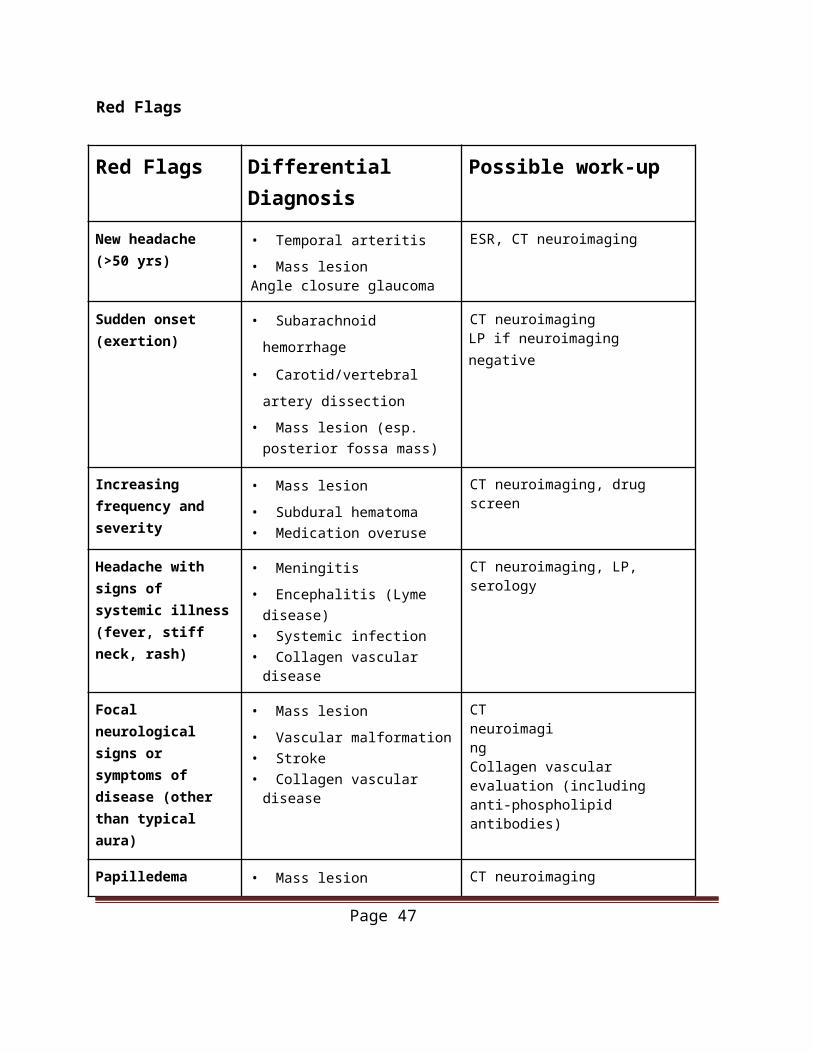
Red Flags
Red Flags Differential Diagnosis Possible work-up
New headache (>50 yrs)
• Temporal arteritis• Mass lesionAngle closure glaucoma
ESR, CT neuroimaging
Sudden onset (exertion)
• Subarachnoid hemorrhage
• Carotid/vertebral artery dissection• Mass lesion (esp. posterior fossa
mass)
CT neuroimagingLP if neuroimaging negative
Increasing frequency and severity
• Mass lesion• Subdural hematoma• Medication overuse
CT neuroimaging, drug screen
Headache with signs of systemic illness (fever, stiff neck, rash)
• Meningitis• Encephalitis (Lyme disease)• Systemic infection• Collagen vascular disease
CT neuroimaging, LP, serology
Focal neurological signs or symptoms of disease (other than typical aura)
• Mass lesion• Vascular malformation• Stroke• Collagen vascular disease
CT neuroimagingCollagen vascular evaluation (including anti-phospholipid antibodies)
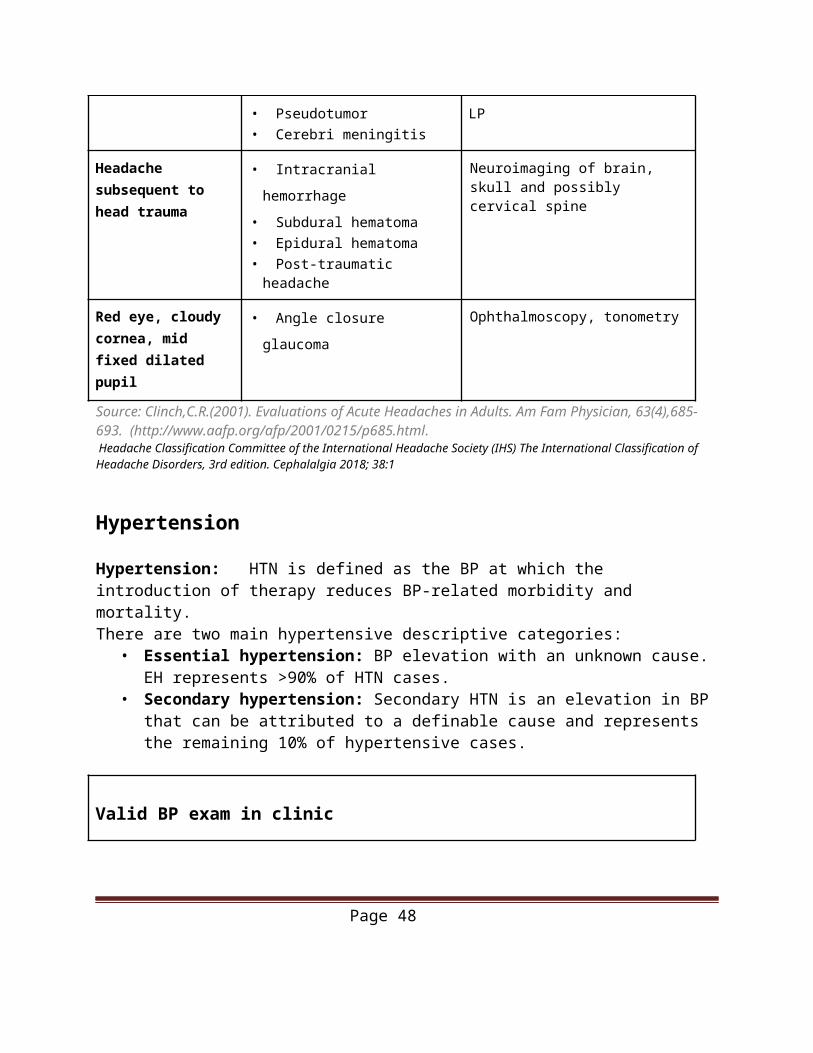
Papilledema • Mass lesion• Pseudotumor• Cerebri meningitis
CT neuroimagingLP
Headache subsequent to head trauma
• Intracranial hemorrhage• Subdural hematoma• Epidural hematoma• Post-traumatic headache
Neuroimaging of brain, skull and possibly cervical spine
Red eye, cloudy cornea, mid fixed dilated pupil
• Angle closure glaucoma Ophthalmoscopy, tonometry
Source: Clinch,C.R.(2001). Evaluations of Acute Headaches in Adults. Am Fam Physician, 63(4),685-693. (http://www.aafp.org/afp/2001/0215/p685.html. Headache Classification Committee of the International Headache Society (IHS) The International Classification of Headache Disorders, 3rd edition. Cephalalgia 2018; 38:1
Page 38
Hypertension
Hypertension: HTN is defined as the BP at which the introduction of therapy reduces BP-related morbidity and mortality. There are two main hypertensive descriptive categories:
• Essential hypertension: BP elevation with an unknown cause. EH represents >90% of HTN cases.
• Secondary hypertension: Secondary HTN is an elevation in BP that can be attributed to a definable cause and represents the remaining 10% of hypertensive cases.
Valid BP exam in clinic
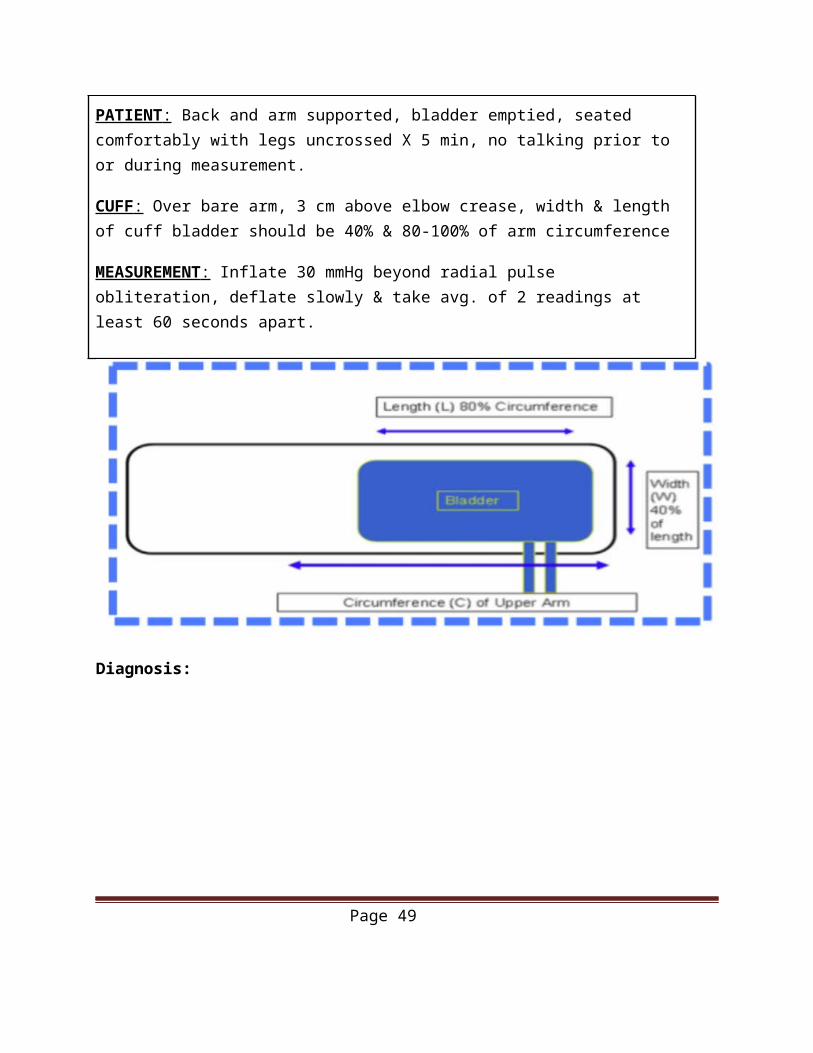
PATIENT : Back and arm supported, bladder emptied, seated comfortably with legs uncrossed X 5 min, no talking prior to or during measurement.
CUFF : Over bare arm, 3 cm above elbow crease, width & length of cuff bladder should be 40% & 80-100% of arm circumference
MEASUREMENT : Inflate 30 mmHg beyond radial pulse obliteration, deflate slowly & take avg. of 2 readings at least 60 seconds apart.
Diagnosis:
Page 39
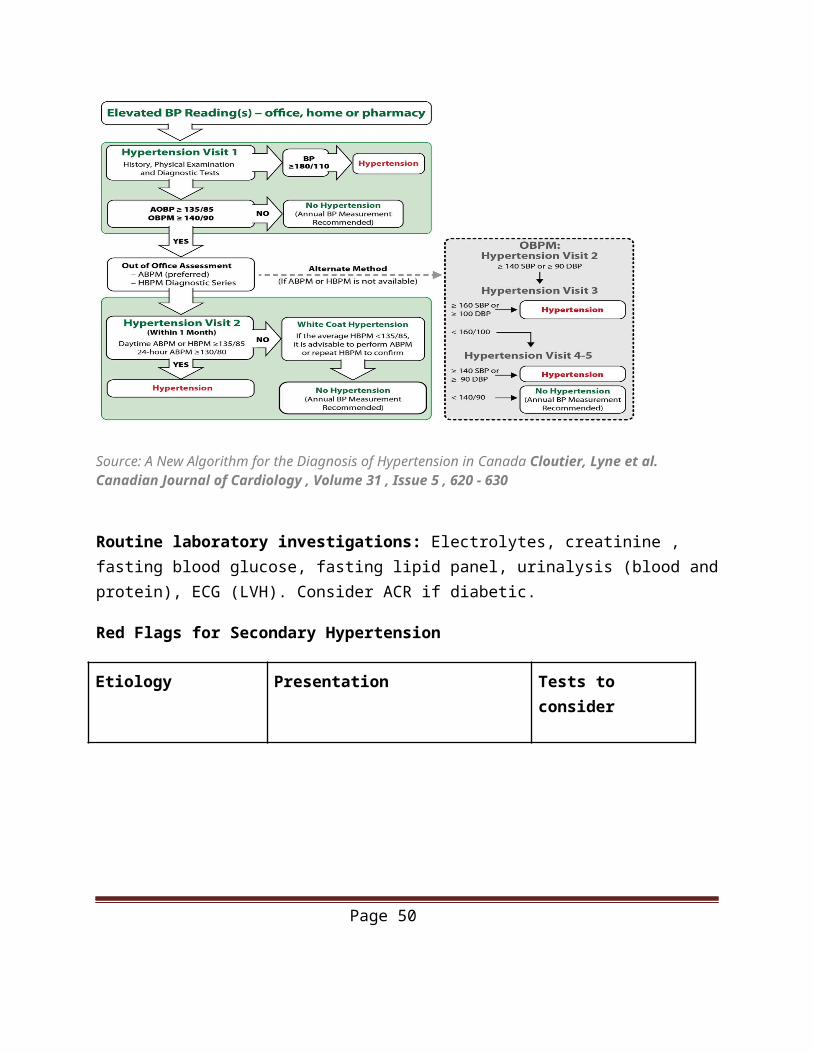
Source: A New Algorithm for the Diagnosis of Hypertension in Canada Cloutier, Lyne et al. Canadian Journal of Cardiology , Volume 31 , Issue 5 , 620 - 630
Routine laboratory investigations: Electrolytes, creatinine , fasting blood glucose, fasting lipid panel, urinalysis (blood and protein), ECG (LVH). Consider ACR if diabetic.
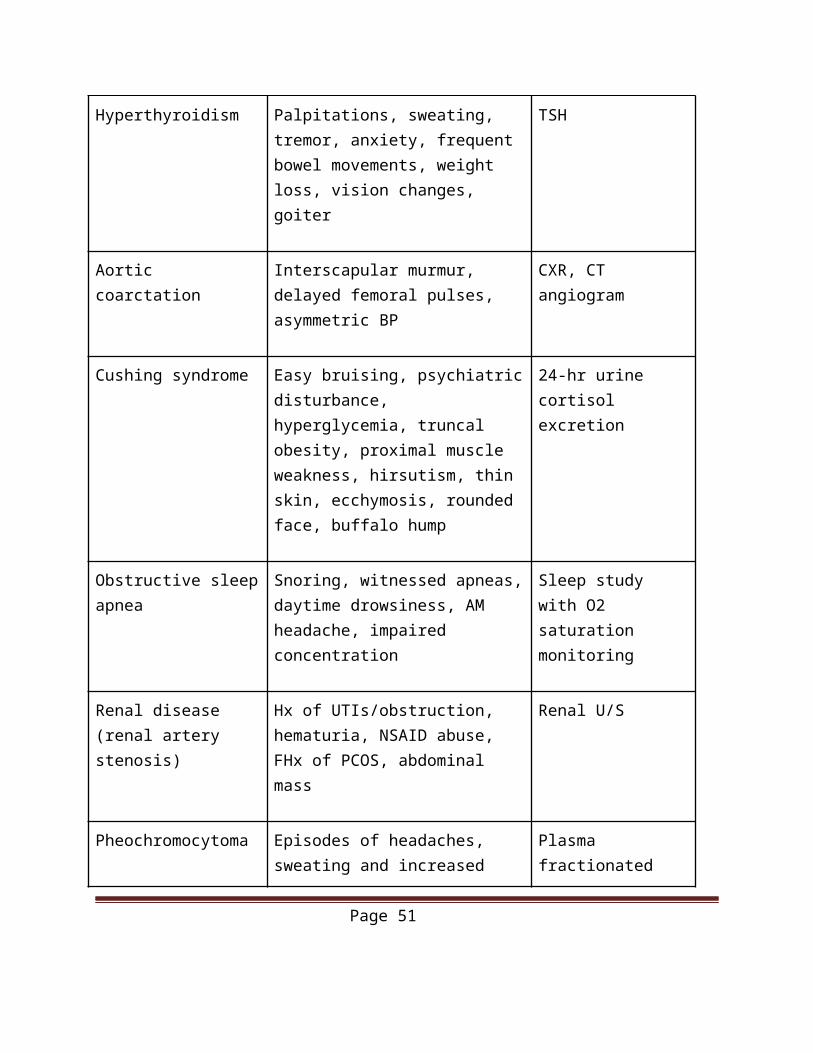
Red Flags for Secondary Hypertension
Etiology Presentation Tests to consider
Hyperthyroidism Palpitations, sweating, tremor, anxiety, frequent bowel movements, weight loss, vision changes, goiter
TSH
Aortic coarctation Interscapular murmur, delayed femoral pulses, asymmetric BP
CXR, CT angiogram
Page 40
Cushing syndrome Easy bruising, psychiatric disturbance, hyperglycemia, truncal obesity, proximal muscle weakness, hirsutism, thin skin, ecchymosis, rounded face, buffalo hump
24-hr urine cortisol excretion
Obstructive sleep apnea Snoring, witnessed apneas, daytime drowsiness, AM headache, impaired concentration
Sleep study with O2 saturation monitoring
Renal disease (renal artery stenosis)
Hx of UTIs/obstruction, hematuria, NSAID abuse, FHx of PCOS, abdominal mass
Renal U/S
Pheochromocytoma Episodes of headaches, sweating and increased heart rate
Plasma fractionated metanephrines
Meds/herbs NSAIDs, OCP, steroids, pseudoephedrine, cocaine
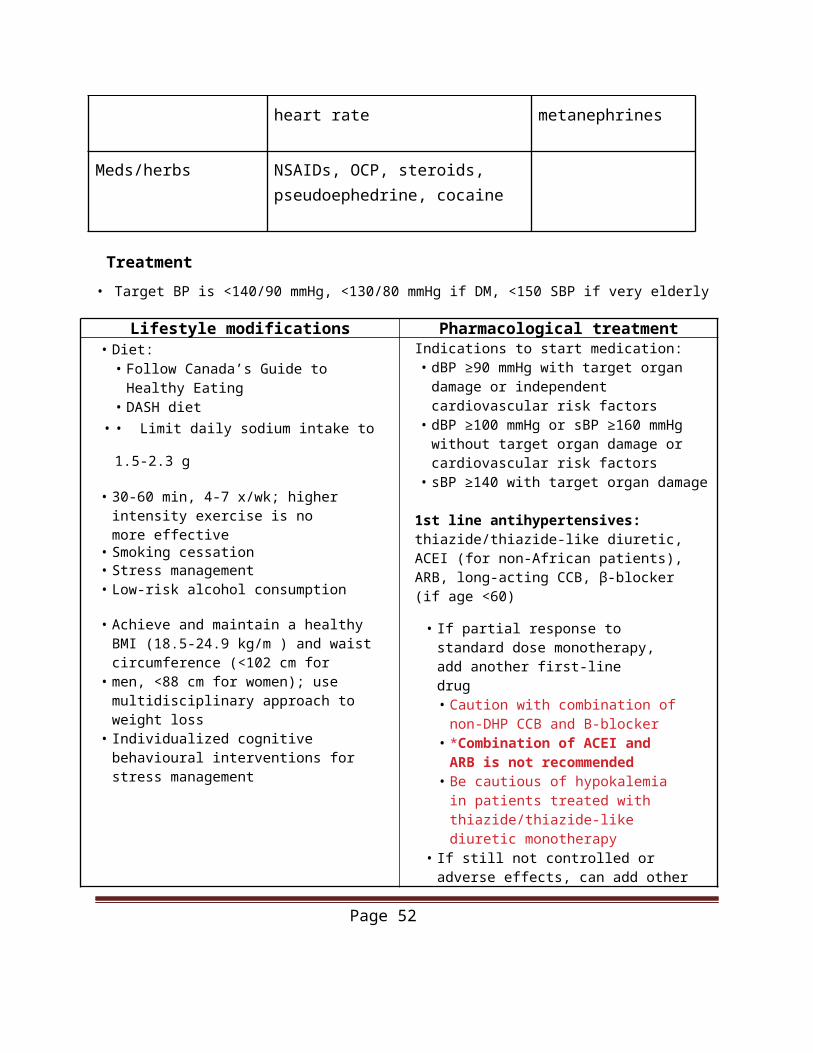
Treatment • Target BP is <140/90 mmHg, <130/80 mmHg if DM, <150 SBP if very elderly
Lifestyle modifications Pharmacological treatment• Diet:
• Follow Canada’s Guide to Healthy Eating
• DASH diet• • Limit daily sodium intake to 1.5-2.3 g
• 30-60 min, 4-7 x/wk; higher intensity exercise is no more effective
• Smoking cessation• Stress management• Low-risk alcohol consumption
• Achieve and maintain a healthy BMI (18.5-24.9 kg/m ) and waist circumference (<102 cm for
Indications to start medication:• dBP ≥90 mmHg with target organ damage
or independent cardiovascular risk factors• dBP ≥100 mmHg or sBP ≥160 mmHg
without target organ damage or cardiovascular risk factors
• sBP ≥140 with target organ damage
1st line antihypertensives: thiazide/thiazide-like diuretic, ACEI (for non-African patients), ARB, long-acting CCB, β-blocker (if age <60)
• If partial response to standard dose monotherapy, add another first-line drug
Page 41
• men, <88 cm for women); use multidisciplinary approach to weight loss
• Individualized cognitive behavioural interventions for stress management
• Caution with combination of non-DHP CCB and B-blocker
• *Combination of ACEI and ARB is not recommended
• Be cautious of hypokalemia in patients treated with thiazide/thiazide-like diuretic monotherapy
• If still not controlled or adverse effects, can add other classes of anti-hypertensives
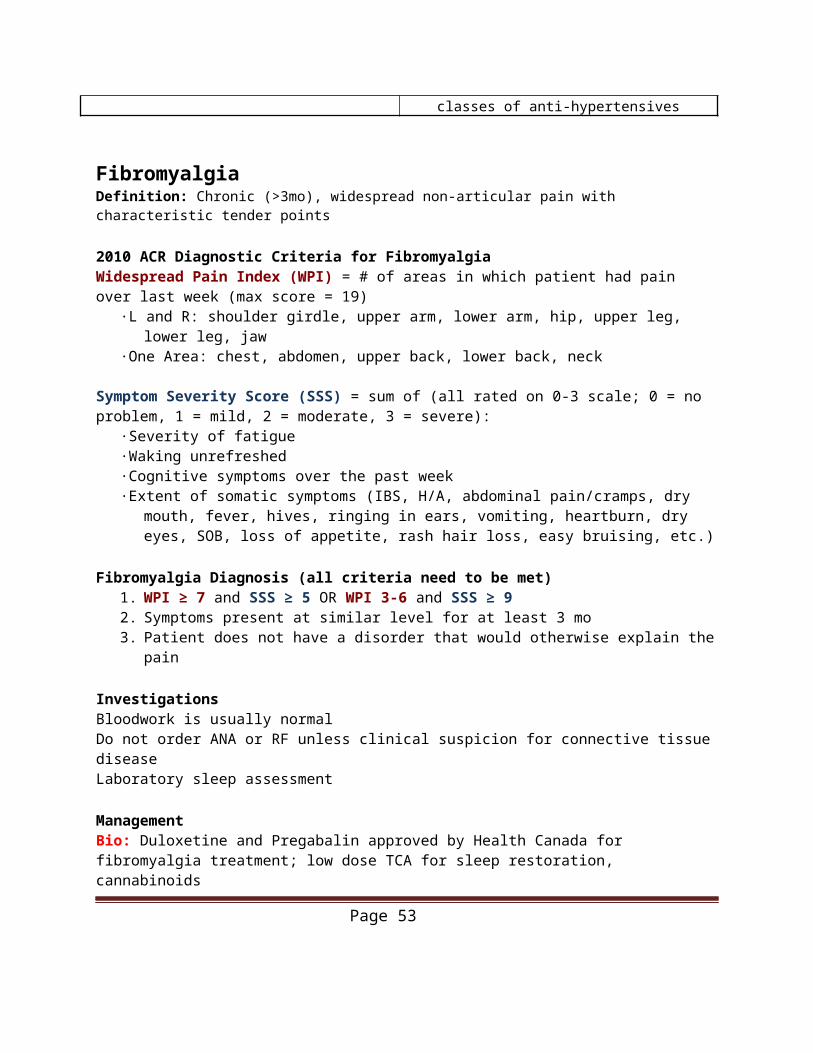
FibromyalgiaDefinition: Chronic (>3mo), widespread non-articular pain with characteristic tender points 2010 ACR Diagnostic Criteria for FibromyalgiaWidespread Pain Index (WPI) = # of areas in which patient had pain over last week (max score = 19)
·L and R: shoulder girdle, upper arm, lower arm, hip, upper leg, lower leg, jaw·One Area: chest, abdomen, upper back, lower back, neck
Symptom Severity Score (SSS) = sum of (all rated on 0-3 scale; 0 = no problem, 1 = mild, 2 = moderate, 3 = severe):
·Severity of fatigue·Waking unrefreshed·Cognitive symptoms over the past week·Extent of somatic symptoms (IBS, H/A, abdominal pain/cramps, dry mouth, fever, hives, ringing in
ears, vomiting, heartburn, dry eyes, SOB, loss of appetite, rash hair loss, easy bruising, etc.) Fibromyalgia Diagnosis (all criteria need to be met)
1. WPI ≥ 7 and SSS ≥ 5 OR WPI 3-6 and SSS ≥ 92. Symptoms present at similar level for at least 3 mo3. Patient does not have a disorder that would otherwise explain the pain
InvestigationsBloodwork is usually normalDo not order ANA or RF unless clinical suspicion for connective tissue diseaseLaboratory sleep assessment ManagementBio: Duloxetine and Pregabalin approved by Health Canada for fibromyalgia treatment; low dose TCA for sleep restoration, cannabinoidsPsycho: CBT, coping skills, stress reductionSocial: exercise program (20-30min 2-3x/week), physical therapy (posture, stretching, muscle strengthening, massage)
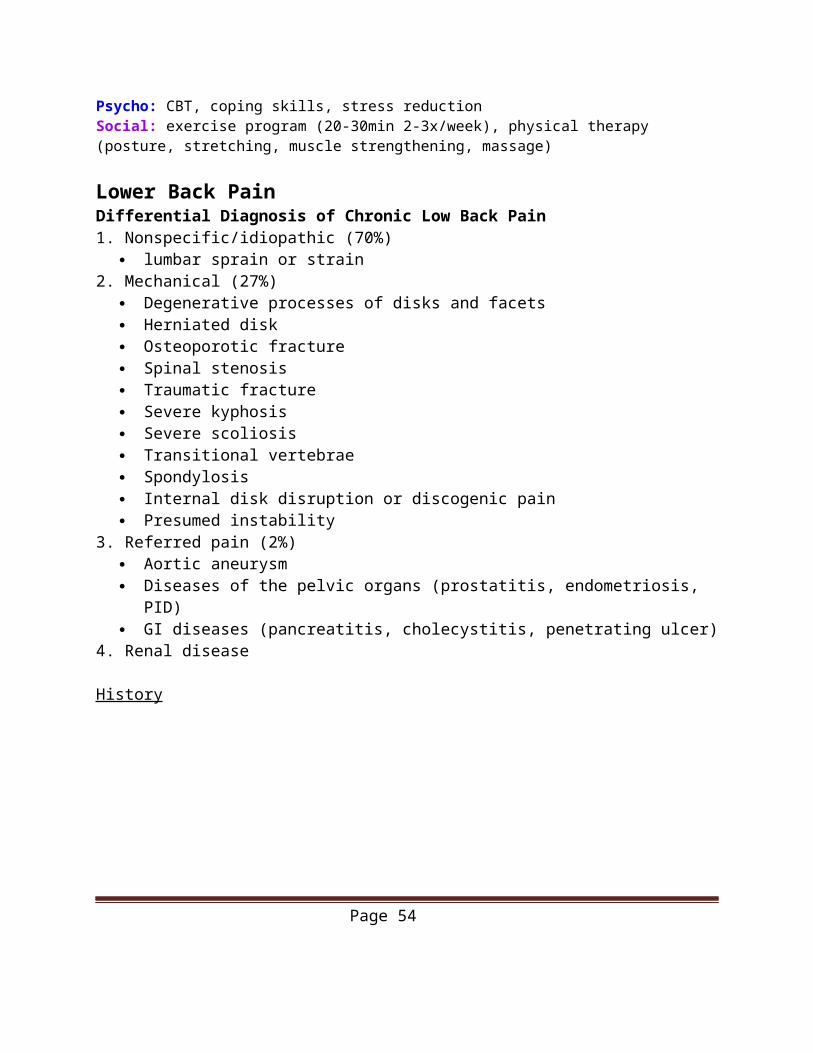
Lower Back PainDifferential Diagnosis of Chronic Low Back Pain
Page 42
1. Nonspecific/idiopathic (70%) lumbar sprain or strain
2. Mechanical (27%) Degenerative processes of disks and facets Herniated disk Osteoporotic fracture Spinal stenosis Traumatic fracture Severe kyphosis Severe scoliosis Transitional vertebrae Spondylosis Internal disk disruption or discogenic pain Presumed instability
3. Referred pain (2%) Aortic aneurysm Diseases of the pelvic organs (prostatitis, endometriosis, PID) GI diseases (pancreatitis, cholecystitis, penetrating ulcer)
4. Renal disease
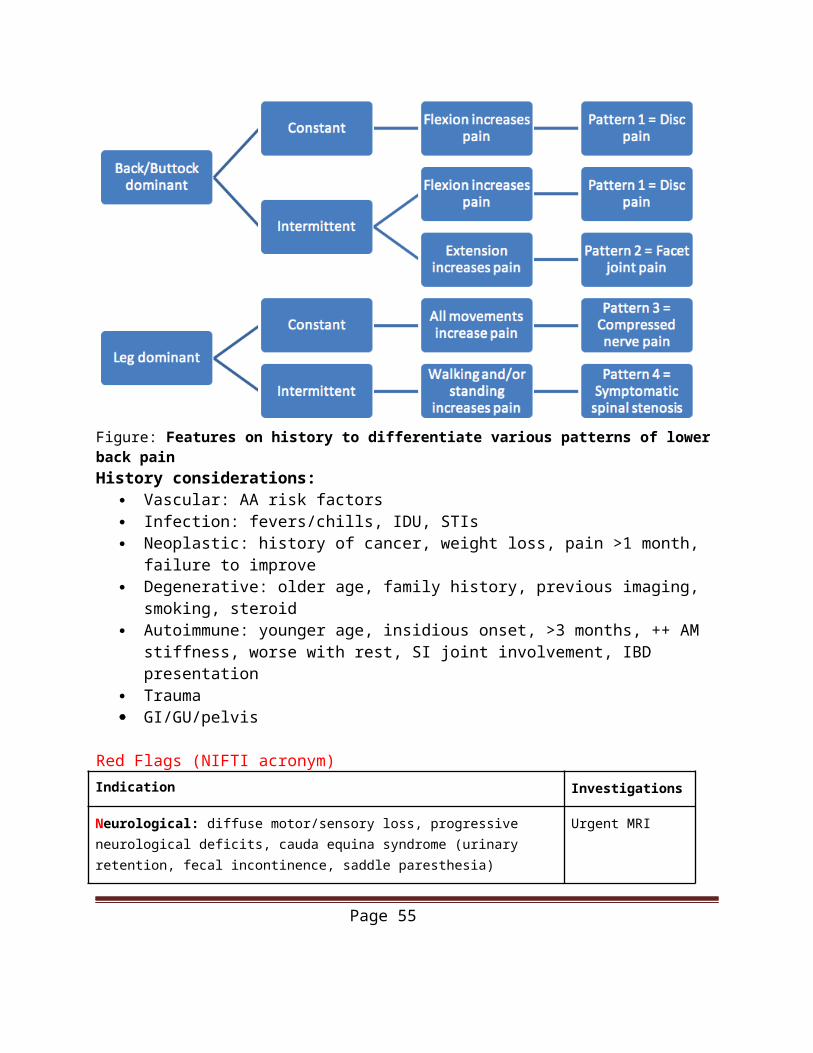
History
Figure: Features on history to differentiate various patterns of lower back painHistory considerations:
Vascular: AA risk factors Infection: fevers/chills, IDU, STIs
Page 43
Neoplastic: history of cancer, weight loss, pain >1 month, failure to improve Degenerative: older age, family history, previous imaging, smoking, steroid Autoimmune: younger age, insidious onset, >3 months, ++ AM stiffness, worse with rest,
SI joint involvement, IBD presentation Trauma GI/GU/pelvis
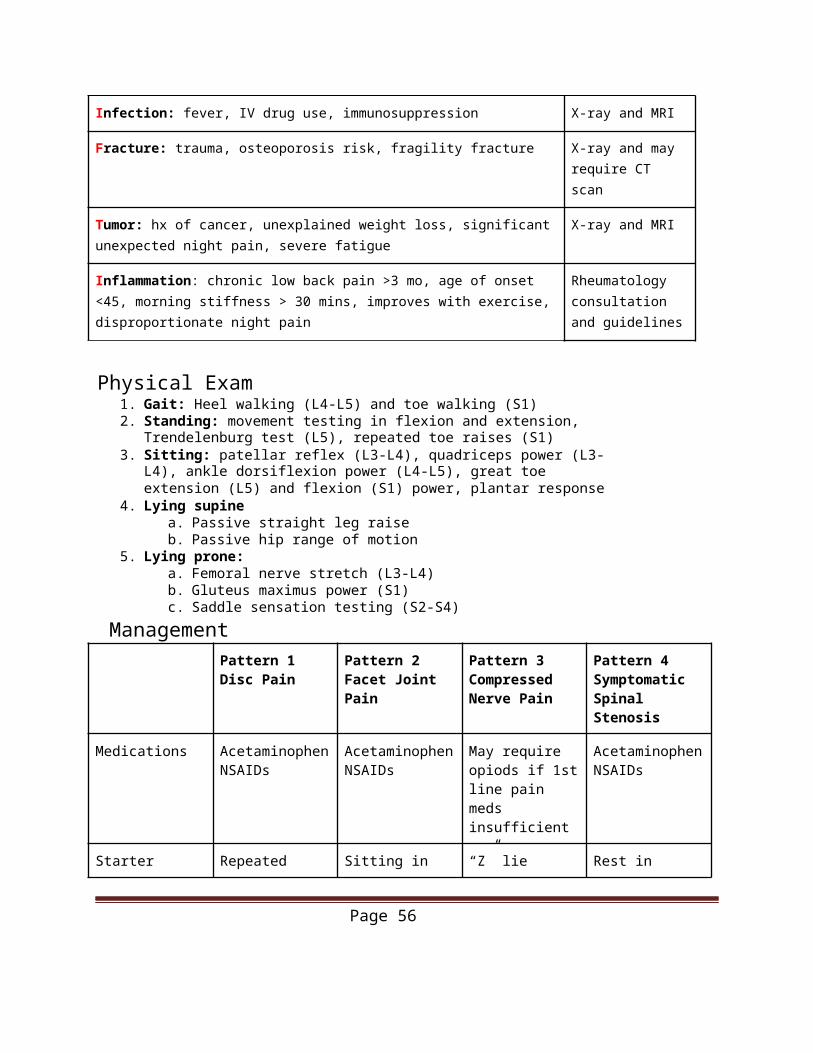
Red Flags (NIFTI acronym)Indication Investigations
Neurological: diffuse motor/sensory loss, progressive neurological deficits, cauda equina syndrome (urinary retention, fecal incontinence, saddle paresthesia)
Urgent MRI
Infection: fever, IV drug use, immunosuppression X-ray and MRI
Fracture: trauma, osteoporosis risk, fragility fracture X-ray and may require CT scan
Tumor: hx of cancer, unexplained weight loss, significant unexpected night pain, severe fatigue
X-ray and MRI
Inflammation: chronic low back pain >3 mo, age of onset <45, morning stiffness > 30 mins, improves with exercise, disproportionate night pain
Rheumatology consultation and guidelines
Physical Exam1. Gait: Heel walking (L4-L5) and toe walking (S1)2. Standing: movement testing in flexion and extension, Trendelenburg test (L5),
repeated toe raises (S1)3. Sitting: patellar reflex (L3-L4), quadriceps power (L3-L4), ankle dorsiflexion power
(L4-L5), great toe extension (L5) and flexion (S1) power, plantar response4. Lying supine
a. Passive straight leg raiseb. Passive hip range of motion
5. Lying prone:a. Femoral nerve stretch (L3-L4)b. Gluteus maximus power (S1)c. Saddle sensation testing (S2-S4)
ManagementPattern 1Disc Pain
Pattern 2Facet Joint Pain
Pattern 3Compressed Nerve Pain
Pattern 4Symptomatic Spinal Stenosis
Medications AcetaminophenNSAIDs
AcetaminophenNSAIDs
May require opiods if 1st line pain meds insufficient
AcetaminophenNSAIDs
Page 44
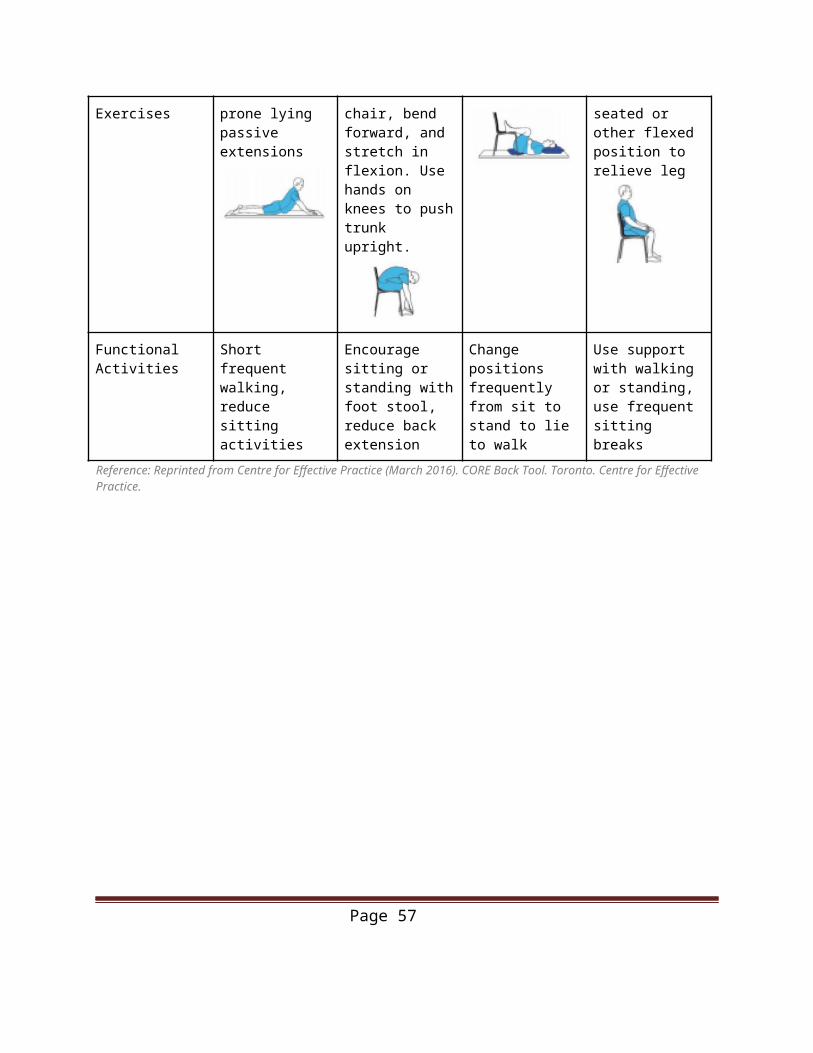
Starter Exercises Repeated prone lying passive extensions
Sitting in chair, bend forward, and stretch in flexion. Use hands on knees to push trunk upright.
“Z” lie Rest in seated or other flexed position to relieve leg
Functional Activities
Short frequent walking, reduce sitting activities
Encourage sitting or standing with foot stool, reduce back extension
Change positions frequently from sit to stand to lie to walk
Use support with walking or standing, use frequent sitting breaks
Reference: Reprinted from Centre for Effective Practice (March 2016). CORE Back Tool. Toronto. Centre for Effective Practice.
Page 45
Acute Otitis Media
Diagnosis• Acute onset of symptoms AND• One or more signs of middle ear effusion (bulging TM, limited TM mobility, air fluid levels
behind TM, or otorrhea) AND• One or more signs of middle ear inflammation (TM redness, otalgia)• Middle ear effusion (TM immobile +/- opacification, loss of bony landmarks, or ruptured TM
with fluid in external ear canal),• Middle ear inflammation (bulging/discolored TM)
TreatmentIndications for immediate antibiotic treatment:
• Age <6 months years old • Fever >38.5°C• Perforated TM with purulent drainage• Significant comorbidities (eg. immune deficiency, cardiac/pulmonary disease, anatomic• abnormalities of head & neck, Down syndrome)• current or previous complicated otitis media
Indications for 48 h observation:• age > 2 years old• reliable parents (able to recognize worsening symptoms and bring child back to clinic for f/u)• *If child worsens/fails to improve over 48 hours (from onset of symptoms), start antimicrobial• therapy
Antibiotics:• Amoxicillin 75-90mg/kg/day divided BID x 5 days (>2 y.o.) or 10 days (<2 y.o.)• IF ALLERGIC TO PENICILLIN: Clarithromycin, Azithromycin, TMP/SMX (but significant
resistance)• IF NO IMPROVEMENT AFTER 2 DAYS: Amox-clav 45-60mg/kg/day divided TID x 10
days• IF TM PERFORATION: Ciprodex 4 drops BID x 5 days
Source: Saux, N. Le, Robinson, J. L. & Society, C. P. Management of acute otitis media in children six months of age and older. Paediatr Child Heal. 21, 39–44 (2016).
Osteoarthritis Definition: Inflammatory arthritis due to articular cartilage degenerationMost common polyarthritis
Clinical Presentation Asymmetric joint pain Worsens with activity Relieved by rest
Page 46
Morning stiffness (<30 min or none) Joint swelling (d/t osteophyte & synovial fluid) Bouchards nodes (PIP) Herbender nodes (DIP)
Risk Factors Age (older) Gender (if <50 M>F, if >50 F>M) Trauma Obesity Endocrine disorders
Investigations Imaging (XRay)
o Joint space narrowingo Productive changes (subchondral sclerosis)o Subchondral cysts o Osteophytes
Note that majority of population >65 years of age have signs of OA on x-ray imaging, however only 33% of these individuals will be symptomatic.
Diagnosis Clinical
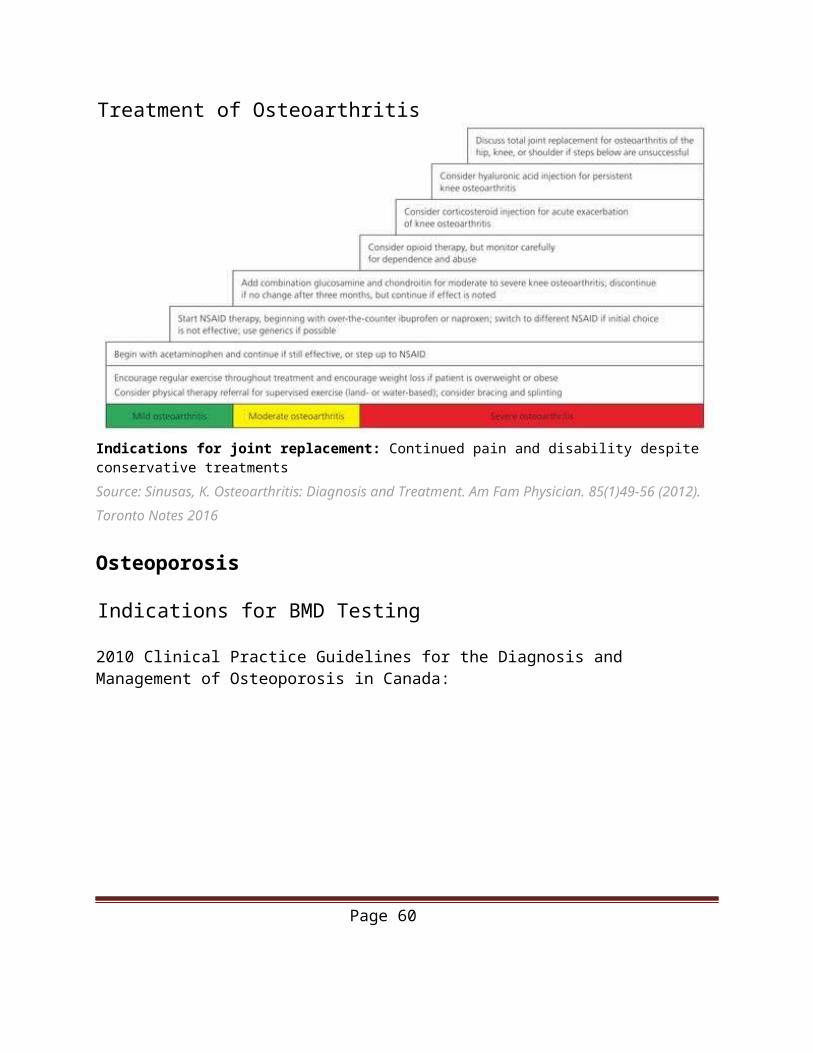
Treatment of Osteoarthritis
Indications for joint replacement: Continued pain and disability despite conservative treatmentsSource: Sinusas, K. Osteoarthritis: Diagnosis and Treatment. Am Fam Physician. 85(1)49-56 (2012).Toronto Notes 2016
Page 47
Osteoporosis
Indications for BMD Testing
2010 Clinical Practice Guidelines for the Diagnosis and Management of Osteoporosis in Canada:
Obtained from Osteoporosis Canada (www.osteoporosis.ca)
Page 48
Assessment of 10-year fracture risk: CAROC or FRAX tool
Treatment Lifestyle modifications: Elemental calcium 1000-1200 mg/d; Vit D 1000 IU/d Exercise: 3x30 min weight-bearing exercises/wk Cessation of smoking, reduce caffeine intake Stop/avoid osteoporosis-inducing medications Drug therapy Bisphosphonate RANKL inhibitors Parathyroid hormone Calcitonin (2nd line) Treatment specific to Post-Menopausal Women SERM HRT
PainNeuropathic Pain
1st Line Tricyclic Antidepressants (eg: amitriptyline), Gabapentinoids (gabapentin, pregabalin), SNRIs (venlafaxine, duloxetine)
2nd Line
Tramadol, Opioid analgesics
3rd Line Cannabinoids
4th Line Methadone, anticonvulsants with lesser activity (eg: lamotrigine, topiramate, valproic acid), tapentadol, topical lidocaine, capsaicin
Source: Canadian Pain Society Pharmacological Treatment Guidelines for Neuropathic Pain, 2017Nociceptive PainStep 1: Acetaminophen and NSAID• Acetaminophen 75mg/kg (max) daily PO in divided doses• Can reduce the need for opioids by 50%• Ibuprofen 600-2400mg daily PO in divided oses TID-QID• Naproxen 500-1000mg daily PO in divided doses BID-TID
Step 2: Tramadol, Tapentadol, low dose step 3 medications• Tramadol 25-75mg PO q4hStep 3: Hydromorphone, Morphine, Oxycodone• Hydromorphone 2mg PO q4h or 1mg SC q4h• Oxycodone 5mg PO q4h
Page 49
• Morphine 10mg PO q4h or 5mg SC q4h
Step 4: Fentanyl and extended release step 3 medications
Adjuvant Pain Medications:• NMDA Antagonist (Ketamine, Memantine)• Anti-depressants (SSRI, SNRI, TCs)• Anticonvulsants (Gabapentin, pregabalin, valproic acid)• Muscle relaxant (Cyclobenzaprine, baclofen)
Other Recommendations1
First line therapy for chronic non-cancer pain: optimize non-opioid pharmacotherapy and non-pharmacological therapy, rather than a trial of opioids
Patients with chronic non-cancer pain with an active substance use disorder and chronic non-cancer pain: avoid the use of opioids
Restrict the prescribed dose to under 90mg morphine equivalents daily rather than no upper, or a higher limit on dosing
Patients with chronic non-cancer pain using opioids and experiencing serious challenges in tapering: refer to a formal multidisciplinary opioids reduction program or use coordinated multidisciplinary collaboration (eg. primary care physician, pharmacist, physical therapist, kinesiologist, psychiatrist, and psychologist)
Sources:1McMaster National Pain Center. The 2017 Draft Recommendations for Use of Opioids in Chronic Non-Cancer Pain. DRAFT January 30, 2017. http://nationalpaincentre.mcmaster.ca/documents/Opioids%20guideline%20English_30Jan2017_correctnumbering.pdfMoulin, D. E., Clark, A. J. & Gilron, I. Pharmacological management of chronic neuropathic pain – Consensus statement and guidelines from the Canadian Pain Society. 12, 13–21 (2007).Rosenquist, EWK. Overview of the treatment of chronic pain. Retrieved from http://www.uptodate. com/ contents/overview of-the-treatment-ofchronic-pain?source=search_result&search=chronic+pain&sele ctedTitle=1%7E150)Sullivan P. Ottawa Anesthesia Primer. 1st ed. Echo book Publishing; 2013.
Anxiety
DSM-V Anxiety Disorders:• Separation Anxiety Disorder• Selective Mutism• Specific Phobia• Social Anxiety Disorder (Social Phobia)• Panic Disorder
Page 50
• Agoraphobia• Generalized Anxiety Disorder• Substance/Medication Induced Anxiety Disorder• Anxiety Disorder due to another Medical Condition• Unspecified Anxiety Disorder
DSM-V Criteria for Generalized Anxiety Disorder• Excessive anxiety and worry most days >/=6 months about a number of events or activities• Worry is difficult to control• Anxiety/worry associated with at least 3/6 symptoms: restlessness, fatigue, difficulty concentrating, irritability,
muscle tension, insomnia
GAD Pharmacological Treatment
VEN venlafaxine, PRE pregabalin, GAB gabapentin, PHE phenelzine, BUS buspirone, QUE quetiapine, PIN pindolol, AC anticonvulsants, AD antidepressant AAP atypical antipsychotics
Page 51
1st line 2nd line 3rd line Adjunct
Panic disorder
SSRI, VEN BDZ, TCA, other AD
MAOI, other AD, AC, AAP
BDZ, AC, AAP, PIN
Social Anxiety Disorder
SSRI, VEN, PRE
BDZ, GAB, PHE
Other AD, AC BUS, AAP
Generalized Anxiety Disorder
SSRI, SNRI, PRE
BDZ, BUS, other AD, QUE
Other AD, AC PRE, AAP
Source: Stein MB, Craske MG. Treating Anxiety in 2017Optimizing Care to Improve Outcomes. JAMA.2017;318(3):235–236. doi:10.1001/jama.2017.6996
DepressionDSM-V Criteria for Major Depressive Disorder
● 2 weeks including depressed mood OR anhedonia with functional impairment AND● Associated with 5/9 symptoms: mood (depressed), sleep (insomnia or hypersomnia), interest
(anhedonia), guilt/worthlessness, energy (decreased), concentration (decreased), appetite changes, psychomotor agitation or retardation, suicidal ideation
First-line SSRI, SNRI, NDRI, NaSSA, RIMAex. Escitalopram (Cipralex) 10mg PO daily, Venlafaxine (Effexor)75mg PO daily
Second-line TCA (Nortriptyline), SARI (Trazodone), Seroquel-XR
Third-line MAOI (Phenelzine)
Page 52
Adjunctive therapy Lithium - 600 mg daily up to therapeutic serum level Aripiprazole (Abilify) 1-2 mg up to 10 mg Olanzapine (Zyprexa) 2.5-5 mg up to 7.5 mg qhs Risperidone (Risperdal) 0.5-1 mg up to 1.5 mg qhs
PsychiatryCommon Psychiatric Medication Side Effects
Medication Class Side Effects
SSRI HANDS: Headache, anxiety, agitation, nausea, diarrhea, sexual dysfunction, sleep disturbances
SNRI Same as SSRI (HANDS) plus increased BP
NDRI Headache, rash, sleep disturbance (insomnia), shaking, anxiety, agitation, emesis, seizures (0.1% over 400mg)
NaSSA Weight gain, increased cholesterol, anti-cholinergic (urinary retention, dry mouth, constipation, blurred vision), drowsiness, orthostatic hypotension
Trazodone Sedation, vivid dreams, headache, dry mouth, priapism (1/6000)
TCA Weight gain, sedation, anti-cholinergic, dizziness, orthostatic hypotension, QTc prolongation
MAOI Orthostatic hypotension, weight gain, sexual dysfunction, ankle edema
Lithium Tremor, alopecia, GI upset, acne, weight gain, hypothyroid, muscle weakness, ECG changes
Sources:Katzman, M. A. et al. Canadian clinical practice guidelines for the management of anxiety, posttraumatic stress and obsessive-compulsive disorders. BMC Psychiatry 14, S1–S1 (2014).American Psychiatric Association. (2013). Major Depressive Disorder. In Diagnostic and statistical manual of mental disorders (5th ed.).Canadian Network for Mood and Anxiety Treatments. Clinical Guidelines for the Management of Major Depressive Disorder in Adults. Retrieved from http://www.canmat.org/resources/CANMAT%20Depression%20Guidelines%202009.pdfAmerican Psychiatric Association. (2013). Generalized Anxiety Disorder. In Diagnostic and statistical manual of mental disorders (5th ed.).
Page 53
Canadian Psychiatry Association. Clinical Practice Guidelines – Management of Anxiety Disorders – Updated 2006. Retrieved from http://publications.cpa-apc.org/media.php?mid=445
Skin ConditionsAcneOptimizing topical Abx therapy (Tetracycline, Doxycycline, Erythromycin, Minocycline) with use of:
• topical retinoids: ↑ efficacy• benzoyl peroxide: ↓ resistance
Other treatment options:• Hormonal contraceptives:• treatment of inflammatory and non-inflammatory acne in women• Spironolactone:• consider as an alternative in women who cannot use isotretinoin. Potential teratogen
Source: Titus, S. & Hodge, J. Diagnosis and Treatment of Acne. Am. Fam. Physician 86, 734–740 (2012). Eczema (Atopic Dermatitis)
Clinical Presentation:
Page 54
Subacute and chronic eczematous reaction associated with prolonged severe pruritus Distribution depends on age. Infants and young children (zero to two years): pruritic, red, scaly, and crusted lesions on
the extensor surfaces and cheeks or scalp. Usually sparing of the diaper area In older children and adolescents (2 to 16 years): less exudation and often demonstrates
lichenified plaques in a flexural distribution, especially of the antecubital and popliteal fossae, volar aspect of the wrists, ankles, and neck (picture
In adults: atopic dermatitis is considerably more localized and lichenified. The areas involved are in most cases the skin flexures
Inflammation, lichenification, excoriations are secondary to relentless scratching Atopic palms: hyperlinearity of the palms (associated with ichthyosis vulgaris)
Associated with: keratosis pillars (hyperkeratosis of hair follicles, “chicken skin”), xerosis, occupational hand dryness
Treatment Algorithm
Source: Adapted from: Ellis C, et al. ICCAD II Faculty. International Consensus Conference on Atopic Dermatitis II (ICCAD II): clinical update and current treatment strategies. Br J Dermatol 2003;148(Suppl 63):3-10
Page 55
Actinic Keratosis (Solar Keratosis)Pre-malignant, common with increasing age. Risk of transformation from AK to SCC (~1/1000) but higher risk if AK is persistent
Clinical Presentation• Ill-defined, scaly erythematous papules or plaques• Commonly found in areas of sun exposure (face, ears, scalp if bald, neck, sun-exposed limbs)• Sandpaper-like, gritty sensation. Easy to appreciate on palpation rather than inspection
InvestigationsBiopsy if resistant to treatment
Management• Destructive: cryotherapy, electrodessication and curettage• Pharmacotherapy: 5-FU cream for 2-3 weeks, Imiquimod cream for 8-10 weeks,
photodynamic therapy• Excision
Basal Cell CarcinomaNon-melanoma skin cancer. Most common malignancy in humans.
Clinical Presentation• noduloulcerative (typical)
• skin-coloured papule/nodule with rolled, translucent (“pearly”) telangiectatic border and depressed/eroded/ulcerated centre.
• pigmented variant• flecks of pigment in translucent lesion with surface telangiectasia• may mimic MM
• superficial variant• flat, tan to red-brown plaque, often with scaly, pearly border and fine telangiectasia at
margin• least aggressive subtype
• sclerosing (morpheaform) variant• flesh/yellowish-coloured, shiny papule/plaque with indistinct borders, indurated
Investigations Biopsy
Management• Imiquimod 5% cream or cryotherapy is indicated for superficial BCCs on the trunk• Shave excision+electrodessication and curettage for most types of BCCs, not
including morpheaform
Page 56
• Mohs surgery• Radiotherapy in advised cases• Vismodegib for metastatic BCC• Life-long follow-up• 95% cure rate if lesion <2cm in diameter or if treated early
Squamous Cell Carcinoma
Non-melanoma skin cancer. Second most common cutaneous neoplasm.
Clinical Presentation• indurated erythematous nodule/plaque with surface scale/crust ± ulceration• more rapid enlargement than BCC• Commonly found on face, ears, scalp, forearms, and dorsum of hands
InvestigationsBiopsy
Management• surgical excision with primary closure, skin flaps or grafting• Mohs surgery• lifelong follow-up (more aggressive treatment than BCC)
Red Eye
History Symptoms Signs Treatment
Allergic Atopy or allergies Itching, rhinitis Bilateral watery eyes, papillae
Cool compression, oral/ topical antihistamine, artificial tears
Bacterial Conjunctivitis Burning, tearing, foreign body sensation, mild photophobia, blurry vision
Purulent discharge, papillae, “may progress to periorbital cellulitis”
Topical antibiotic x1 week
Page 57
History Symptoms Signs Treatment
Gonococcal/ Chlamydia
Sexual contact, possible vertical transmission in neonates
Chronic, unilateral conjunctivitis not responsive to drops. Tearing, foreign body sensation. LUTS+new sexual partner
Mucoid discharge. Follicles
Treat for both gonococcal and chlamydial infection. Ceftriaxone=1g IM once AND azithromycin 1g PO +/- topical abc. Ophthalmology referral
Viral (adenovirus
most common)
Sick contact Recent URTI, burning, itching, foreign body sensation. Mild photophobia. Typically affects one eye first, with spread to other eye after a few days
Clear mucoid discharge. Follicles. Tender pre-auricular lymphadenopathy
Self-limiting (resolves in 2-3 weeks). Contagious forweeks after sx onset. Cold warm compresses. Artificial tears. Proper hand hygiene
Herpes Simplex Keratitis
May be triggered by stress, fever, sun exposure, immunosuppression
Pain, tearing, foreign body sensation, red eye, +/- decreased vision, eyelid edema
Dendritic lesion in epithelium that stains with fluorescein;Corneal hypoesthesia
Topical antiviral such as trifluridine, consider systemic such as acyclovir;No steroids;Ophthalmology referral for possible dendritic debridement
Red Flags for Urgent Ophthalmology Referral:• Decreased visual acuity (infectious keratitis, iritis, angle closure glaucoma) or sudden painless vision loss
(CRAO)• Ciliary flush (infectious keratitis, iritis, angle closure glaucoma)• Photophobia (infectious keratitis, iritis)• Corneal Opacity (infectious keratitis)• Fixed Pupil (angle closure glaucoma)• Severe headache with nausea (angle closure glaucoma)
Page 58
• Trauma: lid/globe locations and intraocular foreign body, chemical burn• Gonococcal conjunctivitis• Orbital cellulitis• Temporal arteritis• Absent red reflex (white reflex, leukocoria) - r/o retinoblastoma• CN III palsy with dilated pupil (IC aneurism or neoplasm)• Proptosis (r/o cavernous sinus fistula or thrombosis)
Common Lids and Lashes Conditions
Condition Hordeolum (Stye) Chalazion Blepharitis Xanthelasma
Definition and manifestation
Definition: acute inflammation of eyelid gland, usually caused by infection (S. aureus)Manifestation: painful, red swelling of a lid
Definition: chronic granulomatous inflammation of Meibomian gland often preceded by an internal hordeolum
Manifestation: Usually no acute inflammatory signs
Inflammation of lid margins.
Two main types:
1. S. aureus: ulcerative, dry scales
2. Seborrheic: no ulcers, greasy scales
Manifestation: itching, tearing, foreign body sensation; thickened, red lid margins, crusting, “toothpaste sign” (discharge with pressure on lids)
Definition: eyelid xanthoma (lipid deposits in dermis of lids).
Manifestation: pale, slightly elevated yellowish plaques or streaks, most commonly in the medial upper lids, often bilateral.
Associated with hyperlipidemia.
Common in elderly, concerning in young
Treatment Warm compress,· Gentle massage· Topical antibiotic (erythromycin ointment bid)· Usually resolves in 2-5 days
Warm compressIf no improvement in 1 mo, consider incision and curettage. If chronic recurrent – biopsy to r/o malignancy
Warm compresses and lid scrubs with diluted baby shampoo Topical or systemic antibiotics PRN If severe – ophthalmologist may prescribe short term corticosteroid
Excision for cosmesis only
Commonly recur
Sources:
Page 59
Anti-infective Review Panel. Anti-infective Guidelines for Community Acquired Infections. Toronto: MUMS Guideline. Clearinghouse; 2013.Dash M, Arnold A. Guide to the Canadian Family Medicine Examination. New York, NY: McGraw- Hill Education; 2013.Jacobs, DS. Conjunctivitis. Uptodate. Retrieved from http://www.uptodate.com/contents/ conjunctivitis?source=search_result&search=conjunctivitis&selectedTitle=1 7E150. Accessed June 2, 2014 Longo DL, Fauci AS, Kasper DL, Hauser SL, Jameson JL, Loscalzo J, eds. Harrison’s Principles of Internal Medicine. 18th ed. New York, NY: The McGraw- Hill Companies; 2012.
Problems in the ElderlyElder Abuse WHO definition: Single or repeated act or lack of appropriate action, occurring in any relationship where there is an expectation of trust that causes harm or distress to an older person
Type of Abuse Physical Emotional Financial Neglect
Screening for Elder Abuse Conflicting evidence if should screen for elderly abuse no uniformly accepted minimum standard of care making it difficult to say when screening becomes
positive can use elder abuse suspicion index (EASI) other resources
o ONPEAo Seniors Health Research Transfer Network (SHRTN)o Canadian Network for the Prevention of Elder Abuse (CNPEA)o National initiative for care of the elderly (NICE)o Brief Abuse Screen for the Elderly (BASE) o Conflict Tactics Scale (CTS)
Suspicion Index (EASI)
Screening Tool: Validated screening tool for elder abuse for use by family practitioners in ambulatory, cognitively intact elderly patients.
Within the last 12 months:1. Have you relied on people for any of the following: bathing, dressing, shopping, banking, or meals?
Yes No Did not answer
2. Has anyone prevented you from getting food, clothes, medication, glasses, hearing aids or medical care, or from being with people you wanted to be with?
Page 60
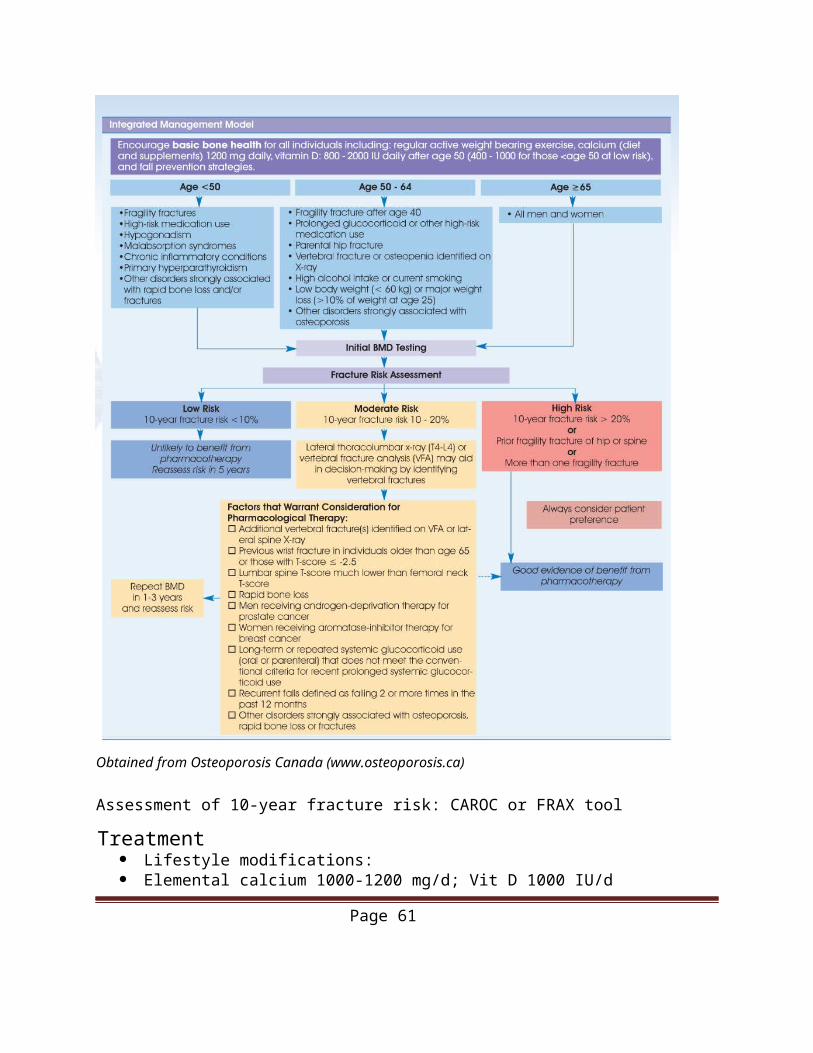
Yes No Did not answer
3. Have you been upset because someone talked to you in a way that made you feel shamed or threatened?
Yes No Did not answer
4. Has anyone tried to force you to sign papers or to use your money against your will? Yes No Did not answer
5. Has anyone made you afraid, touched you in ways that you did not want, or hurt you physically? Yes No Did not answer
6. Doctor: elder abuse may be associated with findings such as: poor eye contact, withdrawn nature, malnourishment, hygiene issues, cuts, bruises, inappropriate clothing, or medication compliance issues. did you notice any of these today or in the last 12 months?
Yes No Did not answer
“Yes” to ≥1 of Q2-Q6 establishes concern for elder abuse
Sources:Ya e MJ, Wolfson C, Lithwick M, Weiss D. Development and validation of a tool to improve physician identification of elder abuse: The Elder Abuse Suspicion Index (EASI) ©. Journal of Elder Abuse and Neglect 2008; 20(3) 276-300. Haworth Press Inc: http://www.tandf.co.uk/journals/haworth-journals.asp© The Elder Abuse Suspicion Index (EASI) was granted copyright by the Canadian Intellectual Property Office (Industry Canada) February 21, 2006. (Registration No. 1036459)World Health Organization. The Toronto declaration on the global prevention of elder abuse. Geneva, Switz: World Health Organization;2002.Yaffe, Mark J., and Bachir Tazkarji. "Understanding elder abuse in family practice." Canadian Family Physician 58, no. 12 (December 2012): 1336-340. Assessment & Management of Falls
Falls are common among older people and can have devastating consequences.
Key Points from CMAJ Review 2014 A targeted history and physical examination, covering potential home hazards, cognitive and visual impairment, functional limitations, medications, orthostatic hypotension, and gait and balance abnormalities, can be used to identify risk factors for falls. No specific assessment tools have been shown to accurately predict the risk of falls. Numerous interventions (single and multicomponent) have been shown to decrease the risk of falls. At a minimum, patients who have experienced a fall should be encouraged to participate in an approved exercise program to help prevent further falls
Page 61
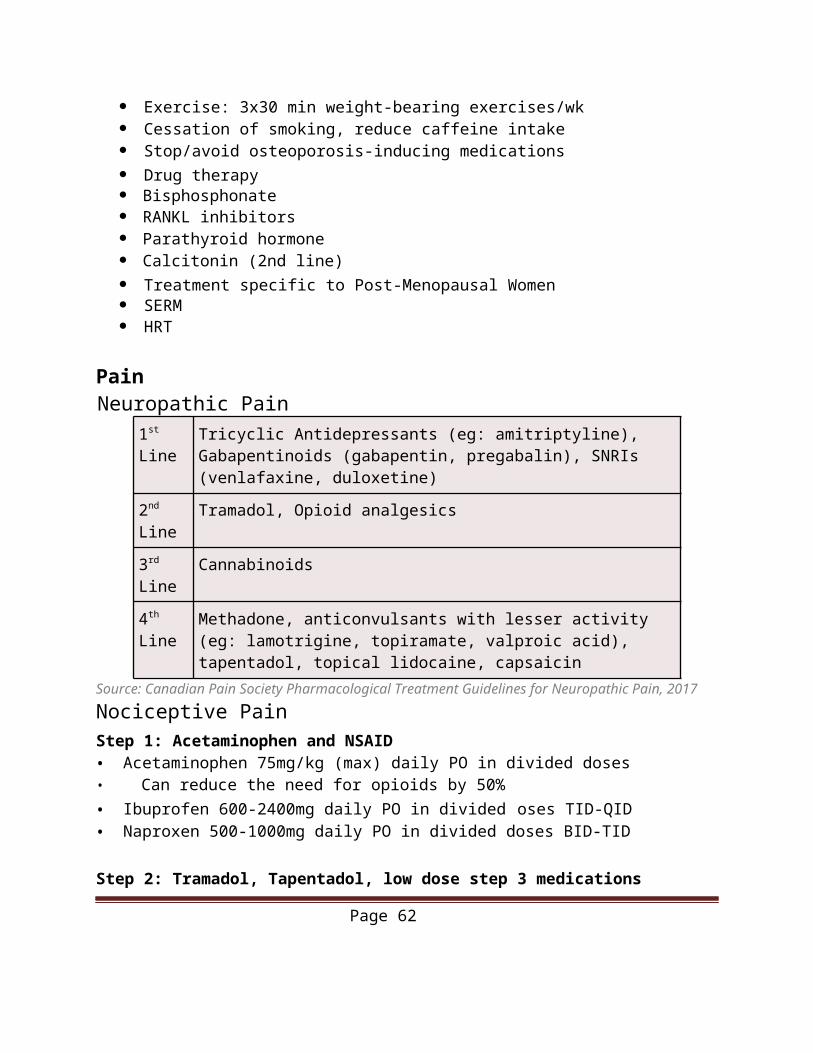
Pocket Reference obtained from: Lee, Aimee; Lee, Kuo-Wei;and Khang. Peter (2013). Preventing Falls in the Geriatric Population. Perm J; 17(4): 37-39.*Note: Timed up & go test has conflicting evidence as accurate assessment tool for risk of future falls
Page 62
Sources:Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society (2010). Summary of the Updated American Geriatrics Society/British Geriatrics Society Clinical Practice Guideline for Prevention of Falls in Older Persons. J Am Geriatr Soc (2010). DOI: 10.1111/j.1532-5415.2010.03234.x (http://www.americangeriatrics.org/files/documents/ health_care_pros/ JAGS.Falls.Guidelines.pdf)Can also refer to Panel on Prevention of Falls in Older Persons, American Geriatrics Society and British Geriatrics Society (2010). Summary of the Updated American Geriatrics Society/British Geriatrics Society Clinical Practice Guideline for Prevention of Falls in Older Persons. J Am Geriatr Soc (2010). DOI:
Page 63
10.1111/j.1532-5415.2010.03234.x (http://www.americangeriatrics.org/files/document health_care_pros/
DementiaCanadian Task Force on Preventive Health Care (2015) Key Points:• No randomized trials have evaluated the benefits of screening for cognitive impairment. • Available data suggest that pharmacologic treatments are not effective in people with mild cognitive impairment and that nonpharmacologic therapies (e.g., exercise, cognitive training and rehabilitation) produce only small benefits, which do not appear to be clinically significant.• Existing studies suggest that about 1 in 10 people without cognitive impairment may erroneously screen positive for mild cognitive impairment using the Mini-Mental State Examination and that 1 in 4 people may incorrectly be classified as positive using the Montreal Cognitive Assessment tool. • The task force recommendation against screening asymptomatic adults 65 years of age and older for cognitive impairment is based on the lack of high-quality studies evaluating the benefits and harms of screening for cognitive impairment, on evidence showing that treatment of mild cognitive impairment does not produce clinically meaningful benefit and on the potentially high rate of false-positive screens that may occur. • The strong recommendation against screening asymptomatic adults 65 years of age and older for cognitive impairment implies that the task force is confident that most individuals will be best served by the recommended course of action. • Practitioners should consider cognitive assessment for patients with signs and symptoms of impairment or when family members or patients express concerns about potential cognitive decline.
Source: Pottie, Kevin, et al. Canadian Task Force “Recommendations on screening for cognitive impairment in older adults." Canadian Medical Association Journal (2015): cmaj-141165.
Comparison of types of Dementia
Type Features
Alzheimer’s Disease (AD)
- Insidious onset, gradual progression- Decreased short term memory (encoding deficit, will notrespond to cues)- Word finding and way finding difficulties- Limited insight
Vascular Dementia (VD)
- Presence of vascular risk factors OR established arterial disease OR neuroimaging evidence- Memory loss (recall deficit, responsive to cues)- Executive skills deficits- Early apraxia and agnosia- Depression, apathy
Lewy Body Dementia (LBD)
- Fluctuating presentation- Visual hallucination, parkinsonism, REM sleep behaviourdisorder
Page 64
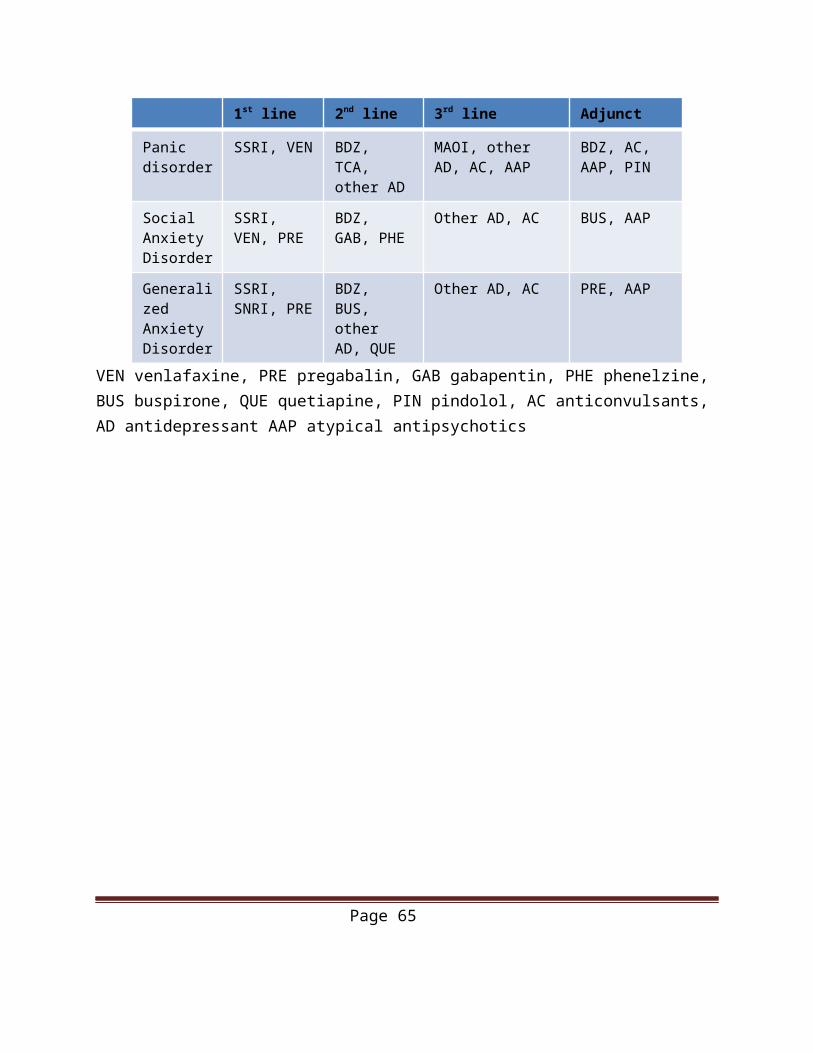
Frontal Temporal Dementia (FTD)
- Early onset (45-64)- Personality change, disinhibition, executive skills deficits- Memory and visualspcial skills presented early
Management“Dr. Dalziel’s Triple Therapy”
1. Prevent the Preventable (as applicable)● Lifestyle changes; improve sensory deficits
2. Treat the Treatable● Mild – moderate AD: Any of the 3 cholinesterase inhibitors (Donezepil, Galantamine, Rivastigmine)● Moderate-severe AD: Memantine (NMDA Antagonist)● VD: Donepezil● Mixed dementia (AD + VD): Galantamine
3. Care for the Caregivers● Referral to Alzheimer’s society● Recognize and address caregiver burden/stress/depression
Sources:Huntington, Kate. “Clerkship Overview of Geriatric Psychiatry.” Powerpoint presentation. Chun, Soojin. “Neurocognitive Disorders (Dementia).” Psychiatry Clerkship Bootcamp. 2016.Powerpoint presentation.
Page 65
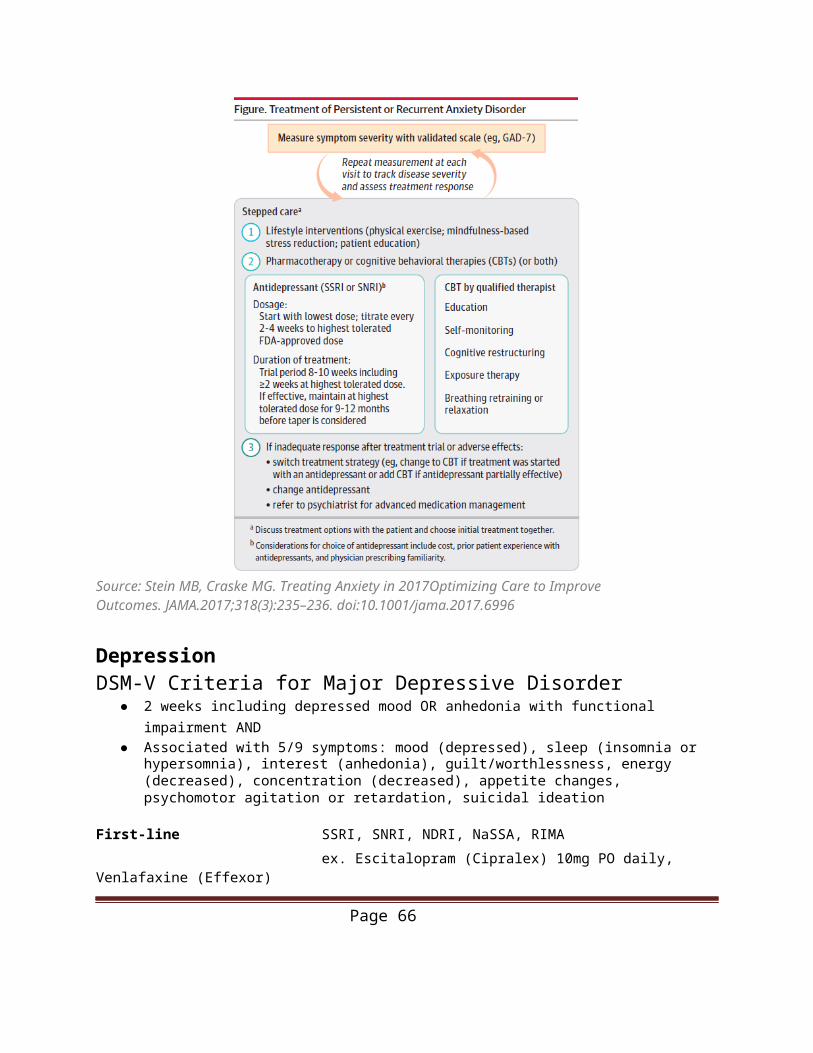
Pseudodementia
Pseudodementia: a term used to describe dementia-like features seen in depressed elderly patients. The underlying cause of the cognitive change is depression, not dementia.
Dementia Depression
Onset Insidious Subacute
Mood Labile Consistently depressed
Mood reactivity (able to enjoy things)
Yes No
Mood or cognition affected first
Cognition affected first Mood affected first
Cooperative Yes No
Aphasia Yes No
History of depression No Yes
Note there is some evidence suggesting that pseudodementia is possibly a prodrome or risk factor for the development of dementia.
Source: National Guidelines for Seniors’ Mental Health. The Assessment and Treatment of Depression. (2006)Kennedy, James. "Depressive pseudodementia–how ‘pseudo’is it really?." Old Age Psychiatrist 62 (2015): 30-37.
Page 66
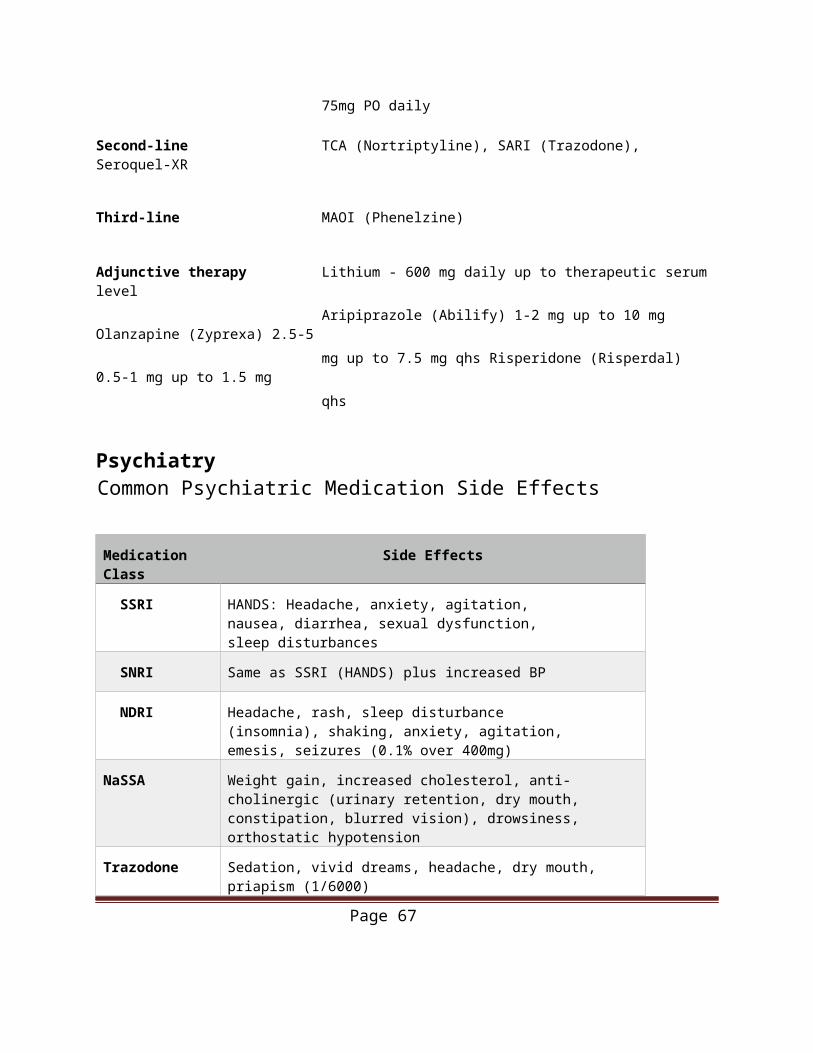
Primary Care PediatricsWell Child Visits
● Follow the Rourke Baby Record from 0-5 years.● Includes information on normal growth and development, nutrition, anticipatory guidance
regarding safety and common complaints, suggested physical examination and incorporates the Immunization Schedule recommended by the National Advisory Committee on Immunization.
● Timing of visits:o Within 1 weeko 2 weeks (optional visit)o 1 montho 2 monthso 4 monthso 6 monthso 9 months (optional visit)o 12-13 monthso 15 months (optional visit)o 18 monthso 2-3 yearso 4-5 years
● Visits are recommended every 1-2 years from ages 6-17.● For well-child visits of older children and adolescents, the Greig Health Record can be
used to guide visits.● The Greig is formatted similarly to the Rourke, and includes age-specific additional
information on psychosocial issues and education regarding safety, injury prevention, and family issues.
● Additional resources are provided that can be● There are three Greig Health Record forms available, for ages 6-9, 10-13, and 14-17.
Greig, A., Constantin, E., Carsley, S., & Cummings, C. (2010). Preventive health care visits for children and adolescents aged six to 17 years: The Greig Health Record–Executive Summary. Paediatrics & child health, 15(3), 157. (http://www.cps.ca/uploads/tools/Greig-Executive-Summary.pdf) linkRourke, L., Leduc, D., & Rourke J. (last updated 20-02-2014). The Rouke Baby Record. (http://www.rourkebabyrecord.ca/pdf/RBR2014Ont_Eng.pdf) link
● Growth should be tracked using the WHO growth charts. Each visit should include measurement of height, weight, and head circumference (up to 2 years of age).o If there is a failure to gain weight but normal height velocity, consider failure to thrive.o If weight gain is normal but height velocity is slowed (<5cm/year), consider constitutional delay, genetic short stature, or an endocrine cause.o If both height and weight are small, consider chronic disease.
Page 67
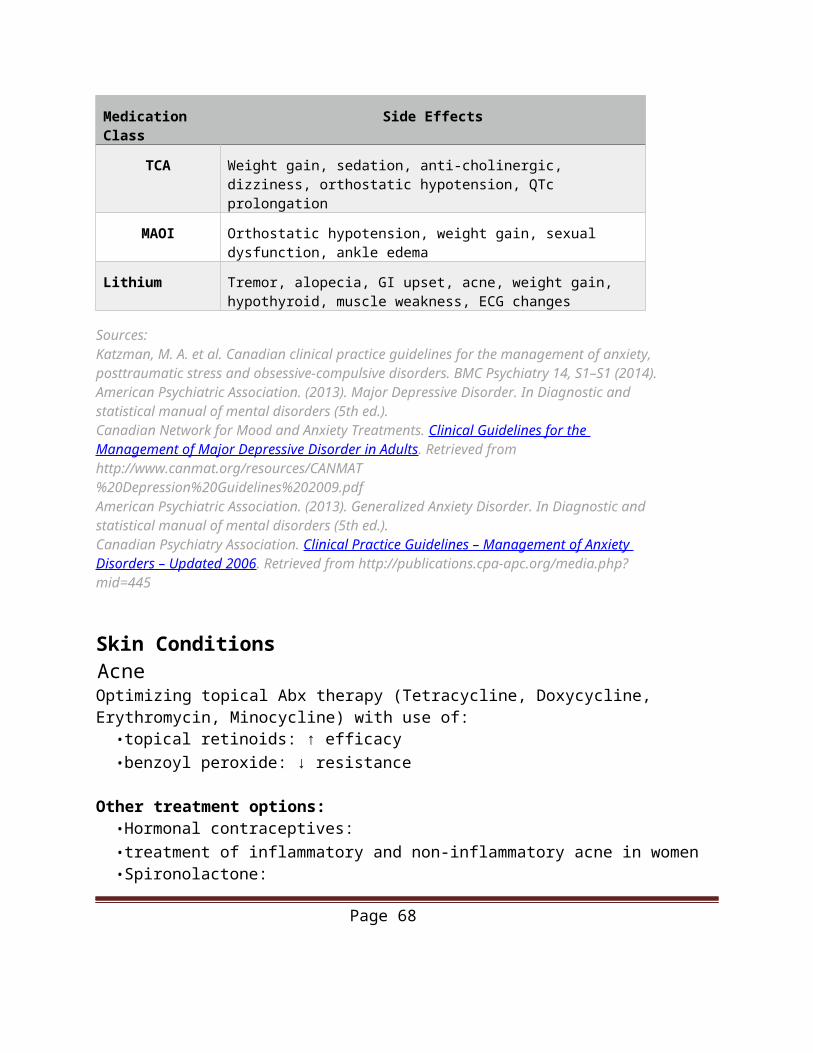
Source: Canadian Pediatric Society. (last updated 05-08-2014). Promoting optimal monitoring of child growth in Canada: Using the WHO growth charts. ( http://www.cps.ca/en/tools-outils/who-growth-charts ) Link
Infant Feeding and Nutrition
Exclusive breastfeeding for healthy term infants is recommended until 6 months of age and can be continued up to 2 years of age or longer with appropriate complementary feeding. Breastfeeding reduces gastrointestinal and respiratory infections and helps to protect against SIDS.
o Newborns require 150 cc (5oz) breast milk or formula equivalent per kg per dayo Infants 2-4 months require 600-900 cc (20-30 oz) per dayo Infants 4-8 months require 750-1080 cc (25-36 oz) per dayo Infants 9 months up to one year require 720-960 cc (24-32 oz) per dayo Supplementation with 400IU Vitamin D is recommended if exclusively breastfeeding
Medications and breastfeeding tool from the Hospital for Sick Children endorsed by CFPC: Mother Risk, available at: http://www.motherisk.org link
Community lactation consultants are available to meet with mothers and their babies and can assist with many issues including poor latch, nipple pain, cracked nipples, infections, poor infant weight gain, and insufficient milk supply. Many community health centres also have breastfeeding accessories like pumps available to rent on a weekly or monthly basis.For infants with tongue-tie (ankyloglossia), the CPS does not recommend routine frenotomy (surgical division of the tongue tie). There may be an association between ankyloglossia and breastfeeding difficulties; the choice to intervene surgically should be made jointly by the family and clinician after consideration of the individual situation.Introduction of solid foods is recommended at 6 months of age. The recommended order of introduction is iron rich foods (meats, legumes, fortified cereals) > vegetables > fruits. Delayed introduction of allergenic foods is not recommended. Lumpy textures should be offered by 9 months of ageConsumption of fruit juices should be limited. Water should be offered to satisfy thirstHomogenized cow’s milk can be introduced after 9-12 months of age, not earlier. Cow’s milk should be limited to less than 750 cc per day. Skim milk can be introduced after 2 years of age with the gradual transition to a lower fat dietNo bottles in bedAn open cup should be introduced approximately 1 year of ageIntroduction of honey should be avoided until 1 year of age due to risk of botulismInquire regarding vegetarian/vegan diets
Sources: Health Canada Infant Feeding Joint Working Group. (last updated 2015-08-18). Nutrition for Healthy Term Infants: Recommendations from Birth to Six Months. ( http://www.hc-sc.gc.ca/fn-an/nutrition/infant-nourisson/recom/index-eng.php )linkHealth Canada Infant Feeding Joint Working Group. (last updated 2015-01-19). Nutrition for Healthy Term Infants: Recommendations from Six to 24 Months. (http://www.hc-sc.gc.ca/fn-an/nutrition/infant-nourisson/recom/recom-6-24-months-6-24-mois-eng.php) linkRowan Legg, A.(2015). Position Statement: Ankyloglossia and breastfeeding. Canadian Paediatric Society 20(4):209-13. ( http://www.cps.ca/en/documents/position/ankyloglossia-breastfeeding )
Page 68
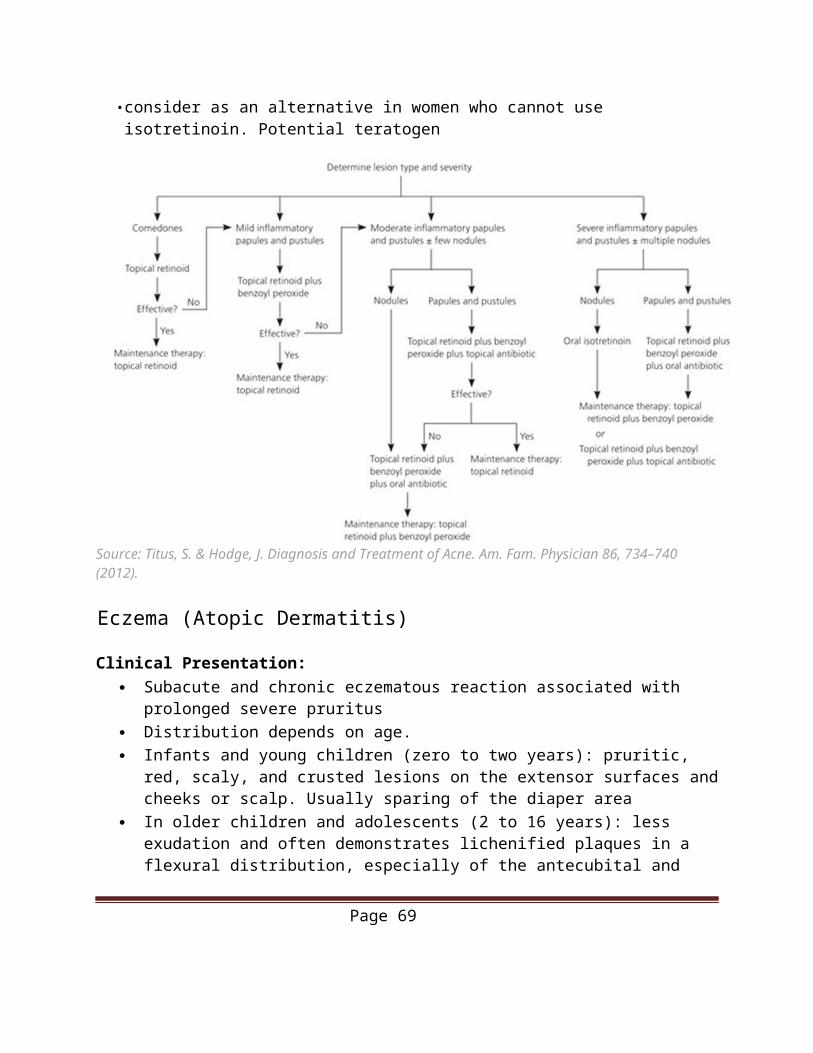
Page 69
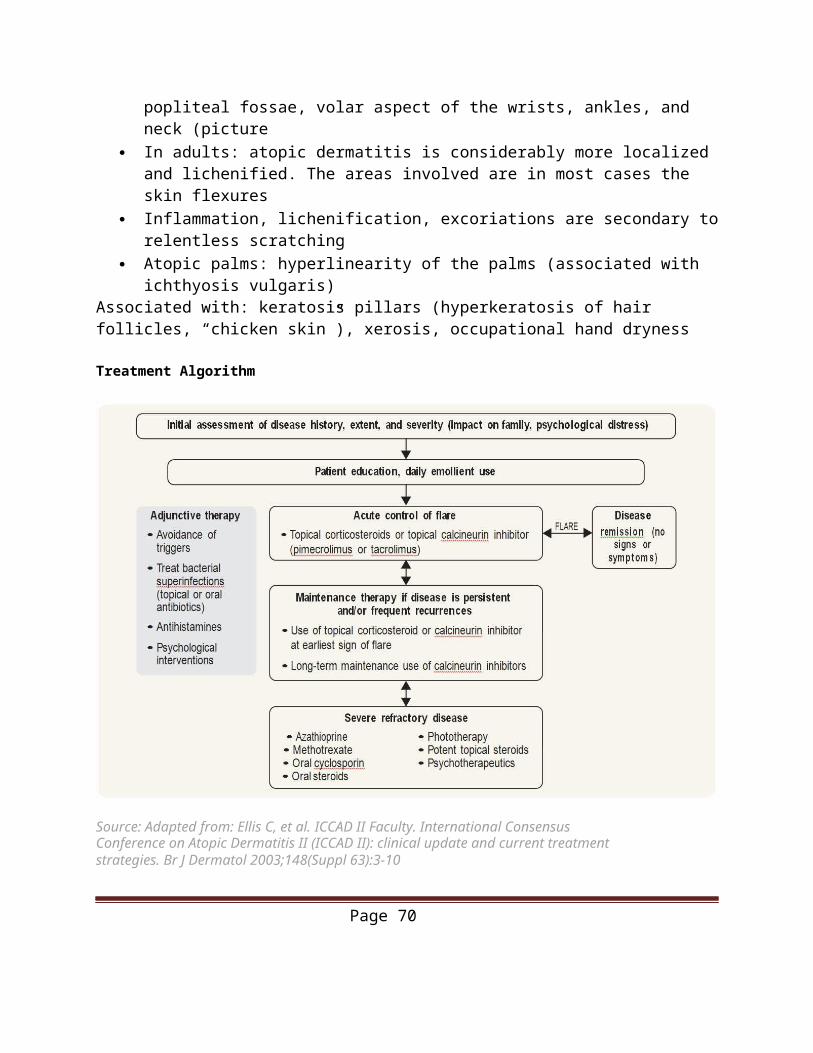
Pain Reduction Strategies for Immunizations Infants:
Breastfeeding during the immunization Use of sweet-tasting solutions e.g. Tootsweet Using the least painful vaccine brand Consideration of topical anaesthetics
Children:
Use the least painful brand of vaccine Keep the child in a non-supine position Rapid injection without aspiration Inject the most painful vaccine last Rub/stroke the skin of the injection site with moderate intensity before and during
vaccination Make use of physician or parent-led distraction or coaching Encourage the child to use slow deep breathing or blowing Avoid telling the child “it won’t hurt”
Source: Taddio, A., Appleton, M., Bortolussi, R., Chambers, C., Dubey, V., Halperin, S., … Shah, V. (2010). Reducing the pain of childhood vaccination: an evidence-based clinical practice guideline. CMAJ : Canadian Medical Association Journal, 182(18), E843–E855. (http://doi.org/10.1503/cmaj.101720)
Page 70
Health Promotion and ScreeningPeriodic Health Examination
Labs/Investigations Immunizations
Male − Fasting lipid profileq3 years at age 40 (earlier if high risk)
− Fasting blood glucoseq3 years at age 40 (more often if high risk)
− Hemoccult Multiphaseq1-2 years at age 50 OR Flexible sigmoidoscopy q10 years if normal and no polyps
− Bone Mineral Densityq1-3 years if moderate risk, q5 years if low risk at age 65 (earlier if at risk)
− Tetanus diphtheria, acellular pertussis vaccine q10 years until age 34
− Tetanus, diphtheria vaccine q10 years age >34
− Influenza vaccine q1 year− Herpes zoster vaccine (age 65)− Pneumococcal Pneu-P-23
vaccine (age 65 or earlier if high risk)
− Acellular pertussis vaccine− Varicella immunity− Rubella Immunity− Human papilloma virus (HPV) vaccine
(2-3 doses, Grade 7)
Females − Same as males except:− Fasting lipid profile at age 50− Mammography q1-2 years from
ages 50-74− Cervical Cytology q3 years from
ages 21-69
− Same as males plus:
Page 71
Breast Cancer Screening
Ontario Breast Screening Program1, 2 Average Risk High Risk
Screening Recommendation
Mammogram every two years for most women
Mammogram and screening breast MRI every year (or, if MRI contraindicated, screening breast ultrasound)
Screening PopulationWomen ages 50 to 74 Women ages 30 to 69 identified as
high risk*
Eligibility
• Healthcare provider referral or self-referral• No acute breast symptoms• No personal history of breast cancer• No current breast implants• No screening mammogram within the last 11 months
• Physician referral• Valid Ontario Health Insurance Plan number• No acute breast symptoms• Meets one of the high risk* criteria
*High Risk Criteria Are known to be carriers of a deleterious gene mutation (e.g., BRCA1, BRCA2) Are the first degree relative of a mutation carrier (e.g., BRCA1, BRCA2) and have declined genetic testing Are determined to be at ≥ 25% lifetime risk of breast cancer -- must have been assessed using either the IBIS or BOADICEA risk assessment tools, at a genetics clinic Have received chest radiation treatment (not chest x-ray) before age 30 and at least 8 years previously.
Other Recommendations
Breast Aware – Patients should be encouraged to be aware of how their breasts normally look and feel so they can identify changes (lumps, dimpling, discharge, skin redness, other changes)2
Women Aged 40-49, Average Risk – Routine screening with mammography may be considered, but is not recommended (weak recommendation - moderate quality evidence)3.
Mammography is associated with reduction in relative risk of death from cancer in this age group, both the number needed to screen and the risk of false positive tests are higher.3
Patients in this group may make personal decisions about mammography after discussion with their health care provider.2
Women Aged 75 and over – Limited data is available for this age group. Assess on an individual basis, taking into account life expectancy.3
Sources:1Cancer Care Ontario: Cancer Screening Guidelines. Revised October 2016 (https://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=273767)2Government of Ontario: Ontario Breast Cancer Screening Program. Revised September 2016. (https://www.cancercare.on.ca/pcs/screening/breastscreening/OBSP/) 3The Canadian Task Force on Preventive Health Care (2011). R e c ommendations on sc r eening f or b r ea s t c an c er in average-risk women aged 40–74 years . CMAJ, 183 (17), 1991-2001.
Page 72

(http://www.cmaj.ca/content/183/17/1991.full.pdf)
Cervical Cancer Screening
Recommendations
Screening Initiation
●Age 21●Postpone to initiation of sexual activity* if not sexually active at
age 21
Screening Interval q3years unless result dictates otherwise
Screening Cessation Age 70 if last 3 pap tests have been normal
*includes intercourse, digital or oral contact of the genital area with a partners of all genders
Special Circumstances
Women who: Screening Interval
Are immunocompromised q1y
Retained their cervix after subtotal hysterectomy
Are pregnant q3y (regular screening guidelines)
Have sex with women
Have received the HPV vaccine
● Any visual cervical abnormalities and/or abnormal symptoms must be investigated regardless of cytology findings.
● See link below for recommended management of different Pap test results.
Page 73
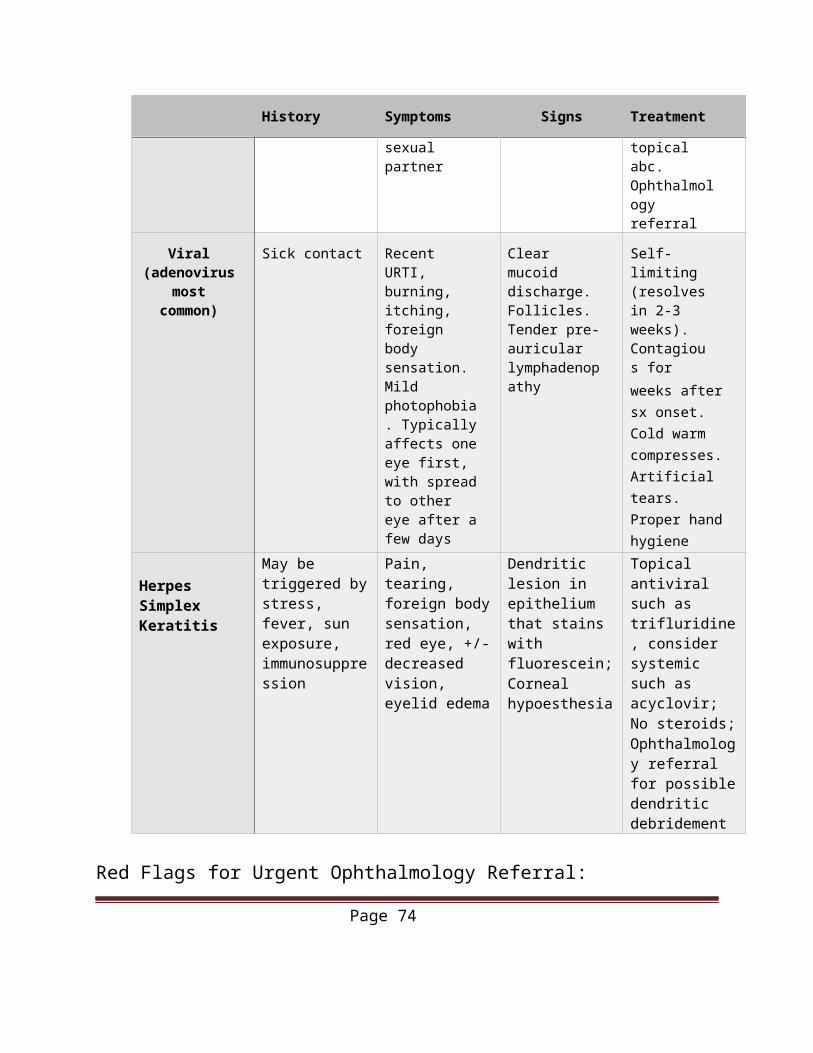
Ontario Cervical Screening Cytology Guidelines
Source:Cancer Care Ontario. Ontario Cervical Screening Cytology Guidelines Summary – Revised October 2016, based on 2012 Guidelines https://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=273767Toronto Notes, Adapted from: Ontario Cervical Screening Cytology Guidelines. May 2012
Page 74
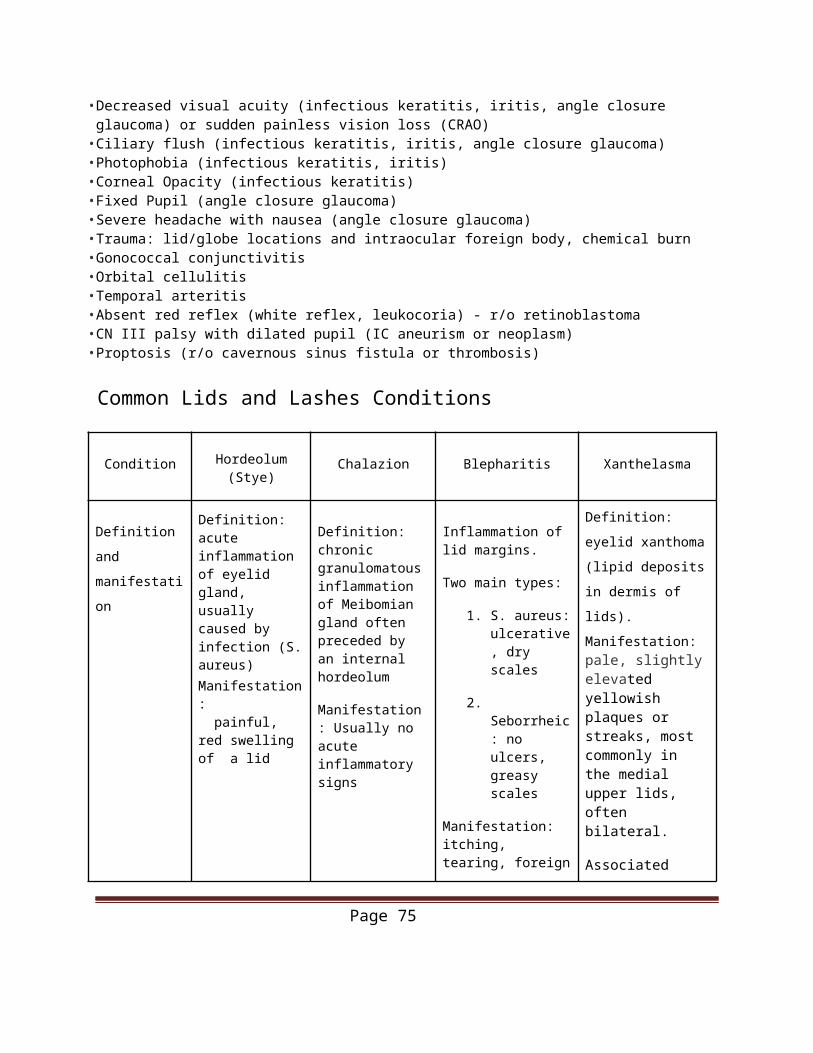
Colorectal Cancer Screening
Average risk: Individuals aged 50 - 74 with no family history of colorectal cancer and no personal history of polyps or inflammatory bowel disease should undergo screening with one of the following strategies1:
• FOBT (either gFOBT or FIT) every two years• Flexible Sigmoidoscopy every ten years
High risk: family history1
First degree relative with the disease diagnosed before age 60• Colonoscopy q5 yrs to begin at age 40• OR 10 yrs earlier than the youngest diagnosis of polyp or cancer in the familyIf diagnosed after age 60, then employ average risk screening to begin at age 40
High risk: hereditary colorectal cancer syndrome and IBD3
Family history of HNPCC• Colonoscopy q1-2 yrs beginning at age 20• OR 10 yrs younger than the earliest case in the family
Familial Adenomatous Polyposis (FAP)Sigmoidoscopy annually to begin at age 10-12Long standing colonic inflammatory bowel disease (Crohn’s or Ulcerative Colitis)
• For pancolitis: begin screening at 8 yrs after onset of disease, continue with colonoscopy q3 yrs in the second decade, colonoscopy q2 yrs in the third decade and colonoscopy annually in the fourth decadeFor left sided colitis, begin screening at 15 years after onset
Other Recommendations Abnormal FOBT should be followed up with a colonoscopy within 8 weeks1
If symptomatic, refer to specialist for evaluation (no role for FOBT at this point)1
There is insufficient evidence to support screening with using metabolomic (blood or urine) tests, DNA (blood or stool) tests, computed tomography colonography, capsule colonoscopy and double contrast barium enema1
Surveillance after polypectomy is based on the number, size, and pathological features of polyp as well as other clinical features such as family history and previous colonoscopy findings2
Sources:1Cancer Care Ontario: Colon Cancer Screening Guidelines. August 2016 https://www.cancercare.on.ca/pcs/screening/coloscreening/cccstandardsguidelines/2Guidelines for surveillance after polypectomy. Gastroenterology 2006. https://www.cancercare.on.ca/common/pages/UserFile.aspx?fileId=13484 link3ASGE guideline: colorectal cancer screening and surveillance. Gastrointestinal Endoscopy 2006. http://pacificcancer.org/Resources/Cancer/Colorectal/CRC_Screening_and_Surveillance.pdf
Page 75
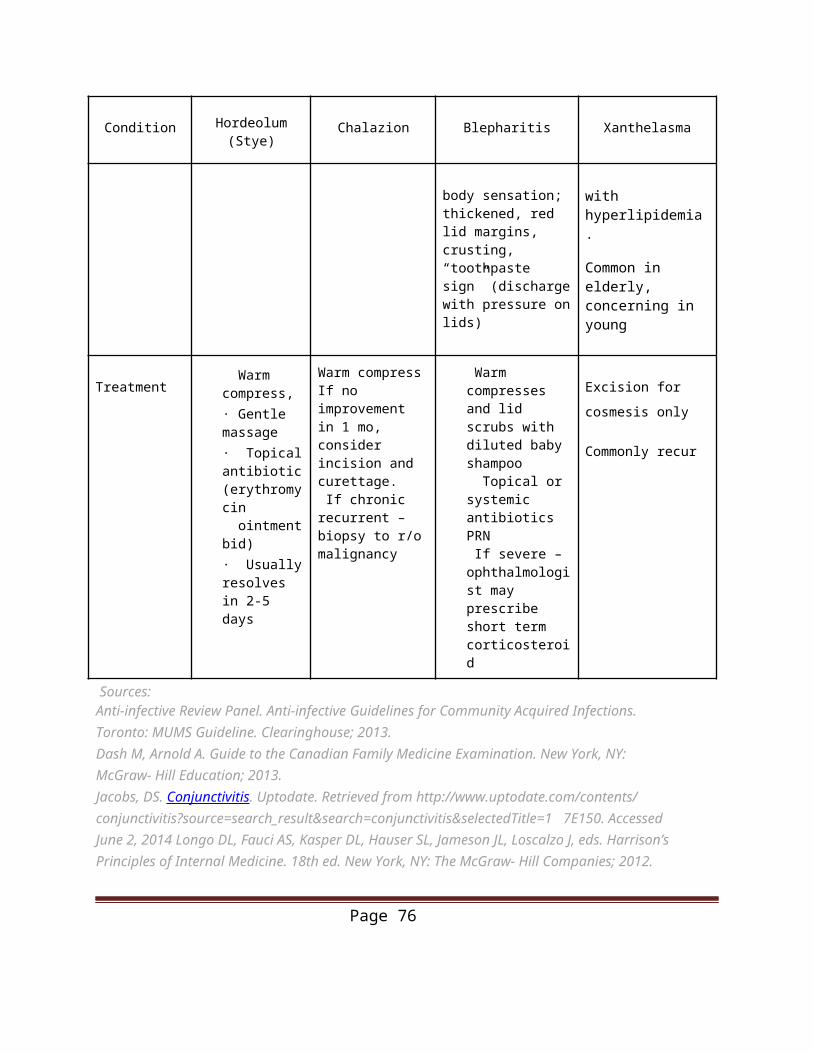
Skin Cancer Screening
Target RecommendationsVery high risk populationIndividuals with ANY of the following risk factors:
• on immunosuppressive therapy after organ transplantation
• personal history of skin cancer• 2 or more first-degree relatives with
melanoma• more than 100 nevi in total or 5+ atypical
nevi• have received more than 250 treatments of• psoralen ultraviolet A radiation (PUVA) for• psoriasis• received radiotherapy for cancer as a child
•Yearly total body skin examination•Counselling on skin self- examination and skin
cancer prevention•In the case of childhood cancer survivors, the site
of radiation therapy should be monitored
High risk populationIndividuals with TWO OR MORE of the following risk factors:
• a first-degree relative with melanoma• many (50-100) nevi• one or more atypical (dysplastic) nevi• naturally red or blond hair• a tendency to freckle• skin that burns easily and tans poorly or not
at all
• Counselling on skin self-examination• Should be seen once a year by a health care
provider trained in screening for skin cancers
Page 76

Smoking Cessation MedicationsMedication Dosing Adverse Effects
NICOTINE REPLACEMENT
THERAPYGum 1st cigarette ≤30 minutes after
waking: 4mg1st cigarette >30 minutes after waking: 2mgWeeks 1-6: 1 piece q1-2 hoursWeeks 7-9: 1 piece q2-4 hoursWeeks 10-12: 1 piece q4-8 hours
-Mouth/jaw soreness
-Hiccups
-Dyspepsia
-Hypersalivation
Effects associated with incorrect chewing technique:-
Light-headedness-
Nausea/vomiting-
Throat and mouth irritation
Lozenge 1st cigarette ≤30 minutes after waking: 4mg1st cigarette >30 minutes after waking: 2 mgWeeks 1–6: 1 lozenge q1–2 hoursWeeks 7–9: 1 lozenge q2–4hours Weeks 10–12: 1 lozenge q4–8 hours-
-Nausea
-Hiccups
-Cough
-Heartburn
-Headache
-Flatulence
-Insomnia
Transdermal Patch >10 cigarettes/day:-21 mg/day x 4 weeks-14 mg/day x 2 weeks-7 mg/day x 2 weeks
≤10 cigarettes/day:-14 mg/day x 6 weeks-7 mg/day x 2 weeks
- Local skin reactions (erythema, pruritus, burning)
- Headache- Sleep disturbances (insomnia, abnormal/vivid dreams): associated with nocturnal nicotine absorption *May wear patch for 16 hours if patient experiences sleep disturbances (remove at bedtime)
Page 77
Medication Dosing Adverse Effects
Nasal Spray 1–2 doses/hour(8–40 doses/day)*One dose = 2 sprays (one in each nostril)
- Maximum: 5 doses/hour or 40doses/day- Duration: 3–6 months
- Nasal and/or throat irritation (hot, peppery, or burning sensation)- Rhinitis- Tearing- Sneezing - Cough- Headache
Oral Inhaler 6–16 cartridges/day Individualize dosing; initially use 1 cartridge q 1–2 hours-
Best effects with continuouspuffing for 20 minutes
-Do NOT inhale into the lungs
(like a cigarette) but “puff” as if lighting a pipe
Duration: 3–6 months
-Mouth and/or throat irritation
-Cough
-Headache
-Rhinitis
-Dyspepsia
- Hiccups
OTHERBupropion 150 mg PO qAM x 3 days, then 150
mgPO BID-
Do not exceed 300 mg/day-
Begin therapy 1–2 weeks
prior to quit date
-Insomnia
-Dry mouth
-Nervousness/difficulty concentrating
Varenicline Days 1–3: 0.5 mg PO qAMDays 4–7: 0.5 mg PO BIDWeeks 2–12: 1 mg PO BID-
Begin therapy 1 week prior toquit date
-Duration: 12 weeks (+/-
additional 12-weeks)
-Nausea
-Sleep disturbances (insomnia,abnormal/vivid dreams)
Constipation
Sources:Rx for Change. Pharmacologic Product Guide: FDA-Approved Medications for Smoking Cessation.Updated March 1, 2015. Copyright © 1999–2015 The Regents of the University of California. Smoking Cessation Flow Sheet
Page 78
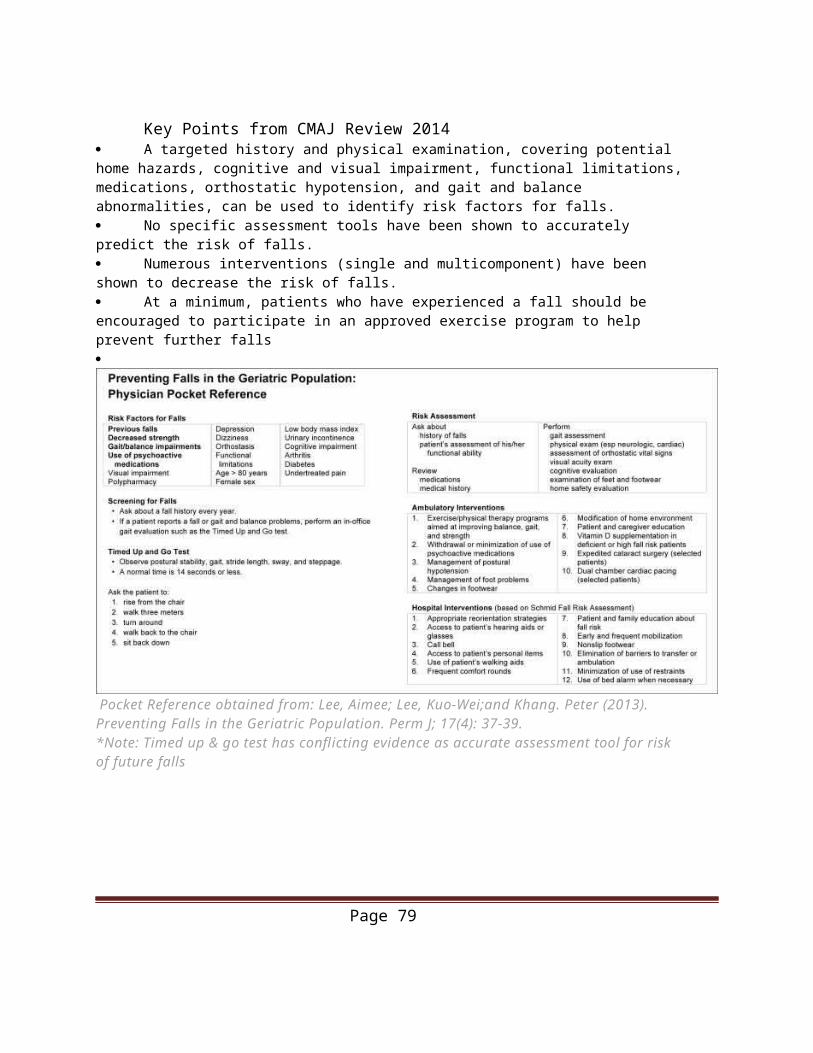
Smoking Cessation Flow Sheet
Source: CTI (2008). Smoking Progress Notes – Annual Patient Profile. (http://www.ctica.org/Smoking_ Cessation_Guideline_Flow_Sheet_updated_Jan2008.pdf)
Page 79
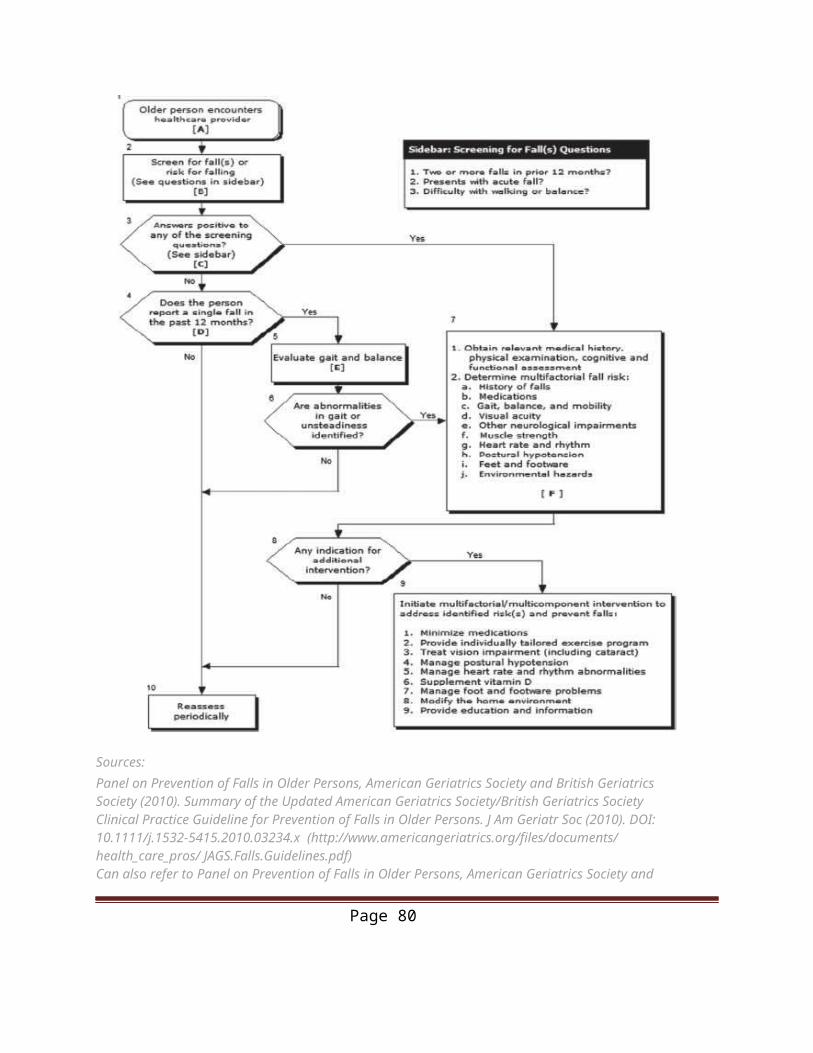
Family PlanningContraception Options
Method Advantages Disadvantages
Combined OCP (Daily)
Effectiveness (99.7% - perfect use,92% - typical use)Cycle control↓ dysmenorrhea,↓ menstrual flow↓ perimenopausal and PMS symptoms↓ risk of ovarian, endometrial,possibly colorectal cancer↓ ovarian cysts
- ↓ acne and hirsutism- ↑ bone density
-Irregular bleeding/spotting
-Breast tenderness, nausea, headache (mild, resolve within a few months usually)
- ↑ VTE risk (9-10/10 000 women/years, 4-5/10 000 at baseline)
- Slight ↑ risk of breast cancer-
Does not increase breast cancer risk-
(Vessey M, Painter R. Oral contraceptive use and cancer.
Findings in a large cohort study, 1968-2004. Br J Cancer 2006;95(3):385–9.)
Transdermal Contraceptiv
e Patch (Weekly)
Effectiveness (99.7% – perfect use,92% - typical use)Same as OCP48-hour “window of forgiveness”
Same as OCP Skin irritationPatch detachment (uncommon) Less effective if >90kg
Vaginal Contracepti
ve Ring(Monthly)
Effectiveness (99.7% - perfect use,92% - typical use)Same as OCP1-week “window of forgiveness
Same as OCP VaginitisVaginal discomfortExpulsion (uncommon)
Progestin Only Pill(Daily)
Effectiveness (99.7% - perfect use,92% - typical use)Can be used post-partum~3-hour window of forgiveness
-Irregular bleeding
-Headache, bloating, acne, breast
-tenderness
-Must take at same time everyday
-No pill-free interval
Depot medroxy-
progesterone
Effectiveness (99.7% - perfect use,97% - typical use)↓ menstrual flow or
Irregular bleeding Delayed return of fertility Headache, ↓ libido, nausea, breast
Page 80
Method Advantages Disadvantages
acetate (DMPA)
(IM progesterone
injection every 12-13 weeks)
Amenorrhea↓ risk of endometrial cancer↓ endometriosis symptoms↓ PMS and chronic pelvic pain symptoms↓ SeizuresPossible ↓ risk of PID and sickle-cell crises
- 6-day “window of forgiveness”
tenderness, weight gain, mood effects
Weight gain- ↓ Bone mineral density (just
monitor and give Calcium + Vit D)
Copper Intrauterine
Device (5 years)
Effectiveness (99.4% - perfect use,99.2% - typical use)Possible ↓ risk of endometrial cancerCan be used as emergencycontraception
-Irregular bleeding
- ↑Menstrual flow-
Dysmenorrhea-
Perforation-
Expulsion-
Increased risk of PID for first 20 days
Hormonal Intrauterine
Device (5 years)
Effectiveness (99.9% - perfect use,99.9% - typical use)↓ Menstrual flow/ Amenorrhea↓ dysmenorrheaMay protect against endometrialhyperplasia
-Irregular bleeding
-Systemic hormonal side effects
-Functional cysts
-Perforation
-Expulsion
-Increased risk of PID (first 20 days)
-Failure (if fails, must exclude ectopic)-
Increased risk of PID for first 20 days
Male Condom (one-time use)
Effectiveness (98%- perfect use,85% - typical use)Protects against STIsNo prescription required
Page 81
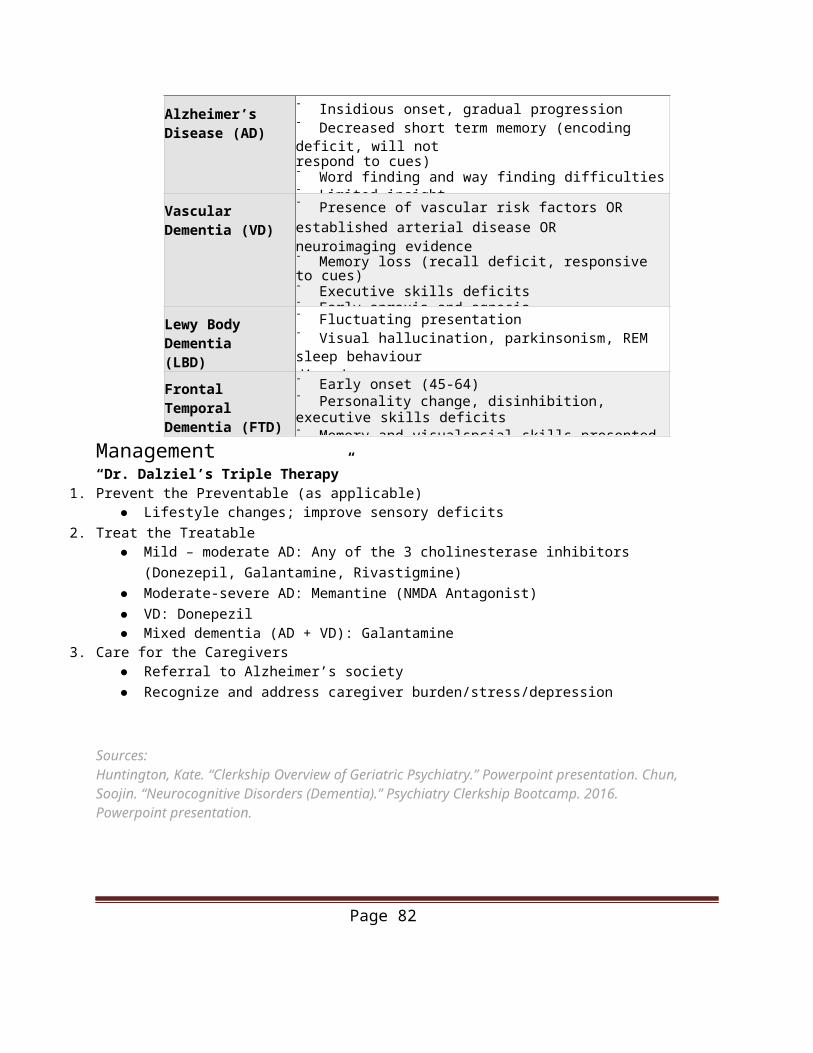
Method Advantages Disadvantages
Female Condon (one-time use)
Effectiveness (95%- perfect use,79% - typical use)Same as male condomFemale controlled
Can be noisy during intercourseCan be difficult to insertCan cause discomfort during intercourse
Diaphragm (one-time use)
Effectiveness (94%- perfect use,84% - typical use)Some protection against STIsCan be used during menses
Can be difficult to insertMust be left in for 6 hours after intercourseMust be used with spermicideDoes not protect against HIVLatex or spermicide allergyMust be fitted by health care providerMay ↑ risk of UTI,
Sponge (one-time use)
Effectiveness (Nulliparous:91% - perfect use, 84% - typical use;Parous: 80% - perfect use, 68% -typical use)One size fits allNo prescription required
Can be difficult to insert and removeMust be left in 6 hours after intercoursePossible spermicide sensitivityShould not be used during menstruationLess effective in multiparous women
Fertility Awareness and Symptothermal
Method
Effectiveness (91-99% - perfect use,80% - typical use)Greater awareness of gynaecologicalhealth
High probability of failure if not used consistently and correctly
Lactational Amenorrhea
Method
Effectiveness 98%-
Menses must have not returned-
Must be fully/nearly fully breastfeeding-
Baby must be < 6 months of ageAbstinence
Effectiveness 100%No STI risk if no exchange of bodyfluids
May be too restrictive for some couplesCan cause frustrationDoes not encourage use of other methods of contraception, if behaviour changes
Source: Fisher, W.A., Black, A (March 27, 2007). Contraception in Canada: a review of method choices, characteristics, adherence and approaches to counseling. CMAJ. 176(7), 953-961.(http:// www.cmaj.ca/content/176/7/953.full.pdf)
Page 82
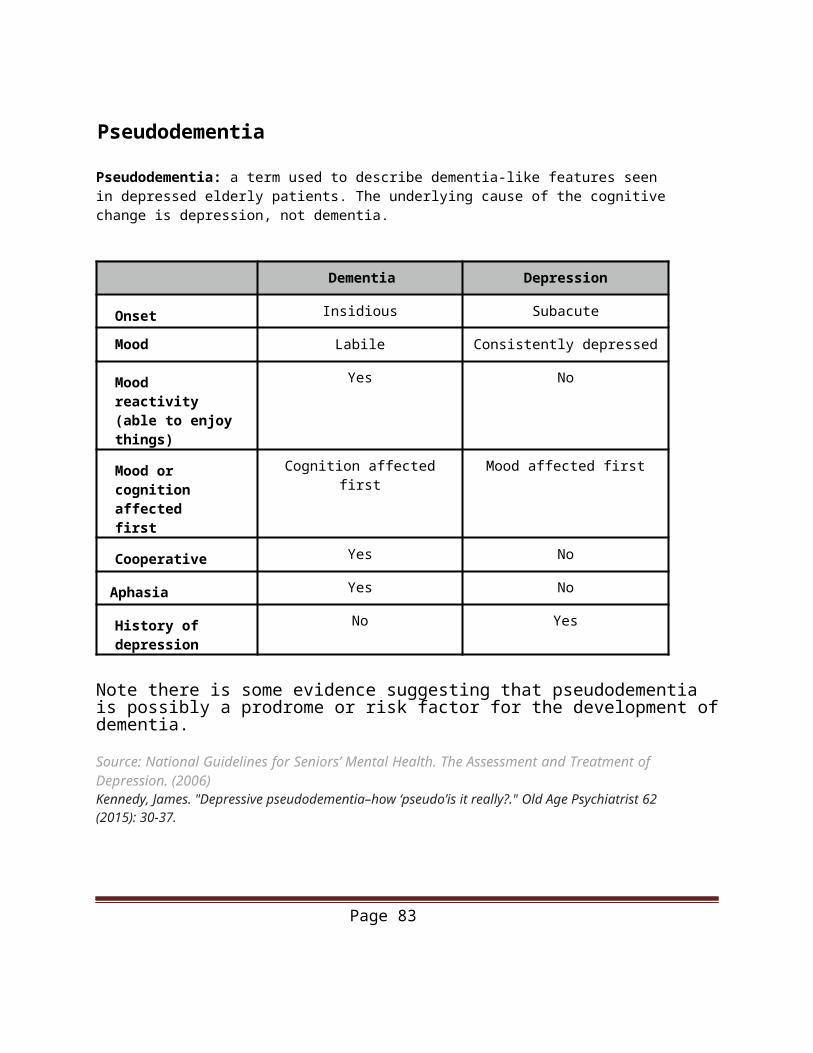
Quick Reference GuideCommon Antibiotics
Condition Microorganism First Line Antibiotic Regimen
Community Acquired Pneumonia - Adult
(outpatient without comorbidities)
S. pneumoniaeM. pneumoniaeC. pneumoniae
Clarithromycin 500mg BID or 1000mg(extended release) once daily x 7-14 daysAmoxicillin 1g TID x7-14 days
Azithromycin 500mg on first day then 250mg x 4 day
Community Acquired Pneumonia
– Children (outpatient without comorbidities)
1 – 3 months: RSV, viruses
3 months – 5 years:S. pneumo, S. aureas, GAS, H. influenza
5 – 18 years: M. pneumonia, C. pneumonia, S. pneumonia, influenza A or B
1-3 months: no antibiotic indicated 3 months – 5 years: Amoxicillin80mg/kg/day divided TID x 7-10days
5 – 18 years: Clarithromycin 15mg/kg/day divided BID x 7-10 days
Acute Pharyngitis Group A Strep Adults: Penicillin V 600mg BID x 10 dayErythromycin 250mg QID x 10d
Children: Pen V 40mg/kg/d divided BID-TID x 10d, max 750mg/d (use adult dosing if>27kg)Erythromycin estolate 40mg/kg/d divided BID-TID x 10d
Otitis Media S. pneumoniaeH. InfluenzaM. catarrhalis
Adults: Amoxicillin 500mg TID x 5 d Cefprozil 250-500mg BID x7-10dChildren: Amoxicillin 80-90mg/kg/ day divided BID or TID (max 3g/day) x5 or 10 daysCefprozil 30mg/kg/d divided BID (see acute otitis media p.x for details)
Otitis Externa P. aeruginosa ColiformsS. aureus
Ciprodex 4 drops BID
Bacterial Sinusitis S. pneumoniaeH. influenzaM. catarrhalisS. aureus
Adults: Amoxicillin 500mg TID x 5-10 dAmoxicillin/Clavulanate 500mg TID x 5-10 daysCefuroxime-AX 250-500mg BID x 5-10dChildren: Amoxicillin 80-90mg/kg/
Page 83
Condition Microorganism First Line Antibiotic Regimen
day divided BID or TID (max 3g/day) x 10-14 daysAmoxicillin/Clavulanate 40-80mg/ kg/day divided BIDCefprozil 30mg/kg/d divided BID x10-14d
Bacterial Conjunctivitis S. aureusS. pneumoniaeH. influenzaM. catarrhalis
Erythromycin 0.5 ointment 1/2 inch QID x5-7 dayContact lens users: Ciprofloxacin 0.3% 1-2 drops QID 5-7 days1-2 dr
Urinary Tract Infection E.coliS. saprophyticus Other gram –ve bacilli
TMP/SMX 1DS tab BID x 3 days Nitrofurantoin 100mg BID x 5 days (CI in pregnancy after 36wk) Cephalexin 250-500 mg QID x 7 days (if pregnant)
Pyelonephritis E. coli
K. pneumonia
P. mirabilis
Ciprofloxacin 500mg BID x 7 days
Urethritis N. gonorrhea
C. trachomatis
Ceftriaxone 250mg IM x 1 AND Azithromycin 1g PO once
Bacterial Vaginosis Overgrowth of:G. vaginalis
M. hominis Anaerobes
Metronidazole 500mg BID PO x 7 days
Peptic Ulcer Disease (non- NSAID)
H. pylori “HP-PAC” BID x7dP: PPI (eg. omeprazole 20mg BID x 7d)A: Amoxicillin 1000mg BID x 7 d C: Clarithromycin 500mg BID x 7d
Page 84
Common Antivirals
Condition Microorganism Antiviral Regimen
Mucocutaneous herpes (>3/year)
Herpes Simplex type 1 or 2 Valacyclovir 2g BID once
Famciclovir 500mg BID x 7 days
Genital Herpes Herpes Simplex type 1 or 2 Acyclovir 400mg TID x 5-7 days
Shingles (initiate within 72 hours of rash onset)
Varicella Zoster Valacyclovir 1g TID x 7 days
Famciclovir 500mg TID x 7 days
Chicken Pox (initiate within 24 hours of rash onset)
Varicella Zoster Valacyclovir 1g TID Famciclovir 500mg TID Prevention: Chickenpox vaccine
Genital Warts Human Papilloma Virus Cryotherapy (liquid nitrogen q1-2 weeks)
Influenza Influenza A or B Oseltamivir (Tamiflu) 75mg daily x 10 days (must begin within 48 hours of exposure/ symptoms)
Source: Anti-infective Review Panel. Anti-infective Guidelines for Community Acquired Infections. Toronto: MUMS Guideline Clearinghouse; 2013.
Page 85
Immunization Schedule
Page 86

Page 87
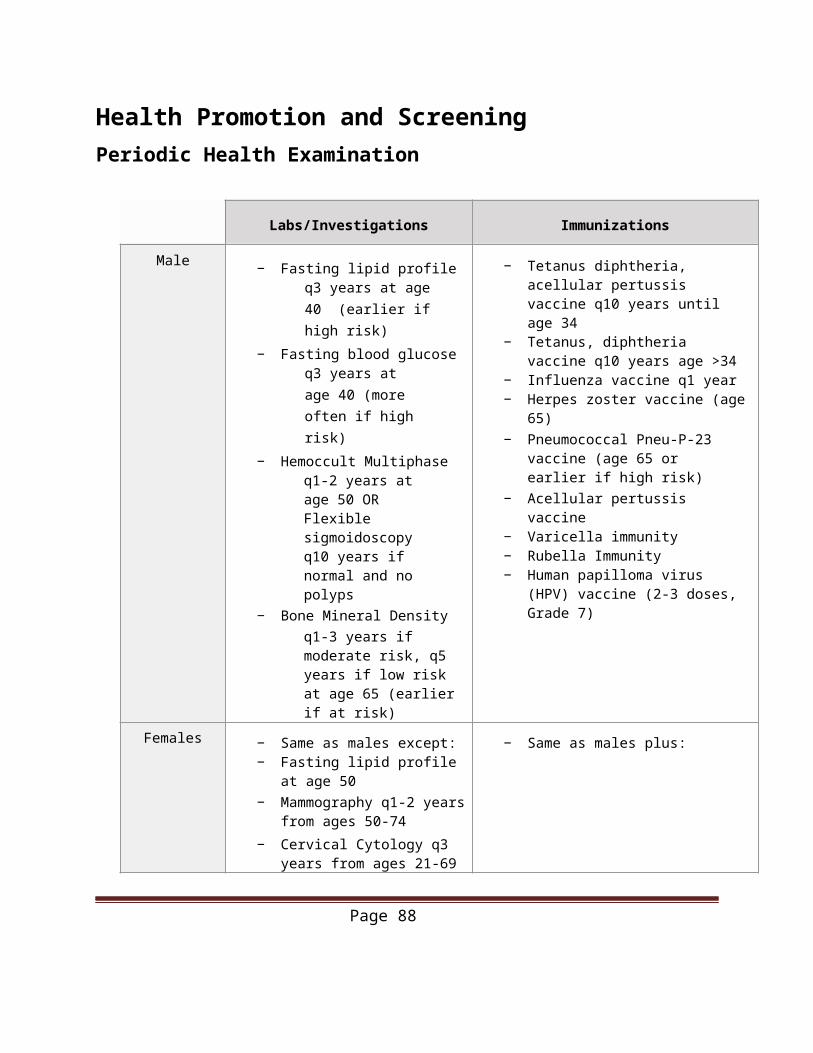
Vaccine Contraindications• Anaphylaxis to a previous dose or constituent (e.g. neomycin)• Significant Immunosuppression (live vaccines)• Pregnancy (live vaccines)
Live Attenuated Vaccines:• BCG• Measles• Mumps• Rubella• Varicella• Yellow fever• Typhoid Ty21a• Vaccinia
Sources:Sur, D., Wallis, D. & O’Connell, T. Vaccinations in Pregnancy. Am. Fam. Physician 68, E299–309 (2003).MacDonnell, Heather, “Immunizations in Canada.” CHEO. Paediatric Clerkship. 2015. Lecture.Government of Ontario. Publicly Funded Immunization Schedules for Ontario – October 2015. © Queen’sPublicly Funded Immunization Schedules for Ontario – December 2016. © Queen’s Printer for Ontario, 20152016 (http://www.health.gov.on.ca/en/pro/programs/immunization/docs/immunization_schedule.pdf)
60
Page 88
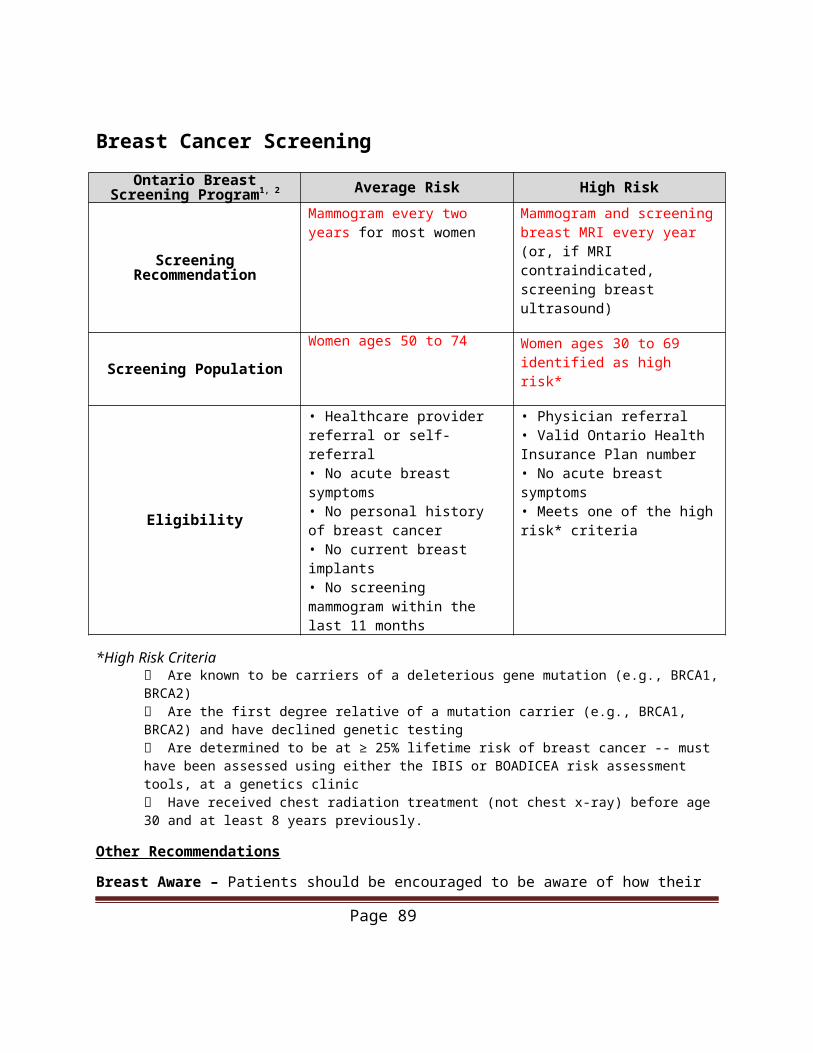
Developmental Milestones
Age Gross Motor Fine Motor Language Social/Cognition
1 month Lifts head to 45 degrees
Follow to midline Startles to loud noise
Smiles spontaneously
2 months Lifts head up when on stomach
Follows past midline
Coos (gurgly sounds), squeals, laughs
Smiles responsively, recognizes caregivers
6 months Sits without support, rolls from back to side
Transfers between hands
Babbles, uses dada/ mama non specifically
Feeds self, stranger anxiety
9 months Pulls to stand Thumb-finger grasp, bangs 2 cubes held in hand
Uses dada/mama specifically
Waves bye, plays pat-a-cake, indicates wants
12 months Stands alone, walks
Puts block in cup, scribbles
2-3 words Imitates activity, play ball
18 months Walks up steps, kicks ball
Builds tower of 4 cubes
Combines words, speech half understandable
Wash and dry hands, brush teeth with help
2 years Jumps, throws ball overhand
Builds tower of 6 cubes
Knows 6 bodyparts, names 1 picture
Names friend, puts on clothing
Sources:Dash M, Arnold A. Guide to the Canadian Family Medicine Examination. New York, NY: McGraw-Hill Education; 2013.Frankenburg, W.K., et al.: The DENVER II: A major revision and restandardization of the Denver Developmental Screening Test.Pediatrics, 89:91-97, 1992Frankenburg, W.K., et al.: The DENVER II Technical Manual 1996, Denver Developmental Materials, Denver, Co.Rourke, L., Leduc, D., Rourke, J. (2014). Rourke Baby Record: Evidence-Based Infant/Child Health Maintenance. Retrieved fromhttp://www.rourkebabyrecord.ca/pdf/RBR2014Ont_Eng.pdf
Page 89
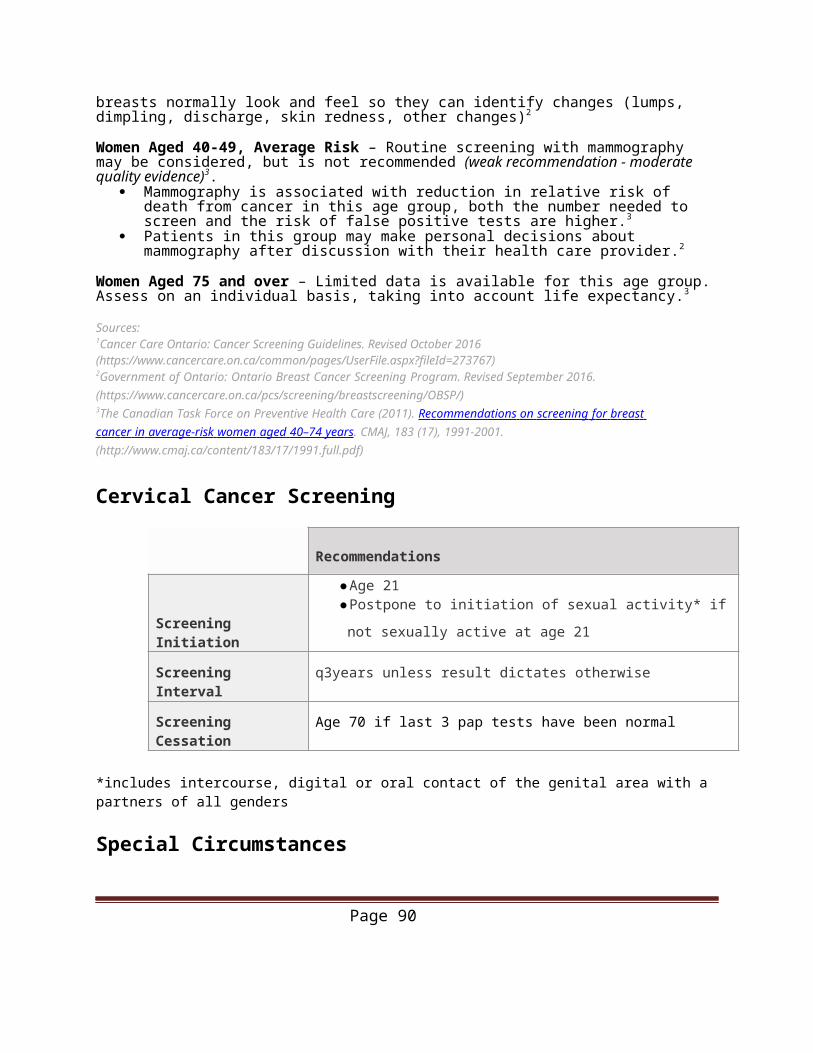
Dermatology GlossaryTerm Characteristics Diameter Example
Macule Flat, non-palpable, change in color of skin <1cm Freckles
Patch Flat, non-palpable, change in color of skin >1cm Vitiligo
Papule Solid raised lesion, well circumscribed <1cm Nevi
PlaqueSolid raised lesion, well circumscribed, superficial, may be flat topped or rounded
>1cm Psoriasis
Nodule Solid palpable lesion, height>width, appreciable depth. <1cm Dermatofibroma
TumourUsually found in dermal or subcutaneous tissue and the lesion may be above level with or below the skin surface
>1cm Lipoma
Vesicle Raised, pus-filled lesion <1cm HSV
Bulla Raised, pus-filled lesion >1cm Burns
Pustule Raised, pus-filled lesion <1cm Pustullar psoriasis
Wheal (Hive/ Urticaria)
Transient, circumscribed elevated papules or plaques often with erythematous borders and pale centres. Often pruritic, formed by edema in the dermis
Allergic reaction
ErosionSuperficial break in the skin due to loss of part or all of the epidermis; heals without scarring
Ulcer Loss of epidermis and at least part of dermis; heals with scarring
Fissure Break in the skin extending from epidermis to dermis
Telegiectasia Foci of visibly dilated capillaries Rosacea
Purpura Red or purple macule or patch that is non-blancheable; area of hemorrhage Coagulopathies
Lichenification Diffuse thickening of the epidermis, accentuating normal skin markings Eczema
Crust Dried exudate of serum, pus or blood originating from a lesion Impetigo
Scales A dry build-up of dead skin cells Psoriasis
Atrophy Thinning of the skin Chronic sun exposure
Source: MacNeal, RJ. (2015). Description of Skin Lesions (https://www.merckmanuals.com/professional/ dermatologic-disorders/approach-to-the-dermatologic-patient/description-of-skin-lesions)
Page 90
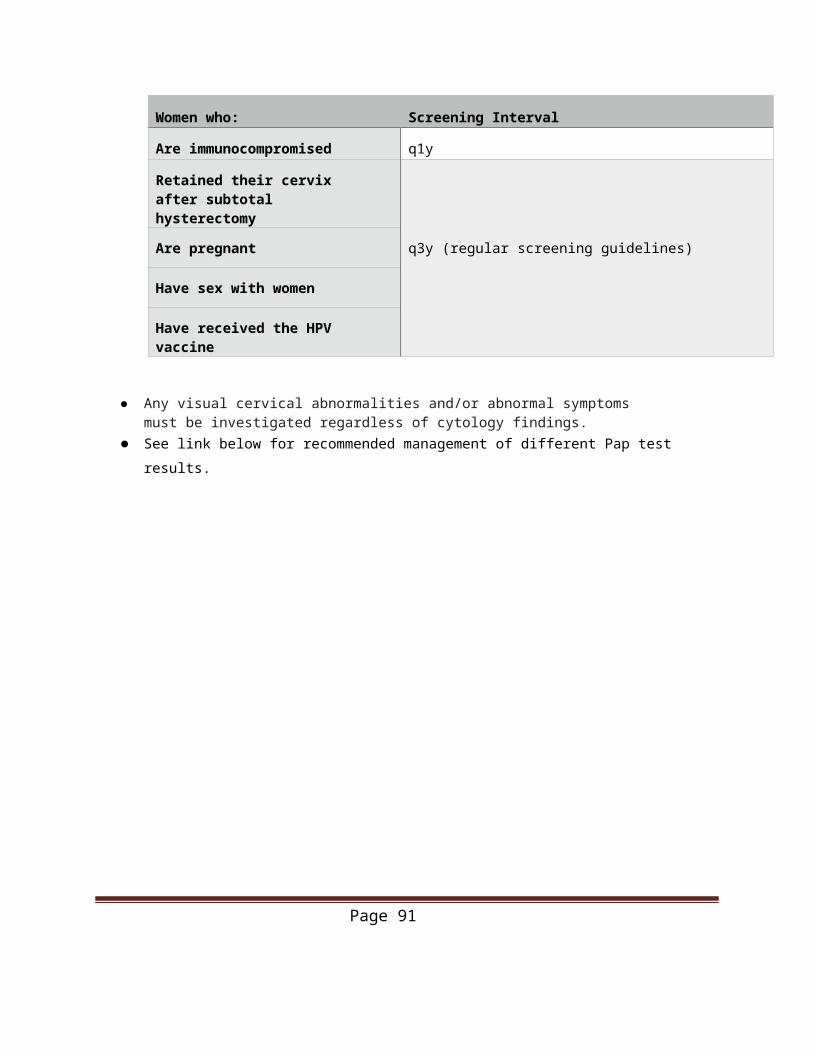
Antenatal Care Timelines
Frequency of visits:● Advise 1st visit 8-10 weeks GA● Every 4 weeks for the first 28 weeks● Every 2-3 weeks until 36 weeks GA● Weekly after 36 weeks GA
➔Add to Antenatal Form 2 at each subsequent visit following initial visit
Initial Visit (Recommended 8-
10 weeks GA)
Complete Antenatal Form 1 and 2Initiate antenatal bloodwork (CBC, Type + Screen, VDRL, Hepatitis B, Rubella, HIV, Pap (if indicated), Chlamydia/Gonorrhea swab, Urine C+S and dip)
Initiate prenatal vitamins if not yet started
11-14 weeks GA Integrated Pregnancy Screening (IPS) U/S and 1 bloodwork (PAPP-A)
11-13 weeks GA Chorionic Villous Sampling (if indicated)
12 weeks GA + Fetal heart rate (FHR) with doppler
15-20 weeks GA 2nd set of IPS bloodwork (MSS)
15-22 weeks GA Amniocentesis (if indicated)
18-20 weeks GA U/S for fetal morphology recommended
20 weeks GA+ Symphysial fundal height (SFH)
24-28 weeks GA Gestational diabetes screen: Glucose tolerance test (50-gram)If >7.8 a 2nd
28 weeks GA WinRho injection for Rh(-) patients
32-34 weeks GA U/S for fetal growth is recommended
35-37 weeks GA Group B Strep (GBS) swabDetermine fetal lie by palpation
40 weeks GA+ U/S for fetal growth and BPP
Source: Summary of ACOG Guidelines for Perinatal Care 7th
Edition. (2012).
Page 91