Embed Size (px)
Citation preview
8 (1980年9月)
ABOUT THE EXPERIENCE OF PREGNANCY AND DELIVERY
OF A PATIENT WITH THE ATYPICAL APLASTIC ANEMIA
Masao YANO
(The 2nd Tokyo National Hospital, Tokyo)
I have experienced a case of atypical aplastic anemia with two episodes of pregnancy
and delivery.
She had two different types of delivery ; the first delivery was done by Caesarian
section and the second delivery was done by vaginal delivery; both of them were successful.
The Caesarian section was better than vaginal delivery in the less amount of bleeding
during delivery.
I think for the pregnancy and delivery in the patient of aplastic anemia, the following
three condition are indispensable;
(1) A medical and paramedical project team.
(2) The artificial induction of labor.
(3) An adequate supply of blood for transfusion.
HEREDITARY SPHEROCYTOSIS WITH EARLY
JAUNDICE IN THE NEONATAL PERIOD
Akiko ADACHIHARA, Toshihiko KUROKAWA, Naomi HONMA,
Mani OKUBO and Yugo ISHIZUKA
(The 2nd Tokyo National Hospital, Tokyo)
Hereditary spherocytosis is a hemolytic disease transmitted by autosomal dominant trait.
The jaundice of the patients with HS in the neonatal period often becomes severe. Then
patients with HS often have past history of blood exchange transfusion because of severe
jaundice in the neonatal period.
We experienced a patient who was suspected to have HS soon after birth for her early
jaundice and her family history, and blood exchange transfusion was done. The patient was
a first born and the product of a 38 weeks gestational normal delivery weighing 2,990 g. The
patient's mother, maternal grandfather and maternal aunt have HS and her mother and
grandfather have past history of splenectomy.
Nausea and vomiting began at 17 hours after birth and jaundice on the skin appeared at
22 hours after birth. Serum total bilirubin level was 12mg/dl at 31 hours after birth and
blood exchange transfusion was done immediately. Jaundice gradually disappeared and the
-760-
(医 療 第34巻 第9号) 9
patient's condition was favorable after that. But severe anemia was noticed at 40 days after
birth. The value of hemoglobin was 7.6 g/dl and 100 ml of blood was transfused to the patient.
Moderate amount of spherocytes were seen in the mother's peripheral blood. On the
contrary, spherocytes were scarcely seen in the patient's peripheral blood. When auto-
hemolytic test was done at 3-months-old, 8.29% of the patient's red blood cells incubated for
48 hours without glucose hemolyzed and the red blood cells incubated with glucose became
spherocytec. Osmotic fragility test of the patient's red blood cell showed normal. This
result may be because of the influence of blood transfusion. Other hemolytic screening
tests such as hemoglobin electrophoresis and Heinz body formation test were normal.
The cause of HS is considered to be decreased lipid on HS erythrocyte membrane.
Severe hemolysis of HS newborns may be related to hypolipidemia in neonatal period. The
value of total cholesterol of the patient's serum before blood exchange transfusion was
57 mg/dl.
STATISTICAL STUDIES ON 8,453 OPERATION CASES OF
THE GASTRIC CANCER FOR 5 YEARS (1963-1967) IN HOKKAIDO
Michio SASAKI, Kazuo KAWASAKI,
Masami OGITA and Takehiro ICHIKAWA
(Sapporo National Hospital, Hokkaido)
Statistical studies were made on 8,453 operation cases of the gastric cancer collected by
Hokkaido Cancer Research Center from total number of 349 main hospitals in Hokkaido and
the results were compared with those from all over the country.
As far as the ratio of gastrectomy (79.4% on the average), total gastrectomy (17.5% on
the average), ratio of the early stage cancer (18.396 on the average) and ration of B I a-
nastomosis which was considered to be the ideal reconstruction method were concerned,
the results showed the gradual improvement for 5 years (1963-1967).
Compared with the results from all over the country, all kinds of factors showed slightly
lower rates. However, if the fact that the hospitals from all over the country except
Hokkaido were equally large in scale was taken into consideration, our Hokkaido cases are
by no means regarded to be on a low level.
-761-
(医 療 第34巻 第9号) 55
新 生 児 期 に 早 期 黄 疸 を 来 し た 遺 伝 性 球 状 赤 血 球 症 の1例
安 達 原 曄 子* 黒 川 叔 彦* 本 間 直 美*
大 久 保 ま り* 石 塚 祐 吾*
要 旨 遺伝性球状赤血球症は, 常染色体性優性遺伝 によつて, 溶血性貧血 を来す疾患 であるが,
我 々は出生直後 にHSを 疑い, 交換輸血 を行つたが, その後 も貧血が持続 してい る症例 を経験 し
た. 患児 の母, 母の妹, 母万祖父 もHSと 診断 されてお り, 母親, 祖父は, 摘脾 も受 けてい る.
患児は, 生後22時 間 ころよ り黄疽が出現 し, 生後34時 間に総 ビリル ビンが12mg/dlと なつたた
めに交換輸血 を施行 した. その後, 生後40日 ころに, 強度の貧血を来 したため, 輸血 を100ml施
行 したが, その後 も貧血気 味であ る. 患児の末梢血 には, 母親の末梢血 に比べ, 球状赤血球 はほ
んのわずか しか認 められないが, 生後3ヵ 月の時点 で, 48時 間, glucose(-)で 艀置 した赤血
球は溶血が元進 してお り, glucoseを 添加 した ものには球状化が み られた. 赤血 球浸透圧抵抗試
験は正常範 囲内にあ り, これは, 輸血の影響が残 つているためか もしれない.
遺伝性球状赤血球症(以 下 「HS」 と略す)は, 常染
色体性優性遺伝 による赤血球異常のために溶血 を来す
疾患で ある. おそ らく, 赤血球膜の異常 によ り, 溶血
がお こると考 え られているが, メカ ニズムは十分 明 ら
か にされていない. 臨床的には, 溶血性黄疸, 貧血,
脾腫を来す. 発症年令はま ち ま ちで あ るが, 後年,
HSと 判明 した症例の中 には, 新生児期に, 強度な黄
疸のために, 交換輸血を受 けた既往の ある者が多い.
しか し, 生後 ま もな くHSを 疑 つて, 交換輸血 を施行
した例1)は 少ない. 我 々は, 母親がHSで あ り, 出生
直後にHSを 疑い, 交換輸血 を行つ た症例を経験 した
ので報告す る.
症 例
患者 生後1日 女 児
主 訴 黄疸
家族歴 患児は第1子 で, 同胞は な い. 父 親 は 健
康. 患 児の母親 と, 母親の妹, 母方祖父がHSと 診断
されている. 母親は黄疸, 貧 血 の た めHSと 診断 さ
れ, 15才 で摘脾 を受けた. それ以後は貧 血 もな く健康
であ る. 母親 には, 兄1人, 妹1人 の2人 の同胞があ
るが, 妹が, 現在20才 で, 貧血, 黄疸 を指摘 されてお
り, HSと 診断 された. いずれ も新生児期 に交換輸血
は受 けていない. 母方祖 父は, 20才 代で貧血のため摘
脾 を受 けた. 他の血縁者 で, 貧血, 黄疸の既往のある
者 はい ない. なお, 母親 には, 流, 早産の既 往 は な
い.
出生後の経過 在胎38週 で本院で出生. 正常分娩.
出生体重2990g. 生後17時 間よ り, 嘔気, 嘔吐がみ ら
れ, 生後22時 間 ごろよ り, 肉眼的に皮膚 の黄疸が認 め
られた. 眼球結膜 に も黄染 を認 めた. 皮膚 のturgorは
低下 していた. 心音純で, 肺聴診上異常所見 な く, 腹
部 には, 肝脾腫大 は認 めなかつた. 神経学 的に も異常
所見はなかつた. 生後31時 間で, 血清総 ビリル ビン値
は12mg/dlで あ り, 明 らか な早発黄疸 と思われたの
で, Maisels2)の 表に準 じて, 生後34時 間で, 患児 と
同型のA型RhD(+)の 血液420mlで 交換輸血 を施
行 した. その後24時 間光線療 法を行 つたが, 黄疸は徐
徐にな くな り, 哺乳力 もよ く, 体重増加 も良好で, 生
後14日 目に退院 した. その後, Hb 7.6g/dlと 貧血著
明なため, 生後40日 に, 父親か ら, 50ml輸 血 を2回
施行 した. 哺乳力良好, 体重増 加良好, 黄疸はみ られ
ないが, 顔色が常 に悪 く, 生後3ヵ 月現在, 貧血著明
であ る. 肝臓は, 辺縁のみ触知 するが, 脾臓は触知 し
ない.
検査所見
1) 末血所見:交 換輸血の翌 日の 所 見 で あ るが,
WBC 7,000/mm3, RBC 401×104/mm3, Hb.
国 立東 京 第 二 病 院 The 2nd Tokyo National
Hospital
*小 児 科 Akiko ADACHIHARA
Toshihiko KUROKAWA
Naomi HONMA
Mari OKUBO
Yugo ISHIZUKA
(Hereditary Spherocytosis with Early Jaundice
in the Neonatal Period)
-807-
56 (1980年9月)
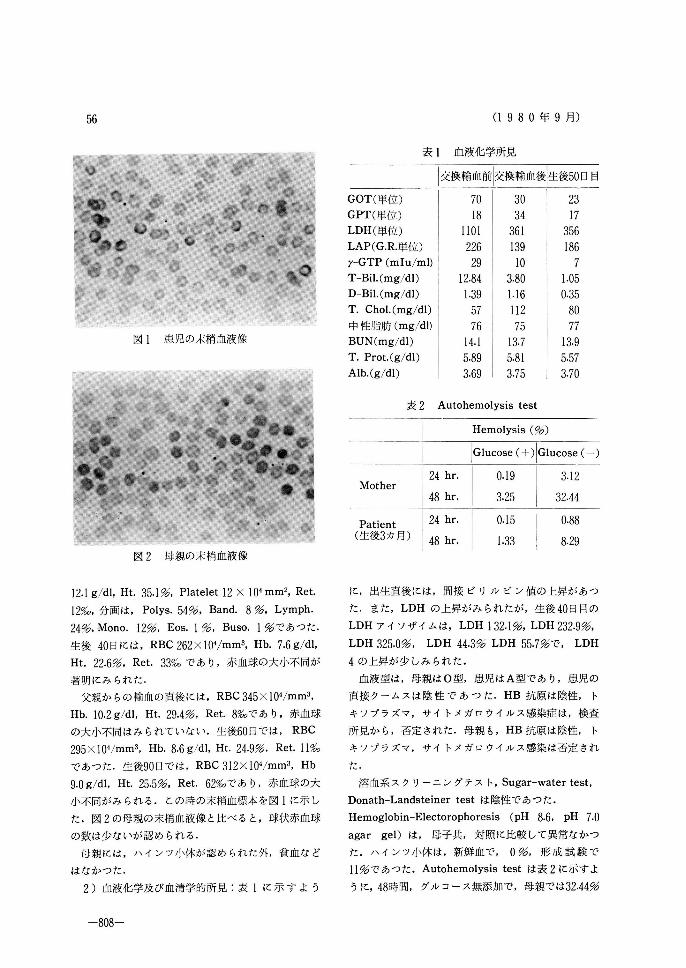
図1 患児の末梢血液橡
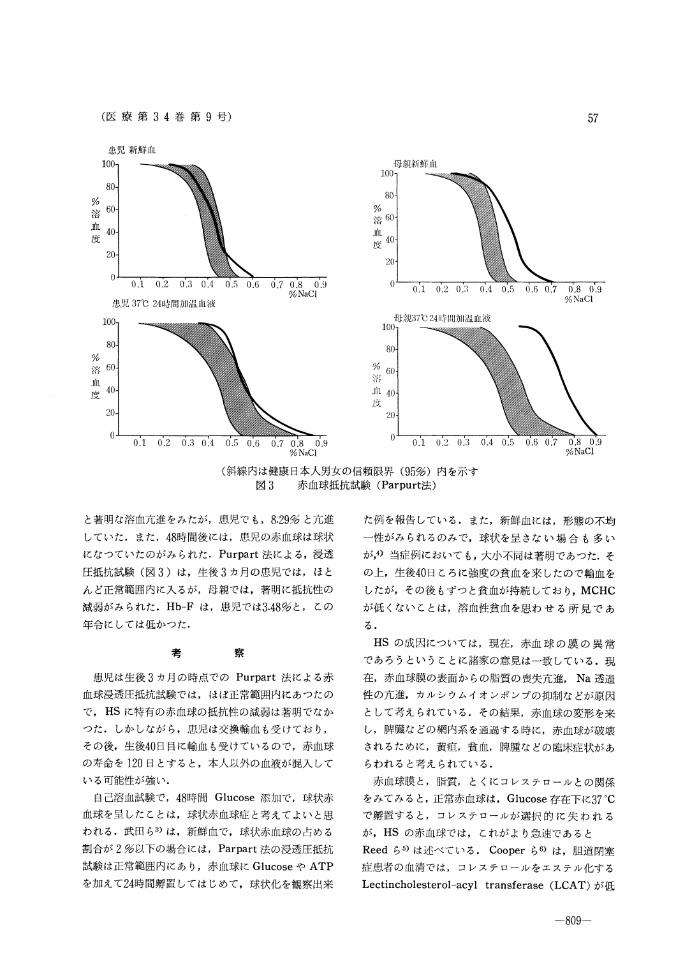
図2 母親の末梢血液像
表1 血液化学所見
表2 Autohemolysis test
12.1g/dl, Ht. 35.1%, Platelet 12×104mm2, Ret.
12‰, 分 画 は, Polys. 54%, Band. 8%, Lymph.
24%, Mono. 12%, Eos. 1%, Buso. 1%で あつ た.
生 後40日 には, RBC 262×104/mm3, Hb. 7.6g/dl,
Ht. 22.6%, Ret. 33‰ で あ り, 赤 血 球 の 大 小不 同が
著 明 に み られ た.
父親 か らの 輸 血 の 直後 には, RBC 345×104/mm3,
Hb. 10.2g/dl, Ht. 29.4%, Ret.8‰ で あ り, 赤血 球
の 大 小不 同 は み られ て い ない. 生 後60日 で は, RBC
295×104/mm3, Hb. 8.6g/dl, Ht. 24.9%, Ret. 11‰
で あ つ た. 生 後90日 で は, RBC 312×104/mm3, Hb
9.0g/dl, Ht. 25.5%, Ret. 62‰ で あ り, 赤 血 球 の大
小 不 同が み られ る. この 時 の 末 梢血 標 本 を図1に 示 し
た. 図2の 母 親 の 末梢 血 液 像 と比 べ る と, 球 状赤 血 球
の 数 は少 ない が 認 め られ る.
母 親 に は, ハ イ ンツ 小体 が 認 め られ た外, 貧 血 な ど
は な か っ た.
2) 血 液 化 学 及 び 血 清学 的 所 見:表1に 示 す よ う
に, 出 生 直後 に は, 間 接 ビ リ ル ビ ン 値 の 上 昇 が あ つ
た. ま た, LDHの 上 昇 が み られ たが, 生 後40日 目の
LDHア イ ソザ イム は, LDH 132.1%, LDH 232.9%,
LDH 325.0%, LDH 44.3% LDH 55.7%で, LDH
4の 上昇 が 少 しみ られ た.
血 液 型 は, 母 親 は0型, 患 児 はA型 で あ り, 患 児 の
直 接 クー ム ス は 陰 性 で あ つ た. HB抗 原 は陰 性, ト
キ ソ プ ラズ マ, サ イ トメ ガ ロ ウ イル ス感 染 症 は, 検 査
所 見 か ら, 否 定 され た. 母 親 も, HB抗 原 は 陰 性, ト
キ ソ プ ラズ マ, サ イ トメ ガ ロ ウ イル ス感 染 は否 定 され
た.
溶血 系 ス ク リー ニ ング テ ス ト, Sugar-water test,
Donath-Landsteiner testは 陰性 で あ つ た.
Hemoglobin-Electorophoresis(pH 8.6, pH 7.0
agar gel)は, 母 子 共, 対 照 に比 較 して 異常 なか つ
た. ハ イ ンツ小 体 は, 新 鮮 血 で, 0%, 形 成 試 験 で
11%で あつ た. Autohemolysis testは 表2に 示 す よ
うに, 48時 間, グ ル コ ー ス無 添 加 で, 母 親 で は32.44%
-808-
(医 療 第34巻 第9号) 57
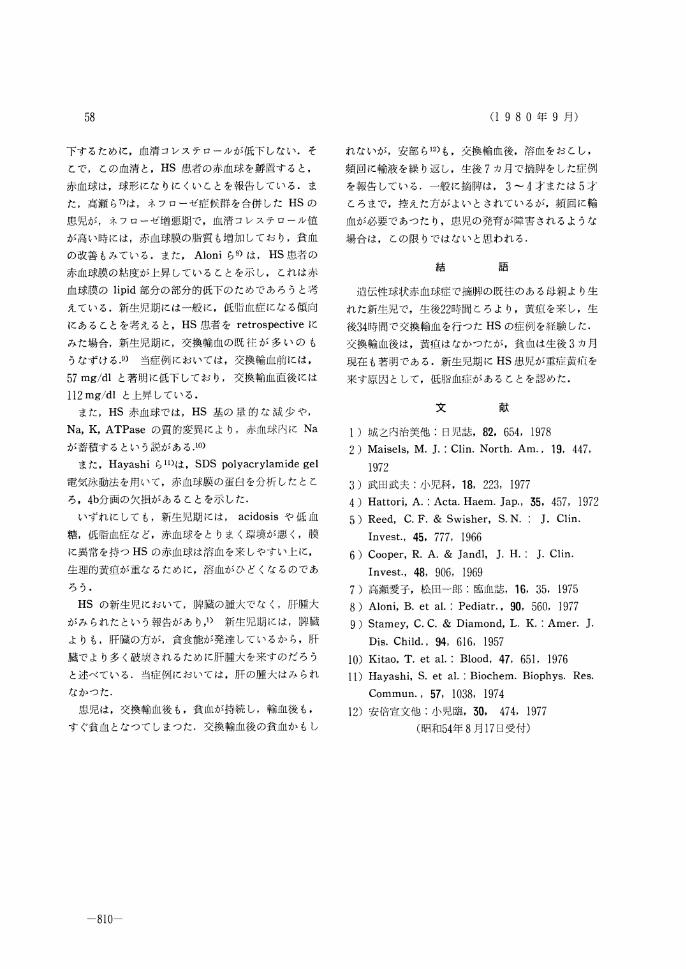
図3 赤血球抵抗試験(Parpurt法)
と著明な溶血元進 をみたが, 患児で も, 8.29%と 亢進
していた. また, 48時 間後には, 患児の赤血球は球状
になつていたのが み られた. Purpart法 による, 浸透
圧抵抗試験(図3)は, 生後3ヵ 月の患児では, ほ と
ん ど正常範 囲内に入 るが, 母親で は, 著明に抵抗性の
減弱がみ られた. Hb-Fは, 患児では3.48%と, この
年令に しては低かつた.
考 察
患児は生後3ヵ 月の時点でのPurpart法 による赤
血球浸透圧抵抗試験では, ほぼ正常範囲内にあつたの
で, HSに 特有の赤血球の抵抗性の減弱は著 明でなか
つた. しか しなが ら, 患児は交換輸血 も受 けてお り,
その後, 生後40日 目に輸血 も受 けてい るので, 赤血球
の寿命を120日 とす ると, 本人以外の血液が混入 して
い る可能性が強い.
自己溶血試験で, 48時 間Glucose添 加で, 球状赤
血球を呈 したことは, 球状赤血球症 と考えてよい と思
われ る. 武 田 ら3)は, 新鮮血 で, 球状赤血球 の占める
割合が2%以 下の場合には, Parpart法 の浸透圧抵抗
試験は正常範囲内にあ り, 赤血球 にGlucoseやATP
を加 えて24時 間孵置 してはじめて, 球状化 を観察出来
た例 を報告 してい る. また, 新鮮血 には, 形 態の不均
一性がみ られ るのみで, 球状 を呈 さな い場 合 も多 い
が,4) 当症 例において も, 大小不同は著明であつた. そ
の上, 生後40日 ころに強度 の貧血 を来 したので輸血 を
したが, その後 もずつ と貧血が持続 してお り, MCHC
が低 くない ことは, 溶血性貧血 を思わ せ る所 見 で あ
る.
HSの 成 因については, 現在, 赤血 球 の膜 の 異 常
で あろうとい うことに諸家の意見 は一致 してい る. 現
在, 赤血球膜の表面か らの脂質 の喪失亢進, Na透 過
性の亢進, カル シウムイオ ンポンプの抑制な どが原因
として考え られている. その結果, 赤 血球の変形 を来
し, 脾臓な どの網内系 を通過す る時に, 赤血球が破壊
され るために, 黄疽, 貧血, 脾腫な どの臨床症状が あ
らわれ ると考 え られ ている.
赤血球膜 と, 脂質, と くに コレステ ロールとの関係
をみてみると, 正常赤血球は, Glucose存 在下 に37℃
で孵置す ると, コレステロールが選択 的 に失 わ れ る
が, HSの 赤血球では, これが よ り急速であ ると
Reedら5)は 述べ ている. Cooperら6)は, 胆道閉塞
症患者 の血清では, コレステ ロールをエステル化す る
Lectincholesterol-acyl transferase(LCAT)が 低
-809-
58 (1980年9月)
下するために, 血清 コレス テロールが低下 しない. そ
こで, この血清 と, HS患 者の赤血球を孵置す ると,
赤血球は, 球形にな りに くいことを報告 している. ま
た, 高瀬 ら7)は, ネフローゼ症 候群 を合併 したHSの
患児が, ネフローゼ増 悪期で, 血清 コレステ ロール値
が高い時には, 赤血球膜 の脂質 も増加 してお り, 貧血
の改善 もみてい る. また, Aloniら8)は, HS患 者 の
赤血球膜 の粘度が上昇 していることを示 し, これは赤
血球膜のlipid部 分の部分的低下の ためで あろうと考
えてい る. 新生児期には一般 に, 低脂血症 にな る傾 向
にあることを考 えると, HS患 者 をretrospectiveに
みた場合, 新生児期に, 交換輸血 の既 往 が 多 い の も
うなずけ る.9) 当症例においては, 交換輸血前には,
57mg/dlと 著明に低下 してお り, 交換輸血直 後には
112mg/dlと 上昇 している.
また, HS赤 血球では, HS基 の 量 的 な 減 少 や,
Na, K, ATPaseの 質 的変異 によ り, 赤血球内にNa
が蓄積す るとい う説があ る.10)
また, Hayashiら11)は, SDS polyacrylamide gel
電気泳動法を用 いて, 赤血球膜の蛋白を分析 したとこ
ろ, 4b分 画の欠損があることを示 した.
いずれ にして も, 新生児期 には, acidosisや 低 血
糖, 低脂血症な ど, 赤血球 をと りま く環境が悪 く, 膜
に異常 を持つHSの 赤血球 は溶血 を来 しやすい上 に,
生理的黄疸が重な るために, 溶 血が ひど くな るのであ
ろう.
HSの 新生児 において, 脾臓の腫大でな く, 肝腫大
がみ られたとい う報告があ り,1) 新生児期には, 脾 臓
よりも, 肝臓の方 が, 貧食能が発達 してい るか ら, 肝
臓でよ り多 く破壊 されるために肝腫大 を来すのだろ う
と述べ てい る. 当症 例においては, 肝の腫大はみ られ
なかつた.
患児は, 交換輸血後 も, 貧 血が持続 し, 輸血後 も,
す ぐ貧血 となつて しまつた. 交換輸血後の貧血か もし
れないが, 安部 ら12)も, 交換輸血後, 溶血 をおこし,
頻回に輸液を繰 り返 し, 生後7ヵ 月で摘脾 を した症例
を報告 してい る. 一般 に摘脾は, 3~4才 または5才
ころまで, 控 えた方が よいとされてい るが, 頻 回に輸
血が必要であつた り, 患児の発育が障害 されるような
場合 は, この限 りではないと思われ る.
結 語
遺伝性球状赤血球症 で摘脾の既往の ある母親よ り生
れた新生児で. 生後22時 間 ころよ り, 黄疸を来 し, 生
後34時 間で交換輸血 を行つたHSの 症例 を経験 した.
交換輸 血後 は, 黄疽はなかつたが, 貧 血は生後3ヵ 月
現在 も著 明である. 新生児期 にHS患 児が重症黄疸 を
来す原 因 として, 低脂血症が ある ことを認めた.
文 献
1) 城之内治美他:日 児誌, 82, 654, 1978
2) Maisels, M. J.:Clin. North. Am., 19, 447,
1972
3) 武 田武 夫:小 児科, 18, 223, 1977
4) Hattori, A.:Acta. Haem. Jap., 35, 457, 1972
5) Reed, C. F. & Swisher, S. N.:J. Clin.
Invest., 45, 777, 1966
6) Cooper, R. A. & Jandl, J. H.:J. Clin.
Invest., 48, 906, 1969
7) 高 瀬 愛 子, 松 田一 郎:臨 血 誌, 16, 35, 1975
8) Aloni, B. et al.:Pediatr., 90, 560, 1977
9) Stamey, C. C. & Diamond, L. K.:Amer. J.
Dis. Child., 94, 616, 1957
10) Kitao, T. et al.:Blood, 47, 651, 1976
11) Hayashi, S. et al.:Biochem. Biophys. Res.
Commun., 57, 1038, 1974
12) 安 倍 宣 文 他:小 児 臨, 30, 474, 1977
(昭 和54年8月17日 受 付)
-810-


















![Anesthetic Management of Delivery in Women With Pregnancy[1]](https://img.pdfslide.net/doc/110x75/577cd0a11a28ab9e7892b646/anesthetic-management-of-delivery-in-women-with-pregnancy1.jpg)