-
7/28/2019 Abraxis Initiation Merriman Sept 09
1/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
September 15, 2009
Abraxis BioScience (ABII) Buy
The Billion Dollar Cancer Company the Street Forgot;
InitiatingCoverage With a Buy Rating
Abraxis BioScience has been off the Streets radar screen for
several
years, due to a number of factors, including a controversial
shareholderwith a dominant equity position, a split with former
marketing partner, Astra-Zenecaand flat U.S. sales of Abraxane. As
a result, the shares are down bymore than 50% year to date, and
average daily volume is a mere 40,000shares. The stock has zero
sell-side coverage.
The good news: new management is in place, ex-U.S. territories
are
coming on stream, and additional Abraxane indications should
beforthcoming. In April of 2009, Abraxis named Lonnie Moulder to
the positionof President and CEO. Moulders previous company, MGI
Pharma, successfullydeveloped and launched the anti-nausea drug,
Aloxi. MGI was then sold for$3.9B in cash in 2008.
Despite the companys past turmoil, we believe the stocks
valuation
more than accounts for past transgressions, and the future looks
in-teresting to us. In our opinion, operational execution could
double Abraxanesales by 2013 as the EU and China territories come
on line. In addition,Abraxis is conducting three ongoing
registration trials of Abraxane; a read-out
of the NSCLC study should happen before year end. In the
meantime, thestock has a technology value of approximately $750M,
3x annualized sales,and 1x the product NPV. The company ended 2Q09
with $258M in cash, suffi-cient to fund operations for the
foreseeable future. Finally, Abraxis owns100% of the worldwide
rights to Abraxane, and would be an attractive acqui-sition
candidate for a large pharma or biotech company looking to augment
itsanti-cancer drug portfolio. We are therefore initiating coverage
with a Buyrating and are establishing a price target range of
$30-33 based on our FY13EPS estimate of $0.74, fully taxed, fully
diluted, and discounted back by 9%for three periods.
Abraxis BioScience, Inc., a biotechnol-ogy company, engages in
the discov-ery, development and delivery of next-generation
therapeutics and core tech-nologies that offer treatments for
can-
cer and other critical illnesses. Thecompanys product pipeline
includesclinical oncology and cardiovascularproduct candidates in
various stages oftesting and development. Its principalproduct
includes Abraxane, a nanopar-ticle chemotherapeutic compound thatis
based on its proprietary tumor tar-geting nab technology platform
for thetreatment of metastatic breast cancer.The company was
formerly known asNew Abraxis, Inc. and changed itsname to Abraxis
Bioscience, Inc. inNovember 2007. Abraxis BioScience isbased in Los
Angeles, California.
Market Cap (M): $1,086
Shares Out. (M): 40.1
Float (M): 26.6
10-Day Avg. Vol.: 60,741
Institutional Ownership: 55.4%
Enterprise Value (M): $807
MCF Estimates
Market Data
Stock Performance
Company Description
Valuation (FY09E)
Key MetricsPrice: $27.07
Rating: Buy
52-Week Range: $24.52-74.50
Book Value/Share: $22.17
Debt/Capital: 0%
Debt (M): $0
Cash (M): $258
EV/Sales: N/M
PE Ratio: N/M
Summary
Investment Conclusion
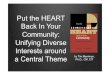
Source: BigCharts.com
Shares of Abraxis BioScience have lost more than half their
value over the past12 months. This is attributable to several
factors, including a split with formermarketing partner,
Astra-Zeneca, and flat U.S. sales of, Abraxane. In our view,the
worst is behind the company and the tide is about to turn for the
shares.Fundamentals have begun to improve, new management is in
place, and piv-otal Phase III Abraxane data in NSCLC should read
out by the end of 2009. TheU.S. sales machine is being fixed, and
Abraxane is launching in China and theEU. Meanwhile, the stock
trades with an enterprise value of approximately$800M, or 2.4x FY09
annualized sales. Abraxis owns all the worldwide rights
toAbraxane.
FY08A FY09E FY10E
SALES (M)
1Q $82.1 $72.6 $93.1
2Q 77.6 85.1 A 97.5
3Q 93.4 84.6 102.0
4Q 92.2 88.3 106.5
FY (Dec) $345.3 $330.6 399.1
EV/S 2.3X 2.4X 2.0X
EPS
1Q $0.09 ($0.63) ($0.50)
2Q (2.13) (0.56)A (0.44)
3Q (0.40) (0.53) (0.42)
4Q (4.56) (0.47) (0.42)
FY (Dec) ($6.93) ($2.20) ($1.77)
P/E N/M N/M N/M
Michael G. King, Jr.Managing Director(646)
[email protected]
MERRIMAN CURHAN
FORD
600 California Street9th FloorSan Francisco, CA 94108(415)
248-5600 Main(415) 248-5690 Fax(800) 909-7897
Tradingwww.mcfco.com
NASDAQ: MERR
Member FINRA/SIPC
Please seeImportantDisclosures on thelast page of
thisreport.
-
7/28/2019 Abraxis Initiation Merriman Sept 09
2/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 2
Table of Contents
Investment ThesisThe Billion Dollar Company the Street
Forgot.....3Company Background: The Cult of Personality.. 3
Investment Risks.. 3
Upcoming Milestones... 4
Company Background.... 5
History is History, The Next Twelve Months Should be
Critical....5
Abraxane: Why Use Anything
Else?.................................................................
6
Breast Cancer: Where Abraxane Earned its Stripes...6
Abraxane Again Proves its Worth in a Head-to-Head Trial Against
Taxotere...9
Data Equals Market Share in Cancer Therapy...12
Let The Data Flow: Abraxane Has a Busy Clinical Trials
Calendar..19
Abraxane Phase III Trials: One Ace in the Hole, Two
Wildcards.... 19
Abraxis PipelineLots Going On Internally and Externally.19
NAB Technology Platform-Big things Come in Small Packages.11
Valuation... 22
Summary and Conclusion. 22
Appendices:A. Senior Management. 23
B. Disease Overview.. 25
C. Compendia Listings.. 27
Figures:
1. Response Rates in Abraxane vs Paclitaxel in Metastatic Breast
Cancer.. 72. Time to Progression in Abraxane vs Paclitaxel in
Metastatic Breast Cancer.7
3. Patient Survival in Abraxane vs Paclitaxel in Metastatic
Breast Cancer.. 8
4.Adverse Events in Phase III Trial of Abraxane vs Standard
Paclitaxel.. 9
5. Confirmed ORR and DCR in Abraxane vs Docetaxel. 10
6. Progression-Free Survival in Abraxane vs Docetaxel.. 117.
Kaplan Meier of PFS curve in Abraxane vs Docetaxel..11
8. Estimated Number of Patients on Abraxane in July 2009.13
9. Estimated Number of Patients on Abraxane on Rolling 12-Month
Average Basis.13
10.Abraxane Revenue Model... 14
11.Abraxane Revenue Build in Metastatic Breast Cancer in the
United States.. 15
12.Abraxane Revenue Build in Metastatic Breast Cancer in the
European Union. 16
13. Abraxane Revenue Build in Metastatic Breast Cancer in China.
17
14.Abraxane Revenue Build in Metastatic Breast Cancer in Rest of
World.18
15.Abraxis BioScience Pipeline.20
16. nab-Particle Diagram.. 21
18. Newly Diagnosed Pancreatic Cancer Cases by Stage.. 26
Income Statement.. 29
Balance Sheet.. 30
8. Annual Taxane Treatments...12
17. nab-Platform.. 21
-
7/28/2019 Abraxis Initiation Merriman Sept 09
3/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 3
Investment Thesis
Abraxis BioScience is a commercial biopharmaceutical company
that markets its only commercial compound,Abraxane, in 36 countries
around the world. The product was approved in the US in January of
2005 for thetreatment of metastatic breast cancer. The shares are
undervalued, in our opinion, based on investor disap-pointment with
managements prior performance and essential control over the
company by principal share-holder, Patrick Soon-Shiong, who owns
over 80% of the equity. However, we believe the company has
aproduct that is fundamentally sound and is approaching several key
sales and clinical catalysts. Moreover, anew management team is in
place that has a demonstrated track record of execution and
eventual sale of aprevious company (MGI Pharma). When juxtaposed
against the undervalued nature of the stock (trading
atapproximately 1x the Abraxane NPV) and lack of Street following,
we find the Abraxis story compelling. Weare therefore initiating
coverage with a Buy rating and a price target range of $30-33.
In our view, the key to the stocks appreciation will be
operational execution, as well as clarity on the strate-gic risks
and benefits of the soon-to-be-spin-off company, Abraxis Health. We
also anticipate that LonnieMoulder, recently-appointed CEO, will
increase the companys visibility in the eyes of the investment
commu-
nity, thereby highlighting the opportunity in the companys
stock. Furthermore, the upcoming spin off ofAbraxis Health should
help investors get a clearer picture of the true operations of
Abraxis BioScience, andpotentially result in a higher
valuation.
Company Background: The Cult of Personality
In the biotechnology space, there are companies that are
controversial, and then there are companies thatare controversial.
We would submit that Abraxis BioScience falls into the latter
category. Until recently,Abraxis was run by the enigmatic Patrick
Soon-Shiong. Dr. Soon-Shiong is the son of a family doctor from
arural Chinese village. The family immigrated to South Africa
during World War II. He finished high school byage 16 and became a
doctor himself by age 23. He took American Pharmaceuticals Partners
public in 2001.After the successful development of Abraxane, he
split the company in two in 2007; APP Pharmaceuticalssold
hospital-based products while Abraxis BioScience developed
proprietary drugs (mostly Abraxane). APPPharmaceuticals was sold to
Fresenius in 2007 for $5.6 billion in a transaction that netted
Soon-Shiong $3billion. When the shares of American Pharmaceuticals
Partners (also referred to as Old Abraxis) were split in2007,
shareholders of APP received one share of Abraxis BioScience for
every four shares of Old Abraxis. Aheated debate accompanied the
terms of the split of Abraxis from APP for the minority
shareholders, asSoon-Shiong was the majority shareholder in both
the old and the new company. The transaction ultimatelywas approved
and closed in 2007. Despite concerns that arose over the
objectivity of the value placed onboth assets, the sale of APP to
Fresenius resulted in the creation of significant value for
all.
Soon-Shiong has now stepped aside as Chairman and CEO of Abraxis
and turned these duties over to LonnieMoulder, who investors may
recall was President and CEO of MGI Pharma. MGI was sold to Eisai
Pharmaceu-ticals of Japan, with the transaction closing in early
2008. Moulder joined Abraxis in April of 2009; subse-quently, three
members of Moulders former MGI Pharma management team, Marty
Duvall, Rick Rodgers,and Mary Lynne Hedley, have also come on
board.
Investment Risks
Shares of Abraxis are closely-held, and there is a single
dominant shareholder. As mentioned,Patrick Soon-Shiong owns more
than 80% of the equity of Abraxis. Therefore, he controls
essentially thecompanys entire decision making process. Shareholder
approval is a fait accompli for all major strategicdecisions.
Further, despite his move to Abraxis Health, Soon-Shiong may still
influence the decisionsmade at Abraxis BioScience.
The shares of Abraxis BioScience are illiquid, and therefore can
be volatile in both directions.Recent data indicates that average
daily volume is just over 40,000 shares per day. Our understanding
isthat much of the downward pressure on the shares so far this year
stems from a small number of share-
-
7/28/2019 Abraxis Initiation Merriman Sept 09
4/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 4
holders seeking to reduce their positions. The downward price
movement may be exacerbated by thelack of liquidity in the
stock.
Abraxis is a single-product company. Despite our enthusiasm over
the outlook for Abraxane growth,the fortunes of the company rise
and fall with Abraxane. The taxane market is highly competitive,
andTaxol (paclitaxel) is now a generic drug with multiple
suppliers. The cancer field is under tremendouseconomic pressure to
reduce the use of expensive therapies, and the current cost of a
cycle of Abraxanecould come under scrutiny.
Alternative formulations of paclitaxel are being explored. While
none have passed Phase III trialsand a proprietary vitamin-E based
formulation of paclitaxel from Sonus Pharmaceuticals failed a
PhaseIII trial, there are still a number of novel taxane
formulations are under development by a number ofparties.
Investor due-diligence will likely turn up few key opinion
leaders with a favorable point ofview of Abraxane. While our due
diligence checks have never turned up a negative comment on
Abrax-ane from a member of the thought-leader community, the
reaction has been more of a ho-hum re-
sponse. Thought leaders find the science behind Abraxane to be
mundane, and are usually more inter-ested in novel cytotoxic or
targeted therapy compounds. This clearly has not stopped the
widespreadadoption of Abraxane amongst community oncologists, who
find its tolerability and ease of infusion to bea significant
benefit to their patients.
Abraxis Health spin-off could raise concerns about BioSciences
financial commitment to thecorporate offspring. In addition to
providing Abraxis Health with $25 million of its cash, BioScience
willalso provide Abraxis Health with access to a $200 million line
of credit. This may raise concerns regard-ing whether BioScience is
taking on too much financially or managerially, or may raise
concerns aboutthe use of BioSciences cash which has been reduced to
approximately $225 million from $700 million in2007.
Operating margins are well below industry norms. Please see our
full margin analysis for additionaldetail. However, despite gross
margins that are in line with those seen at other major
biotechnologycompanies, Abraxiss operating margins are well below
the norm. This is because the companys SG&A
levels are double or triple the norm for the industry. If the
company cannot succeed in bringing thesemore in line with those in
the industry, the shares may continue to lag.
Litigation overhang. In June of 2008, Abraxis announced that it
intended to appeal a jury verdict thatfound Abraxis as infringing a
patent held by Elan that covers nanoparticle anticancer agents
(U.S. patentnumber 5,399,363) . The jury awarded Elan damages of
$55 million, and Abraxis has accrued $57.4 mil-lion to meet this
liability if the appeal ultimately fails.
Upcoming Milestones
According to managements projections:
Launch Abraxane in China and Korea
Continue Abraxane rollout throughout Europe
Complete Phase III trial of Abraxane in non-small cell lung
cancer and report top-line results
Complete enrollment in registration trials of Abraxane in
melanoma and pancreatic cancer
Complete spin-out of Abraxis Health
-
7/28/2019 Abraxis Initiation Merriman Sept 09
5/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 5
Company Background
There are some stocks that have stories, and there are others
that have STORIES. Abraxis is a company inthe latter category.
Charismatic and controversial Executive Chairman, Patrick
Soon-Shiong, MD, built thecompany nearly single-handedly over the
last decade. Started as a manufacturer of generic drugs (the
twopredecessor companies to Abraxis were known as American
Bioscience and American Pharmaceutical Part-ners), the turning
point in the companys history came with the licensure of Abraxane,
an albumin-boundtaxane molecule that received approval in January
of 2005 for the treatment of metastatic breast cancer.Many
investors were skeptical at the time of Abraxanes approval, as the
study was designed for non-inferiority to Taxol (paclitaxel), a
design that the FDA typically discourages. Abraxane did, however,
producea significantly higher response rate compared to
conventional paclitaxel, and had a superior side effect pro-file,
and the drug was approved under the FDAs 505 (b)2 pathway.
The company has also had fits and starts with previous CEOs and
corporate partner relationships. Moulderwas proceeded by at least
three other erstwhile CEOs with large pharma experience, who
subsequently leftthe company. As we mentioned previously, the
Abraxane marketing relationship with Astra-Zeneca wasshort-lived.
There has also been investor speculation that a sale process of
Abraxis may have taken placewithin the past years time. If this is
true, the lack of a buyer at a significant premium may be the
reason theshares have been so severely punished since late
February.
History is History, the Next Twelve Months Should be
Critical
Given the drama in the companys past, why would we in good
conscience recommend the purchase of ABIIshares at this point in
time? Two words: value and change. We enumerate our reasons for our
positiveoutlook on the stock.
Valuation is compelling by most metrics. As a loss-making
enterprise, Abraxis BioScience cannot bemeasured on a P/E or PEG
basis like its large-cap peers. However, by other traditional
biotech marketvaluation metrics, we find the shares compelling. At
current prices, Abraxis has a market cap of approxi-mately $1.1
billion. After deducting net cash (cash minus debt, or in this case
$258 million in cash vs.
zero debt), the enterprise value is $807 million. If we
annualize the companys revenue run-rate to dateof approximately
$300 million, this leaves us with an enterprise value to revenue
ratio of less than 3.This compares favorably to the large cap peer
group from the Merriman Biotech Balance Sheet whichcurrent trades
at and EV/Sales ratio of 6.5. According to our analysis of M&A
transactions over the pastfive years suggests product and company
acquisitions in the 5-6x sales on average and values as high as10x
sales in certain transactions that were highly competitive.
Change in management critical to unlocking unrealized value. In
our view, one of the keys to theunlocking of unrealized value in
Abraxis shares is through the recent changes in management. Our
per-spective on why this time the change in Abraxis may be
different this is time is based on two factors:first, Patrick
Soon-Shiong is devoting his entire management time to Abraxis
Health; second, LonnieMoulder has joined the company and brought
members of his previous team from MGI Pharma alongwith him. The
assemblage of this team is reminiscent of those that ran Peninsula
Pharmaceuticals as wellas Allos Therapeutics, both of whom sold
their companies to large pharma/biotech acquirers.
Abraxane has franchise value. While Abraxane is not the sexiest
product from a technology perspec-tive, what is attractive to large
pharma and biotechnology companies is an established sales base and
aworldwide reach. One company that comes to mind is Johnson and
Johnson, which owns worldwiderights to Doxil, a
liposome-encapsulated version of the generic drug, doxorubicin.
J&J acquired theserights when it acquired Alza, a specialty
pharmaceutical company with novel drug-delivery technology.J&J
also has ex-U.S. rights to Velcade, the proteasome inhibitor
developed by Millennium Pharmaceuti-cals, now owned by Takeda. We
would submit that Abraxane is analogous to both products; Abraxane
isa unique formulation of a generic drug, with differentiated
therapeutic properties like those of a proprie-tary drug.
-
7/28/2019 Abraxis Initiation Merriman Sept 09
6/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 6
We believe operating margins have nowhere to go but up. We point
out that Abraxiss SG&A levelsare amongst the highest as a
percentage of revenue of nearly any company with which we are
familiar,with the exception of those that are in launch mode. In
contrast, Abraxis is a company with a productthat is well past this
stage, although is by no means mature (please see our comparative
margin analysisbelow). The good news is that, for every 1%
improvement in SG&A expense, approximately $0.15 can beadded to
Abraxiss bottom line. We urge management to do all in its power to
reduce expenses and per-mit a greater percentage of Abraxane
revenue to flow to the bottom line.
Abraxis Health spin-off could result in a higher multiple for
BioScience . While it is still early andwe will not spend a lot of
time in this report discussing it, the proposed spin-off of Abraxis
Health mayultimately have a beneficial impact on how investors
value Abraxis BioScience. Since BioScience will bemore of a
pure-play after the spin-off, the shares may be afforded a higher
multiple of sales and earn-ings (assuming eventual profitability).
The full set of Abraxis Health documents that have been producedto
date can be found at the following url:
http://www.sec.gov/cgi-bin/browse-edgar?action=getcompany&CIK=0001452016&owner=exclude&count=40
Abraxane: Why Use Anything Else?
Abraxane, formerly referred to as ABI-007 and nab-paclitaxel,
uses Abraxiss proprietary nano-particle tech-nology to improve both
the safety and efficacy of paclitaxel (Taxol). Because it obviates
the need to use thesolvent, Cremophor EL, the drug can be infused
rapidly, generally within 30 minutes, compared to threehours for
conventional paclitaxel. Unlike paclitaxel, which requires special
tubing, Abraxane uses conven-tional iv tubing for the drugs
administration. Further, Cremophor EL is formulated with ethanol
and togetherthey form the vehicle in which the Taxol is carried.
Data has begun to emerge that the solvent is the sourceof much of
Taxols toxicity. Head to head clinical data suggests that Abraxane
not only lacks much of the tox-icity of the taxanes, but in many
cases has been shown to have superior efficacy as well. We will
discussthese data below.
Breast Cancer: Where Abraxane Earned its StripesThe pivotal
clinical trial that supported the FDA approval of Abraxane was
published in the November 1,2005, Journal of Clinical Oncology. The
principal investigator of the trial was William Gradishar from
North-western University in Chicago. Dr. Gradishar is one of the
more widely-accomplished clinicians in the breastcancer space,
having done work with hormone therapy and Herceptin in the past. He
has also proven to be agreat champion for Abraxane.
The study was unusual in the sense that it took multiple
sub-types of patients with metastatic breast cancer.There were
approximately an equal proportion of patients who were treated in
the study for first and secondline MBC, and patients with multiple
lines of prior therapy were also allowed in the study (42% first
line,41% second line, 10% third line and 7% beyond third line). The
study successfully achieved its primary end-point of a superior
response rate to that of polyethylated castor-oil (Cremophor) based
paclitaxel (please seeTable 1 for details). Overall, 33% of
patients achieved a response to Abraxane, while 19% did so to
conven-tional paclitaxel. Use of Abraxane was also associated with
a statistically significant improvement in time to
tumor progression (TTP), 23 vs. 17 weeks). Despite the fact that
patients were receiving a 49% higher doseof paclitaxel in the
Abraxane arm, the side effect of Grade 4 neutropenia (low white
blood cell count) wasskewed significantly in favor of the Abraxane
patients (9% vs. 22%). Grade 3 sensory neuropathy (tinglingand
numbness in the extremities) was the most significant side effect
that went against Abraxane; however,the symptoms typically resolved
within three weeks. Finally, no hypersensitivity reactions were
seen despitethe absence of pre-medication in the Abraxane-treated
arm of the trial. We discuss each of these aspectsbelow.
-
7/28/2019 Abraxis Initiation Merriman Sept 09
7/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 7
Figure 1: Response Rates in Abraxane vs. Paclitaxel in
Metastatic Breast Cancer
Source: Gradishar et al. Phase III Trial of Nanoparticle
Albumin-Bound Paclitaxel Compared with Polyethylated Castor
Oil-Based Paclitaxelin Women with Breast Cancer, J Clin Oncol.
2005
As can be seen, the Abraxane-treated patient population achieved
superior response rates irrespective ofwhich line of therapy they
received. In fact, we highlight the fact that Abraxane produced
responses in thesecond line setting that equaled those of
paclitaxel in the front-line setting. The response benefit was
alsoconsistently seen irrespective of whether anthracycline drugs
had been previously received, dominant metas-tatic organ site, or
age. The statistics in some subgroups did not achieve significance
because of small num-bers.
Figure 2: Time to Progression in Abraxane vs. Paclitaxel in
Metastatic Breast Cancer
Source: Gradishar et al. Phase III Trial of Nanoparticle
Albumin-Bound Paclitaxel Compared with Polyethylated Castor
Oil-Based Paclitaxelin Women with Breast Cancer, J Clin Oncol.
2005
The TTP numbers clearly favor Abraxane and are highly
significant. The curves separate early (betweenweeks 16 and 24, and
stay separated even way out in the tail of the Kaplan-Meier
curve.
ABI-007 (260 mg/m ) Standard Paclitaxel (175 mg/m )# of
patients/ # of patients/
Response Total # of patients % 95% CI (%) Total # of patients %
95% CI (%) p
Complete and partial response
All Patients 76/229 33 27.09 to 39.29 42/225 19 13.58 to 23.76
0.001
First-line therapy 41/97 42 32.44 to 52.10 24/89 27 17.75 to
36.19 0.029
Second-line or greater therapy 35/132 27 18.98 to 34.05 18/136
13 7.54 to 18.93 0.006
Prior anthracycline therapy
Adjuvant and/or metastatic 60/176 34 27.09 to 41.09 32/175 18
12.56 to 24.01 0.002
Metastatic only 31/115 27 18.85 to 35.07 18/130 14 7.91 to 19.78
0.01
Dominant metatstatic organ site
Visceral 59/176 34 26.55 to 40.50 34/182 19 13.02 to 24.34
0.002
Nonvisceral 17/50 34 20.87 to 47.13 8/43 19 6.97 to 30.24 NS
Age, years
< 65 68/199 34 27.58 to 40.76 36/193 19 13.16 to 24.16
-
7/28/2019 Abraxis Initiation Merriman Sept 09
8/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 8
Figure 3: Patient Survival in Abraxane vs Paclitaxel in
Metastatic Breast Cancer
Source: Gradishar et al. Phase III Trial of Nanoparticle
Albumin-Bound Paclitaxel Compared with Polyethylated Castor
Oil-Based Paclitaxelin Women with Breast Cancer, J Clin Oncol.
2005
Notes: (A) Patient survival over time (B) Patient Survival over
time in patients who received second-line or greater therapy. P
values fromlog-rank test. Survival indicates time from first dose
of study drug to date of death.
The administration of Abraxane produces a robust improvement in
patient survival (p=0.024) in patients re-ceiving the drug in the
second-line MBC setting. The magnitude of benefit is clearly less
in the first line set-ting; however, this may be due to the paradox
seen in trials of agents in first-line MBC, as patient crossoverto
second-line therapies tends to have a confounding effect on
mortality outcomes (e.g., Avastin).
-
7/28/2019 Abraxis Initiation Merriman Sept 09
9/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 9
Figure 4: Adverse Events in Phase III Trial of Abraxane vs
Standard Paclitaxel
Source: Gradishar et al. Phase III Trial of Nanoparticle
Albumin-Bound Paclitaxel Compared with Polyethylated Castor
Oil-Based Paclitaxelin Women with Breast Cancer, J Clin Oncol.
2005
Notes: (A) Adverse events (all grades) reported in more than 20%
of patients in either treatment group. ANC, absolute neutrophil
count.(B) Treatment-related grade 3 and 4 adverse events reported
in 5% of patients in either group. Data are based on adverse event
report-
ing. (*) P < .05, Cochran-Mantel-Haenszel test. GGT - gamma
glutamyl transferase
The adverse event profile of Abraxane is clearly superior to
that of conventional paclitaxel, as illustrated bythe chart above.
Abraxane clearly produces lower neutropenia, with less than half
the rate of Grade 4 neu-tropenia. Abraxane appears to be somewhat
worse on the CNS-mediate side effects such as sensory neu-ropathy,
fatigue, arthralgia and myalgia. However, as we pointed out before,
sensory neuropathy resolveswithin three weeks (see Figure 4 above).
The incidence of the other side effects, while greater than those
ofpaclitaxel, occur at relatively low rates and were transient in
nature.
From a product label perspective, Abraxis is only able to cite
its response rate relative to paclitaxel from anefficacy
standpoint. The side effect profile of both drugs is described in
great detail, providing the Abraxissalesforce with a compelling
safety data set over which to engage treating physicians.
Abraxane Again Proves its Worth In a Head-to Head Trial Against
Taxotere
In June of 2009, Abraxis and its clinical investigators, led by
Dr. Gradishar, published the results of a PhaseII head-to-head
trial of three different doses and two regimens (100mg/m2 or
150mg/m2 or every week or300mg/m2 every three weeks) of Abraxane
against Taxotere (docetaxel) given at the conventional dose
of100mg/m2 every three weeks. These results were published in the
August 1, 2009, edition of the Journal ofClinical Oncology. Again,
this was a metastatic breast cancer patient population; however,
this study wasrestricted to only those patients who were previously
untreated. The results demonstrated that the
150mg/m
2
dose arm of the trial provided a statistically significant
improvement in progression-free survival(PFS). This result was seen
whether progression was measured at the clinical site or by an
independent radi-ologist. Response rates as measure by the
independent radiologist in both the 100mg/m2 and the 150mg/m2were
higher than those of docetaxel, but failed to achieve statistical
significance. However, the investigator-assessed response rates
seen with both weekly doses favored Abraxane. Finally, the 300mg/m2
every threeweeks dose regimen failed to show any difference between
itself and docetaxel. As was seen in the registra-tion trials,
Grade 3/4 neutropenia was lower in the Abraxane arm compared to the
docetaxel arm.
-
7/28/2019 Abraxis Initiation Merriman Sept 09
10/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 10
Figure 5: Confirmed ORR and DCR in Abraxane vs Docetaxel
Source: Gradishar et al. Significantly Longer Progression-Free
Survival With nab-Paclitaxel Compared with Docetaxel as First-Line
Therapyfor Metastatic Breast Cancer, J Clin Oncol. 2009
In this data set we highlight the impressive disease control
rate (DCR) of the 150mg/m2 weekly Abraxanedose of 80%, or greater
than a 35% improvement vs. docetaxel. Further, nearly one-third of
patients experi-enced stable disease for 16 weeks or greater,
nearly a 35% improvement vs. docetaxel. It is generally rec-
ognized in the cancer field that stable disease, in addition to
response rates, is predictive of survival.
nab - Paclitaxel300mg/m2 q3w 100mg/m2 Weekly 150mg/m2 Weekly
Docetaxel 100mg/m2
ORR and DCR (n=76) (n=76) (n=74) q3w (n=74) p
Confirmed ORR Overall: .224
No. 28 34 36 26
% 37 45 49 35
95% CI 26.0 to 47.7 33.6 to 55.9 37.3 to 60.0 24.3 to 46.0
PR
No. 27 34 36 26
% 36 45 49 35
CR
No. 1 0 0 0
% 1 0 0 0
DCR Overall: .027; 100 mg/m v D: .009;
No. 52 57 50 43 150 mg/m v D: .017
% 68 75 80 58
95% CI 58.0 to 78.9 65.3 to 84.7 70.6 to 88.9 46.9 to 69.3
SD 16 weeks
No. 24 23 23 17
% 32 30 31 23
Confirmed ORR Overall:
-
7/28/2019 Abraxis Initiation Merriman Sept 09
11/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 11
Figure 6: Progression-Free Survival in Abraxane vs Docetaxel
Source: Gradishar et al. Significantly Longer Progression-Free
Survival With nab-Paclitaxel Compared with Docetaxel as First-Line
Therapyfor Metastatic Breast Cancer, J Clin Oncol. 2009
The 150mg/m2 weekly Abraxane dose produces a PFS benefit that is
both highly significant and clinicallyrelevant. The associated p
value of 0.0065 of the comparison to docetaxel is impressive, as is
the hazardration (HR) of 0.495, indicating a greater than 50%
reduction in events in the Abraxane-treated patientpopulation vs.
that in the doectaxel arm.
Figure 7: Kaplan Meier of PFS curve in Abraxane vs Docetaxel
Source: Gradishar et al. Significantly Longer Progression-Free
Survival With nab-Paclitaxel Compared with Docetaxel as First-Line
Therapyfor Metastatic Breast Cancer, J Clin Oncol. 2009
Here the curves separate early and stay separated throughout the
24 months of follow-up.
nab- Paclitaxel300mg/m2 q3w 100mg/m2 Weekly 150mg/m2 Weekly
Docetaxel 100mg/m2
Variable (n=76) (n=76) (n=74) q3w (n=74) p HR
No. 32 32 34 33
% 42 42 46 45
Median progression-free survival, mos. 11.0 12.8 12.9 7.5
Overall .0498; 150 mg/m2 v D: 0.495
95% CI 150 mg/m2 v D: .0065
Investigator assessment
No. 44 59 36 44
% 57 68 49 59
Median progression-free survival, mos. 10.9 7.5 14.6 7.8
Overall: .008; 100 mg/m2 100 mg/m2 v 150 mg/m2:
v 150 mg/m2: .001; 1.972; 150 mg/m2 v D:
95% CI 8.9 to 14.6 7.2 to 9.3 10.0 to 18.9 6.3 to 11.0 150 mg/m2
v D: 0.12 0.568
Notes :
q3w: Every 3 Weeks D: docetaxel
HR: Hazard ratio
Independent radiologist assessment
Patients who died or experienced progression
Patients who died or experienced progression
-
7/28/2019 Abraxis Initiation Merriman Sept 09
12/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 12
Data Equals Market Share In Cancer Therapy
Figure 8: Annual Taxane Treatments (Data in 000s)
Source: Company reports, Plan A, IMS Global Health Oncology
Analyzer; IntrinsiQ Research, ROW extrapolation from IMS.
Recent market data indicates that docetaxel (Taxotere) had the
highest share amongst the various conven-tional chemotherapeutic
regimens used for first line metastatic breast cancer. In contrast,
Abraxane heldmarket share in the mid-teens overall and the
low-teens in first line MBC. These numbers have been rela-tively
static over the past 18 months. Within the taxane space (paclitaxel
and docetaxel), we can look atAbraxanes market share in two
different ways. In the month of July, data provided to us by the
companyindicates that 35% of patients treated with a taxane
received Abraxane (4795/13727). Breaking these num-bers down
further by treatment line, we find the following:
USA
78
25
34
76
159
Europe
3822
63
68
141
ROW
105
44
34
16
52
Breast NSCLC Ovarian Prostate Other
-
7/28/2019 Abraxis Initiation Merriman Sept 09
13/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 13
Figure 9: Estimated Number of Patients on Abraxane in July
2009
Source: IntrinsiQ.
On a rolling 12-month average basis (August 2008-July 2009),
there were just over 54,000 patients treatedwith a taxane through
all lines of therapy. Of these, just over 17,000 patients (32%)
received Abraxane.Breaking these figures down again as before, we
find the following:
Figure 10: Estimated Number of Patients on Abraxane on Rolling
12-Month Average Basis
Source: IntrinsiQ.
Given that the market share numbers for Abraxane have stayed
relatively stable, why then do we projectgrowth in the U.S. market?
The answer is straightforward: data and promotion. As we mentioned
earlier, webelieve the Gradishar article will help reinforce in the
minds of treating physicians that Abraxane is a trulydifferentiated
taxane from the others. Therefore, we would expect Abraxane to see
increased use in the first
line MBC setting despite the fact that the drug is neither
labeled nor promoted for that indication. Second,the recent
management changes have brought about stability after a tumultuous
two-plus years of its co-promotion agreement with AstraZeneca. In
the brief period of time since the announcement of Abraxiss
re-acquisition of the marketing rights to Abraxane in November of
2008, the size of the salesforce promotingthe drug has gone from
135 down to a low of 75, and only recently returned to a more
normal level of 95.In our view, a focused, motivated salesforce
with a great product to promote is elemental for success.
Par-enthetically, we would add that it is commendable that Abraxane
sales have remained flat during the timethat the salesforce was
undergoing this turmoil. Please see our full Abraxane model for our
projectedgrowth rates.
Line # of Patients1st Line 1,589
2nd Line 1,343
3rd Line 1,863
Line # of Patients
1st Line 5,197
2nd Line 4,528
3rd Line 7,399
-
7/28/2019 Abraxis Initiation Merriman Sept 09
14/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 14
Figure 11: Abraxane Revenue Model
Source: Company reports and Merriman Curhan Ford estimates.
ABRAXANE 1Q09 2Q09 3Q09 4Q09 2009FY 1Q10 2Q10 3Q10 4Q10 2010FY
2011FY 2012FY 2013FY 2014FY 2015FY
Total $71.8 $77.2 $82.6 $86.1 $322.2 $90.6 $94.8 $99.0 $103.3
$387.7 $477.5 $562.7 $652.4 $740.6 $827.3
Growth 26% 23% 20% 20% 20% 23% 18% 16% 14% 12%
Metatstatic Breast Cancer 1Q09 2Q09 3Q09 4Q09 2009FY 1Q10 2Q10
3Q10 4Q10 2010FY 2011FY 2012FY 2013FY 2014FY 2015FY
Total $59.4 $63.5 $66.1 $68.9 $257.8 $72.5 $75.9 $79.2 $82.6
$310.2 $386.8 $461.4 $541.5 $622.1 $703.2
Growth y/y 22% 20% 20% 20% 20% 25% 19% 17% 15% 13%
United States $57.0 $59.8 $61.9 $63.5 $242.2 $65.0 $66.6 $68.3
$69.9 $269.7 $301.2 $333.8 $366.0 $397.6 $425.4
% of total MBC 96% 94% 94% 92% 94% 90% 88% 86% 85% 87% 78% 72%
68% 64% 60%
Growth y/y 14% 11% 10% 10% 11% 12% 11% 10% 9% 7%
Cost Per Vial $800 $800 $800 $800 $800 $840 $840 $840 $840 $840
$882 $926 $954 $982 $1,012
First Line 20.0 21.2 22.4 23.2 86.8 24.1 24.9 25.7 26.5 101.3
113.5 130.3 143.4 150.9 165.6
% of total MBC 34% 33% 34% 34% 34% 33% 33% 32% 32% 33% 29% 28%
26% 24% 24%
% of US Sales 35% 35% 36% 37% 36% 37% 37% 38% 38% 38% 38% 39%
39% 38% 39%
Growth y/y 21% 18% 15% 14% 17% 12% 15% 10% 5% 10%
Second Line 19.2 20.4 21.0 21.6 82.2 22.0 22.6 23.2 23.8 91.8
102.5 114.8 128.7 151.9 157.0
% of total MBC 32% 32% 32% 31% 32% 30% 30% 29% 29% 30% 27% 25%
24% 24% 22%
% of US Sales 34% 34% 34% 34% 34% 34% 34% 34% 34% 34% 34% 34%
35% 38% 37%
Growth y/y 15% 11% 11% 10% 12% 12% 12% 12% 18% 3%
Third Line 17.8 18.2 18.5 18.7 73.2 18.8 19.1 19.3 19.5 76.7
85.2 88.7 94.0 94.8 102.8
% of total MBC 30% 29% 28% 27% 28% 26% 25% 24% 24% 25% 22% 19%
17% 15% 15%
% of US Sales 31% 30% 30% 29% 30% 29% 29% 28% 28% 28% 28% 27%
26% 24% 24%Growth y/y 6% 5% 4% 4% 5% 11% 4% 6% 1% 8%
Europe $0.7 $0.7 $0.7 $0.7 $2.7 $2.0 $2.5 $3.1 $3.6 $11.1 $27.0
$48.3 $74.2 $96.6 $127.6
% of total MBC 1% 1% 1% 1% 1% 3% 3% 4% 4% 4% 7% 10% 14% 16%
18%
Growth y/y 196% 277% 358% 439% 317% 142% 79% 54% 30% 32%
Cost Per Vial $350 $350 $350 $350 $350 $368 $368 $368 $368 $368
$386 $405 $417 $430 $443
First Line 0.3 0.3 0.3 0.3 1.1 0.8 1.1 1.3 1.6 4.8 11.7 20.9
37.3 47.4 61.0
% of total MBC 0% 0% 0% 0% 0% 1% 1% 2% 2% 2% 3% 5% 7% 8% 9%
% of Europe Sales 40% 40% 40% 40% 40% 40% 42% 43% 44% 43% 43%
43% 50% 49% 48%
Growth y/y 201% 302% 402% 503% 352% 145% 79% 79% 27% 29%
Second Line 0.3 0.3 0.3 0.3 1.1 0.8 1.0 1.2 1.4 4.3 10.4 19.8
25.8 35.1 47.1
% of total MBC 0% 0% 0% 0% 0% 1% 1% 1% 2% 1% 3% 4% 5% 6% 7%
% of Europe Sales 42% 42% 42% 42% 42% 40% 39% 39% 38% 39% 39%
41% 35% 36% 37%
Growth y/y 184% 255% 326% 397% 290% 141% 90% 30% 36% 34%
Third Line 0.1 0.1 0.1 0.1 0.5 0.4 0.5 0.6 0.6 2.0 4.9 7.6 11.1
14.1 19.6
% of total MBC 0% 0% 0% 0% 0% 1% 1% 1% 1% 1% 1% 2% 2% 2% 3%
% of Europe Sales 19% 19% 19% 19% 19% 20% 19% 18% 17% 18% 18%
16% 15% 15% 15%
Growth y/y 210% 272% 334% 397% 303% 138% 56% 46% 27% 39%
China $1.8 $3.0 $3.5 $4.7 $12.9 $5.5 $6.7 $7.9 $9.1 $29.3 $58.6
$79.3 $101.3 $127.8 $150.2
% of total MBC 3% 5% 5% 7% 5% 8% 9% 10% 11% 9% 15% 17% 19% 21%
21%
Growth y/y 214% 127% 126% 94% 126% 100% 35% 28% 26% 17%
Cost Per Vial $450 $450 $450 $450 $450 $473 $473 $473 $473 $473
$496 $521 $547 $574 $603
First Line 0.7 1.3 1.3 2.0 5.2 2.6 3.3 3.9 4.6 14.5 29.0 40.4
47.7 62.4 72.2
% of total MBC 1% 2% 2% 3% 2% 4% 4% 5% 6% 5% 8% 9% 9% 10%
10%
% of China Sales 37% 44% 37% 42% 40% 48% 49% 50% 50% 49% 50% 51%
47% 49% 48%
Growth y/y 302% 151% 201% 134% 176% 101% 39% 18% 31% 16%
Second Line 0.8 1.2 1.6 2.0 5.5 2.0 2.3 2.7 3.1 10.1 20.7 27.4
37.7 46.2 55.1
% of total MBC 1% 2% 2% 3% 2% 3% 3% 3% 4% 3% 5% 6% 7% 7% 8%
% of China Sales 45% 40% 45% 42% 43% 35% 35% 34% 34% 35% 35% 34%
37% 36% 37%
Growth y/y 148% 99% 74% 59% 84% 104% 32% 38% 23% 19%
Third Line 0.3 0.5 0.6 0.8 2.2 0.9 1.1 1.2 1.4 4.7 9.0 11.6 15.8
19.2 22.8
% of total MBC 1% 1% 1% 1% 1% 1% 1% 2% 2% 2% 2% 3% 3% 3% 3%
% of China Sales 18% 16% 18% 17% 17% 17% 16% 16% 15% 16% 15% 15%
16% 15% 15%
Growth y/y 198% 132% 99% 79% 113% 91% 30% 36% 21% 19%
MBC (Partnered) 1Q09 2Q09 3Q09 4Q09 2009FY 1Q10 2Q10 3Q10 4Q10
2010FY 2011FY 2012FY 2013FY 2014FY 2015FY
ROW $0.0 $0.0 $0.0 $1.1 $1.1 $2.4 $3.5 $4.7 $6.0 $16.7 $39.0
$55.5 $79.0 $97.4 $120.2
% of total MBC 0% 0% 0% 2% 0% 3% 5% 6% 7% 5% 10% 12% 15% 16%
17%
Growth y/y 468% 1472% 134% 42% 42% 23% 23%
Cost Per Vial $400 $400 $400 $400 $400 $420 $420 $420 $420 $420
$441 $463 $486 $511 $536
First Line 0.0 0.0 0.0 0.3 0.3 0.9 1.6 2.2 2.8 7.5 19.4 27.5
39.0 49.5 63.6
% of total MBC 0% 0% 0% 0% 0% 1% 2% 3% 3% 2% 5% 6% 7% 8% 9%
% of China Sales 0% 0% 0% 7% 2% 17% 23% 28% 31% 26% 33% 35% 39%
39% 42%
Growth y/y 804% 2311% 157% 42% 42% 27% 29%
Second Line 0.0 0.0 0.0 0.4 0.4 0.9 1.2 1.6 2.1 5.8 12.3 18.3
26.7 32.4 37.7
% of total MBC 0% 0% 0% 1% 0% 1% 2% 2% 3% 2% 3% 4% 5% 5% 5%
% of China Sales 0% 0% 0% 8% 3% 17% 17% 21% 23% 20% 21% 23% 26%
25% 25%
Growth y/y 459% 1452% 112% 49% 46% 21% 17%
Third Line 0.0 0.0 0.0 0.4 0.4 0.6 0.7 0.9 1.1 3.3 7.4 9.8 13.3
15.5 18.9
% of total MBC 0% 0% 0% 1% 0% 1% 1% 1% 1% 1% 2% 2% 2% 2% 3%
% of China Sales 0% 0% 0% 8% 3% 10% 11% 12% 12% 11% 13% 12% 13%
12% 13%
Growth y/y 198% 794% 121% 32% 37% 17% 21%
Royalty Rate 20% 20% 20% 20% 20% 20% 20% 20% 20% 20% 20% 20% 20%
20% 20%
ROW Royalty Revenue $0.0 $0.0 $0.0 $0.2 $0.2 $0.5 $0.7 $0.9 $1.2
$3.3 $7.8 $11.1 $15.8 $19.5 $24.0
Off Label Sales 1Q09 2Q09 3Q09 4Q09 2009FY 1Q10 2Q10 3Q10 4Q10
2010FY 2011FY 2012FY 2013FY 2014FY 2015FY
Total $12.4 $13.7 $16.5 $17.2 $64.4 $18.1 $19.0 $19.8 $20.7
$77.5 $90.7 $101.3 $110.9 $118.5 $124.1
% of total Abraxane rev 17% 18% 20% 20% 20% 20% 20% 20% 20% 20%
19% 18% 17% 16% 15%
Growth y/y 46% 38% 20% 20% 20% 17% 12% 9% 7% 5%
-
7/28/2019 Abraxis Initiation Merriman Sept 09
15/31
-
7/28/2019 Abraxis Initiation Merriman Sept 09
16/31
-
7/28/2019 Abraxis Initiation Merriman Sept 09
17/31
-
7/28/2019 Abraxis Initiation Merriman Sept 09
18/31
-
7/28/2019 Abraxis Initiation Merriman Sept 09
19/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 19
Let the Data Flow: Abraxane Has a Busy Clinical Trials
Calendar
A quick search using the term Abraxane on ClinicalTrials.gov
returns 38 trials that include the term and arecurrently enrolling
patients (the number balloons to more than 63 if all trials are
included). Even if one nar-rows the search by including the term
Phase III, 13 studies still pop up. As impressive as this is,
clearlyAbraxis must focus on those studies that are most likely to
provide the greatest return for dollar invested.Those studies
conducted beyond the aegis of Abraxis can serve multiple purposes:
first, they may help formthe hypothesis for Abraxis-sponsored
trials; second, they may be the material for publication and
eventualcompendia listing (see Appendix C), and; third, they may be
the subject of presentations and abstracts atmedical conferences
that could drive off-label use. According to Abraxis, the company
is sponsoring threePhase III studies, 15 Phase II studies and 11
Phase I/II studies. In addition, over there are over 60
investi-gator-sponsored studies for which the company is providing
assistance. For our purposes, we will focus onthose studies that
Abraxis can control. The totality of this clinical trial portfolio
can have a meaningful benefiton the companys commercial
prospects.
Abraxane Phase III Trials: One Ace in the Hole, Two
Wildcards
The three most important trials Abraxis has ongoing are in
melanoma, panreatic cancer and non-small celllung cancer (NSCLC).
Given that paclitaxel is already a standard of care in conjunction
with platinum agents(either carboplatin or cisplatin) for the
treatment of newly diagnosed Stage IIIB/IV metastatic NSCLC, weview
this trial as the one with the highest probability of success.
Multiple trials with both carbo- and cisplatinhave demonstrated
survival improvement in this setting, and, at least in the U.S.,
platinum-based therapiesare still the standard of care for first
line therapy (although Alimta-based regimens may make further
inroadsagainst platinum-based therapies). Abraxiss other two
registration-directed studies in melanoma and pan-creatic cancers
are based on provocative data from single-arm trials. However, it
has not yet been estab-lished that taxanes can provide clinical
benefit in these two tumor settings. Thus, we have only built a
modelfor the potential use of Abraxane in NSCLC, but are not
incorporating our estimates into our projections atthis time.
However, to give the reader a sense of the commercial opportunity
for Abraxane in NSCLC, wewould make the following points:
1. Non-Small Cell Lung Cancer is one of the largest of all tumor
types, with the patient population approxi-mately equal to the sum
of both breast and colorectal cancer.
2. Use of the combination of a platinum-based drug (carboplatin)
with paclitaxel accounts for approximatelyone-quarter of all
regimens used in first-line NSCLC. Addition of Avastin
(bevacizumab) to carbotaxoladds another 8-10% of patients, while
carboplatin with Taxotere (docetaxel) add an additional 3-5%.
3. Despite recent therapeutic advances, mortality from NSCLC
remains high. Further, the concept ofmaintenance therapy, i.e., use
of an active regimen beyond the standard number of cycles
typicallyused to achieve a response. In our view, the activity and
tolerability of Abraxane, although as yet un-proven, makes it an
ideal candidate for such therapy.
Abraxis Pipeline-Lots Going on Internally and Externally
In addition to the registration studies that Abraxis is
undertaking in NSCLC, melanoma and pancreatic can-cer, there are a
number of ongoing trials sponsored both by Abraxis and others that
may drive additional useof Abraxane in various settings. Abraxis is
sponsoring two late-stage studies we find interesting: one
thatexamines the use of Abraxane in breast cancer in the adjuvant
setting, while the other examines the use ofAbraxane in a
taxane-refractory patient population ( a true acid-test of
Abraxanes activity). As we previouslymentioned, a search on
www.clinicaltrials.gov using the terms Abraxane, nab-paclitaxel, or
ABI-007, turnup hundreds of references (between 425 and 1200
depending on whether one wants to look at all trials oronly those
that are currently open to enrollment). Amongst the more
interesting of these are combinationstudies with targeted therapies
such as Avastin, Erbitux, Herceptin (we point out that the NCCN
guidelinesrecommend paclitaxel as the preferred background
chemotherapy in HER 2+ breast cancer treated with Her-
-
7/28/2019 Abraxis Initiation Merriman Sept 09
20/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 20
ceptin) and Sutent, amongst others, including experimental
targeted agents. These studies will likely be thesubject of future
publications and presentations that may drive additional use and
inform the design of regis-tration-quality studies.
Beyond Abraxane, we would highlight two development candidates
with significant commercial potential (thefull Abraxis pipeline can
be viewed in the diagram below.
Figure 16: Abraxis BioScience Pipeline
Source: Company reports.
ABI-008 is a nano-particle version of Sanofi-Aventiss Taxotere
(docetaxel). The drug is in Phase II trials forthe treatment of
chemotherapy-nave metastatic, hormone-refractory prostate cancer.
We remind the readerthat Taxotere is the current standard of care
for this indication. According to the trial information on
Clinical-Trials.gov, the study should read out sometime in
mid-2010. Another intriguing, yet early, compound is ABI-013
(CY196), a microtubule inhibitor that is optimized for the nab
platform.
NAB Technology Platform-Big things Come in Small Packages
The key to the Abraxis product platform is the companys nab
albumin-based drug delivery technology. Albu-min is the most
abundant protein in the human body, and Abraxis has harnessed its
properties to create avaluable and versatile drug delivery
platform. When albumin is used as the key protein in the
ProtoSpheretechnology, the resulting vehicle is referred to as a
nab (naoparticle albumin-bound) particle. Albumin hasmultiple
capabilities that make it well-suited for use as a delivery
vehicle. These properties include:
Albumin can carry water insoluble molecules, including
nutrients, vitamins and hormones
Given their increased metabolic rate, tumors exhibit an
increased appetite for nutrients, which are car-ried to the tumor
by albumin
Albumin can carry substances across the endothelial barrier (the
layer of cells that constitute the vascu-lar system)
Albumin binds to the gp60 receptor on endothelial cells, forming
caveolae (indentations in the cell mem-brane that get pinched off
and form small vesicles inside the cell) that transports albumin
and its payload
Drug and Indication Preclinical Phase I Phase II Phase III
MarketedABI-007 (nab -paclitaxel)
Breast (metastatic)
Lung (Advanced NSCLC)
Malignant Melanoma (Stage IV)
Pancreatic (Advanced)
ABI-008 (nab -docetaxel)Microtubule Stabilizer -
Prostate (Hormone Refractory)
ABI-009 (nab- rapamycin)
mTOR inhibitor - Solid Tumors
ABI-010 (nab -17AAG)
Hsp90 inhibitor - Solid Tumors
ABII-011 (nab- 5404)
Dual Microtubule and Topoisomerase-1
inhibitor - Solid Tumors
ABI-011 (nab- CY196)
-
7/28/2019 Abraxis Initiation Merriman Sept 09
21/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 21
across the cell membrane
Albumin binds to SPARC (secreted protein acidic and rich in
cysteine), a protein that binds albumin andconcentrates nutrients
in the interstitium. Tumors secrete this protein at abnormally high
levels
In effect, the nab technology functions as a Trojan horse that
facilitates the escape of paclitaxel from thevasculature and into
the tissue compartment. Once in the tissue space, SPARC proteins
concentrate the pa-clitaxel payload that is then sopped up
preferentially by cells of the tumor. The nab platform is
exceptionallyversatile, and can be applied to a variety of
compounds (please see the Abraxis BioScience product
platformbelow).
Figure 17: nab-Particle Diagram
Source: Company reports.
Figure 18: nab-Platform
Source: Company reports.
1. Albumin-bound paclitaxeldisaasociates in the bloodstream.
2. Binds to gp60 on endothelialcell wall.
3. Caveolae transport drug totumor interstitium.
4. Surface SPARC binds albumin-drug complex.
-
7/28/2019 Abraxis Initiation Merriman Sept 09
22/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 22
Valuation
As mentioned previously, we find the valuation of the shares of
Abraxis BioScience to be extremely compel-ling. At a recent price
in the $26 range, the companys market cap is just over $1 billion.
Subtracting $258million in net cash (the company has zero debt)
leaves a technology (enterprise) value of approximately$800
million. On a trailing 12-month (TTM) basis, the shares trade at a
modest 2.4 times TTM EV/Revenue.Book value is $889 million, giving
an Price/BV of 1.2x. On a standard discounted future earnings
basis, wearrive at a one year price target range of $30-33. Please
see our detailed financial models for all estimatesand projections.
Please note that our financial projection do not account for any
changes in the cost structureas a result of the Abraxis Health
spin-off.
Summary and Conclusion
In sum, we find the shares of Abraxis BioScience to be extremely
attractive at current levels, the companyspast notwithstanding.
Valuation is compelling, the new management is competent and
motivated, and the
lead product has a worldwide franchise which the company
controls. Abraxane roll-out in ex-U.S. territoriesshould drive
strong comparative numbers throughout the course of 2010. As
operational improvements arerealized and the spin-off of Abraxis
Health places more of the BioScience operations in the limelight,
valua-tion should increase accordingly, in our view. We are
therefore initiating coverage with a Buy rating and atarget range
of $30-33.
-
7/28/2019 Abraxis Initiation Merriman Sept 09
23/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 23
Appendix A: Management Team
According to information from the company:
Lonnie Moulder, Vice Chairman, President and Chief Executive
Officer
Mr. Moulder joined Abraxis BioScience in 2009. Previously, he
was vice chairman of Eisai Corporation ofNorth America following
its acquisition of MGI PHARMA, INC., where he served as president
and chief execu-tive officer since 2003. Mr. Moulder joined MGI
PHARMA in 1999 as executive vice president and was subse-quently
promoted to president and chief operating officer. Prior to that,
he was a member of the foundingmanagement team and vice president
business development and commercial affairs of Eligx, Inc., a
venture-stage biomedical company. Mr. Moulder served for 16 years
in a number of commercial roles for HoechstMarion Roussel (now
Sanofi Aventis) and its predecessor companies. He began his career
as a clinical phar-macist. Mr. Moulder was a board member of the
Biotechnology Industry Organization (BIO) and is a memberof the
Board of Visitors of the Temple University school of Pharmacy. He
earned a bachelor of science degreein pharmacy from Temple
University and a master of business administration degree from the
University ofChicago.
Patrick Soon-Shiong, M.D. Executive Chairman
Dr. Soon-Shiong is the Executive Chairman and Chief Executive
Officer of Abraxis Health. He was recentlyappointed Executive
Director of the UCLA Wireless Health Institute, and is Professor of
Microbiology, Immu-nology, and Molecular Genetics Professor of
Bioengineering at UCLA.
Dr. Soon-Shiong holds a degree in Medicine from the University
of the Witwatersrand, Johannesburg, SouthAfrica, and a Master of
Science from the University of British Columbia. He is a fellow of
the American Col-lege of Surgeons and the Royal College of
Physicians and Surgeons of Canada. Dr. Soon-Shiong performedthe
worlds first encapsulated islet transplant in a diabetic patient.
He developed the first FDA approved pro-tein nanoparticle delivery
technology for the treatment of metastatic breast cancer and this
drug is beingdeveloped for lung, melanoma, gastric and pancreatic
cancer. He is a co-inventor of over 50 issued U.S. pat-ents, has
published more than 100 scientific papers, and founder of two
publicly traded pharmaceutical com-panies, American Pharma Partners
and Abraxis Bioscience.
Dr. Soon-Shiongs research has been recognized by national and
international awards such as the Associa-tion for Academic Surgery
Award for Research, the American College of Surgeons Schering
Scholar, theRoyal College Physicians and Surgeons Research Award,
the Peter Kiewit Distinguished Membership in Medi-cine Award, and
the International J.W. Hyatt Award for Service to Mankind. Dr.
Soon-Shiong received the2006 Gilda Club Award for the advancement
of cancer medicine and is a recipient of a 2007 Ellis Island
Medalof Honor as well as the St. Mary Medical Center Life
Achievement Award in 2007 and the St. Johns HealthCenter Caritas
Award in 2007.
In 2008, he received the Medical Visionary Award from the
Pancreatic Cancer Action Network for his work inpancreatic
cancer.
Dr. Soon-Shiong currently serves on the Board of Directors for
the National Institute of Transplantation aswell as the Technology
Council for the new Center for Cancer Nanotechnology Excellence at
NorthwesternUniversity which is part of the National Cancer
Institutes (NCI) five-year initiative for nanotechnology in
can-
cer research. He also serves on two advisory boards for the RAND
Corporation, the RAND Center for AsiaPacific Policy and the RAND
Health Board of Advisors. Dr. Soon-Shiong recently joined the Board
of Trusteesfor the Saint Johns Health Center in Los Angeles,
California and the Advisory Board of the California Nano-Systems
Institute at UCLA. He also recently joined the Advisory Board for
the Institute for Technology Ad-vancement (ITA) at UCLA School of
Engineering & Applied Science, as well as the Board of
Councilors of theUSC Viterbi School of Engineering.
In 2009 he was appointed to the Presidents Council at RAND
Corporation, Chairman of the Steering Commit-tee of Life Sciences
of the X-Prize Foundation and Founding Board member to Dossia
Foundation.
-
7/28/2019 Abraxis Initiation Merriman Sept 09
24/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 24
Mary Lynne Hedley, Ph.D., Executive Vice President and Chief
Scientific Officer
Dr. Hedley most recently served as Executive Vice President of
Eisai Corporation of North America followingEisais acquisition of
MGI PHARMA, INC. where she had served as Executive Vice President
and Chief Scien-tific Officer since 2005. She joined MGI PHARMA in
2004 as Senior Vice President and General Manager. Pre-viously, Dr.
Hedley co-founded ZYCOS, Inc., a biotechnology company, and held
roles of progressivelygreater responsibility ultimately leading to
her serving as the companys President and Chief Executive Offi-cer.
Dr. Hedleys early research career consisted of two consecutive
postdoctoral fellowships at Harvard Uni-versity from 1989 through
1996. She earned her bachelor of science degree in Microbiology
from Purdue Uni-versity and her doctorate degree in Immunology from
the University of Texas, Southwestern Medical Center.She is a named
inventor on multiple patents in the field of immunology, and has
been widely published in avariety of peer-reviewed journals. Dr.
Hedley is the recipient of multiple awards and fellowships, is a
fre-quent guest lecturer, and an active volunteer in educational as
well as local community organizations.
Rick Rodgers, Senior Vice President and Chief Financial
Officer
Mr. Rodgers joined Abraxis BioScience in 2009. Previously, he
was Senior Vice President, Controller and
Chief Accounting Officer of MGI Pharma until the companys
acquisition by Eisai Corporation in 2008. In2003, Mr. Rodgers was
Corporate Controller of MedSource Technologies and from 1997 to
2002, he heldvarious senior positions at ADC Telecommunications
Inc. Prior to that, he held finance and accounting posi-tions at
several private and public companies. Mr. Rodgers began his
financial career in accounting at ArthurAnderson & Co. Mr.
Rodgers earned his bachelor of science degree in Financial
Accounting from St. CloudState University, Minn., and his master of
business administration degree in Finance from the University
ofMinnesota, Carlson School of Business.
Bruce Wendel, Executive Vice President, Corporate
Development
Mr. Wendel became executive vice president of corporate
development of Abraxis BioScience in May 2006.Mr. Wendel joined
American Pharmaceutical Partners (APP) in 2004 as vice president of
corporate develop-ment. He began his 14 years with Bristol-Myers
Squibb as in-house counsel before shifting to business andcorporate
development. While at Bristol-Myers Squibb, as vice president,
corporate development interna-tional medicines, he led teams that
completed several major acquisitions, divestitures and alliances
around
the world. These transactions included a $225 million
divestiture of Bristol's U.S. diagnostic division as wellas the
acquisition of three pharmaceutical firms in Argentina, South
Korea, and Peru, and a co-promotionalliance with SmithKline Beecham
for Avandia. Before joining APP, he served as vice president,
business de-velopment and licensing for IVAX Corporation, a generic
drug manufacturer, where late last year he com-pleted the company's
acquisition of 3M's European respiratory business. Previously, Mr.
Wendel served in thelegal departments of Playtex and Combe. He
earned a Juris Doctorate degree from Georgetown UniversityLaw
School where he was an editor of Law & Policy in International
Business, and a B.S. from Cornell Univer-sity.
Marty J. Duvall, Senior Vice President, Global Marketing and
International Commercial Operations
Mr. Duvall joined Abraxis BioScience in 2009. Mr. Duvall most
recently served as Chief Business Officer, Mor-photek, a subsidiary
of Eisai Corporation of North America, following Eisais acquisition
of MGI PHARMA, INC.,where he served as Sr. Vice President,
Commercial Operations (2004-2006) and Sr. Vice President,
Commer-cial Strategy and Development (2007-2008). Previously, Mr.
Duvall served for nearly 19 years in a number
of commercial roles at Sanofi-Aventis and its predecessor
companies. During that tenure, his responsibilitiesincluded Vice
President, Global Medical and Marketing, with a focus on Taxotere,
and Vice President, Mar-keting for the U.S. Oncology Business Unit.
He earned a bachelor of science degree in chemistry fromMuhlenberg
College, a master degree in chemistry from The Johns Hopkins
University, and a master of busi-ness administration degree from
the University of Kansas.
-
7/28/2019 Abraxis Initiation Merriman Sept 09
25/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 25
Appendix B: Diseases Overview
Breast Cancer
According to the American Cancer Society, breast cancer is the
leading site for new cases and deaths amongwomen worldwide.
According to SEER estimates, more than 193,000 women will be newly
diagnosed in2009. It is estimated that 40,000 Americans will die
from breast cancer in 2009. There are over 2.5 millionwomen in the
United States that have a history of breast cancer. The overall
five year survival rate is 89.1%,though the rate decreases to 27%
if the cancer has metastasized at diagnosis. 85% of breast cancer
casesbegin in the mammary ducts. 60% of diagnosed cases are in a
localized stage, another 33% have alreadyspread to regional lymph
nodes, and 5% have already metastasized. The two main divisions of
breast cancerare invasive and Ductal Carcinoma in Situ (DCIS).
Invasive occurs when abnormal cells from inside lobules orducts
break out into nearby breast tissue allowing cancer cells to spread
to lymph nodes and metastasize toother organs in advanced stages.
DCIS is when the abnormal cells grow inside mammary ducts
withoutspreading to other sites.
Metastatic breast cancer is an advanced stage of breast cancer.
Of all such cases in the US, most are reoc-
currences. The five year survival rate is lower than earlier
stages and treatment goals are to prolong life andreduce symptoms
to improve quality of life. Hormone therapy may be used on tumors
with positive hormonereceptors (ER+) and works to shrink tumors
throughout the body. When it is not an option, chemotherapy
isusually considered which can stop the growth of the tumor, kill
cancer cells that have spread to other partsof the body and reduce
symptoms. According to the National Comprehensive Cancer Network
(NCCN) guide-lines for breast cancer, the preferred single agents
to treat metastatic breast cancer are anthracyclines, tax-anes,
anti-metabolites and other microtubule inhibitors. The preferred
taxanes are paclitaxel, docetaxel andalbumin-bound paclitaxel
(Abraxane).
Melanoma A Killer in the Sun
Cutaneous melanoma continues to challenge the medical
establishment, proving to be quite difficult to man-age.
Approximately 68,000 patients are diagnosed with cutaneous melanoma
each year, nearly 9,000 will die
from the disease. According to the National Cancer Institute
Surveillance, Epidemiology and End Results(SEER) database, there
has been a 619% increase in annual diagnoses from 1950 to 2000, and
a 165% in-crease in annual mortality from this cancer. Of all the
cancers, it is the fifth most common in men, and theseventh in
women. It is also the second most common cancer in women ages 20-29
years.
This is despite an effort to reduce the incidence by earlier
screening and increased education. However, cer-tain genetic
predispositions such as blond or red hair, blue eyes, presence of
freckles, and inability to tan,combined with lifestyle choices such
as sun tanning, outdoor activities leading to sunburn and
infrequent useof sunblock contribute to the growing problem. In
addition, certain people have been found to have muta-tions in the
melanocortin-1 gene, which may predispose them to melanoma. Other
implicated mutations oc-cur in the CDKN2A and CDK4 genes,
prevalently found in families with hereditary melanoma. Additional
riskfactors include prior primary cutaneous melanoma, family
history of melanoma, and multiple clinically atypi-cal moles. While
UV-light has been historically thought to cause cancer, some recent
research suggests thatit may have a role in attenuating the bodys
immune system, allowing these other de novo mutations to sur-
vive.Screening and education remain the best hope for melanoma
sufferers. ABCD evaluations of early lesionscheck for asymmetry,
border irregularity, color variegation and diameter greater than
6mm or increasedsize. In a mass screening study from 1992 to 1994,
about 2% of 282,000 patients screened had suspiciouslesions, of
which 8% turned out to be melanoma. Despite increased awareness,
direct reduction in mortalityhas not been realized.
-
7/28/2019 Abraxis Initiation Merriman Sept 09
26/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 26
Non-Small Cell Lung Cancer (NSCLC)
According to the World Health Organization (WHO), there are over
1.2 million cases of lung and bronchialcancer world wide each year,
causing approximately 1.1 million deaths annually. It is estimated
that morethan 219,000 people will be diagnosed with lung cancer in
the United States in 2009. According to the Na-tional Cancer
Institute, lung cancer is the single largest cause of cancer deaths
in the United States, and isresponsible for nearly 30 percent of
cancer deaths in this country. The overall five-year survival rate
from1999-2005 from 17 SEER (Surveillance, Epidemiology, and End
Results) geographic areas was 15.6%. Themedian survival of patients
with untreated metastatic non-small cell lung cancer is only four
to five months,with a survival rate of one year of only 10%. (Rapp
E. Pater JL, Willan A., et al. Chemotherapy can prolongsurvival in
patients with advanced non-small cell-lung cancer. JClin Oncol
1988; 6:633-41)
NSCLC is the most common form of the disease and accounts for
almost 80% of all lung cancers, with anestimated market opportunity
of over $2 billion. There are three sub-types of NSCLC. Squamous
cell carci-noma makes up 25-30% of NSCLC cases, adenocarcinoma
accounts for 40%, and large-cell carcinomamakes up 10-15% and tends
to grow and spread quickly making it harder to treat.
Standard therapeutic strategies such as surgery, chemotherapy or
radiotherapy have reached a plateau(Yang, et al. Non-small cell
lung cancer: epidemiology, risk factors, treatment and
survivorship. Mayo ClinicProc 2008;83:584^94). Current standard of
advanced NSCLC are now commonly stratified into
bevacizu-mab-eligible (Avastin, Genentech/Roche) and
bevacizumab-ineligible patients. Under the National Compre-hensive
Cancer Network (NCCN) Guidelines for NSCLC, albumin-bound
paclitaxel can be substituted for pacli-taxel or docetaxel for
patients who experienced hypersensitivity reactions after receiving
paclitaxel or do-cetaxel despite premedication or 2) for patients
in whom the standard premedications (dexamethasone, H2blockers, H1
blockers) are contraindicated.
Pancreatic Cancer
Cancer of the pancreas is the fourth leading cause of
cancer-related deaths in the United States with over35,000 deaths
estimated in 2009 and over 42,000 new cases are expected to be
diagnosed in 2009. The
pancreas consists mostly of exocrine glands and a small
percentage (5%) of endocrine glands. Tumorsformed in exocrine
glands are more common, nearly all of which (95%) are
adenocarcinomasa cancer thatstarts in gland cells. Adenocarcinomas
usually begin in the ducts of the pancreas.
Figure 19: Newly Diagnosed Pancreatic Cancer Cases by Stage
Source: National Cancer Institute Surveillance Epidemiology and
End Results
Pancreatic cancer typically spreads rapidly and is often goes
undiagnosed until the cancer has spread beyond
the primary site thus making it difficult to treat. According to
SEER estimates, 53% of newly diagnosed casesare already
metastasized. According to the American Cancer Society (ACS), about
20% of cases live at leastone year after diagnosis, while less than
4% will be alive after five years. The National Comprehensive
Can-cer Network (NCCN) Panel currently recommends gemcitabine
monotherapy as standard front-line therapyfor patients with
metastatic disease.
Stage % #
Localized 7% 2,973
Regional 26% 11,042
Distant 53% 22,509
Unstaged 14% 5,946
-
7/28/2019 Abraxis Initiation Merriman Sept 09
27/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 27
Appendix C: Compendia Listings
Source: Company reports.
Indication Compendia Date
Single Agent 1st Line MBC DrugPoints/DrugDex 2007
Single Agent & Combination 1st Line Advanced NSCLC NCCN
October 2008
DrugDex January 2009
Single Agent Head and Neck DrugPoints/DrugDex 2006
Single Agent Anal DrugPoints/DrugDex 2006
-
7/28/2019 Abraxis Initiation Merriman Sept 09
28/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 28
Public Companies Mentioned in this ReportAstraZeneca (LSE:AZN,
$27.40, Not Rated)Elan (ELN, $7.58, Not Rated)Johnson and Johnson
(JNJ, $60.29, Not Rated)Takeda (TSE:4502, JPY 3,820.00, Not
Rated)Sanofi-Aventis (SNY, $35.40, Not Rated)
-
7/28/2019 Abraxis Initiation Merriman Sept 09
29/31
-
7/28/2019 Abraxis Initiation Merriman Sept 09
30/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
September 15, 2009 30
Source: Company reports.
Balance Sheet
$ in million 2006 A 2007 A 2008 A
Assets
Current Assets:
Cash and equivalents 0.5 705.1 306.4
Cash collateral for reacquistion of agreement - - 300.6
Accounts receivable 27.6 43.9 37.0
Related party receivable 0.2 2.0 1.9
Inventories 80.1 73.7 63.5
Prepaid expenses and other current assets 7.1 18.6 33.8
Deferred income taxes 21.2 33.7 65.6
Total Current Assets 136.8 877.0 808.8
PP&E 116.2 145.1 166.7
Investment in Drug Source Co 5.5 9.3 10.2
Intangible assets 243.4 205.2 175.3
Goodwill 241.4 241.4 241.4Other non-current assets 21.5 24.3
36.2
Total Assets 764.8 1,502.3 1,438.6
Liabilities and Equity
Current Liabilities:
Accounts payable 24.1 33.6 39.1
Accrued liabilities 29.9 54.9 53.0
Accrued litigation costs - - 57.6
Reacquisition payable - - 268.0
Related party payable - 7.0 -
Income taxes payable 18.5 5.0 0.7
Deferred revenue 39.2 41.3 4.2
Total current liabilities 111.7 141.8 422.7
Deferred income taxes, non-current 29.0 32.4 62.7Long-term
portion of deferred revenue 158.1 121.1 8.2
Other non-current liabilities 6.9 9.5 15.5
Total Liabilities 305.8 304.9 509.1
Stockholder's Equity
Common Stock - 0.0 0.0
Additional PIC - 1,192.5 1,203.1
Accumulated deficit - 4.1 (272.7)
Accumulated other comprehensive loss 0.9 0.8 (1.0)
Parent Company investment 458.2 - -
Less: treasury stock
Total Stockholder's Equity 459.0 1,197.4 929.5
Noncontrolling Interest - -
Total Equity 459.0 1,197.4 929.5
Total L&E 764.8 1,502.3 1,438.6
-
7/28/2019 Abraxis Initiation Merriman Sept 09
31/31
MERRIMAN
CURHAN
FORD
BiotechnologyLife Sciences
Abraxis BioScience (ABII) Buy
IMPORTANT DISCLOSURESThis research has been prepared by Merriman
Curhan Ford & Co., a wholly owned subsidiary of Merriman Curhan
Ford Group,
Inc. Some companies Merriman Curhan Ford & Co. follows are
emerging growth companies whose securities typically involve
ahigher degree of risk and more volatility than the securities of
more established companies.The securities discussed in Merriman
Curhan Ford & Co. research reports may be unsuitable for some
investors depending on theirspecific investment objectives,
financial status, risk profile, or particular needs. Investors
should consider this report as only a singlefactor in making their
investment decisions and should not rely solely on this report in
evaluating whether or not to buy or sell the se-curities of the
subject company.Regulation Analyst Certification (Reg. AC)All of
the views expressed in this research report accurately reflect the
research analyst's personal views about any and all of the sub-ject
securities or issuers. No part of the research analyst's
compensation was, is, or will be, directly or indirectly, related
to the specificrecommendations or views expressed by the research
analyst in the subject company of this research report. Research
analysts arenot directly compensated for specific revenue generated
by the firms investment banking transactions/activities.General
DisclosuresMCF & Co. expects to receive or intends to seek
compensation for investment banking services for all of the
companies in its re-search universe in the next three months.
Investors should assume that MCF & Co. is soliciting or will
solicit investment banking orother business relationships from the
companies covered in this report in the next three months.Security
prices in this report may either reflect the previous days closing
price or an intraday price, depending on the time of distribu-
tion. Designated trademarks and brands are the property of their
respective owners.Specific Disclosures- MCF & Co. has not
received compensation for investment banking services within the
last 12 months, and does not expect to receive orintend to seek
compensation for investment banking services in the next three
months, from Abraxis BioScience, Inc.- Within the last 12 months
MCF & Co. has not managed or co-managed a public offering for
Abraxis BioScience, Inc.- MCF & Co. makes a market in ABII and
as such buys and sells from customers on a principal basis.-
Neither Michael King nor a member of his household owns shares of
ABII.- Neither MCF & Co. nor its officers, principals,
employees, or owners own options, rights, or warrants to purchase
ABII.- No MCF & Co. employee serves on the board of directors
of Abraxis BioScience, Inc.- Neither Michael King nor a member of
his household serves on the board of directors of Abraxis
BioScience, Inc.- Neither MCF & Co. nor its affiliates
beneficially owns 1% or more of an equity security of Abraxis
BioScience, Inc.Key to Investment Rankings (expected total share
price return inclusive of dividend reinvestment, if applicable)
MCF & Co. archives and reviews outgoing and incoming email.
Such may be produced at the request of regulators. Sender acceptsno
liability for any errors or omissions arising as a result of
transmission. Use by other than intended recipients is
prohibited.
The information contained herein is based on information
obtained from sources believed to be reliable but is neither
all-inclusive norguaranteed by Merriman Curhan Ford & Co. No
independent verification has been made as to the accuracy or
completeness of theinformation. Opinions, if any, reflect our
judgment at the time the report is first published and are subject
to change without no-tice. Merriman Curhan Ford & Co. does not
undertake to advise you of changes in its opinion or
information.Member FINRA / SIPC. Copyright 2009. All rights
reserved. Additional information supporting the statements in this
report is avail-able upon request.
Rating Percent ofUniverse
No. ofStocks
Description
Percent of companies under researchcoverage from which MCF &
Co. re-ceived compensation for investment
banking services provided in the previ-ous 12 months or expects
to receive or
intends to seek in the next threemonths
Buy 77% 77MCF & Co. expects the stock price to appreciate10%
or more over the next 12 months. Initiate or
6%
Neutral 21% 21MCF & Co believes the stock price is fairly
valuedat current levels. Maintain position or take no ac-tion.
0%
Sell 2% 2MCF & Co. expects the stock price to depreciateover
the next 12 months. Sell or decrease position.
0%