Embed Size (px)
Citation preview

ABSENT UMBILICAL ARTERY*
A REVIEW OF 113 CASESBY
GORDON L. BOURNEt and KURT BENIRSCHKEtFrom the Departments ofPathology and Obstetrics, Boston Lying-in Hospital and
Harvard Medical School, Boston, Mass.
(RECEIVED FOR PUBLICATION MARCH 23, 1960)
The umbilical cord normally contains two arteriesand one vein embedded within Wharton's jellywhich is, in turn, enclosed by an epithelial membrane.
Hyrtl (1870) described the absence of one of theumbilical arteries in 12 instances (four infants andeight placentae) of which only two infants weremalformed, one suffering from spina bifida and bothhaving cleft palates. He also noted that maleinfants were affected more often than female infantsand that females lacking one umbilical artery weremore frequently malformed and often anencephalic.Neither the observation of male dominance nor thehigher incidence of abnormalities in females havesubsequently been confirmed, although there is ahigh incidence of anencephalic deformity in thefemale infants. He collected a total of 58 casesfrom the literature to add to the 12 of his own.Browne (1925) reported a premature infant in
whom the umbilical cord contained a single arteryand the umbilical vein was replaced by a capillarynetwork. Javert and Barton (1952) reported theresults of the examination of 1,000 abortuses inwhich histological sections from 104 umbilical cordswere examined. Only one was found to containa single artery.
Benirschke and Brown (1955) described a retro-spective study of 55 infants in whom one arterywas missing from the entire length of the umbilicalcord. Of these 55 only 13 (24%) were consideredto be normal children and of the remaining 42there were 27 (64 %) who suffered from a wide rangeof congenital abnormalities, many of whom hadmultiple defects. Placental abnormalities werecommon (39 %). Little (1958) examined the umbili-cal cords of 1,200 consecutive deliveries, finding
* This work was supported in part by U.S. Public Health GrantNo. RG.4966.
t Nuffield Travelling Fellow. Present address: Senior Registrar,St. Bartholomew's Hospital, London.
t Present address: Department of Pathology and Microbiology,Dartmouth Medical School, Hanover, New Hampshire.
that 12 (1 %) contained only one artery throughout,and in four (0'3%Y.) the arteries fused locally nearthe placenta; congenital abnormalities were presentin 25%. Recently Benirschke and Bourne (1960)reported the incidence of absent umbilical arteryto be 15 (1 %) in 1,500 consecutive deliveries. Eight(53 %) were considered to be developmentallynormal, although one was stillborn, whilst seven(470%) were found to possess major or minor con-genital abnormalities. Only 12 (80 %) remainalive, one of whom has survived operative treatmentfor oesophageal atresia and tracheo-oesophagealfistula.
It seems fairly certain that the overall incidenceof this abnormality is in the region of 1% of alldeliveries. Furthermore, they report that absentumbilical artery occurred seven times (7 %) in aseries of 100 consecutive unselected twin pregnancies.This is much higher than has hitherto been supposed.
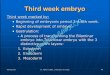
Materials and MethodA total of 113 infants in whom one umbilical
artery was absent (Fig. 1) has been studied at theBoston Lying-in Hospital and the Children's MedicalCentre, Boston, Mass. The series is composed of55 cases first observed in a mainly retrospectivestudy, 15 cases reported to be present in the exami-nation of 1,500 consecutive placentae, together witha further 43 instances observed during the pastthree years in the Pathology Department of theBoston Lying-in Hospital. With the exception ofsome of the 55 instances which were retrospective,the examination consisted of a gross evaluation ofthe placenta together with a microscopic study ofat least three blocks of tissue. These included sec-tions from the middle portion of the umbilicalcord, a segment of rolled membrane and a sectionof full thickness placental tissue. In the event ofabsence of an umbilical artery from the histologicalsection of the cord, the secundines, which had been
534
copyright. on A
ugust 24, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.35.184.534 on 1 Decem
ber 1960. Dow
nloaded from

ABSENT UMBILICAL ARTERY
FIG. 1.-Absence of one umbilical artery. Section of the umbilicalcord showing the dilated vein and a single artery. Note the muscularwall and small lumen of the artery. There are no residual ducts or
vessels present. (H. and E. x 10.)
stored awaiting 'histological clearance', were re-
examined to confirm the absence of an artery fromthe entire length of the cord. In instances of foetaldeath confirmation of the absence of one of theintra-abdominal vessels was sought at necropsy.Owing to the high incidence of associated congenitalabnormalities, it was the usual practice to informthe paediatrician immediately upon the finding ofa single umbilical artery. This assisted in the earlydiagnosis of oesophageal atresia in at least one
infant.A total of approximately 6,000 deliveries occur
each year in the Boston Lying-in Hospital. Withthe exception of the consecutive series mentionedabove the placentae are examined in the laboratoryonly when indicated by such conditions as maternalillness or disease; foetal distress, abnormality or
prematurity; plural pregnancy; hydramnios andother complications of pregnancy as well as patientsof clinical or pathological interest.
It is realized that 98 of the total 113 cases are
derived from selected material from which it mightbe erroneous to draw definite and final conclusions.The reasons for the selection of the material fromwhich these cases are derived, however, are so
diverse that there is ample justification for the analysisof certain factors.
Maternal FactorsAge. An analysis of the ages of the 1 3 mothers
who were delivered of infants lacking one umbilical
artery is shown in Table 1. It is noticeable that26 (62%) of the 42 primigravidae were under theage of 25, whereas only 13 (22%) of the 59 multi-gravidae were under the same age. Compared withthe average ages of a control series of patients,this series shows an increased incidence of theanomaly among the younger primigravidae and theolder multigravidae. The age groups of the totalseries, however, conform fairly closely to thoseof the controls, because the increased incidenceat the younger end of the primigravidae scalebalances the similar, but less well marked, rise atthe older end of the multigravidae scale. Thesefindings are in broad agreement with Baird andWalker (1959), who state 'The incidence of foetaldeformity ... is highest in the 15-19 age group anddecreases with age till thirty-five; a slight rise occursin the age group 35 and over'.The average age of the 19 mothers of infants
with central nervous system anomalies, 28-3 yearscompared with 28-5 years, failed to confirm thatthese, in particular, occur in a high age group(Hegnauer, 195 1).
Parity. Forty-two of the mothers were primi-gravidae and 59 were multigravidae whose parityvaried from one to 15. These are shown in detailin Table 2 and agree essentially with the controlseries except for the high number pregnant for the
TABLE 1ANALYSIS OF AGES OF MOTHERS DELIVERED OF
INFANTS LACKING ONE UMBILICAL ARTERY
Age Primigravida Multigravida Total(years)
20 5 1 621-25 21 12 3326-30 8 15 2331-35 6 17 2336-40 2 12 1441 - 2 2
Total.. .. 42 59 101
Average age.. 25-3 30-7 28 5
TABLE 2GRAVIDITY
Gravidity No.
1 422 213 i 154 115 36 57 18 2
15 1
Total .. 101
535
copyright. on A
ugust 24, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.35.184.534 on 1 Decem
ber 1960. Dow
nloaded from

ARCHIVES OF DISEASE IN CHILDHOOD
sixth time, an observation that is not consideredto have any significance.The 59 women who had been pregnant previously
had produced a total of Ill live born infants, 12stillbirths (a rate of 103 per 1,000) and 32 abortions.Four of the 111 live born infants died in the new-born period so that only 107 (69%) infants survivedthe newborn period out of a total of 155 previouspregnancies. This incidence (31 Y.) of foetal lossin the past history of these patients is surprisinglyhigh and much greater than the 11 % of the controlseries.
Maternal Diseases. A high incidence of pre-eclampsia (30%) was described by Benirschke andBrown (1955). This was not confirmed by Little(1958). Both authors agree that the large numberof pre-eclamptic patients in Benirschke's series wasthe result of material selection and that it did notreflect the true incidence of this complication ofpregnancy. This series of 113 cases includes the55 described by Benirschke, together with a further58 additional cases in which pre-eclampsia wasdiagnosed in only five (9%) instances. Thisindicates that pre-eclampsia is not associated withthe absence of an umbilical artery either as an aetio-logical factor or as a result of the abnormality.Altogether a total of 19 patients (16%) were foundto be suffering from pre-eclampsia in the total of 113.The association, however, of pre-eclampsia and
a single artery in a total of 19 patients resulted inseven stillbirths, three neonatal deaths and nineliving infants, which illustrates that this combination,even if it is fortuitous, is particularly lethal to thefoetus.A careful study of the general health of the mothers
has not disclosed any factor that might influencethe pregnancy so as to predispose the foetus to thisparticular anomaly. The high incidence of foetalwastage in the previous pregnancies of multigravidahas been described; a high proportion (8 %) ofpatients suffered from antepartum haemorrhage.Two otherwise normal infants suffered from
erythroblastosis foetalis due to rhesus incom-patibility, one being stillborn and the other dying onthe first day. Four of the mothers suffered fromepilepsy (grand mal).
Hydramnios. The incidence of foetal abnor-mality is particularly high in association withhydramnios. Macafee (1950) stated that the inci-dence of foetal abnormality was 460% in a series ofhydramniotic pregnancies. It is not surprising,therefore, that there should be a fairly high incidenceof hydramnios in association with absence of an
umbilical artery. Nineteen (19 %) patients wereconsidered to suffer from hydramnios in the 101 inwhom adequate information was available and thisfigure is probably a conservative estimation, becausein the original study of 55 cases only four werepresent, 15 occurring in the last 58 patients. Thishigh incidence of hydramnios was not confirmedby Little (1958). It is interesting that all 19 (100%)of these infants suffered from congenital abnor-malities and that 12 were stillborn; five died in theneonatal period and the two who survive do sobecause of successful surgical treatment of oeso-phageal atresia. The association between hydram-nios and oesophageal atresia is now accepted(Scott and Wilson, 1957), and in one of the survivingpatients the early diagnosis of oesophageal atresiawas hastened by the finding of umbilical arteryaplasia within a few hours of the birth of the infant.
Heredity. There is little or no evidence to showthat this condition is of an hereditary nature. Onlyone mother was known to suffer from any majorcongenital abnormality (pulmonary stenosis) andone had congenital syphilis. No abnormalitieswere known to be present in the male parents butthey were, necessarily, not subjected to the samescrutiny as the mother. Furthermore, the widerange of associated congenital abnormalities seemsto mitigate against a single hereditary factor.Four mothers (4 %) suffered from grand mal, whichmight be significant, but the numbers are too smallto justify the assumption that it was in any waya causative factor.There is, however, some evidence that the anomaly
forms part of a diathesis in which abnormalities arefrequently multiple and may be recurrent. Theseassumptions are based upon the past history of 59multigravid patients in which 48 (31 %) out of atotal 155 pregnancies failed to produce a living child.It is unfortunate that more detail was not availableconcerning the loss of these infants, but such infor-mation as is available does not reveal any definiterecurrence of single umbilical artery abnormality,although several are known to have producedabnormal infants previously. Several mothers havesubsequently produced normal children, all of whompossessed two umbilical arteries. That thesepatients experience a greater than average difficultyin producing living normal children is definite andit is possible that the finding of arterial abnormalitiesin the umbilical cord may lead to the recognitionof such 'high-risk' patients even in their first preg-nancy. The parents of one infant were known to berelated cousins; there was no other recorded evidenceof consanguinity.
536
copyright. on A
ugust 24, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.35.184.534 on 1 Decem
ber 1960. Dow
nloaded from

ABSENT UMBILICAL ARTERYTABLE 3
DETAILS OF 15 (1%) AFFECTED INFANTS FROM 1500 CONSECUTIVE DELIVERIES
Gestational Complication FoetalNumber Sex Twins Age (weeks) of Pregnancy Anomalies Follow-up
I M _ 35 Chorioamnionitis None found Not traced2 F _ 39 Placental infarct None found Normal3 F F/F 38 None Forked xyphoid Normal development
monochorial4 M - 42 Irregular heart 0-130; None found Normal
discharge meconium5 M M/M 38 650 g. lighterthan other Hydrocele, abnormal Developing normally;
monochorial twin cardiac rhythm bigger than twin6 M - 38 None Slight club foot-right Normal development7 F - 40 None None found Normal8 F F/M 38 None Hyperteleorism, short No problem
dichorial fingers9 F - 37 Hydramnios Oesophageal atresia Operated, survived
and fistula, sacralanomaly
10 F - 37 Hydramnios Anencephaly Stillborn11 F - 40 None None found Normal12 F - 40 None None found Normal13 M - 37 None Renal agenesis, atresia Died
ani, accessory pan-creas, equinovarus
14 F - 37 Maternal floor infarc- None found Stillborntion; long cord
15 F - 40 Long cord None found Not traced
(After Benirschke and Bourne, 1960.)
The InfantsIncidence. In the examination of a series of
1,500 consecutive placentae a total of 15 (1 %) of theumbilical cords were found to contain only oneartery throughout their length. Seven (46 %) ofthese 15 infants suffered from congenital abnor-malities, of which three were of major significance(Table 3). One was a stillborn anencephalic andone died from renal agenesis. There were eight(53%) normally developed infants of which one wasa macerated stillbirth in whom no congenitalabnormality could be found.The overall mortality in this short series is three
out of 15 (20%) with one further child survivingoperative repair ofan oesophageal fistula and atresia.The relatively high incidence of twin infants in
this consecutive series (20%) is confirmed to someextent by the fact that in a series of 100 consecutivetwin deliveries an absent umbilical artery was
present seven (7 %) times. The overall incidence ofone in 100 is confirmed by Little (1958) and byBourne (1961) who recognized the condition five timesin 475 (one in 95) consecutive umbilical cords.A similar incidence is also reported by Emig(personal communication).
The Fate of the Infants. It is realized that thetotal series of 113 cases is partially selected, butnevertheless an analysis of these patients is veryinformative. Table 4 shows the fate of these infants.
Live Infants. Only 48 (42 %) are alive, of whom14 (29 %) are known to suffer from congenital
TABLE 4FATE OF THE INFANTS
Infants Nos. %
Total .113 100
Alive . . 48 42Normal infants .. . 34Known congenital abnormality 14
Dead ... .. .. 65 58Congenital anomaly incompatible with life 39Congenital anomaly compatible with life
in infants dead of other causes .. .Possible anomaly in unexamined infants . 15No anomaly .6
abnormalities; 27 infants were either seen or wereconsidered by their medical attendant to be bothphysically and mentally normal. It was impossibleto trace seven infants, all of whom, according totheir records, were normal when last examined. Inthe absence of any information to the contrarythese infants are considered to be living and normal.
It has been possible to trace all 14 infants whoare alive and who suffer from congenital abnor-malities of varying severity. Several of these infants(Table 5) are not expected to reach adult life andtwo survive only because of successful surgicalrepair of oesophageal atresia.
Dead Infants. Sixty-five (58 %) of the infantsdied or were born dead, of whom 59 (91 %) weresuffering from definite or probable congenitalabnormalities (Table 4), and only six (9 %),who died of known causes, were considered to benormally developed for their maturity.
537
copyright. on A
ugust 24, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.35.184.534 on 1 Decem
ber 1960. Dow
nloaded from

ARCHIVES OF DISEASE IN CHILDHOODTABLE 5
KNOWN ABNORMALITY COMPATIBLE WITH LIFE IN 14 SURVIVORS
Maturity Weight Sex Abnormality Follow-up Remarks(weeks) (lb.) (years)
40 7-1 F Congenital heart disease 17 Twin41 5-1 M Oesophageal atresia 6 Successful operation36 7-1 M Brain cysts 4 Very poor prognosis37 5d11 M Hydrocele, umbilical hernia, inguinal hernia 432 3-6 M Mental defect; optic fundi abnormal 3 Poor prognosis42 4 15 F Multiple haemangiomata 242 6-2 M Arthrogryphosis multiplex cystica, cryptorchid 232 2 5 M Cryptorchid 2 Twin39 8-0 F Marfan's syndrome: arachnodactyle 138 5-13 M Sternal abnormality 1 Twin38 3-2 M Cardiomegaly (?) cause 1 Twin38 5*8 M Talipes equinovarus 0638 5S1 F Hyperteleorism 0O5 Twin36 4-6 F Oesophageal atresia 0| 5 Successful operation
Congenital abnormality of such a major degreeas to be incompatible with life was present in 39(60%) of these children, whilst five (8%) who diedfrom other causes were suffering from anomaliesthat probably contributed to their death, and 15(22%) were considered to be suffering from acongenital abnormality, although severe macerationor lack of a post mortem examination preventedexact diagnosis.Absence of one umbilical artery seems, in itself,
to be a simple and innocuous congenital abnormality,but it is associated with a perinatal mortalityinvolving 58% of the affected infants, together witha further 12% who are alive but abnormal in someway. Such a relationship is considered to besignificant.
Congenital Abnormalities. The types of congenitalabnormality from which the affected infants sufferedhave been classified into systems. These are listedin Table 6 and they are detailed in Table 7.The majority of the babies suffered from multiple
defects which, if serious, are listed separately so thatthe total is greater than the number of infantsconcerned. No system or peculiar abnormality isparticularly prominent, although aplastic lesions of
TABLE 6CONGENITAL ABNORMALITIES
Abnormalities Nos. %
Known congenital abnormalities (mostlymultiple) .58 I 51
Gastro-intestinal . . 31Skeletal . . 28Genito-urinary . . 27Cardiovascular . . 21Neurological . . 19Others . . 10
Possible abnormality (unexamined, dead) 151 4No known abnormality .40 35
Total number of cases 113 100
TABLE 7
DETAILS OF CONGENITAL ABNORMALITIES
Abnormality Nos.
Gastro-intestinalOesophageal atresiaImperforate anusExomphalosMalrotation of gutHerniaeCleft palateCysts of larynx
SkeletalTalipes equinovarusPoly and syndactyleSpine (excluding spina bifida)PhocomeliaArthrogryphosisAchondroplasiaArachnodactyleCongenital dislocation hipMicrophthalmia
Genito-urinarySexual aplasiaRenal aplasiaPolycystic kidneysUndescended testesMegalouretersHypospadiasCryptorchidRecto-vaginal fistulaClitoral hyperplasiaDouble uterus
CardiovascularInterventricular defect'Congenital heart diseaseFallot tetralogyTriloculare.CardiomegalyCoarctation of aortaAbsent valves
Neurological.AnencephalyHydrocephalySpina bifidaMental defectAngioma.Brain cysts.CyclopsNerve paralysis
OthersTurner's syndromeHyperteleorismHaemangiomataPulmonary aplasiaSplenomegalyAsplenia .
Abnormal optic fundiCystic pancreasCystic liver
.. .. .. ~31.. .. .. ~~~8.... .. ~6
.... .. 28.. .. .. ~~9.. .. .. ~~6
.. .. .. S~~~
.... .. ~~2
.... .. ~~2
27
21
19
10
538
5543322
l
4
215
442
2
112
ll
I
copyright. on A
ugust 24, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.35.184.534 on 1 Decem
ber 1960. Dow
nloaded from

ABSENT UMBILICAL ARTERYTABLE 8
INFANTS DEAD OF ABNORMALITIES INCOMPATIBLEWITH LIFE
Stillborn Neo-natalAbnormality Death Total
Anencephaly .5 - 5Hydrocephaly .. 2 2 4Exomphalos .. .. .. 1I 2Congenital heart disease 4 11 15Cyclops .. .. .. 1 - 1Cranial nerve paralysis - 1Spina bifida .... - 4 4Renal aplasia .... 1 2 3Gastro-intestinal aplasia - 4 4
Total .14 2539
TABLE 9KNOWN ABNORMALITIES IN INFANTS DEAD
OF OTHER CAUSES
Cause of Death Abnormality
Broncho-pneumonia SyndactyleHyaline membrane Tracheo-oesophageal fistulaStillborn macerated Unilateral renal hypoplasiaStillborn macerated Cleft palateStillborn macerated Talipes equinovarus
the alimentary and genito-urinary tracts are morefrequent, and lesions of the central nervous systemless frequent than might be expected.
Thirty-nine infants died of congenital abnor-malities incompatible with life (Table 8). Congenitalheart disease is the most common abnormalityconsidered incompatible with life. Table 9 showsthe anomalies present in those five infants whosedeath was considered to be due mainly to otherreasons.The congenital abnormalities from which the
surviving infants suffer together with their weightand maturity at birth, sex, period of follow-up andcomments are shown in Table 5. Several of thesechildren will not survive to reach adult life. Eight(57%O) were premature by weight although only two(14%) were born before the 36th week of gestation.This is not surprising if the absence of an umbilicalartery slows the actual growth of a foetus in utero,but it does not necessarily prevent the foetus frommaturing. It is upon maturation rather than actualbody weight that the infant subsequently dependsfor its survival.
Trivial abnormalities such as cutaneous naevi andminor haemangiomata have not been included inthis series. The number of uncomplicated or singlemalformations is very low. There are only 14(24%) whilst the number of multiple abnormalities,44 (76%) is much higher than expected. The greatincrease in the incidence of congenital abnormalitiesin this series is due mainly, but not entirely, to a risein the number of multiple abnormalities. Neel
(1958) found that only 14*9% of malformedchildren had multiple defects; Schull (1958) reportedthat the percentage of infants with multiple abnor-malities rose to 34 * 3 % if the parents were related.
Sex. It was suggested by Hyrtl (1870) that thereis a male preponderance associated with this abnor-mality. This was not supported by Benirschke andBrown (1955) or Little (1958), nor is it supportedin the present series, which contains 55 female and49 male infants. There is one hermaphrodite andthe sex of eight infants is not recorded. An analysisof the various abnormalities, the stillbirths, survivinginfants or maturity also fails to show any sexdomination (other than those which are expected,such as the anencephalic infants, all five of whomwere female). There is, in this series, a total of16 twin infants, whose sex is predominantly female.There are, in fact, 13 female and three male infants.No reason is offered for this apparent femaledominance, which despite the small number of cases,does appear to be significant.
Side of Absence. It is only possible to definethe absent side at necropsy. Unfortunately ade-quate information is available upon only 22 infantsin whom the artery was absent, 12 times on the rightside and 10 times on the left. The intra-abdominalpart of the umbilical artery was easily recognizablein more than half the babies, although in some itexisted as a very thin threadlike structure. Fig. 2demonstrates absence of the right artery. Thedissection displays the branches of the aorta as seenfrom the dorsal aspect and shows marked aplasiaof all the aortic branches on the right side. Asimilar developmental abnormality of these vesselswas frequently noted at necropsy, but the corre-sponding lower limb was never smaller than thecontralateral limb. When present, deformities ofthe lower limbs were usually more severe uponthe affected side.
Maturity and Weight. The maturity of 109infants is known out of a total of 113. Six werenon-viable, i.e. born before the 28th week of preg-nancy, and 103 were viable. Table 10 shows thematurity, sex, average birth weight and averageplacental weight of the infants. The average birthweight is lower than normal, especially in the moremature age groups. The average placental weightis also less than normal. It seems reasonableto suppose that the absence of an umbilical arterycould cause a diminution of oxygen supply to thefoetus and this theory receives some support fromthe small average foetal weight. There is, however,no compensating enlargement of the placenta.
539
copyright. on A
ugust 24, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.35.184.534 on 1 Decem
ber 1960. Dow
nloaded from

ARCHIVES OF DISEASE IN CHILDHOOD
FIG. 2.-The viscera of a stillborn infant dissected and photographedfrom the dorsal aspect. The aorta is normal. The left iliac, umbilicaland femoral arteries are normal. The right common iliac artery,which is about one quarter of its normal size, is distributed mainlyalong its internal iliac branches. The right umbilical and femoralarteries have no visible lumen and exist as threads in connective tissue.
Infants suffering from congenital abnormalitiestend to be born prematurely and in this series 56(59 %) of the 95 viable infants of known weight werepremature by weight at birth.
TABLE 10MATURITY, SEX AND AVERAGE BIRTH WEIGHT OF
INFANTS WrTH AVERAGE PLACENTAL WEIGHTS
Sex Average AverageMaturity Number (if known) Birth Weight Placental(weeks) Weight
M F lb. oz. (oz.)
<28 6 2 1 - -28 2 1 1 1 8 829 2 1 1 4 1030 2 1 1 2 15 1231 1 - 1 2 12 932 5 2 3 2 12 1333 4 2 2 3 1 1 1434 3 2 1 2 14 1235 12 5 7 3 13 1536 9 5 3 5 4 1837 11 5 6 5 2 1438 11 6 5 6 5 1539 7 3 4 6 13 1740 20 8 12 6 5 2241 6 3 2 6 7 1942 6 3 3 5 12 14
>42 2 - 2 5 0 17Not known 4
Total .. 113 48 55
Placentae. A relatively high incidence of placentalabnormality was recorded by Benirschke and Brown(1955), and Little (1958) reported an increasedfrequency of velamentous insertion of the umbilicalcord. In this series there was a total of 32 (29%)placentae that showed gross abnormality including,velamentous insertion of the cord (12); circum-margination (five); circumvallation (five); lobed(four); placenta praevia (three) and maternal floorinfarct (three). Massive infarction of the maternalsurface of the placenta with resulting intra-uterineasphyxia has been noted by Benirschke and Bourne(1960) to occur in successive pregnancies and to beassociated with absence of an umbilical artery.
Accidental ante-partum haemorrhage occurred insix pregnancies from which only one infant sur-vived; four were stillborn and one died after 24hours. Placenta praevia was present on threeoccasions. A history of threatened abortion wasgiven by eight patients, an episode which did notappear to affect adversely the infant's chance ofsurvival.
Twins. The incidence of absent umbilical arteryis greatly increased in plural pregnancy. In thepresent series of 113 babies the abnormality occurred16 times (14%) in twin pregnancies; only five (31 %)of these 16 infants are alive and well.
In a consecutive series of 100 twin pregnancies theabnormality was present on seven occasions. Thisincidence of 7% of twin pregnancies, or 3-5% oftwin infants, as compared with an overall incidenceof 1% appears to be a significant increase.A similar unexplained observation (Stevenson,Worcester and Rice, 1950) is the finding of adoubled incidence of foetal malformation in twinpregnancies.
Benirschke and Bourne (1960) considered that theincrease of this anomaly might be caused by arelatively higher proportion of monozygous twins.This appeared to be correct in a smaller number,but the present larger series of 16 infants does notsupport the theory. Six (37%/) infants weremonozygous because of monochorial placentation,while 10 (63%) were dizygous because of dichorialplacentation or heterosexual twins, so that theyobey the general rule regarding the zygosity oftwins, which states that nearly one-third are mono-zygous and two-thirds dizygous.
Discussion
Variations in the number of vessels in the umbilicalcord are known to occur, but the available informa-tion upon their origin and significance is sparse. The
540
copyright. on A
ugust 24, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.35.184.534 on 1 Decem
ber 1960. Dow
nloaded from

ABSENT UMBILICAL ARTERY
most important vascular aberration is absence of oneof the two umbilical arteries through the length of theumbilical cord and is associated with atresia of thecorresponding intra-abdominal portion of the artery.This abnormality is present in I % of pregnancies andin 7% of twin pregnancies. Anastomoses betweenthe umbilical arteries normally occur at the placentalend of the umbilical cord either in the cord itselfor in the adjacent placenta. These anastomosespresumably serve to equate the intra-arterial pres-sures and ensure equal distribution of blood through-out the placenta. They may also act as an arterialshunt when a portion of the foetal placental circu-lation is closed for physiological or pathologicalreasons and could, therefore, exert a profoundinfluence upon the ability of the foetus to maintainits placental reserve or to resist the anoxic effectsof large placental infarcts.
Foetal Abnormalities. The incidence of congenitalabnormality amongst an average population isbetween 1% and 2.50% of all live and stillbirths(Malpas, 1937; Logan, 1951; Lewis, 1956) of whichapproximately half are gross foetal abnormalities.Absence of one umbilical artery appears to be thecommonest major congenital abnormality of thehuman foetus.
There is a significant rise in the incidence ofcongenital abnormalities associated with foetuseshaving only one umbilical artery. The width ofthe range of the congenital abnormalities suggeststhat the absence of an umbilical artery is not asecondary effect but is probably a primary lesionto which, some at least, of the associated anomaliesare secondary.
It is possible that these abnormalities are theresult of the hypoxia to which the foetus is subjectedduring the organo-genetic period. The efficiencyof a single artery or the date of closure of a secondartery, are not standard so that both the time anddegree of relative oxygen lack would vary widely.There is no suggestion that all the anomalies inthis series are caused by a single agent, as some areconsidered to be hereditary (Potter, 1952) but, if afactor such as anoxia were playing a part in theirproduction, it would have to be capable of actingover a long period in order to account for the widevariety of abnormalities concerned.
However, the majority of anencephalic infantspossess two normal umbilical arteries, which indi-cates that either absence of an umbilical artery hasno teratogenetic influence, or, if it does, that thereare other agents which are equally effective. Similararguments can be forwarded concerning the otherabnormalities of this series, in that they also are
considered to occur in the presence of two normalumbilical arteries so that the precise embryologicaland developmental significance of absence of oneumbilical artery is unknown.The high incidence of associated foetal abnor-
mality occurring in babies with only one umbilicalartery suggests that the 'anomalies' are in some wayconnected. The presence of only one artery in theumbilical cord may constitute a severe impedimentto normal foetal development by causing a resistanceto the blood flow and possible lack of oxygen to thefoetus. This, together with an absence of thejuxtaplacental umbilical arterial anastomosis, mayalso be a cause of intra-uterine death. This seriesincludes 16 twin infants and the fact that 14 (88 %)of these infants were smaller than their normalsiblings does support the theory that a singleumbilical artery impairs normal growth.Minor congenital abnormalities are conspicuous
by their absence in this series. When two factorsthat are known to be associated with major con-genital abnormalities are combined, such as hydram-nios and absent umbilical artery, the foetal loss isparticularly high.
Cardiac Malformation. There are several reasonswhy a high incidence of cardiac abnormalities mightbe associated with absent umbilical artery. Initself the absence is an anomaly of the cardiovascularsystem and other changes may occur because theartery normally develops during the period of rapidformation of the circulatory system. A heavystrain would certainly be imposed upon the heartif a functioning artery underwent degeneration inearly foetal life. It has been shown that a singleartery can support an apparently normal foetusbut the resistance to blood flow and degree of cardiacoverload must, at times, be considerable and maypredispose to abnormalities within the heart. Onemight assume that measuring the diameter of theremaining artery would offer some means by whichone could determine if an increased resistance toblood flow had existed in intra-uterine life. Un-fortunately, the thick muscular wall causes theirlumina to vary greatly after delivery, so that thereis no reliable method whereby their functionalefficiency within the uterus can be assessed (Rey-nolds, 1952).
Aetiology. It is disappointing that even such alarge series does not give any definite indicationof the cause of this abnormality. There is no definiteevidence that the condition is familial or recurrent,although it does occur in the children of womenwho have a poor reproductive ability. It is more
541
copyright. on A
ugust 24, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.35.184.534 on 1 Decem
ber 1960. Dow
nloaded from

ARCHIVES OF DISEASE IN CHILDHOODfrequent in the younger primigravida and the oldermultigravida. The fact that four mothers sufferedfrom epilepsy is interesting but the number is toosmall to be significant.We have considered the possibility that the vessel
which was formed in a normal manner has subse-quently ceased to function, and atrophied. Sucha cessation of function would cause some anoxia,however transient, which could easily disturb theembryological development of the foetus and causecongenital abnormalities. The time at which theartery ceased to function would be the teratogenetictermination period and as such would determinewhich foetal organs would be most severely affected.If the time varied widely, so would the malformation.The theory that the artery once was present and
functioning is supported to some extent by the in-variable presence of an intra-abdominal umbilicalartery, albeit often attenuated, on the affected side.It is, however, difficult to accept that a properlyfunctioning umbilical artery could entirely disappearfrom the umbilical cord without leaving somehistological evidence of its presence. In fourinstances, however, the residual arterial structurewas present and, having a diameter much greaterthan that of the vitelline vessels, it is assumed thatthese remnants are aplastic umbilical arteries.
It is our opinion that the second umbilical arterywas never satisfactorily formed within the umbilicalcord in the majority of the infants in this seriesbut, that in a few instances, a functioning vessel waspresent at some stage of foetal development.
Clinical Importance. Absence of an umbilicalartery, occurring in 1 % of patients, is associatedwith a high incidence of foetal abnormality (65 %).Many of these abnormalities are not obvious, norare they readily apparent upon simple generalexamination of the newborn. In most maternityunits the placenta, membranes and umbilical cordare examined, weighed and measured and it wouldbe a simple procedure to examine routinely thecut end of the cord. The vessels are easily identifiedand the finding of a single artery should stimulate afurther and more detailed examination of the infant.Such an observation might be of great benefit if thepresence of unsuspected abnormality were to beconsidered in those cases of single umbilical arteryencountered. Benirschke and Bourne (1960) reportthat the diagnosis of oesophageal atresia was madesix hours after delivery in an infant who was re-examined following the reported finding of a singleumbilical artery. The child is well one year aftersurgical treatment for the condition. The impor-tance of hydramnios in association with absent
umbilical artery is stressed, for, in this series, allof the 19 infants in whom this combination waspresent suffered from a major congenital abnor-mality.
Prognosis. Details of the congenital abnor-malities suffered by the affected children have beenrecorded together with the prognosis both beforeand after delivery. Absence of one umbilicalartery does in itself diminish a child's chance ofsurvival. The incidence of intra-uterine asphyxia,stillbirth and prematurity is higher than normal.The anomaly appears to cause a slowing of intra-uterine growth so that the average birth weight isless than the expected normal average. It is inter-esting to note that these infants, when healthy, aresimilar to twin infants in this respect because theirability to survive depends more upon their maturitythan weight. This series produces further con-firmation that this principle applies also to the singlepregnancies.When the infants are born alive their prognosis is
identical to that of their associated abnormality,if present, together with superimposed prematurity.As stated above, they withstand prematurity fairlywell and, having survived the newborn period, theydevelop physically and mentally into normal chil-dren, provided, of course, that they are not en-cumbered by the frequently associated congenitalabnormalities.
SummaryA total of 113 cases of absence of one umbilical
artery are presented and analysed, together with areview of the literature.The abnormality is slightly increased amongst
the younger primigravidae and the older multi-gravidae, but does not increase in incidence as parityrises. A total of 59 multiparous women had had155 previous pregnancies from which only 107(69%) infants survived. A total foetal loss of 48(31 %) is considered excessive and indicates thatthese women, as far as reproduction is concerned,belong to a high risk group. Hydramnios occurred19 times; all (100%) the infants suffered from majorcongenital abnormalities and only two survive asa result of surgical treatment for oesophagealatresia. There is, at present, no evidence to showthat the condition is hereditary.The incidence of absent umbilical artery is 1 % of
all births and 7% of twin pregnancies.The foetal loss in a consecutive series was 20%
but in the total of 113 instances the foetal loss was65 (58 %). Fourteen of the 48 infants who surviveare known to suffer from congenital abnormalities.
542
copyright. on A
ugust 24, 2021 by guest. Protected by
http://adc.bmj.com
/A
rch Dis C
hild: first published as 10.1136/adc.35.184.534 on 1 Decem
ber 1960. Dow
nloaded from

ABSENT UMBILICAL ARTERY 543Major congenital abnormalities were present in
58 (51 %) of the infants; only 40 (35 %) were develop-mentally normal and a further 15 (14%) werethought to suffer from a congenital anomaly. Theabnormalities were mostly multiple and not con-fined to any particular system. Obstructive lesionsor atresia of the gastro-intestinal and urinarytracts were relatively common.
Fifty-six (59 %) of the 95 viable infants of knownweight were premature by weight at birth, but theaverage weight of all the infants at birth was lessthan normal. The placenta was considered to beabnormal in 32 (29 %) of the pregnancies.
It is suggested that routine examination of the cutend of the umbilical cord at delivery might resultin early diagnosis ofsome ofthe associated congenitalabnormalities.
REFERENCESBaird, D. and Walker, J. (1959). British Obstetric and Gynaecological
Practice, ed. E. Holland. 2nd ed., p. 924. Obstetrics.Heinemann, London.
Benirschke, K. and Bourne, G. L. (1960). The incidence and prog-nostic implications of congenital absence of one umbilicalartery. Amer. J. Obstet. Gynec., 79, 251.and Brown, W. H. (1955). A vascular anomaly of the umbilicalcord. Obstet. Gynec., 6, 399.
Boume, G. L. (1961). The Human Amnion, Chorion and UmbilicalCord. Lloyd-Luke, London. (In preparation.)
Browne, F. J. (1925). On the abnormalities of the umbilical cordwhich may cause antenatal death. J. Obstet. Gynaec. Brit. Emp.,32, 17.
Hegnauer, H. (1951). Missbildungshaufigkeit und Gebaralter.Geburtsh. u. Frauenheilk., 11, 777.
Hyrtl, J. (1870). Die Blutgefasse der menschlichen Nachgeburt innormalen und abnormen Verhaltnissen. Braumuller, Vienna.
Javert, C. T. and Barton, B. (1952). Congenital and acquired lesionsof the umbilical cord and spontaneous abortion. Amer. J.Obstet. Gynec., 63, 1065.
Lewis, T. L. T. (1956). Progress in Clinical Obstetrics andGynaecology, p. 130. Churchill, London.
Little, W. A. (1958). Aplasia of the umbilical artery. Bull. SloaneHosp. Wonm. N.Y., 4, 127.
Logan, W. P. D. (1951). Incidence of congenital malformationsand their relation to virus infections during pregnancy. Brit.med. J., 2, 641.
Macafee, C. H. G. (1950). Hydramnios. J. Obstet. Gynaec. Brit.Emp., 57, 171.
Malpas, P. (1937). The incidence of human malformations and thesignificance of changes in the maternal environment in theircausation. Ibid., 44, 434.
Neel, J. V. (1958). A study of major congenital defects in Japaneseinfants. Amer. J. hum. Genet., 10, 398.
Potter, E. L. (1952). Pathology of the Fetus and the Newborn. YearBook Publishers, Chicago.
Reynolds, S. R. M. (1952). The proportion of Wharton's jelly inthe umbilical cord in relation to distention of the umbilicalarteries and vein, with observations on the folds of Hoboken.Anat. Rec., 113, 365.
Schull, W. J. (1958). Consanguinity and the etiology of congenitalmalformations. Pediatrics, Suppl. No. 1, p. 195.
Scott, J. S. and Wilson, J. K. (1957). Hydramnios as an early signof oesophageal atresia. Lancet, 2, 569.
Stevenson, S. S., Worcester, J. and Rice, R. G. (1950). 677 Con-genitally malformed infants and associated gestational charac-teristics. Pediatrics, 6, 37.
AddendumSince writing this article it has been discovered that
one of the infants considered to be developmentallynormal is, in fact, suffering from a marked degree ofmental retardation. copyright.
on August 24, 2021 by guest. P
rotected byhttp://adc.bm
j.com/
Arch D
is Child: first published as 10.1136/adc.35.184.534 on 1 D
ecember 1960. D
ownloaded from