Embed Size (px)
Citation preview

Pulmonary rehabilitation as a mechanism to reduce hospitalizations for acute exacerbations of chronic obstructive pulmonary disease: A systematic review and meta-analysisRunning Head: Pulmonary rehabilitation for exacerbations of COPD
Correspondence to:Elizabeth Moore, Imperial College London.National Heart and Lung Institute, Emmanuel Kaye Building, 1B Manresa Road, London, SW3 6LRE: [email protected] T: 0207 594 8824
Authors:Elizabeth Moore, MSc, Department of Respiratory Epidemiology Occupational Medicine and Public Health, Imperial College London, London, UKThomas Palmer, MSc, Department of Primary Care and Pubic Health, Imperial College London, London, UKDr Roger Newson, PhD, Department of Primary Care and Pubic Health, Imperial College London, London, UKProf Azeem Majeed, Department of Primary Care and Pubic Health, Imperial College London, London, UKDr Jennifer K Quint, MRCP, PhD, Department of Respiratory Epidemiology Occupational Medicine and Public Health, Imperial College London, London, UKDr Michael A Soljak, PhD, Department of Primary Care and Pubic Health, Imperial College London, London, UK
Word count: abstract = 265; main text = 3567
Conflicts of Interest Statement
JKQ reports grants from the Medical Research Council (MRC), GlaxoSmithKline (GSK), British Lung Foundation (BLF), Wellcome Trust, during the conduct of the study, and personal fees from AstraZeneca and GSK outside of the submitted work. MS reports other current research grants from Arthritis Research UK, Public Health England and the EU EITHealth Programme, with no conflicts of interest. No other conflicts of interest are reported.
Abbreviations: COPD = Chronic Obstructive Pulmonary Disease; AECOPD = Acute Exacerbation of COPD; GP = General Practitioner; ER = Emergency Room; PR = pulmonary rehabilitation; UC = Usual Care; ED = Emergency Department; FEV1 = Forced Expiratory Volume in 1 second; FCV = Forced Vital Capacity; CI = Confidence Intervals; SD = Standard Deviation; RCT = randomised controlled trial; OR = odds ratio; ICD = International Classification of Diseases
Key words: COPD, exacerbations, hospitalizations, pulmonary, rehabilitation
1
AbstractBackground: Acute exacerbations of COPD (AECOPD) have a significant impact on healthcare
utilization, including physician visits and hospitalizations. Previous studies and reviews have shown
that pulmonary rehabilitation has many benefits but the effect on hospitalizations for AECOPD is
inconclusive.
Methods: A literature search was carried out to find studies that might help determine, using a
meta-analysis, the impact of pulmonary rehabilitation on AECOPD, defined as unscheduled or
emergency hospitalizations and emergency room (ER) visits. Cohort studies and randomised
controlled trials (RCTs) reporting hospitalizations for AECOPD as an outcome were included. Meta-
analyses compared hospitalization rates between eligible pulmonary rehabilitation recipients and
non-recipients, before and after rehabilitation.
Results: 18 studies were included in the meta-analysis. Results from ten RCTs showed that the
control groups had a higher overall rate of hospitalizations than the pulmonary rehabilitation groups
(0.97 hospitalizations/patient-year, 95% Confidence Intervals (CIs) 0.67, 1.40; 0.62
hospitalizations/patient-year, 95% CI 0.33, 1.16 respectively). Five studies compared admission
numbers in the 12 months before and after rehabilitation, finding a significantly higher admission
rate before compared to after (1.24 hospitalizations/patient-year, 95% CIs 0.66, 2.34; 0.47
hospitalizations/patient-year, 95% CIs 0.28, 0.79 respectively). The pooled result of three cohort
studies found the reference group had a lower admission rate compared to the pulmonary
rehabilitation group (0.18 hospitalizations/patient-year, 95% CI 0.11, 0.32 for reference group versus
0.28 hospitalizations/patient-year, 95% CI 0.25, 0.32 for pulmonary rehabilitation).
Conclusions: Although results from RCTs suggested that pulmonary rehabilitation reduces
subsequent admissions, pooled results from the cohort studies did not, likely reflecting the
heterogeneous nature of individuals included in observational research and the varying standard of
pulmonary rehabilitation programmes.
2
Introduction
COPD 1 is a major cause of morbidity and is expected to be the third largest cause of death globally
by 2020.2 COPD is characterized by airflow limitation that is usually progressive, and not fully
reversible.3 Patients with COPD can experience exacerbations; episodes of deterioration
characterized by worsening symptoms including increased dyspnoea, cough, sputum production,
and airflow obstruction.4 Acute exacerbations of COPD (AECOPD) may require admission to hospital
which can put a heavy burden on health systems. In the United Kingdom COPD exacerbations are the
second most common cause of emergency hospital admission with an annual cost to the National
Health Service of over £800 million.5 In the United States the total economic burden of COPD in 2007
was calculated to be $42.6 billion and one study reported mean costs of $647 (SD $445) for
Emergency Room (ER) visits. 6
Pulmonary rehabilitation is an important intervention in the management of COPD. The American
Thoracic Society7 and the European Respiratory Society define pulmonary rehabilitation as “a
comprehensive intervention based on a thorough patient assessment followed by patient-tailored
therapies, which include, but are not limited to, exercise training, education, and behaviour change.”
The intention of pulmonary rehabilitation is to improve the physical and psychological condition of
people and to promote long-term adherence of health-enhancing behaviours.” It is a key component
of the multi-disciplinary management of COPD8 and can improve exercise capacity, dyspnoea,
activities of daily living, muscle strength, and self-efficacy.9 A recent systematic review has also
shown that pulmonary rehabilitation can improve quality of life.10 Given the evidence of these
benefits, a recent Cochrane Editorial stated that no further systematic reviews are required to show
that pulmonary rehabilitation improves patient-related outcomes.
However, the evidence relating to whether it reduces ER visits and hospitalizations for AECOPD is
less definitive. A previous systematic review by Puhan et al11 found that pulmonary rehabilitation
significantly reduced hospitalizations and mortality in patients who had recently suffered an
exacerbation of COPD. However more evidence is needed relating to all COPD patients, as the
majority of COPD patients participate in pulmonary rehabilitation courses when stable.
The main objective of this review was to identify and review RCTs and observational studies which
examined whether pulmonary rehabilitation reduces hospitalizations for AECOPD, by assessing the
effects of this area of physical therapy on all patients with a defined diagnosis of COPD, rather than
only those who have recently exacerbated.
3

Materials and methods
We used methods as outlined in the Preferred Reporting Items for Systematic Reviews and Meta-
Analyses (PRISMA) Statement.12 A protocol was devised for the search strategy and is included in the
supplementary materials.
Types of studies, participants and outcomes
Searches were conducted for RCTs and non-randomised cohort studies comparing the effects of
pulmonary rehabilitation with usual care on ER visits and hospitalizations for AECOPD. Studies
comparing hospitalizations within individuals before and after the pulmonary rehabilitation
programme were also included. Only studies that included participants with a confirmed diagnosis of
COPD of any severity were reviewed. Pulmonary rehabilitation programmes of any duration from
inpatient, outpatient or community settings were assessed. The primary outcomes were
unscheduled hospitalizations and ER visits for AECOPD. We also searched for studies reporting
exacerbations recorded by GP visits and mortality rates as secondary outcomes.
Electronic searches
MEDLINE, MEDLINE In-Process & Other Non-Indexed Citations, EMBASE, BIOSIS & Science Citation
Index were searched up until September 2015 using PRISMA guidelines.12 The search strategy was
devised to search all articles relating the terms “COPD”, “pulmonary rehabilitation”,
“hospitalizations” and “mortality”. Terms were combined using the AND Boolean logic
operator. The search strategy used in each database is included in the supplementary materials.
Screening
Titles and abstracts were screened and studies deemed to be relevant based on the
inclusion/exclusion criteria were then reviewed in full by two reviewers. The eligibility criteria were
as follows:
4

Inclusion criteria:
· Population: COPD patients (mild, moderate, & severe)
· Intervention: pulmonary rehabilitation (home- , community-, or hospital-based). Included
rehabilitation on stable COPD and after AECOPD.
· Comparison: Compared pulmonary rehabilitation versus control (or usual care), and studies
that compared hospitalizations before and after rehabilitation.
· Outcomes: physician and ER visits with AECOPD as the primary reason for admission/visit
according to the International Classification of Disease (ICD): ICD-9 and ICD-10 codes.
Mortality rates were also considered as a secondary outcome.
· Setting/Design: Observational studies and RCTs. We included the former as the use of high
quality observational and electronic health records data is becoming increasingly accepted.
Exclusion criteria:
· Studies that include all respiratory diseases combined with COPD in the statistical analysis.
· Those that include asthma (ICD-9 493; ICD-10 J45) in the study cohort.
· Programmes that included interventions from other healthcare professionals such as
pharmacy and dietetics so that it was unclear if pulmonary rehabilitation was the
intervention being assessed. However pulmonary rehabilitation programmes that included
education on these topics were still included.
· Studies which had a large proportion of missing data, performed inadequate statistical
analysis, or lacked COPD admission/hospitalisation data.
· References by the same author that repeated results of the same study.
· Not in English or translated.
· Conference abstracts lacking full details of the methods, interventions and analysis.
Statistical methods
Analyses used Version 14 of the Stata statistical software.13 We used Poisson regression models with
Huber variances clustered by study, with combinations of study and treatment (pulmonary
rehabilitation or control) as observational units, patient-years at risk as the time-at-risk variable, and
incident count as the outcome variable. The regression model parameters were a mean rate per
person-year for each combination of study type (RCT, cohort, or before and after) and treatment
(rehabilitation or control). In an alternative parameterisation of the same model, we estimated
control rate and pulmonary rehabilitation /control rate ratio. We also estimated a mean rate
5

difference for each study type, and a combined grand mean rate difference for all study types, using
the add-on Stata package scenttest,14 which is a front-end for the Stata margins command. We
produced pseudo-forest plots, in which the data points were rates or rate differences, for the
individual studies, for each study type and for all study type. These pseudo-forest plots were
different from forest plots in that there were no confidence limits for the rates, rate ratios and rate
differences for the individual studies, as the original publications did not always contain sufficient
information to estimate these, although they did give total incident counts and total person-years at
risk. We used these methods because the individual studies frequently gave only total incident
counts and total person-years at risk, without giving any information about the distribution of
incidents among individual patients. This implied that we could not estimate overdispersion or
underdispersion, and therefore implied that we could not compute confidence intervals for single-
study incidence rates and incidence rate ratios that were robust to overdispersion and/or
underdispersion. However, by making individual studies the primary sampling units, making study-
treatment combinations the observational units, and using clustered Huber variances, we could
make inference about mean population rates in the population of studies, and about their
differences and ratios. Note that the confidence limits were asymmetric, because of the log link
transformation used in the Poisson regression.
Assessment of risk of bias in included studies
Included studies were individually assessed for the level of risk of bias according to Cochrane
guidelines15 across the main domains including random sequence generations, allocation
concealment, blinding of participants, blinding of outcome, attrition bias and reporting bias. Cohort
studies were assessed using the Newcastle-Ottowa scale 16.
Figure 1. Flow chart showing the screening of articles
6

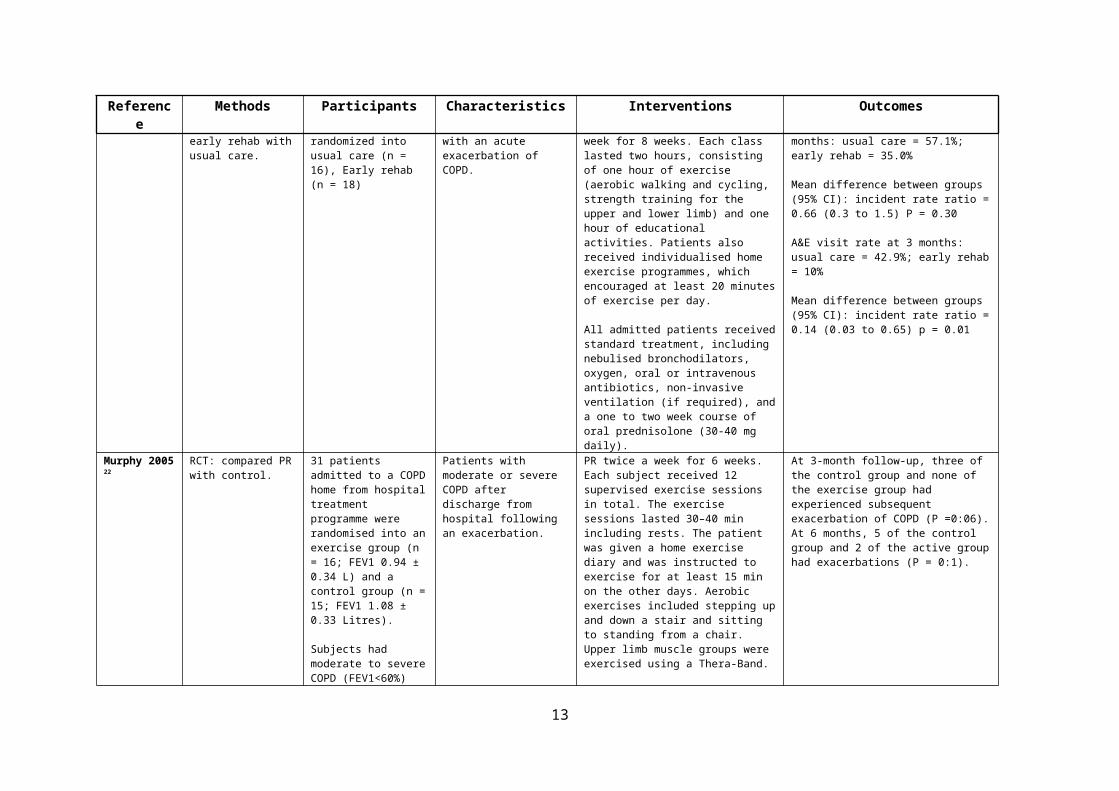
Table 1: Detailed description of studies involving patients who were post-AECOPD
Reference Methods Participants Characteristics Interventions Outcomes
Behnke 2003 17 RCT: Examined the effects of an 18-month home-based training on the rate of hospitalizations in Germany. COPD patients were recruited as in-patients admitted to a specialised hospital because of an exacerbation.
26 patients randomised into a training (n = 14) and a control group (n = 12) .
Severe COPD patients recovering post- exacerbation
1) Training group performed a 10-day hospital-based supervised training, while those of the control group did not.
2) Home-based training: training group were instructed to practice 15 min of walking at home 3 times per day, in each session achieving 125% of the best 6-minute treadmill distance at discharge. Control group did not receive specific instructions for exercise, neither during the hospital stay nor at home. The home-based programme was performed over 18 months, extending the initial 6-month trial, where only exercise performance and quality of life had been evaluated.
Total numbers over 18 months were 14 admissions in the control group and 3 admissions in the training group, which were significantly different (p = 0.026). The 6-min treadmill distance was, on average, higher (p<0.001) in the training than in the control group. Training group = 518m (95% CI 438; 597); control = 208m (148; 270).
Boxall 2005 18 RCT: to evaluate the effectiveness of a 12-week home-based PR program.
Intervention group = 23, control group = 23
Age >60.
Housebound patients with severe COPD who were 2-weeks free from worsening symptoms.
Intervention group: 12 week home-based PR programme. Patients received an individually tailored supervised walking and arm exercise program as well as individual multidisciplinary education sessions on COPD management. Included walking and arm exercises once daily. 1 weekly visits from physiotherapist for first 6 weeks and then fortnightly visits until week 12. During the control phase, patients did not receive any treatment in addition to usual medical care. These patients were offered the pulmonary PR after 12 weeks.
Both groups demonstrated improvements in 6MWT (intervention vs control mean, 39.0 vs 4.1 m [23.9% vs. 2.8%]; P = .023). Total scores in the St George’s respiratory questionnaire also improved in both groups (-5.9% vs. -1.4%; P = .020)
Analysis of hospital admission rates 3 months after randomization reveals that 5 patients in each group were admitted to the hospital due to exacerbation (intervention vs control [n], 5 vs 5; P = 1.00)
7

Reference Methods Participants Characteristics Interventions Outcomes
Eaton 2009 19 RCT: PR versus usual care on health care utilisation.
Acute health-care utilization at 3 months defined as the number of COPD-related readmissions and unscheduled emergency visits. Data were obtained from hospital and primary health-care records and reconciled with patient home diary records by assessors blinded to the intervention allocation.
Randomised into early rehab = 39 patients, Usual care = 45
COPD patients who had been admitted with an exacerbation.
Intervention group had inpatient and outpatient PR. Inpatient rehab: 30 min daily exercise including walking and upper & lower limb strengthening, commenced as early as medically appropriate.
Outpatient PR: 1 hour twice weekly for 8 weeks including supervised exercise training and education.
Usual care participants were reviewed by a dedicated study COPD nurse to ensure that they received standardized care in accordance with COPD guidelines. They also received standardized advice on the proven benefits of exercise and maintaining daily activities.
19 (40%) patients assigned to early rehabilitation satisfied the a priori definition of adherence (attendance at 75% of rehabilitation sessions).
The rehabilitation group demonstrated a 23% (95% CI: 11–36%) risk of readmission at 3 months, compared with 32% (95% CI: 19–45%) for the usual care group; the absolute risk reduction was 9% (95% CI: -9.5–26%).
Ko 2011 20 RCT comparing PRP with usual care 24 24. Accident & Emergency Department (AED) visits and hospitalizations in the subsequent 12 months were obtained from the patients, with verification of their medical records.
60 patients (30 in PRP group and 30 in Usual Care)
Patients who had been admitted with AECOPD were referred to examine effects of early outpatient PRP.
PRP 3 times a week for 8 weeks (2 hours per session) started in the same week as the baseline assessment. Supervised exercise training, including the use of treadmill, arm cycling, and arm and leg weight training, intensity adjusted by the physiotherapist, based on the tolerability and physiological variables (oxygen saturation and heart rate) of the patient. Patients were also advised to perform home exercises for at least 20 min a day.
UC group: subjects were seen by the nurse specialist at the baseline assessment as for the PRP group. They were not offered any training sessions by the physiotherapist but given simple instructions to have regular exercise at home, including walking every day and also performing some muscle stretching exercise.
Mean number of A&E attendances at 12 monthsPR = 1.57 ± 1.57Usual care = 1.47 ± 2.64
Mean number of re-admissions at 12 monthsPR = 1.00 ± 1.20Usual care = 1.03 ± 1.87.
There was a trend towards fewer readmissions in the PRP group than the UC group at the first 3 months, but this effect was lost over time and there was no difference between the two groups at 12 months (P = 0.67)
8
Reference Methods Participants Characteristics Interventions Outcomes
Man 2004 21 RCT: Compared early rehab with usual care.
42 COPD patients randomized into usual care (n = 16), Early rehab (n = 18)
Patients admitted with an acute exacerbation of COPD.
Early rehab: 2 classes per week for 8 weeks. Each class lasted two hours, consisting of one hour of exercise (aerobic walking and cycling, strength training for the upper and lower limb) and one hour of educational activities. Patients also received individualised home exercise programmes, which encouraged at least 20 minutes of exercise per day.
All admitted patients received standard treatment, including nebulised bronchodilators, oxygen, oral or intravenous antibiotics, non-invasive ventilation (if required), and a one to two week course of oral prednisolone (30-40 mg daily).
Hospital readmission rate at 3 months: usual care = 57.1%; early rehab = 35.0%
Mean difference between groups (95% CI): incident rate ratio = 0.66 (0.3 to 1.5) P = 0.30
A&E visit rate at 3 months: usual care = 42.9%; early rehab = 10%
Mean difference between groups (95% CI): incident rate ratio = 0.14 (0.03 to 0.65) p = 0.01
Murphy 2005 22 RCT: compared PR with control.
31 patients admitted to a COPD home from hospital treatment programme were randomised into an exercise group (n = 16; FEV1 0.94 ± 0.34 L) and a control group (n = 15; FEV1 1.08 ± 0.33 Litres).
Subjects had moderate to severe COPD (FEV1<60%) and a long history of cigarette smoking.
Patients with moderate or severe COPD after discharge from hospital following an exacerbation.
PR twice a week for 6 weeks. Each subject received 12 supervised exercise sessions in total. The exercise sessions lasted 30–40 min including rests. The patient was given a home exercise diary and was instructed to exercise for at least 15 min on the other days. Aerobic exercises included stepping up and down a stair and sitting to standing from a chair. Upper limb muscle groups were exercised using a Thera-Band.
Subjects in the control group received their standard medical treatment without any form of rehabilitation exercises or lifestyle changes advice.
At 3-month follow-up, three of the control group and none of the exercise group had experienced subsequent exacerbation of COPD (P =0:06). At 6 months, 5 of the control group and 2 of the active group had exacerbations (P = 0:1).
Rasekaba 2009 23
Cohort study of COPD patients who were eligible to participate in the chronic disease management pulmonary rehab (CDM) program. Compared
CDM-PR Cohort n = 29, Opt-out Cohort n = 24.
Patients with confirmed spirometry COPD diagnosis (FEV1/FVC<70%) and absence of physical
Patients were referred for CDM by GPs, respiratory specialists or acute hospital services during an emergency admission.
The CDM-PR Program was a once-weekly, 8-week programme consisting of 1 hour of physiotherapy and 45 minutes of education.
The exercise sessions consisted of a warm-up, rotating around a seven-station circuit of aerobic and resistance training for both the
Emergency department admissions
12 month beforeCDM-PR (n = 29) = 17.11Opt out group ( n= 24) = 11.04 (p = 0.415)
12 month after
9

Reference Methods Participants Characteristics Interventions Outcomes
CDM-PR Cohort and Opt-out Cohort between for acute hospital care utilization 12 months before and after the introduction of CDM-PR.
limitation to participation in exercise were included.
upper and lower body, followed by a cool-down.
Education topics: exercise, respiratory system and COPD, diet and nutrition, psychological effects and stress management, medications, energy conservation.
CDM-PR (N = 29) = 2.03Opt out group (n = 22) = 14.96 ( p = < 0.001)
Revitt 2013 24 Cohort study not included in meta-analysis. Data were collected from patients who attended an outpatient PR assessment at Glenfield Hospital, Leicester, from November 2006 to October 2008. All patients had been referred following an admission for an acute exacerbation of COPD (AECOPD).
One hundred sixty (87 males) patients with COPD. Readmission data for 155 patients
Patients who were referred by the Early Discharge Service after an admission for an exacerbation.
PR 2 x / week for 4 weeks. Patients continued with a 3-week structured unsupervised home exercise programme. Each session lasted for 2 hours with 1 hour of supervised exercise training and 1 h of education.
Incidence rate ratio = 0.623 (95% CI: 0.462–0.840) (P = 0.002). There was a 37.7% reduction in incidence of admissions in year post PR compared to the year prior to PR.
Seymour 2010 25
RCT: compared PR with usual care.
COPD patients with a ratio of FEV1 to FVC of <0.7. Usual care (n=30), PR (n=30)
Patients who had been admitted for an exacerbation of COPD and were randomized to receive either PR or usual care.
Participants were incorporated into standard PR classes consisting of twice-weekly exercise and education sessions (each lasting 2 hour) for a period of 8 weeks. Exercise was a mixture of limb strengthening and aerobic activities, tailored to individual baseline function. Patients in both the UC and PR groups were provided with general information about COPD prior to randomization and offered outpatient appointments with their general practitioner or respiratory team.
Hospital or ED attendance for exacerbationUC (N=30) = 17 (57%) PR (N=30) = 8 (27%)Odds Ratio (95% CI) PR vs UC* = 0.28 (0.10 to 0.82) p = 0.02
10

Table 2: Detailed description of studies involving stable COPD patients
Reference Methods Participants Characteristics Interventions Outcomes
Foglio 1999 26 Observational study of COPD patients before and after a day-hospital based Pulmonary Rehab Programme (PRP). Compared recorded hospitalizations
32 COPD patients with a history of smoking (>20 pack-years) and were ex-smokers.
Patients with stable COPD. The PR programme included optimization of the pharmacological treatment and three 3-hour sessions per week for 8-10 weeks, including: 1) supervised incremental exercise until achieving 30-minute continuous cycling at 50-70% of the maximal load achieved on an incremental cycloergometer exercise test carried out at admission; 2) abdominal, upper and lower limb muscle activities lifting progressively increasing light weights (300-500 g), shoulder and full arm circling.
Compared recorded hospitalizations 2 years before PRP, 1 year before PRP, and 1 year after PRP of the 26 COPD patients. 2 years before PRP: 7 patients had 0, 12 patients had 1, 6 patients had 2, 1 patient had 3 admissions.1 year before PRP: 8 patients had 0, 14 patients had 1, 4 patients had 2, and 0 patients had 3 admissions.1 year post PRP discharge: 24 patients had 0, 2 patients had 1, and 0 patients had 3 admissions.
11

Reference Methods Participants Characteristics Interventions Outcomes
Guell 200027 RCT with follow-up at 3, 6, 9, 12, 18, and 24 months to examine the short- and long-term effects of an outpatient PR program for COPD patients on hospitalization rate.
Randomly assigned 30 patients to the control group and 30 to rehabilitation. COPD patients age ≤75 years and had an FEV1 ≤70% of reference values, FEV1/FVC <65%, and no indication for prescribing home oxygen therapy.
None had experienced an exacerbation or been hospitalized in the previous month.
PR patients engaged in a program of five 30-min sessions weekly on a stationary cycle ergometer, without supplemental oxygen. Started with a workload equivalent to 50% of the maximal load (Wmax) achieved during the baseline progressive exercise test. The load increased in increments provided the patient’s heart rate, arterial oxygen saturation, and blood pressure were stable and exercise was well tolerated. Patients also began a program of home exercise with either 30min of pedalling on a stationary cycle or 1 hour of walking. During the subsequent 6 months, patients attended a single weekly session of exercises for breathing and arm-leg coordination in sitting position (maintenance). Patients were instructed to continue doing their exercises at home without supervision, and they were followed for 1 year.
All 60 patients completed 6 months of follow-up.
The total number of hospitalizations in the control group was 39 with an average of 1.3 ± 1.8 hospitalizations per patient, ranging from 0 to 6. The total number in the PR group was 18 with an average of 0.6 ± 1.0 hospitalizations per patient, ranging between 0 and 4. The difference was not statistically significant (p = 0.57).
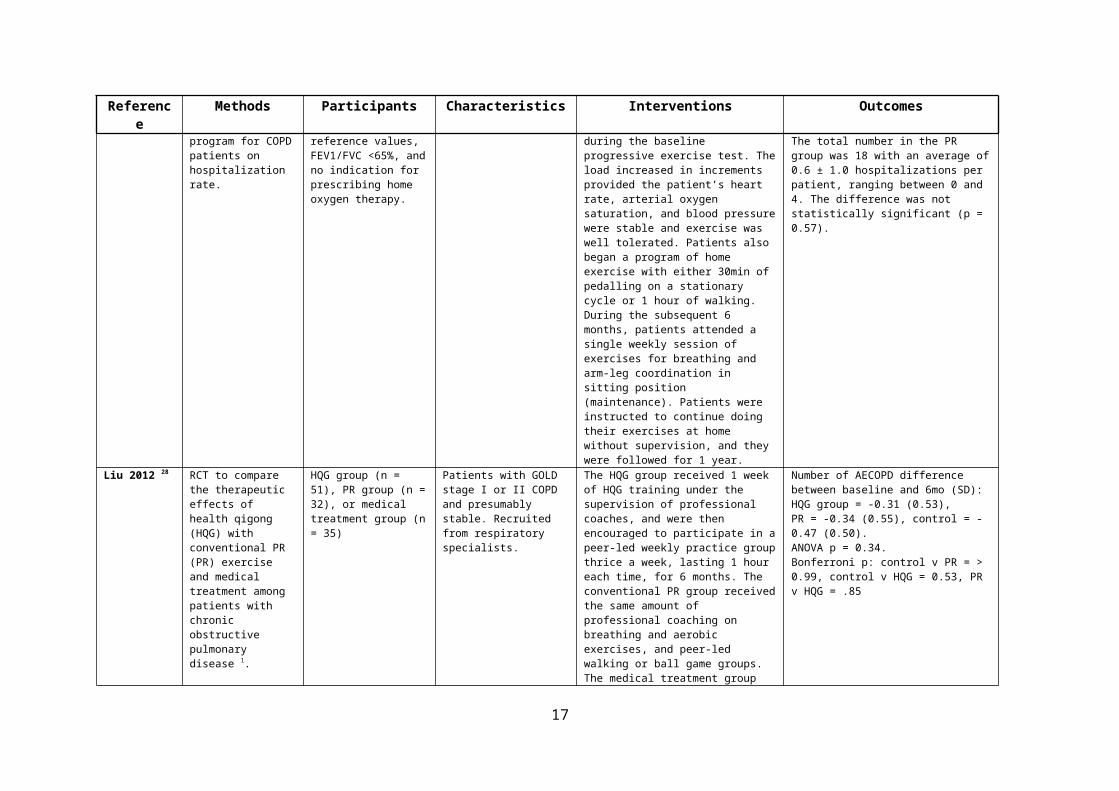
Liu 2012 28 RCT to compare the therapeutic effects of health qigong (HQG) with conventional PR (PR) exercise and medical treatment among patients with chronic obstructive pulmonary disease 1.
HQG group (n = 51), PR group (n = 32), or medical treatment group (n = 35)
Patients with GOLD stage I or II COPD and presumably stable. Recruited from respiratory specialists.
The HQG group received 1 week of HQG training under the supervision of professional coaches, and were then encouraged to participate in a peer-led weekly practice group thrice a week, lasting 1 hour each time, for 6 months. The conventional PR group received the same amount of professional coaching on breathing and aerobic exercises, and peer-led walking or ball game groups. The medical treatment group only received health education on self-exercise. Baseline data were taken before randomization, and outcomes were ascertained at the 6-month follow-up by blinded assessors.
Number of AECOPD difference between baseline and 6mo (SD): HQG group = -0.31 (0.53), PR = -0.34 (0.55), control = -0.47 (0.50). ANOVA p = 0.34. Bonferroni p: control v PR = > 0.99, control v HQG = 0.53, PR v HQG = .85
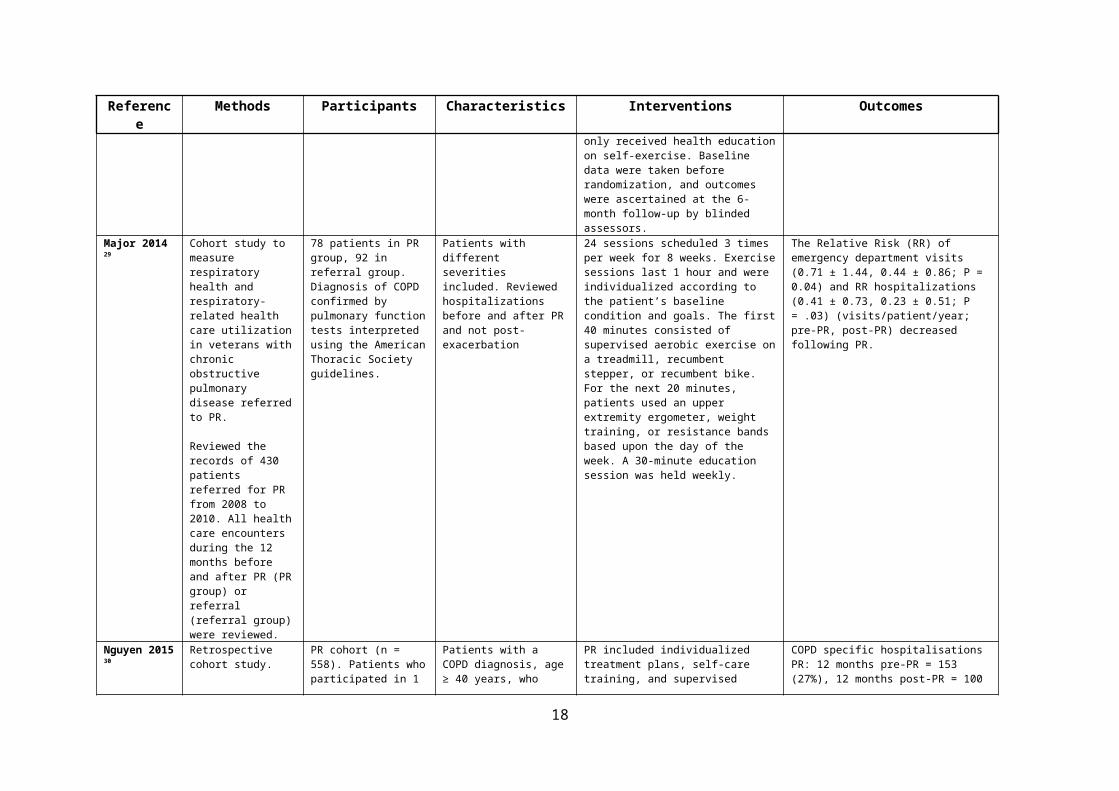
Major 2014 29 Cohort study to measure respiratory health and respiratory-related health care utilization in veterans with chronic obstructive
78 patients in PR group, 92 in referral group. Diagnosis of COPD confirmed by pulmonary function tests interpreted using the American Thoracic Society
Patients with different severities included. Reviewed hospitalizations before and after PR and not post-exacerbation
24 sessions scheduled 3 times per week for 8 weeks. Exercise sessions last 1 hour and were individualized according to the patient’s baseline condition and goals. The first 40 minutes consisted of supervised aerobic exercise on a treadmill, recumbent
The Relative Risk (RR) of emergency department visits (0.71 ± 1.44, 0.44 ± 0.86; P = 0.04) and RR hospitalizations (0.41 ± 0.73, 0.23 ± 0.51; P = .03) (visits/patient/year; pre-PR, post-PR) decreased following PR.
12
Reference Methods Participants Characteristics Interventions Outcomes
pulmonary disease referred to PR.
Reviewed the records of 430 patients referred for PR from 2008 to 2010. All health care encounters during the 12 months before and after PR (PR group) or referral (referral group) were reviewed.
guidelines. stepper, or recumbent bike. For the next 20 minutes, patients used an upper extremity ergometer, weight training, or resistance bands based upon the day of the week. A 30-minute education session was held weekly.
Nguyen 2015 30 Retrospective cohort study.
PR cohort (n = 558). Patients who participated in 1 of 13 PR programs between January 1, 2008, and August 1, 2013, and were continuously enrolled in the health plan ≥ 12 months prior to and after PR.
Cohort 2: Matched non-PR control (n = 1114) did not participate in PR but were matched on age, gender and FEV1
Cohort 3: declined PR controls (n = 90). Patients who were referred to PR but declined because of transportation barriers, scheduling conflicts, or competing responsibilities.
Patients with a COPD diagnosis, age ≥ 40 years, who were treated with a bronchodilator or steroid inhaler. Not post-exacerbation.
PR included individualized treatment plans, self-care training, and supervised exercise.
COPD specific hospitalisationsPR: 12 months pre-PR = 153 (27%), 12 months post-PR = 100 (18%) p = < 0.001Controls: 12 months pre = 108 (10%), 12 months post = 112 (10%) p = 0.81
COPD specific hospitalisations per patientPR: 12 months pre-PR = 0.38 ±0.7, 12 months post-PR = 0.3 ± 0.9 p = 0.05controls: 12 months pre = 0.14 ± 0.5, 12 months post = 0.14 ± 0.5, p = 0.80
13

Reference Methods Participants Characteristics Interventions Outcomes
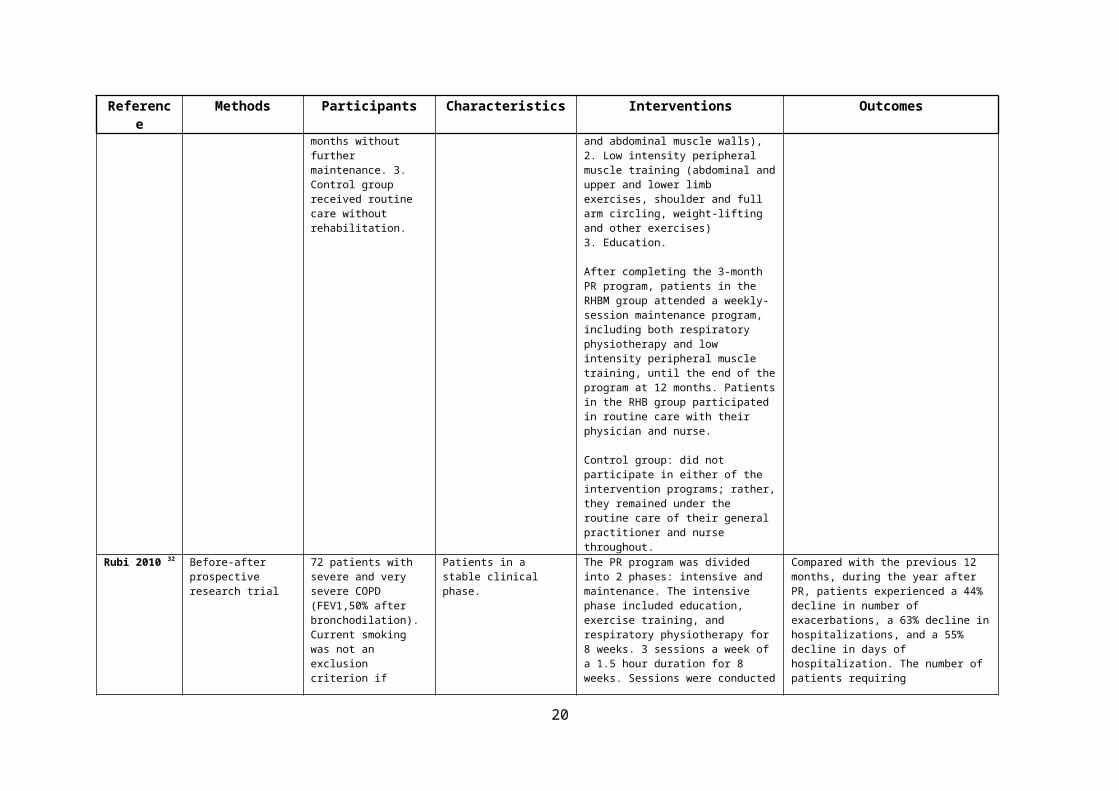
Roman 2013 31 RCT: involving 3 groups of patients with moderate COPD to compare number of hospitalizations.
1. RHBM group received PR for 3 months and rehabilitation maintenance for 12 months. 2. RHB group received PR for 3 months without further maintenance. 3. Control group received routine care without rehabilitation.
Patients with moderate COPD recruited by their family physician. Presumably in a stable condition.
PR = three 60-minute sessions each week for 3 months. Included:1. Respiratory physiotherapy (self-conscious breathing control, diaphragmatic breathing control, and exercises for the chest wall and abdominal muscle walls),2. Low intensity peripheral muscle training (abdominal and upper and lower limb exercises, shoulder and full arm circling, weight-lifting and other exercises)3. Education.
After completing the 3-month PR program, patients in the RHBM group attended a weekly-session maintenance program, including both respiratory physiotherapy and low intensity peripheral muscle training, until the end of the program at 12 months. Patients in the RHB group participated in routine care with their physician and nurse.
Control group: did not participate in either of the intervention programs; rather, they remained under the routine care of their general practitioner and nurse throughout.
12-month evaluation ofCOPD exacerbations. Mean number of hospitalizations (CI 95%):
Control (n = 32) 0.2 (−0.05-0.5)RHB (n = 33) 0.2 (−0.04-0.4)RHBM (n = 32) 0.1 (−0.02-0.3)
14

Reference Methods Participants Characteristics Interventions Outcomes
Rubi 2010 32 Before-after prospective research trial
72 patients with severe and very severe COPD (FEV1,50% after bronchodilation). Current smoking was not an exclusion criterion if patients accepted to enrol in a smoking-cessation program.
Patients in a stable clinical phase.
The PR program was divided into 2 phases: intensive and maintenance. The intensive phase included education, exercise training, and respiratory physiotherapy for 8 weeks. 3 sessions a week of a 1.5 hour duration for 8 weeks. Sessions were conducted in groups of 4 to 6 participants. Exercises were increasing in intensity or duration based on individual progress within each session. Patients also received an individualized exercise program to perform at home that was monitored in successive visit. Patients were evaluated every 2 to 3 months by their chest physician and nurse, and psychosocial support was provided if needed.
Compared with the previous 12 months, during the year after PR, patients experienced a 44% decline in number of exacerbations, a 63% decline in hospitalizations, and a 55% decline in days of hospitalization. The number of patients requiring hospitalizations went from 50 (74.6%) in the previous year to 27 (40.2%) 1 year after PR, which accounts for a 46% reduction.
15
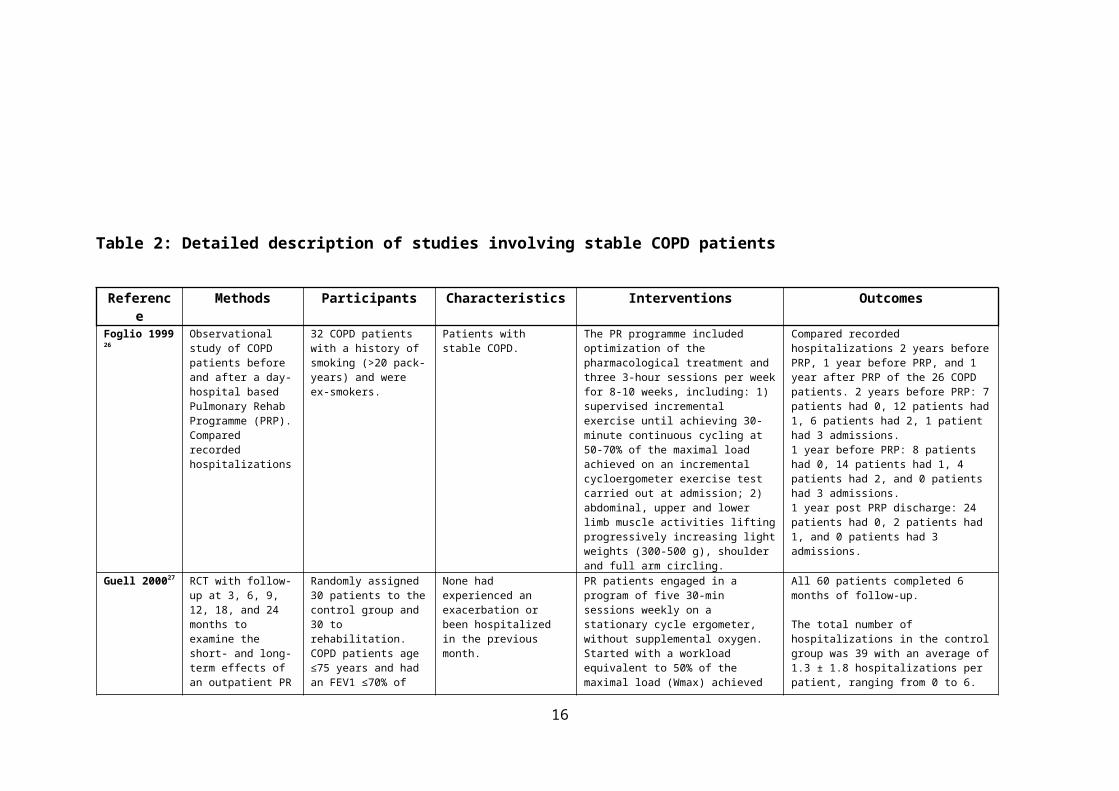
Table 3: Studies involving COPD patients where it was unclear if they were stable or post-AECOPD
Reference Methods Participants Characteristics Interventions Outcomes
Cecins 200833 Before-after study: The number of hospitalizations for a COPD exacerbation and total bed-days (calculated by adding bed-days from all admissions) in the 12-month period before PR and the 12-month period following PR were recorded. Data were collected by patient report and verified by searching hospital databases for patients’ admissions to hospital for a COPD exacerbation and the days spent in hospital.
Patients with a medical diagnosis of COPD (post-bronchodilator FEV1 < 80%, FEV1/FVC< 70%) admitted between 1998-2003
Patients not necessarily post exacerbation. Referred from outpatient respiratory clinics.
2 exercise classes (75min duration) each week for 8 weeks. Exercise training: 20-minute walking program within an enclosed hospital corridor, flexibility and stretching exercises, and a six station exercise circuit in a gym. The 20-minute high-intensity walking program was initially prescribed at an intensity equivalent to 80% of the average walking speed achieved on the pre-PR 6-minute walk test (6MWT). The circuit comprised of upper and lower limb exercises aimed at improving muscle strength and endurance. The intensity or duration of each exercise was increased weekly within symptom tolerance. In addition to the supervised classes, patients were instructed to complete a home exercise program on an additional 2 or 3 days each week.
187 (73%) of the 256 patients who entered PR completed the program.There was a 46% reduction in the number of patients admitted to hospital (71 to 38) with a COPD exacerbation and a 62% reduction in total bed-days (1131 to 432) following PR. Observed 12 months before and 12 months after.No of admissions 12 months before = 71No of admissions 12 months after = 38
16
Reference Methods Participants Characteristics Interventions Outcomes
Golmohammadi 2004 34
Observational study (not included in meta-analysis)
Data from 210 COPD patients. Age > 45 years, a significant history of smoking (>10 pack-years), and persistent symptoms of cough, sputum production and/or dyspnoea at rest or upon exertion even with optimal medical therapy.
Patients were divided into 4 severity groups based on GOLD stages. Some stable and some with more severe COPD.
10 key components of rehabilitation: breathing exercises, education, endurance training, upper extremity conditioning, psychosocial support, adaptations in activities of daily living, relaxation techniques, nutritional counselling, inspiratory muscle conditioning, and interval training. Once enrolled, each participant completed a program over 6 weeks (3 days a week) or 8 weeks (2 days a week). Each class lasts 2.5 hours.
Following PR, there was a slight but non-significant fall in the rate of emergency visits for patients who started the program. Compared to a year prior to enrolment the rate of emergency visits decreased by 24.8% (p = 0.09) one year after PR. Emergency visits before programme:Stage 1 = 41.2 (13.0)stage 2A = 57.0 (14.7)stage 2B = 29.5 (12.3)stage 3 = 41.0 (13.7)
Emergency visits after programmeStage 1 = 13.6 (7.9) p = .085stage 2A = 44.8 (11.2) p = .714stage 2B = 16.3 (6.7) p = .346stage 3 = 54.4 (27.6) p = .974
Hui 2003 35 Before-after study to see if PR program (PRP) improved hospital utilization in patients with COPD.
36 patients with COPD and FEV1 < 60% predicted.
Patients who were referred by specialists or GPs, not necessarily post-exacerbation.
PR programme twice weekly for 8 weeks. Consisted of increasing exercise endurance training, as well as upper and lower limb exercise training. Endurance exercise training commenced with walking, progressing to bicycle ergometer with subsequent addition of steps and jogging on a mini trampoline as appropriate. Incremental progression was based on performance at each session.
In the 12 months following completion of program, hospitalization was reduced compared to prior to starting the program.12 months pre = 1.2 episodes of hospitalizations per patient per year12 months post = 0.6 episodes of hospitalizations per patient per year
Scherer 1998 36 Retrospective chart review of hospitalizations and length of stay following completion of an outpatient PR
74 patients with COPD of which 27 (37%) were male, 47 (63%) were female. Mean age = 69
Mean FEV1/FVC = 48.
Patients with moderate and stable COPD. Not clear if had a recent exacerbation.
PR programme: 36 x 1.5 hour group classes (3 x per week) including education and exercises
26/72 patients had been hospitalised in the year prior to attending PR
Post-PR No. of patients admitted:1 year after (n= 72) = 15 (p = 0.005)2 years after (n = 66) = 15 (p = 0.046)
17
Reference Methods Participants Characteristics Interventions Outcomes
programme in New York. Questionnaire sent to all patients who had completed the programme with items on demographic characteristics, hospitalizations, exercise routine, and patient satisfaction. A retrospective chart review was carried out to compare no. of hospitalisations after PR with before.
72 patients completed the questionnaire.
3 years after (n = 47) = 6 (p = 0.057)4 years after (n = 29) = 2 (p = 0.006)5 years after (n = 15) = 4 (p = 0.589)6 years after (n = 9) = 1 (p = 0.157)
Wright 1983 37 Before-after observational study. Patient reported number of hospitalizations after completion of a 10-week multidisciplinary PR programme in the form of a questionnaire.
57 patients with COPD responded to the questionnaire.
Symptomatic COPD but medically stable. Not clear if had a recent exacerbation.
10-week, 18 visit programme (3 visits in the first 4 weeks then 1 visit per week for the remaining 6 weeks). Each visit lasted 2 hours (1 hour of exercise and 1 hour of education). Exercise included treadmill walking, cycling, and upper extremity exercises. Education topics included diet, medications and energy consumption.
Of the 57 patients who responded to the questionnaire, 16 had episodes of hospitalisation in the year before PR. Of these patients (change group), 4/16 had episodes of hospitalization in the year after PR.
The 41 patients who had no episodes of hospitalization before PR remained free of episodes in the year after.Total no. of episodes for change group year before PR = 497 (mean = 31)Total no. of episodes for change group year after PR = 34 (mean = 2)
18

Results
Results of the searches
The searches yielded over 6,500 studies and following screening of titles and abstracts, 181 full
articles were reviewed.
After the full review process 21 studies were deemed eligible for inclusion. Of these 18 reported
outcomes that could be included in the meta-analysis including 10 RCTs, three cohort studies, and 5
studies comparing admissions one year before and one year after pulmonary rehabilitation (before-
after studies). The three studies that were not included in the meta-analysis 24,34,36 did not report
hospital admission numbers that could be converted for the analysis and are reviewed separately.
There were not enough studies reporting mortality rates and exacerbations recorded by GP visits
and therefore we decided not to include either of these secondary outcomes in the analyses.
Figure 1 shows the screening process and reasons for excluding studies. 35 studies were excluded
for not reporting the main outcomes of interest (e.g. they reported improvements in other domains
of interest such as physical activity, or only reported quality of life and mortality alone, not
hospitalizations), 47 had incorrect comparators (e.g. included other interventions such as pharmacy
and dietetics), 15 were conference abstracts or posters and did not have enough details in the
abstracts to be critically reviewed, and 11 were systematic reviews or meta-analyses that included
results from separate studies already included. Unlike the current review, the previous reviews
considered other outcomes such as measures of quality of life, exercise capacity, pulmonary function
and mortality but not specifically hospitalizations. No studies were removed because of missing or
incomplete data. Only 3 studies were not included because they were not in the English language
and translation was not available. Finally, 11 studies were excluded because the study population did
not have COPD or had other conditions such as asthma or bronchiectasis. The number of patients
included in RCTs ranged between 26-69, 16-177 in the before/after studies, and 51-1,672 in the
cohort studies. Nine out of 21 studies investigated the effects of pulmonary rehabilitation after
AECOPD. Tables 1-3 give details of the 21 studies, separated into those that looked at post-AECOPD,
stable patients, and those where it was unclear if they involved stable or post-AECOPD patients.
19
Hospitalization rates
Table 4 gives full details of the number of patients, person-years at risk, the number of
exacerbations, and hospitalization rates per person-years at risk by treatment group for each type of
study. Overall there was a lower hospitalization rate per person-year at risk for the pulmonary
rehabilitation groups (0.39) compared to the control groups (0.47).
Hospitalization rates per patient-year by study type are shown in Figure 2. For the RCTs the control
groups had a higher overall rate of hospitalizations/patient-year than the pulmonary rehabilitation
groups (0.97 hospitalizations/patient-year, 95% CI 0.67, 1.40 for control versus 0.62
hospitalizations/patient-year, 95% CI 0.33, 1.16 for pulmonary rehabilitation). In the pre- and post-
rehabilitation comparison, there was a significantly higher rate of hospitalizations/patient-year in the
year before rehabilitation (1.24 hospitalizations/patient-year, 95% CI 0.66, 2.34) compared to after
rehabilitation (0.47 hospitalizations/patient-year, 95% CI 0.28, 0.79). However, for the cohort
comparison the ‘control’ groups overall had a lower rate of hospitalizations/patient-year compared
to pulmonary rehabilitation (0.18 hospitalizations/patient-year, 95% CI 0.11, 0.32 for control versus
0.28 hospitalizations/patient-year, 95% CI 0.25, 0.32 for pulmonary rehabilitation). This result
appears to have been influenced predominantly by the results from Nguyen et al 30, a large study
with 1,114 patients in the control group (of which 112 patients were hospitalised in the year post-
rehabilitation) and over 500 in the intervention group (of which 100 were hospitalised in the year
post-rehabilitation).
The hospitalization rate ratios (Figure 3) favoured pulmonary rehabilitation in the RCTs (0.64 95% CI
0.44, 0.93) and before/after studies (0.38 95% CI 0.30, 0.49). However the three cohort studies 23,29,30
did not favour rehabilitation (1.53 95% CI 0.78, 3.02, p = 0.22). Finally, the differences in
hospitalization rates per person-year are shown in Figure 4 and show that pulmonary rehabilitation
was favoured in the RCTs and before/after studies but not in the three cohort studies. Individual
results for each study for person-years at risk and hospital admission rates are shown in Figure 5.
Three studies were not included in the meta-analysis but also found positive relationships between
pulmonary rehabilitation and hospitalizations. An observational study by Golmohammadi et al34
reported a 24.8% decrease in the rate of emergency visits in the year following rehabilitation.
Similarly, in a study of re-exacerbation rates of patients following an AECOPD, Revitt et al 24 reported
a 37.7% reduction in the incidence of exacerbations in the year post-rehabilitation compared to the
year prior to pulmonary rehabilitation. Finally, a study by Scherer and Schmieder 36 carried out a
chart review of hospitalizations one year before and after rehabilitation for up to six years. 26 out of
72 patients were hospitalised in the year before and in the year following pulmonary rehabilitation,
20

only 15 were hospitalized (p = 0.01). Six years after rehabilitation, only nine patients were followed
up, one of whom had an exacerbation to hospital (p = 0.16).
Sensitivity analysis: stable COPD
A sensitivity analysis was carried out to analyze the effect of pulmonary rehabilitation on
hospitalizations from studies which looked at stable COPD patients and results from seven studies
(see Table 2) were included. Figure 6 shows the admission rates per patient-year by study type and
year following the post-hoc sensitivity analysis. Results (Table 5) appeared to be in the same
direction as the main analysis, but only the before-after studies showed a conclusively significant
effect.
Risk of bias in included studies
Results from two risk of bias assessments are shown in Figures 7 and 8: one for RCTs based upon the
Cochrane Risk of Bias tool, and the other for the cohort and before-after studies based upon a
combination of the Cochrane tool and the Newcastle-Ottowa scale. Details of the individual
assessments for each study can be found in the supplementary materials.
Table 4. Patients, person-years at risk, hospitalizations and hospitalization rates per person-year at risk in studies in the meta-analysis by treatment group
Control group: Pulmonary Rehabilitation group:Reference Patients Patient-
yearsHospitaliz
ationsRate Patients Patient-
yearsHospitaliz
ationsRate
RCT:Behnke 2003 12 18.0 14.0 0.78 14 21.0 3.0 0.14Boxall 2005 23 11.5 16.0 1.40 23 11.5 11.0 0.96Eaton 2009 50 12.5 23.0 1.84 19 4.8 4.0 0.84Guell 2000 30 60.0 39.0 0.66 30 60.0 18.0 0.30Ko 2011 30 30.0 30.9 1.03 30 30.0 30.0 1.00Liu 2012 35 17.5 33.6 1.92 32 16.0 33.3 2.08Man 2004 16 4.0 9.1 2.28 18 4.5 6.3 1.40Murphy 2005 15 7.5 5.0 0.67 16 8.0 2.0 0.25Roman 2013 23 23.0 4.6 0.20 22 22.0 4.4 0.20Seymour 2010 30 7.5 10.0 1.33 30 7.5 2.0 0.27Total 264 191.5 185.2 0.97 234 185.3 114.0 0.62Cohort:Major 2014 78 78.0 46.0 0.60 78 78.0 17.9 0.23Nguyen 2015 1114 1114.0 156.0 0.14 558 558.0 167.4 0.30Rasekaba 2009 22 22.0 21.0 0.96 29 29.0 2.0 0.07
21

Total 1214 1214.0 223.0 0.18 665 665.0 187.4 0.28Before and after:Cecins 2008 177 177.0 127.0 0.72 177 177.0 61.0 0.35Foglio 1999 26 26.0 22.0 0.85 26 26.0 2.0 0.08Hui 2003 36 36.0 43.0 1.19 36 36.0 21.6 0.60Rubi 2010 72 72.0 172.8 2.40 72 72.0 64.8 0.90Wright 1983 16 16.0 41.6 2.60 16 16.0 4.8 0.30Total 327 327.0 406.4 1.24 327 327.0 154.2 0.47All study types:Grand Total 1805 1732.5 814.6 0.47 1226 1177.3 455.5 0.39
Table 5 Admission rates per patient-year by study type and treatment for stable COPD patients
Treatment Rate (95% CI)RCT:
Control 0.768 (0.387, 1.527)PR 0.568 (0.180, 1.788)
Cohort:Control 0.169 (0.104, 0.276)
PR 0.291 (0.270, 0.315)Before and after:
Control 1.988 (1.260, 3.137)PR 0.682 (0.337, 1.379)
Figure 2. Admission rates per patient-year by study type and treatment
Figure 3. Admission rate ratios (PR/Control) by study type
Figure 4. Differences in admission rate per person-year (PR - Control) by study type
Figure 5. Results from Individual Studies: a) Person-years at risk; b) Admission rates per person-
year at risk.
Figure 6. Admission rates per patient-year by study type and year for stable COPD patients
Figure 7. Risk of bias assessment – randomised controlled trials
Figure 8. Risk of bias assessment – cohort studies
Discussion
The findings of these studies provide evidence that pulmonary rehabilitation reduces
hospitalizations for AECOPD in the short term. Results from RCTs and cohort studies showed lower
admission rates after rehabilitation compared to usual care. Additionally, studies that compared
COPD hospital admission numbers before and after pulmonary rehabilitation showed an overall
reduction in admission rates. After a sensitivity analysis including studies that looked at stable COPD,
the same pattern was found.
22

Only one study did not favour pulmonary rehabilitation when compared to the control group.30 A
larger proportion of patients in the rehabilitation group (18%) were hospitalized one year after the
programme compared to the control group (10%). However, a 27% reduction in hospitalizations
from baseline was observed in the rehabilitation group, whereas hospitalization in the control group
did not change.
It is interesting to see in this large study by Nguyen and colleagues 30 that hospitalizations appeared
to be worse in the rehabilitation group compared to the control group one year after the
programme. Pulmonary rehabilitation participants in this study had a high prevalence of diabetes
(21%), depression (21%), and heart failure (16%) than those in the control group. Furthermore, there
were significant differences in socioeconomic characteristics, race/ethnicity, FEV1 % predicted,
Charlson Comorbidity Index, and health care resource use. This may partly explain why pulmonary
rehabilitation was not as effective in the rehabilitation group but also illustrate the possibility that
those who are referred to such programmes have more contact with healthcare services. In contrast
to the results of Nguyen et al30, one UK based cohort study24 reported a 37.7% reduction in the
incidence of admissions in the year post pulmonary rehabilitation compared to the year prior.
The current review compared the results of three different study designs, each with their own
advantages and disadvantages which should be taken into consideration when interpreting these
results. RCTs have experimental advantages that are well known but are often limited by ethical
considerations and smaller study groups. Cohort studies can be done over long periods of time with
large numbers of participants but can be subjected to confounding. Finally, before-after comparison
studies can overcome some of the ethical concerns of RCTs but can also be biased by regression to
the mean. For these reasons we looked at outcomes from different study types.
There are a number of limitations that mean the results should be interpreted with caution. Firstly,
the small sample sizes of the groups included reduce the strength of the findings of studies in this
review. There was a high risk of bias for blinding of participants and in some cases, an unclear or high
risk with blinding of assessors due to the nature of these studies. Small trials and inadequate
randomisation of allocation sequence, inadequate concealment or no blinding may exaggerate
intervention effects38. In three of the cohort studies26,29,32 participants were either entirely or mostly
male participants thus reducing the representativeness of the exposed and increasing the risk of
selection bias. Although the prevalence of COPD is believed to be higher in men than women39 the
results of these studies are not necessarily generalizable to the population.
23

Heterogeneity between studies was not assessed in this review but the interventions varied
considerably. Nearly all of the studies included met the BTS guidelines9 for pulmonary rehabilitation,
including a minimum of twice weekly supervised sessions, between 6-12 weeks duration and a
combination of muscle resistance and aerobic training. However, the programmes still varied
between studies in duration, frequency of sessions, types of exercises, the inclusion of home
exercise programmes, and the degree to which education was incorporated. A sensitivity analysis on
the ‘dose’ of interventions was not done because of the heterogeneity between studies. Another
possible limitation is that admission numbers were based upon hospital counts and it was not always
clear if the admissions to hospital were specifically due to an AECOPD. The long term effects of
pulmonary rehabilitation on admissions is unclear as the pooled results compared 1 year before and
1 year after pulmonary rehabilitation. Only one study looked at the long term effects 36 up to six years
after. The studies reviewed also did not assess the effects of repeat attendance to rehabilitation
programmes as this was often not stated in studies, and this requires further investigation.
Another reason for discrepancies between studies may be because there is no standardisation or
accreditation for pulmonary rehabilitation programmes. This may result in significant variation in
method of delivery and quality of programmes. As the results from Nguyen et al30 highlighted,
although some studies have attempted to adjust for comorbidities and to match the comparison
groups, there may be differences between those who participate in pulmonary rehabilitation and
those who do not. Finally, a recent national UK clinical audit has revealed that many patients are not
being referred or have to wait longer than recommended to receive pulmonary rehabilitation and
therefore the true benefits are not necessarily being captured40.
A systematic review by Puhan and colleagues11 found that pulmonary rehabilitation post AECOPD
significantly reduced hospitalizations (pooled Odds Ratio: 0.22 95% CI: 0.08, 0.58; I2 = 51%).
Participants had previously exacerbated and the follow-up duration ranged from 3 to 18 months.
This current review compared hospitalizations for COPD patients one year before and after a
rehabilitation programme, and found that hospitalizations generally declined one year after the
programme or had lower rates when compared to the control groups. In contrast to the review by
Puhan et al11 that assessed the effects of pulmonary rehabilitation after AECOPD, the current study
assessed a variety of patient groups, not all of them had recently been admitted for an exacerbation.
However, as in the review by Puhan et al11, studies that were included in this analysis generally had
small sample sizes and methodological shortcomings with blinding and concealment that may have
been sources of potential bias. Nevertheless, the results from Puhan et al11 and those from the RCTs
included in this review, suggest that pulmonary rehabilitation may be an effective intervention for
reducing future hospitalizations.
24
Other reviews have also investigated the benefits of pulmonary rehabilitation. Ochmann et al41
reported positive long-term functional effects of rehabilitation and evidence of secondary benefits
including reductions in the use of healthcare resources. Another42 examined the role of pulmonary
rehabilitation in the peri- and early post-hospitalization setting on reducing the risk of readmission
but reported less positive results from recent trials. The authors discussed poor referral rates for
post-hospitalization pulmonary rehabilitation as a potential barrier for reducing readmissions.
In other studies pulmonary rehabilitation has been shown to be cost-saving and can reduce
healthcare utilisation20 with one study showing an overall cost saving of £152 per patient per
pulmonary rehabilitation programme.43 However, translating the cost of exacerbations in terms of
hospitalizations and the impact of physiotherapy on healthcare usage requires further investigation.
Models are being developed using validated records of COPD exacerbations from electronic
healthcare records44 to determine the potential cost savings in terms of exacerbation reduction and
health care utilization reduction that could be achieved if all eligible COPD patients attended
pulmonary rehabilitation classes.
Conclusions and future research
Pulmonary rehabilitation is an extremely valuable intervention for improving many aspects of COPD
patient’s lives. This review provides some evidence to suggest that providing rehabilitation is
beneficial for reducing hospitalizations and therefore healthcare consumption. Evidence has shown
that admissions after a course of pulmonary rehabilitation are lower than before therapy. Also,
when compared to usual care, admissions can be reduced with rehabilitation. However, pooled
results from the cohort studies did not favour pulmonary rehabilitation and suggest that for some
patients it may not reduce the risk of future hospitalizations. Due to the heterogeneous nature of
the studies and methodological limitations further research is needed, particularly in terms of
detecting if admissions were specifically for AECOPD, and the subsequent cost savings for healthcare
services. Given that all patients with moderate to severe COPD should be referred to pulmonary
rehabilitation, and overall results from this systematic review suggest pulmonary rehabilitation has
an impact on reducing hospitalizations, this work should help to convince potential patients and
healthcare providers of its importance.
25
Acknowledgements
This study was funded by a research grant from the UK Chartered Society of Physiotherapy (CSP).
The funder was not involved in the design or conduct of the study. However we wish to acknowledge
helpful comments received from an Expert Group coordinated by CSP which included Alison Coe,
Anne Bruton, Becca Bryant, Brenda O’Neill, Ian Culligan, Jamie Forrester, Jane Mullins, Judith
Colligan, Julia Bott, Kat Savage, Marianne Mulligan, Marie Buxton, Noel Baxter, Rhiannon Kendrick
and Sally Singh.
Contributorship statementMS and JKQ conceived the study. EM and MS carried out searches and articles were screened and
reviewed by EM, TP and MS. RN performed the statistical analyses. EM and TP produced the first
drafts and all authors contributed to subsequent drafts. MS and JKQ approved the final version.
References
1. COPD Working Group HQO. Pulmonary rehabilitation for patients with chronic pulmonary disease (COPD): An evidence-based analysis. Ontario Health Technology Assessment Series. 2012;12(6):1-75.
2. World Health Organization (WHO). World Health Statistics 2008. 2008. http://www.who.int/gho/publications/world_health_statistics/EN_WHS08_Full.pdf
3. Global Initiative for Chronic Obstructive Lung Disease (GOLD). Global strategy for the diagnosis, management, and prevention of chronic obstructive pulmonary disease. 2015. www. goldcopd.org/guidelines-global-strategy-for-diagnosis-management.html
4. Anthonisen NR, Manfreda J, Warren CP, Hershfield ES, Harding GK, Nelson NA. Antibiotic therapy in exacerbations of chronic obstructive pulmonary disease. Ann Intern Med. 1987;106(2):196-204.
5. NHS. COPD Commissioning Toolkit: a resource for commissioners. 2012. https://www.gov.uk/government/publications/commissioning-toolkit-for-respiratory-services
6. Dalal AA, Shah M, D'Souza AO, Rane P. Costs of COPD exacerbations in the emergency department and inpatient setting. Respir Med. 2011;105(3):454-460.
7. McCamley C, Hyde E, Watson C, Moodley Y. The COPD linkage service reduces hospital admissions in patients with COPD. Respirology. 2012;17:63.
8. Spruit MA, Singh SJ, Garvey C, et al. An official American Thoracic Society/European Respiratory Society statement: key concepts and advances in pulmonary rehabilitation. Am J Respir Crit Care Med. 2013;188(8):e13-64.
9. Bolton CE, Bevan-Smith EF, Blakey JD, et al. British Thoracic Society guideline on pulmonary rehabilitation in adults. Thorax. 2013;68 Suppl 2:ii1-30.
26
10. McCarthy B, Casey D, Devane D, Murphy K, Murphy E, Lacasse Y. Pulmonary rehabilitation for chronic obstructive pulmonary disease. Cochrane Database Syst Rev. 2015;2:CD003793.
11. Puhan MA, Gimeno-Santos E, Scharplatz M, Troosters T, Walters EH, Steurer J. Pulmonary rehabilitation following exacerbations of chronic obstructive pulmonary disease. [Review][Update of Cochrane Database Syst Rev. 2009;(1):CD005305; PMID: 19160250]. Cochrane Database of Systematic Reviews. 2011;10.
12. Moher D, Liberati A, Tetzlaff J, Altman DG. Preferred reporting items for systematic reviews and meta-analyses: the PRISMA statement. BMJ. 2009;339.
13. StataCorp. Stata: Release 14. Statistical Software. College Station, TX: StataCorp LP;. 2015.
14. Newson R. SCENTTEST: Stata module to compute scenario arithmetic means and their difference. 2015. https://ideas.repec.org/c/boc/bocode/s457904.html
15. Higgins J, Green S. Cochrane handbook for systematic reviews of interventions. Chichester, UK: John Wiley & Sons Ltd., 2008.
16. Wells G, Shea B, O’Connell D, Peterson J, Welch V, Losos M TP. The Newcastle-Ottawa Scale (NOS) for assessing the quality of nonrandomised studies in meta-analyses.
17. Behnke M, Jorres RA, Kirsten D, Magnussen H. Clinical benefits of a combined hospital and home-based exercise programme over 18 months in patients with severe COPD. Monaldi Archives for Chest Disease - Pulmonary Series. 2003;59(1):44-51.
18. Boxall AM, Barclay L, Sayers A, Caplan GA. Managing chronic obstructive pulmonary disease in the community. A randomized controlled trial of home-based pulmonary rehabilitation for elderly housebound patients. Journal of cardiopulmonary rehabilitation. 2005;25(6):378-385.
19. Eaton T, Young P, Fergusson W, et al. Does early pulmonary rehabilitation reduce acute health-care utilization in COPD patients admitted with an exacerbation? A randomized controlled study. Respirology. 2009;14(2):230-238.
20. Ko FW, Dai DL, Ngai J, et al. Effect of early pulmonary rehabilitation on health care utilization and health status in patients hospitalized with acute exacerbations of COPD. Respirology. 2011;16(4):617-624.
21. Man WD, Polkey MI, Donaldson N, Gray BJ, Moxham J. Community pulmonary rehabilitation after hospitalisation for acute exacerbations of chronic obstructive pulmonary disease: randomised controlled study. BMJ. 2004;329(7476):1209.
22. Murphy N, Bell C, Costello RW. Extending a home from hospital care programme for COPD exacerbations to include pulmonary rehabilitation. Respiratory Medicine. 2005;99(10):1297-1302.
23. Rasekaba TM, Williams E, Hsu-Hage B. Can a chronic disease management pulmonary rehabilitation program for COPD reduce acute rural hospital utilization? Chronic Respiratory Disease. 2009;6(3):157-163.
24. Revitt O, Sewell L, Morgan MDL, Steiner M, Singh S. Short outpatient pulmonary rehabilitation programme reduces readmission following a hospitalization for an exacerbation of chronic obstructive pulmonary disease. Respirology. 2013;18(7):1063-1068.
25. Seymour JM, Moore L, Jolley CJ, et al. Outpatient pulmonary rehabilitation following acute exacerbations of COPD. Thorax. 2010;65(5):423-428.
26. Foglio K, Bianchi L, Bruletti G, Battista L, Pagani M, Ambrosino N. Long-term effectiveness of pulmonary rehabilitation in patients with chronic airway obstruction. European Respiratory Journal. 1999;13(1):125-132.
27
27. Guell R, Casan P, Belda J, et al. Long-term effects of outpatient rehabilitation of COPD: A randomized trial. Chest. 2000;117(4):976-983.
28. Liu XD JH, Ng BHP, Gu YH, Wu YC, Lu G. Therapeutic effects of qigong in patients with COPD: a randomized controlled trial. Hong Kong J Occup Ther. 2012;22(1):8.
29. Major S, Moreno M, Shelton J, Panos RJ. Veterans with chronic obstructive pulmonary disease achieve clinically relevant improvements in respiratory health after pulmonary rehabilitation. Journal of Cardiopulmonary Rehabilitation & Prevention. 2014;34(6):420-429.
30. Nguyen HQ, Harrington A, Liu ILA, Lee JS, Gould MK. Impact of pulmonary rehabilitation on hospitalizations for chronic obstructive pulmonary disease among members of an integrated health care system. Journal of Cardiopulmonary Rehabilitation and Prevention. 2015;35(5):356-366.
31. Roman M, Larraz C, Gomez A, et al. Efficacy of pulmonary rehabilitation in patients with moderate chronic obstructive pulmonary disease: a randomized controlled trial. BMC family practice. 2013;14:21.
32. Rubi M, Renom F, Ramis F, et al. Effectiveness of Pulmonary Rehabilitation in Reducing Health Resources Use in Chronic Obstructive Pulmonary Disease. Archives of Physical Medicine and Rehabilitation. 2010;91(3):364-368.
33. Cecins N, Geelhoed E, Jenkins SC. Reduction in hospitalisation following pulmonary rehabilitation in patients with COPD. Australian Health Review. 2008;32(3):415-422.
34. Golmohammadi K, Jacobs P, Sin DD. Economic evaluation of a community-based pulmonary rehabilitation program for chronic obstructive pulmonary disease. Lung. 2004;182(3):187-196.
35. Hui KP, Hewitt AB. A simple pulmonary rehabilitation program improves health outcomes and reduces hospital utilization in patients with COPD. Chest. 2003;124(1):94-97.
36. Scherer YK, Schmieder LE. Pulmonary rehabilitation: is it cost effective? The Journal of the New York State Nurses' Association. 1998;29(3-4):16-20.
37. Wright RW, Larsen DF, Monie RG, Aldred RA. Benefits of a community-hospital pulmonary rehabilitation program. Respiratory Care. 1983;28(11):1474-1479.
38. Kjaergard LL, Villumsen J, Gluud C. Reported methodologic quality and discrepancies between large and small randomized trials in meta-analyses. Ann Intern Med. 2001;135(11):982-989.
39. Chapman KR, Tashkin DP, Pye DJ. Gender bias in the diagnosis of COPD. Chest. 2001;119(6):1691-1695.
40. Steiner M H-BJ, Lowe D, Searle L, Skipper E, Welham S, Roberts CM. Pulmonary Rehabilitation: Steps to breathe better. National Chronic Obstructive Pulmonary Disease (COPD) Audit Programme. Pulmonary Rehabilitation services in England and Wales 2015. National clinical audit report. London: RCP. 2016. https://www.rcplondon.ac.uk/projects/national-copd-audit-programme-pulmonary-rehabilitation-workstream
41. Ochmann U, Jorres RA, Nowak D. Long-term efficacy of pulmonary rehabilitation: A state-of-the-art review. Journal of Cardiopulmonary Rehabilitation and Prevention. 2012;32(3):117-126.
42. Maddocks M, Kon SS, Singh SJ, Man WD. Rehabilitation following hospitalization in patients with COPD: can it reduce readmissions? Respirology. 2015;20(3):395-404.
28

43. Griffiths TL, Phillips CJ, Davies S, Burr ML, Campbell IA. Cost effectiveness of an outpatient multidisciplinary pulmonary rehabilitation programme. Thorax. 2001;56(10):779-784.
44. Wehrmeister FC, Knorst M, Jardim JR, et al. Pulmonary rehabilitation programs for patients with COPD. Jornal Brasileiro de Pneumologia. 2011;37(4):544-555.
Appendix
Figure 9. Risk of bias assessment for RCT’s: details of individual studies
Figure 10. Risk of bias assessment for cohort studies and before-after studies
Figure 11. Person-years at risk in studies in the meta-analysis
Figure 12. Admissions rates per person-year at risk in studies in the meta-analysis
Figure 13. Study treated/untreated rate ratios (with symbol size proportional to total patient-years at risk)
Figure 14. Study treated-untreated rate differences (with symbol size proportional to total patient-years at risk)
29





























