Embed Size (px)
Citation preview
Abstracts of work presentedat the
2017 Spring Meetingof the
British Geriatrics Society
26 - 28 April 2017Sage, Gateshead/Newcastle

These abstracts are copied directly from the online submission sys-tem and are edited for uniformity of format. Authors are invited and
given at least a week to notify the sub-editor of amendments.
Abd Hamid, M A IAbdulla, AAblett, AAhmad, FAitken, EAkram, ZAlcock, LAlder, SAlexander, HAllan, LAnderson, SAndrews, AArcher, JArnott, RArora, AAucott, L S
Baczynska, A MBallinger, CBarlas, R SBaxter, MBaxter, RBaylis, DBeckett, NBennett, HBettencourt-Silva, J HBirtles, PBisheswar, RBoardman, ABond, C JBoulton, CBowles, K MBriggs, SBrittain, KBrock, PBrooke, SBrown, LBryan, RBulgiba, ABunn, J GBurgon, VBurgoyne, N
Carlisle, JCarroll, CCarter, BChin, A VChivers, NChoo, W YChu, A S Clark, A BConnolly, AConroy, SCooper, CCopeland, RCozens, GCroft, SCronin, ACumming, KCumming, R G
Davies, JDavies, KDavies, NDavis, DDe Roos, BDennison, E M
Dodds, RDodds, SDonaldson, A I CDos Santos, M EDoshi, MDotchin, CDrayson, JDuinmaijer, A
Eastment, JEaton, PEdward, G DEdwards, CElliott, CEngstrom, GEvans, L
Farooq, HFisher, JFlatt, AFleming, JFogarty, AFoster, E JFox, AFox, NFrancis, NFrith, J
Galna, BGalvin, JGani, NGarland, AGarside, MGeorge, JGeoteyn, JGibson, VGiwa, AGoh, C HGordon, A LGosrani, SGowing, SGranic, AGray, KGray, W KGrounds, M DGrout, G
Hagan, MHairi, N NHartle, AHarvey, MHeagerty, AHeward, JHewitt, JHill, K DHill, MHohenberg, M IHowlett, WHowson, F F AHumphreys, NHunt, K
Irani, TIrwin, C
Jaafar, M HJacques, R
Jagger, CJalal, HJohansen, AJohnston, HJohnstone, A MJones, R
Kafri, M WKamaruzzaman, S BKandiben, SKaur, YKellet-Wright, JKersh, RKhoo, E MKhor, H MKilsby, AKing, KKirkwood, T B LKisoli, AKissima, J
Lakhani, D LLaw, JLea, SLee, P L Lennon, L TLewis, L ALim, S E RLim, W FLoh, D ALowe, G
MacKenzie, LMadzlan, M FMann, JMarsh, AMartin-Ruiz, CMason, SMat, SMathew, PMavrodaris, AMcCarthy, KMcCartney, JMcCormack, TMcCormack, VMcDonald, MMetcalf, A KMiller, C JMiller, NMohdHairi, FMoriarty, EMossop, HMoug, SMyint, P K
Nell, JNewton, J LNoblet, G
Oates, LO’Keeffe, COuslander, J GOwen, SOxtoby, J
Paddick, S-M
3461, 638133459592578912295
52534552114572149816312844256427602934642820
5717134, 35, 381534344156436, 44, 531244643210, 4534
643, 47292536
44, 476152725, 263, 48, 621748
24484554194763
184248246041333919, 38, 39, 40
5947346427634214385, 12, 42603343, 44, 473, 6235, 46, 48, 614430
11345761573, 621, 6351244148532942
1348
3764
43242824546
4550, 51341748235138, 50, 51733434862
22632934493055153429
513425, 2674364371124148572614225834124711, 5, 45, 63
5919, 4032
6164476329
3, 48, 62
Page, CPapachristou, EPapacosta, OParrott, APatchett, CPatel, H PPattison, TPearce, LPeramalah, DPeters, SPhelan, FPichel, APotter, J FPrice, R OPurkis, APutnam, H
Rai, SRamsay, S ERawles, LReynolds, HRichards, KRichardson, SRiglin, JRoberts, H CRobinson, LRobinson, SRochester, LRogathi, JRogers, ARose, TRoshaslina, RRosli, RRutter, S
Saedon, N ISawicka, Z SSayer, A A
Scheibl, FShahrul, S BShavlakadze, TShaw, S CSingh, ISkelly, RSmith, T OSoiza, R LStechman, MSteffan, BStone, LStrain, W DStrassheim, VStrike, GStuart, SSubramanian, PSyddall, H E
Tan, MTan, M P
Tan, P JTappen, RTay, H STaylor, MThornton, JTippu, ZTunster, H
Urasa, S
Vardon, EVon Zglinicki, T
Wakeman, RWalker, R
Wannamethee, S GWard, KWardle, DWestbury, LWeston, KWhincup, P HWiblin, LWilliams, LWood, A DWoodbridge, SWoodcock, TWright, H
Yarwood, VYoung, C
749499730, 36, 44, 52271342321574, 45315546
284919582122452, 53, 5519535946559353412
38, 50, 512136, 43, 44, 47, 52, 53, 55243844525460545123, 62154033, 55593544
2734, 35, 37, 38, 40, 50, 5150, 51471016, 18, 20481324
48
1443
28
3, 46, 48, 58, 61, 6249182336,446149561745175729
4854
Table of Contents
Platform Presentations
Wednesday ......................................................................................... 1 - 5
Posters
Clinical Quality ......................................................................................... 6 - 33Biology and Social GerontologyBone, Muscle and Rheumatology
.........................................................................................
.........................................................................................34 - 3536 - 37
Cardiovascular ......................................................................................... 38 - 40Education and Training ......................................................................................... 41 - 42Epidemiology ......................................................................................... 43 - 48Eyes, Ears and TeethFalls, Fractures and Trauma
.........................................................................................
.........................................................................................49
50 - 51Health Services Research ......................................................................................... 52 -55Neurology and Neurosciences ......................................................................................... 56Other Medical ConditionsParkinson’s Disease
.........................................................................................
.........................................................................................57
58 - 61Psychiatry ......................................................................................... 62
Platform Presentations
Friday, Session L ......................................................................................... 63 - 64

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
1
Scientific Research – Epidemiology [PLATFORM PRESENTATION]
COGNITIVE IMPAIRMENT AND OUTCOMES IN OLDER UNSELECTED ACUTE SURGICAL ADMISSIONS: A MULTICENTRE STUDY
A Ablett1, K McCarthy2, B Carter3, L Pearce4, M Stechman5, S Moug6, J Hewitt7, P K Myint1 1. University of Aberdeen, 2. North Bristol NHS Trust, 3. King’s College London, 4. Manchester Royal Infirmary, 5. University Hospital of Wales, 6. University of Glasgow, 7. Cardiff University
Introduction The prevalence of cognitive impairment is set to rise. One valid method of measuring cognitive function is through using the Montreal Cognitive Assessment (MoCA). Consequently, we were interested in investigating the outcome of older surgical patients with poor cognition who are admitted to the acute surgical setting.
Methods We identified older surgical patients who had lowest 25% of cognition using consecutive acute surgical admission data from Older Persons Surgical Outcomes Collaboration (www.OPSOC.eu) (2013 and 2014). The effect of having a low MoCA score on relevant outcomes of receipt of surgical intervention, 30- and 90-day mortality, readmission within 30-days and hospital length of stay were examined using multivariate logistic regression models, adjusting for age, sex, polypharmacy, haemoglobin, albumin and having diabetes for the first outcome and additionally controlling for surgical intervention for other outcomes.
Results A total of 660 older patients admitted to five surgical units (mean age (SD) = 77(8.1) years) were included. 148 (22.4%) had a MoCA score in the lowest 25% (≤17). The emergency operation rate was 12.0% (N=79) in this cohort. Characteristic comparisons with the rest of the group showed increasing age, length of hospital stay, polypharmacy and low haemoglobin levels were all significantly associated with having a low MoCA score. A low MoCA score was not associated with sex, low albumin, diabetes or receiving surgical intervention. Multivariate analyses showed low MoCA group had increased 30-day mortality (adjusted odds ratio=2.84 (95% CI:1.29-6.23; P = 0.009) compared to the remaining cohort. No significant association was found between having a low MoCA score and the other outcomes including receipt of surgical intervention.
Conclusion Whilst low MoCA doesn’t appear to preclude the receipt of emergency surgical intervention among older people, our findings highlight the poor prognosis associated with cognitive impairment in older surgical patients.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
2
Scientific Research – Neurology and Neurosciences [PLATFORM PRESENTATION] WHAT IS THE EFFECT OF DELIRIUM UPON THE TRAJECTORY OF COGNITIVE DECLINE IN THE LEWY BODY DISORDERS? A RETROSPECTIVE EXAMINATION OF EPISODES OF DELIRIUM IN A LONGITUDINAL COHORT OF PEOPLE WITH PARKINSON’S DISEASE (PD), PARKINSON’S DISEASE DEMENTIA (PDD) AND DEMENTIA WITH LEWY BODIES (DLB) V McCormack, L Allan, D Davis, S Richardson, B Steffan Newcastle University
Introduction Delirium is a common neurocognitive syndrome that affects up to 40% of elderly inpatients. Consequences of delirium include increased institutionalisation, morbidity and mortality. It has been shown to exacerbate cognitive decline in Alzheimer’s disease (AD) but no work has explored the impact of delirium on Lewy Body dementias - Dementia with Lewy Bodies (DLB) and Parkinson’s Disease Dementia(PDD).
Participants 47 patients previously enrolled in clinicopathological study who had donated to Newcastle Brain Tissue Resource. This comprised 28 DLB/PDD, 9 AD, 6 Parkinson’s Disease, and 4 controls.
Methods From hospital notes of participants, case “vignettes” were created documenting the verbatim comments by clinicians with regard to behaviour and cognition. Vignettes were assigned a delirium diagnosis by senior clinical researchers who were blinded to disease status. Cognitive function was based on performance in CAMCOG and MMSE assessments.
Results Delirium was present in 60.4% of admissions. 39 patients (83%) had at least one episode of delirium. Direct reference of “Delirium” was only documented in 6 vignettes. Baseline CAMCOG and MMSE scores were higher in those that did not have an episode of delirium. This difference was not statistically significant (p=0.149). Longitudinal modelling did not show cognitive decline in relation to delirium incidence.
Commentary Delirium was common and clinically under-recognised in the cohort. Cognitive function was not seen to decline in response to delirium however this may be due to practice effects and survival bias. Future work should explore the relationship between delirium and cognitive decline in LBDs prospectively.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
3
Scientific Research – Psychiatry and Mental Health [PLATFORM PRESENTATION]
EXTERNAL VALIDATION OF A SHORT SCREENING TOOL FOR DEMENTIA IN A RESOURCE POOR, LOW LITERACY SETTING
L Stone1, J Heward1, S-M Paddick2, K Gray2, C Dotchin2, R Walker2
1. The Medical School, Newcastle University, Newcastle Upon Tyne, UK, 2 Northumbria Healthcare NHS Foundation Trust, North Tyneside General Hospital, North Shields, UK
Introduction Cognitive screening tools for dementia have been repeatedly shown to be biased in populations with low levels of education and literacy. The IDEA-IADL study (Collingwood, Global Health Action, 2014; 7) validated a tool in the Hai District of Tanzania which was free from educational bias, incorporating a cognitive screen and an informant interview assessing function. This comprised instrumental activities of daily living (IADLs), developed to be culturally appropriate for the region. Internal validation of the data found that reducing the number of IADL items from 11 to 3 minimally decreased the Area Under the Receiver Operating Curve (AUROC) from 0.939 to 0.923. The study aims to externally validate this shortened tool, with increased efficiency for use in a resource poor environment.
Methods 329 participants were screened using the shortened IDEA-IADL tool in four villages in the Hai District. This was in conjunction with the local enumerator for each village (responsible for demographic surveillance). A stratified sample was subsequently assessed according to ‘gold standard’ DSM-IV dementia criteria by a doctor, blinded to screening results. AUROC values were calculated to determine the screen performance.
Results AUROC was lower than expected at 0.878. Assessment of the sub-sections of the screen found the IADLs were the primary contributor to this reduced score, varying from 0.687 to 0.939, depending on assessor. On regression modelling, whilst controlling for age, gender and presence of dementia, there was no association between a positive screen and the absence of formal education (Odds Ratio 2.776, p=0.106).
Conclusions The shortened screening tool has been externally validated. Whilst it remains free from educational bias, the research exposes the unreliable nature of more subjective measures of function when carried out by unskilled assessors. Screen performance appears to be assessor dependent and the effect of training and experience in healthcare needs further analysis.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
4
Scientific Research – Epidemiology [PLATFORM PRESENTATION] DETERMINANTS OF POST-DISCHARGE FALLS AND FRACTURES AFTER STROKE OVER LONG TERM FOLLOW UP E J Foster1, R S Barlas1, A B Clark2, J H Bettencourt-Silva1, K M Bowles2,3, A K Metcalf2,3, J F Potter2,3, P K Myint1,2,3
1 University of Aberdeen, 2. University of East Anglia, 3. Norfolk and Norwich University Hospital Background Neurological deficits post-stroke and associated reduced bone mass lead to increased fall and fracture risk, known to be associated with increased mortality. Despite recent advances identifying risk factors for falls post-stroke in survivors, they remain poorly understood. This study aimed to investigate which factors increased the risk of falls and fractures after stroke.
Methods We analysed data from a regional stroke register, between 2003-2015. The data entry team documented paper-based records at baseline. Incident falls and fractures were followed up by record linkage. Univariate and multivariate Cox Proportional Hazard models were constructed - adjusting for patient/stroke characteristics and co-morbidities - analysing over 10-years follow up.
Results 7248 patients discharged after acute stroke (89.6% ischaemic) were included. The mean age (SD) was 76.3±12.1 years; 50.6% women. 1136 (15.7%) had an incident fall; and 666 (9.2%) an incident fracture during the 10-year follow up (median 6.94 years). Increasing age [HR 1.04(95%CI:1.03-1.04)], falls history [1.42(1.14-1.75)], atrial fibrillation [1.18(1.03-1.35)], previous stroke/TIA [1.16(1.01-1.32)] and hyperlipidaemia [1.36(1.01-1.81)] were identified as risk factors for falls post-discharge; while, increasing age [1.03(1.02-1.03)], falls history [1.82(1.39-2.37)] and atrial fibrillation [1.21(1.02-1.43)] were associated with increased risk of fracture post-discharge. Male sex [falls 0.77(0.68-0.87), fractures 0.63(0.53-0.75)], Total Anterior Circulation Stroke [falls 0.58(0.46-0.72), fractures 0.59(0.44-0.79)] and a pre-stroke modified Rankin Score (measure of pre-stroke disability) of 3-5 [falls 0.78(0.65-0.95), fractures 0.69(0.54-0.89)] were associated with reduced risk of falls and fractures. Previous malignancy was also associated with reduced fall risk [0.76(0.62-0.93)].
Conclusion We identified new personal and stroke-related fall and fracture risk factors post-stroke. This knowledge may allow earlier targeted preventative measures to be instituted, preventing future fall and fracture risk among stroke survivors.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
5
Scientific Research – Other Medical Conditions [PLATFORM PRESENTATION] EFFECT OF NON-MEAT, HIGH PROTEIN SUPPLEMENTATION ON QUALITY OF LIFE AND CLINICAL OUTCOMES FOR OLDER PEOPLE LIVING IN CARE HOMES: SYSTEMATIC REVIEW AND META-ANALYSIS A I C Donaldson1,2, T O Smith3, S Alder2, A M Johnstone4, B De Roos4, L S Aucott5, A L Gordon6, P K Myint1,2
1. AGEING Group, University of Aberdeen, 2. NHS Grampian, 3. University of East Anglia, 4. Rowett Institute of Nutrition and Health, University of Aberdeen, 5. Medical Statistics Group, University of Aberdeen, 6. University of Nottingham Background Malnutrition affects one third of older people living in care homes. This is associated with several poor outcomes which may negatively impact quality of life (QOL). There is a particular risk of protein energy malnutrition which may be addressed by high protein oral nutritional supplements. The purpose of this study was to perform a systematic review and meta-analysis of randomised controlled trials (RCTs) performed in care homes, using a non-meat, high protein intervention to assess the effect of supplementation on QOL and clinical outcomes in older people.
Methods We searched EMBASE, AMED, CINAHL, MEDLINE, and the Cochrane Registry of Clinical Trials, OpenGrey, clinicaltrials.gov, the WHO clinical trial registry and the ISRCTN and NIHR trial portfolio (inception to 1st April 2016) for RCTs assessing a non-meat, high-protein dietary intervention; for people aged >65 years; and conducted in residents in care homes. We excluded trials where participants were recruited during acute hospital or rehabilitation unit admissions, or conducted in sheltered housing. Two reviewers independently assessed trials for inclusion, extracted data, and assessed trial quality and risk of bias using Cochrane Risk of Bias tool.
Results Searches identified 375 potentially relevant papers of which 17 papers from 16 trials with 1246 participants fulfilled the inclusion criteria. Meta-analysis of four trials which reported on QOL outcome showed no significant effect of protein supplementation (standardised mean difference (SMD): 0.57; 95% CI: -0.77 to 1.90; p=0.41; 4 trials). Among trials reporting on adverse events there was no significant difference in the number reported (Risk ratio (RR): 1.11; 95% CI: 0.70 to 1.76; 7 trials) and likewise for those reporting on deaths (RR: 0.53; 95% CI: 0.22 to 1.25; 4 trials). Meta-analysis showed significant increase in mean body weight (MD: 3.30; 95% CI 2.05 to 4.55; p<0.00001; 7 trials) and mean body mass index (MD 1.24; 95% CI: 0.79 to 1.70; p <0.00001; 5 trials). There was a strong risk of selection and performance bias due to the lack of blinding in the majority of studies (14 trials; 88%).
Conclusion High-protein oral supplements can improve markers of nutritional status (body weight and BMI) in care home residents. However there is insufficient high-quality evidence to determine the effect of non-meat, high protein interventions for older adults in care homes with regard to QOL.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
6
Clinical Quality A SIMPLE, EFFECTIVE AND CONVENIENT REGIME FOR TREATMENT OF VITAMIN D DEFICIENCY IN OLDER PEOPLE A Abdulla, A Garland, J Davies Dept of Clinical Gerontology, The Princes Royal University Hospital, Kings College Foundation Trust
Introduction Vitamin D (VitD) deficiency increases risk of falls and osteoporotic fractures in older people. Population studies have also shown a correlation with diabetes, cancer, hypertension, myocardial events, infections, and there is now a consensus on the importance of treating VitD deficiency. A variety of treatment strategies have been recommended but no agreement as to which intervention is best suited for older patients. Regardless of severity, recent guidelines recommend weekly loading regimes for 6 to 12 weeks followed by daily maintenance 800-2000 IU. Our null hypothesis was that a short course of intensive VitD replacement would be quicker, more convenient, and equally effective in replenishing depleted stores.
Method We conducted an audit looking at our practice and its effectiveness as an easy, short, effective, and compliant regime of treating VitD deficiency in older patients. On an acute geriatric ward, patients with VitD deficiency/insufficiency were prescribed a 2 week course of ergocalciferol 50,000 IU/day. A daily maintenance dose of calcium/VitD (1.5gm/400IU) was also started. Levels were checked within 4 week of completion. Demographics including age, gender, renal function, pre and post vitD levels were recorded. Patients in CKD stage 4 were excluded.
Results 54 patients were included. 12 were lost to follow up. Mean age was 82 years. 72% were female. The median level of VitD was 30.7 nmol/L (range 8-67) [normal >80]. Renal function, determined by eGFR, was abnormal in 78% (16 CKD stage II, 17 in stage III). Following 14 days treatment, all patients demonstrated significant improvement in VitD levels. The median change was 265%. No side effects were noted and none reached overdose levels (≥ 380 nmol/L).
Discussion Our results show that this regimen of VitD replacement is effective in replenishing stores in older people. Compared to recommended strategies which span over 6-12 weeks, this protocol ensures rapid replacement, is effective and safe with no side-effects. The short duration should also increase compliance, as intermittent dosing is less easily adhered to by patients and staff, and therefore less effective.
Although a small study, the results also suggest that for patients with VitD levels below 20 nmol/L, a 2 week course is probably not sufficient and may be worth considering 3 weeks of treatment at the same dose.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
7
Clinical Quality IMPROVING THE RECORDING OF COMPREHENSIVE GERIATRIC ASSESSMENT AND SAFETY FACTORS BY USE OF A CHECKLIST A Kilsby, S Brooke, C Patchett, A Marsh, C Page, J George Department of Elderly Care, Cumberland Infirmary, North Cumbria University Hospitals, Carlisle
Introduction Comprehensive geriatric assessment (CGA) has been shown to improve quality of life, reduce institutionalisation and reduce mortality in frail older people1. However a recent national benchmarking audit found that only 46% of medical assessment units and 87% of specialised geriatric wards routinely used CGA2.
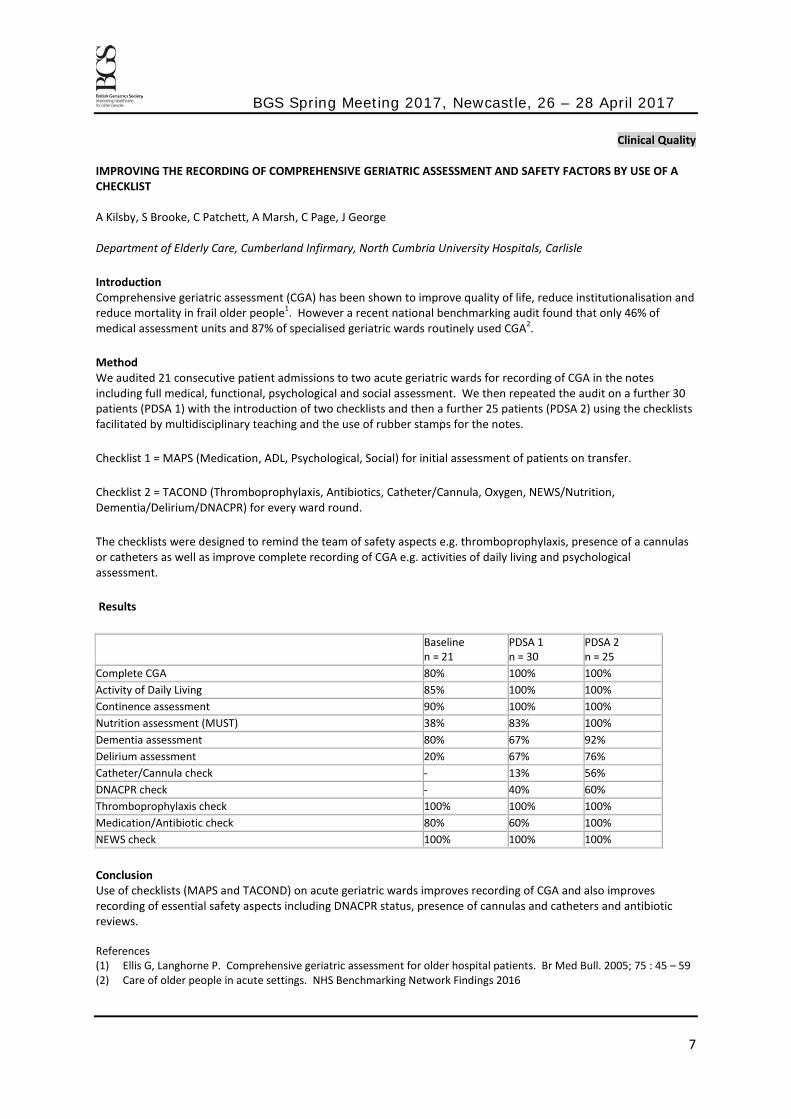
Method We audited 21 consecutive patient admissions to two acute geriatric wards for recording of CGA in the notes including full medical, functional, psychological and social assessment. We then repeated the audit on a further 30 patients (PDSA 1) with the introduction of two checklists and then a further 25 patients (PDSA 2) using the checklists facilitated by multidisciplinary teaching and the use of rubber stamps for the notes.
Checklist 1 = MAPS (Medication, ADL, Psychological, Social) for initial assessment of patients on transfer.
Checklist 2 = TACOND (Thromboprophylaxis, Antibiotics, Catheter/Cannula, Oxygen, NEWS/Nutrition, Dementia/Delirium/DNACPR) for every ward round.
The checklists were designed to remind the team of safety aspects e.g. thromboprophylaxis, presence of a cannulas or catheters as well as improve complete recording of CGA e.g. activities of daily living and psychological assessment.
Results
Baseline n = 21
PDSA 1 n = 30
PDSA 2 n = 25
Complete CGA 80% 100% 100% Activity of Daily Living 85% 100% 100% Continence assessment 90% 100% 100% Nutrition assessment (MUST) 38% 83% 100% Dementia assessment 80% 67% 92% Delirium assessment 20% 67% 76% Catheter/Cannula check - 13% 56% DNACPR check - 40% 60% Thromboprophylaxis check 100% 100% 100% Medication/Antibiotic check 80% 60% 100% NEWS check 100% 100% 100%
Conclusion Use of checklists (MAPS and TACOND) on acute geriatric wards improves recording of CGA and also improves recording of essential safety aspects including DNACPR status, presence of cannulas and catheters and antibiotic reviews. References (1) Ellis G, Langhorne P. Comprehensive geriatric assessment for older hospital patients. Br Med Bull. 2005; 75 : 45 – 59 (2) Care of older people in acute settings. NHS Benchmarking Network Findings 2016
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
8
Clinical Quality PREVENTING FRACTURES: CAN DOCTORS IMPROVE THEIR BONE PROTECTION PRESCRIBING? F Ahmad1, R Bisheswar1, A Andrews2 1. Royal London Hospital; 2. A Andrews
Evidence-base Correct prescribing of bone protection in the elderly is important to minimise the risk of osteoporosis, thus to prevent fragility fractures. 50% of patients with hip fractures who were previously independent become dependent on others. This results in social, financial and psychological implications on the patient and prolonged hospital stays.
Therefore, we aim to check whether the correct bone protection was prescribed, according to NICE, to patients on the geriatrics and acute wards, over the age of 65 years, in a month’s period. This was then re-audited after our strategy was put in place.
Change Strategies Before re-audit, posters were put on the acute and geriatrics wards on guidance on how and when to prescribe bone protection and were explained. Also, recommendations were verbally delivered to doctors and drug charts were checked.
Change Effects Over the course of a month, in cycle 1, 15 patients met the criteria of having bone protection. 7/15 (46.7%) were correctly prescribed bone protection. The most common reason why patients met the criteria for bone protection was ‘all patients over 65 years with a history of fall and are housebound’.
After our intervention, 23 out of 33 (70%) were prescribed the correct bone protection. ‘Patients over the age of 65 and are housebound’ was the main reason for bone protection being prescribed. This was also the commonest category doctors had missed bone protection prescribing for, that being 7 patients.
The acute wards showed an improvement in correct bone protection prescribing from 25% to 50%. The geriatrics wards improved from 55% to 76%.
Conclusion Even though, there was an improvement in correct bone protection prescribing, further improvement can be made, more so, on the acute wards. It has been identified that mainly housebound patients missed out on bone protection. Post re-audit, further education of correct bone protection prescribing was delivered in the doctors meeting to inform them in which categories they fell short.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
9
Clinical Quality DOES A WEEKLY COMMUNITY GERIATRIC CLINIC IN PEACEHAVEN REDUCE HOSPITAL ATTENDANCES? N Francis1, T Rose1, A Parrott2, P Birtles2, J Archer1, H Alexander1 1. Brighton and Sussex University Hospitals Trust, 2. High Weald Lewes Havens Clinical Commissioning Group (HWLH CCG)
Introduction Life expectancy in Peacehaven is over nine years less than in other parts of the Lewes district. Peacehaven has some of the highest A and E attendance rates for those aged over 65 in the county. (East Sussex JSNA March 2016). We were tasked by HWLH CCG to implement a service to try and address these inequalities.
Intervention We set up a weekly community Geriatric clinic at the Meridian Surgery in Peacehaven in September 2014 with a dedicated email inbox to facilitate referrals from GPs. 259 referrals were seen by October 2016. 161 (62%) were female with a mean age of 78.9 years. 141 (54%) were seen in the clinic and 118 (46%) were seen at home.
Improvement After 12 months a random sample of 19 cases was examined by the CCG Urgent Care Clinical Lead. The average time between referral and assessment was 17 days. In 10 cases the Geriatrician was deemed to have added value to the patient’s management. By 1st May 2016 168 patients had been seen. There were 82 A and E attendances from this group in the six months prior to their community assessment and 61 attendances in the six months thereafter. This is a 26 % reduction. The data suggests that the reduction in non-elective admissions is closer to 34%.
Discussion Changing a clinic from hospital to community based was relatively straightforward. We were fortunate in that space within a modern practice became available. Referral numbers have been maintained over the last six months and may now increase, necessitating an expansion of the service. We plan to look at the admission data in more detail to identify any reduction in length of stay and to see whether the service provides a cost benefit to the health economy.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
10
Clinical Quality A FULL AUDIT CYCLE: QUALITY OF MEDICATION INFORMATION IN IMMEDIATE DISCHARGE LETTERS K Cumming, H S Tay Department of medicine for the elderly, Aberdeen Royal Infirmary, Aberdeen, Scotland
Topic Immediate discharge letters (IDLs) relay key information between secondary and primary care. Polypharmacy review and de-prescribing are key aspects of comprehensive geriatric assessment, therefore accurate medication information in IDLs is essential. The quality of IDL medication information for patients discharged from the Geriatric Assessment Unit (GAU), Aberdeen royal infirmary (ARI) was audited.
IDLs for 100 patients were screened and the following data collected; documented medication changes, reasons for medication initiation, termination or dose changes recorded, and clinical indication for discharge medication provided.
Intervention Loop 1 results (Table 1) identified that the quality of medication information in IDLs was suboptimal. Loop 1 results, recommendations for improvement and sample “ideal IDLs” were presented at the geriatric department weekly education meeting, and disseminated in writing. Reminder/education posters for documentation of medication in IDLs were also placed at work stations.
Improvement These simple strategies showed improvement in the standard of documented medication information in IDLs (see loop 2 results, Table 1).
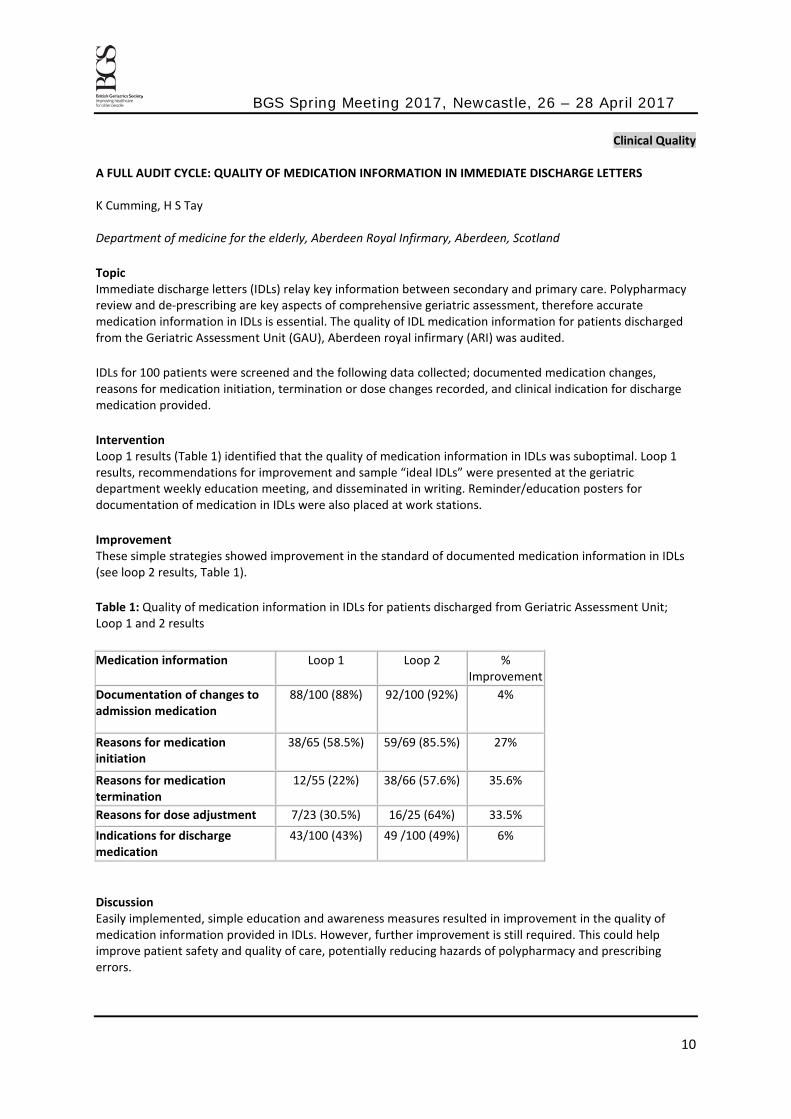
Table 1: Quality of medication information in IDLs for patients discharged from Geriatric Assessment Unit; Loop 1 and 2 results
Discussion Easily implemented, simple education and awareness measures resulted in improvement in the quality of medication information provided in IDLs. However, further improvement is still required. This could help improve patient safety and quality of care, potentially reducing hazards of polypharmacy and prescribing errors.
Medication information Loop 1 Loop 2 % Improvement
Documentation of changes to admission medication
88/100 (88%) 92/100 (92%) 4%
Reasons for medication initiation
38/65 (58.5%) 59/69 (85.5%) 27%
Reasons for medication termination
12/55 (22%) 38/66 (57.6%) 35.6%
Reasons for dose adjustment 7/23 (30.5%) 16/25 (64%) 33.5% Indications for discharge medication
43/100 (43%) 49 /100 (49%) 6%
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
11
Clinical Quality DO ELECTRONIC DISCHARGE DOCUMENTS ACCURATELY REFLECT THE INPATIENT STAY? M Hagan1, P Mathew2 1. Nottingham City Hospital, 2. Department of Complex Needs, Lincoln County Hospital
Background It was identified that the Department of Complex Needs (DOCN) was receiving 2-3 calls a week from primary care asking for clarification regarding the content of electronic discharge documents (EDDs). The purpose of this quality improvement project (QIP) was to improve EDD writing to enhance patient care post-discharge.
Innovation The notes of all patients discharged in one week from the three elderly care wards were cross referenced with the EDD. The results were presented at the DOCN weekly meeting. There were 2 interventions.
1. “How to write an EDD” presentation covering the importance of the EDD (transfer of information, useful reference when patients are readmitted but notes unavailable), highlighting the current standard of EDD writing, and pointers for improvement.
2. An aide memoire attached to the screens of all ward computers used for EDD writing plus the presentation.
A further notes and EDD review was undertaken post implementation of each intervention.
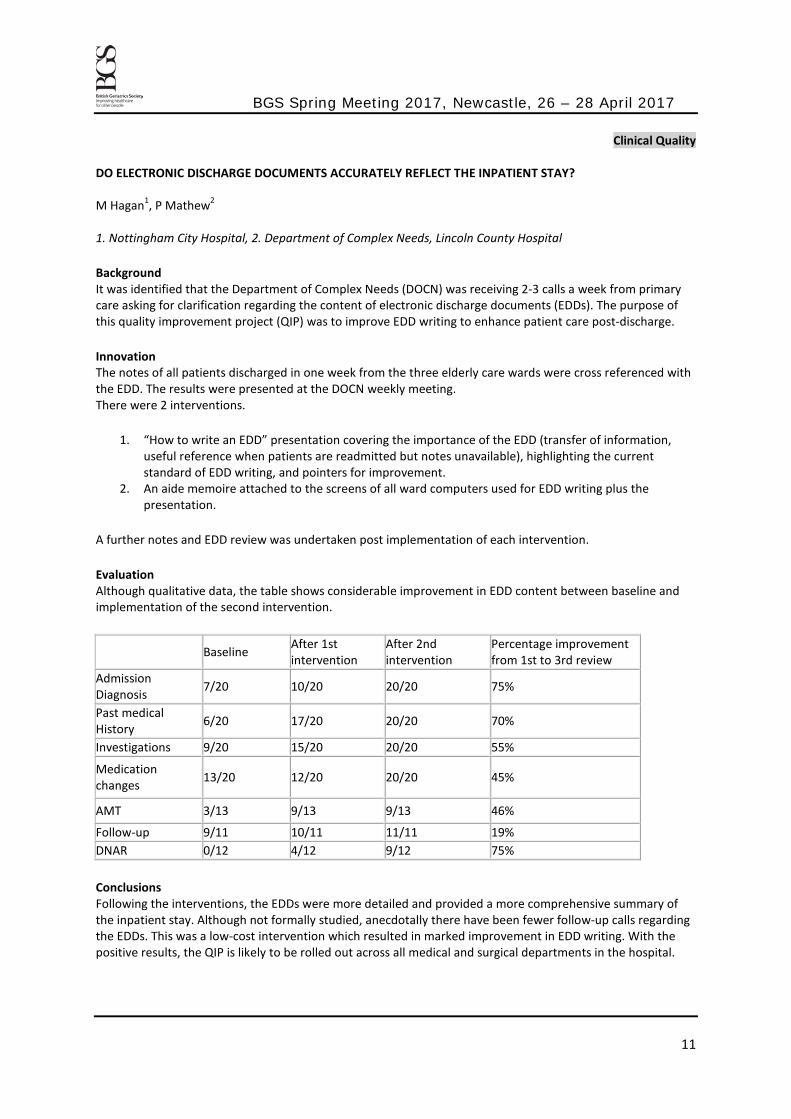
Evaluation Although qualitative data, the table shows considerable improvement in EDD content between baseline and implementation of the second intervention.
Baseline After 1st intervention
After 2nd intervention
Percentage improvement from 1st to 3rd review
Admission Diagnosis 7/20 10/20 20/20 75%
Past medical History 6/20 17/20 20/20 70%
Investigations 9/20 15/20 20/20 55%
Medication changes 13/20 12/20 20/20 45%
AMT 3/13 9/13 9/13 46%
Follow-up 9/11 10/11 11/11 19% DNAR 0/12 4/12 9/12 75%
Conclusions Following the interventions, the EDDs were more detailed and provided a more comprehensive summary of the inpatient stay. Although not formally studied, anecdotally there have been fewer follow-up calls regarding the EDDs. This was a low-cost intervention which resulted in marked improvement in EDD writing. With the positive results, the QIP is likely to be rolled out across all medical and surgical departments in the hospital.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
12
Clinical Quality IMPROVING THE RECOGNITION AND REFERRAL OF OLDER PATIENTS WITH COGNITIVE IMPAIRMENT PRESENTING TO THE EMERGENCY ASSESSMENT UNIT OF A DISTRICT GENERAL HOSPITAL R Arnott1, R Copeland1, E Moriarty1, A L Gordon2, S Rutter1
1. Dept of Elderly Care, Kings Mill Hospital, Nottinghamshire, 2. Division of Medical Sciences and Graduate Entry Medicine, University of Nottingham
Topic NICE guidelines recommend screening patients over 65 years admitted to hospital for delirium. A Care Quality Commission report in July 2015 found our hospital did not do this. Therefore the Emergency Department implemented 4-point Abbreviated Mental Testing (AMT4) but with no onward pathway for those flagged as cognitively impaired. (AMT4<4.)
Intervention A plan-do-study-act (PDSA) approach was adopted to coordinate cognitive screening between departments.
PDSA cycle 1: According to the new pathway, only patients scoring AMT4<4 required AMT10. Those with AMT10<8 required CAM assessment and onward liaison psychiatry referral. We aimed for: 90% of patients over 75 to have AMT4 within 24 hours of admission with liaison psychiatry referral in all cognitively impaired patients.
PDSA cycle 2: Introduction of a new proforma combining AMT4, AMT10 and CAM to improve compliance.
Improvement PDSA cycle 1: 143 sets of notes audited over 1 month for compliance with the pathway. Results were poor: AMT4 completion was below target (88% at 24h) with 34 (27%) patients receiving unnecessary AMT10 assessment. Only 4 patients had CAM assessment and only half with new cognitive impairment were referred to Liaison Psychiatry.
PDSA cycle 2: 39 sets of notes audited over 3 weeks. AMT 4 completion rates were above target (97% at 24h) and compliance with the pathway improved, however only 4 patients had CAM completed and only 3/5 patients with new cognitive impairment were referred to Liaison Psychiatry.
A survey of 17 doctors found that 58% did not regularly complete AMT10 and 47% were unfamiliar with the CAM assessment.
Conclusion The pathway and guidelines regarding liaison psychiatry referral improved AMT4 completion, but ongoing assessment remained suboptimal. Attention to competencies in completing assessment scales and promoting understanding of the rationale for cognitive assessment and liaison psychiatry referral will be the focus of future improvements.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
13
Clinical Quality THE APPROPRIATE USE OF CONSENT FORMS PRE-OPERATIVELY FOR ORTHOGERIATRIC PATIENTS Z Tippu, T Irani, A Fox, E Aitken Care of the Elderly Department, University Hospital Lewisham Background Capacity to consent to treatment and intervention is deemed to be decision and time specific. Patients undergoing significant trauma and physiological insult, such as neck of femur (NOF) fractures, are known to have higher rates of delirium, which may affect capacity. Our aim was to determine appropriate use of consent forms in ortho-geriatric patients presenting with neck of femur fractures.
Methods/ Intervention A closed loop retrospective analysis was undertaken in patients presenting with neck of femur fractures, between April 2015- February 2016, with a subsequent re-analysis between May 2016- June 2016. Information extracted from the NOF proformas included Abbreviated Mental Test Score (AMTs) pre- & post-operatively, a background history of cognitive impairment, and the presence of confusion. Intervention between cycles included better availability and awareness of junior surgical staff to varying consent forms and the accompanying mental capacity assessment form, alongside modifications to the proformas, prompting formal capacity assessment.
Results A total of 62 patients were included within the study (Cycle 1: 35; Cycle 2: 27), age= 82 years (±8.2); female (%)= 72.6; average length of stay= 18.7 days (±13.8). 17 patients (Cycle 1: 10; Cycle 2: 7) were deemed to not have capacity by having a consent form 4 complete. Across cycles 91% of patients had AMTs completed pre-operatively, with 61% complete post-operatively. AMTs scores pre-operatively were greater in those patients with consent form 1 as opposed to those with consent from 4 (consent form 1: 9.3 (±1.2) vs. consent form 4: 3.9 (±3.2)). 88.2% of patients were seen pre-operatively by an ortho-geriatrician, compared to 70.4% of patients in cycle 2.
25% of patients in cycle 1 had a completed accompanying mental capacity assessment form, increasing to 60% in cycle 2. On retrospective analysis by an ortho-geriatric SpR, three patients assessed to not have capacity at time of admission had an inappropriate consent form filled.
Conclusion Interventions have resulted in a greater awareness and utilisation of the mental capacity assessment form, allowing surgical juniors a clear guidance as to the four components of capacity assessment. Earlier intervention by ortho-geriatricians pre-operatively may aid in cases of complex capacity assessment.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
14
Clinical Quality DELAYED TRANSFERS OF CARE: AIMING TO UNBLOCK THE BED CRISIS E Vardon1, A Giwa1, D Baylis2 Medicine for Older People, University Hospital Southampton (UHS)
Background Delayed transfers of care (DToC) rose 30% to 188,300 delayed days in the year ending August 2016 costing £900 million. DToC causes harm via morbidity, mortality, readmissions and functional deconditioning; reduced patient flow and cancelled elective procedures. The Social Care Act (2014) provides a framework to help address this challenge. University Hospitals Southampton (UHS) is large acute NHS trust; this service improvement work evaluated the effect on DToC of a large trust-wide intervention centred on moving to a social care act compliant system.
Innovations: Clear discharge pathways were defined and a bespoke IT system developed. A large team of ward based discharge officers were recruited. The patient choice policy was reinvigorated and ‘Continuing Health Care (CHC) in 5 days’ processes were introduced. A Trust wide education program supported this and the recruitment of a discharge leader accountable to all partnership organizations. Data was collected for 50 and 41 patients pre- and post-interventions.
Evaluation: Interventions reduced bed days lost attributable to hospital processes from 259 to 164 and mean days to discharge for fast track patients from 20 to 11. Complaints reduced from 10% to 2%, however adverse events rose from 30% to 46%. Delays attributable to the wider system increased but the mean number of bed days lost remained stable at 14, in comparison to a national increase.
Conclusions: UHS has successfully made internal systems and processes more streamlined resulting in a reduction in internal delays and fewer complaints; adverse events rose. Last year the trust performed favourably when compared to regional and national pictures. The ‘bottle neck’ seen in delays has been shifted towards the wider system and challenges with the provision of community care; greater capacity and innovative discharge to assess pathways are being developed in conjunction with the local STP which will form a third phase of data collection shortly.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
15
Clinical Quality CORTRAK EAS AT ROYAL DEVON AND EXETER (RD&E) W F Lim, N Chivers, A Connolly, W D Strain Royal Devon and Exeter NHS Foundation Trust, University of Exeter Medical School
Background After stroke complicated by impaired swallow reflex, nasogastric tubes (NGT) are used to maintain nutrition. Placement of NGT requires a position check using a chest X-ray (CXR) when no aspirate can be drawn. This results in recurrent exposure to ionising radiation, and delays using the NGT awaiting confirmation of placement.
CORTRAK is a NGT with a transmitter on the tip allowing position check using a handheld receiver. This system comes with a capital outlay of £12,000 and a cost per unit of £51 vs. £7 per standard NGT. We audited whether this device reduced exposure to CXR or delays utilising the NGT.
Method We evaluated the use of the CORTRAK device on 16 consecutive patients on the acute stroke unit compared to 26 patients receiving conventional NGT. Appropriate training was provided. All patients were treated on the acute stroke unit and were clinically determined to require a NGT. Number of insertions and CXRs required were recorded. Proportion of patients on proton pump inhibitor (PPI) was documented. Nursing opinions were sought by means of a free text questionnaire.
Results Patients who had the CORTRAK device had the same frequency of re-siting. Use of CXR was similar using CORTRAK device compared with conventional NGT. Delays to initiating use of NGT were similar with the two devices.
Table 1, primary results of audit Standard CORTRAK N 26 16 Patients on PPI 10 (38%) 6(38%) Median CXR per patient (Range) 2 (0-8) 2(0-7) Mean CXR per patient 3.3 2.9 Median NGT Insertion 4 4
Nurses reported that, although the confidence in siting the CORTRAK NGT was greater, the need for two nurses to implement the device delayed insertion. Further, the loss of contact with the patients by watching the screen was a concern to nurses.
Conclusion In our audit, CORTRAK did not reduce number of CXR and increased time to insertion because of the need for two staff members. Therefore, it was determined to be not cost-effective we have reverted to conventional NGT.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
16
Clinical Quality FRAILTY SCREENING- A USEFUL TOOL IN THE DEVELOPMENT OF A SPECIALIST FRAILTY SERVICE AND MODELLING FLOW OF FRAIL PATIENTS WITH AN NHS TOUNDATION TRUST A Boardman, M Taylor Blackpool Teaching Hospitals NHS Foundation Trust
Introduction Frailty is increasingly being recognised as playing an important role in patient flow. Within our trust, the effect of frailty on patient flow has thus far been poorly understood, with no real understanding as to the numbers of patients within our service who are classified as being frail. In order to gain a greater understanding of the burden of frailty within our patient population, a system was developed whereby patients are screened at the point of referral from GP or A&E using the Leicester Frailty Tool. This forms a mandatory component of patient admissions under medical and surgical teams. We have reviewed data collected following the implementation of screening in order to model the flow of frail patients and predict the numbers eligible for admission into specialty frailty services currently being developed within the trust.
Methods A review of data collected between 27/06/16 and 30/08/2016 from the trust digital referrals system ‘CAT unit tracker’ was carried out. Data was collected on patient date and time of admission, presenting complaint and frailty score. Frailty was defined using two tools; the Leicester Frailty Tool and the BGS Silver Book recommendations. Presentation data was reviewed to determine eligibility for frailty unit admission. Data was analysed using statistical process charts.
Results 3756 patients were admitted via the CAT wards between 27/06/16 and 30/08/16. Of these, 1058 (28%) were identified as being frail. 291 (8%) were retrospectively identified as having frailty not initially identified at screening.
724 patients were identified as being eligible for Frailty unit care. A mean of 14.1 patients per day were deemed eligible for specialty frailty services (Upper control limit = 51.5, Lower control limit = -23.2).
Conclusion We project that 14 patients per day admitted to our trust would be eligible for admission under Care of the Older Person and specialist frailty services. Currently within our trust, three wards are dedicated Care of the Older Person wards, meaning a number of patients admitted do not have access to specialist care. Understanding the numbers of patients involved has helped develop a greater understanding of the local population, thus allowing development of an effective clinical service. The review of real world data taken from a representative local population is an important component in service development and improvement.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
17
Clinical Quality EXPERIENCE OF SETTING UP A HOSPITAL CARERS CAFé IN SALISBURY DISTRICT HOSPITAL J Drayson, Y Kaur, L Williams, S Woodbridge, C Carroll Salisbury District Hospital, Odstock Road, Salisbury, Wiltshire
Introduction There is an aging population in the UK with more complex long term conditions. Increasing numbers of people have to care for friends and family members, often with little or no support. The number of carers is likely to increase in the future, and they face increasing challenges.
We set up a carers’ cafe at Salisbury District Hospital, (a medium sized DGH) to bridge the gap between carers, voluntary organisations and charities to improve help and support for carers for anyone over the age of 18. Preliminary research showed there was limited support available in the local community. We also hoped that carers would establish a network of friends and contacts to draw upon.
Methods We secured funding from the local League of Friends, and recruited volunteers from the local Alzheimer's Society, Age UK and Carers in Wiltshire. We promoted it on local media, with posters around the hospital and secured a site in the hospital canteen. After 4 months of consultation we launched in July 2015. It initially ran every fortnight, but due to popular demand it was changed to weekly. All carers who attended were asked to fill out a short survey.
Results 60 people completed surveys between July 2015 and July 2016. Demographics showed a elderly female preponderance for carers and a male preponderance for those being cared for. Most were not aware of other cafes or had been to a carers’ cafe before, and most had not had any formal care assessment. There was an overwhelmingly positive response to the Cafe with almost everyone recommending it to others.
Discussion Setting up the carers’ cafe was an excellent way to reach out to carers who may otherwise have not been aware of the services offered by the voluntary sector. It serves as a focal point in the hospital and is now part of the fabric of hospital life. It was relatively easy to set up and this model could easily be replicated in other hospitals. One interesting piece of feedback was that people did not like the use of the word 'carer' as it was felt to have negative connotations - this could be an interesting discussion for the future.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
18
Clinical Quality FOCUSED MULTIDISCIPLINARY TEAM (MDT) BASED BOARD ROUNDS CAN SIGNIFICANTLY REDUCE LENGTH OF STAY (LOS) AND INCREASE WARD PRODUCTIVITY K Ward, H Farooq, M Taylor Blackpool Victoria Hospitals
Introduction Ward 26, Blackpool Victoria Hospital, is a female Care of the Older Person (CoOP) ward. Data collected on current length of stay suggested that there was a problem with performance on the ward. To address the perceived problem it was agreed that the ward team would look at how they could improve the internal processes and improve care for the patients.
Four teams of consultants had patients on the ward (as well as patients on a second ward), leading to multiple, overlapping ward rounds. There was a brief board round each day involving the nurses, therapists and discharge team. The board round function was primarily to agree when referrals should be done, rather than goal setting.
Methods It was decided that from the beginning of March 2016 each ward in CoOP would have 2 consultant teams who only worked on each ward. This would mean fewer ward rounds would take place. It was also decided that the board round would be developed into a more dynamic process, with challenge mechanisms built in, attendance by the medical teams and goals set and recorded in the notes. The day to day LOS was displayed on the ward and number of discharges. Data were collected on LOS, patients admitted to the ward each week, readmission rates and mortality. LOS data and ward admissions were analysed using Statistical Process Control Charts and mean presented with Upper Control Limit (UCL) and Lower Control Limit (LCL). Mortality and Readmission rates were analysed using Fishers Exact test.
Results Pre intervention the Mean LOS on the test ward over 6 months was 12.9 days (UCL 26.7, LCL -0.9). Post intervention (over six months) the mean LOS was 8.75 days (UCL 20.1, LCL -2.6). Ward admissions climbed from a mean of 17.1 days (UCL 320, LCL 2.3) to 19.8 days (UCL 32.1, LCL 7.4). Mortality rates fell from 11% pre change, to 9.5% following change (non-significant). Readmission rates were also non-significant, at 16.2% pre change and 17.8% post change.
Conclusion Focused, goal setting MDT board rounds can have a positive impact on LOS. This appears to have no negative impact on mortality or readmission rates.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
19
Clinical Quality MASSIVE OPEN ONLINE COURSES (MOOCS): EDUCATING AND EMPOWERING OLDER ADULTS ABOUT FALLS L Robinson, C Elliott, J L Newton, L Rawles, J Frith Faculty of Medical Sciences Graduate School, Newcastle University, UK, Institute of Cellular Medicine, Newcastle University, UK, Newcastle upon Tyne Hospitals NHS Foundation Trust, UK
Background Massive open online courses (MOOCs) are an educational tool available to anyone with access to the Internet. They have the potential to educate the public on a large scale. Falls are highly prevalent and associated with significant morbidity and mortality. NICE guidelines recommend educating those at risk of falling.
Aim To explore whether the Ageing Well: Falls MOOC influenced learners’ awareness of falls prevention and their intention to undertake strategies to reduce falls risk.
Methods A four-week, open-access, online course to educate and empower people about falls opened in September 2014. On completion, learners discussed online what actions they intended to take to prevent falls in the future. Using the Theory of Planned Behaviour as a theoretical model, we performed a secondary qualitative analysis of learners’ comments and intentions.
Results Of 3434 learners, 58% completed the course. One third were aged 56-65 and one third were aged over 65 years. Most enrolled from a desire to maintain their health, or because they had witnessed devastating effects of falls in others. Participants engaged with the course because of its practical focus on health promotion, rather than illness avoidance. Most felt more aware of their risk and felt better equipped to manage falls. There was a sense of increased confidence, particularly in seeking support from health professionals and in taking action to reduce their own risk of falling.
Conclusions These findings suggest that this novel, large-scale educational intervention has the potential to empower people to make decisions, influence their intentions and take action to reduce their falls risk. This MOOC also challenges the misconception that older adults do not use the Internet and demonstrate a high level of motivation to engage with health promotion messages regarding healthy ageing.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
20
Clinical Quality IMPLEMENTING RED TO GREEN METHODOLOGY ON A CARE OF THE OLDER PERSON (CoOP) WARD N Burgoyne1, M Taylor2 1. University of Central Lancashire, 2. Blackpool Teaching Hospital Introduction The Emergency Care Intensive Support Team (ECIST) and NHS Improvement have recommended the use of Red and Green Days to help improve patient care and patient flow. The principle is that any day where planned tasks are carried out are classed as green days, and those days where important events for the patient journey have not been carried out are “Red Days”. The ESIST recommendations do not specify exactly what constitutes a “Red Day” but instead gives guidance as how to interpret it locally.
The change As part of a project to improve the care on a CoOP ward it was decided to implement Red and Green Days within a Multidisciplinary Board (MDT) Round with clear goal setting. It was agreed that the MDT would agree “Mission Critical Events” and record these in the patient notes. The team used a PDSA (Plan Do Study Act) approach to fine tune how methodology would work on the ward. The team monitored the impact on the method on the team. The authors collected data on the reasons for Red Days over a two week period (weekends excluded).
Results Initially there was a dip in team morale. Some team members felt the recording of the cause of a “Red Day” was a personal attack. By giving continual feedback as to what was trying to be achieved and efforts to develop a more open ward culture staff soon accepted the challenge.
Over two weeks there were 89 red days in 250 bed days (35.6%). 47 (53%) of these were “internal waits” (e.g. investigations - 16, communications with families or patients - 15, internal transfers – 12) and 42 “external waits” (e.g. social worker – 15, Package of Care – 12, Availability of Care Home – 8)
Conclusion When implementing Red and Green days it is important to be aware that some staff may find the continual challenge difficult and take “Red Days” personally.
A finding that is counterintuitive to most clinicians is that the majority of waits are not due to social services and we have control of at least half of the delays on our wards
Locally we have developed a “Red-Green app” that captures the causes of “Red Days” to identify and manage common themes.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
21
Clinical Quality THE PICTURE OF FRAILTY AT MID YORKSHIRE Z S Sawicka1, F Phelan2, K Richards3, R Baxter4, H Bennett5 1. Elderly Care Department, Mid Yorkshire NHS Trust, 2. Elderly Care Department, Hull Royal Infirmary 1,2,4 and 5. Elderly Care Department, Mid Yorkshire Hospitals NHS Trust, Wakefield, 3 Elderly Care Department, Hull Royal Infirmary, Hull Introduction Defining clinical frailty is now recognised as essential at the hospital front door in order to triage patients effectively. If the correct frailty score is used it should be possible to identify those patients who will gain most benefit from comprehensive geriatric assessment led by geriatricians. Method Having used the Rockwood Clinical Frailty Score over the last few years within our elderly medicine department, it became clear that a large percentage of the patients identified as frail by the score were still not receiving appropriate inpatient care led by geriatricians. This led to our development of a new Frailty Scoring Tool based on a similar tool being using at Hull Royal Infirmary, based on the frailty tool developed by Healthcare Improvement Scotland. Applying this to our current patient cohort has allowed us to identify numbers of patients with moderate and severe frailty who would benefit from geriatrician led assessment, and map numbers of beds required on our planned Older Persons Assessment Unit as part of the Future Hospitals Programme of the Royal College of Physicians.
Results The burden of frailty was assessed over a week in March 2016. During this period 851 individuals over the age of 65 were seen in the Emergency Department. Of those presenting with frailty markers admitted to Medicine, 41.9% presented with confusion or had known dementia. 23% were from care homes either residential or nursing homes. 18% had carers more than three times a day. Of those with frailty admitted to medicine, 19.8% presented with fragility fractures and 32.3% presented with falls.
Using our new Frailty Scoring Tool we analysed the burden of frailty over a week in August. Similar results were seen as with the initial March analysis. We also examined the conversion rate for emergency attendance to admission stratified by frailty severity. Calculation of average admission rates for those with moderate and severe frailty was also undertaken. These figures have allowed re-evaluation of the bed numbers required at Acute Hospital Reconfiguration planned in May 2017.
Discussion It is clear a pathway is needed to help staff identify those who are most appropriate for a frailty service. Minimal access to eFi in the acute setting means that a screening tool is needed to ensure patient safety.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
22
Clinical Quality “WALK THIS WAY” - HOW WELL CAN A MULTIDISCIPLINARY TEAM RECOGNISE VARIOUS WALKING AIDS? C J Miller, D L Lakhani University Hospitals of Leicester, Leicester Royal Infirmary
Introduction The prescription by Physiotherapists of walking aids is an established, evidence-based strategy in the management of falls and safer mobility in frail older people. An appropriate, patient-tailored aid can promote independence whilst incorrect selection or utility is associated with increased risk of falls and injury. It is important, particularly at times of crisis, de-compensation and hospital admission that patients use the correct aid during recovery and rehabilitation. This depends on all members of the multidisciplinary healthcare professional team (MDT) having a basic knowledge of various types of walking aids enabling the correct recommendations to be made for each patient.
Method Members of the UHL Geriatrics Department MDT were asked to identify nine graphically depicted, commonly used walking aids (walking stick, Fischer stick, Tripod stick, Quadrapod stick, Zimmer frame, wheeled Zimmer frame, three wheeled walker, four wheeled (seated) walker, gutter frame). A response was considered correct if any commonly used term was stated for each picture.
Results 158 responses were collected over 2 months. Walking aids were poorly recognised amongst the MDT (average 55%). Commonly used aids (Zimmer frame, walking stick) were better recognised that those less frequently used.
Large variances were noted dependent upon job role and seniority. Therapists reliably recognised all walking aids. Recognition improved with seniority within medically trained staff, and was better amongst healthcare assistants when compared to their qualified nursing colleagues.
Conclusion(s) Walking aids are prescribed interventions made by trained healthcare professionals. This provision should be accurate for all patients in all settings. In the same way that one would not prescribe ‘universal’ spectacles if the patient’s own were not available nor routinely switch between classes of anti-hypertensives if a particular drug is unavailable, we should ensure that patients are provided the correct walking aid to maximise recovery potential and decrease risk of inpatient falls. Sufficient knowledge of the patient’s tailored requirements at point of admission would mitigate against erroneous mobility recommendations during discharge planning.
We have highlighted a knowledge deficit in junior medical and nursing staff within our institution that could potentially result in adverse outcomes downstream. We recommend further evaluation of the provision of walking aids for inpatients including the rationale for the choice of prescription (anecdotally disproportionate increased use of wheeled zimmer frames in our inpatients) and the potentially consequential outcomes.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
23
Clinical Quality ‘DAYS SINCE’ SIGNS AND THEIR IMPACT ON VISITING FRIENDS AND RELATIVES D Wardle, S Peters, R Kersh Doncaster Royal Infirmary
Introduction Pressure ulcers, falls and cases of C. difficile in our in-patient population carry significant morbidity and mortality. Whilst sometimes unavoidable, we must take steps to ensure no avoidable cases occur through human factors. This requires a motivated multidisciplinary team working together to promote a culture of patient safety.
At Doncaster Royal Infirmary, we display posters on the doors of our Care of the Elderly wards showing how many days since a case of C. difficile, a fall or new pressure ulcer occurred. Sharing this information promotes transparency and a sense of pride amongst staff, with every additional day a reward for the sometimes onerous daily tasks that keep patients safe. Recently a case of C. difficile on one ward returned the count from 1300 days to zero. This resulted in an almost grief-like response amongst staff, exemplifying the pride these signs generate. Whilst their impact on ward teams is undoubted, we have never considered the impact on visiting friends and relatives who also see the signs on a daily basis.
Methods and Results We surveyed 28 friends and relatives and asked whether they read the signs, understood them and how they made them feel. Of the 28 people surveyed, 58% (n=16) actually read the signs. Only 32% (n=9) and 64% (n=18) of people felt they fully understood what C. difficile and a pressure ulcer is respectively. People were fairly ambivalent in terms of how the signs made them feel, with an average anxiety rating 5.7/10 (10 = very anxious) and an average reassurance rating of 4.5/10 (1 = very reassuring). Interestingly 100% (n=28) of people felt that displaying these signs was a ‘good thing’ overall.
Discussion This survey shows that people appreciate the transparency of the signs, albeit without fully understanding what they mean. This may explain why people were ambivalent in terms of how the signs made them feel. We will change the wording of the signs in the coming weeks to aid understanding and re-survey to assess the impact. Transparency of information is undoubtedly a powerful motivator for clinical teams, but we must not forget the potential impact this has on the most important people in hospitals – patients and their visiting relatives.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
24
Clinical Quality WHAT IS NEEDED TO IMPLEMENT AND EVALUATE FALLS PREVENTION MOST EFFECTIVELY? J Fleming1, J Eastment2, H Johnston2, H Tunster2, J Riglin3, M Hill3, H Jalal3, F Scheibl1, A Mavrodaris2 1. Cambridge Institute of Public Health, University of Cambridge; 2. Public Health Directorate, Cambridgeshire County Council; 3. Cambridgeshire and Peterborough NHS Foundation Trust Introduction A framework of complex interventions to reduce falls and fall-related admissions has been developed by a multi-agency working group across Cambridgeshire & Peterborough to form an integrated evidence-based Falls Prevention Programme. Current services, funded by a raft of health and care partners involved, deliver within and towards these approaches. However, there is no systematic overview of effectiveness, nor of quality and join-up with and between services. Moreover, there is a lack of detailed understanding of the elements essential for translating this framework, which spans different approaches for varying needs across the population, into tangible improvements at operational level.
Method This project to identify and understand what is needed to a) implement and b) evaluate local falls prevention activity most effectively is using opportunities offered by IT re-configurations and new service innovations. Three work packages employ complementary methods to maximise learning from the assessment of implementation roll-out.
WP1 Understanding fall prevention service implementation in practice: an observational study of new services developing in real time (case studies: pilot project embedding a dedicated falls lead within a local neighbourhood team; development of falls specialist health trainer roles).
WP2 Understanding enablers and barriers for falls prevention programmes: a qualitative study exploring multiple perspectives from practitioners across services, older people and families.
WP3 Understanding data for falls prevention programmes: action research with information managers and data users developing county-wide “Falls Dashboard” to enhance delivery and evaluation of fall prevention.
Results and Conclusion(s) There is a need for robust intelligence to inform the implementation and evaluation of falls prevention programmes in the context of real world delivery with variability in structures and resource constraints in differing settings. Findings from this evaluation in progress across a diverse county will be informative for other initiatives elsewhere.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
25
Clinical Quality MOUTH CARE MATTERS (MCM) IS A HEALTH EDUCATION ENGLAND TRAINING INITIATIVE FOCUSSED ON IMPROVING THE ORAL HEALTH OF OLDER PEOPLE. THE HOSPITAL ARM OF THE PROGRAMME WAS DEVELOPED AND PILOTED AT EAST SURREY HOSPITAL AND IS CURRENTLY BEING ROLLED OUT ACROSS ALL ACUTE TRUSTS IN KENT, SURREY AND SUSSEX J Mann, M Doshi Surrey and Sussex Healthcare Trust
Background Oral health deteriorates in hospital. Particularly in the elderly and vulnerable, poor oral health is associated with hospital acquired infections, poor nutritional intake, longer stays and increased costs. Maintaining good oral health is important for patient dignity, ability to communicate and remains a key element of compassionate care.
Innovation A multidisciplinary team of dental professionals was recruited. Their aim was to provide ward and classroom-based training to staff about the importance of mouth care and the skills required to carry it out. A mouth care policy was created. Effective tools for mouth care were made available on the wards such as toothbrushes and denture pots. Doctors’ training raised awareness of issues surrounding poor oral health and recognition of indications for intervention.
Evaluation MCM training sessions were well received with 90% of attendees stating that oral health care training should be mandatory. Audits showed an improvement in mouth care recording by 70%. The MCM team received an average of 50 referrals each month for patients requiring additional help with oral health related issues. 100% of wards now stock the appropriate tools. The number of dentures reported missing rose sharply from an annual average of 5 to 20 in the inaugural year. Oral health training is now mandatory for non- medical clinical staff and on the programme for junior doctors training.
Conclusions MCM is successfully integrating oral health into general health within the trust. The rise in denture-loss reporting is due to increased awareness of the issue. Incorporating oral health teaching into the statutory training and curriculum for health professionals will help ensure sustainability of the programme. There is ongoing lack of knowledge and training amongst junior doctors surrounding oral health care. Future development of the MCM programme will include working to include oral health for doctors included at undergraduate and postgraduate levels.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
26
Clinical Quality A SERVICE IMPROVEMENT PLAN TO RAISE AWARENESS OF THE IMPACT OF DENTURE LOSS ON INPATIENTS AND REDUCE THE NUMBER OF DENTURES LOST AT SURREY AND SUSSEX HEALTH TRUST (SASH) J Mann, M Doshi Surrey and Sussex Healthcare Trust
Background The loss of dentures for inpatients can have a detrimental effect on their well-being. Self-respect and dignity become compromised along with their ability to eat meals, communicate clearly and long-term recovery.
Many have worn their dentures for over 10 years and may not easily adapt to replacements (Michaeli L, Davis D & Foxton R, Gerodontology 2007; 24; 117–120). The denture-making process can take months.
Trust-wide between 2011-2015, a yearly average of 5 dentures were reported missing, despite the dental department remaking 10 annually. The most common reasons for reported loss were: patient transit between wards, loss within bed linen and dentures mistakenly discarded while wrapped in tissues.
Innovation Several measures were put in place to raise awareness and combat potential loss. A specific pathway for reporting and constructing new dentures was implemented. Bedside ‘Sunflower’ visuals helped to identify those with dentures while specific pots were installed on wards. Training aimed to alert healthcare staff about the impact of denture loss and time required to make a denture.
Results Revealingly, since the above changes were instigated 10 months ago, 20 dentures have been reported missing, suggesting the number of dentures lost may have been underestimated.
Conclusions Thus far positive feedback has been reported from both patients and staff regarding the training and changes put in place. There is a clear pathway at SASH, but at other trusts within Kent, Surrey and Sussex there is no specific pathway in place. Future aims are to ensure a replicable pathway is defined nationally.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
27
Clinical Quality MEDICAL STUDENTS AS ADVOCATES - IMPROVING CARE FOR OLDER ADULTS M Tan, M E Dos Santos, T Pattison Department of Ageing and Complex Medicine, Salford Royal NHS Foundation Trust
Background Geriatric Medicine is a speciality whose ethos is to provide high-quality patient-centred care for every older person. Obtaining patient feedback allows us to identify areas for improvement and work towards a patient-led healthcare service. Medical students can be encouraged to play an active part in the continuous quality improvement of how we care for older adults. Drawing on principles described in the “ASK ONE QUESTION” campaign coined by the Institute for Healthcare Improvement Open School for Health Professionals (Carson-Stevens A et al. Am J Med Qual. 2013. 28(2)174), we aimed to enable University of Manchester medical students to become advocates in identifying ways to improve care for older patients.
Sampling Methods Over a two-year period we recruited medical students completing placements in Geriatric Medicine at Salford Royal Hospital. We requested that during each patient encounter they ask, “What could we have done to improve your care?”. In groups they presented a chosen patient with that individual’s feedback at the end. In total, we obtained 104 pieces of feedback.
Results The most common feedback was that patients could not think how their care could be improved (22/104). A large proportion of suggestions were communication based; communication regarding current admission (14/104 patients), communication regarding discharge (5/104) and communication between members of the MDT (4/104). Other recommendations included; getting home sooner (13/104), and more therapy (8/104 patients). A total of 28 themes for improvement were obtained.
Conclusions Medical students have understanding of the healthcare system and available time to explore patient’s thoughts, some of which may be overlooked by the clinical team. This student led patient feedback survey has highlighted communication with patients about their care, as an area for improvement in our local Geriatric department. Medical students are tomorrow’s doctors and empowering them to identify ways of improving patient-centred care can be invaluable to all parties.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
28
Clinical Quality COGNITIVE IMPAIRMENT - PROFILING ITS IMPLICATIONS FOR PATIENTS WITH HIP FRACTURE A Johansen, C Boulton, V Burgon, S Rai, R Wakeman National Hip Fracture Database, Royal College of Physicians, London
Introduction Over a quarter of patients are known to have dementia when they present with hip fracture, and screening for cognitive impairment identifies many others in whom this diagnosis has not previously been made, and who are at high risk for delirium, the commonest complication of hip fracture.
Method Screening using the abbreviated mental test (AMT) has become routine in all trauma units since the National Hip Fracture Database was established in 2007. An AMT result was reported for 94.9% of cases in 2015. We examined the implications of this test for these patients.
Results Of those screened at presentation, 22,595 (37.5%) had a low AMT score (<8/10), while 37,632 (62.5%) had a normal AMT. The group with abnormal AMT included more women (74.5% cf 70.3%), was older (mean 85.6, cf 81.0 years), with fewer admissions from home (51.1% cf 93.6%), 10 times more from a care home (43.2% cf 4.1%). Over twice as many had fallen in hospital (5.7% cf 2.3%). They were less likely to reach an orthopaedic ward within 4 hours, and tended to be graded as less fit for anaesthetic, but time to operation was unaffected (75% of both groups getting to theatre within 36 hours), and encouragingly were more likely to receive a nerve block (45.0% cf 42.5%) as part of pain management. They were less likely to mobilise by the first postoperative day (72.2% cf 82.1%), less likely to return home (30.5% cf 58.1%), and faced a two-fold increased risk of dying as an inpatient (9.5% cf 4.6%).
Discussion These figures may be helpful in understanding the scale of problems facing this key patient group, but potentially oversimplify a complex issue. The interplay between dementia, quality of care and outcome warrants further investigation.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
29
Clinical Quality INTRODUCTION OF A TARGETED INTERVENTION ‘FRAILTY PASSPORT’ TO ACHIEVE REDUCTION OF ADMISSIONS AND LENGTH OF STAY FOR ‘HIGH INTENSITY’ PATIENTS
N Humphreys2, G Lowe2, H Wright1, N Davies1, S Lea1, A Arora1, R Bryan1, J Oxtoby1
1 University Hospitals of North Midlands NHS Trust, 2 Staffordshire & Stoke-on-Trent Partnership NHS Trust
Background Frail Older people often have multiple hospital admissions and this remains a challenge nationally. Analysis of admissions data from University Hospitals of North Midlands NHS Trust (UHNM) identified a cohort of ‘high intensity users’ who had 3+ admissions and 40+ bed days during a 12 month period. These 705 patients used 47,000 bed days, accounting for 130 hospital beds daily (April 2015-16).
This project evaluated a targeted service intervention placing the patient at the centre, aimed at reducing unplanned admissions and length of stay by establishing an integrated care plan, bridging communication and care between all providers.
Innovation UHNM Clinical Information System (CIS) identified ‘high intensity patients’ over 65 years. A collaborative approach across emergency, acute, community and social care took a review of the care provided and implemented a ‘Frailty Passport’; and assigned an integrated case worker to co-ordinate care between primary, secondary care and social services. Patients hold their Frailty Passport and all decisions are made based on how the patient describes their need.
Evaluation Between January and June 2016, 46 patients aged over 65 years participated in the project, mean age, 79.48 years (SD 7.84).
Following intervention, the admissions and bed days by this cohort was reduced by 53% of the proportional pre intervention totals.
Comparing admissions and bed days in the month prior to recruitment with the month following recruitment, an initial reduction of 24% and 11% was recorded respectively. This reduction continues each month. The first five patients who were involved with the project for 5 months, produced a combined reduction in bed days of 40.6% and a 71.4% reduction in admissions.
The greatest reduction in admissions (28%) and bed days (40%) is recorded between month 2 and 3.
Conclusions Our data suggests the introduction of a Frailty Passport which is patient centred and individualised, with targeted intervention has benefitted patients by reducing admissions and bed days with the greatest reduction occurring during the first 3 months. Collaboration across the whole service provision has also improved patient experience and compliance.
Further analysis will focus on longer term benefits and economic impact.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
30
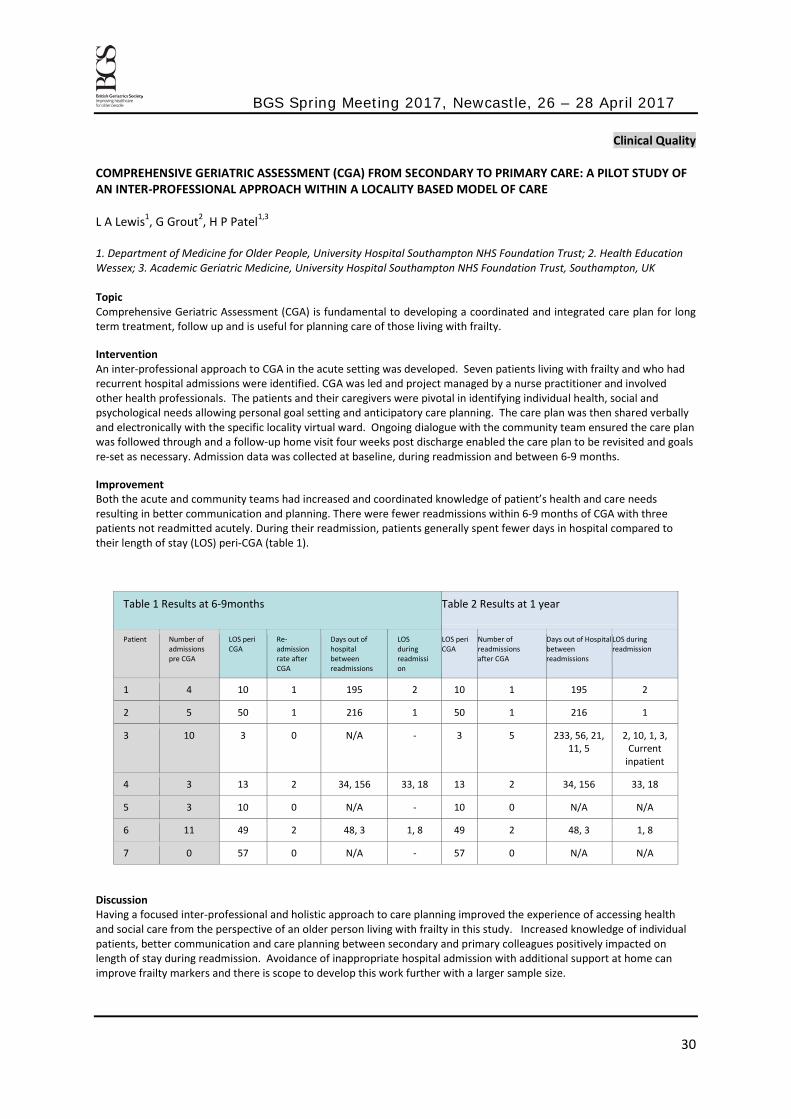
Clinical Quality COMPREHENSIVE GERIATRIC ASSESSMENT (CGA) FROM SECONDARY TO PRIMARY CARE: A PILOT STUDY OF AN INTER-PROFESSIONAL APPROACH WITHIN A LOCALITY BASED MODEL OF CARE L A Lewis1, G Grout2, H P Patel1,3 1. Department of Medicine for Older People, University Hospital Southampton NHS Foundation Trust; 2. Health Education Wessex; 3. Academic Geriatric Medicine, University Hospital Southampton NHS Foundation Trust, Southampton, UK Topic Comprehensive Geriatric Assessment (CGA) is fundamental to developing a coordinated and integrated care plan for long term treatment, follow up and is useful for planning care of those living with frailty.
Intervention An inter-professional approach to CGA in the acute setting was developed. Seven patients living with frailty and who had recurrent hospital admissions were identified. CGA was led and project managed by a nurse practitioner and involved other health professionals. The patients and their caregivers were pivotal in identifying individual health, social and psychological needs allowing personal goal setting and anticipatory care planning. The care plan was then shared verbally and electronically with the specific locality virtual ward. Ongoing dialogue with the community team ensured the care plan was followed through and a follow-up home visit four weeks post discharge enabled the care plan to be revisited and goals re-set as necessary. Admission data was collected at baseline, during readmission and between 6-9 months.
Improvement Both the acute and community teams had increased and coordinated knowledge of patient’s health and care needs resulting in better communication and planning. There were fewer readmissions within 6-9 months of CGA with three patients not readmitted acutely. During their readmission, patients generally spent fewer days in hospital compared to their length of stay (LOS) peri-CGA (table 1).
Table 1 Results at 6-9months Table 2 Results at 1 year
Patient Number of admissions pre CGA
LOS peri CGA
Re-admission rate after CGA
Days out of hospital between readmissions
LOS during readmission
LOS peri CGA
Number of readmissions after CGA
Days out of Hospital between readmissions
LOS during readmission
1 4 10 1 195 2 10 1 195 2
2 5 50 1 216 1 50 1 216 1
3 10 3 0 N/A - 3 5 233, 56, 21, 11, 5
2, 10, 1, 3, Current
inpatient
4 3 13 2 34, 156 33, 18 13 2 34, 156 33, 18
5 3 10 0 N/A - 10 0 N/A N/A
6 11 49 2 48, 3 1, 8 49 2 48, 3 1, 8
7 0 57 0 N/A - 57 0 N/A N/A
Discussion Having a focused inter-professional and holistic approach to care planning improved the experience of accessing health and social care from the perspective of an older person living with frailty in this study. Increased knowledge of individual patients, better communication and care planning between secondary and primary colleagues positively impacted on length of stay during readmission. Avoidance of inappropriate hospital admission with additional support at home can improve frailty markers and there is scope to develop this work further with a larger sample size.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
31
Clinical Quality DNACPR – TRAINING FOR CONVERSATIONS WITH PATIENTS C J Bond, R O Price UCLH, Department of Geriatric Medicine Topic Discussions around end of life and resuscitation can be difficult for clinicians as well as for patients and relatives. Training to improve the quality of these conversations and our understanding of the ethical and legal issues involved can improve our confidence and is likely to enhance the patient experience. Increasing clinician’s awareness of the advantages to adopting a patient centred approach may encourage adherence to recent changes in expected practice in DNACPR decision making. Intervention A ‘talking DNACPR’ course incorporating high fidelity communication simulation sessions, group work and expert facilitation has been running at UCLH since November 2014. The course is available to consultants, registrars and Band 7+ nurses and allied health professionals. Candidates have the opportunity to observe and participate in simulation sessions with professional actors, in addition to self-reflection and group work relating to ethical, legal, cultural and religious perspectives in DNACPR decision making.
Improvement 37 candidates attended the course between November 2014 and October 2016. Post-course survey data demonstrate significant improvement in confidence in approaching difficult conversations with patients, relatives and colleagues. Open ended response questions within the survey suggest that candidates found the course useful and likely to result in changes to their clinical practice. Participation in the simulation was the element scored most highly by candidates as useful or influential. Discussion The DNACPR course is challenging to implement in that appropriate facilities, professional actors and expert facilitation are required, resulting in significant cost. It is clear in justifying the expense for this course that the outcomes we hope to improve are important, but they are also intangible and hence difficult to measure. Our hope is that an improved quality of communication will benefit clinicians and the organisations we work for as well as our patients.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
32
Clinical Quality NEW PRACTICE DEVELOPMENT - IMPROVING EDUCATION AMONGST THE MULTIDISCIPLINARY TEAM A Cronin, G Noblet Aintree University Hospital, Liverpool
Background Adequate education and training for staff in clinical areas focusing on care and compassion for frail older people is needed (NHS England, February 2014). Geriatricians should be seen as educators and awareness-raisers (Oliver D, Burns E: Future Hospital Journal 2016:3(1)49–54). The importance of involving our colleagues who assist in the care of our patients on the ward should not be under-valued.
Innovation The project was commenced on a 36 bedded geriatric ward in an acute hospital trust. At the time of initiation, morale was low due to staffing shortages and work load. Hosting “Sharing Knowledge Sessions” was thought to offer an opportunity to enhance staff value and development whilst having a beneficial effect on patient care. Staff were asked to list topics they would like to learn more about. Ten to fifteen minute sessions were held with 3-4 attendees at a time; and repeated as many times as necessary to allow all members of the team on shift to participate. All members of the team took responsibility for presenting a topic if it was relevant to their expertise e.g. therapy lead the patient positioning session. Topics included constipation, resuscitation, delirium and dementia.
Evaluation Qualitative data was collected which showed overwhelmingly that the sessions were considered a success. There was an improvement in patient care through the greater understanding of the reasons behind practice and management e.g. stool charts were completed more accurately after the constipation session.
Conclusions In order to provide good care for our elderly population we need to recognise the importance of the multidisciplinary team in that process. The creation of an environment which enhanced personal development allowed for staff to feel valued and appreciated in their duty thus positively impacting on the continuing care of our patients. The sessions are on-going and we are hoping to demonstrate sustained change.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
33
Clinical Quality IMPROVING MEDICINES MANAGEMENT IN INPATIENTS WITH PARKINSON'S DISEASE: INTRODUCING THE OPTIMAL CALCULATOR S Gowing1, K King1, G Strike1, N Fox2 1. University Hospitals Southampton NHS Foundation Trust, 2. Poole Hospital NHS Foundation Trust
Topic Medicines management is crucial in the care of the patient with Parkinson’s Disease (PD) when they are admitted to hospital either electively or in an emergency. This can become more difficult when Parkinson's patients are nil-by-mouth, unable to swallow or unable to absorb their usual PD drugs due to intercurrent illness. Missed doses can result in clinical complications and increased length of hospital stay.
Intervention We created a web-based conversion calculator to help non-specialist clinical staff manage patients with PD when they are admitted to hospital and better plan for elective admissions.
Improvement The introduction of the calculator saw a significant reduction in missed doses of Parkinson’s medications from 97% to 50.9%. The average number of missed doses came down from 6 per patient per admission to 1.33. In the initial audit 6 patients were nil by mouth, 50% of these had a nasogastric tube inserted for administration of Parkinson’s medication and for the 3 who didn’t, none of them were converted to a Rotigotine patch.
Following the introduction of the calculator, 6 patients were nil by mouth, 1 had a nasogastric tube inserted and 3 were converted to Rotigotine. Of note, the average length of stay of patients with Parkinson’s disease was reduced from 13.38 to 9.66 days following the introduction of the calculator.
Discussion Prior to implementing the calculator we sought agreement from the hospital Drugs and Therapeutics Committee as well as a number of stakeholders. In order for the introduction of the calculator to have maximal effect we undertook a series of teaching sessions for medical and nursing staff within the trust. Due to regular rotations of junior medical staff, the ward pharmacists have played a crucial role in the sustainability of the intervention as they are more permanent members of staff in ward areas. The results discussed above have shown that there has been a significant improvement in the number of missed doses and length of stay of PD patients which is due to a combination of both the calculator and staff education.
The PD conversion calculator is available at www.parkinsonscalculator.com and also through both the Parkinson’s UK and British Geriatrics Society websites.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
34
Scientific Research – Biology and Social Gerontology EFFECTS OF MULTICOMPONENT EXERCISE AND THERAPEUTICLIFESTYLE (CERGAS) INTERVENTION ON COGNITIVE FUNCTION IN LOWER INCOME ELDERLY POPULATION: A CLUSTER RANDOMISED CONTROLLED TRIAL R Rosli1, D A Loh2, W Y Choo2, F MohdHairi3, D Peramalah2, S Kandiben2, P L Lee2, N Gani2, M F Madzlan2, M A I Abd Hamid2, Z Akram4, A S Chu5, A Bulgiba2, R G Cumming6,7, M P Tan1, A V Chin1, N N Hairi2 1. Department of Medicine, Faculty of Medicine, University of Malaya, 2. Department of Social and Preventive Medicine, University of Malaya, Kuala Lumpur, Malaysia, 3. Department of Social and Preventive Medicine, University of Malaya, Kuala Lumpur, Malaysia, 4. Department of Oral Pathology, Faculty of Dentistry, University of Malaya, Kuala Lumpur, Malaysia, 5. Fitness First Malaysia, Malaysia, 6. Concord Hospital, Concord, NSW, Australia, 7. Sydney School of Public Health, University of Sydney, Sydney, NSW, Australia
Background To evaluate the effects of a multiComponent Exercise and theRApeuticlifeStyle (CERgAS) intervention program on cognitive function lower income elderly population in Malaysia.
Methods A six-week cluster randomized community-based intervention programme was conducted among individuals aged 60 years and above, residing in public housing. Participants were randomised to multicomponent group exercises, nutrition education, oral care education and psychosocial support, or a general health education booklet. The Mini Mental State Examination (MMSE) was measured as a secondary outcome at baseline, immediately post-intervention, 3-months and 6-months. Intention to-treat (ITT) analysis was used.
Results 256 individuals (intervention=168; control=88) were recruited. Based on MMSE sub-domains, there was no significant decline in registration (mean difference (95% confidence interval) = -0.06 (-0.13, 0.01), attention (-0.07 (-4.81, 0.33) and delayed recall (-0.17 (-0.39, 0.04) among the intervention group at 6 months compared to baseline. Participants in the control group however showed a significant decline in the MMSE sub-domain of registration (-0.18 (-0.35, 10.1), attention (-0.51 (-0.91,-0.12) and delayed (-0.32 (-0.60, -0.03) recall at 6 months compare to baseline.
Conclusion A combined multi-component exercise and lifestyle intervention was effective in reducing the decline in MMSE within an older, lower income population. Our findings represent a major breakthrough in measures for prevention of cognitive decline in the South-East Asian population and will inform public policies for our rapidly increasing older population.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
35
Scientific Research – Biology and Social Gerontology PICTURE-BASED MEMORY IMPAIRMENT SCREEN FOR DEMENTIA: INFLUENCE OF ETHNICITY AND EDUCATION LEVEL AMONG THE ELDERLY IN MALAYSIA R Roshaslina1, T M Pin1, W K Gray2, P Subramanian3, A V Chin1 1. Ageing and Age-Associated Disorders Research Group, Faculty of Medicine, University of Malaya, 2. Northumbria Healthcare NHS Foundation Trust, North Tyneside General Hospital, UK, 3. Department of Nursing Science, Faculty of Medicine, University of Malaya
Introduction Differences in linguistic properties, literacy level, and cultural acceptance may cause difficulties and are known as major limitation factors in identifying dementia in developing countries where the greatest increase in prevalence of dementia is expected to be seen. This study aimed to investigate the influence of multi-ethnicity and education level on Picture-based Memory Impairment Screen (PMIS) among elderly in Malaysia.
Methods The PMIS, Identification and Intervention for Dementia in Elderly Africans (IDEA) cognitive screen and Mini Mental State Examination (MMSE) were administered to a convenience sample of elderly individuals (≥60years) from the community and outpatient clinics at the University of Malaya Medical Centre, Kuala Lumpur, Malaysia. Consensus diagnosis was performed by two geriatricians blinded to PMIS scores using the Diagnostic and Statistical Manual of Mental Disorders, Fifth Edition (DSM-V) clinical criteria.
Results A total of 564 participants were recruited with median (interquartile range, IQR) age of 71.5 (67-83) and median years of education 11.0 (9-13). About 317 (55.4%) were female and 255 (44.6%) were male. The majority were Chinese (n=361, 63.1) followed by Indian (n=133, 23.3%) and Malay and Others (n=78,13.6%). Based on DSM-V classification among 75 randomly selected individuals, participants with major neurocognitive disorder (n=33, 64%) (T-test, p<0.05) showed poorer performance in PMIS compared to those with no neurocognitive disorder (n=42, 56%). In univariate analyses, fewer years of education and differences in ethnicity were insignificantly associated with performance of PMIS (Kruskal-wallis test, p>0.05). After adjustment for DSM-V classification in multivariable logistic regression, fewer years of education and differences in ethnicity remain insignificantly (p>0.05) different in performance of PMIS.
Conclusions PMIS performance showed no influence on ethnicity and education level among our elderly. This study may give options for healthcare providers on available screening tools that consider cultural and educational factors in screening dementia.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
36
Scientific Research – Bone, Muscle and Rheumatology
SARCOPENIA AND BONE HEALTH IN COMMUNITY DWELLING OLDER ADULTS: FINDINGS FROM THE HERTFORDSHIRE SARCOPENIA STUDY (HSS) H P Patel1,2, E M Dennison1, L Westbury1, A A Sayer1,2,3,4, C Cooper1,3
1. MRC Lifecourse Epidemiology Unit, University of Southampton, 2. Academic Geriatric Medicine, University of Southampton, 3. Ageing, Geriatrics and Epidemiology, Institute of Neuroscience, Newcastle University, 4. NIHR Newcastle Biomedical Research Centre, Newcastle University and Newcastle upon Tyne NHS Foundation Trust, 5. Musculoskeletal Biomedical Research Unit, University of Oxford Introduction Muscle and bone share similar embryological origins and musculoskeletal disease has a significant impact on health in later life. There is growing interest in the relationship between bone health and sarcopenia in older adults as both sarcopenia and osteoporosis are independently associated with disability, falls and mortality. Our aim was to determine if sarcopenia was associated with adverse bone health indices among community dwelling older adults.
Methods One hundred and five men aged 68–76 years were recruited to the Hertfordshire Sarcopenia Study (HSS) for detailed characterisation of muscle including measures of muscle mass, strength and function. Dual energy x-ray absorptiometry (DXA) was used to measure whole body, lumbar spine and femoral neck bone mineral content (BMC) and bone mineral density (BMD) as well as total muscle mass.
Results Results were available for 103 participants with mean age (SD) 72.5 (2.5), BMI 27.2 (3.5) kg/m2, lean mass (kg) 56.4 (6.7), grip strength (kg) 38.7 (8.3) and gait speed (m/s) 1.10 (0.20). Seven (7 %) men had sarcopenia as defined by the European Working Group on Sarcopenia in Older People (EWGSOP) criteria. These men had lower BMC (g) (SD) (p<0.02) for the whole body 2838.3 (422.7) vs 2386.2 (368.5); lumbar spine 78.5 (16.3) vs 63 (12.6) and femoral neck 48.7 (7.5) vs 40.2 (6). They also had lower BMD (g/cm2) (SD) (p<0.05) for the lumbar spine 1.1 (0.18) vs 0.96 (0.15) and femoral neck 1.03 (0.14) vs 0.92 (0.11).
Conclusions We have shown that there are altered bone health parameters in older men with sarcopenia suggesting interventions should be targeted at improving both muscle and bone function for the potential of improving overall musculoskeletal health and maintaining independence in older people. This work now requires replication a larger cohort that includes women.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
37
Scientific Research – Bone, Muscle and Rheumatology VITAMIN D DEFICIENCY IS ASSOCIATED WITH ETHNICITY AND KNEE PAIN SEVERITY IN A MULTI-ETHNIC SOUTH EAST ASIAN NATION S Mat1, M H Jaafar1, T M Pin1,2 1. Ageing and Age-Associated Disorders Research Group, University of Malaya, 2. Department of Medicine, Faculty of Medicine, University of Malaya
Introduction Reduced circulating 25-hydroxyvitamin D have been correlated with many health conditions, including chronic pain. Previous studies mainly from Northern America and Europe have suggested with darker skin tones are associated with vitamin D deficiency which may mediate observed differences in joint pain. The purpose of this study was to examine whether variations in vitamin D levels contribute to ethnic differences in knee pain in our Asian population.
Method This was a cross-sectional study from the Malaysian Elders Longitudinal Research (MELoR) study consisting of 1010 individuals from representative groups of community dwelling older persons (57% female), aged 86.5 (54-94) years. 313 were ethnic Malays, 367 Chinese and 330 Indians. Participants were asked if they had knee pain and the severity symptoms of knee pain were measured on a visual analogue scale. Levels of serum 25-hydroxy vitamin D [25-(OH)D], the ideal indicator of vitamin D status, were measured using routine laboratory techniques.
Result The ethnic groups with darker skin tones, Malays and Indians, had significantly lower levels of vitamin D compared to the ethnic Chinese [Mean in ng/L (SD): 18.54 (7.11), 18.87 (7.23), and 24.88 (6.77) respectively; p=<0.001]. The former two ethnic groups were also more likely to report the presence of knee pain [N (%): 140 (44.6%), 180 (32.3%), 89 (24.1%) respectively; p=<0.001]. Low levels of vitamin D predicted increased risk of self-reported knee pain. In the mediation analysis, group differences in vitamin D however did not predicted group differences in pain severity, after adjustment for confounders.
Conclusion While our data clearly demonstrates ethnic differences in Vitamin D level and self-reported knee pain, difference in Vitamin D did not mediate the ethnic differences in knee pain. Our study therefore challenges the findings of a recent study conducted in Florida suggesting that the vitamin D differences with skin tone accounted for differences in knee pain between individuals with different ethnic groups.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
38
Scientific Research - Cardiovascular
INITIAL ORTHOSTATIC HYPOTENSION IS ASSOCIATED WITH BETTER TIMED-UP AND GO AND GRIP STRENGTH IN URBAN OLDER MALAYSIANS
N I Saedon1, J Frith2, C H Goh1, S B Shahrul1, A V Chin1, H M Khor1, M P Tan1 1. Department of Medicine, Faculty of Medicine, University of Malaya, Kuala Lumpur, 2. Institute for Cellular Medicine, Newcastle University UK
Introduction Romero-Ortuno et al (2011) suggested that initial orthostatic hypotention (IOH) is associated with increased frailty in older adults. We therefore evaluated this relationship among community-dwelling older adults recruited to a longitudinal study of ageing in urban Malaysia, the Malaysian Elders Longitudinal Research (MELoR) study.
Objective To relationship with time-up-and-go (TUG), functional reach (FR) and hand grip (HG) with IOH.
Methods Haemodynamic data was available for 1245 older adults aged 55 years and above selected through stratified random sampling from the electoral roll. Postural blood pressure change was assessed during five minutes’ supine rest followed by three minutes of standing using non-invasive continuous blood pressure measurements (Task Force, CNSystems, Austria). Initial orthostatic hypotension (IOH) is defined as a systolic (SBP) drop >40mmHg or diastolic BP (DBP) drop >20mmHg within 15 seconds of standing. TUG, FR and HG were measured on the same occasion using established protocols. Comparisons were made between individuals with and without IOH.
Results Three hundred and twelve (25%) participants had IOH. Individuals with IOH had significantly faster timed-up and go (TUG) (11.7(4.7) vs 12.7(4.0)s, p=0.021) and functional reach (27.2(7.7) VS 24.5(7.3)cm, p= <0.001). They were also found to have a better mean dominant hand grip (25.3(8.0) VS 22.5(7.9)kg, p=0.006). All three variables remained statistically significant after adjustment for age and gender.
Conclusion Our findings using TUG, FR and HG as surrogates of frailty contrasted that of the previously mentioned study. We will be evaluating this relationship further by assessing frailty using published frailty scales.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
39
Scientific Research - Cardiovascular BOLUS WATER DRINKING FOR ORTHOSTATIC HYPOTENSION IN OLDER PEOPLE: A PHASE 2 STUDY J Frith Institute of Cellular Medicine, Newcastle University and the Falls and Syncope Service, Newcastle Hospitals
Introduction Older people with orthostatic hypotension (OH) are frequently told to drink plenty of fluids and avoid dehydration. However, much of this advice is extrapolated from studies of bolus water drinking in younger cohorts with autonomic failure.
Aim To determine the basic efficacy of bolus water drinking in older people with OH.
Methods An early phase study design was undertaken to see whether an oral bolus of water resulted in a predefined response – a reduction in orthostatic systolic BP drop by ≥10 mmHg (a response previously demonstrated to improve symptoms). Using the A’Hern approach, a sample size of 25 would be required, with the required response seen in ≥six participants (alpha 0.05, beta 0.8).
Participants aged >60 with OH were recruited from Newcastle’s Falls and Syncope Service. All medications were withheld ≥12 hours beforehand. Participants rested supine for 10 minutes before standing upright for 3 minutes while undergoing beat-to-beat BP monitoring. A 480 ml bolus of water was then taken orally, within 5 minutes. Postural BP was repeated 15 minutes later. Continuous BP was summarised into 5 second averages. Paired sample t-test was used to compare means.
Results Median age of the 25 participants was 74 years (range 60-92), with a median Charlson Comorbidity Score of 4 (3-8); median number of regular medications was 4 (0-13). Three were prescribed midodrine and five, fludrocortisone.
Mean baseline BP was 128/75 mmHg (standard deviation 21/13), this increased to 132/80 (SD 28/18) mmHg following the oral bolus of water [median bolus 480 ml (288-480)]. Mean postural BP drop was 41/19 mmHg (22/13). This reduced to 33/15 (19/12) mmHg following water.
The basic level of efficacy was observed in 14/25 participants, meeting the required criteria. Statistical analysis demonstrated similar baseline BPs; however, after the water bolus, standing systolic BP was significantly higher, particularly towards the end of standing, whereas diastolic BP was significantly greater during the first minute of standing.
Conclusions Bolus water drinking meets a predefined level of efficacy in this phase 2 study and will be explored further in a phase 3 clinical trial. Bolus water drinking resulted in a statistically significant increase in standing BP. Bolus water drinking may be more effective than simply staying hydrated for older people with OH.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
40
Scientific Research: Cardiovascular DROXIDOPA FOR ORTHOSTATIC HYPOTENSION: A SYSTEMATIC REVIEW AND META-ANALYSIS V Strassheim1, J L Newton1,2, M P Tan3, J Frith1,2
1Falls & Syncope Service, Newcastle upon Tyne Hospitals NHS Trust, 2. Institute of Ageing, Newcastle University, 3. Ageing and Age-Associated Disorders Research group, University of Malaya, Malaysia
Introduction This systematic review and meta-analysis aims to determine the efficacy and safety of droxidopa in the treatment of orthostatic hypotension (OH), following its recent approvals in the US.
Methods MEDLINE, EMBASE, PubMed, Cochrane Controlled Trials Register, Web of Science, ProQuest and the WHO Clinical Trials Registry were searched. Studies were included if they randomised adults with OH to droxidopa or to control, and outcomes related to symptoms, daily activity, blood pressure or adverse events. Data was extracted independently by two reviewers. Risk of bias was judged against the Cochrane risk of bias tool and quality of evidence measured using GRADE criteria. A fixed-effects model was used for pooled analysis.
Results Of 224 identified records, four studies met eligibility, with a pooled sample size of 494. Mean age was 67 years (range 18-92). Study duration was between one and eight weeks. Droxidopa was effective at reducing dizziness [mean difference -0.97 (95% confidence interval -1.51, -0.42)], overall symptoms [-0.52 (-0.98, -0.06)] and difficulty with activity [-0.86 (-1.34, -0.38)]. Droxidopa was also effective at improving standing systolic blood pressure [3.9 (0.1, 7.69)]. Rates of adverse events were similar between droxidopa and control groups, including supine hypertension [odds ratio 1.93 (0.87, 4.25)].
Conclusions Droxidopa is safe and effective at reducing the symptoms associated with neurogenic OH. It results in a modest increase in standing BP without increasing the risk of supine hypertension.
Registration: PROSPERO ID CRD42015024612

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
41
Scientific Research – Education and Training
TEACH ME OR GUIDE ME? WHAT DO JUNIOR DOCTORS WANT TO LEARN ABOUT GERIATRIC MEDICINE AND HOW, DURING THEIR FIRST YEAR OF PRACTICE? M I Hohenberg Western Sydney University, Sydney Australia
Background Educational objectives have been well-defined by educators for doctors in their first year of practice after medical school; for example the UK Foundation Programme and the Australian Curriculum Framework for Junior Doctors. However there has been little research on intern (first year doctors after medical school) perspectives of what they feel would be important to learn during their internship, and how they wish to learn.
Aims To develop a grounded theory of interns geriatric learning needs and learning preferences during their first year of practice.
Methods All 32 interns at St Vincent’s Hospital Sydney were invited to participate in the research study in the final month of their internship. 22 interns consented and completed the semi-structured interview, where three educationally significant experiences during their internship were explored. An unstructured discussion completed the interview, reviewing any missed educational topics of significance to the intern. Interviews were recorded, transcribed and manually coded using a validated open axial approach by a single researcher. Emerging geriatric themes formed the basis of results and were validated through member checking. Ethical approval was granted by the parent institution and University.
Results A total of seven interns highlighted educational experiences related to geriatric medicine. Interns highlighted that important areas to cover during a geriatric term include: learning about the multi-disciplinary team (50%), an initial orientation to the practice of geriatric medicine (41%), prescribing sedatives, antipsychotic and analgesic medications (32%), and effective palliative care including the holistic aspects of care (27%). Two learning methods were described as significantly beneficial: structured and unstructured reflective practice (100%) and developing proactivity for their learning in the workplace environment (86%). However 50% of interns described how they felt they lacked the understanding of how to learn from a negative experience they had; a lack of senior support of interns was identified as potentially limiting their learning opportunities (50%); this was particularly evident in non-metropolitan locations.
Conclusions This study has highlights a novel grounded theory of junior doctor geriatric learning needs during their first year of practice. The results demonstrate the value of investigating and understanding intern perspectives in local hospitals or educational networks, incorporating these insights into curriculum development or departmental geriatric education programmes, improving the validity of geriatric education.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
42
Scientific Research – Education and Training HOW CAN WE ATTRACT MORE PEOPLE TO GERIATRIC MEDICINE? A SURVEY OF UK SPECIALIST REGISTRARS IN GERIATRIC MEDICINE P Brock1, J Fisher1, M Garside1, V Gibson1, K Hunt2, S Briggs3, A L Gordon4 1. Northumbria Healthcare NHS Foundation Trust, 2. The Newcastle Hospitals NHS Foundation Trust, 3. University Hospital of South Manchester NHS Foundation Trust, 4. University of Nottingham
Introduction In the United Kingdom, a modest growth in demand for training in Geriatrics has failed to keep pace with the increased health service demand for fully-trained geriatricians (Fisher J, Garside M, Hunt K. Clinical Medicine 2014;14(2):102-6) This may, in part, be due to negative perceptions towards the specialty, and the patient cohort, amongst junior doctors (Samra R, Griffiths A, Cox T. Age and Ageing 2015;44:776-83) and medical students (Robbins T, Crocker-Buque T, Forrester-Paton C. Age and Ageing 2011;40(3):405-08).
We asked current UK Geriatric medicine registrars how they thought the speciality could attract more people to work in it.
Methods All current UK Geriatric medicine registrars were invited to participate in an online survey which included the question: ‘Do you have any ideas how the specialty might attract more people to work in it?’. The survey was available for a six-month period (01/10/2015 to 31/03/2016).
An inductive, iterative approach to analysis was employed. Two researchers coded free-text responses individually, before then comparing, challenging and refining their respective analyses until consensus on a unifying coding framework was agreed.
Results 269 responses were received (response rate 42%). Themes included: the need for increased exposure to Geriatrics prior to specialisation, particularly whilst undergraduate; the transformative power of Geriatricians as role models; strategies to improve the experience of being a medical registrar. Critically, many registrars felt the speciality needed to be promoted more pro-actively and that greater emphasis ought to be placed on the opportunities for sub-specialisation and flexible training.
Conclusions Our data, from current UK geriatric medicine registrars, provided unique insight into why doctors opt for a career in geriatric medicine. We call on the professional bodies responsible for geriatric medicine training to heed the suggestions offered; facilitating implementation of these strategies may help promote recruitment to the specialty and strengthen the geriatrician workforce of tomorrow.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
43
Scientific Research - Epidemiology GRIP STRENGTH AND INFLAMMATORY BIOMARKER PROFILES IN VERY OLD ADULTS A Granic1,2,3, K Davies1,2,3, C Martin-Ruiz1,3,4, C Jagger3,5, T B L Kirkwood3,6, T von Zglinicki4,6, A A Sayer1,2,3,7,8 1. Institute of Neuroscience, 2. NIHR Newcastle BRC in Ageing and Chronic Disease, Newcastle University, and Newcastle upon Tyne HNS Foundation Trust, 3. Newcastle University Institute for Ageing, 4. Newcastle University Ageing Biology Centre, 5. Institute of Health and Society, 6. Institute for Cell and Molecular Biosciences, Newcastle University, Newcastle upon Tyne, 7. Academic Geriatric Medicine, 8. MRC Lifecourse Epidemiology Unit, University of Southampton University, Southampton
Introduction Weak grip strength (GS) and chronic, low-grade inflammation have been implicated in the aetiology of sarcopenia, frailty, disability and mortality in older adults. Given the interrelationships between inflammatory biomarkers, a summary variable may provide better insight into the relationship between inflammation and muscle strength, particularly in very old adults (aged ≥85) who are at highest risk of muscle weakness. However, this approach has not been investigated in this age group.
Methods We used mixed models to explore the association between GS measured four times over 5 years in 813 participants in the Newcastle 85+ Study, and inflammatory components identified by principal component analysis (PCA). Cut-offs of ≤27 kg (men) and ≤16 (women) were used to define sub-cohorts with weak and normal GS at each assessment.
Results PCA identified 3 components, which explained 70% of the total variance in 7 baseline biomarkers in 724 participants with GS data. Basal interleukin-6 (IL-6) and tumor necrosis factor (TNF-α) had the highest loadings on Component 1; stimulated IL-6 and TNFα and homocysteine the highest on Component 2; high-sensitivity C-reactive protein (hsCRP) loaded positively and albumin negatively to Component 3 . In mixed models with adjustment for key confounders (health, lifestyle factors, and anthropometry), only Component 3 was associated with GS. An increase of 1 SD of Component 3 was associated with a reduction of 0.41 kg (P=0.03) in GS initially in all participants, but not with GS decline over time. Similar conclusions held for those in the weak and normal GS sub-cohorts: 1 SD increase in Component 3 was associated with 0.31 kg and 0.51 kg (P≤0.03) lower GS at baseline, respectively but not with GS decline.
Conclusion We have identified three inflammatory biomarker profiles but only the one including hsCRP and albumin showed an association with baseline GS independent of key risk factors. These findings need to be corroborated in future studies investigating the relationship between inflammatory profiles and muscle strength in older adults.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
44
Scientific Research - Epidemiology NEUROMUSCULAR JUNCTION-RELATED GENE EXPRESSION AND PHYSICAL PERFORMANCE IN OLDER MEN: FINDINGS FROM THE HERTFORDSHIRE SARCOPENIA STUDY (HSS) A Granic1,2,3, L D Westbury4, H E Syddall4, H P Patel4,5, R Dodds 1,6, C Cooper4, G Cozens7, M D Grounds7, T Shavlakadze7, A A Sayer1-4,6 1. Institute of Neuroscience, 2. NIHR Newcastle BRC in Ageing and Chronic Disease, Newcastle University, and Newcastle upon Tyne HNS Foundation Trust, 3. Newcastle University Institute for Ageing, Newcastle, 4. MRC Lifecourse Epidemiology Unit, 5. NIHR Southampton BRC, University of Southampton and University Hospital Southampton NHS Foundation Trust, 6. Academic Geriatric Medicine, University of Southampton, Southampton, UK, 7. School of Anatomy, Physiology and Human Biology, University of Western Australia, Australia
Introduction Age-related changes in gene expression associated with the neuromuscular junction (NMJ) indicating myofibre denervation have been implicated in age-related loss of muscle mass and function (sarcopenia). Despite the evidence from both animal and human studies for NMJ degeneration in muscle ageing, little is known about whether changes in NMJ-related gene expression correlate with physical performance (PP) and sarcopenia in older adults.
Methods We used linear regression to explore the association between 5 individual measures, as well as a composite measure of PP, lean mass, and mRNA expression of 15 genes associated with NMJ denervation, in 96 community-dwelling, healthy older men (mean age 72) from the Hertfordshire Sarcopenia Study. Measures of PP were gait speed, the Timed Up-and-Go test, chair rises, one-legged stand, grip strength (GS), and a composite PP score. Lean mass (kg) was determined by dual-energy x-ray absorptiometry. NMJ-related gene expression was measured in muscle biopsies obtained from the Vastus lateralis using qRT-PCR, and quantified by normalized cycle threshold values (ΔCt). Higher ΔCt indicated higher gene expression.
Results All the men had high mean PP scores. Gene expression in relation to PP was heterogeneous. In age-adjusted analysis, significant associations were observed with 9 genes, particularly with nicotinic acetylcholine receptor subunits α, γ, δ (CHRNA, CHRND, CHRNG), and myosin heavy chain 3 (MYH3). Higher expression of CHRNA, and CHRND was associated with stronger GS (p<0.03), and better performance in the composite PP score (p≤0.01). CHRNG was up-regulated in men with higher one-legged stand, composite PP score, and lean mass (p≤0.04). Higher expression of MYH3 was associated with better GS and composite PP score (p≤0.03). No association was found between NMJ gene expression and walking speed.
Conclusion In this cohort of healthy older men with high functional status, we observed heterogeneous expression of genes implicated in myofibre denervation in relation to PP. Larger studies are needed to clarify whether changes in NMJ gene expression may differ by physical activity, and thus affect functional decline in older adults.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
45
Scientific Research - Epidemiology PREDICTIVE VALUE OF THE INTRACELLULAR TO EXTRACELLULAR WATER RATIO VERSUS THE BLOOD UREA NITROGEN TO CREATININE RATIO IN OLDER HOSPITALISED PATIENTS G D Edward 1, A D Wood 1, K Cumming 1,2, M W Kafri 1,3, R L Soiza 1,2, J F Potter 4, P K Myint 1,2,4 1. University of Aberdeen, Aberdeen, 2. Aberdeen Royal Infirmary, Aberdeen, 3. Birzeit University, Palestine, 4. University Of East Anglia, Norwich
Introduction Dehydration is highly prevalent and associated with increased morbidity and mortality in hospital inpatients, particularly among older people. Non-invasive methods of detecting dehydration could be clinically useful in predicting outcomes of acutely unwell patients. The ratio of intracellular water (ICW) to extracellular water (ECW), a marker of dehydration, can be quickly calculated through use of bioelectrical impedance analysis (BIA), although its reliability is disputed. The blood urea nitrogen (BUN) to creatinine (Cr) ratio, calculated from routine admission blood tests, could also be used in detecting dehydration.
Methods Data from two prospective cohort studies were used: patients with fragility fractures (n=125) and stroke patients (n=40). The diagnostic accuracy of the two ratios were evaluated for the outcomes of length of stay and discharge destination. Logistic regression models were generated to estimate the odds ratio for poor discharge (rehabilitation, death) and prolonged hospital stay, defined as lasting more than ten days. Analyses were adjusted for age, sex and condition.
Results N= 165, 115 were female. The mean age of participants was 76.7 (±9.2) years and median length of hospital stay was 6 days. A BUN:Cr ratio of >15 was associated with increased odds for prolonged stay (OR 1.88; CI 0.63-5.64) and increased odds for a poor discharge destination (OR 2.98; CI 0.76-11.65) (p for both >0.05). An ICW:ECW ratio below the 25th percentile was associated with increased odds for prolonged length of stay (OR 1.32; CI 0.52-3.33) and significantly increased odds for poor discharge destination (OR 3.36; CI 1.15-9.81) (p <0.05).
Conclusion The ICW:ECW ratio measured using BIA is fast, non-invasive and could be used in clinical settings to predict outcome in older patients, and appears to be a better prognostic indicator than blood test based estimation of hydration status. Further research should be carried out to establish whether this ratio can be used in other age groups.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
46
Scientific Research - Epidemiology
HYPERTENSIVE END ORGAN DAMAGE IN AN ELDERLY COHORT OF TANZANIANS
H Putnam1, R Jones1, J Rogathi2, W Gray3, R Walker3, 4 1. Newcastle University, 2. Kilimanjaro Christian Medical College, 3. Northumbria Health Care NHS Foundation Trust, 4. Institute of Health and Society, Newcastle University
Background Hypertension - a leading cause of morbidity and mortality - is a growing issue in Sub-Saharan Africa. Prevalence is high in the elderly population of Northern Tanzania but, surprisingly, not linked to increased mortality. Little evidence is available on the physiological effects of hypertension in Africans.
Aim Establish the prevalence of hypertensive end organ damage (EOD) in an elderly cohort of Tanzanians. It was hypothesized that rates of EOD would be surprisingly low amongst this population of survivors.
Methods 412 participants (age ³76) from two villages in Northern Tanzania were followed up from a 2010 hypertension study. Interview established demographics, medical history and assessed cognition. Examination included blood pressure (BP) measurement, ankle-brachial pressure index (ABPI), lying-standing BP, electrocardiogram and dip-stick urinalysis. Prevalence of self-reported visual loss, stroke, peripheral arterial disease (PAD), orthostatic hypotension, left ventricular hypertrophy (LVH), proteinuria and arterial stiffness was reported and correlated with hypertension status and severity.
Results Of 246 participants assessed (59.7%, 53.3% female), 69.1% were hypertensive (BP>140/90mmHg). Treatment and control levels were low (30.6% and 7.7% respectively). Overall prevalence of EOD was as follows: self-reported visual loss – 58.9%, PAD – 28.0%, orthostatic hypotension – 24.4%, proteinuria – 15%, LVH– 13.8%, stroke – 5.3%. Hypertension was significantly associated with PAD (p=0.003), proteinuria (p=0.046) and LVH (p=0.026). Interestingly, hypertensives were noted to have lower rates of arterial stiffness (p=0.130) and cognitive decline (p=0.131).
Conclusion Contrary to the hypothesis, prevalence of EOD in this cohort of elderly Africans is similar to elderly cohorts in developed countries. A beneficial effect of hypertension on arterial calcification and cognition cannot be ruled out. This may go some way to explaining why previous studies have found no increased mortality risk amongst hypertensives in this population, and requires further exploration.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
47
Scientific Research - Epidemiology DIFFERENCES IN PHYSICAL PERFORMANCE ACROSS A MULTI-ETHNIC COHORT OF OLDER ADULTS: INSIGHTS FROM THE HEALTHY AGING RESEARCH INITIATIVE H Mossop1,2, A Granic1,2,3, A A Sayer1,2,3,4, G Engstrom5, K Davies1,2,3, R Dodds1,4, J Galvin7, J G Ouslander6, R Tappen5 1. Institute of Neuroscience, Newcastle University (NU), 2. NIHR Newcastle BRC in Ageing and Chronic Disease, NU, and Newcastle upon Tyne NHS Foundation Trust, 3. NU Institute for Ageing, 4. Academic Geriatric Medicine, University of Southampton, 5. Christine E. Lynn College of Nursing, Florida Atlantic University (FAU), 6. Charles E. Schmidt College of Medicine, FAU, 7. Institute for Healthy Aging and Life Span Studies, FAU, Boca Raton, FL, US
Introduction Physical performance (PP) tests have been developed to measure physical function of older adults, and their relationship with various health outcomes, such as frailty. We aimed to explore differences in PP in relation to health and lifestyle factors among ethnically diverse community-dwelling older adults from one geographic area.
Methods Objective measures of upper (grip strength (GS), arm curls (AC)) and lower (chair stands (CS)) body strength and mobility (gait speed (GSp), steps-in-2-minutes) were assessed across African-American, Afro-Caribbean, Hispanic, and European-Americans aged 60+ living in Florida and participating in the Healthy Aging Research Initiative (HARI) study.
Participant characteristics and PP measures were compared amongst ethnic and age groups (dichotomised at 75 years) using ANOVA. Multivariable linear regression models were explored, stratified by ethnicity, to identify health and lifestyle factors associated with poor PP.
Results Overall 578 participants had PP assessed; 105 African-American, 209 European-American, 122 Hispanic and 142 Afro-Caribbean; 72% (417/578) female, mean age 74.2. The European-American cohort consisted of a higher proportion of men (82/209; 39%) and were slightly older (mean age 77). PP measures are summarised in Table 1. European-Americans had better performance in CS and GSp and Hispanics worse steps-in-2-minutes test. GS was similar amongst ethnicities and also by age group within African-American and Afro-Caribbean cohorts. Multivariable models showed no association between upper body strength and gender in Afro-Caribbeans; however associations between GSp and GS with depression risk was greater than for other ethnic groups.
Conclusion PP measures and associated risk factors varied across ethnic groups. Better understanding of ethnic differences in physical health will help in designing interventions and recognising unmet needs for health and social services.
Table 1
PP measure African-American European-American Hispanic Afro-Caribbean
GS (Kg) 104; 17.2 (8.5) 206; 19.5 (10.8) 119; 18.0 (9.0) 135; 18.7 (10.1) AC (Number in 30 seconds) 94; 13.1 (5.2) 186; 15.2 (5.5) 109; 13.2 (4.2) 128; 11.3 (4.7)
GSp (time (seconds) to walk 4m) 102; 5.9 (2.7) 203; 4.6 (2.6) 113; 6.0 (3.0) 138; 6.3 (3.4)
CS (Number in 30 seconds) 70; 9.8 (2.5) 170; 12.3 (4.3) 96; 10.9 (4.1) 109; 10.2 (2.9)
Steps-in-2-minutes 59; 86.6 (52.9) 140; 90.7 (42.7) 67; 76.1 (48.5) 90; 98.3 (54.3)
Data are Number with data; mean (SD)

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
48
Scientific Research - Epidemiology RISK FACTORS FOR HIV-ASSOCIATED NEUROCOGNITIVE DISORDER IN OLDER PEOPLE IN NORTHERN TANZANIA P Eaton1, J Kellet-Wright1, A Flatt1, S M Paddick2, C Irwin3, J McCartney3, J Thornton3, V Yarwood3, A Duinmaijer4, A Kisoli5, S Urasa5, W Howlett5, R Walker6, C Dotchin6, W K Gray6 1. The Medical School, Newcastle University, Newcastle upon Tyne, UK, 2. Institute of Neuroscience, Newcastle University, Newcastle upon Tyne, UK, 3. The London School of Hygiene & Tropical Medicine, London, UK, 4. Haydom Lutheran Hospital, Mbulu, Manyara, Tanzania, 5. Kilimanjaro Christian Medical Centre, Kilimanjaro, Tanzania, 6. Northumberland Tyne and Wear NHS Trust, Newcastle upon Tyne, UK
Introduction HIV-associated Neurocognitive Disorder (HAND) is a highly prevalent cause of HIV-related morbidity in Sub-Saharan Africa (SSA). Previous reliable studies on risk factors for the condition have only been conducted in high income countries (HIC). Furthermore, no studies conducted in SSA have focused on risk factors for HAND in older individuals, who make up an increasingly higher proportion of the HIV positive population. Method A cross-sectional observational study was conducted at an outpatient clinic in northern Tanzania. 254 patients aged 50 and over underwent a diagnostic assessment involving a neuropsychological test battery, measured against locally obtained normative data, psychiatric screens and neurological/medical examinations. A structured questionnaire and examination of clinic records were used to screen for potential risk factors. 27 patients were excluded from the final analyses due to certain confounding conditions that significantly affected cognition and prevented a diagnosis of HAND. Logistic regression analyses were carried out on the final sample of 227 patients to investigate correlations between symptomatic HAND and potential demographic, social and clinical risk factors. Results Preliminary results show 25.9% of patients were diagnosed with symptomatic HAND. Presence of symptomatic HAND was not related to clinical factors including but not exclusive to lower nadir or current CD4 counts, time since HIV diagnosis and differing antiretroviral regimens. Illiteracy, living alone and Geriatric Depression Scale (GDS) ≥5 were independently associated with a diagnosis of symptomatic HAND (p<0.05). Conclusions Clinical and treatment factors were not found to be risk factors, which differs from previous studies in HIC. In contrast, Illiteracy and living alone stood out as social risk factors in this setting and population subgroup. Social isolation represents a potentially modifiable risk factor. This risk factor profile also demonstrates similarities to Alzheimer’s disease, which has been previously suggested in other lines of research. Additionally, depressive symptoms were associated with a diagnosis of symptomatic HAND.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
49
Scientific Research: Eyes, ears and teeth ASSOCIATIONS BETWEEN POOR ORAL HEALTH AND INCIDENT FRAILTY: RESULTS FROM A POPULATION-BASED COHORT OF OLDER BRITISH MEN S E Ramsay1, E Papachristou2, O Papacosta2, L T Lennon2, P H Whincup3, S G Wannamethee2 1. Newcastle University, 2. UCL, 3. St George’s University of London
Introduction Studies demonstrating a link between poor oral health of older people and frailty are mostly cross-sectional or have limited oral health and frailty measures. We investigated the association of objective and subjective measures of oral health with frailty cross-sectionally and prospectively over a three-year follow-up period.
Methods The study comprises a socially and geographically representative sample of men aged 71-92 examined in 2010-12 across 24 British towns. Oral health measures included tooth count, periodontal disease, self-rated oral health, dry mouth symptoms, difficulty eating. Frailty was defined using the Fried phenotype (≥three of weight loss, grip strength, exhaustion, slowness, low physical activity). Incident frailty was based on self-reported frailty phenotype components from follow-up postal questionnaires in 2014.
Results Among 1622 men, 303 (19%) were frail at baseline (71-92 years). Having <21 teeth, edentulism, fair/poor self-rated oral health, difficulty eating, and dry mouth was associated with increased risks of being frail. Associations of edentulism, dry mouth and self-rated oral health remained significant on adjustment for age, smoking, social class, history of cardiovascular disease or diabetes, medications related to dry mouth and interleukin-6. Increasing number of oral health problems was also significantly associated with frailty on full adjustment. Among 1284 men followed-up for 3 years, 107 (10%) became frail. The risk of incident frailty was higher in participants with ≥three dry mouth symptoms (odds ratio (OR) =2.22, 95%CI 1.26-3.88), and in participants with one (OR=2.79, 95%CI 1.32-5.89), two (OR=2.81, 95%CI 1.26-6.26) or ≥three (OR=3.83, 95%CI 1.49-9.84) oral health problems in fully adjusted models.
Conclusions Poor oral health, particularly dry mouth and accumulation of oral health problems, were associated with increased risks of being frail, and of developing frailty in older age. Poor oral health needs to be identified and managed in frail older people and could be important in preventing frailty.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
50
Scientific Research – Falls, Fractures and Trauma DOES A MULTIFACTORIAL INTERVENTIONAL PROGRAMME ON FALLS PREVENTION IN OLDER FALLERS IMPROVE FRAILTY OUTCOMES? PRELIMINARY RESULTS FROM THE MALAYSIAN FALLS ASSESSMENT INTERVENTION TRIAL (MYFAIT) H M Khor1,2, P J Tan1, N I Saedon1,2, S B Kamaruzzaman1,2, M P Tan1, 2 1. Ageing and Age-Associated Disorders Research Group, Faculty of Medicine, University of Malaya, Malaysia. 2. Geriatric Division, Department of Medicine, Faculty of Medicine, University of Malaya, Malaysia
Introduction Falls and frailty are intertwined with many shared adverse risk factors such as reduced mobility, hospitalization and mortality. Interventional studies to modify frailty are mostly randomized studies focusing on exercise training and nutrition. We aim to investigate if the MyFAIT intervention programme could reduce frailty among older fallers.
Methods Elderly fallers who presented to outpatient clinics and the emergency department at University Malaya Medical Centre were recruited. One group received tailored multifactorial interventions targeting 6 specific risk factors whereas the comparison group received lifestyle advice with continued conventional care. Assessment for frailty was performed using a 42 variable multidimensional frailty index (MFI) based on deficit accumulation and the Fried’s phenotype criteria. All patients would be reassessed after 12 months.
Results Frailty measures were available at baseline and follow-up for 142 patients. The mean age of the participants was 74.4 years (standard deviation (SD) = 6.8 years) and 69.7% women. The intervention group showed significant improvement in their MFI (-0.04 , 95% CI: -0.06, -0.02; p<0.01) and Fried phenotype score (-0.32, 95%CI: -0.58, -0.54; p=0.02). The control group has also improved MFI (-0.05, 95% CI: -0.07, -0.02; p<0.01) at 12 months. There was a non-significant difference in improvement in frailty scores in between groups comparison with 2.8% (95% CI: -20.94%, -15.25%; p=0.76) reduction in frailty according to MFI score and 22.8% (95% CI: -51.2%, 5.6%; p=0.12) reduction with the FRIED phenotype criteria.
Conclusion The multidimensional frailty index in both groups improved with or without multifactorial falls prevention intervention. Further research into other targeted interventions is needed to evaluate the frailty syndrome among older fallers.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
51
Scientific Research – Falls, Fractures and Trauma
THE EFFECTS OF A TAILORED MULTIFACTORIAL INTERVENTION ON RATE OF FALL AND TIME-TO-FIRST FALL IN MALAYSIA
P J Tan1, E M Khoo2, K D Hill3, L MacKenzie4, S B Kamaruzzaman1, H M Khor1, N I Saedon1, M P Tan1
1. Ageing and Age-Associated Disorders Research, Faculty and Department of Medicine, University of Malaya, Kuala Lumpur, Malaysia, 2. Department of Primary Care Medicine, Department of Medicine, University Malaya Medical Centre, Kuala Lumpur, Malaysia, 3. School of Physiotherapy and Exercise Science, Faculty of Health Science, Curtin University, Perth, Australia, 4. School of Occupational Therapy, Faculty of Health Sciences, The University of Sydney, Sydney, Australia
Introduction While older adults globally fall over, studies on intervention have mainly been conducted in Caucasian populations in Europe, North American and Australasia. Our aim was to assess the effects of tailored multifactorial intervention on falls among urban community-dwelling older fallers.
Methods The Malaysian Falls Assessment and Intervention Trial (MyFAIT) was a pragmatic, single-blind randomized controlled trial. Community-dwelling adults aged 65 years or older with two or more falls or one injurious fall over 12 months were recruited. Participants were randomized to the intervention group to tailored multifactorial interventions including a modified Otago program, home hazards modification, cardiovascular intervention, visual intervention, medication review, fall education and footwear review. Participants randomized to the control group continued usual care. Primary outcomes were rate of fall and time-to-first fall recorded prospectively for 12 months using fall diaries with daily entries.
Results Our intention-to-treat analysis included 262 participants (IG=130, CG=132), mean age 75.3 years ±7.2 ,67% female. At least one fall occurred in 52% of participants at follow-up. There was no significant difference in rate of fall between intervention (155 falls, 1.22 falls per person ±1.8) and control (143 falls, 1.08 falls per person ±1.4) groups [Incidence Rate Ratio of 1.024 (95%CI 0.906-1.154), p=0.663]. Mean time-to-first fall was 169.8 days ±153.6. Cumulative hazard risk was also not significantly different between intervention (167.4 days ±148.2) and control (172.1 days, ±159.2 SD) groups [Hazard Risk Ratio of 0.931 (95%CI 0.664-1.305), p=0.678].
Conclusion Tailored multifactorial intervention had no significant effect on rate of fall and time-to-first fall. This may be a marker of the feasibility of conducting a multifactorial intervention among community-dwelling older adult fallers due to challenges in intervention adherence, staff compliance and the current infrastructure in Malaysia.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
52
Scientific Research – Health Services Research WHY DO OLDER PEOPLE PARTICIPATE IN INTENSIVE RESEARCH: A QUALITATIVE STUDY A M Baczynska1,2,3, S C Shaw4, H P Patel1,2,4, A A Sayer1,2,3,5,6, H C Roberts1,2,3 1. Academic Geriatric Medicine, University of Southampton, 2. NIHR Southampton Biomedical Research Centre, University Hospital Southampton NHS Foundation Trust, 3. NIHR CLAHRC: Wessex, University of Southampton 4. MRC Lifecourse Epidemiology Unit, University of Southampton, 5. Ageing, Geriatrics & Epidemiology, Institute of Neuroscience, Newcastle University, 6. NIHR Newcastle Biomedical Research Centre, Newcastle University and Newcastle-upon-Tyne NHS Foundation Trust
Introduction Participants of the Hertfordshire Sarcopenia Study, a birth cohort based intensive research study, fasted overnight and travelled several hours each way to the research facility for investigations to assess muscle mass and function including blood tests and a vastus lateralis muscle biopsy. The study has recruited 274 participants aged 76-84 years despite the intensity of the research procedures. We aimed to explore the motivating factors, barriers to participation and experience of the participants in order to identify key aspects which support recruitment of older people.
Methods We conducted semi-structured interviews with 13 participants (10 women) at a research facility at an English hospital in May-October 2015. The interviews were audio-taped, transcribed verbatim, coded and analysed thematically by three researchers. The analysis aimed to identify commonalities and differences among the participants and elicit a wide range of participants’ views and perspectives.
Results We identified personal motives for participation (potential health benefit for self and family; curiosity; comparing own fitness to others; socialising), but altruistic motives (benefit for other people; belief in importance of research) were also important. Participants voiced a number of external motives related to the study uniqueness, organisation and safety record; family support; and just ‘being asked’. Barriers to participation included anxiety about the biopsy and travel distance. Importantly, personal contact with researchers prior to consent, dedicated research staff, time and clinic space as well as efficient running of the study day increased participant satisfaction.
Conclusions Personal and altruistic reasons for participation were important motivators for these older people to participate in intensive research. Although they valued belonging to a unique birth cohort with previous research experience, personal contact with the research team before and after consent provided reassurance, aided recruitment to this intensive study and could be replicated by other researchers.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
53
Scientific Research – Health Services Research THE IMPACT OF TRAINED MEALTIME VOLUNTEER ASSISTANTS FOR OLDER IN-PATIENTS F F A Howson1-3, S Robinson4, C Cooper4, C Ballinger2, A A Sayer1-6, H C Roberts1-3 1. Academic Geriatric Medicine and 2. NIHR CLAHRC: Wessex, 3. University of Southampton; University Hospitals Southampton NHS Foundation Trust; 4. MRC Lifecourse Epidemiology Unit, University of Southampton; 5. Ageing Geriatrics & Epidemiology, Newcastle University; 6. NIHR Newcastle Biomedical Research Centre, Newcastle University and Newcastle-upon-Tyne NHS Foundation Trust
Introduction Poor nutrition among older people in hospital is common, expensive and associated with poor healthcare outcomes. Contributory factors widely recognised include acute illness, altered mealtime routines and also insufficient mealtime assistance from time-pressured staff. We have previously demonstrated that trained volunteers safely improved mealtime care in one ward. We aimed to evaluate the wider implementation of trained mealtime volunteers.
Methods Volunteers were trained to help patients aged ≥ 70 years in 11 wards across Medicine for Older People (MOP), Acute Medical Unit, Orthopaedics and Adult Medicine departments in one English hospital. In a mixed methods study the numbers of volunteers recruited, trained and their activity was recorded. Acceptability of the volunteer mealtime assistant programme was evaluated through interviews and focus groups with patients, ward staff and volunteers. The total cost of the programme was evaluated.
Results 65 volunteers helped at 846 weekday lunchtime and evening meals (median 8 mealtimes each volunteer, range 1-109) with typically 1-2 volunteers / ward / mealtime. 80% volunteers were female and a range of ages (17-76 years), ethnicity, working roles and previous experience were represented. The highest proportion of feeding assistance was in MOP: 56% of those helped, compared to 34-35% in other wards. Patients reported poor appetite but realised the importance of nutrition. Patients and nurses were positive about volunteer mealtime assistance, recognizing that they were good at encouraging reluctant eaters. Volunteers valued their training as did the patients. The volunteers released £17,200- £32,400 nursing time (based on band 3 to 5 pay scales) above the costs of their training.
Conclusions This is the largest study of trained mealtime volunteers. Volunteers of differing ages and experience were appreciated by patients and staff in all four departments and were very cost-effective. Training was essential and valued by staff and patients as well as volunteers.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
54
Scientific Research – Health Services Research CLINICAL OUTCOMES OF ACUTELY UNWELL PATIENTS WITH DEMENTIA AND IT RELATIONSHIP TO THE HOSPITAL DESIGN C Young1, C Edwards2, I Singh3 1. Medical student, School of Medicine, Cardiff University, Cardiff UK, 2. Consultant Clinical Scientist, Academic Dermatologist, Aneurin Bevan University Health Board, UK, 3. Consultant Geriatrician, Department of Geriatric Medicine, Ysbyty Ystrad Fawr, Aneurin Bevan University Health Board, Wales. UK
Introduction Hospitalisation is hazardous for frail older people and particularly for those with dementia. Dementia friendly environments have been proposed to promote patient well-being, mobility and engagement with staff/family; however, there has been little emphasis on hospital design. The objective of this study was to profile and compare the clinical outcomes of acutely unwell patients with dementia admitted to two different hospital environments.
Methods This prospective observation study was conducted for 100 acutely unwell dementia patients admitted at Ysbyty Ystrad Fawr (hospital with 100% single-rooms) and Royal Gwent Hospital (traditional multi-bedded wards - MBW) under the same University Health Board.
Results A total of 50 patients were observed at each hospital. There was no statistically significant difference in the mean age of patients admitted to single-rooms (83.4±8.4 years) or MBW (82.8±8.4 years, p=0.73), 60% were females. Most patients (73%, n=73/100) were admitted from their own homes, the demographic profile and clinical characteristics of the patients was similar in both hospitals. The mean Charlson co-morbidity index was similar (single-rooms = 5.0±1.4; MBW = 5.1±1.1). The reasons for acute admission varied widely, though falls were the most common reason for admission to both sites.The mean total length of stay (LoS) was significantly higher for patients discharged from single-rooms (62.23 ± 41.79 days) as compared to those from MBW (42.47±40.50 days, p=0.027).
Six patients experienced inpatient fall (IF) in each hospital site. There was no significant difference in the incidence of IF (single-rooms = 12, MBW = 8, p=0.175). There were no significant differences in the number of recurrent fallers (p=0.629). There was no significant difference in terms of falls-related injury, discharge to a new care home, 30-day readmission or mortality. Advancing age, presence of BPSD and admission to a single room were the only factors found to be associated with increased LoS (p= 0.007, 0.017, 0.027 respectively).
Conclusion The single room environment appears to influence LoS as previously being reported (Knight S, JCCG 2016, 7(3):87–92), but following the introduction of quality improvement initiatives to prevent inpatient falls (Singh I, BMJQuality.u210921.w4741), single-rooms do not appear to be associated with higher inpatient falls incidence. We propose more research to understand the relationship between single rooms and LoS.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
55
Scientific Research – Health Services Research AMBULATORY ACTIVITY OF OLDER INPATIENTS ON ACUTE GERIATRIC MEDICINE WARDS S E R Lim1,2,3, A Purkis3, G Strike3, M Baxter3, A Rogers2, A A Sayer1,2,3,4,5,H C Roberts1,2,3 1. Academic Geriatric Medicine and 2. NIHR CLAHRC: Wessex, University of Southampton, 3. University Hospital Southampton NHS Foundation Trust, 4. Ageing, Geriatrics & Epidemiology, Institute of Neuroscience, Newcastle University, 5. NIHR Newcastle Biomedical Research Centre in Ageing and Chronic Disease, Newcastle University and Newcastle upon Tyne NHS Foundation Trust
Introduction Accelerometers are often used to objectively measure physical activity in older people. We conducted a literature review which demonstrated few studies examining the ambulatory activity of hospitalised older people. We aimed to describe the pattern of ambulatory activity of older inpatients and evaluate the use of the StepWatch Activity Monitor (uniquely able to measure gait ≤ 0.4 metre/second) in this population.
Methods An observational cross-sectional study was conducted on the acute Geriatric Medicine wards of one hospital. Inclusion criteria were patients aged ≥70 years, able to mobilise prior to admission and to provide written consent. Ambulatory activity was measured using the ankle-worn StepWatch Activity Monitor (SAM) for ≤ 7 consecutive days, recording the total step count per 24-hour day. The accuracy of SAM was examined by comparing measured and observed step count over 40 metres.
Results 42 patients (mean age 87.5 years ± 4.6) had a median device wear time of 4 consecutive days (IQR 2-7 days) and median daily step count of 636 steps (IQR 298-1468 steps). Analysis demonstrated two peak periods of ambulatory activity, between 8am–12pm and 6pm–8pm. However, 33 patients (79%) were considerably mobile between 10pm and 6am, with a median step count of 94 steps (IQR 36 - 289 steps). A subgroup analysis of 13 patients (mean age 86.3 years, median gait speed 0.55metre/second) who completed the 40 metre walk demonstrated a mean absolute percentage error between the observed and SAM step count of 8.6% (SD 10.5). Bland-Altman analysis demonstrated good level of agreement between both measures (mean difference = -8.23 steps; CI -17.99 – 1.53).
Conclusions Ambulatory activity was very low in this patient group who walked slowly. Despite the slow gait speed the SAM was an accurate measure of ambulatory activity in these older acute medical inpatients. An understanding of the variation in daily activity levels can help researchers and clinicians implement time-specific interventions to address this important issue.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
56
Scientific Research – Neurology and Neurosciences CONNECTION IN THE CONTEXT OF ATYPICAL PARKINSONISM; A QUALITATIVE STUDY L Wiblin1, K Brittain2 1. Clinical Ageing Research Unit, Newcastle University, Newcastle upon Tyne, NE4 5NU, 2. Ageing & Health, Department of Nursing, Midwifery & Health, Northumbria University
Introduction Progressive Supranuclear Palsy and Multiple System Atrophy are atypical Parkinsonian (AP) disorders known to be relentlessly progressive, life-limiting conditions producing rapid disability and death when compared to Parkinson’s disease.
Methods The aim of this qualitative study was to explore the concerns of patients and their carers with PSP and MSA. Participants were purposively sampled from a larger clinical study considering quality of life and palliative care needs in MSA and PSP. This strategy was used to produce a range of sex, age and disease severity. There was no exclusion in terms of severity; participation using speech aids such as light-writers was encouraged to allow a rich breadth of experience.
Semi-structured interviews were carried out with a digital recording device. Interviews were carried out until saturation was reached. Interviews were transcribed verbatim. Thematic analysis was performed, aided by NVivo 11 (Braun and Clarke, 2006). 19 interviews took place with 9 patients (5 with MSA and 4 with PSP) and 10 carers.
Results Connection was a prevalent theme that emerged from analysis. Sub-themes included communication with peers and medical professions, speech difficulties, social-life and relationships, how information and education and how a sense of person can allow a continued sense of belonging. Two participants were anarthric yet could relay their experience using electronic devices.
Conclusions Previous work in AP has shown that patients and carers find a lack of knowledge and medical communication adds to uncertainty and distress (Moore and Guttman, 2014). Even minor speech dysfunction in PD has been linked to poorer QoL (Miller et al, 2011, Walshe and Miller 2011). Work in Parkinson’s disease has also shown the impact of disease on connection (Hudson et al, 2006). AP can have more profound effects on the ability to communicate. This work reinforces the need to strive for good communication and seeking to maintain means for patients and carers to remain connected, especially in conditions affecting speech.
References
1. Clarke Ba. Qualitative Research in Psychology, 2006:77-101. 2. Moore T, Guttman M. Movement disorders clinical practice 2014;1:188-93. 3. Miller N, Andrew S, Noble E, Walshe M. Disability and rehabilitation 2011;33:204-10. 4. Walshe M, Miller N. Disability and rehabilitation 2011;33:195-203. 5. Hudson PL, Toye C, Kristjanson LJ. Palliative medicine 2006;20:87-94.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
57
Scientific Research – Other Medical Conditions OPTIMISING BLOOD PRESSURE MEASUREMENT AND TREATMENT BEFORE ELECTIVE SURGERY. TAKING THE PRESSURE OFF A Hartle1, T McCormack2, J Carlisle3, S Anderson4, A Pichel5, N Beckett6, T Woodcock7, A Heagerty4 1. St Mary’s Hospital, London, 2. Whitby Group Practice, Whitby, 3. Torbay Hospital, Torquay, 4. University of Manchester, Manchester, 5. Manchester Royal Infirmary, Manchester, 6. Guys’ and St Thomas’ Hospital, London, 7. Hampshire, UK Introduction Uncertainty exists around the management of peri-operative blood pressure (BP). Postponement of planned surgical procedures due to elevated BP has been estimated at 100/day in the UK. The Association of Anaesthetists of Great Britain and Ireland and the British Hypertension Society recognised the need for a nationally agreed policy statement in regard to this.
Method A Working Party consisting of four members from each society (academics and clinicians with interests, including vascular anaesthesia, cardiology, geriatrics and general practice (GP)) was formed. The scope of the guideline was agreed and a systematic review carried out with the quality of evidence described using the Grading of Recommendations Assessment, Development and Evaluation approach. The Council and Executive of the respective societies gave final approval.
Results The main recommendations were;
1 GPs should refer patients for elective surgery with mean BPs in primary care (PC) in the past 12 months of less than 160/100mmHg
2 Secondary care should accept such referrals 3 Pre-operative assessment clinics need not measure the BP of such patients 4 GPs should refer hypertensive patients for elective surgery after BP readings are less than
160/100mmHg. 5 Surgeons should ask GPs for PC BP readings from the last 12 months if undocumented in the referral
letter. 6 Pre-operative assessment staff should measure the BP of patients who attend without evidence of
normotension in PC in the preceding 12 months. 7 Elective surgery should proceed for patients who attend the pre-operative assessment clinic without
documentation of normotension in PC if their BP is less than 180/110mmHg in clinic.
Conclusion These recommendations are meant to be practical. Most importantly, hospital departments should recognise that the presence of stage 1 and 2 hypertension has little impact on early outcomes after elective surgery and to determine care based on the measurements taken in PC.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
58
Scientific Research – Parkinson’s Disease DROOLING IN PARKINSON'S DISEASE: A CASE FOR DIVIDED ATTENTION H Reynolds1, N Miller2, R Walker3 1. Speech-Language Therapist, South Tyneside NHS Foundation Trust, Queen Elizabeth Hospital, Gateshead, 2. Professor of Motor Speech Disorders, Newcastle University and Honorary Speech-Language Therapist Newcastle Hospitals NHS Foundation Trust, 3. Consultant Physician, Northumbria Healthcare NHS Foundation Trust, North Tyneside General Hospital/ Honorary Professor of Ageing and International Health, Institute of Health and Society, Newcastle University
Introduction Drooling is a frequently reported non motor symptom in Parkinson’s Disease (PD) with significant psychosocial impact and negative health consequences including increased risk of aspiration. Drooling occurs due to reduced efficiency and variable frequency of saliva swallows, rather than hyper-salivation, compounded by poor posture and mouth opening. It is reported to occur most frequently during cognitively distracting concurrent tasks suggesting an impact from divided attention in a dual task situation. However, this supposition has not been systematically examined. This study assessed whether frequency of saliva swallows reduced, and drooling severity and frequency increased, when people with PD engaged in a distracting cognitively demanding task.
Methods 18 patients with idiopathic PD reporting daytime drooling on the Unified Parkinson’s Disease Rating Scale (UPDRS) were recruited. They completed the Radboud Oral Motor Inventory for PD saliva questionnaire and the Montreal Cognitive Assessment. UPDRS drooling score, disease stage, duration, gender and age were recorded. Swallow frequency and drooling severity and frequency were measured at rest and during a distracting computer based language task.
Results There was no significant difference between drooling severity at rest and during distraction (Wilcoxon signed rank test z=-1.724, p=.085). There was a significant difference between at rest and distraction conditions for both drooling frequency (Wilcoxon signed rank test z=-2.041, p=.041) and swallow frequency (Wilcoxon signed rank test z=-3.054, p=.002). Participants swallowed less frequently and drooled more frequently during the distraction task.
Conclusions The frequency of saliva swallows and drooling are affected by divided attention in a dual task paradigm. Further studies are needed to explore the exact role of attention in saliva management and the clinical applications in assessment and treatment.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
59
Scientific Research – Parkinson’s Disease MOTOR IMPAIRMENTS ARE ASSOCIATED WITH FEAR OF FALLING IN PEOPLE WITH PARKINSON’S DISEASE J Nell1, S Stuart1, B Galna1,2, L Alcock1, L Rochester1 1. Institute of Neuroscience/ Newcastle University Institute for Ageing, Newcastle University, NE4 5PL, UK, 2. School of Biomedical Sciences, Newcastle University, NE2 4HH, UK
Introduction Parkinson’s disease (PD) is a common, clinically heterogeneous, neurodegenerative disease, which is characterised by motor symptoms such as gait deficit. Motor and non-motor (e.g. visual and cognitive) dysfunctions are common in PD and lead to increased falls risk. Fear of falling (FoF) has been associated with increased falls prevalence in PD, and likely relates to motor and non-motor dysfunction. Understanding the features that underpin FoF will improve therapeutic management. The objective of this study was to quantify and interpret important contributors to FoF in PD.
Methods 70 participants with mild-to-moderate PD (Hoehn and Yahr Stage I:17, II:43, III:10) recruited from Movement Disorder Clinics in Newcastle upon Tyne were assessed for FoF using the Falls Efficacy Scale International (FES-I). Falls history was gained retrospectively over the 12-months prior to assessment. A range of demographic, clinical, visual, cognitive and gait outcomes were also obtained. The associations between FES-I and secondary outcomes were assessed using Spearman correlations, with variables demonstrating significance entered into multivariate regression models and Receiver Operating Characteristic (ROC) curves to determine significant predictors of FoF.
Results Motor symptoms of reduced gait speed (beta=-0.239, p=0.007), greater UPDRS II score (self-evaluation of motor experiences of Activities of Daily Living (ADL)) (beta=0.611, p<0.001), and a history of previous falls (beta=0.278, p=0.016) predicted FoF in PD. Notably, non-motor visual and cognitive deficits did not directly predict FoF in PD (F=0.692, p=0.678).
Conclusions Impaired gait speed, impaired ADL function and a history of falls are associated with FoF in people with mild-to-moderate PD. The complex causal interaction between FoF, motor symptoms and falls remains unclear. Speculatively, interventions that target motor symptoms may help reduce FoF.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
60
Scientific Research – Parkinson’s Disease OMISSION OF DOPAMINERGIC DRUGS IN HOSPITALIZED PARKINSON’S PATIENTS: A STUDY OF DRUG AVAILABILITY R Skelly, L Brown, S Gosrani, A Fogarty Royal Derby Hospital and University of Nottingham Introduction Omission of dopaminergic medication is common in hospitalized Parkinson’s patients and can lead to avoidable deterioration in motor function. This study aimed to determine how much medication is omitted because it is not available, and which medications were implicated.
Methods In a large district general hospital data were extracted for all admissions with a diagnosis of Parkinson’s Disease from 1st April 2012 to 31st March 2014. We then extracted medication data from the electronic drug prescription and administration system. We included all L-dopa preparations, ropinirole, pramipexole, rotigotine, pergolide, bromocriptine, selegiline and rasagiline.
Results There were 827 admissions among 472 patients. There were 34,168 scheduled doses of 36 different preparations of dopaminergic medication and 3322 (9.7%) doses omitted. 875 (26% of omitted doses, 2.6% of scheduled dopaminergic medication) were omitted because medication was not available. 351 (42.4%) hospitalizations and 257 (54.5.%) patients had at least 1 dose of medication not available. For L-dopa, dopamine agonists and MAOIBs: 581 (1.9%), 235 (8.1%) and 59 (7.7%) doses respectively were unavailable (Chi –squared test, p<0.001). For Stalevo, 30 (4.0%) doses were unavailable compared to 551 (1.9%) doses of other L-dopa preparations (p<0.001).
Conclusion This study confirms poor availability of dopaminergic medication to hospitalized PD patients: more than 50% of patients missed at least one dose as the drug was not available. Dopamine agonists, and MAOIBs are less readily available than L-dopa preparations. Among L-dopa preparations Stalevo (L-dopa, carbidopa and entacapone) is less readily available than co-careldopa and co-beneldopa. The variety of preparations used is large and wards cannot hold a complete stock. We recommend pharmacists ensure wards know where in the hospital to obtain PD medication. We recommend movement disorder specialist agree a substitution policy with pharmacy departments so suitable alternatives can be dispensed pending procurement of usual medication.
BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
61
Scientific Research – Parkinson’s Disease CAN PEOPLE WITH PARKINSON’S DISEASE EXERCISE AT HIGH INTENSITY, AND DOES THIS IMPROVE THEIR CARDIORESPIRATORY FUNCTION? A FEASIBILITY STUDY USING A STEPPED-WEDGE DESIGN M Harvey, W K Gray, K Weston, M McDonald, S Dodds, L Oates, R W Walker Northumbria Healthcare NHS Foundation Trust and Teesside University
Background Although there is a growing body of literature regarding the benefits of exercise for people with Parkinson’s disease (PD), there is little consensus on the relative merit of an particular type of exercise compared to another for this patient group. Most previous studies have used a combination of resistance and endurance exercises using conventional gym equipment.
Objective To assess whether people with PD are able to exercise at ≥85% of maximal heart rate during High Intensity Interval Training (HIIT) and whether this improved their cardiorespiratory function.
Design A stepped-wedge design was used.
Setting Participants were assessed at the Parkinson’s clinic, North Tyneside General Hospital. Exercise sessions took place at the Speedflex clinic, Jesmond, Newcastle-upon-Tyne.
Patients A total of 20 participants with Idiopathic Parkinson’s Disease (IPD) (Hoehn and Yahr stage 1-3) were randomly assigned to an immediate start or delayed start exercise group. Allocated was stratified by age and sex.
Intervention Each group performed three HIIT sessions per week for 12 weeks. Each session consisted of four-minute periods of HIIT designed to elicit ≥85% max heart rate and this was repeated four– six times per session. Sessions were designed to be progressive with regard to the intensity and duration of the exercise periods.
Main Outcome Measure: The primary outcome measures were a heart rate of ≥85% of predicted maximum and change in cardiorespiratory fitness (VO2max) from pre- to post-intervention.
Results The intervention group all achieved a heart rate of ≥85% of predicted maximum, with a significant increase across the intervention period (average 0.23% per week p=0.019) after adjusting for the influence of group allocation, age, sex and Hoehn and Yahr stage. There was a significant improvement in VO2max (p = 0.041) from pre- to post-intervention and notable improvements in cognition and distance walked in 6 minutes, which did not reach significance. There was no obvious trend in changes to quality of life or cardiac output.
Discussion Patients with PD can exercise at ≥85% of maximal predicted heart rate. Mean peak heart rate and cardiorespiratory fitness improved across the intervention period. Such exercise programmes should be considered for people with PD and the relative merits of this form of exercise evaluated against more conventional programmes.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
62
Scientific Research – Psychiatry and Mental Health PREDICTORS OF COGNITIVE DECLINE IN RURAL TANZANIA J Heward1, L Stone1, C Dotchin2, R Walker2, S-M Paddick2, K Gray2, J Kissima2 1. Faculty of Medical Sciences, Newcastle University 2. Northumbria Healthcare NHS Foundation Trust
Introduction Cognitive decline (CD) represents a spectrum of deficits ranging from normal cognitive aging to dementia, which has a significant financial and psychosocial burden worldwide. Due to a demographic transition, the incidence of dementia in sub-Saharan Africa (SSA) is set to rise significantly. This study aimed to identify predictors of CD in the Hai District, Tanzania, which could enable early CD identification and intervention, in order to reduce its burden.
Method A cohort of 417 over-65s in the rural Hai District was recruited for a 2014 study that validated an educationally unbiased dementia screening tool (SIDSA). In 2016, 329 subjects were re-screened using the SIDSA and further assessed for potential predictors of CD, functional status measured using Instrumental Activities of Daily Living (IADLs) and potential confounders including depression and sensory impairment. Any significance of association between potential predictors and CD, defined based on functional status and change in SIDSA score since 2014, was assessed using chi-squared testing and logistic regression.
Results Approximately one-quarter of subjects underwent CD between 2014 and 2016. Independent predictors of CD (p<0.05) were older age (Odds Ratio (OR) = 3.897, 95% Confidence Interval (CI) = 1.663, 9.131), retirement (OR = 2.864, 95% CI = 1.468, 5.584), lower grip strength (OR = 0.939, 95% CI = 0.889, 0.993), lower educational attainment (OR = 0.860, 95% CI = 0.767, 0.966) and, surprisingly, having no past history of stroke (OR = 10.023, 95% CI = 1.261, 79.648).
Conclusion This study reveals some predictors that could be used to identify target groups for future early interventions for CD, including grip strength, which may represent a potential cheap and simple tool for identification of those at risk of CD. The significant association between having no past history of stroke and CD could be an artifact of inaccurate self-reporting of medical history in this setting.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
63
Scientific Research – Epidemiology [PLATFORM PRESENTATION]
HYPOALBUMINAEMIA PREDICTS IMPORTANT CLINICAL OUTCOMES IN OLDER UNSELECTED ACUTE SURGICAL ADMISSIONS: AN INTERNATIONAL MULTICENTRE STUDY A Ablett1, J Goeteyn2, L Evans3, J Law4, S Owen3, J Hewitt3, P K Myint1: On Behalf Of Older Persons Surgical Outcome Collaboration 1. University of Aberdeen, 2. University Hospital Ghent, 3. Cardiff University, 4. Manchester Royal Infirmary
Introduction Hypoalbuminaemia is known to be associated with mortality in hospitalised patients. However, the association between low albumin and outcome in older people (≥ 65 years) admitted to the acute surgical setting is not clearly understood.
Methods Our international cohort was drawn from the Older Persons Surgical Outcomes Collaboration (www.OPSOC.eu) (2013-2015). The effect of having hypoalbuminaemia (defined as albumin ≤35g/L) on outcomes of receipt of emergency surgical intervention, 30- and 90-day mortality, readmission within 30-days and hospital length of stay were examined using multivariate logistic regression models, adjusting for age, sex, polypharmacy, haemoglobin for the outcome of the receipt of surgical intervention and additionally controlling for surgical intervention for other outcomes. We then examined the association by additionally adjusting for frailty using the clinical frailty scale.
Results N=1084 patients from six surgical units (mean age (SD) = 76.8(8.1) years) from England, Scotland, Wales and Belgium were included. 568 (49.7%) had hypoalbuminaemia. The emergency operation rate was 16.2% (N=185). Characteristic comparisons between those with hypoalbuminaemia at the time of admission and those without showed increasing age, low haemoglobin levels, length of hospital stay and frailty were all significantly associated with having hypoalbuminaemia. Meanwhile, hypoalbuminaemia was not associated with sex, polypharmacy or receiving surgical intervention. Multivariate logistic analyses showed hypoalbuminaemia was associated with both 30-day (adjusted odds ratio (aOR)=2.43 (95%CI:1.25-4.74; P =0.009) and 90-day mortality (aOR 2.39 (1.47-3.88; P <0.001), increased length of hospital stay (aOR 1.02 (1.01-1.04; P = 0.001). No significant association was found between hypoalbuminaemia and all other selected outcomes.
Conclusion Hypoalbuminaemia is a risk factor associated with poor 30- and 90-day mortality and length of stay outcome in older surgical patients aged 65 years or over. Further investigations are required to better understand this relationship to help develop strategies to improve these important outcomes in older surgical patients.

BGS Spring Meeting 2017, Newcastle, 26 – 28 April 2017
64
Scientific Research – Health Services Research [PLATFORM PRESENTATION]
URGENT CARE AXIS FOR THE OLDER ADULT: WHERE IS BEST TO TARGET AN INTERVENTION? J G Bunn1, C O’Keeffe1, R Jacques1, S Croft1, S Conroy2, S Mason1 1. School of Health and Related Research, University of Sheffield, Sheffield, S1 4DA, 2. Department of Health Sciences, 22-28 Princess Road West, Leicester, LE1 6TP
Background The urgent care axis is the pathway of the patient from community, through the emergency department (ED) to admission or discharge from hospital. An ageing population has resulted in more older patients presenting to EDs, but there is a dearth of evidence addressing the effectiveness of interventions to manage this group of patients. We explored the current axis across EDs in Yorkshire and Humber (Y&H) for patients ≥75 years, to identify where interventions could be most effectively targeted.
Methods Routine hospital data (RHD) for ED attendances across 18 EDs in Y&H from 2014 were retrospectively analysed. Mode and time of arrival to the ED, length of ED stay, diagnosis, ED outcome and length of inpatient stay were analysed for all patients, dichotomised to ≥75 years and <75 years. Binary logistic regression was performed for categorical variables comparing old and young, with non-parametric analysis for continuous data. Descriptive analysis was undertaken for patients admitted for ≤48 hours; a cohort in whom an alternative management strategy may be more appropriate. Rates and length of admission across Y&H were analysed, as were the frequency of admissions with conditions that can potentially be managed without inpatient stay, conditions previously defined in the literature.
Results There were 1,312,534 ED attendances across Y&H, 224,810 (17.1%) were ≥75 years. Older patients were significantly more likely to attend the ED via ambulance services than the younger cohort (OR 6.68, 95% CI 6.61-6.75, p<0.001), and once within the department had a significantly longer stay (p<0.001) and rate of admission (OR 4.92, CI 4.88-4.97, p<0.001). Across Y&H 118.343 (52.6%) of older adults were admitted, but rates varied across the region from 16.3% to 64.2%, as did proportions admitted for ≤48 hours (26.5% to 54.8%). 16.9% of older adult admissions were with conditions that met criteria for potentially avoidable admissions: varying across Y&H from 15.3% to 19.1%. Discussion Despite current interventions large numbers of older adults are presenting to EDs mainly by ambulance, with many consequentially being admitted. Significant proportions are admitted for short periods with avoidable conditions that might be safely managed outside inpatient stay; representing a cohort who could be amenable to future intervention. Variation across the region in management of this cohort warrants further study.

published by British Geriatrics Society
Marjory Warren House31 St John’s SquareLONDON EC1M 4DN
Tel: + 44(0) 207 608 1369Email: [email protected]: www.bgs.org.uk





























