Embed Size (px)
Citation preview

Accelerating Spread of Community-Based Strategies to Reduce Maternal, Newborn
and Child Health Challenges in Ghanaby
Nana A. Y. Twum-Danso, MD, MPHDirector, Project Fives Alive!
Institute for Healthcare Improvement
5th Annual International Conference of the African Science Academy Development Initiative
La Palm Royal Beach Hotel, Accra, GhanaNovember 10-11, 2009

Presentation Outline
• Background
• Successful Community-Based Strategies
• Summary

BACKGROUND
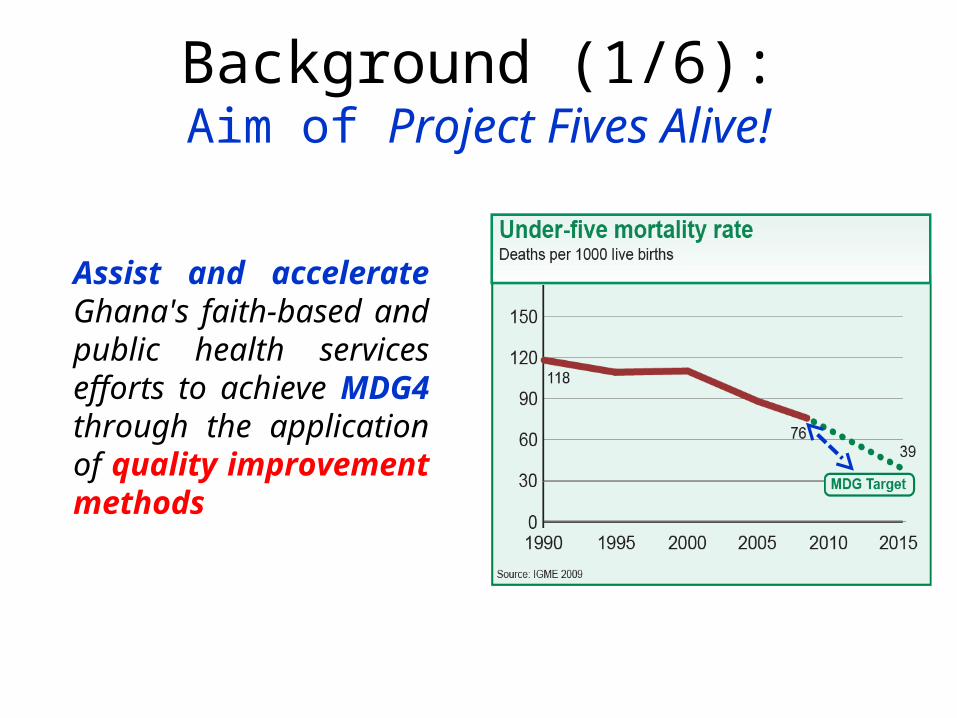
Background (1/6):Aim of Project Fives Alive!
Assist and accelerate Ghana's faith-based and public health services efforts to achieve MDG4 through the application of quality improvement methods

Community Level1. Low/no risk awareness, prevention & management
2. Low valuation of women & children’s lives
3. Lack of financial means and/or health insurance
4. Distance from health services
5. Unattractive health services (staff attitudes, cultural incompatibility etc.)
Background (2/6):Drivers of Under-5 Deaths in Ghana
Health Facility Level1. Lack of patient-centeredness in design of health services
2. Irregular and/or inappropriate preventive care
3. Late and/or inappropriate therapeutic care
4. Unreliable referral system from clinics to hospitals
5. Inequity in health services provision
6. Unreliable generation & movement of health information

Resources
Knowledge & Training
Systems Approach
Background (3/6):Enablers of Under-5 Survival in Ghana

Background (4/6):QI Strategies - The Model for Improvement
What are we trying toaccomplish?
How will we know that achange is an improvement?
What change can we make thatwill result in improvement?
Model for Improvement
PlanAct
DoStudy
Source: Associates for Process Improvement
• Method of continuous quality improvement
• Provides a framework work for developing and testing change ideas, learning and re-design
• Emphasizes small changes that are non-threatening and non-disruptive
• Relies on input and ideas from frontline providers

Background (5/6):QI Strategies – Improvement Collaborative Network
Assessment and Design
Period
Learning Session 1
© Institute for Healthcare Improvement
Learning Session 2
ACTIVITY PERIOD
Repeated improvement
cycles:
Learning Session 3
12 -24 months
Intensive support from project staff & DHMT
ACTIVITY PERIOD
Repeated improvement
cycles:
Improvement Collaborative NetworkHealth Facilities
Start Small, Accelerate Learning & Scale-up Rapidly
Wave 1 26 clinics & 2 hospitals from 4 districts/dioceses
Jul’08 to present

• Care Pathway
Background (6/6):Focus of QI Work

SELECTION OF SUCCESSFUL STRATEGIES

Antenatal Care:Activate CBVs to identify pregnant women in community early,
provide health education, refer to clinic for ANC, midwife follows-up
NHI free for maternity & early infant care; small scale testing of pregnancy registers
NHI free for maternity & early infant care; small scale testing of pregnancy registers

Skilled Delivery:Engage TBAs to accompany labouring women to health facility; TBA can stay and serve as delivery companion

Skilled Delivery:Engage chiefs & elders on risks of labour and delivery &
enlist their help in promoting skilled delivery

Skilled Delivery:Video show in community on risks of unskilled delivery
followed by Q&A session and health promotion

Skilled Delivery:Mobile telephone contact between labouring women and
health staff for transport or domiciliary midwifery

Postnatal Care:Home visits by health staff on Day 1 or 2 for neonates born
at home and home visits on Day 6 or 7 for all neonates

Postnatal Care:Home visits by CBVs on Day 4 to screen for danger signs and remind mothers to follow up at health center on Day 6 or 7

• Data were collected on each change idea tested• 6 to 12 months of baseline data and at least 6 months of post-
intervention data• Used time-series analysis to determine successful change ideas.• Developed strict criteria for determining successful change ideas:
Change Package:Development of a change package for scale up
Score Definition
0No evidence or suggestions of improvement
1Suggestions of improvement but not enough time to meet test of evidence
2
Evidence of improvement but not sustained OR not enough time to assess sustainability
3Evidence of improvement which has been sustained

• Change Package
Scaling Up Change Package
Sept’09 to Jun’11
Wave 2~300 QI teams from
38 districts
SUMMARY

• Local knowledge, innovation and testing of changes at the community level can reduce delay in seeking care for MNCH
• Local generation and use of data key to:– Frontline health provider empowerment to develop and test
changes iteratively for continuous improvement– Improving data quality from primary sources
• Processes across care continuum can be accelerated with Improvement Collaborative Network model through:– peer-to- peer learning– deliberate spreading of successful change ideas/best practices
• Change package can facilitate spread of local successes or best practices on a large scale to achieve higher coverage and improved health outcomes in non-innovation sites
Summary

Can the achievement of MDG4 in Ghana be further accelerated?
We believe we can!

Acknowledgements
• Team– George B. Akanlu– Isaac A. Amenga-Etego
– Ireneous N. Dasoberi– Solomon A. Atinbire– Phoebe Bala– Francisca Bagna– Chrysanthus Kubio– James Tobiga– Pierre M. Barker
• Institutions– Ghana Health Service– National Catholic Health
Service– Institute for Healthcare
Improvement– Bill & Melinda Gates
Foundation