Embed Size (px)
Citation preview

CentralBringing Excellence in Open Access
Archives of Paediatrics and Developmental Pathology
Cite this article: Sanz-Mengibar JM, Santonja-Medina F (2017) Correlation between Sagittal Spinal Curves and Gross Motor Function in Children with Typical Development and With Spastic Bilateral Cerebral Palsy. Pilot Study. Arch Paediatr Dev Pathol 1(2): 1009.
*Corresponding authorJose Manuel Sanz-Mengibar, UK and Clinica de Rehabilitacion, 113 Gauden Road, SW4 6LE, UK, Tel: 447726764081; Email:
Submitted: 11 May 2017
Accepted: 08 June 2017
Published: 11 June 2017
Copyright© 2017 Sanz-Mengibar et al.
OPEN ACCESS
Keywords•Cerebral palsy•Gross motor function•GMFCS•Locomotor stages•Lumbar spine•Thoracic spine
Research Article
Correlation between Sagittal Spinal Curves and Gross Motor Function in Children with Typical Development and With Spastic Bilateral Cerebral Palsy. Pilot StudyJose Manuel Sanz-Mengibar1* and Fernando Santonja-Medina2
1UK and Clinica de Rehabilitacion, UK2Department of Traumatology, University of Murcia and V. de la Arrixaca University Hospital, Spain
Abstract
Purpose: To understand the role of gross motor function and sagittal spinal curves in subjects with typical development (TD) and those with Cerebral Palsy.
Method: Inclinometer measurements during Sit a Reach test from 76 TD children, and 55 with CP were plotted with their gross motor level: Thoracic kyphosis (SR Thoracic kyphosis), lumbar curve (SR Lumbar curve) and Lumbo-horizontal angle (L-H fx).
Results: LS correlates only with SR thoracic kyphosis in both groups (0.498; p<0.001) and this curve does not depend on the age (DT -0.271; p<0.001 and CP 0.306; p<0.01). In children with TD, L-H fx correlates with age (0.553; p<0.001) and not with LS (0.2556; p<0.001).
Conclusions: SR Thoracic and lumbar curves explain locomotor skills in children with TD, while pelvic flexion is related to age. In children with CP, only SR Thoracic curve is related to the locomotor stage while the lumbar spine and pelvis adapt atypically.
INTRODUCTIONStudies on the measurement of the ontogenic development of
the spine in the sagittal plane of babies and toddlers with TD are limited. Prenatal and neonatal measurement of the spinal curves [1,2] are subject to variability due to the body positioning. Supine position offers limited access to the spine, while resting head and limb position is difficult to obtained in prone. On the other hand, sagittal spinal curve vary dynamically within a range during the execution of a selective motor patter [3], and would require to be accessible at any age or developmental stage. In order to be able to compare within groups, also static measurements should be standardized to be easily accessible. On top of that, measurements should be sensible to curves changes and maybe specific to different variables like age or gross motor level. Inclinometer quantification provide good validity, reliability and correlation with radiographic measurements [4], and measurements in maximal flexion like the Sit and Reach test (SR) expose the spine deficits in older children [5]. When looking for a standardized paediatric tool for spine measurement, it can be observed that the assessment of the muscle tone includes passive movements of the distal segment, while the trunk remains stable in a lying
position. Some examples of these tests are the Popliteal Angle test [6], the Scarf Sign [7], and the Heel to Ear test [8]. The Duncan-Ely test [9,10] rates the shortening of the ventral biarticular muscles observing the compensatory movement of the pelvis in relation to the stabilized thigh. The Thomas test [11,12] can be interpreted as the reversed Duncan-Ely test, where distal movement is assessed in relation to the pelvis. Some of these static and standardized measurements assess the sagittal curves of the spine when the limbs are stabilized in specific positions. The quantification with an inclinometer of the sagittal spinal curves in trunk flexion during SR [5,13] shows similar kinematic features to the Popliteal Angle test, [14,15] but it focuses on the measurement of the proximal segment (spine).
On the other hand, the relationship between spinal curves on the sagittal plane during gait and gross motor function in children with cerebral palsy (CP) has been previously studied [3]. It is widely accepted that gross motor and locomotor function are limited to a combination of compensatory movements coming from lower limb alterations and postural control deficits [16]. Measuring the impact of distal patterns of movement on proximal segments including the spine is technically complex

CentralBringing Excellence in Open Access
Sanz-Mengibar et al. (2017)Email:
Arch Paediatr Dev Pathol 1(2): 1009 (2017) 2/6
during dynamic activities other than walking and therefore there is limited data on the sagittal spinal curves in children with lower gross motor function levels [3]. Research on the relationship between other functional maturation stages of the Central Nervous System and spinal curves has not been found. The quantification of sagittal curves is useful to understand the normative values of a healthy spine in teenagers and adults, and has helped to report postural adaptation to different factors like intense sport training [17-19]. Adaptations due to lack of spine flexibility in children with CP in comparison with children with typical development (TD) from age five have also been described [20].
GOALTo understand the normative values of the spinal curves in
the sagittal plane of babies and toddlers, as well as to understand the relationship between gross motor function and these curves in children with TD and those with CP.
METHODSParticipants
Children with bilateral spastic CP and their siblings and volunteers with TD were recruited from two early intervention centres, four rehabilitation centres and two schools in Spain, United Kingdom, Italy and Germany. Data from children at risk of neurological impartment, but CP diagnosis was possible due to young age, were stored separately and add to the final database only when their condition was confirmed. Inclusion criteria were confirmed diagnosis of bilateral spastic CP and under 18 years of age. Consent was obtained by their legal representatives for the use of data for scientific purposes.
Children with an unclear medical diagnosis or associated spine orthopaedic conditions were excluded. 55 children with CP and 76 children with TD were included in the study. Some of the children with TD were reassessed more than once during their gross motor development until a total of 100 measurements were achieved. This may help us to understand how age or functional maturation impact on the spine of the same subject. TD children were between 2 weeks and 11 years old, with and average of 2,75 years of age. CP children were between 2 and a half months and eighteen years old, with an average of 6’3 years of age. Sample features and age groups according to Gross Motor Function Classification System (GMFCS) can be observed in Table 1.
Measurements
The extensibility of the posterior muscle chain of the lower limbs was assessed with the SR test [5,13-15] in centimetres, performing a maximal trunk flexion with the children sitting on the plinth with their knees and arms extended. The distance between the fingertips and the heel was measured with a ruler on the plinth. Measurements taken beyond the heel were considered as positive values.
In order to rate the maximal flexion of the pelvis, the Lumbo-horizontal angle in flexion (L-H fx) [21-23] was measured with a goniometer. L-H fx is the anterior angle between the horizontal line and the lumbosacral spine. branches of the goniometer were
aligned with the horizontal line and the spinous processes of L5 to S2.
While the children were in maximal flexion, measures of the sagittal curves of the thoracic and lumbar spine were also performed. In order to quantify the thoracic and lumbar curves, an inclinometer was placed at the beginning of the curve at T1-T2, T12-L1 and L5-S1 [5]. The assessment of thoracic and lumbar curve in flexion with an inclinometer (ISOMED, Inc., Pórtland, OR) provides good validity, reliability and correlation with radiographic measurements [4]. Not all the tests that describe the sagittal curves of the spine [5,19], can be performed in babies and children with neurological disorders, due to their inability to stand independently.
GMFCS [24], currently considered to be the gold standard in children with CP, was used to classify the gross motor function. In order to be able to assess and also to compare with children with TD, Locomotor Stages (LS) [25,26] were also used. “GMFCS level 0” was used for healthy children. We have previously shown good reliability of these classification systems in CP, as well as high correlation coefficients between them [27]. In independent walkers, the duration in months of experience using this pattern was also noted.
Statistical analyses
Statistical analyses were performed using the STATA, 12.0 y SPSS, 15.0 software packages for Windows. We examined the strength of the association between gross motor function level and the sagittal spinal curves using Spearman rank correlation. Correlation coefficient r ≥ 0.8 is considered a “high” correlation, r = 0.6 – 0.8 indicates a “good” correlation, r = 0.4 – 0.6 is considered a “moderate” correlation and r ≤ 0.4 indicates a “poor” correlation [28].
The association of capability to understand gross motor function level according to the spinal curves was investigated using Ordinary Least Squares (OLS), taking into account the ordinal nature of the dependent variables for the use of this regression model (GMFCS and LS).
RESULTSNo statistically significant differences in gross motor
function level (according to LS) or the time being able to walk independently were found between both groups of children. Age differences between the group of children with CP and those with TD were significant, but with a poor correlation coefficient (0.383, p<0.001). Statistically significant differences of the sagittal plane measurements among both groups of children, gross motor functional levels and ages, are shown in Table 2.
Children with typical development
Normative values of the sagittal spinal curves and pelvis flexion during SR test in children between zero and nine years old are shown in Table 3. In Table 4, the impact of gross motor function and age in the sagittal plane measurements can be observed; however, there was poor correlation between Thoracic kyphosis in SR and age, as well as between L-H fx and gross motor function. Figure 1 shows how thoracic kyphosis in SR increases during TD, while lumbar kyphosis in SR test is reduced over time,

CentralBringing Excellence in Open Access
Sanz-Mengibar et al. (2017)Email:
Arch Paediatr Dev Pathol 1(2): 1009 (2017) 3/6
Table 1: Sample distribution. LS= “Locomotor Stage”.
Typical development n=100 Bilateral cerebral palsy n= 55
GMFCS I II III IV V
n= 14 11 10 10 10
LS 0 1 2 3 4 5 6 7 8 9 LS 0 1 2 3 4 5 6 7 8 9
n= 13 5 11 3 - 2 6 18 8 34 n= 6 4 2 2 4 2 15 12 5 3
Table 2: Overall correlations n=155(* p<0.01, ** p<0.001, *** p<0.0001).
Cerebral palsy vs Typical Development GMFCS Locomotor
Stages Corrected ageMonths of
Independent walking
Sit and Reach
L-H fx 0.415** 0.421** 0.13 0.567** 0.345**
SR (cm) -0.268** -0.334** -0.232** -0.654** -0.514**
Thoracic kyphosis 0.214** 0.164* 0.498** 0.426** 0.389**
Lumbar curve -0.139 -0.142 -0.317** -0.306** -0.171*
CP= Children with Cerebral palsy TD=Children with typical development
Figure 1 Typical developments of the thoracical and lumbar curvesin Sit and Reach Test.
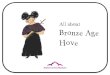
Figure 2 Sit and Reach test(cm).Typical development of the hamstrings extensibility (A) and according to the functional development in children with cerebral palsy (B and C).
until the age of nine months, when values remain more or less stable until the age of 12 years.
Children with spastic bilateral cp
Correlation between gross motor function and sagittal spinal curves can be observed in Table 5. There is no clear relationship between sagittal plane measurements and GMFCS. Thoracic kyphosis in SR was correlated to LS, but only poor correlation with GMFCS can be observed.
Significant regressions were found in many sagittal curves measurements according to their gross motor function or age (Supplemental digital content Tables), supporting the correlation tendencies in both groups of children. Figure 2 illustrates the development of hamstring extensibility over time in children with TD according to DDP, and how this varies in relation to the gross motor level achieved for children with CP (similar for both GMFCS and LS).
DISCUSSIONThe age at emergence of gross motor milestones has
remained remarkably similar over 20 years in children with TD [29]. In our current sample of children with TD there are no subjects older than 12, however the normative values from that age have been previously described in other studies by these

CentralBringing Excellence in Open Access
Sanz-Mengibar et al. (2017)Email:
Arch Paediatr Dev Pathol 1(2): 1009 (2017) 4/6
Table 3: Average normative data.
Sit and Reach
Lumbo Horizontal angle in flexion Sit and Reach (cm) Thoracic kyphosis Lumbar curve
1 to 3 months 95.3º (SD 10.9) 13.6 (SD 4.0) 44.9º (SD 7.2) 44.7º (SD 10.2)
3 to 6 months 86.4º (SD 13.8) 14.3 (SD 2.1) 45.25º (SD 18.2) 38.3º (SD 21.6)
6 to 9 months 80.8º (SD 4.7) 14.5 (SD 4.3) 48.0º (SD 15.2) 23.0º (SD 9.0)
9 to 12 months 76.4º (SD 5.8) 17.1 (SD 3.6) 55.0º (SD 7.0) 17.8º (SD 8.8)
12 to 15 months 82.4º (SD 6.0) 16.4 (SD 1.9) 60.8º (SD 9.3) 19.0º (SD 14.9)
15 to 24 months 79.7º (SD 5.3) 15.9 (SD 2.7) 55.3º (SD 22.7) 22.8º (SD 22.7)
2-4 years 88.8º (SD 6.5) 12.2 (SD 4.1) 63.5º (SD 11.5) 19.0º (SD 10.8)
4-6 years 97.3º (SD 11.7) 6.2 (SD 5.4) 63.3º (SD 10.3) 27.7º (SD 13.0)
6-12 years 106.7º (SD 9.2) -2.85 (SD 5.3) 77.2º (10.5) 19.4º (SD 9.2)
12-18 years14 ˂100° ≥ (-2cm) 40°-65° 10°-30°
Table 4: Correlations of the sagittal spinal curves in children with typical development assessed with Locomotor Stages (* p<0.01, ** p<0.001, *** p<0.0001).
Locomotor stages Corrected age Months of independent walking
Sit and Reach
Lumbo Horizontal angle in flexion 0.2556 0.553** 0.593**
Si and Reach (cm) -0.5001* 0.592** -0.813**
Thoracic kyphosis 0.5656* -0.271** 0.559**
Lumbar curve -0.4215* 0.424** -0.216*
Table 5: Correlations of the sagittal spinal curves in children with cerebral palsy assessed with GMFCS and Locomotor Stages (* p<0.01, ** p<0.001, *** p<0.0001) (* p<0.01, ** p<0.001, *** p<0.0001)
GMFCS GMFCS-age locomotor Stages Corrected age Months of walking
Sit and Reach
Lumbo-horizontal angle in Flexion 0.0598 0.2438 0.0943 0.416** 0.204
Sit and Reach (cm) -0.0797 -0.3530* -0.065 0.621** -0.382**
Thoracic kyphosis -0.3342* -0.1134 0.4668* -0.306* 0.241
Lumbar curve 0.0492 -0.2308 -0.1402 -0.094 -0.135
Figure 3 Measurement of the spinal curves during Sit and Reach test with a goniometer.
authors in our previous trials [13]. Pelvic flexion in SR test is reduced progressively over time from birth until age 2, whilst the distance between fingertips and heels in the SR test increases in this period at the expense of thoracic kyphosis flexion and possibly limb growth.
Gross motor function according to GMFCS is not related with any sagittal plane measurements at any developmental age.
However, a tendency to correlate with the thoracic kyphosis during SR test can be observed (previously shown with LS as well), but disappears when plotting this curve with a variable that combines the GFMCS level and the age group. This supports the correlation between SR Thoracic kyphosis and independent gross motor function without support from any environmental factors (assessed with LS), and not by activity or participation components (GMFCS) [27,30], or age.
SR test assesses hamstring extensibility. As equinus foot deformity is often observed in children with CP, we had to modify this test by measuring the distance between the fingertips and the heels without using the SR box [5,13,14]. The distance between the fingertips and the heels was defined by age in both groups. However, in children with TD this measurement also depended on the LS level, probably because age and locomotor function develop simultaneously.
L-H fx rates the maximal flexion of the pelvis, which is dependent on hamstring extensibility. Significant differences in measurements between children with CP and those with TD were found in our sample. L-H fx values were not related to

CentralBringing Excellence in Open Access
Sanz-Mengibar et al. (2017)Email:
Arch Paediatr Dev Pathol 1(2): 1009 (2017) 5/6
locomotor function. They were also distributed differently over time between both groups of children, as shown in Figure 2. In children with TD, L-H fx correlates positively with the amount of time they have been walking independently (0.553; p<0.001), and with age (0.593; p<0.001). This means that the degree of pelvic flexion is reduced over time during TD and from LS=7. Independent walking is therefore an important locomotor pattern within the gross motor milestones in TD for hamstring extensibility, however it does not play the same role in children with CP. Likewise, Lumbar curve during SR test is related to the LS and age in children with TD (LS -0.421; p<0.001), but not in children with CP. Age will therefore impact differently on the spine of children with CP depending on whether the ability to walk independently is available or not.
The thoracic kyphosis during SR test has specific values according to LS, regardless of the child’s development (TD or CP). In TD, Thoracic kyphosis during SR test increases as age and LS develop. In children with CP, thoracic kyphosis during SR test is poorly correlated with age, probably because improvement in LS are observed at different ages depending on the neurological injury. This means that Thoracic kyphosis during SR tests may be a predictor of locomotor function in both groups of children. According to our data, the greater the flexion in this curve, the higher the LS.
By adapting to reach maximum locomotor function, the child with CP develops a pathological gait pattern that compromises primary, secondary and compensatory characteristics [31]. The requirement of a thoracic spine posture in order to perform a specific locomotion could explain the postural adaptations at lumbar level in children with CP in comparison with those with TD [32]. Pelvic and hip orthopaedic deformities frequently associated in children with CP [33], could be explained by the lumbar spine compensatory curve. We proofed in previous research that there is a specific postural control in the basal and maintenance of lumbar spine in the sagittal plane during gait, for the transition among GMFCS I-III levels [27]. Higher classifications of gross motor skills correlate with more extended lumbar spine and in children with CP who cannot walk independently, the effect of development is reversed, flexing the trunk in relation to the pelvis [3] (Figure 3).
This is also supported by the fact that the ability to walk impacts on the lumbar curve during SR test, and reduces the probability of the appearance of these deformities. Trunk control in sitting is correlated with parameters related to anterior-posterior movements during gait [34-36]. We also found spine position on the sagittal plane during SR test as an important factor for locomotor function, however, it would be interesting to measure transversal and frontal plane in future research.
Results of therapeutic interventions in children with CP should be quantified according to functional improvement [37]. Without postural measurements, qualitative improvement can only be deduced from other aspects such as gait speed, functional independence or acquisition of new skills. Trials finding “non significant differences” that failed to assess quality of movement may have missed important changes in this underlying component of motor skill [38]. Incorporating postural improvements of the
spine towards normative values may provide a more reliable assessment of functional improvement.
The sample size of children in the CP group was smaller that in the TD group and this is therefore a study limitation. Both groups, however, were homogenous. It is unlikely that the main findings in the study were as a result of chance, as indicated by the low p values. However, the data should be interpreted with caution due to a limited sample for every age group. The descriptive and regression values of children with CP cannot be used clinically because a larger sample of functional level in combination with age groups is required; nevertheless, our pilot results showed significant correlation. This study provides normative data of spinal curves at an early age and to our knowledge, no other research on this description of babies and toddlers has been found. These measurements on the sagittal plane during SR test allow clinicians and researchers to assess children at any age or gross motor level.
CONCLUSIONSThoracic and lumbar curves during SR test explain locomotor
skills in children with TD, while pelvic flexion is related to age. In children with CP, only thoracic curve during SR test is related to the locomotor stage while the lumbar spine and pelvis adapt atypically. Lumbar compensation may be useful in assessing the ability to walk independently over time
ACKNOWLEDGMENTSWe would like to thank all the children, parents, and
professionals who collaborated on this research, Mr. Alberto Gobbicchi and Dr. Thein Win for proof reading.
REFERENCES1. Mangione P, Gomez D, Senegas J. Study of the course of the incidence
angle during growth. Eur Spine J. 1997; 6: 163-167.
2. Choufani E, Jouve JL, Pomero V, Adalian P, Chaumoitre K, Panuel M. Lumbosacral lordosis in fetal spine: genetic or mechanic parameter. Eur Spine J. 2009; 18: 1342-1348.
3. Sanz-Mengibar JM, Altschuck N, Sanchez-de-Muniain P, Bauer C, Santonja-Medina F. Position between trunk and pelvis during gait depending on the gross motor function classification system. Pediatr Phys Ther. 2016.
4. Saur PM, Ensink FM, Frese K, Seeger D, Hildebrandt J. Lumbar range of motion: reliability and validity of the inclinometer technique in the clinical measurement of trunk flexibility. Spine. 1996; 21: 1332-1338.
5. Santonja F. Las desviaciones sagitales del raquis y su relación con la práctica deportiva. In: Ferrer V, Martínez L, Santonja F. Escolar, Medicina y Deporte. Albacete: Diputación Provincial, 1996; 251-268.
6. Steele K, Damiano D, Eek M, Unger M, Delp S. Characteristics associated with improved knee extension after strength training for individuals with cerebral palsy and crouch gait. J Pediatr Rehabil Med. 2012; 5: 99-106.
7. Dubowitz LMS, Dubowitz V, Goldberg C. Clinical assessment of gestational age in the newborn infant. J Pediatr. 1970; 77: 1-10.
8. Allen MC, Capute AJ. Tone and Reflex Development before Term. Pediatrics. 1990; 85: 393-399.
9. Lee SY, Sung KH, Chung CY, Lee KM, Kwon SS, Kim TG, et al. Reliability and validity of the Duncan-Ely test for assessing rectus femoris

CentralBringing Excellence in Open Access
Sanz-Mengibar et al. (2017)Email:
Arch Paediatr Dev Pathol 1(2): 1009 (2017) 6/6
spasticity in patients with cerebral palsy. Dev Med Child Neurol. 2015; 57: 963-968.
10. Marks MC, Alexander J, Sutherland DH, Chambers HG. Clinical utility of the Duncan-Ely test for rectus femoris dysfunction during the swing phase of gait. Dev Med Child Neurol. 2003; 45: 763-768.
11. Szopa A, Domagalska–Szopa M, Kidoń Z, Syczewska M. Quadriceps femoris spasticity in children with cerebral palsy: measurement with the pendulum test and relationship with gait abnormalities. J Neuroeng Rehabil. 2014; 11: 166.
12. Hislop H. Daniels and Worthingham’s muscle testing: Techniques of Manual Examination. 8th ed. Philadelphia, PA: Saunders; 2007.
13. Santonja F, Ferrer V, Andújar P. Síndrome de los isquiosurales cortos. In: Arribas JM, Castelló JR, Rodríguez N, Santonja F. Cirugía Menor y procedimientos en Medicina de Familia. 2nd ed. Madrid: Jarpyo editors; 2006; 1563-1572.
14. Ayala F, Sainz de Baranda P, De Ste Croix M, Santonja, F. Reproducibility and criterion-related validity of the sit and reach test and toe touch test for estimating hamstring flexibility in recreationally active young adults. Phys Ther Sport. 2012; 13: 219-226.
15. Ayala F, Sainz de Baranda P, Cejudo A, Santonja F. Pruebas angulares de estimación de la flexibilidad isquiosural: descripción de los procedimientos exploratorios y valores de referencia. Rev Andal Med Deporte. 2013; 6: 120-128.
16. Heyrman L, Hilde F, Molenaers G, Jaspers E, Monari D, Nieuwenhuys A, Desloovere K. Altered trunk movements during gait in children with spastic diplegia: Compensatiory or underlying trunk control deficit? Res Dev Disabil. 2014; 35: 2044-2052.
17. Sanz-Mengibar JM, Sainz-de-Baranda P, Santonja-Medina F. Training intensity and sagittal curvature of the spine in male and female artistic gymnasts. J Sports Med Phys Fitness. 2017.
18. López-Miñarro PA, Rodríguez PL, Santonja FM. Posture of the thoracic spine during latissimus dorsi pulldown behind the neck position exercise in recreational weight lifters. Gaz Med Ital. 2009; 168: 347-352.
19. Sainz de Baranda P, Santonja Medina F, Rodríguez-Iniesta M. Tiempo de entrenamiento y plano sagital del raquis en gimnastas de trampolín. Rev Int Med Cienc Act Fis Dep. 2010; 10: 521-536.
20. Abdulwahab SS. Spinal flexibility and physical disability status in patients with cerebral palsy. Acta Orthop Traumatol Turc. 1996; 30: 425-427.
21. Santonja F, Andújar P, Martínez I. Ángulo lumbo-horizontal y valoración de repercusiones del Síndrome de Isquiosurales Cortos. Apunts Med Esport. 1994; 31: 103-111.
22. Santonja F, Pastor A. Cortedad isquiosural y actitud cifótica lumbar. Caso clínico. Selección. 2003; 12: 151-156.
23. Santonja F, Genovés JL. Radiología. Consideraciones en Ortopedia. In: Santonja F, Martínez I. Valoración Médico-Deportiva del Escolar. Murcia: Universidad de Murcia 1992; 279-302.
24. Jooyeon K, Ji-Hea W, Jin-Gang H. The Reliability and Concurrent Validity of the GMFCS for Children with Cerebral Palsy. J Phys Ther
Sci. 2011; 23: 255-258.
25. Schulz P, Vojta V, Ernst WK. Follow up in 577 children with different infantile cerebral palsy syndromes treated by reflex locomotion according to Vojta. In: B.V. Taguchi K, Igarashi M, Mori S: Elsevier Science editors. Vestibular and neural front. Proceedings of the 12th International Symposium on Posture and Gait. Japan. 1994; 219-222.
26. Maurer-Burkhard B, Smoor I, Von Reumont A, Deckstein G, Stierle I, Rupp R, et al. Validity and reliability of a locomotor stage-based functional rating scale in spinal cord injury. Spinal Cord. 2016; 54: 619-625.
27. Sanz Mengibar JM, Santonja-Medina F, Sanchez-de-Muniain P, Canteras-Jordana M. Can Clinical Assessment of Locomotive Body Function Explain Gross Motor Environmental Performance in Cerebral Palsy? J Child Neurol 2016; 31: 474-480.
28. Jooyeon K, Ji-Hea W, Jin-Gang H. The Reliability and Concurrent Validity of the GMFCS for Children with Cerebral Palsy. J Phys Ther Sci. 2011; 23: 255-258.
29. Darrah J, Bartlett D, O Maguire T, Avison WR, Lacaze-Masmonteil T. Have infant gross motor abilities changed in 20 years? A re-evaluation of the Alberta Infant Motor Scale normative values. Dev Med Child Neurol. 2014; 56: 877-881.
30. World Health Organization. International classification of functioning, disability and health (ICF). Geneva, Switzerland. 2001.
31. Heyrman L, Hilde F, Molenaers G, Jaspers E, Monari D, Nieuwenhuys A, et al. Altered trunk movements during gait in children with spastic diplegia: Compensatiory or underlying trunk control deficit? Research in Developmental Disabilities. 2014; 35: 2044-2052.
32. Prosser LA, CK Lee S, Barbe MF, VanSant AF, Lauer RT. Trunk and hip muscle activity in early walkers with and without cerebral palsy-a frequency analysis. J Electromyogr Kinesiol. 2010; 20: 851-859.
33. Hägglund G, Lauge-Pedersen H, Wagner P. Characteristics of children with hip displacement in cerebral palsy. BMC Musculoskelet Disord. 2007; 26: 101.
34. Sæther Rannei, Helbostad Jorunn, Adde Lars, Brændvik Siri, Lydersen Stian, Vik Torstein. The relationship between trunk control in sitting and during gait in children and adolescents with cerebral palsy. Dev Med Child Neurol. 2015; 57: 344-350.
35. Winter DA. Human balance and posture control during standing and walking. Gait Posture. 1995; 3: 193-214.
36. Wolf SI, Mikut R, Kranzl A, Dreher T. Which functional impairments are the main contributors to pelvic anterior pelvic during gait in individuals with cerebral palsy? Gait and Posture. 2014; 39: 359-364.
37. Tedroff K, Löwing K, Åström E. A prospective cohort study investigating gross motor function, pain, and health-related quality of life 17 years after selective dorsal rhizotomy in cerebral palsy. Dev Med Child Neurol. 2015; 57: 484-490.
38. Wright FV, Rosenbaum P, Fehlings D, Mesterman R, Breuer U, Kim M. The Quality Function Measure: reliability and discriminant validity of a new measure of quality of gross motor movement in ambulatory children with cerebral palsy. Dev Med Child Neurol. 2014; 56: 770-778.
Sanz-Mengibar JM, Santonja-Medina F (2017) Correlation between Sagittal Spinal Curves and Gross Motor Function in Children with Typical Development and With Spastic Bilateral Cerebral Palsy. Pilot Study. Arch Paediatr Dev Pathol 1(2): 1009.
Cite this article