Embed Size (px)
Citation preview

1
ACROMEGALY IS ASSOCIATED WITH INCREASED CANCER RISK: A SURVEY IN ITALY. 1
Massimo Terzolo1, Giuseppe Reimondo
1, Paola Berchialla
2, Emanuele Ferrante
3, Elena Malchiodi
3, Laura 2
De Marinis4, Rosario Pivonello5, Silvia Grottoli6, Marco Losa7, Salvatore Cannavo8, Diego Ferone9, Marcella 3
Montini10, Marta Bondanelli
11, Ernesto De Menis
12, Chiara Martini
13, Efisio Puxeddu
14, Antonino Velardo
15, 4
Alessandro Peri16, Marco Faustini-Fustini17, Patrizia Tita18, Francesca Pigliaru19, Giulia Peraga1, Giorgio 5
Borretta20, Carla Scaroni21, Nicoletta Bazzoni22, Antonio Bianchi4, Alessandro Berton6, Andreea Liliana 6
Serban3, Roberto Baldelli
23, Letizia Maria Fatti
24, Annamaria Colao
5, and Maura Arosio
3 for the Italian 7
Study Group of Acromegaly* 8
9
1Internal Medicine 1, Department of Clinical and Biological Sciences, University of Turin, San Luigi 10
Gonzaga Hospital, Orbassano, Italy; 2Statistical Unit, Department of Clinical and Biological Sciences, 11
University of Turin, San Luigi Gonzaga, Hospital, Orbassano, Italy; 3Endocrinology and Diabetology Unit, 12
Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Department of Clinical Sciences and 13
Community Health, University of Milan, Milan, Italy; 4Pituitary Unit, Department of Endocrinology, 14
Catholic University of the Sacred Heart, Rome, Italy; 5Division of Endocrinology, Department of Clinical 15
Medicine and Surgery, University Federico II di Napoli, Naples, Italy; 6Division of Endocrinology, Diabetes 16
and Metabolism, Department of Medical Science, University of Turin, ASOU Città della Salute e della 17
Scienza, Turin, Italy; 7Pituitary Unit, Department of Neurosurgery, San Raffaele Scientific Institute, 18
University ‘Vita- Salute’, Milan, Italy; 8Department of Clinical and Experimental Medicine-Endocrinology 19
Unit, University of Messina, Messina, Italy; 9Endocrinology Unit, Department of Internal Medicine & 20
Medical Specialties (DiMI), Center of Excellence for Biomedical Research (CEBR) IRCCS, AOU San 21
Martino-IST, San Martino Hospital, University of Genova, Genova, Italy; 10Ambulatori di Endocrinologia, 22
Humanitas Gavazzeni, Bergamo, Italy; 11Section of Endocrinology and Internal Medicine, Department of 23
Medical Sciences, University of Ferrara, Ferrara, Italy; 12Internal Medicine, San Valentino Hospital, 24
Montebelluna, Treviso, Italy; 13Internal Medicine, Department of Medicine, DIMED, University of Padova, 25
Padova, Italy; 14Department of Medicine, Section of Internal Medicine and Endocrine and Metabolic 26
Sciences, University of Perugia, Perugia, Italy; 15Department of Internal Medicine, Section of Endocrinology 27
Page 1 of 29 Accepted Preprint first posted on 14 July 2017 as Manuscript ERC-16-0553
Copyright © 2017 by the Society for Endocrinology.

2
and Metabolism, University of Modena, Modena, Italy; 16Endocrine Unit, Department of Experimental and 28
Clinical Biomedical Sciences "Mario Serio", University of Florence, Florence, Italy; 17IRCCS Istituto delle 29
Scienze Neurologiche di Bologna (ISNB), Bologna, Italy; 18Endocrinology, AO Garibaldi-Nesima, Catania, 30
Italy; 19Endocrinology and Diabetes, Department of Medical Sciences, University of Cagliari, Cagliari, Italy; 31
20Division of Endocrinology and Metabolism, Santa Croce and Carle Hospital, Cuneo, Italy; 21Endocrinology 32
Unit, Department of Medicine , DIMED University of Padua, Padua, Italy; 22Endocrinology, Sant’Antonio 33
Abate Hospital, Gallarate, Varese, Italy; 23Endocrinology Unit, Regina Elena National Cancer Institute, 34
Rome, Italy; 24Division of Endocrine and Metabolic Diseases, San Luca Hospital, IRCCS Istituto 35
Auxologico Italiano, Milan, Italy. 36
37
Italian Study Group of Acromegaly* 38
Participating centres: 39
1. Department of Clincal Sciences and Community Health, University of Milan, Unit of Endocrine Diseases 40
and Diabetology, ‘S. Giuseppe’ Hospital, Multimedica Group, Arosio M, Montefusco L. 41
2. Internal Medicine 1, Department of Clinical and Biological Sciences, University of Turin, San Luigi 42
Gonzaga Hospital, Orbassano, Italy, Angeli A, Terzolo M, Reimondo G, Zaggia B, Peraga G. 43
3. Department of Clinical Sciences and Community Health, University of Milan, Unit of Endocrinology and 44
Diabetes, Fondazione IRCCS Ca` Granda Ospedale Maggiore Policlinico, Spada A, Ferrante E, Malchiodi 45
E, Ronchi CL, Serban AL 46
4. Department of Molecular and Clinical Endocrinology and Oncology, University of Naples, Lombardi G, 47
Colao A, Pivonello R. 48
5. Department of Medicine, University of Padua, Sicolo N, Martini C, Maffei P. 49
6. Department of Internal Medicine, Section of Endocrinology and Metabolism, University of Modena, 50
Velardo A. 51
7. Department of Medicine and Pharmacology, University of Messina, Trimarchi F, Cannavo` S. 52
8. Unit of Internal Medicine, S. Valentino Hospital, Montebelluna (Treviso) De Menis E. 53
Page 2 of 29
3
9. Pituitary Unit, Pituitary Unit, Department of Endocrinology, Catholic University of the Sacred Heart, 54
Rome, Italy, De Marinis L, Bianchi A, Cimino V. 55
10.Section of Endocrinology and Internal Medicine Department of Medical Sciences, University of Ferrara, 56
Italy Degli Uberti EC, Ambrosio MR, Bondanelli M. 57
11. Division of Endocrinology, Ospedali Riuniti di Bergamo, Pagani G, Montini M, Attanasio R. 58
12. Department of Internal Medicine, Endocrine Unit, Bellaria Hospital, Bologna, Faustini-Fustini M, Kara E 59
13. Endocrine Unit, Department of Experimental and Clinical Biomedical Sciences "Mario Serio", 60
University of Florence, Florence Mannelli M, Peri A. 61
14. Endocrinology Unit, Department of Medicine DIMED, University Hospital of Padova, Padova, Padova, 62
Italy. Mantero F, Scaroni C, Ceccato F. 63
15. Pituitary Unit, Department of Neurosurgery, San Raffaele Scientific Institute, Universita` Vita-Salute, 64
Milan, Mortini P, Losa M. 65
16. Division of Endocrinology and Metabolism, S. Croce and Carle Hospital, Cuneo, Borretta G, Razzore P. 66
17. Department of Internal Medicine and Endocrine Sciences, University of Perugia, Angeletti G, Della 67
Torre D, Puxeddu E. 68
18. Endocrinology and Diabetes, Department of Medical Sciences, University of Cagliari, Mariotti S, 69
Pigliaru F. 70
19. Division of Endocrinology, Diabetology and Metabolism, Department of Internal Medicine, University 71
of Turin, Ghigo E, Grottoli S, Berton A 72
AOU Città della Salute e della Scienza di Torino, Dipartimento di Scienze Mediche, Università di Torino 73
20. Endocrinology Unit, S. Antonio Abate Hospital, Gallarate, Milan, Mainini AL, Bazzoni N. ( opp UO di 74
Endocrinologia, ospedale Sant’Antonio Abate, Gallarate) 75
21. Endocrinology Unit, Regina Elena National Cancer Institute, Rome, Appetecchia M, Baldelli R. 76
22. Endocrinology, Department of Internal and Specialistic Medicine, University of Catania, Garibaldi- 77
Nesina Hospital, Catania, Vigneri R, Tita P. 78
Page 3 of 29

4
23. Endocrinology Unit. Department of Internal Medicine & Medical Specialties (DiMI), Center of 79
Excellence for Biomedical Research (CEBR) IRCCS, AOU San Martino-IST , S Martino Hospital, 80
University of Genova, Genova Minuto F, Nazzari E, Ferone D 81
24. Division of Endocrinology and Metabolic Diseases, IRCCS San Luca Hospital, Istituto Auxologico 82
Italiano, University of Milan, Cavagnini F , Fatti L, Persani L 83
84
Short Title: Cancer risk in acromegaly 85
Keywords: Acromegaly, cancer, GH, IGF-I 86
Word count: 3476 87
88
Correspondig author 89
Giuseppe Reimondo, MD, PhD 90
Internal Medicine 1 - Department of Clinical and Biological Sciences, University of Turin, San Luigi 91
Gonzaga Hospital 92
Regione Gonzole 10 - 10043 Orbassano (TO), Italy 93
Phone: +39 0119026292 94
Fax: +39 0116705456 95
e-mail: [email protected] 96
97
98
99
100
Page 4 of 29
5
ABSTRACT 101
It is debated if acromegalic patients have an increased risk to develop malignancies. 102
The aim of the present study was to assess the standardized incidence ratios (SIRs) of different types of 103
cancer in acromegaly on a large series of acromegalic patients managed in the somatostatin analogs era. 104
It was evaluated the incidence of cancer in an Italian nationwide multicenter cohort study of 1512 105
acromegalic patients, 624 men and 888 women, mean age at diagnosis 45 +/- 13 years, followed–up for a 106
mean of 10 years (12573 person-years) in respect to the general Italian population. 107
Cancer was diagnosed at 124 patients, 72 women and 52 men. The SIRs for all cancers was significantly 108
increased compared to the general Italian population (expected: 88, SIR 1.41; 95%CI, 1.18-1.68, p<0.001). 109
In the whole series, we found a significantly increased incidence of colorectal cancer (SIR 1.67; 95% 110
CI,1.07-2.58, p=0.022), kidney cancer (SIR 2.87; 95% CI 1.55-5.34, p<0.001) and thyroid cancer (SIR 3.99; 111
95% CI, 2.32-6.87, p<0.001). The exclusion of 11 cancers occurring before diagnosis of acromegaly (all in 112
women) did not change remarkably the study outcome. In multivariate analysis, the factors significantly 113
associated with an increased risk of malignancy were age and family history of cancer, with a non-significant 114
trend for the estimated duration of acromegaly before diagnosis. 115
In conclusion we found evidence that acromegaly in Italy is associated with a moderate increase in cancer 116
risk. 117
118
Page 5 of 29

6
INTRODUCTION 119
120
Acromegaly is an uncommon disease sustained by hypersecretion of GH and IGF-I and is associated with 121
remarkable complications that may reduce life expectancy of these patients (Melmed 2009, Katznelson et al. 122
2014). However, the effective control of GH and IGF-I excess is able to reduce considerably the burden of 123
disease. Recent population-based studies have showed that acromegalic patients have lower standard 124
mortality ratios than previously reported (Sherlock et al. 2010), reflecting improved treatment modalities that 125
became available in recent years, such as somatostatin-receptor ligands (SRL) and pegvisomant (Bogazzi et 126
al. 2013, Biermasz 2014, Mercado et al. 2014) The impact of acromegaly on life expectancy comes mainly 127
through cardiovascular and cerebrovascular events, since diabetes mellitus and hypertension are frequent 128
complications of GH and IGF-I excess (Melmed 2001) Recently, we did a large-scale epidemiological 129
analysis on 1512 acromegalic Italian patients and found that vascular disease and cancer were the main 130
causes of death. Mortality was higher in patients with persistently active disease, and IGF-I levels at 131
diagnosis, GH at the last follow-up, cancer, and pituitary radiotherapy were independent predictors of 132
mortality (Arosio et al. 2012). 133
That acromegaly may cause cancer, and that mortality due to cancer contributes to shorten survival of 134
patients with acromegaly, remains an unsolved issue (Melmed 2001, Loeper & Ezzat 2008, Boguszewski & 135
Ayuk 2016). A wealth of preclinical data supports the view that the GH-IGF system plays an important role 136
in cancer development and progression (Loeper & Ezzat 2008, Pollak 2008, Weroha & Haluska 2012, 137
Brahmkhatri et al. 2015). Moreover, in human studies there is convincing evidence that circulating IGF-I 138
concentrations at the higher limit of the normal range are linked with an increased risk of several types of 139
cancers, although the excess risk seems moderate (Renehan et al. 2004, Clayton et al. 2011). Despite a sound 140
rationale, studies that addressed the association between acromegaly and cancer produced controversial 141
results, partly due to the different methodological approaches used (case-control and population-based 142
design) (Loeper & Ezzat 2008, Ayuk & Boguszewski 2016). Moreover, it is plainly evident that most studies 143
did not have the statistical power to demonstrate a moderate excess risk of cancer, as expected from the 144
outcome of studies in the general population and case-control studies on acromegaly (Figure 1). 145
Page 6 of 29

7
A recent meta-analysis of case-control studies employing colonoscopy showed that acromegaly is associated 146
with an increased risk of colon neoplasms, both colon adenomas, a premalignant condition that may lead to 147
overt cancer, and colon cancers. Results were consistent among the different studies with no significant 148
heterogeneity and showed an overall excess risk of about two times (Rokkas et al. 2008). Another meta-149
analysis of case-control studies focusing on thyroid cancer showed an increased risk of both nodular thyroid 150
disease and thyroid cancer in acromegaly, and again results were quite homogeneous across studies, although 151
with less precise estimate due to the low number of events (Wolinski et al. 2014). 152
Population-based studies addressing cancer incidence in acromegaly produced controversial findings that 153
may be likely explained by difference in methodology and variable sample size (Table 1). Also population-154
based studies addressing whether cancer mortality may contribute to overall mortality of acromegaly came to 155
mixed conclusions, with some studies showing an association while others did not (Table 2). However, it has 156
been already argued that studies focusing on mortality are less helpful in answering the question whether 157
acromegaly is associated with cancer because the prevalent cardiovascular mortality may have obscured 158
cancer mortality. In the reported series, the median age at death was less than 60 years, thus most patients 159
died before they could develop clinically evident cancer (Loeper & Ezzat 2008, Boguszewski & Ayuk 2016). 160
The aim of the present study was to assess the standardized incidence ratios (SIRs) of different types of 161
cancer in acromegaly in a nationwide multicenter cohort study in Italy on a large series of acromegalic 162
patients who have been treated in the SRL era. 163
164
165
MATERIALS AND METHODS 166
Subjects 167
We have evaluated the prevalence of neoplasia from an Italian series of 1512 patients who were proactively 168
followed in 24 tertiary referral centers in Italy. Patient characteristics are given in Table 3. Inclusion criteria 169
were age at diagnosis >18 years and diagnosis of acromegaly made between 1 January 1980 and 31 170
December 2002 according to standard biochemical criteria at the time of enrollment, with at least 1-year 171
follow-up after diagnosis. The mean follow-up time from diagnosis to the end of the study was 120 months 172
(median: 90 months; interquartile range [IQR]: 42–170 months). Follow-up was closed at the end of 2012. 173
Page 7 of 29
8
Data were collected retrospectively by local investigators in a computerized dataform developed using 174
Access 2000 software (Microsoft Corporation 1999) and approved by all participants. All patients gave their 175
informed consent to the collection of data according to the local ethic committee indications. Briefly, we 176
collected for each patients: demographics, estimated date of appearance of typical acromegalic signs, GH 177
and IGF-I levels at diagnosis and last follow-up, novel diagnosis of malignancies during follow-up, data on 178
family history of cancer, smoking, drinking, participation in oncology screening programs. For further details 179
on data capture and assessment see Arosio et al. (Arosio et al. 2012). 180
181
Statistical analysis 182
Cancer registrations were coded using the International Classification of Diseases ICD-9, and data were 183
compared to the general Italian population using the cancer registry AIRTUM (Associazione Italiana Registri 184
Tumori, www.registri-tumori.it). The expected number of cancers was calculated by multiplying the number 185
of person-years by the appropriate national, gender-, age-, calendar year-, and site-specific cancer incidence 186
rate for each five-year age group and calendar year of observation. Risks of cancer were estimated by 187
computing the SIRs, defined as the observed to expected number of cancers for all acromegaly patients 188
combined, and by gender, age, and years of follow-up. The 95% confidence intervals (CI) were computed 189
assuming that the observed number follows a Poisson distribution (Liddell 1984). 190
Descriptive statistics were worked out. Continuous data were presented as medians and interquartile ranges, 191
or means and standard deviations. Discrete data are given as counts and percentages. Chi-square test was 192
performed to compare categorical data between groups and the Mann-Whitney U test was used to compare 193
continuous data. Levels of significance were set at p<0.05. 194
The individual effect of patient and clinical variables on the risk of cancer was evaluated by a logistic 195
regression model and a univariate estimate of the Odds Ratios (OR) were presented along with their 95% 196
confidence intervals (CI). A multivariable model was then considered. Variables were entered into the model 197
following a variable selection strategy, which was based on clinical judgement and statistical selection 198
procedures. Model fit was considered as significantly improved on the basis of the Akaike Information 199
Criterion (AIC) applied backwards for each model (i.e. starting from a model with all relevant variables, 200
Page 8 of 29

9
eliminating those that were not significant), at a significance level of 0.05. Interactions among variables were 201
assessed by the Wald’s test. 202
Page 9 of 29

10
203
RESULTS 204
205
Cancer incidence 206
We found 124 patients with diagnosis of cancer in our study cohort of 1512 acromegalic followed-up for a 207
mean period of 10 years (12573 person-years). Fourteen patients had multiple cancers. Eleven subject 208
registrations occurred before the date of diagnosis of acromegaly (8 breast, 2 colorectal, 1 uterus cancers) but 209
were included in the analysis, since diagnosis of cancer preceded that of acromegaly of less than 5 years, 210
which is within the time lag occurring between onset and clinical diagnosis of acromegaly in our cohort 211
(Arosio et al. 2012). Raw data of observed malignancies are given in supplemental table 1. In a separate 212
analysis, we restricted SIR calculation to the malignancies observed only after the clinical diagnosis of 213
acromegaly. 214
Overall, SIR for all cancers was increased compared to the general Italian population (SIR 1.41; 95%CI, 215
1.18-1.68, p<0.001). In the whole series, we found a significantly increased incidence of colorectal cancer 216
(SIR 1.67; 95% CI, 1.07-2.58, p=0.022), kidney cancer (SIR 2.87; 95% CI 1.55-5.34, p<0.001) and thyroid 217
cancer (SIR 3.99; 95% CI, 2.32-6.87, p<0.001). We assessed the SIRs of different cancer types in the female 218
and male gender, respectively (Table 4). In female patients, incidence of all malignancies was increased (SIR 219
1.51; 95% CI, 1.20-1.91, p<0.001), as it was incidence of thyroid cancer, colorectal cancer, and breast 220
cancer. In male patients, incidence of all malignancies was increased (SIR 1.29; 95% CI, 1.0-1.7, p=0.06), as 221
it was incidence of thyroid cancer, kidney cancer, and colorectal cancer. 222
The analysis of the malignancies observed only after the clinical diagnosis of acromegaly confirmed an 223
increased SIR for all cancer in the overall population (SIR 1.28; 95%CI, 1.07-1.55, p=0.007). All the 224
prevalent malignancies were observed in female patients; however, the incidence of all malignancies was 225
still increased (SIR 1.28; 95%CI, 1.00-1.65, p<0.05) while the incidence of breast cancer (SIR 0.83; 95% CI, 226
0.50-1.41, p=NS) and colorectal cancer (SIR 1.55; 95% CI, 0.84-2.89, p=NS) were not different from the 227
general female population. 228
A comparable number of patients with or without cancer were submitted to proactive oncologic screening as 229
part of their management (65% in patients with cancer vs. 60% in patients without cancer). 230
Page 10 of 29
11
Predictive factors of cancer were analyzed in univariate analysis (age, gender, duration of acromegaly before 231
diagnosis, presence of diabetes, active disease at last follow-up, GH/IGF-I at baseline and last follow-up, 232
pituitary radiotherapy, family history of cancer). Factors significantly associated with an increased risk of 233
cancer were age, family history of cancer, disease duration before diagnosis, presence of diabetes and 234
previous pituitary radiotherapy. Pertinently, we observed only 3 cases of brain cancer. In multivariable 235
analysis, factors significantly associated with an increased risk of cancer were age and family history of 236
cancer, while there was a non-significant trend for duration of acromegaly (Table 5). 237
Page 11 of 29
12
238
DISCUSSION 239
240
Whether acromegaly is associated with increased risk of cancer remains an endless debate. In general, case-241
control studies focusing on a specific tumor type produced more homogeneous figures, as demonstrated by a 242
meta-analysis of colonoscopy-based studies (Rokkas et al. 2008). Since case-control studies may lead to 243
overestimation of risk due to ascertainment bias and problems related to matching with specific patient 244
groups, the “well-worried” bias, it has been suggested that population-based studies are more appropriate for 245
assessing cancer risk (Renehan & Brennan 2008). 246
However, population-based studies produced discrepant data for a number of reasons. First, due to the rarity 247
of acromegaly only nationwide surveys may have adequate statistical power. Second, coverage and accuracy 248
of national cancer registries, as well as duration and completeness of follow-up, are keys for an adequate 249
comparison with the general population. Third, the retrospective nature of these studies is an obvious 250
limitation, particularly when considering that some studies date back to the sixties (Wright et al. 1970, 251
Alexander et al. 1980), when treatment of acromegaly was far less effective. As a consequence, patients with 252
uncontrolled acromegaly may have died before entering the age when cancer usually occurs; thus, 253
competitive cardiovascular morbidity may have hindered cancer incidence and, particularly, cancer mortality 254
(Loeper & Ezzat 2008, Boguszewski & Ayuk 2016). 255
The aim of the present study was to evaluate the incidence of cancer in a series of 1512 acromegalic patients 256
followed up for 10 years at 24 tertiary referral centers in Italy. Most patients were treated after the 257
introduction of SRL in clinical practice, thus representing a modern series. We found that the overall 258
incidence of cancer was increased compared to the general population with a SIR of 1.41 (95%CI, 1.18-259
1.68). The excess risk is only moderate and this may explain why less powered studies produced 260
controversial findings. Since acromegaly is usually recognized many years after its biological onset, we 261
included in the analysis the malignancies diagnosed within a period of 5 years prior to the clinical diagnosis 262
of acromegaly, to account for the long period of exposure to excess GH and IGF-I preceding the diagnosis. 263
Even if malignancies detected during this time span are considered formally as prevalent, they occur under 264
the influence of hormone excess that is present albeit undiagnosed. Pertinently, a recent survey in Denmark 265
Page 12 of 29

13
identified increased morbidity over the 3 years preceding diagnosis of acromegaly (Dal et al., 2016). 266
However, we also did a separate analysis including only the malignancies diagnosed after the clinical 267
diagnosis of acromegaly to provide a more conservative estimate of the risk. The results of this analysis 268
overall confirmed an excess cancer risk with the exception of breast cancer. 269
Only three studies in the literature have a size comparable to the present one, but only two were nationwide 270
surveys. Ron et al. (Ron et al. 1991) analyzed a cohort of 1041 male inpatients with acromegaly in the US 271
and found an increased incidence compared to non-acromegalic hospitalized patients, who served as controls 272
(SIR, 1.6; 95% CI, 1.3-1.9). This increased risk was mainly attributable to gastrointestinal cancers, in 273
particular colon cancer. However, the study may be criticized for the inclusion of only male patients 274
admitted to hospital and for not having used tumor incidence rates of the general population as reference 275
(Loeper & Ezzat 2008). Orme et al. (Orme et al. 1998) made a large epidemiological study in the UK, 276
analyzing a cohort of 1239 subjects with acromegaly, and found that the risk for all malignancies was 277
reduced compared to the general population (SIR, 0.76; 95% CI, 0.60-0.95), although there was a non-278
significant increase in the incidence of colon cancer (SIR, 1.68; P=0.06). However, they excluded 279
approximately 17% of cancer registrations that occurred before the diagnosis of acromegaly. Since the 280
diagnosis of acromegaly is usually made years after its biological onset, excluding such cases may cause an 281
underestimation of the phenomenon (Loeper & Ezzat 2008, Boguszewski & Ayuk 2016). Baris et al. (Baris 282
et al. 2002) made an epidemiological study in Sweden and Denmark, analyzing a cohort of 1634 patients, 283
and found an increased risk for all malignancies (SIR, 1.5; 95% CI, 1.3-1.8), in particular of the digestive 284
tract. 285
More recently, three smaller studies have been published that provided controversial results. Kauppinen-286
Makelin et al. (Kauppinen-Makelin et al. 2005), in a nation-wide survey in Finland, analyzed 334 patients 287
and found an increased cancer incidence (SIR, 1.5; 95% CI, 1.1-1.9). Due to the low number of events, it 288
was impossible to make stratification per cancer type, but colon and thyroid cancer were the most frequently 289
observed. Petroff et al. (Petroff et al. 2015) analyzed 446 patients from the German Acromegaly Registry 290
and found that cancer incidence was non-significantly lower than the general population (SIR, 0.75; 95% CI, 291
0.55-1.00). They found a two times higher incidence of thyroid cancer in acromegalic patients that was not 292
significant due to the low number of events. However, the study has limits in representing only a sample of 293
Page 13 of 29

14
the German Acromegaly Registry and in the methodology used to ascertain cancer registration, which was 294
not always based on referring to medical records but included also phone interview. Moreover, 16% of 295
patients were lost to follow-up. Cheng et al. (Cheng et al. 2015) reported on 408 acromegalic patients 296
followed at 3 referral centers in Canada and found that cancer incidence was higher than in the general 297
population (OR, 2.87; 95% CI, 1.57-5.25). In this cohort, diabetes was associated to the risk of malignancy. 298
The present study has strengths in the large population sample and long follow-up with all cancer 299
registrations confirmed by the physicians who proactively managed the patients. Our study cohort was 300
collected in many referral centers; thus it is representative of the acromegalic population in Italy. It is also 301
representative of a cohort treated in a modern way as demonstrated by the overall mortality data (Arosio et 302
al. 2012) in a range comparable to those observed in more recent studies (Katznelson et al. 2014, Sherlock et 303
al. 2010, Mercado et al. 2014). Our findings on cancer incidence are in close agreement with the nationwide 304
survey in Finland (Kauppinen-Makelin et al. 2005) that was done in the same time period (SIR of the present 305
study, 1.41; SIR of the Finnish study, 1.5). The outcome of the German study (Petroff et al. 2015), which is 306
also a contemporary series, is at variance but the above-mentioned differences in study methodology may 307
explain the discrepancy. 308
Due to our large sample size, we were able to consider separately cancer incidence between sexes and make 309
a meaningful stratification of different cancer types. Risk of cancer was higher in women (SIR 1.51; 95% CI, 310
1.20-1.91) than in men (SIR 1.29; 95% CI, 1.0-1.7), and this may be attributable to the fact that women were 311
older in our series. Cancers found to be more consistently increased were thyroid cancer, kidney cancer and 312
colorectal cancer. These findings are consistent with abundant evidence linking the IGF system with 313
development and progression of all these cancers (Loeper & Ezzat 2008, Pollak 2008, Weroha & Haluska 314
2012, Brahmkhatri et al. 2015, Renehan et al. 2004, Clayton et al. 2011, Giovannucci et al. 2000, Pekic & 315
Popovic 2013). 316
The increased risk of colon neoplasia in acromegaly is the most widely agreed; thus, the Endocrine Society 317
Guidelines suggested incorporating colonoscopy at diagnosis in the management of acromegaly-related 318
comorbidities (Katznelson et al. 2014). Higher risk of breast cancer has been reported in an old study 319
(Nabarro 1987), while recent studies found only non-significant increase in risk (Baris et al. 2002, 320
Kauppinen-Makelin et al. 2005, Petroff et al. 2015). However, assessing the prevalence in acromegaly of 321
Page 14 of 29
15
breast cancer is particularly challenging since it may be looked at only in women, thus substantially halving 322
the sample size. In addition, IGF-I excess could have different effects depending on the menopausal state, 323
and on the levels of other sex and growth hormones, further increasing complexity (Renehan et al. 2004, 324
Tworoger et al. 2011). In recent reports, there is increasing evidence that thyroid cancer is more frequent in 325
patients with acromegaly than in control groups (Wolinski et al. 2014). A recent cross-sectional prospective 326
study in Spain found that either benign nodular thyroid disease or thyroid cancer were more frequent in 123 327
patients with acromegaly than in 50 matched controls applying highly sensitive ultrasound methodology and 328
standardized use of FNA cytology (Reverter et al. 2014). Conversely, the association between acromegaly 329
and kidney cancer has been less frequently reported (Cheung & Boyages 1997, Baris et al. 2002, Kauppinen-330
Makelin et al. 2005). Interestingly, expression of the IGF-I receptor has been associated with poor survival in 331
patients with early-stage renal cancer (Parker et al. 2004). 332
The present study is the first to provide a multivariate analysis aiming at identifying predictors of cancer in 333
acromegaly. We found that age and family history of cancer were significant independent factors associated 334
to cancer risk, and these findings are biologically plausible. Moreover, a non-significant trend between 335
cancer risk and delay in acromegaly diagnosis was apparent, but it is known that the estimate of duration of 336
acromegaly is admittedly imprecise and operator dependent. We did not find evidence of an association 337
between values of GH and IGF-I, or both, and cancer risk. Orme et al. (Orme et al. 1998) found a higher 338
cancer-related mortality in patients with elevated post-treatment GH but no clear link between GH and IGF-I 339
levels and cancer incidence in acromegaly has been definitively proven. This does not discredit the view that 340
GH and IGF-I are implicated in cancer development in acromegaly. It has to be pointed out that the 341
hormonal evaluation at diagnosis or at the last follow-up may give only a poor estimate of patient’s exposure 342
to GH and IGF-I in the course of a chronic disease such as acromegaly. Moreover, other factors may play 343
important roles in determining the risk of neoplasia in acromegaly, such as insulin, insulin resistance, IGF-344
BP1 and BP3, obesity, body composition and leptin levels (Melmed 2001, Boguszewski & Ayuk 2016, 345
Giovannucci et al. 2000, Pekic & Popovic 2013, Tworoger et al. 2011). In this line, it is interesting the 346
finding of Cheng et al. (Cheng et al. 2015) that acromegalic patients with diabetes had more malignant 347
tumors than non-diabetic patients. In our cohort, diabetes was associated with cancer risk only in univariate 348
analysis. The alternative hypothesis that cancer risk in acromegaly is due to common underlining genetic 349
Page 15 of 29

16
factors should be also considered (Loeper & Ezzat 2008, Boguszewski & Ayuk 2016, Renehan & Brennan 350
2008). 351
Limitations of our study are its retrospective nature, as for previous epidemiological studies, the consequent 352
lack of data on the cumulative GH exposure, that has been recently suggested as a very important 353
determinant of morbidity and mortality (Varadhan et al. 2016), and the fact that patients have been submitted 354
in many centers to proactive oncologic screening, since previous studies conducted in Italy have suggested 355
an association between acromegaly and colon neoplasia (Terzolo et al. 2005) or thyroid cancer (Gasperi et 356
al. 2002, Tita et al. 2005). However, the rate of patients who underwent cancer screening was alike between 357
patients with and without cancer; thus, it is unlikely that our findings are explained by an ascertainment bias. 358
In conclusion, we found evidence that acromegaly is associated with a moderate increase in cancer risk in a 359
nation-wide survey in Italy. 360
361
Declaration of Interest: PB, EF, EM, LDM, SG, DF, MM, MB, EDM, CM, EP, AV, MFF, PT, FP, GP, GB, 362
CS, NB, AB, AB, ALS, RB, LMF, MA have nothing to declare. MT received lecture fees from Pfizer. GR 363
received grant support from Novartis. RP received grant support from Novartis, Pfizer, Ipsen. ML received 364
lecture fees from Pfizer, Ipsen. SC received grant support from Novartis, Ipsen, Italfarmaco, Pfizer. AP 365
received grant support from Novartis. AC received grant support from Novartis, Pfizer, Ipsen. 366
367
Funding: This research did not receive any specific grant from any funding agency in the public, 368
commercial or not-for-profit sector 369
Page 16 of 29
17
370
371
REFERENCES 372
373
Alexander L, Appleton D, Hall R, RossWM & Wilkinson R 1980 Epidemiology of acromegaly in the 374
Newcastle region. Clin Endocrinol (Oxf) 12 71–79. 375
Arosio M, Reimondo G, Malchiodi E, Berchialla P, Borraccino A, De Marinis L, Pivonello R, Grottoli S, 376
Losa M, Cannavo` S, et al. 2012 Predictors of morbidity and mortality in acromegaly: an Italian survey. 377
Eur J Endocrinol. 167 189–198. 378
Ayuk J, Clayton RN, Holder G, Sheppard MC, Stewart PM & Bates AS 2004 Growth hormone and 379
pituitary radiotherapy, but not serum insulin-like growth factor-1 concentrations, predict excess mortality 380
in patients with acromegaly. J Clin Endocrinol Metab. 89 1613–1617. 381
Bałdys-Waligórska A, Krzentowska A, Gołkowski F, Sokołowski G & Hubalewska-Dydejczyk A 2010 382
The prevalence of benign and malignant neoplasms in acromegalic patients. Endokrynol Pol. 61 29-34. 383
Baris D, Gridley G, Ron E, Weiderpass E, Mellemkjaer L, Ekbom A, Olsen JH, Baron JA & Fraumeni 384
JF Jr. 2002 Acromegaly and cancer risk: a cohort study in Sweden and Denmark. Cancer Causes Control 385
13 395–400. 386
Barzilay J, Heatley GJ & Cushing GW 1991 Benign and malignant tumors in patiens with acromegaly. 387
Arch Intern Med 151 1629–1632 388
Bengtsson BA, Eden S, Ernest I, Oden A & Sjogren B 1988. Epidemiology and long-term survival in 389
acromegaly. A study of 166 cases diagnosed between 1955 and 1984. Acta Med Scand 223 327–335 390
Biermasz NR 2014 Pituitary gland: mortality in acromegaly reduced with multimodal therapy. Nat Rev 391
Endocrinol. 10 708-710. 392
Page 17 of 29

18
Bogazzi F, Colao A, Rossi G, Lombardi M, Urbani C, Sardella C, Cannelli A, Scattina I, Manetti L, Del 393
Sarto S, et al. 2013 Comparison of the effects of primary somatostatin analogue therapy and pituitary 394
adenomectomy on survival in patients with acromegaly: a retrospective cohort study. Eur J Endocrinol. 395
169 367–376. 396
Boguszewski CL & Ayuk J 2016 Acromegaly and cancer risk: an old debate revisited. Eur J 397
Endocrinol. 175 147-156 398
Brahmkhatri VP, Prasanna C & Atreya HS 2015 Insulin-like growth factor system in cancer: novel 399
targeted therapies. Biomed Res Int. 2015 538019. 400
Cheng S, Gomez K, Serri O, Chik C & Ezzat S 2015The role of diabetes in Acromegaly Associated 401
Neoplasia PLoS One; 10 e0127276. 402
Cheung NW & Boyages SC 1997 Increased incidence of neoplasia in females with acromegaly. Clin 403
Endocrinol (Oxf) 47 323–327. 404
Clayton PE, Banerjee I, Murray PG & Renehan AG 2011 Growth hormone, the insulin-like growth 405
factor axis, insulin and cancer risk. Nat Rev Endocrinol. 7 11-24. 406
Dagdelen S, Cinar N & Erbas T 2014 Increased thyroid cancer risk in acromegaly. Pituitary. 17 299– 407
306. 408
Dal J, Feldt-Rasmussen U, Andersen M, Kristensen LØ, Laurberg P, Pedersen L, Dekkers OM, Sørensen 409
HT, Jørgensen JO. Eur J Endocrinol. 2016 175 181–190 410
Gasperi M, Martino E, Manetti L, Arosio M, Porretti S, Faglia G, Mariotti S, Colao AM, Lombardi G, 411
Baldelli R, et al. 2002 Prevalence of thyroid diseases in patients with acromegaly: results of an Italian 412
multi-center study. J Endocrinol Invest 25 240–245. 413
Giovannucci E, Pollak MN, Platz EA, Willett WC, Stampfer MJ, Majeed N, Colditz GA, Speizer FE & 414
Hankinson SE 2000 A prospective study of plasma insulin-like growth factor-1 and binding protein-3 415
and risk of colorectal neoplasia in women. Cancer Epidemiol Biomarkers Prev. 9 345–349. 416
Page 18 of 29

19
Gullu BE, Celik O, Gazioglu N & Kadioglu P 2010 Thyroid cancer is the most common cancer 417
associated with acromegaly. Pituitary. 13 242–248. 418
Higuchi Y, Saeki N, Iuchi T, Uchino Y, Tatsuno I, Uchida D, Tanaka T, Noguchi Y, Nakamura S, 419
Yasuda T, et al. 2000 Incidence of malignant tumors in patients with acromegaly. Endocr J 47 (Suppl) 420
57–60. 421
Holdaway IM, Rajasoorya RC & Gamble GD 2004. Factors influencing mortality in acromegaly. J Clin 422
Endocrinol Metab. 89 667–674. 423
Katznelson L, Laws ER Jr, Melmed S, Molitch ME, Murad MH, Utz A & Wass J 2014 Acromegaly: an 424
Endocrine Society Clinical Practice Guideline. J Clin Endocrinol Metab 99 3933-3951. 425
Kauppinen-Mäkelin R, Sane T, Välimäki MJ, Markkanen H, Niskanen L, Ebeling T, Jaatinen P, Juonala 426
M; Finnish Acromegaly Study Group, Pukkala 2010 Increased cancer incidence in acromegaly--a 427
nationwide survey. Clin Endocrinol. 72 278–279. 428
Kurimoto M, Fukuda I, Hizuka N & Takano K 2008 The prevalence of benign and malignant tumors in 429
patients with acromegaly at a single institute. Endocr J. 55 67–71. 430
Liddell FD 1984 Simple exact analysis of the standardised mortality ratio. J Epidemiol Community 431
Health. 38 85-8. 432
Loeper S & Ezzat S 2008 Acromegaly: re-thinking the cancer risk. Rev Endocr Metab Disord. 9 41–58. 433
Maione L, Brue T, Beckers A, Delemer B, Petrossians P, Borson-Chazot F, Chabre O, François P, 434
Bertherat J, Cortet-Rudelli C, Chanson P; French Acromegaly Registry Group. Changes in the 435
management and comorbidities of acromegaly over three decades: the French Acromegaly Registry. Eur 436
J Endocrinol. 2017 176 645-655 437
Melmed S 2001 Acromegaly and cancer: not a problem? J Clin Endocrinol Metab. 86 2929-2934. 438
Melmed S 2009 Acromegaly pathogenesis and treatment. J Clin Invest. 119 3189-3202. 439
Page 19 of 29
20
Mercado M, Gonzalez B, Vargas G, Ramirez C, De los Monteros AL, Sosa E, Jervis P, Roldan P, 440
Mendoza V, Lopez-Félix B, et al. 2014 Successful mortality reduction and control of comorbidities in 441
patients with acromegaly followed at a highly specialized multidisciplinary clinic. J Clin Endocrinol 442
Metab. 99 4438-4446. 443
Mustacchi P & Shimkin MB 1957 Occurrence of cancer in acromegaly and in hypopituitarism. Cancer 444
10 100–104. 445
Nabarro JD 1987 Acromegaly. Clin Endocrinol. (Oxf) 26 481–512. 446
Orme SM, McNally RJ, Cartwright RA & Belchetz PE 1998 Mortality and cancer incidence in 447
acromegaly: a retrospective cohort study. United Kingdom Acromegaly Study Group. J Clin Endocrinol 448
Metab. 83 2730–2734. 449
Parker AS, Cheville JC, Blute ML, Igel T, Lohse CM & Cerhan JR 2004 Pathologic T1 Clear Cell Renal 450
Cell Carcinoma: Insulin-Like Growth Factor-I Receptor Expression and Disease-Specific Survival. 451
Cancer 100 2577–82. 452
Pekic S & Popovic V 2013 GH therapy and cancer risk in hypopituitarism: what we know from human 453
studies. Eur J Endocrinol. 169 R89–R97. 454
Petroff D, Tönjes A, Grussendorf M, Droste M, Dimopoulou C, Stalla G, Jaursch-Hancke C, Mai M, 455
Schopohl J & Schöfl C 2015 The Incidence of Cancer Among Acromegaly Patients: Results From the 456
German Acromegaly Registry. J Clin Endocrinol Metab. 100 3894-902. 457
Pines A, Rozen P, Ron E & Gilat T 1985 Gastrointestinal tumors in acromegalic patients. Am J 458
Gastroenterol. 80 266–269. 459
Pollak M 2008 Insulin and insulin-like growth factor signalling in neoplasia. Nat Rev Cancer 8 915-928. 460
Popovic V, Damjanovic S, Micic D, Nesovic M, Djurovic M, Petakov M, Obradovic S, Zoric S, Simic 461
M, Penezic, et al. 1998 Increased incidence of neoplasia in patients with pituitary adenoma. The 462
Pituitary Study Group. Clin Endocrinol (Oxf) 49 441–445. 463
Page 20 of 29

21
Rajasoorya C, Holdaway IM, Wrightson P, Scott DJ & Ibbertson HK 1994 Determinants of clinical 464
outcome and survivial in acromegaly. Clin Endocrinol (Oxf) 41 95–102. 465
Renehan AG & Brennan BM 2008 Acromegaly, growth hormone and cancer risk. Best practice, 466
research. Clinical endocrinology, metabolism 22 639–657. 467
Renehan AG, Zwahlen M, Minder C, O’Dwyer ST, Shalet SM & Egger M 2004 Insulin-like growth 468
factor (IGF)-I, IGF binding protein-3, and cancer risk: systematic review and meta-regression analysis. 469
Lancet 363 1346-1353. 470
Reverter JL, Fajardo C, Resmini E, Salinas I, Mora M, Llatjós M, Sesmilo G, Rius F, Halperin I, Webb 471
SM, et al. 2014 Benign and malignant nodular thyroid disease in acromegaly. Is a routine thyroid 472
ultrasound evaluation advisable? PlosOne 9 e104174. 473
Rokkas T, Pistiolas D, Sechopoulos P, Margantinis G & Koukoulis G 2008 Risk of colorectal neoplasm 474
in patients with acromegaly: a meta-analysis. World J Gastroenterol. 14 3484–3489. 475
Ron E, Gridley G, Hrubec Z, Page W, Arora S & Fraumeni Jr JF 1991 Acromegaly and gastrointestinal 476
cancer. Cancer 68 1673–1677. 477
Sherlock M, Ayuk J, Tomlinson J, Toogood AA, Aragon-Alonso A, Sheppard MC, Bates AS & Stewart 478
PM 2010 Mortality in patients with pituitary disease. Endo Rev 31 301-342. 479
Terzolo M, Reimondo G, Gasperi M, Cozzi R, Pivonello R, Vitale G, Scillitani A, Attanasio R, Cecconi 480
E, Daffara F et al. 2005 Colonoscopic screening and follow-up in patients with acromegaly: a 481
multicenter study in Italy. J Clin Endocrinol Metab. 90 84-90. 482
Tita P, Ambrosio MR, Scollo C, Carta A, Gangemi P, Bondanelli M, Vigneri R, degli Uberti EC & 483
Pezzino V 2005 High prevalence of differentiated thyroid carcinoma in acromegaly. Clin Endocrinol 484
(Oxf). 63(2) 161-167. 485
Tworoger SS, Rosner BA, Willett WC & Hankinson SE 2011 The combined influence of multiple sex 486
and growth hormones on risk of postmenopausal breast cancer: a nested case-control study. Breast 487
Page 21 of 29

22
Cancer Res. 13 R99. 488
Varadhan L, Reulen RC, Brown M & Clayton RN 2016 The role of cumulative growth hormone 489
exposure in determining mortality and morbidity in acromegaly: a single centre study. Pituitary 19 251-490
261. 491
Weroha SJ & Haluska P 2012 The insulin-like growth factor system in cancer. Endocrinol Metab Clin 492
North Am. 41 335–350. 493
Wolinski K, Czarnywojtek A & Ruchala M 2014 Risk of Thyroid Nodular Disease and Thyroid Cancer 494
in Patients with Acromegaly – Meta-Analysis and Systematic Review. PlosOne 9 e8878. 495
Wright AD, Hill DM, Lowy C & Fraser TR 1970 Mortality in acromegaly. Quarterly Journal of 496
Medicine 39 1–16. 497
Page 22 of 29

1
FIGURE LEGENDS 1
Figure 1 – Sample size of the population-based studies on acromegaly and cancer. 2
Page 23 of 29

Table 1 – Cancer incidence data in studies with more than 200 patients.
*Hospitalized patients
NA=Not Available
Author, year Study
Period
Patients
(n°)
Follow-up
(years or
person
years)
Age at
diagnosis
CANCER
n°, (%)
SIR
95% CI
P value
Ron, 1991 1969-1985 1041* 8619 NA 89 (8.5) 1.6
1.3-1.9
NA
Orme, 1998 1958-1995 1239 16778 NA 79 (6.4) 0.76
0.60-0.95
1
Popovic, 1998 1992-1998 220 4.5 49.5 23 (10.5) 3.39
2.12-5.12
<0.01
Baris, 2002 1965-1993 1634* 14724 50.4 177 (10.8) 1.5
1.3-1.8
NA
Kauppien-
Makelin, 2010
1980-2006 333 10.7 47.5 48 (14.4) 1.5
1.1-1.9
NA
Petroff, 2015 NA 374 6656 45.7 44 (11.8) 0.75
0.55-1.00
0.051
Cheng, 2015 NA 408 10.2 43.2 55 (13.4) 2.87
1.57-5.25
NA
Dal, 2016 1991-2010 405 10.6 48.7 NA 1.4
0.9-2.2
NA
Maione, 2017 1977-2012 999 6728 43 men
48.5 women
94 (10.1%) 1.34
(0.94–1.87)
men
1.24
(0.77–1.73)
women
NA
Page 24 of 29

Table 2 – Cancer mortality data in studies with more than 150 patients
Author, year N. Follow-up
Duration
(years or
person/years)
Age at
death
Overall
SMR
Cancer-related
SMR
(95% CI)
P
value
Nabarro 1987 256 20 NA 1.26 0.96
(NA)
NA
Bengtsson 1988 166 30 NA NA Overall: 2.68
Female: 3.3
(NA)
<0.01
Rajasoorya
1994
151 12 57 NA 1
(NA)
NA
Orme 1998 1362 NA NA 1.6 1.16
(0.92–1.44)
0.1
Ayuk 2004 419 13 NA 1.26 0.91
(0.59-1.39)
0.65
Holdaway 2004 208 13 ± 9 62 ± 2
1.87 0.92
(NA)
NA
Dal, 2016 405 10.6 NA 1.3 1.1
(0.7-1.9)
NA
NA=Not Available, SMR=Standard Mortality Ratio, CI=Confidence Interval
Page 25 of 29
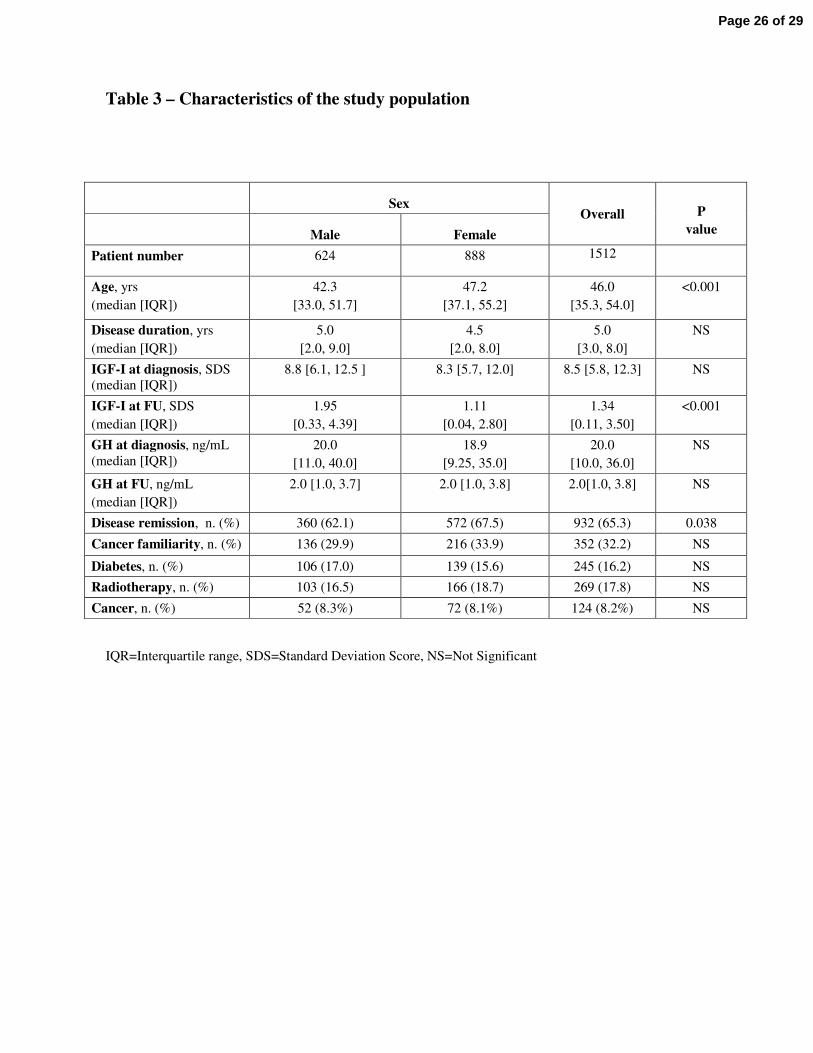
Table 3 – Characteristics of the study population
Sex
Overall
P
value
Male Female
Patient number 624 888 1512
Age, yrs
(median [IQR])
42.3
[33.0, 51.7]
47.2
[37.1, 55.2]
46.0
[35.3, 54.0]
<0.001
Disease duration, yrs
(median [IQR])
5.0
[2.0, 9.0]
4.5
[2.0, 8.0]
5.0
[3.0, 8.0]
NS
IGF-I at diagnosis, SDS
(median [IQR])
8.8 [6.1, 12.5 ] 8.3 [5.7, 12.0] 8.5 [5.8, 12.3] NS
IGF-I at FU, SDS
(median [IQR])
1.95
[0.33, 4.39]
1.11
[0.04, 2.80]
1.34
[0.11, 3.50]
<0.001
GH at diagnosis, ng/mL
(median [IQR])
20.0
[11.0, 40.0]
18.9
[9.25, 35.0]
20.0
[10.0, 36.0]
NS
GH at FU, ng/mL
(median [IQR])
2.0 [1.0, 3.7] 2.0 [1.0, 3.8] 2.0[1.0, 3.8] NS
Disease remission, n. (%) 360 (62.1) 572 (67.5) 932 (65.3) 0.038
Cancer familiarity, n. (%) 136 (29.9) 216 (33.9) 352 (32.2) NS
Diabetes, n. (%) 106 (17.0) 139 (15.6) 245 (16.2) NS
Radiotherapy, n. (%) 103 (16.5) 166 (18.7) 269 (17.8) NS
Cancer, n. (%) 52 (8.3%) 72 (8.1%) 124 (8.2%) NS
IQR=Interquartile range, SDS=Standard Deviation Score, NS=Not Significant
Page 26 of 29

Table 4 – Cancer incidence data broken down by gender
Cancer type Observed Expected SIR 95% CI p-value
Female
All malignancies 72 47.6 1.51 1.2-1.91 <0.001
Breast cancer 22 16.8 1.31 0.86-1.99 0.21
Colorectal cancer 12 6.4 1.86 1.06-3.28 0.03
Thyroid cancer 8 2.5 3.22 1.61-6.44 0.01
Male
All malignancies 52 40.2 1.29 1.0-1.7 0.06
Colorectal cancer 8 5.6 1.44 0.72-2.88 0.31
Kidney cancer 7 1.9 3.73 1.78-7.83 <0.001
Thyroid cancer 5 0.8 6.51 2.71-15.65 <0.001
Overall
Colorectal cancer 20 12 1.67 1.07-2.58 0.022
Kidney cancer 10 3.5 2.87 1.55-5.34 <0.001
Thyroid cancer 13 3.3 3.99 2.32-6.87 <0.001
SIR=Standard Incidence Ratio, CI=Confidence Interval
Page 27 of 29

Table 5 – Predictive factors of cancer in multivariable analysis.
Factor OR P value
Age 5.39
CI 95%: 2.08 – 13.9
< 0.001
Family history of cancer 1.73
CI 95%: 1.03 – 2.92
0.04
Disease duration 1.27
CI 95%: 0.97 – 1.64
0.08
Pituitary radiotherapy 1.76
CI 95%: 0.89 – 3.45
0.10
Diabetes 1.39
CI 95%: 0.76 – 2.57
0.28
Gender 1.19
CI 95%: 0.69 – 2.05
0.51
IGF-I at last visit 1.03
CI 95%: 0.76 – 1.38
0.87
OR=Odds Ratio, CI=Confidence Interval
For continuous variables, OR are reported for an interquartile range increase, i.e. 19 years of difference for
age and 1.5 SDS for IGF-I
Page 28 of 29
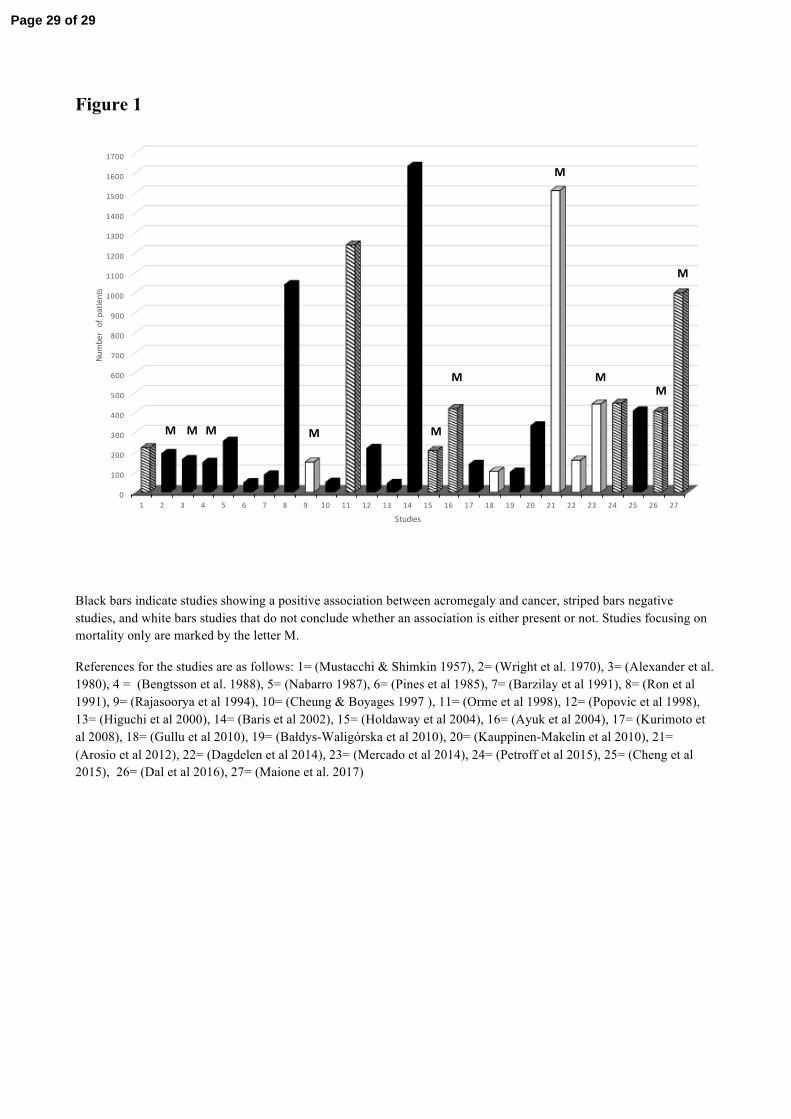
Figure 1
Black bars indicate studies showing a positive association between acromegaly and cancer, striped bars negative studies, and white bars studies that do not conclude whether an association is either present or not. Studies focusing on mortality only are marked by the letter M.
References for the studies are as follows: 1= (Mustacchi & Shimkin 1957), 2= (Wright et al. 1970), 3= (Alexander et al. 1980), 4 = (Bengtsson et al. 1988), 5= (Nabarro 1987), 6= (Pines et al 1985), 7= (Barzilay et al 1991), 8= (Ron et al 1991), 9= (Rajasoorya et al 1994), 10= (Cheung & Boyages 1997 ), 11= (Orme et al 1998), 12= (Popovic et al 1998), 13= (Higuchi et al 2000), 14= (Baris et al 2002), 15= (Holdaway et al 2004), 16= (Ayuk et al 2004), 17= (Kurimoto et al 2008), 18= (Gullu et al 2010), 19= (Bałdys-Waligórska et al 2010), 20= (Kauppinen-Makelin et al 2010), 21= (Arosio et al 2012), 22= (Dagdelen et al 2014), 23= (Mercado et al 2014), 24= (Petroff et al 2015), 25= (Cheng et al 2015), 26= (Dal et al 2016), 27= (Maione et al. 2017)
0
100
200
300
400
500
600
700
800
900
1000
1100
1200
1300
1400
1500
1600
1700
1 2 3 4 5 6 7 8 9 10 11 12 13 14 15 16 17 18 19 20 21 22 23 24 25 26 27
Numberofp
atients
Studies
M M M M M
M M
M
M
M
Page 29 of 29





























