Embed Size (px)
Citation preview
Prepared by
John Packham, PhD
University of Nevada School of Medicine
Patricia Durbin
Executive Director
Great Basin Primary Care Association of Nevada
December 2009
Access All Nevada:
Preserve, Strengthen & Expand
COMMUNITY HEALTH CENTERS

Thank you to our members,
partners and healthcare
stakeholders for contributions
of data, information,
dedication and foresight.
We also extend a special
appreciation to the National
Association of Community
Health Centers.
Thanks for this publication &
design to Misty Levis, GBPCA
Director of Member Services
and Communications
A Note to Readers
Thank you for taking the time to explore the issues raised in Access All Nevada. We believe them to be vital to the health of each person in our state. As we go to print on this edition of the report, health care reform is on the minds of millions of Americans. That nearly 50 million people in our country, including over 600,000 Nevadans, do not have adequate health insurance coverage is more than a disgrace, it is an epidemic that kills thousands of people every year. And while insurance reform is critical, we must also recognize that insurance coverage alone does not equal access to care. Everyone must have access to a high quality and cost effective medical home, as well as, the means to pay for care.
At Great Basin Primary Care Association of Nevada, we believe the medical home solution for our state is the continued development of Community Health Center (CHC) sites and increasing the number of health care professionals who serve in them. It is at the CHCs that community members can access the highest quality and most affordable health care regardless of their ability to pay. Dedicated doctors, nurses, pharmacists and other medical providers are available at the centers to
meet patient’s needs. CHCs have been a vital resource for Nevadans health care needs since 1985 and continue to be so.
With that in mind, we present our report on how Nevada can expand our CHC resources, increase the health care workforce and provide access to care for more Nevadans. It is these efforts that will lead to real reform of our state’s fragile health care system and better lives for everyone.
We look forward to continuing our work with you throughout this process.
Sincerely,
Patricia Durbin
Executive Director

Access All Nevada
IMPROVING ACCESS TO CARE 1
MEDICALLY UNDERSERVED NEVADANS 1
PROVIDING A HEALTH CARE HOME 1
THE PIVOTAL ROLE OF NEVADA’S COMMUNITY HEALTH CENTERS 2
BETTER CARE FOR LOWER COSTS 4
MEDICALLY UNDERSERVED POPULATIONS IN NEVADA 4
NEVADA’S COMMUNITY HEALTH CENTERS 5
COMMUNITY HEALTH CENTERS AT THE CORE OF THE HEALTH CARE SAFETY NET IN NEVADA 6
INVESTING IN NEVADA’S COMMUNITIES ‐ HEALTH SYSTEM AND ECONOMIC IMPACTS 10
GOALS AND OBJECTIVES 12
STRATEGIES AND REQUIREMENTS 13
EXPAND CAPITAL AND OPERATING REVENUE 14
STRENGTHEN HEALTHCARE WORKFORCE 16
CHALLENGES AND OPPORTUNITIES 18
BACKGROUND DATA AND REPORTS 19

1
● ● ● The vision of ACCESS All Nevada is to improve access to medical care for an additional 80,000 Nevadans by 2015. ● ● ●
Improving Access to Care
Medically Underserved Nevadans
ACCESS All Nevada contains an ambitious set of strategies to increase access to primary and preventive
services for medically disenfranchised Nevadans. The vision of ACCESS All Nevada is to improve access to
medical care for an additional 80,000 Nevadans by 2015 through the expansion of Community Health
Center (CHC) services and sites across the state. This plan documents the strengths of Nevada’s CHCs
and their success in meeting the most pressing needs of the medically underserved in Nevada. The plan
also presents strategies aimed at improving the ability of Nevada’s health centers to develop and grow
in a manner that ensures all Nevadans have access to high quality health care.
Providing a Health Care Home For the Medically Disenfranchised Nevadans
Today, nearly 60 million Americans – including many
who have health insurance coverage – are “medically
disenfranchised.” The medically disenfranchised are
those people with no or inadequate access to a primary
care physician due to local shortages of such physicians.
They are a subset of medically underserved populations
who typically face multiple barriers to accessing care, including the general lack of physicians
willing or able to treat them in their community. In 2005, there were an estimated 675,000
medically disenfranchised Nevadans – a figure that is undoubtedly grown as a result of the
nationwide economic recession, rising unemployment across the state, and swelling ranks of
the uninsured in Nevada.
The medically disenfranchised are at greater risk for being unable to establish a “medical
home” due to the shortage of primary care physicians where they live. Medical homes are
patient‐centered, regular, and continuous sources of care, coordinated by a team of medical
professionals committed to cost‐effective, high quality health care. The medical home model of
primary care has been shown to prevent sickness, manage chronic illnesses, and reduce the
need for avoidable, costlier care such as emergency department visits or hospitalizations. As
national policy makers once again focus on health care reform, there is widespread agreement
that an expansion of health insurance coverage is needed to improve the nation’s health.

2
● ● ● For more than forty years, the nation’s federally-supported Community Health Centers have provided a medical home for millions of medically underserved people and thousands of communities across the country. ● ● ●
However, while health insurance facilitates access to care, it does not guarantee access to a
usual source of care or a medical home. Indeed, people who have a medical home but no
health insurance typically receive more primary care than those who have insurance but no
source of usual care. Those who have both health insurance and a medical home have the best
health outcomes.
For more than forty years, the nation’s federally‐supported Community Health Centers or
Federally‐Qualified Health Centers (FQHCs) have provided a medical home for millions of
medically underserved people and thousands of communities
across the country. In addition to providing high quality,
affordable primary and preventive services to low income and
traditionally underserved communities, many CHCs have added
oral health, behavioral health, and pharmaceutical services, thus
expanding the original medical home concept to a much more
comprehensive “health care home” for residents of their
communities. Currently, over 1,200 health centers across the
country serve as the health care home for over 18 million people
in over 6,300 communities. In 2008, Nevada’s CHCs provided a
health care home for nearly 80,000 Nevadans across the state.
The Pivotal Role of Nevada’s Community Health Centers
Prior to the economic recession, access to affordable primary
care represented one of the most persistent challenges to our
health care system. Despite the fact that health centers have added 2 million people to their
patient rolls since the recession began, the number of medically disenfranchised in our state
and nation continues to grow. Additionally, rising costs, narrowing revenue streams from both
public and private insurers, and steady increases in newly uninsured and chronically ill patients
threaten CHC’s ability to meet growing need. To meet these challenges and to reduce the ranks
of the medically disenfranchised, the National Association of Community Health Centers
(NACHC) has launched ACCESS for ALL America. The aim of this nationwide plan is to expand the
reach and ability of CHCs to provide care to those without a health care home.
The vision of ACCESS for All America is to preserve, strengthen, and expand health centers from
a stable base to reach a total of 30 million patients by 2015 – nearly twice the number served

3
● ● ● The aim of ACCESSAllNevada is to double the number of Nevadans served by Community Health Centers increasing access for an additional 80,000 medically disenfranchised by 2015.
● ● ●
today – and, ultimately, all medically underserved people. The strategy for growth revolves
around the core mission of Community Health Centers – to serve those in need – and includes
four key elements: revenue growth to support increased operating costs and the expansions of
services in existing CHCs; capital financing for new construction, renovation of existing CHCs,
and other capital improvements to maximize the quality and cost‐effectiveness of patient care
provided by all CHC physicians and staff; the preservation and strengthening of Medicare,
Medicaid, SCHIP, and other crucial public health insurance programs; and strengthened support
for vital federal and state health professions training programs to ensure an adequate clinical
workforce in medically underserved areas.
ACCESS All Nevada documents the strengths of Nevada’s
Community Health Centers and their success in meeting the
most pressing needs of the medically underserved in Nevada.
The plan also presents strategies aimed at improving the
ability of Nevada’s Community Health Centers to develop and
grow in a manner that ensures that all Nevadans have access
to high quality health care. Great Basin Primary Care
Association (GBPCA) and its member health centers fully
support the goals of ACCESS for All America. The aim of
ACCESS All Nevada is to double the number of Nevadans
served by Community Health Centers and thus increase access
to medical services for an additional 80,000 medically
disenfranchised individuals in Nevada by 2015. Achieving this
goal will require a significant investment of resources by
Nevada’s health centers, working in partnership with other
safety net providers and public agencies in Nevada. Great
Basin Primary Care Association fully endorses the NACHC’s ACCESS for All America plan and has
worked with Nevada’s health centers and other safety‐net providers to develop a plan for
geographic and service expansion in support of these goals.
4
● ● ● By any measure, most health professions are in short supply in Nevada and vast areas of the state are medically underserved. ● ● ●
Better Care for Lower Costs
Medically Underserved Populations in Nevada
Nevada’s Community Health Centers serve as the health care home for thousands of low‐
income and medically underserved Nevadans across the state. One in ten Nevadans live at or
below the Federal Poverty Level (FPL) and 14.9% of children aged 18 and under live in poverty.
An estimated 479,298 Nevadans or 17.5% of the state’s population were uninsured the entire
year of 2008. Recent personal income and health insurance estimates from the Census Bureau
suggest that the number of uninsured Nevadans and those in poverty have only grown since
the onset of the nationwide recession that has added another 682,000 Americans to the ranks
of the uninsured over the past year. The same Census Bureau report indicates that the number
of people living in poverty jumped by 2.6 million to 39.8 million over the past year.
In addition to financial access barriers, Nevada is plagued by
chronic shortages of primary care physicians, dentists, and
other health professionals. Nevada ranks 46th among US
states in the number of physicians and primary care
physicians per resident population, 42nd in dentists per
capita, and 50th among all states for both general and
specialty surgeons. Similarly, despite important strides taken
by state lawmakers earlier this decade to double nursing
program enrollment, Nevada ranks 49th among US states in
the number of employed registered nurses per capita.
Worse, Nevada is bordered by states with serious nursing shortages in their own right, including
California (45th), Utah (46th), Idaho (47th), and Arizona (50th).
By any measure, most health professions are in short supply in Nevada and vast areas of the
state are medically underserved. Presently, 10 of the state’s 17 counties have been designated
by the federal government as single‐county Health Professional Shortage Areas (HPSAs), 11 are
dental shortage areas, and 14 are mental health HPSAs. While health professions shortages are
greater in rural versus urban regions of Nevada, many of the census tracts in the state’s three
urban counties – Carson City, Clark County, and Washoe County – have been designated as
primary medical care HPSAs.

5
● ● ● For the past two decades, health centers have provided high quality, affordable primary care and preventive services to the state’s most vulnerable populations. ● ● ●
Nevada’s Community Health Centers
Community Health Centers are well positioned to meet the health care needs of low‐income
and other medically underserved populations in Nevada. CHCs are local, non‐profit,
community‐owned health care providers serving low‐income and medically underserved
communities. For the past two decades, health centers have provided high quality, affordable
primary care and preventive services to the state’s most vulnerable populations and to
communities who otherwise confront financial, geographic, language, and cultural barriers to
accessing care. Nevada’s health centers are located in
medically underserved areas of the state and annually
provide access to care for thousands Nevadans regardless of
insurance status or ability to pay. Health centers have tailored
their services to fit the special needs and priorities of the
state’s increasingly diverse communities, including primary
care and preventive services provided in a linguistically and
culturally appropriate manner. Presently, 50.6% of Nevada’s
CHC patients are of Hispanic or Latino ancestry and 62.3%
have family incomes at or below the Federal Poverty Level.
The state’s two Community Health Centers – Health Access
Washoe County (HAWC) and Nevada Health Centers (NHC) –
provide a health care home to nearly 80,000 Nevadans with
41 sites in medically underserved areas of nine of Nevada’s 17
counties. HAWC and NHC are grant‐supported Federally
Qualified Health Centers or FQHCs that meet certain criteria
under the Medicare and Medicaid Programs of the Social Security Act and receive funds under
the federal CHC Program. Both centers participate in Healthcare for the Homeless Programs
that target homeless individuals and families and provide primary care and substance abuse
services to local residents. Both centers are governed by boards comprised of 51%
consumer/patient directors who reflect the demographic and socioeconomic characteristics of
the patients and communities they serve.
Community Health Center sites in Nevada include two mobile dental vans serving southern and
northeastern Nevada, one “mammovan” providing statewide mammography and breast cancer
screening services, and seven “WIC” clinics serving women, infants and children. Two
additional CHC satellite sites in Mesquite and Overton managed by Canyonlands Community
Health Care are based in Page, Arizona. Nevada’s health centers provide comprehensive
6
● ● ● In 2008, CHCs provided primary care and preventive services to 79,163 patients in Nevada. Patient visits or “clinic encounters” totaled 197,316. CHCs provided an additional 7,414 mammograms; 16,057 immunizations; and oral health services to 11,789 residents of the state. ● ● ●
primary and other health services, as well as services that help their patients access care such
as transportation, translation, and case management. Nevada’s CHCs are also critical providers
of maternal and child health services, such as annual well‐child check‐ups, childhood
immunizations, and parental education about child development.
In 2008, CHCs provided primary care and preventive services to 79,163 patients in Nevada.
Patient visits or “clinic encounters” totaled 197,316 or 2.5 visits per health center patient.
Health centers in Nevada provided 7,414 mammograms and 16,057 immunizations to low‐
income residents of medically underserved areas of the state. Nevada CHCs also provided oral
health services, such as oral exams and restorative services, to 11,789 residents of the state.
Nearly three in five (58.5%) health center patients is
uninsured. Another 15.3% are covered by Medicaid or
Nevada CheckUp (SCHIP), 4.7% are covered by Medicare,
and the remaining 21.5% have private insurance.
Community Health Centers at the Core of the Health Care Safety Net in Nevada
The traditional health care “safety net” in Nevada
comprises a broad range of locally‐oriented organizations
and professionals that – either by legal mandate or
explicitly adopted missions – offer care to patients
regardless of ability to pay. A substantial proportion of
safety‐net patients are uninsured, underinsured, socially
disadvantaged, or otherwise vulnerable. Community
Health Centers lie at the core of Nevada’s health care
safety net.
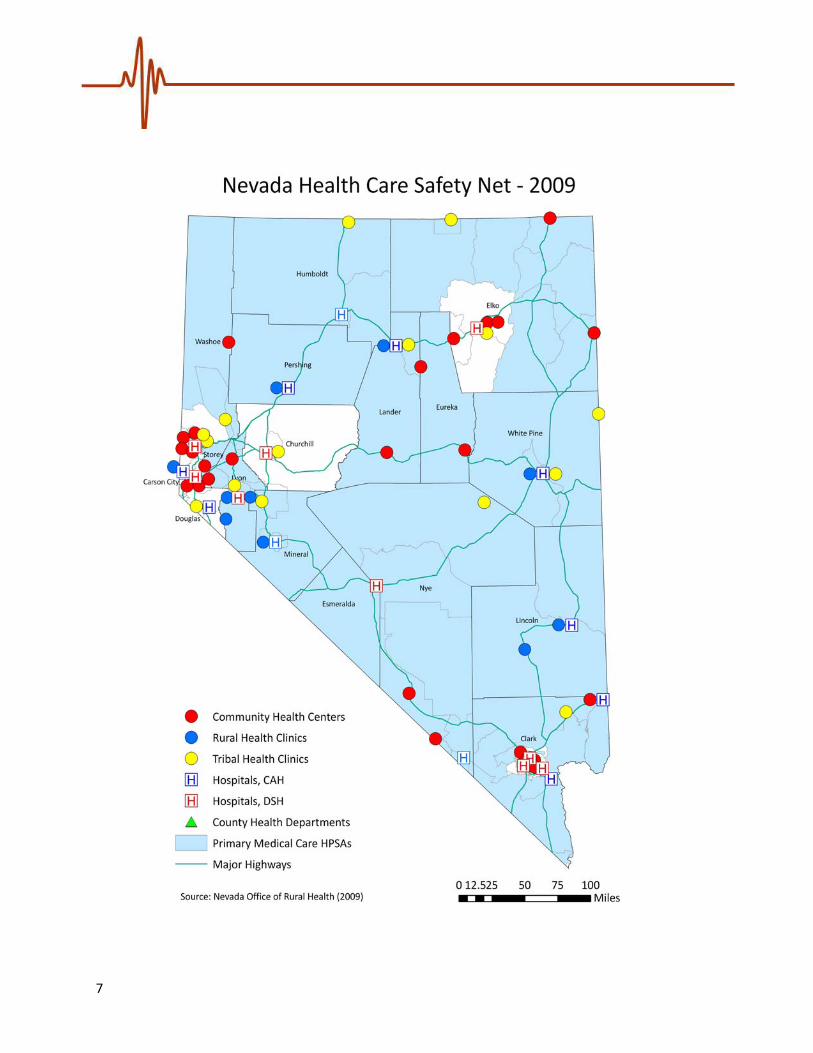
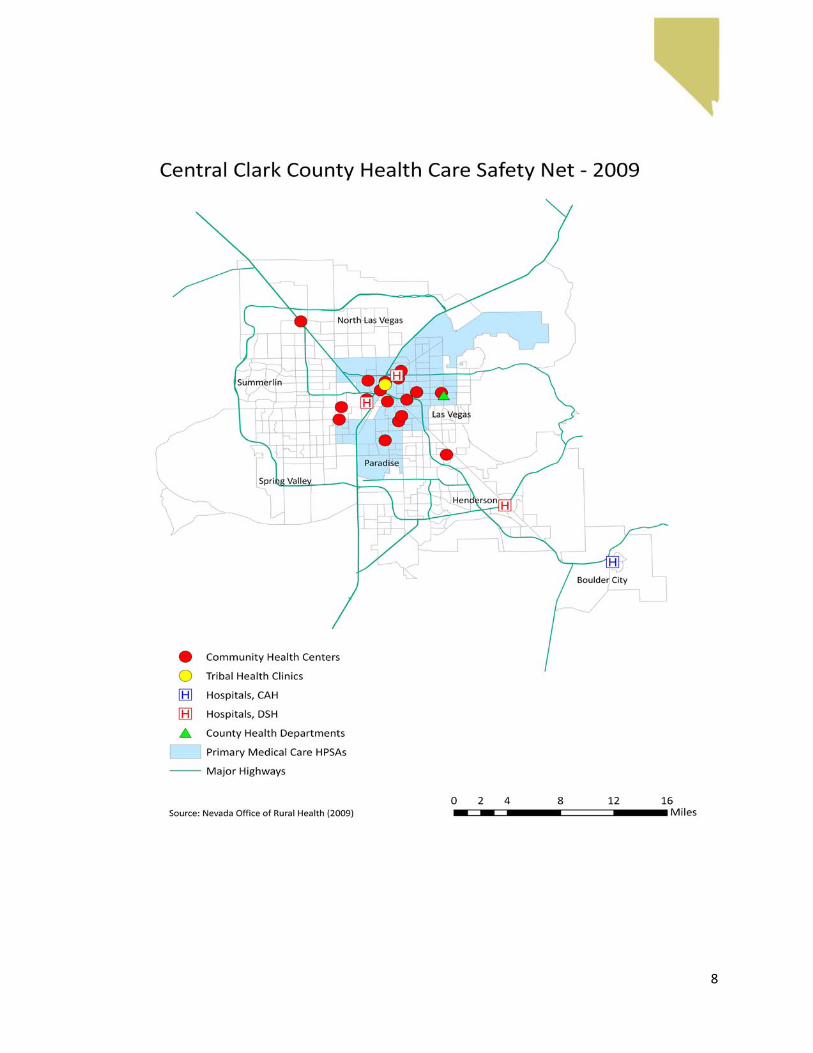
The following maps highlight the statewide and regional
distribution of CHC sites in relation to federally‐designated Primary Medical Care Health
Professional Shortage Areas or “HPSAs” (the blue shaded regions of each map). These maps
also underscore the distribution of other safety‐net providers, including hospital‐based Rural
Health Clinics (RHCs), tribal clinics and health centers, county health departments, Critical
Access Hospitals (CAHs), and hospitals that receive disproportionate share payments from the
Centers for Medicare and Medicaid services for treating uninsured and low‐income patients.
7
8

9

10
● ● ● In 2006, expenditures on avoidable emergency department visits totaled $113 million. Improving access to a health care home would save taxpayers and hospitals millions. ● ● ●
These maps reveal that the majority of the state’s 42 health center sites are
concentrated in urban census tracts of Clark County and northwestern Nevada and that
they are closely aligned with primary medical care HPSAs in each of those regions.
Additionally, a dozen CHC sites are distributed across sparsely populated areas of rural
and frontier of the state and rural areas of both Clark and Washoe County. In many
frontier communities of Nevada, CHCs represent the sole source of medical services.
Investing in Nevada’s Communities - Health System and Economic Impacts
Enhanced capital and operating support for Community Health Center sites and services
represent cost‐effective investments in Nevada’s health system and economy.
Numerous studies have found that, in addition to providing affordable services
vulnerable populations, health centers provide high
quality medical care that reduces overall health system
expenditures and have produced cost savings to
taxpayers and patients. In particular, health centers
play a vital role in reducing avoidable emergency room
visits and preventable hospitalizations. For example,
compared to Medicaid patients treated by non‐CHC
providers, those Medicaid patients treated by CHCs
are between 11% and 22% less likely to be hospitalized
for preventable conditions and are 19% less likely to
use hospital emergency rooms for avoidable
conditions. In general, patients served by health
centers have lower hospital admission rates, lower
lengths of hospital stays, and lower outpatient and
other health care costs than those in underserved areas without health centers. In
2006, expenditures on avoidable emergency department visits totaled $113 million.
Improving access to a health care home for Medicaid patients and other low‐income
residents of Nevada would save taxpayers and hospitals millions in avoidable ER visits.
In addition to generating overall health system savings and efficiency, Community
Health Centers play a critical role in local economic development by directly creating
jobs and income for residents of low‐income communities through normal clinical
activities and indirectly generating employment and payroll in other businesses in the

11
● ● ● According to the National Association of Community Health Centers, CHCs had an overall impact of $33.6 million on the Nevada economy in 2005. ● ● ●
community through health center spending and health center employee spending.
According to estimates prepared by the National Association of Community Health
Centers, CHCs had an overall impact of $33.6 million on the Nevada economy in 2005.
The experience of Elko Family Medical and Dental Center in Elko, Nevada highlights the
significant economic impact of just one health center on the local economy. In addition
to providing a wide range of essential medical and dental care to local residents, the
Elko CHC generates substantial direct and secondary employment and payroll impacts
on the local economy. The Elko Family Medical and Dental Center serves the 48,000
residents of Elko County. The center provides a wide range of primary care, including
family medicine, women’s health, pediatrics, physical exams, occupational health,
STD/HIV education and screening, family planning, periodic screenings for children and
adults, well‐child care and immunizations, prenatal and newborn care, chronic illness
management, health education, and laboratory and radiology services. The center
recently began offering dental services, including
restorative and preventive care, dental examinations
and cleanings, sealants, fluoride treatments, extractions,
x‐rays, fillings, and oral health education.
In 2008, the Elko Family Medical and Dental Center
spent $2.96 million on operations. When the
expenditures of other businesses as a result of the
center are included in the analysis, the community
health center directly and indirectly generated an
estimated $4.30 million in spending in the Elko area.
During the same year, the center employed 31 county
residents. When the employment created by other businesses as a result of the center is
included in the analysis, the community health center directly and indirectly generate a
projected total of 44 jobs in the local economy. Finally, the CHC generated $2.43 in
payroll in 2008. When the payroll generated by other businesses as a result of the
center is included in the analysis, the center generated an estimated total of $3.04
million in payroll for the local economy. In other words, the economic impact of the Elko
Family Medical and Dental Center is not simply limited to the 31 jobs and $2.4 million in
payroll created by center operations – the center generated an additional 13 jobs and
$608,000 in payroll in the community as a result of the indirect and induced impact of
normal business and clinical operating activity.

12
● ● ● The goal of the ACCESSAllNevadaplan is to preserve, strengthen, and expand the Community Health Center safety-net in Nevada.
● ● ●
Goals and Objectives
The goal of the ACCESS All Nevada plan is to preserve, strengthen, and expand the
Community Health Center safety net in Nevada. The vision of all Community Health
Centers in Nevada is to double the number of medically underserved Nevadans who do
not have a health care home by the year 2015 – in particular, the centerpiece of the
ACCESS All Nevada plan is to increase the number of patients served by the state’s
Community Health Centers from 79,163 in 2008 to 160,000 by 2015. With additional
resources, staffing, and support, an expansion of CHC sites and services could offer
financially accessible and conveniently located primary care and preventive services –
including a full range of medical, dental, behavioral health, and pharmacy services – to
every uninsured person in Nevada who currently lacks a health care home. CHC service
expansion also includes increased access to specialty
care services, including specialty services provided
through the statewide telemedicine network.
As such, the ACCESS All Nevada plan is consistent with
our state’s efforts: (1) to preserve, strengthen, and
expand the health care safety net in Nevada and the
United States; (2) to increase the number of medically
disenfranchised Nevadans served by CHCs; and (3) to
support the ACCESS for All America goal of serving 30
million patients by the year 2015. By 2015, Nevada’s
Community Health Centers will serve as the statewide
foundation for a high‐quality, performance based
health care system, grounded in primary care and the establishment of health care
homes for medically underserved Nevadans. Nevada CHCs will also provide access to
mental health, dental, and pharmacy services in every health center, as well as specialty
referrals and specialty telemedicine consultations for CHCs patients at every CHC site in
rural and frontier Nevada.
The following strategies and requirements outline steps that will be undertaken by
Great Basin Primary Care Association, Community Health Centers and tribal clinics, and
other safety‐net providers to achieve ACCESS All Nevada goals and objectives by 2015.
13
● ● ● GBPCA estimates that a minimum 12 new start or expansion sites will need to be developed in Nevada by 2015. ● ● ●
● ● ● Expansion efforts must include not only existing CHCs and primary care providers interested in applying for FQHC status but also tribal health centers across the state. ● ● ●
Strategies and Requirements
Over the past five years, the number of Community Health Center delivery sites in
Nevada has grown by nearly 100 percent. In order to meet the ACCESS All Nevada goal
of serving an additional 80,000 medically disenfranchised
Nevadans, a similar level of CHC delivery‐site expansion will
need to occur between now and 2015. Great Basin Primary
Care Association (GBPCA) estimates that a minimum 12
new start or expansion sites will need to be developed in
Nevada by 2015. GBPCA also estimates that the number of
primary care physicians, physician assistants, and nurse
practitioners serving in CHC sites will need to increase from
a current 46 full‐time equivalent (FTE) personnel to 92 FTE
to achieve a functional level of service in new and existing
sites by 2015. In turn, the service delivery and staffing expansion envisioned by ACCESS
All Nevada will require comprehensive strategies to expand operating and capital
revenue to CHCs in Nevada, as well as strategies to increase the number of primary care
physicians and other clinicians required to staff new and expanded CHC services in
Nevada.
The development of new service delivery points will be a combination of expansions by
current CHCs, the expansion of school‐based CHC services,
tribal applications for Section 330 funding, and new
community organizations in medically underserved
communities. The development of new delivery sites also
includes the exploration of “FQHC look‐alike status” for
existing primary care practices in both rural and urban areas
of Nevada. Both Nevada Health Centers and Health Access
Washoe County are exploring expansion opportunities based
on the successful opening of CHC delivery sites in Clark,
Storey, and Washoe Counties over the past two years and
areas of the state that remain medically underserved areas.
Additionally, community development and health center
feasibility activities are being undertaken in thirteen tribal
clinics statewide, including the Washoe Tribe of Nevada,
which is currently developing a Section 330 application for
health center funding support. Expansion efforts must include not only existing CHCs
14
● ● ● While ARRA funding represents a major infusion of much-needed capital and operating revenue for Nevada’s CHCs, additional long-term revenue is needed to support CHC service and expansion and capital improvement projects envisioned in ACCESS All Nevada. ● ● ●
and primary care providers interested in applying for FQHC status but also tribal health
centers across the state.
Expand Capital and Operating Revenue
A principal obstacle to the expansion of Community Health Centers in Nevada is the
continuing challenge of capital development – that is, building new facilities in medically
underserved areas of Nevada, renovating and expanding existing CHC facilities serving
low‐income and uninsured Nevadans, and ensuring that all CHCs are wired with cutting‐
edge health information technology (HIT). The development of new CHC sites and
services and the recruitment health professionals to staff these facilities will thus
require a significant expansion of capital and operating revenue to Community Health
Centers in Nevada over the next five years.
Funding recently released through the American Recovery and Reinvestment Act of
2009 (ARRA) will allow Nevada CHCs to take major steps toward addressing the
operating and capital needs of CHC expansion over the next couple of years. ARRA
funding included a historic investment in Community
Health Centers of $2 billion. Earlier this year the
Department of Health and Human Services (DHHS)
released $155 million to establish 126 new health
centers. Of this funding stream, Nevada received
$478,135 which will support care for an additional
2,770 patients and will result in 20 jobs created or
retained in Nevada. DHHS also released $338 million
in so‐called Increased Demand for Services (IDS).
Nevada health centers received IDS funding totaling
$1.46 million which will allow Nevada CHCs to serve
an additional 6,432 patients. Finally, in the coming
year, Nevada is slated to receive $3.08 million in
ARRA funding to support CHC capital improvement
projects.
While ARRA funding represents a major infusion of
much‐needed capital and operating revenue for
Nevada’s CHCs, additional long‐term revenue is
needed to support CHC service expansion and capital
improvement projects envisioned in ACCESS All Nevada. Historically, Nevada health
15
centers have relied on federal funds, state and local grants, and limited capital
campaigns to maintain and expand existing CHC sites and services. Today, however,
innovative strategies must be undertaken to assure that health centers have the capital
and operating revenue needed to provide high quality services to existing patients and
to expand services to the thousands of medically disenfranchised Nevadans discussed in
this plan.
Between now and 2015, strategies and requirements to expand capital and operating
revenue to community health centers in Nevada must include:
Ongoing efforts to leverage ARRA funding to help with CHC capital infrastructure
needs and the full implementation of electronic medical records in every CHC in
Nevada, including costs for system maintenance, upgrades, and information
technology staff.
Advocacy with Nevada’s congressional delegation for reinstatement of statutory
authority of CHCs to use federal expansion dollars for the construction.
Work with safety‐net advocates in Nevada and state lawmakers to establish a
funding stream to Nevada CHCs through state line‐item funding.
Collaboration with the same safety‐net advocates and state law makers to
ensure that Nevada Medicaid and Nevada Checkup payment and reimbursement
policies do not have a negative impact on the ability of CHCs to support service
expansion or the ability of CHCs to accumulate capital for expansion and other
capital improvement projects.
Work with national advocates and federal lawmakers to develop a new paradigm
of CHC capital financing that includes a federal credit enhancement source that
can be used in conjunction with tax‐exempt bonds; a tax credit allocation
specifically for health centers; and a single national issuer to provide streamlined
access to the tax exempt bond and tax credit markets.
Advocacy for improved reimbursement for CHC services from Medicare,
Medicaid, Nevada Checkup (SCHIP), and other programs, including
reimbursement for telemedicine services and consultations.

16
Work with Nevada’s congressional delegation on legislation that would authorize
FQHCs to form Managed Care Entities and other efforts resulting in a reduction
of the uninsured patient mix of CHCs in Nevada.
Coordinate CHC legislative and advocacy efforts with other safety net providers
and access‐expansion efforts in Nevada, including Great Basin HealthNet based
in southern Nevada and Access to Healthcare Network based in northern
Nevada.
Strengthen Healthcare Workforce Education, Training, and Development to Ensure an Adequate Primary Care and Clinical
Workforce to Staff Community Health Centers in Nevada
A second major obstacle to the expansion of Community Health Centers is the
continuing challenge of recruiting and retaining primary care physicians and clinicians to
staff centers. Over the past decade, the shortage of primary care providers and other
health care workers has worsened across the nation. Consequently, fast‐growing states
like Nevada have experienced difficulties in recruiting health care professionals as the
demand for health care has grown. Community Health Centers and other safety‐net
providers in medically underserved areas of the state have found themselves at a
competitive disadvantage with employers offering better salaries in more affluent urban
practices and facilities in Nevada. Thus, as the reach and capacity of Nevada’s CHCs
continues to grow, there must be concerted strategies to address the root causes of
health workforce shortages and efforts to create incentives for clinical graduates to
choose primary care and services in medically underserved areas of Nevada.
Between now and 2015, strategies and requirements to strengthen health workforce
education, training, and development to ensure an adequate primary care and clinical
workforce to staff Community Health Centers in Nevada must include:
Work with Nevada’s congressional delegation for the reauthorization and
expansion of the National Health Service Corp (NHSC), and advocate for increase
funding and eligibility for National Health Service Corp and other federally‐
supported loan forgiveness programs.
17
Educate and inform Nevada’s congressional delegation on the need to
strengthen and expand Title VII and Title VIII health professions training
programs to continue to produce the needed primary care workforce, promote
service in underserved communities, and promote a racially diverse and
culturally competent workforce.
Work with safety‐net advocates in Nevada and state law makers to increase
funding and eligibility for Nevada Health Service Corp and other state‐supported
loan forgiveness programs for primary care physicians and health professionals
willing to practice in medically underserved areas of the state.
Efforts to increase tuition‐assistance funding and eligibility for health
professionals supported through the Nevada Western Interstate Commission for
Higher Education Program for health professionals willing to practice in
medically underserved areas of the state.
Increase utilization of foreign medical school graduates through the J‐1 Visa
Waiver Program administered by the State of Nevada Primary Care Development
Center (PCO).
Engage secondary educational institutions, the Nevada Area Health Education
Centers Program (AHEC), Nevada Office of Rural Health (NORH), and health care
education programs in the Nevada System of Higher Education (NSHE) in the
development of “grow our own” strategies designed to steer Nevada youth into
the health professions and to encourage them to return to their communities to
provide health care continuity.
Expand partnerships with medical, nursing, dental, and allied health programs in
the Nevada System for Higher Education (NSHE), including the development of
medical residency slots in rural and other medically underserved areas of the
state and the development of rotations in community‐based, ambulatory care
settings such as Community Health Centers.

18
Challenges and Opportunities
For Nevada’s Community Health Centers
Between now and 2015, Nevada’s Community Health Centers face daunting challenges
to providing primary care services to their communities and expanding access to care to
thousands of medically disenfranchised Nevadans who lack a health care home. These
challenges include state and regional health workforce shortages, rising numbers of
uninsured Nevadans and the erosion of employer‐sponsored coverage, a severe
economic recession and associated state budgetary crisis, and the uncertain future of
CHCs in current health reform efforts. Nonetheless, goals and strategies envisioned
with ACCESS All Nevada represent a unique opportunity for Community Health Centers
to improve access to medically disenfranchised Nevadans and medically underserved
areas of the state at a time when those needs have never been greater. Making the
goals of improved access in Nevada a reality will require significantly increased financial
resources and renewed partnerships among Community Health Centers, Great Basin
Primary Care Association, and those public and private agencies that provide safety‐net
services in Nevada.

19
Background Data and Reports
The following data and reports were utilized in the development of the ACCESS All Nevada plan.
Abramson, S.S. Holes in the Net: Surveying the Impact of the Current Economic Recession on the
Health Care Safety Net. American Public Health Association Issue Brief (April 2009).
Great Basin Primary Care Association. Nevada’s Study of Uninsured Populations. (January 2009).
Great Basin Primary Care Association. Application for PCA New Competition (HRSA‐09‐181).
(November 2008).
National Association of Community Health Centers. Primary Care Access: An Essential Building
Block of Health Reform (March 2009).
National Association of Community Health Centers. A Sketch of Community Health Centers:
Chart Book 2009 (March 2008).
National Association of Community Health Centers. Access Transformed: Building a Primary
Care Workforce for the 21st Century (August 2008).
National Association of Community Health Centers. Access Capital: New Opportunities for
Meeting America’s Primary Care Infrastructure Needs (March 2008).
National Association of Community Health Centers. Access Granted: The Primary Care Payoff
(August 2007).
National Association of Community Health Centers. Access Denied: A Look at America’s
Medically Disenfranchised (March 2007).
Packham, J. and T. Griswold. Nevada Rural and Frontier Health Data Book, 2009 Edition.
Nevada Office of Rural Health (January 2009).
Price, S., J. Packham, and T. Griswold. The Impact of the Elko County Health Care System on the
Local Economy. Nevada Office of Rural Health (February 2008).
Uniform Data System (UDS) reports generated by Health Access Washoe County (HAWC) and
Nevada Health Centers. (July 2009)

515 West 4th Street
Carson City, NV 89703
Tel: 775‐887‐0417
Fax: 775‐887‐3562
www.gbpca.org