Embed Size (px)
Citation preview

268
JOURNAL OF PALLIATIVE MEDICINEVolume 9, Number 2, 2006© Mary Ann Liebert, Inc.
Access to Hospice for African Americans: Are They Informed about the Option of Hospice?
RAMONA L. RHODES, M.D.,1 JOAN M. TENO, M.D., M.S.,1 and LISA C. WELCH, Ph.D.2
ABSTRACT
Objective: To examine whether African Americans are informed about hospice services, andto examine demographic or disease factors that may influence receipt of information abouthospice.
Design: Retrospective cohort study.Setting: Twenty-two states that accounted for nearly 70% of deaths in the United States in
2000.Measurements: A mortality follow-back survey was conducted. Based on sampled death cer-
tificates from 22 states, informants listed on the death certificates were contacted by telephoneregarding the decedent’s dying experience. Among those persons not receiving hospice ser-vices, the respondents were asked if hospice was presented as an option for care at the endof life.
Results: Of 1578 interviews, 111 decedents were non-Hispanic, African Americans (averageage, 71.5 years; 56% female). Of those, 32 (30.3%) of the decedents received hospice services,while 77 (68.5%) did not. Slightly more than half of African Americans (60; 53.8%) were notinformed about hospice services and 12 (8.9%) were informed but did not enroll. Cancer suf-ferers were more likely to be counseled about hospice (p � 0.001).
Conclusion: Slightly more than half of African Americans were not informed about hospiceservices, and of those who were informed, cancer was the leading cause of death. Informa-tion about hospice should be provided to patients regardless of diagnosis, and disseminationof information should be done aggressively in the African American community in an effortto make hospice a viable option for end-of-life care.
INTRODUCTION
IN RESPONSE TO CONCERNS over use of life-sus-taining treatment and inadequate symptom
control, hospice is now a service available to allMedicare participants. Currently there are morethan 2500 hospice programs in operation nation-wide1; however, not all terminally ill patientshave access to the services these programs pro-
vide. Certain minority groups are among thosewho have been found to underutilize hospice—one such group being African Americans. The un-derutilization of hospice by African Americanshas been long-standing. Several studies haveshown that not only were African Americansmore likely to choose more aggressive life-sus-taining treatments,2,3 they were less likely to beenrolled in hospice at the end of life. For instance,
1Center for Gerontology and Health Care Research, Brown University, Providence, Rhode Island.2Department of Sociology and Criminal Justice Studies, Southern Illinois University, Edwardsville, Illinois.
Brief Reports

Greiner et al.4 reported that African Americanswere found to have 40% lower hospice use thanwhites, and that hospice use was negatively as-sociated with African American race/ethnicityindependent of income and access to healthcare.Christakis and colleagues5 found that 92.4% ofMedicare beneficiaries enrolled in hospice werewhite. Additionally, Welch et al.6 found that fam-ily members of African American decedents weretwo and a half times as likely as those of whitedecedents to report one or more problems withbeing informed about end-of-life medical care.Though many factors have been hypothesized ascontributors to this dynamic, the reason for thisunderutilization has never been clearly under-stood.
No studies were identified that examined theinfluence of providing information about the useof hospice services by African American patients.Lack of awareness may serve as a potential bar-rier to the use of hospice services for AfricanAmericans. Using a 22-state mortality follow-back survey, we examined the use of hospiceamong African Americans and whether lack ofbeing informed represents a potential barrier tohospice use. Additionally, we examined the char-acteristics of those African Americans who wereinformed about hospice services.
METHODS
This cross-sectional, retrospective study useddata from a mortality follow-back survey ofdeaths for the year 2000. The survey involvedcontacting the informant listed on the death cer-tificate (usually a close family member) by tele-phone to ask whether he or she was one of thepeople most knowledgeable about the decedent’slast few weeks of life. If not, the informant wasasked to identify another person who wouldknow about the circumstances of the decedent’sdeath and dying experience. The interview coop-eration rate was 65%. The details of the study de-sign have been published previously7; informa-tion is also available at �www.chcr.brown.edu/dying/info4researchers.htm�.
Use of hospice services
The following question was used to ascertainwhether the decedent utilized hospice services,“At any time during the last month of (his/her)
life was hospice involved in the care of (patientname)?” For those persons not using hospice ser-vices in the last month of life, the respondent wasasked, “As far as you know was hospice pre-sented as an option for (patient)’s care?”
Sample
Decedents were selected based on a two-stageprobability sample, which was designed to selectstates and then individuals within states.7 Thestates chosen were based on 1998 U.S. mortalitydata. Eight states accounted for nearly one half ofthe deaths in the United States in 1998,and werepurposely selected. Seventeen of the remaining42 states were randomly selected; however, 3states chose not to participate. Deaths in the 22sampled states accounted for 70.4% of all deathsfor the year 2000. Of those, 111 decedents wereAfrican American. Based on sampling design,these 111 decedents were representative of149,328 African American deaths in the year 2000.
Decedents were categorized as non-Hispanicblack (or African American), non-Hispanic white,Hispanic, or other based on the informant re-sponses. To characterize which non-HispanicAfrican American decedents were informedabout hospice services, we examined age, lead-ing cause of death, type of insurance, level of ed-ucation, whether death was expected or not, andwhether the decedent lived alone.
Analysis
All analyses were done using SUDAAN ver-sion 8.0 (RTI International, Research TrianglePark, NC) in a SAS-based environment (SAS In-stitute, Cary, NC) to account for the complex sam-pling design. A descriptive analysis was done toexamine the percentages of being informed abouthospice and use of hospice services by AfricanAmericans. The association of decedent charac-teristics and being provided with informationabout hospice was examined with either the �2
test for ordinal or dichotomous variables or the ttest for continuous variables.
RESULTS
Baseline characteristics
Table 1 outlines the baseline characteristics ofAfrican American decedents included in the sam-
INFORMING AFRICAN AMERICANS ABOUT HOSPICE 269

ple. Fifty-five percent of decedents were women.The four leading causes of death were heart dis-ease, cancers of various types, dementia, and con-gestive heart failure. Fifty-two percent of AfricanAmerican decedents had some form of advanceddirective.
Hospice enrollment and being informed for African American decedents
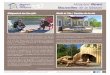
Figure 1 shows the distribution of AfricanAmerican decedents according to hospice enroll-ment and being informed. Of the total number ofAfrican Americans included in the sample, 30.3%chose to enroll in hospice. Almost 9% of the dece-dents (8.9%) were informed about hospice andchose not to enroll. These decedents represent22.6% of the total number of African Americandecedents who were informed about hospice.Slightly more than half (53.8%) of the AfricanAmerican decedents were not informed abouthospice. Respondents for 4.7% of the decedentsdid not know if the decedent had been informedabout hospice, and about 1% of respondents didnot know if the decedent had been enrolled inhospice. The results of our exploratory analysisare shown in Table 2. This univariate exploratoryanalysis was conducted to characterize personsinformed about hospice services versus those notinformed about hospice services. More of thosedying of cancer, the second leading cause ofdeath, were informed compared to the othercauses of death noted (p � 0.001). There were nosignificant differences in gender, type of insur-
ance, and expectation of death associated with be-ing informed about hospice. Other factors in-cluding level of education and living status werenot statistically significant as well.
DISCUSSIONS
Previous research has shown that AfricanAmericans are less likely to enroll in hospice ser-vices. Whether this reflects patient preferences orlimited access to hospice services is unknown. Forinstance, by using the 1993 National MortalityFollowback Survey, Greiner and colleagues4
found that African Americans were less likely toenroll in hospice even after controlling for factorssuch as income and access to health care. Bornand colleagues8 reported that the lack of aware-ness of hospice and the prohibitive cost of healthcare served as barriers to hospice utilization forlow-income urban African Americans. Further-more, although studies have suggested that geo-graphic variations in hospice use favor urbanareas,9,10 those services may not penetrate areaswhere African Americans, members of our eth-nic groups and poor people reside. Our study uti-lized a national sample of death certificatesdrawn from 22 states to examine both the use of
RHODES ET AL.270
TABLE 1. BASELINE CHARACTERISTICS OF AFRICAN
AMERICAN DECEDENTS, n � 111
All decedents All decedentsCharacteristic (n) (%)a
Average age at time of 71.5death, years
Genderb
Female 60 55.9Male 49 44.1
Leading causes of deathHeart disease 43 33.8Cancer 32 31.5Dementia 7 8.0CHF 3 2.3
Advanced directive 58 51.5
aAll percentages are based on weighted values.bGender data were not available for two decedents.CHF, congestive heart failure.
FIG. 1. Percentages of hospice enrollment and being in-formed for African American decedents.

hospice and whether African Americans, specifi-cally, were informed about hospice services. Inour study, thirty percent of African Americandecedents were enrolled in hospice. Another53.8% of the decedents in the sample were not in-formed about hospice services and 8% chose notto enroll. These results suggest that the lack ofparticipation in hospice services may, in part, bethe result of dying persons and their families notbeing informed about the availability of hospice.
Certain limitations should be taken into ac-count when interpreting the results of this study.African Americans were less likely to participatein this survey (p � 0.001).7 Future research needsto oversample African Americans to have ade-quate power to examine the associations of so-ciodemographic and other characteristics withbeing informed about hospice services. Second,because the majority of dying persons are unableto be interviewed in the last month of life, our re-search design was a mortality follow-back surveythat relied on bereaved family members to reporton the use of hospice services and to determinewhether dying persons were informed about the
availability of hospice. While proxies may be in-accurate reporters of subjective states, McPhersonand Addington-Hall11 noted in a summary of theavailable studies, that proxies were able to reporton objective information. Finally, our survey re-spondents noted an increased percentage of hos-pice use of 30% compared to 10.6% nationally for2000.12 This, in part, can be explained by the factthat our survey included nontraumatic deathsonly. Additionally, persons with hospice experi-ence were more likely to agree to participate inthis survey. This response bias may have resultedin an overestimate of hospice use by AfricanAmerican decedents as well as percentages ofAfrican Americans being informed about hos-pice. In spite of these limitations, this is one of theonly national studies to date to examine whethernot being informed about hospice serves as a bar-rier to its utilization in the African American com-munity.
Hospice underutilization in the African Amer-ican community has been long-standing and notfully understood. In our study, one in five per-sons informed about hospice did not utilize this
INFORMING AFRICAN AMERICANS ABOUT HOSPICE 271
TABLE 2. ANALYSIS OF DECEDENTS, INFORMED VERSUS NOT INFORMED
Informed, %a Not informed, %a
n � 42b,c n � 60b p value
Female 51.6 63.8 0.290Cause of death
Heart disease 32.5 51.6 0.007Cancer 32.7 13.4 0.001Dementia 9.4 8.0 0.860CHF 0.0 2.3 0.250
Insurance 0.310Medicare 60.7 73.4Medicaid 2.3 5.5Private 4.5 7.7None 20.0 7.0Other 12.6 6.3
Death (unexpected) 0.080Extremely 17.0 48.1Very much 7.8 13.8Somewhat 22.1 11.7A little 11.4 9.0
Education 0.150Less than HS 47.6 55.9High School 43.4 20.3Some College 7.7 13.54� years of college 0.6 7.8�4� years of college 0.8 2.5
Living Alone 10.4 15.2 0.130
aAll percentages are based on weighted values.bData was not available for 9 decedents.cData was not available for 2 decedents.

option for care at the end of life. Factors such associoeconomic status, mistrust of the health caresystem, religious beliefs, cultural beliefs, and lackof knowledge about hospice have been hypothe-sized as contributors to this dynamic8,13–15; how-ever, few studies have investigated whetherAfrican Americans are informed about hospiceservices. In this national sample of death certifi-cates, bereaved family members reported thatslightly more than one-half of the African Amer-icans were not informed. A second important ob-servation is that the majority (77.3%) of personsinformed about hospice services chose to enrollin hospice. Future research should be done to in-vestigate if information about hospice truly is notbeing disseminated to people of all racial and eth-nic backgrounds. Based on these results, we rec-ommend that an important focus of the future beto counsel persons on the availability of hospiceas an option for end-of-life care.
ACKNOWLEDGMENTS
We gratefully acknowledge financial supportprovided by The Robert Wood Johnson Founda-tion, Grant 037188. We also thank Susan Miller,Ph.D., M.B.A., Lynn McNicoll, M.D., and John B.Murphy, M.D. for their reviews of an earlier ver-sion of the manuscript.
REFERENCES
1. Porter S, Knight CF: Unipac One: The Hospice/Pal-liative Medicine Approach to End-of-Life Care, 2nded. New York: Mary Ann Liebert, Inc., 2003.
2. Hopp FP, Duffy SA: Racial variations in end-of-lifecare. J Am Geriatr Soc 2000;48:658–663.
3. McKinley ED, Garrett JM, Evans AT, Danis M: Dif-ferences in end-of-life decision making among blackand white ambulatory cancer patients. J Gen InternMed 1996;11:651–656.
4. Greiner KA, Perera S, Ahluwalia JS: Hospice usage byminorities in the last year of life: Result from the Na-tional Mortality Followback Survey. J Am Geriatr Soc2003;51:970–978.
5. Christakis NA, Escarce JJ: Survival of Medicare pa-tients after enrollment in hospice programs. N Engl JMed 1996;335:172–178.
6. Welch LC, Teno JM, Mor V: End-of-life care in blackand white: Race matters for medical care of dying pa-tients and their families. J Am Geriatr Soc 2005;53:1145–1153.
7. Teno JM, Clarridge BR, Casey V: Family perspectiveson end-of-life care at the last place of care. JAMA2004;291:88–93.
8. Born W, Geiner KA, Sylvia E: Knowledge, attitudes,and beliefs about end-of-life care among inner-cityAfrican Americans and Latinos. J Palliat Med 2004;7:247–256.
9. Vernig BA, Kind S, McBean M, Fisher E: Geographicvariation in hospice use prior to death. J Am GeriatrSoc 2000;48:1117–1125.
10. Luckan NA, Ostir GV, Freeman JL, Mahnken JD,Goodwin JS: Decreasing variation in the use of hos-pice among older adults with breast, colorectal, lungand prostate cancer. Med Care 2004;42:116–122.
11. McPherson CJ, Addington-Hall JM: Judging the qual-ity of care at the end of life: Can proxies provide re-liable information? Soc Sci Med 2003;56:95–109.
12. National Home and Hospice Care Data: Centers forDisease Control and Prevention. �www.cdc.gov/nchs� (Last accessed November 16, 2004.)
13. Jackson F, Schim SM, Seeley S, Grunow K, Baker J:Barriers to hospital care for African Americans:Problems and solutions. J Hosp Palliat Nurs 2000;2:65–72.
14. Reese DJ, Ahern RE, Nair S, O’Faire JD, Warren C:Hospice access and use by African Americans: Ad-dressing cultural and institutional barriers throughparticipatory action research. Soc Work 1999;44:549–559.
15. Reese DJ, Melton E, Ciaravino K: Programmatic bar-riers to providing culturally competent end-of-lifecare. Am J Hosp Palliat Care 2004;21:357–364.
Address reprint requests to:Ramona L. Rhodes, M.D.
Center for Gerontology and Health Care ResearchBrown University2 Stimson Avenue
Box G-ST 311Providence, RI 02912
E-mail: [email protected]
RHODES ET AL.272