-
ACEs and ABI: A Trauma-Informed Approach
Noshene Ranjbar M.D.University of ArizonaNovember 11, 2020
-
Disclosures
The presenter has no financial conflicts of interest to
disclose.
Assistant Professor, University of Arizona Department of
Psychiatry
Faculty, Andrew Weil Center for Integrative Medicine
Faculty, The Center for Mind-Body Medicine
Faculty, Integrative Psychiatry Institute
Board Member, American Board of Integrative Medicine
-
Learning Objectives
Define Developmental trauma and adverse childhood experiences
(ACEs)
Understand Psychoneuroimmunology of trauma & ACEs as related
to acquired brain injuries (ABI)
Gain Insight from the polyvagal theory and mind-body medicine as
related to the impact and mitigation of ACES
-
Overview
Stress, ACEs and Trauma-Informed Care
How Does ABI fit into ACEs?
Caregiver Factors
An Integrative Approach
-
Case Example of ABI and ACEs: Ana
• 11-year old girl, suddenly developed seizures after a fever
and GI illness
• Generalized tonic-clonic, intractable• Ambulance called,
rushed to ED, hospitalized• Unable to break seizures despite
multiple medication trials• Induced medical coma for 6 weeks•
Diagnosed with Febrile Infection Related Epilepsy Syndrome (FIRES)•
Eventually controlled seizures with high dose CBD oil as part of
a
clinical trial, in addition to anti-epileptic meds
https://www.abc.net.au/news/2017-10-11/how-teenage-girls-around-the-world-want-to-create-change/9030504
-
Pre-ABI Medical and Developmental History• Healthy, met all
developmental milestones
• No prior significant illnesses, surgeries, or injuries
• No medications
• Enjoyed dancing, cheerleading, and playing in the school
band
• Social, easily made friends, got along well with parents and
older brother Jose
• All A’s in school
-
Pre-ABI Family History
• Dad on service-connected disability with the VA due to severe
PTSD from Iraq, also alcohol use disorder
• Mom with anxiety and depression, executive director of a
marketing company
• Paternal grandfather with alcoholism and depression
history
• Older brother, healthy
-
Pre-ABI Social History• Both parents Hispanic, very large
extended family
• At times Dad would get drunk and yell at Mom and/or Annie and
her brother
• Mom managed most of the finances and household activities
while working full time
-
ABI Treatment Course
• Numerous hospitalizations and medication trials
• Due to specialized needs, most appointments and
hospitalizations occurred 2 hours from home
• Regression of emotion & behavioral regulation, memory and
cognition
• Utilized biofeedback, neurofeedback, mind-body skills
training, and individual psychotherapy
• Puberty and individuation process
• Took appx 1.5 years to regain much of cognitive and executive
function
-
Post-ABI • Mom and Dad divorced 2 years after the start of the
illness
• Jose developed depression and started experimenting with
alcohol at age 14, significant anger towards Ana
• Traumatic incident with Dad • Dog died suddenly due to a
car
accident• Custody battle between Mom and
Dad
https://www.sgdivorcelawyer.sg/blog/getting-a-divorce-in-singapore-in-2020
-
Post-ABI, Cont’d
• 6 years post-ABI, age 17• Some improvement in relationship
with
Jose• Final year of high school• Back to dancing and playing
music• Still attends monthly individual
psychotherapy • Avoiding re-unification counseling with
Dad
-
Some questions to consider:
• What were some of the potential pre-disposing factors to Ana’s
ABI?
• What resiliency factors helped Ana in recovery?• How has Ana’s
ACE changed from pre- to post-ABI?• What impact has Ana’s ABI
treatment course had on her
neurodevelopment and current prognosis?• How have her caregivers
managed her ABI and what impact
has their stress and ability to manage their stress had on the
outcome?
-
Stress, ACEs & Trauma
-
Stress
• Hans Selye, an endocrinologist, defined stress in 1936 as “the
[physiological] response of the body to any demand for change”.
• Eustress: beneficial stress -either psychological, physical
(i.e. exercise) or biochemical/hormonal. Greek for “good
stress”
14
-
We are born with our brainstem and limbic system hardwired for
survival
Dr. Dan Siegel, Hand Model of the Brain:
https://www.youtube.com/watch?v=gm9CIJ74Oxw
https://www.youtube.com/watch?v=gm9CIJ74Oxw
-
Trauma
-“injury”— to our mind, body, and spirit
“Individual trauma results from an event, series of events, or
set of circumstances that is experienced by an individual as
physically and emotionally harmful or threatening and that has
lasting adverse effects on the individual’s physical, social,
emotional, or spiritual well-being” (SAMHSA, 2014)
-
Causes of TraumaWar
Torture
Natural disasters
Racism and Historical Trauma
Poverty
Child Abuse
Spousal Abuse
Rape and other violent crimes
Health crisis—life threatening illness
Health care itself
Witnessing any of these
In fact, all of us have been or will be traumatized 17
-
Who Does Trauma Affect?• 82% of individuals in the U.S. have
experienced at
least one traumatic event in their lifetime• 8-18% of
trauma-exposed individuals develop PTSD• 7-19% develop Major
Depressive Disorder• “Co-morbid” conditions with PTSD have been
reported to be as high as 37%• Risk of developing PTSD after
trauma exposure is
twice as high in women than in men
18Patel R, Spreng RN, Shin LM, Girard TA. Neurocircuitry models
of posttraumatic stress disorder and beyond: A meta-analysis of
functional neuroimaging studies. Neurosci Biobehav Rev. 2012
Oct;36(9):2130-42.
-
Post-Traumatic Stress Disorder
In PTSD there may be a prolonged Fight or Flight Response with
agitation, hyper-arousal, etc.
Freezing is also a response to overwhelming trauma and a
possible prelude to PTSD, and an ongoing response characteristic of
PTSD.
• Parasympathetic system overdrive• Feeling stuck, inert, unable
to feel or act• Avoidance• Possible long-term consequences –
depression and
withdrawal• More research necessary
19
-
Post-Traumatic Stress DisorderPTSD is a kind of fixation—the
characteristics that follow describe
some of its subjective and objective components. They do not
adequately convey the experience.
Re-experience of the Original Trauma• Intrusive recollections•
Nightmares• Flashbacks• Intense distress at reminders of the
trauma
20
-
Post-Traumatic Stress Disorder
• Sleep disturbance• Persistent increased arousal• Irritability•
Concentration impairment• Hyper-vigilance• Exaggerated startle
response• Heightened physiological reactivity
• Increased heart rate• Sweating
21
-
Forgotten or hidden trauma?
-
Understanding Trauma
Complexity… spectrum
Not caused by the event itself
May or may not lead to…
Any experience that overwhelms the system
May come to any or all of us
and, associated with zip code…
Not a weakness
Can transform into a strength
-
Trauma and the Brain
24
-
Trauma Physiology
Trauma may cause prolonged changes in:
• Brain structure• Systemic neurological
functioning • Cellular performance• Endocrine function• Memory
processes
(c) 2017 Center for Mind-Body Medicine
-
Trauma Physiology, Cont’d
1. Hyperactivation of the Amygdala2. Alteration in
Hippocampal
Functioning and Volume3. Hypoactivation of key prefrontal
cortex areas: hypersensitivity to potential trauma and decreased
ability to mobilize judgment, make decisions, feel grounded in body
and have empathy for others
26Patel R, Spreng RN, Shin LM, Girard TA. Neurocircuitry models
of posttraumatic stress disorder and beyond: A meta-analysis of
functional neuroimaging studies. Neuroscience & Biobehavioral
Reviews. 2012 Oct; 36(9):2130-42.
Image credit:
http://sage.buckinstitute.org/wp-content/uploads/2015/12/cerebro-ganglios-basales-cortex.png
-
Hormonal Changes• Increased levels of
Catecholamine, CRF, ACTH, cortisol, opioids
• Interruption of circadian cycles• Inhibition of conscious
memory
(amnesia) and dissociation• Prolonged arousal in animals
may cause permanent change • If more aggressive, then
aggression• If defensive, then become more
inhibited• Feedback loop
27
Image credit:
http://image.slidesharecdn.com/metabolicresponsetoinjury-140213142949-phpapp01/95/metabolic-response-to-injury-12-638.jpg?cb=1392301873
Bremner JD, Narayan M. The effects of stress on memory and the
hippocampus throughout the life cycle: implications for childhood
development and aging. Development Psychopathology. 1998;
10(4):871-885.
-
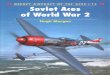
Hormonal Changes - Cortisol
• Short-term healthy stress response• Prolonged stress response•
Physiological effects↑ Abdominal fat deposits↓ Sensitivity of fat
cells↑ Cholesterol↑ Appetite ↓ Immunity ↓ Cells in
hippocampusCompromise in gut function & the microbiome
28
Hypothalamus
Corticotropin Releasing Hormone (CRH)
Anterior Pituitary
Adrenocorticotropin (ACTH)
Adrenal Cortex
Cortisol
-
Chronic/excess Stress Influences the Onset and Course of
Virtually All Illness
Coronary Heart Disease Gastrointestinal Dysfunction
Progression of HIV/AIDS Headaches
Recurrence of Herpes Premature Death
Asthma Eczema
Common Cold Anxiety and related disorder
Acute Clinical Incidents such as Cardiac arythmia, sudden
Death
Cancer
Depression Sleep-related ailment
Obesity PTSD
Diabetes Alzheimer's and cognitive decline
Pain and Chronic Pain Cellular Aging
(c) 2017 Center for Mind-Body MedicineSource: Institute of
Medicine
29
-
The Polyvagal Theory
-
1. “We start out trying to use our “social engagement system” to
look at each other and resolve things warmly; that’s our first,
myelinated vagus parasympathetic circuit.”
2. “If social engagement fails, we devolve into more primitive
fight/flight animals, where our sympathetic circuits take
over.”
3. “And if that fails, our ancient reptilian unmyelinated vagus
circuit takes over and knocks us out into immobilization, called
dissociation in humans.”
-
Credit: Peter Levine, PhD
(c) 2017 Center for Mind-Body Medicine 33
-
“Tend and Befriend” Modifies Fight/Flight/Freeze Responses
• Mediated by oxytocin (from the pituitary gland)
• Potentiated by opioids and estrogen• Reduces SNS activity and
cortisol release• Is inhibited by naloxone, an opiate
antagonist
34Taylor S., et al. (2003). Biobehavioral responses to stress in
females: tend and befriend, not fight or flight. Psych Rev.,
107:411-429.
-
The Autonomic Nervous System
The Gas PedalSympathetic
Healthy: respond to demandsExcess: “Fight or Flight”
Response
The BrakesParasympathetic
Healthy: Relax, Rest, & RestoreExcess: “Freeze” Response
https://optimizeme.nl/en/blog/2017/03/03/measure-resilience-heart-rate-variability-using-smartphone/?noredirect=en_US
-
Childhood or Developmental Trauma
36
-
37http://image.slidesharecdn.com/scunthorpeteacherspdfjan2015-150104153728-conversion-gate01/95/attachment-trauma-emotional-regulation-in-school-to-make-sense-of-nonsensical-behaviour-teachers-safeguarding-conference-barton-local-collaborative-trust-january-2015-4-638.jpg?cb=1420386741
-
Adverse Childhood Experiences Study(ACES)
• Followed 17,000 people in Southern California since 1995
(http://www.cdc.gov/violenceprevention/acestudy/)
• Felitti and others• Assessed for stressful childhood
experiences, found
significant correlations to prevalence of chronic disease
(examples: autoimmune, pain/headaches, heart disease), health risk
behaviors (alcohol/drug use, obesity/over eating, smoking), mental
health, reproductive health, etc.
• Extensive subsequent studies, now being used in primary care,
schools, etc.
© Embody Your Mind, LLC
http://www.cdc.gov/violenceprevention/acestudy/
-
ACE – List of Stressors• Physical abuse• Sexual abuse• Emotional
abuse• Physical neglect• Emotional neglect• Mother treated
violently• Household substance abuse• Household mental illness•
Parental separation or
divorce• Incarcerated household
member
© Embody Your Mind, LLC
Source: npr.org
-
Experiential Activity
What is your ACE score?
-
Experiential Activity
What is your resilience score?
-
ACE – Key Findings
• Childhood trauma was very common, even in employed white
middle-class, college-educated people with great health
insurance
• Direct link between childhood trauma & adult onset of
chronic disease, depression, suicide, being violent and a victim of
violence
• More types of trauma → ↑ risk of health/social/emotional
problems• People usually experience >1 type of trauma – rarely
is it only sexual
abuse or only verbal abuse, etc.
-
ACE – Key Findings
• The higher your ACE score, the higher your risk of health,
social and emotional problems
• 2/3 had at least 1, 87% of those respondent had 2 or more
• Example correlations: ACE score ≥ 4 → ↑likelihood of chronic
pulmonary lung disease 390%; hepatitis 240%; depression 460%;
suicide, 1,220%
-
ACE score ≥6 associated with:
• 273% ↑ odds of reporting depression• 2436% ↑ odds of
attempting suicide• 373% ↑ odds of reporting drug use• 284% ↑ odds
of reporting moderate-heavy drinking after
adjusting for sociodemographic factors (Merrick 2017)
-
Demographics
• Original study participants -- mostly white,
middle/upper-middle class, college-educated, employed, with access
to quality health care
• Implications – rates are very high across society;
marginalized populations often have higher rates of exposure
-
Image Credit: http://www.acestudy.org
See http://communityresiliencecookbook.org/by-the-numbers/ for
additional learning
http://communityresiliencecookbook.org/by-the-numbers/
-
Expanded list of ACEs may include:• sibling and peer
victimization• bullying• medical procedures, illness, surgery•
property crimes • parental death when you were a child • community
violence • spanking • racism• losing a parent to deportation•
living in an unsafe neighborhood• involvement with the foster care
system
• parent experiencing life threatening illness • being homeless•
living in a war zone• being an immigrant• moving many times•
witnessing a sibling being abused• witnessing a parent or other
caregiver or
extended family member being abused
• involvement with the criminal justice system• attending a
school that enforces a zero-
tolerance discipline policy
© Embody Your Mind, LLC
-
Mechanisms still being elucidated:
• Development of coping mechanisms – eating, smoking,
promiscuity, alcohol and other self-medicating
• Related to the complex effects of unrelieved stress –
impacting CNS/ANS neurodevelopmental – endocrine/HPA, inflammation,
immune response (mind-body medicine, psychoneuroimmunology)
• Epigenetic mechanisms• Psychological inflexibility recently
found to be a significant mediator between
ACEs and depression/anxiety states (Makriyanis et al. 2019)
-
Shared Neurophysiological Mechanisms
Changes in neurochemistry
Alteration to autonomic
activity
Alteration to hypothalamic-
pituitary-adrenal (HPA)
neuroendocrine axis
Breakdown of faciliatory and
inhibitory nociceptive physiology
Breakdown of inflammatory and immune
processes Whole System State: Multi-Directional Changes &
Interactions
© Embody Your Mind
-
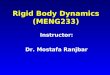
ACEs, Chronic Stress, and/or Trauma May Impact Autonomic Nervous
System Physiology Mind-Body Skills
Training Can Assist with Improving
Regulation Capacity Chronic Over-
Activation/ Hyper-Arousal StatesExample Symptoms: High Tone,
Inability
to Relax, Anxiety
Optimal Range for Eustress,
Performanceand
Homeostasis- - - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - - - - - - - - -
- - - - - - - - - - - - - - - - - - - - - - - - -Sympathetic –
Activate (The “Gas Pedal”)
Parasympathetic – Settle (The “Brake Pedal”)
,
Chronic Shut-Down/ Hypo-Arousal States
Example Symptoms: Fatigue, Lethargy, Low Mood, Weakness,
FaintingRanjbar & Erb 2019
-
Mitigating Influences
• Education• High quality parenting programs, primary
prevention• Wide-spread MB self-care skills training• Buffer: safe,
stable, nurturing relationships and environments
for all children and their families; for all impacted by ACEs•
The valence of your patient/provider (person to person) interaction
is
a key feature in therapeutic outcomes
Metzler et al. (2017) Adverse childhood experiences and life
opportunities: Shifting the narrative. Children and Youth Services
Review (72), 141-149.
https://doi.org/10.1016/j.childyouth.2016.10.021 © Embody Your
Mind, LLC
https://doi.org/10.1016/j.childyouth.2016.10.021
-
© Embody Your Mind, LLC
PCEs – Positive Childhood Experiences
The PCEs score included 7 items asking respondents to report how
often or how much as a child they: (1)felt able to talk to their
family about feelings; (2)felt their family stood by them during
difficult times; (3)enjoyed participating in community traditions;
(4)felt a sense of belonging in high school (not including those
who did
not attend school or were home schooled);(5)felt supported by
friends; (6)had at least 2 nonparent adults who took genuine
interest in them; and(7)felt safe and protected by an adult in
their home.
Bethell C, Jones J, Gombojav N, Linkenbach J, Sege R. Positive
Childhood Experiences and Adult Mental and Relational Health in a
Statewide Sample: Associations Across Adverse Childhood Experiences
Levels. JAMA Pediatr. Published online September 09, 2019.
doi:10.1001/jamapediatrics.2019.3007
-
PCE Study – Results/Relevance
• A dose-response association with adult mental and relational
health, analogous to the cumulative effects of multiple ACEs
• PCEs may have lifelong consequences for mental and relational
health despite co-occurring adversities such as ACEs
• Supports the salutogenic model and WHO’s definition of health
as reflecting well-being despite the presence or absence of
illness, injury, disease, or adversity
• A joint inventory of ACEs and PCEs, such as the positive
experiences assessed here, may improve efforts to assess needs,
target interventions, and engage individuals in addressing the
adversities they face by leveraging existing assets and
strengths
-
© Embody Your Mind, LLC
Asking as treatment?
• Biopsychosocial evaluation (asking the questions in medical
examination) → ↓35% in DOVs* – n=130,000 patients*
• Comparison - only 11% reduction in DOVs* in a sample of 11,000
patients for traditional biomedical evaluation where the
elicitation of the context of life history is not a part of the
subjective/intake
• *Felitti, V.M. (2017). Future Applications of the Adverse
Childhood Experiences Research. Journal of Child & Adolescent
Trauma, 10, 205–206.
• Recent: California implementing widespread screening 2019-2020
(Dr. Burke-Harris)
*DOV=doctor office visits
-
CulturalCollectivist Influence
Language
Traditions Values
BeliefsHistory
Existential
Structural/PhysicalCommunity/Society
Built & Natural EnvironmentOrganizational/Institutional
Systemic/Policy
RelationalInterpersonal
Social
IndividualExperience
PhysicalCognitiveEmotionalSpiritual
Description: Individuals are embedded within various constructs
of “environment” (social, structural, physical, cultural) with all
layers having complex interactions within the whole of their
experience. Cultural-Ecological Model
-
Image Credit: worldreliefdurham.org
-
Shame?• Deep, often subtle/unconscious, painful emotion• A sense
of being fundamentally flawed, inferior,
inadequate, “wrong at one’s very core”• Linked to blame/fault in
one’s experience• Universal, though experientially & culturally
influenced• If history of childhood abuse, stress, trauma,
bullying,
marginalization, unstable emotional environment, etc. –
likelihood for shame as an unconscious informant to one’s
experience is increased
• Normalize experience – listen, validate, enactive compassion,
non-fixing stance, presence…
© Embody Your Mind, LLC
-
© Embody Your Mind, LLC
Trauma-Informed Care Practical ApplicationsHistory Taking
• ”Look back, but don’t stare…”• Scope of practice• Resourcing,
orienting, grounding skills • Application of awareness, expression
and regulation skills
influences and re-educates trauma biology without directly
addressing/”treating” the trauma content
• If it arises…
-
© Embody Your Mind, LLC
How to inquire?• Presence, relaxed confidence/comfort, and
functional education are
critical… • Remember from the subjective overview: “Even if you
think it has
nothing to do with your present concern, I am wondering if
you’ve experienced any accidents, injuries, or trauma…” (ACEs
included…)
-
62
Image credit:
http://www.slideshare.net/JaneGilgun/resilience-adult-attachment-in-cases-of-child-trauma/24
-
63
Image credit:
http://www.slideshare.net/JaneGilgun/resilience-adult-attachment-in-cases-of-child-trauma/13
-
64Image credit:
http://www.slideshare.net/JaneGilgun/resilience-adult-attachment-in-cases-of-child-trauma/13
-
Historical Trauma
65Image credit:
https://laramieharlow.files.wordpress.com/2013/12/historical-trauma.png
-
Historical Trauma
66
•
•
-
•Pain that is not transformed... gets transmitted
• Richard Rohr
67
-
Is ABI considered an ACE?
-
Common Causes of ABI
• Strokes• Lack of oxygen to the brain• Blows to the head-- AKA
traumatic brain injury (TBI).
-
Common Causes of TBI
• Road traffic accidents• Falls• Sporting injuries• Violence •
Violent physical child abuse
-
Consequences of ABIs
• Impairments to physical, mental, cognitive, emotional &
social functioning
• Symptoms sometimes readily observed, but many times subtle and
can go undetected
• Hemiplegia • Epilepsy• Anxiety and depression• Executive
dysfunction and cognitive difficulties• Personality change
-
Consequences of ABI, Cont’d
• Potential indirect consequences: • Unemployment• Social
isolation• Relationship breakdown• Substance use • Homelessness•
Other mental health conditions
-
ABI during development
• Many potentially traumatic elements of pediatric injury during
the “event” & beyond
• Injury events are often sudden, painful, and potentially
life-threatening.• Injury can occur from intentional and
unintentional sources, spectrum of
traumatic elements and meanings for each person• Immediate
aftermath of injury may have additional traumatic stressors
including treatment course
-
Early Assessment and Intervention
• Need to identify those at risk for developing PTSD after
injury• Injury severity is not a good indicator of PTSD risk;• Time
constraints in emergency and acute care preclude in-depth
assessment of emotional status of all injured children.
(Screening of ASD symptoms and other risk factors can be
useful.)
• There is a need for practical, effective ways to screen in the
emergency and medical settings
-
ACEs and ABI
-
Prior ACEs impacts recovery from TBI
• Exposure to adverse childhood experiences is associated with
increased risk of traumatic brain injury.
• Specific types of ACEs associated with risk of TBI: childhood
physical abuse, psychological abuse, household member
incarceration, and household member drug abuse
• Clinicians and researchers should inquire about adverse
childhood experiences in all people with traumatic brain injury as
pre-injury health conditions can affect recovery
-
Persons with prior ACEs increases risk for TBI
• Those who experienced sexual abuse, physical abuse, household
mental illness and had incarcerated household members in childhood
had greater odds of reported TBI, after adjusting for age,
race/ethnicity, gender & income
• Those reporting 3 ACEs (AOR=4.16, 95% CI (1.47 to 11.76)) and
4 or more ACEs (AOR=3.39, 95% CI (1.45 to 7.90)) had significantly
greater odds of reporting TBI than those with zero ACEs
• Prevention of early adversity may reduce the incidence of TBI;
however, additional research is required to elucidate the potential
pathways from ACEs to TBI, and vice versa.
Guinn, A. S., Ports, K. A., Ford, D. C., Breiding, M., &
Merrick, M. T. (2019). Associations between adverse childhood
experiences and acquired brain injury, including traumatic brain
injuries, among adults: 2014 BRFSS North Carolina. Injury
prevention, 25(6), 514-520.
-
Purpose:
• Acquired Brain Injuries, caused by a range of illnesses and
injuries, can lead to long-term difficulties
• for individuals; mental health problems, cognitive and
executive impairment and psychosocial
• problems including relationship breakdown, substance abuse and
potentially homelessness. The study
• aimed to seek and gain a more definitive understanding of the
inter-relationship of Acquired Brain Injury,
• substance abuse and homelessness by identifying key themes
associated with the inter-relationship
• between these variables.
-
Materials and methods:
• The study recruited eight participants through homeless
organisationsand treatment centres. Participants were screened for
suitability (Brain Injury Screening Index; Drug Abuse Screening
Tool; Alcohol Use Disorders Identification Test and then
participated in recorded semi-structured interviews, transcribed
and analysed using Interpretative Phenomenological Analysis.
-
Results:
• The study identified five master themes: Adverse Childhood
Experiences and Trauma; Mental Health; Cognitive Decline and
Executive Function; Services; Relationships.
-
Conclusion
• Healthcare professionals need to engage with children, their
families, and adults, who have been exposed to adverse childhood
experiences and should employ routine screening tools for brain
injury to ensure their presence is factored into developing
appropriate models of intervention.
-
IMPLICATIONS FOR REHABILITATION
• Need person-centred approaches to intervention for those with
acquired brain injury who are homeless
• and have substance abuse issues.• Need to screen for the
presence of acquired brain injury when
engaging with individuals who are• homeless or have substance
abuse.• Need screening of acquired brain injury and adverse
childhood
experiences to improve access to• services post-brain
injury.
-
• Focusing in on the peri-trauma phase will help improve
understanding of how parents’ own appraisals of the child’s medical
event and coping assistance may influence how children appraise and
cope during the medical event. By improving understanding of these
factors, preventive interventions can be better tailored and
thereby more effective.
-
Trauma-Informed Care
-
Trauma-Informed Care
• Three key elements of trauma-informed care:
• (1) realizing the prevalence of trauma; • (2) recognizing how
trauma affects all individuals
involved: patient, provider, and/or within any program,
organization, or system, including its own workforce;
• (3) responding by putting this knowledge into practice
-
Trauma-Informed Care
Organizational structure and treatment
framework
Involves understanding, recognizing, and
responding to the effects of of trauma
Emphasizes physical, psychological and
emotional safety for both consumers and
providers
Helps survivors rebuild a sense of control and
empowerment.
87http://www.traumainformedcareproject.org/
http://www.traumainformedcareproject.org/
-
Healing Centered Engagement
• TIC can be expanded following integrative principles• Trauma
is not just individualistic, it is collectivist • Must address the
social determinants to health• Ultimately must focus on possibility
rather than pathology• Involve culture, spirituality, civic action,
group/collective healing• Integrative wisdom - moving beyond a
focus on details/content/“why” to “what’s
right with me”, “what am I learning”, and how can I be in the
best possible relationship to my experience
-
Post-Traumatic
Growth
Purpose & Meaning
Spiritual Context
Motivator for Change
Seed for Compassion
Seeking Relationship
Cultivates Resilience
-
Caregiver Factors
-
Overview of caregiver stress
• Since 1970s research has explored the short/long-term impact
of TBI on caregivers
• Example mental health consideration: Informal/non-professional
caregivers play a key role in preventing suicide among people with
moderate to severe brain injuries Caregivers are most often female
and there is a heavy reliance on informal networks to provide
support
Blake, Holly. “Caregiver Stress in Traumatic Brain Injury.”
International Journal of Therapy and Rehabilitation 15, no. 6 (June
1, 2008): 263–71Kuipers P, Lancaster A (2000) Developing a suicide
preven-tion strategy based on the perspectives of people with brain
injuries. J Head Trauma Rehabil15(6): 1275–84Chan J (2007) Carers’
perspective on respite for persons with acquired brain injury. Int
J Rehabil Res30(2): 137–46
-
High impact• Research has focused more on psychological
impact:
• Psychological symptoms are common and may include depression,
anxiety, stress, and burden
• Caregivers’ physical health may also be affected• Underscores
mind-body (psychophysiological) mechanisms and the importance
of mind-body integrated self-care and support
• ~48–60% of caregivers experience depression • Feelings of
strain and depression may not lessen over time
-
Role changes• Changes to social roles, disturbances in
relationship with the patient,
decreases in leisure time, and reduction in social
circle/engagement• Loneliness and social isolation are frequently
cited problems (Romano, 1974;
Lezak, 1988).
• Caregivers often assume ↑ domestic workload and/or take on
greater responsibilities such as looking after children, becoming a
‘bread winner’ or dealing with finances (McKinlay et al, 1981;
Brooks and McKinley, 1983; Kreutzer et al, 1994). Caregivers also
report that the caregiving role can often prevent them from
obtaining gainful employment (Chan, 2007).
-
Factors influencing level of caregiver stress• Level of
behavioral and cognitive change
• Cognitive and behavioral problems in the brain-injured person
are more likely to be associated with high levels of strain for the
family than problems with physical functioning (Thomsen, 1984;
Allen et al, 1994; Watanabe et al, 2000).
• Patient coping strategies• Pre-injury family functioning
• Appears to be a significant factor in how caregivers and
relatives cope. • Differences in long-term adaptation and coping
efficacy are related to pre-TBI family
characteristics (Wesolowski and Zencius, 1994). •
Characteristics of well-functioning families include: strong
cohesion, understood
identity, firm boundaries, and open communication (Sachs, 1991).
• ‘Vulnerable’ families show less of these characteristic and can
be seriously damaged by
the occurrence of TBI in the family (Wesolowski and Zencius,
1994)
-
Caregiver characteristics (Blake 2008)
• Certain characteristics in the caregiver may add to the
stress/burden of caregiving:
• Expressed emotion • Higher levels of expressed emotion were
associated with greater anxiety, although levels of
expressed emotion were best predicted by caregiver status, with
sole caregivers exhibiting greater expressed emotion than joint
family caregivers. (Flanagan (1998))
• Coping strategies• Capacity for/use of cognitive restructuring
or reframing, maintaining enjoyable activities,
and pursuing emotional support through organized family support
groups • Appraisal of the situation• Strength of social support
-
Positive Effects?• Some caregivers report positive effects
including personal reward from
the caregiving experience, although greater personal reward is
reported by parents of TBI patients than spouses (Allen et al,
1994).
• Study of 180 significant others of people with TBI, Machamer
et al (2002) m
• Majority of caregivers reported positive aspects to
caregiving, such as being happy to have had the opportunity to care
for the person with TBI (93%) and feeling good about their ability
as a caregiver (92%)
• Measured both positive and negative effects of caregiving on
the Modified Caregiver Burden Scale
-
An Integrative Approach to Assessment&
Treatment
-
What is Integrative Psychiatry?
Lake J, Helgason C, Sarris J, MHSc. Integrative Mental Health
(IMH): Paradigm, Research, and Clinical Practice. 2012; 8.
-
Traditional Interventions to support ABI
• Needs assessment • Therapeutic education• Respite•
Community-based services• Family interventions
• Include elements of assessment, educational workshops,
follow-up work-shops, individualized family support and individual
and/or marital/couples counseling
• Rehabilitation programs
-
Building Blocks of Wholeness
Self-regulation Sound nutrition Sound sleepHealthy
relationships with family and peers
Connection with nature
Fun MovementSound decision
making and wisdom
Spirituality (sense of meaning and
purpose)
-
Therapeutic Approaches to Traumatic Stress
• Cognitive Processing Therapy (CPT)
• Prolonged Exposure• Trauma-Focused Cognitive
Behavioral Therapy (TF-CBT)• Dialectical Behavioral
Therapy (DBT)• Acceptance and Commitment
Therapy (ACT)
Desensitization and Reprocessing (EMDR)
• Mind-body Skills Groups (MBSG)Accelerated Resolution
Therapy (ART)Somatic ExperiencingNeurofeedbackNutritional
supplements
-
Nutrition and TBI
• Enteral or parenteral• Calories, protein, electrolytes,
vitamins, minerals, trace elements and fluids. • ”Nutritional goals
should be achieved within 5–7 days of injury”• Enteral nutrition --
reduce the incidence of ventilator-associated pneumonia•
Perioperative period
• Immune-enhancing additions (glutamine, alanine, omega-3 fatty
acids and nucleotides), may improve surgical outcomes.
‘Carney N, Totten AM, O'Reilly C, et al. Guidelines for the
management of severe traumatic brain injury, fourth edition.
Neurosurgery 2017;80:6–15Heyland DK, Novak F, Drover JW, et al.
Should immunonutrition become routine in critically ill patients? A
systematic review of the evidence. JAMA 2001;286:944–53.Peng R, Li
H, Yang L, et al. Immunonutrition for traumatic brain injury in
children and adolescents: protocol for a systematic review and
meta-analysis. BMJ Open2020;10:e037014.
doi:10.1136/bmjopen-2020-037014
-
Nutrition and ABI
• Omega-3’s?• Vitamin D?• Zinc?• Glutamine?• Broadspectrum
micronutrients?
Scrimgeour, A. G., & Condlin, M. L. (2014). Nutritional
treatment for traumatic brain injury. Journal of Neurotrauma,
31(11), 989-999.Lewis, M. D. (2016). Concussions, traumatic brain
injury, and the innovative use of omega-3s. Journal of the American
College of Nutrition, 35(5), 469-475.
-
Nutrition and TBI
Kaplan, B. J., Leaney, C., & Tsatsko, E. (2016).
Micronutrient Treatment of Emotional Dyscontrol Following Traumatic
Brain Injury. Ment Health, 4(5), 1078.
-
Mind-body medicine (MBM) focuses on exploring and supporting the
relationships among the spirit, mind,
brain, body, and behavior.
…supports all levels within each person’s being: physical,
emotional, mental, social, behavioral, environmental,
historical, and spiritual factors…
-
Mind-Body Medicine…
“…regards as fundamental an approach that respects and enhances
capacity for self-knowledge and self care.”
National Center for Complementary and Integrative Health
-
A quick overview of the science…
-
Caring for Other, Self, & “Co-Regulation”
We are only as effective in facilitating others’ stress
reduction and healing as we are in our own awareness, expression,
and ability to regulate our bodies and minds...
If we do not know what we feel, we will not be able to know what
others feel…
Community/relational based healing – co-regulation and
attunement
-
The Science of Connection: Oxytocin• Associated with social
engagement,
attachment, bond formation, social and emotional processing
circuitry (ventral vagal complex), has anxiolytic effects, enhances
parasympathetic response and increases heart rate variability
(Ellingsen 2015)
• The importance of healthy relationships; considered part of
the pain/healing environment...
• Administering oxytocin intranasally increases recognition of
both positive and negative emotion in others, increases empathizing
and cooperation with in-group others*
Keeler et al. 2015 - The neurochemistry and social flow
of singing: bonding and oxytocin
-
Biofeedback - Biosquares
113
Biosquares(c) 2017 Center for Mind-Body Medicine
-
Autogenics & Biofeedback
(c) 2017 Center for Mind-Body Medicine 114
-
Wilderness & Trauma Science
115
-
Lessons from the Wild
116
http://www.slideshare.net/bwitchel/pcaworkshop2014
-
Experiential ActivityShaking and Movement
-
Mind-Body Medicine Techniques
• Meditation• Biofeedback• Guided Imagery• Autogenics• Creative
expression• Movement & Music• Mindful Eating & Nutrition•
Group Support
-
Expanding Evidence for Individual Modalities
• ≈ 462,000 citations in CAM/IM subset of PubMed database
• Meditation (stress reduction, immune function, cancer, HTN,
attention, brain structure, insomnia)
• Guided Imagery (stress reduction, immune function, post-op
outcomes, PTSD, cancer, pain)
• Group Support (HIV, cancer, immune function, chronic pain,
insomnia, CHD)
• Hypnosis, Autogenics & Biofeedback (cancer, chronic pain,
immune function, migraine, mood, stress reduction)
• Creative expression (headaches, trauma, chronic pain, stress
reduction)
• Mindful Exercise (CVD, DM, cancer, depression, chronic pain,
immune function, stress reduction)
• Mindful Eating and Nutrition (Cancer, CHD, obesity,
hyperlipidemia, immune function)
-
Staples, J. K., Abdel Atti, J. A., & Gordon, J. S. (2011).
Mind-body skills groups for posttraumatic stress disorder and
depression symptoms in Palestinian children and adolescents in
Gaza.
Mind-Body Skills Group
3 main components to each session:• Psychoeducation•
Experiential• Sharing
-
Mind-Body Skills Group
• Randomized Controlled PTSD Study with Kosovar high school
students
• Students in the intervention group (n=38) had significantly
lower PTSD scores following participation in 12-session mind-body
skills group program than those in the control group (n=40)
• Scores remained significantly decreased at 3- month
follow-up
Journal of Clinical Psychiatry 2008; 69 (9): 1383-92
-
Mind-Body Skills Groups
• Mind-body skills groups have demonstrated effectiveness on
reducing burnout in medical students and physicians
• Offering trainings and groups online since COVID
West CP, Dyrbye LN, Rabatin JT, et al. Intervention to Promote
Physician Well-being, Job Satisfaction, and Professionalism. JAMA
Intern Med. 2014;174(4):527.Gordon JS. Mind-body skills groups for
medical students: reducing stress, enhancing commitment, and
promoting patient-centered care. BMC Med Educ. 2014;14:198–198.
-
Lots of Free Websites and Apps
http://medicalcenter.osu.edu/patientcare/healthcare_services/integrative_medicine/clinical-services/Pages/Mindfulness-Practices.aspx
-
What does co-regulation mean?
-
Integrated, Biopsychosocial Care
• … an approach to care that puts the patient at the center and
addresses the full range of influences that affect a person’s
health.
• …beyond solely the amelioration of symptoms • …support each
person to explore all levels and possible factors within
the spectrum of: • ~life – well-being - health – illness –
disease – death~
• Acknowledges the complex inseparability of biological,
behavioral, psychosocial, spiritual, cultural, historical, and
environmental influences
© Embody Your Mind, LLC
-
Social Determinants of Health
• Conditions in the environments in which people are born, live,
learn, work, play, worship, and age that affect a wide range of
health, functioning, and quality-of-life outcomes and risks
• Conditions may be broken into components found in “place”:•
Social• Economic• Physical
© Embody Your Mind, LLC
-
Examples of socioeconomic determinants
• Availability of resources to meet daily needs (e.g., safe
housing and local food markets)
• Educational, economic, and job opportunities
• Access to health care services• Transportation options• Social
support, norms &
attitudes (e.g., discrimination, racism, & distrust of
government)
• Exposure to crime, violence, & social disorder (e.g.,
presence of trash, lack of cooperation in a community)
• Socioeconomic conditions • Access to mass media and
emerging technologies (e.g., cell phones, the Internet, &
social media)
• Culture• Language, immigration status
© Embody Your Mind, LLC
-
Examples of physical determinants• Natural environment, such as
green space (e.g., trees and grass) or
weather (e.g., climate change)• Built environment, such as
buildings, sidewalks, bike lanes, and roads• Worksites, schools,
and recreational settings• Exposure to toxic substances and other
physical hazards• Physical barriers, especially for people with
disabilities• Aesthetic elements (e.g., lighting, fountains,
artwork, benches)
© Embody Your Mind, LLC
-
Resources that enhance quality of life can have a significant
influence on population health outcomes.
© Embody Your Mind, LLC
-
Resources
• www.nctsn.org • www.cmbm.org• www.traumahealing.org•
www.aacap.org• www.acceleratedresolutiontherapy.com• www.awcim.org•
https://www.youtube.com/playlist?list=PLjAbmS83087mS0AJYD6p6VSLDy7SKQZsy•
https://www.youtube.com/watch?v=iCvmsMzlF7o&t=5s
http://www.cmbm.org/http://www.cmbm.org/http://www.traumahealing.org/http://www.aacap.org/http://www.acceleratedresolutiontherapy.com/http://www.awcim.org/https://www.youtube.com/playlist?list=PLjAbmS83087mS0AJYD6p6VSLDy7SKQZsyhttps://www.youtube.com/watch?v=iCvmsMzlF7o&t=5s
-
With special Thanks to:
• Matt Erb, PT• James Gordon, M.D. and The Center
for Mind-Body Medicine
-
Questions?
-
Bibliography• Asher, G. N., Gerkin, J., & Gaynes, B. N.
(2017). Complementary therapies for mental health
disorders. Medical Clinics, 101(5), 847-864.• Asmundson, G. J.,
Coons, M. J., Taylor, S., & Katz, J. (2002). PTSD and the
experience of pain:
research and clinical implications of shared vulnerability and
mutual maintenance models. The Canadian Journal of Psychiatry,
47(10), 930-937.
• Card, P. (2017). VA/DoD clinical practice guideline for the
management of posttraumatic stress disorder and acute stress
disorder.
• Emerson D, Sharma R, Chaudhry S, & Turner J (2009)
Trauma-Sensitive Yoga: Principles, Practice, and Research.
International Journal of Yoga Therapy: 2009, Vol. 19, No. 1, pp.
123-128.
• Felitti, V., Anda, R., Nordenberg, D., Williamson, D., Spitz,
A., Edwards, V., . . . Marks, J. (1998). Relationship of childhood
abuse and household dysfunction to many of the leading causes of
death in adults: The Adverse Childhood Experiences (ACE) study.
American Journal of Preventive Medicine, 14(4), 245-258.
doi:10.1016/S0749-3797(98)00017-8
• Hodas, GR. (February 2006). Responding to Childhood Trauma:
The Promise and Practice of Trauma Informed Care. Pennsylvania
Office of Mental Health and Substance Abuse Services.
http://www.childrescuebill.org/VictimsOfAbuse/RespondingHodas.pdf.
Accessed May 23, 2019.
• Kaplan BJ, Rucklidge JJ, Romijn AR (2015) A randomized trial
of nutrient supplements to minimize psychological stress after a
natural disaster Psychiatry Research, August 30, 228(3), Pages
373–379
-
Bibliography, Cont’d• Matsumura, K., Noguchi, H., Nishi, D.,
Hamazaki, K., Hamazaki, T., & Matsuoka, Y. J. (2017). Effects
of omega-3
polyunsaturated fatty acids on psychophysiological symptoms of
post-traumatic stress disorder in accident survivors: A randomized,
double-blind, placebo-controlled trial. Journal of affective
disorders, 224, 27-31.
• Pistrang, N., Barker, C., & Humphreys, K. (2008). Mutual
help groups for mental health problems: A review of effectiveness
studies. American journal of community psychology, 42(1-2),
110-121.
• Payne, P., Levine, P. A., & Crane-Godreau, M. A. (2015).
Somatic experiencing: using interoception and proprioception as
core elements of trauma therapy. Frontiers in psychology, 6,
93.
• Ranjbar, N., & Erb, M. (2019). Adverse Childhood
Experiences and Trauma-Informed Care in Rehabilitation Clinical
Practice. Archives of Rehabilitation Research and Clinical
Translation, 100003.
• Rucklidge JJ, Blampied N, Gorman B, Gordon H, Sole E (2014)
Psychological functioning 1 year after a brief intervention using
micronutrients to treat stress and anxiety related to the 2011
Christchurch earthquakes: A Naturalistic Follow-up Hum.
Psychopharmacol Clin Exp. doi: 10.1002/hup.2392
• Substance Abuse Mental Health Services Administration
(SAMHSA). A Treatment Improvement Protocol: Trauma-Informed Care in
Behavioral Health Services. 2014.
https://store.samhsa.gov/shin/content//SMA14-4816/SMA14-4816.pdf.
• Siqveland, J., Hussain, A., Lindstrøm, J. C., Ruud, T., &
Hauff, E. (2017). Prevalence of posttraumatic stress disorder in
persons with chronic pain: a meta-analysis. Frontiers in
psychiatry, 8, 164.
-
Bibliography, Cont’d• Staples JK, Abdel Attai JA, Gordon JS.
Mind-body skills groups for posttraumatic stress disorder and
depression symptoms in Palestinian children and adolescents in
Gaza. Int J Stress Manag. 2011; 18(3): 246-262. doi:
10.1037/a0024015
• Staples, J. K., & Gordon, J. S. (2005). Effectiveness of a
mind-body skills training program for healthcare professionals.
Alternative therapies in health and medicine, 11(4), 36-43.
• Van der Kolk, B. A., Hodgdon, H., Gapen, M., Musicaro, R.,
Suvak, M. K., Hamlin, E., & Spinazzola, J. (2016). A randomized
controlled study of neurofeedback for chronic PTSD. PloS one,
11(12), e0166752.
• Van der Kolk, B. A., Spinazzola, J., Blaustein, M. E., Hopper,
J. W., Hopper, E. K., Korn, D. L., & Simpson, W. B. (2007). A
randomized clinical trial of eye movement desensitization and
reprocessing (EMDR), fluoxetine, and pill placebo in the treatment
of posttraumatic stress disorder: treatment effects and long-term
maintenance. Journal of clinical psychiatry, 68(1), 37.
• Van der Kolk, B. A., Stone, L., West, J., Rhodes, A., Emerson,
D., Suvak, M., & Spinazzola, J. (2014). Yoga as an adjunctive
treatment for posttraumatic stress disorder: A randomized
controlled trial. J Clin Psychiatry, 75(6), e559-65.
• Waits, W., Marumoto, M., & Weaver, J. (2017). Accelerated
resolution therapy (ART): a review and research to date. Current
psychiatry reports, 19(3), 18.
• Warner, E. T., Hammerschlag, R., Lian, N., & Hollifield,
M. (2007). Acupuncture for posttraumatic stress disorder: a
randomized controlled pilot trial. The Journal of Nervous and
Mental Disease.
-
Bibliography, Cont’d• SAMHSA - Substance Abuse Mental Health
Services Administration. A Treatment Improvement
Protocol: Trauma-Informed Care in Behavioral Health Services.
2014.
https://store.samhsa.gov/shin/content//SMA14-4816/SMA14-4816.pdf.
Accessed March 18, 2018.
• K. Hopper E, Bassuk E, Olivet J. Shelter from the Storm:
Trauma-Informed Care in Homelessness Services
Settings~!2009-08-20~!2009-09-28~!2010-03-22~! Vol 3.; 2010.
doi:10.2174/1874924001003020080
• Brunner E, Dankaerts W, Meichtry A, O’Sullivan K, Probst M.
Physical Therapists’ Ability to Identify Psychological Factors and
Their Self-Reported Competence to Manage Chronic Low Back Pain.
Physical therapy. 2018;98(6):471-479.
• Menschner C, Maul A. Key Ingredients for Successful
Trauma-Informed Care Implementation. April 2016.
http://www.chcs.org/media/ATC_whitepaper_040616.pdf. Accessed June
12, 2018.
• Arnow BA, Hunkeler EM, Blasey CM, et al. Comorbid depression,
chronic pain, and disability in primary care. Psychosom Med.
2006;68(2):262-268. doi:10.1097/01.psy.0000204851.15499.fc
• Merikangas KR, Ames M, Cui L, et al. The impact of comorbidity
of mental and physical conditions on role disability in the US
adult household population. Arch Gen Psychiatry.
2007;64(10):1180-1188. doi:10.1001/archpsyc.64.10.1180
• Druss BG, Marcus SC, Olfson M, Tanielian T, Elinson L, Pincus
HA. Comparing the national economic burden of five chronic
conditions. Health Aff (Millwood). 2001;20(6):233-241.
doi:10.1377/hlthaff.20.6.233
-
Bibliography, Cont’d• Bair MJ, Robinson RL, Katon W, Kroenke K.
Depression and pain comorbidity: A literature review. Archives of
Internal
Medicine. 2003;163(20):2433-2445.
doi:10.1001/archinte.163.20.2433• Outcalt SD, Kroenke K, Krebs EE,
et al. Chronic pain and comorbid mental health condition.
2015;38:535-543.
doi:10.1007/s10865-015-9628-3• Lerman SF, Rudich Z, Brill S,
Shalev H, Shahar G. Longitudinal associations between depression,
anxiety, pain, and pain-
related disability in chronic pain patients. Psychosom Med.
2015;77(3):333-341. doi:10.1097/PSY.0000000000000158• Sharp TJ,
Harvey AG. Chronic pain and posttraumatic stress disorder: mutual
maintenance? Clin Psychol Rev.
2001;21(6):857-877.• Boakye PA, Olechowski C, Rashiq S, et al. A
Critical Review of Neurobiological Factors Involved in the
Interactions
Between Chronic Pain, Depression, and Sleep Disruption. Clin J
Pain. 2016;32(4):327-336. doi:10.1097/AJP.0000000000000260
• Otis, J.D., Keane, T.M., Kerns, R.D. (2003). An examination of
the relationship between chronic pain and post-traumatic stress
disorder. Journal of Rehabilitation Research and Development,
40(5), 397-406.
• Fishbain, D.A., Pulikal, A., Lewis, J.E., Gao, J. (2017).
Chronic Pain Types Differ in Their Reported Prevalence of Post
-Traumatic Stress Disorder (PTSD) and There Is Consistent Evidence
That Chronic Pain Is Associated with PTSD: An Evidence-Based
Structured Systematic Review Pain Medicine, 18(4), 711–735.
• Coppens, E., Van Wambeke, P., Morlion, B., Weltens, N., Giao
Ly, H., Tack, J., Luyten, P., Van Oudenhove, L. (2017). Prevalence
and impact of childhood adversities and post-traumatic stress
disorder in women with fibromyalgia and chronic widespread pain.
European Journal of Pain, First published: 24 May 2017.
-
Bibliography, Cont’d• Kemp AH, Quintana DS. The relationship
between mental and physical health: insights from the study of
heart rate
variability. Int J Psychophysiol. 2013;89(3):288-296.
doi:10.1016/j.ijpsycho.2013.06.018• De Hert M, Correll CU, Bobes J,
et al. Physical illness in patients with severe mental disorders.
I. Prevalence, impact of
medications and disparities in health care. World Psychiatry.
2011;10(1):52-77.• SAMHSA. Morbidity and Mortality in People with
Serious Mental Illness. October 2006.
https://www.samhsa.gov/sites/default/files/grants/pdf/sm-17-008-revised.pdf.
Accessed June 1, 2018.• Halfon N, Larson K, Slusser W. Associations
between obesity and comorbid mental health, developmental, and
physical
health conditions in a nationally representative sample of US
children aged 10 to 17. Acad Pediatr. 2013;13(1):6-13.
doi:10.1016/j.acap.2012.10.007
• Halfon N, Larson K, Son J, Lu M, Bethell C. Income Inequality
and the Differential Effect of Adverse Childhood Experiences in US
Children. Acad Pediatr. 2017;17(7S):S70-S78.
doi:10.1016/j.acap.2016.11.007
• Halfon N, Larson K, Lu M, Tullis E, Russ S. Lifecourse Health
Development: Past, Present and Future. Vol 18.; 2013.
doi:10.1007/s10995-013-1346-2
• Hefferon K, Grealy M, & Mutrie N. (2009). Post-traumatic
growth and life threatening physical illness: A systematic review
of the qualitative literature. British Journal of Health
Psychology, 14(2): 343-378.
-
Bibliography, Cont’d• Corrigan F, Fisher J, Nutt D. Autonomic
dysregulation and the Window of Tolerance
model of the effects of complex emotional trauma. J
Psychopharmacol. 2010;25(1):17-25. doi:10.1177/0269881109354930
• Ogden P, Minton K, Pain C. Trauma and the Body: A Sensorimotor
Approach to Psychotherapy. 1st ed. New York: W.W. Norton; 2006.
• PORGES, STEPHEN W. “The Polyvagal Theory: New Insights into
Adaptive Reactions of the Autonomic Nervous System.” Cleveland
Clinic Journal of Medicine 76, no. Suppl 2 (April 2009): S86–90.
https://doi.org/10.3949/ccjm.76.s2.17.
• Kolacz, Jacek, and Stephen W Porges. “Chronic Diffuse Pain and
Functional Gastrointestinal Disorders After Traumatic Stress:
Pathophysiology Through a Polyvagal Perspective.” Frontiers in
Medicine 5 (2018): 145.
https://doi.org/10.3389/fmed.2018.00145.
• Stanley, Sharon. Relational and Body-Centered Practices for
Healing Trauma: Lifting the Burdens of the Past. New York:
Routledge, Taylor & Francis Group, 2016.
• Whatmore, George B., and Daniel R. Kohli. “Dysponesis: A
Neurophysiology Factor in Functional Disorders.” Behavioral Science
13, no. 2 (March 1, 1968): 102–24.
https://doi.org/10.1002/bs.3830130203.
https://doi.org/10.3949/ccjm.76.s2.17https://doi.org/10.3389/fmed.2018.00145https://doi.org/10.1002/bs.3830130203
-
Bibliography, Cont’d• Bowlby J, Robertson J. A two-year old goes
to hospital. Proc R Soc Med 1953;46(6):425-7.• Mead V. Adverse
Babyhood Experiences (ABEs) Resources. 2020• Meadows AL, Marsac ML.
Early-Life Trauma and Diabetes Management: An Under-Recognized
Phenomenon in Transition-Aged Youth. Clin Diabetes
2020;38(1):93-95. doi: 10.2337/cd19-0012 [published Online First:
2020/01/25]
• Robertson J, Freud A. A Mother's Observations on the
Tonsillectomy of Her Four-Year-Old Daughter. The Psychoanalytic
Study of the Child 1956;11(1):410-27. doi:
10.1080/00797308.1956.11822796
• Robertson J. Hospitalization as Medical Trauma for children
(wiki) with James Robertson (husband and wife).
• Robertson J. Hospitalization can be traumatizing (notes and
wiki). 1970s• Robertson J, Robertson J. John, 17 months. Lancet
1970;1(7648):673-4. doi: 10.1016/s0140-
6736(70)90904-9 [published Online First: 1970/03/28]• Robertson
J, Robertson J. Quality of substitute care as an influence on
separation responses. J Psychosom
Res 1972;16(4):261-5. doi: 10.1016/0022-3999(72)90008-6
[published Online First: 1972/08/01]
-
Bibliography, Cont’d• Robertson J, Robertson J. Young children
in brief separation. A fresh look. Psychoanal Study Child
1971;26:264-315. doi: 10.1080/00797308.1971.11822274 [published
Online First: 1971/01/01]• Robertson J, Robertson J. Substitute
mothering. Nurs Times 1973;69(47):1611-4. [published Online
First: 1973/11/29]• Robertson J. [Mother-child interaction
during the 1st year of life]. Psyche (Stuttg) 1977;31(2):167-
82. [published Online First: 1977/02/01]• Robertson J. [Young
children in hospital. 1]. Kango Gijutsu 1974;20(2):156-68.
[published Online
First: 1974/02/01]• Robertson J. [Young children in hospital.
2]. Kango Gijutsu 1974;20(3):154-63. [published Online
First: 1974/03/01]• Scaer R. Doctor Addresses Prevalence of
Medical Trauma. Somatic Experiencing Trauma Institute• The National
Child Traumatic Stress Prevention Network. The National Child
Traumatic Stress
Prevention Network.• Center for Pediatric Traumatic Stress.
Medical Events & Traumatic Stress in Children and Families. •
Center for Pediatric Traumatic Stress. Pediatric Medical Traumatic
Stress: A Comprehensive Guide.
-
Bibliography, Cont’d• Marsac ML, Kassam-Adams N, Delahanty DL,
et al. Posttraumatic stress following acute medical trauma in
children: a proposed model of bio-psycho-social processes during
the peri-trauma period. Clin Child Fam Psychol Rev
2014;17(4):399-411. doi: 10.1007/s10567-014-0174-2 [published
Online First: 2014/09/14]
• Kassam-Adams N, Garcia-Espana JF, Marsac ML, et al. A pilot
randomized controlled trial assessing secondary prevention of
traumatic stress integrated into pediatric trauma care. J Trauma
Stress 2011;24(3):252-9. doi: 10.1002/jts.20640 [published Online
First: 2011/05/20]
• Kassam-Adams N, Marsac ML, Kohser KL, et al. Pilot Randomized
Controlled Trial of a Novel Web-Based Intervention to Prevent
Posttraumatic Stress in Children Following Medical Events. J
Pediatr Psychol2016;41(1):138-48. doi: 10.1093/jpepsy/jsv057
[published Online First: 2015/06/20]
• Kassam-Adams N, Bakker A, Marsac ML, et al. Traumatic Stress,
Depression, and Recovery: Child and Parent Responses After
Emergency Medical Care for Unintentional Injury. Pediatr Emerg Care
2015;31(11):737-42. doi: 10.1097/PEC.0000000000000595 [published
Online First: 2015/11/05]
• Kassam-Adams N, Marsac ML, Garcia-Espana JF, et al. Evaluating
predictive screening for children's post-injury mental health: New
data and a replication. Eur J Psychotraumatol 2015;6:29313. doi:
10.3402/ejpt.v6.29313 [published Online First: 2015/12/18]
• Ramsdell KD, Morrison M, Kassam-Adams N, et al. A Qualitative
Analysis of Children's Emotional Reactions During Hospitalization
Following Injury. J Trauma Nurs 2016;23(4):194-201. doi:
10.1097/JTN.0000000000000217 [published Online First:
2016/07/16]
-
Bibliography, Cont’d• Hildenbrand AK, Day SB, Marsac ML.
Attending to the Not-so-Little "Little Things": Practicing
Trauma-Informed Pediatric Health Care. Glob
Pediatr Health 2019;6:2333794X19879353. doi:
10.1177/2333794X19879353 [published Online First: 2019/10/22]•
Kassam-Adams N, Kenardy JA, Delahanty DL, et al. Development of an
international data repository and research resource: the
Prospective
studies of Acute Child Trauma and Recovery (PACT/R) Data
Archive. Eur J Psychotraumatol 2020;11(1):1729025. doi:
10.1080/20008198.2020.1729025 [published Online First:
2020/04/15]
• Kraan T, Velthorst E, Smit F, et al. Trauma and recent life
events in individuals at ultra high risk for psychosis: review and
meta-analysis. Schizophr Res 2015;161(2-3):143-9. doi:
10.1016/j.schres.2014.11.026 [published Online First:
2014/12/17]
• Galler J, Rabinowitz DG. The intergenerational effects of
early adversity. Prog Mol Biol Transl Sci 2014;128:177-98. doi:
10.1016/B978-0-12-800977-2.00007-3 [published Online First:
2014/11/21]
• Chow EJ, Leger KJ, Bhatt NS, et al. Paediatric
cardio-oncology: epidemiology, screening, prevention, and
treatment. Cardiovasc Res2019;115(5):922-34. doi:
10.1093/cvr/cvz031 [published Online First: 2019/02/16]
• Christian-Brandt AS, Santacrose DE, Farnsworth HR, et al. When
Treatment is Traumatic: An Empirical Review of Interventions for
Pediatric Medical Traumatic Stress. Am J Community Psychol
2019;64(3-4):389-404. doi: 10.1002/ajcp.12392 [published Online
First: 2019/10/17]
• Knox BL, Luyet FM, Esernio-Jenssen D. Medical Neglect as a
Contributor to Poorly Controlled Asthma in Childhood. J Child
Adolesc Trauma2020;13(3):327-34. doi: 10.1007/s40653-019-00290-0
[published Online First: 2020/10/23]
• Riordan JP, Blakeslee A, Levine PA. Attachment Focused-Somatic
Experiencing®: Secure Phylogenetic Attachment, Dyadic Trauma, and•
Completion Across the Life Cycle. International Journal of
Neuropsychotherapy 2019;7(3):57-90.
-
Bibliography, Cont’d• Andersen V, Möller S, Jensen PB, et al.
Caesarean Delivery and Risk of Chronic Inflammatory Diseases
(Inflammatory Bowel Disease,
Rheumatoid Arthritis, Coeliac Disease, and Diabetes Mellitus): A
Population Based Registry Study of 2,699,479 Births in Denmark
During 1973–2016 Clin Epidemiol 2020;12(287-293)
• Mead VP. Adverse babyhood experiences (ABEs) increase risk for
infant and maternal morbidity and mortality, and chronic illness.
Journal of Prenatal and Perinatal Psychology and Health
2020;34(4)
• oderquist J, Wijma K, Wijma B. Traumatic stress after
childbirth: The role of obstetric variables. J Psychosom Obstet
Gynaecol 2002;23(1):31-9. doi: 10.3109/01674820209093413 [published
Online First: 2002/06/14]
• Koliouli F, Gaudron CZ, Raynaud J-P. Stress, coping, and
post-traumatic stress disorder of French fathers of premature
infants. Newborn Infant Nurs Rev 2016;16(3)
• Scaer R. The trauma spectrum: Hidden wounds and human
resiliency. New York: W.W. Norton 2005.• Mead VP. Adverse babyhood
experiences (ABEs): 10 indicators of risk for infant and maternal
complications that highlight opportunities for
prevention and repair. Perinatal Care Through a Trauma Informed
Lens: GOLD Learning Online Continuing Education 2020.• Klaus MH,
Jerauld R, Kreger NC, et al. Maternal attachment. Importance of the
first post-partum days. N Engl J Med 1972;286(9):460-63.• Schmitz
K. Vulnerable Child Syndrome. Pediatr Rev 2019;40(6):313-15. doi:
10.1542/pir.2017-0243 [published Online First: 2019/06/04]• Karin
Kushniruk. Traumatic Birth History as a Predictor for Burnout in
NICU Nurses: Time for a Paradigm Shift. Journal Prenatal and
Perinatal
Psychology and Health 2019;34(2):129-49.• Emerson WR. Treating
Cesarean Birth Trauma During Infancy and Childhood. Journal of
Prenatal and Perinatal Psychology & Health
2001;15(3):177-92.• Madrid A, editor. Repairing maternal-infant
bonding problems. New York: John Wiley and Sons, 2007.•
-
Bibliography, Cont’d• Coughlin M. Trauma-informed,
neuroprotective care for hospitalised newborns and infants. Infant
2017;13(5):1-4.• Widstrom AM, Brimdyr K, Svensson K, et al.
Skin-to-skin contact the first hour after birth, underlying
implications and clinical practice. Acta Paediatr
2019;108(7):1192-204. doi: 10.1111/apa.14754 [published Online
First: 2019/02/15]
• Horsch A, Vial Y, Favrod C, et al. Reducing intrusive
traumatic memories after emergency caesarean section: A
proof-of-principle randomized controlled study. Behav Res Ther
2017;94:36-47. doi: 10.1016/j.brat.2017.03.018 [published Online
First: 2017/04/30]
• Lopez U, Meyer M, Loures V, et al. Post-traumatic stress
disorder in parturients delivering by caesarean section and the
implication of anaesthesia: a prospective cohort study. Health Qual
Life Outcomes 2017;15(1):118. doi: 10.1186/s12955-017-0692-y
[published Online First: 2017/06/05]
• Yehuda R, Engel SM, Brand SR, et al. Transgenerational effects
of posttraumatic stress disorder in babies of mothers exposed to
the World Trade Center attacks during pregnancy. J Clin Endocrinol
Metab 2005;90(7):4115-8.
• Kennell JH, Klaus MH. Bonding: recent observations that alter
perinatal care. Pediatr Rev 1998;19(1):4-12.• Saywitz KJ, Goodman
GS, Nicholas E, et al. Children's memories of a physical
examination involving genital touch: implications for reports of
child sexual
abuse. J Consult Clin Psychol 1991;59(5):682-91. [published
Online First: 1991/10/01]
• Aho AC, Erickson MT. Effects of grade, gender, and
hospitalization on children's medical fears. J Dev Behav Pediatr
1985;6(3):146-53.• Porcelli P, Fava GA, Rafanelli C, et al.
Anniversary reactions in medical patients. J Nerv Ment Dis
2012;200(7):603-6. doi:
10.1097/NMD.0b013e31825bfb2e
• Fisher DJ. Remembering Robert J. Stoller (1924-1991).
Psychoanal Rev 1996;83(1):1-9. [published Online First:
1996/02/01]• Wintgens A, Boileau B, Robaey P. Posttraumatic stress
symptoms and medical procedures in children. Can J Psychiatry
1997;42(6):611-6.• Field T, Alpert B, Vega-Lahr N, et al.
Hospitalization stress in children: sensitizer and repressor coping
styles. Health Psychol 1988;7(5):433-45.• Romino SL, Keatley VM,
Secrest J, et al. Parental presence during anesthesia induction in
children. AORN J 2005;81(4):780-3, 85-9, 92; quiz 93-6.• Spitz RA.
Hospitalism: An inquiry into the genesis of psychiatric conditions
in early childhood: Psychoanalyt Study Child 1945.
-
Bibliography, Cont’d• Sapolsky, Robert M. Why Zebras Don’t Get
Ulcers / Robert M. Sapolsky. 3rd ed. New York:
Times Books, 2004.• Sapolsky, Robert M. Behave: The Biology of
Humans at Our Best and Worst. New York,
New York: Penguin Press, 2017.• Levine, Peter A, Ph. D, Gabor
Mate M. D, and Inc OverDrive. In an Unspoken Voice. S.I.:
North Atlantic Books, 2012.
http://api.overdrive.com/v1/collections/v1L2BowAAAC4HAAA1k/products/0300b3d1-2f8a-46f6-be7d-76b1c804fdae.
• Levine, Peter A. Waking the Tiger: Healing Trauma: The Innate
Capacity to Transform Overwhelming Experiences. Berkeley, Calif:
North Atlantic Books, 1997.
• Cruceanu, Cristiana, Natalie Matosin, and Elisabeth B Binder.
“Interactions of Early-Life Stress with the Genome and Epigenome:
From Prenatal Stress to Psychiatric Disorders.” Stress and Behavior
14 (April 1, 2017): 167–71.
https://doi.org/10.1016/j.cobeha.2017.04.001.
• Ruby, J. Graham, Kevin M. Wright, Kristin A. Rand, Amir
Kermany, Keith Noto, Don Curtis, Neal Varner, et al. “Estimates of
the Heritability of Human Longevity Are Substantially Inflated Due
to Assortative Mating.” Genetics 210, no. 3 (November 1, 2018):
1109. https://doi.org/10.1534/genetics.118.301613.
http://api.overdrive.com/v1/collections/v1L2BowAAAC4HAAA1k/products/0300b3d1-2f8a-46f6-be7d-76b1c804fdaehttps://doi.org/10.1016/j.cobeha.2017.04.001https://doi.org/10.1534/genetics.118.301613
-
Bibliography, Cont’d• Kearney, David J., Carol A. Malte, Carolyn
McManus, Michelle E. Martinez, Ben Felleman, and Tracy
L. Simpson. “Loving-Kindness Meditation for Posttraumatic Stress
Disorder: A Pilot Study.” Journal of Traumatic Stress 26, no. 4
(August 2013): 426–34. https://doi.org/10.1002/jts.21832.
• Payne, Peter, and Mardi A. Crane-Godreau. “The Preparatory
Set: A Novel Approach to Understanding Stress, Trauma, and the
Bodymind Therapies.” Frontiers in Human Neuroscience 9 (2015): 178.
https://doi.org/10.3389/fnhum.2015.00178.
• Van der Kolk, BA, Stone, L, West, J, Rhodes, A, Emerson, D,
Suvak, M & Spinazzola, J. (2014). Yoga as an Adjunctive
Treatment for Posttraumatic Stress Disorder: A Randomized
Controlled Trial. Journal of Clinical Psychiatry, 75, e1-e7
• Casement, MD, Swanson, LM (2012). A meta-analysis of imagery
rehearsal for post-trauma nightmares: effects on nightmare
frequency, sleep quality, and posttraumatic stress, Clin
PsycholRev., Aug 32(6): 566-74
• Levine, Peter A. Waking the Tiger: Healing Trauma: The Innate
Capacity to Transform Overwhelming Experiences. Berkeley, Calif:
North Atlantic Books, 1997.
• Gordon, J. S. (2019). The transformation: Discovering
wholeness and healing after trauma. San Francisco: HarperOne.
• Scaer, R. C. (2014). The Body Bears the Burden: Trauma,
Dissociation, and Disease. Retrieved from
https://books.google.com/books?id=0-ySnQEACAAJ
• Van der Kolk, B. A. (2014). The body keeps the score: Brain,
mind, and body in the healing of trauma. New York: Viking.
https://doi.org/10.1002/jts.21832https://doi.org/10.3389/fnhum.2015.00178https://books.google.com/books?id=0-ySnQEACAAJ
-
Bibliography, Cont’d• Ogden P, Minton K, Pain C, Siegel DJ, van
der Kolk BA. Trauma and the Body. 2006. WW Norton &
Co. New York.• Streeter, C. C., Gerbarg, P. L., Saper, R. B.,
Ciraulo, D. A., & Brown, R. P. (2012). Effects of yoga on
the autonomic nervous system, gamma-aminobutyric-acid, and
allostasis in epilepsy, depression, and post-traumatic stress
disorder. Medical hypotheses, 78(5), 571–579.
• Naparstek, B. (2004). Invisible heroes: Survivors of trauma
and how they heal. New York, NY: Bantam Books.
• Kirmayer, L. J., Kienzler, H. , Hamid Afana, A. and Pedersen,
D. (2010). Trauma and Disasters in Social and Cultural Context. In
Principles of Social Psychiatry (eds C. Morgan and D. Bhugra).
doi:10.1002/9780470684214.ch13
• Kolacz, Jacek, and Stephen W Porges. “Chronic Diffuse Pain and
Functional Gastrointestinal Disorders After Traumatic Stress:
Pathophysiology Through a Polyvagal Perspective.” Frontiers in
Medicine 5 (2018): 145.
https://doi.org/10.3389/fmed.2018.00145.
• Sachs-Ericsson, Natalie, Kiara Cromer, Annya Hernandez, and
Kathleen Kendall-Tackett. “A Review of Childhood Abuse, Health, and
Pain-Related Problems: The Role of Psychiatric Disorders and
Current Life Stress.” Journal of Trauma & Dissociation 10, no.
2 (April 3, 2009): 170–88.
https://doi.org/10.1080/15299730802624585.
• Gordon, J. S. (2019). The transformation: Discovering
wholeness and healing after trauma. San Francisco: HarperOne.
https://doi.org/10.3389/fmed.2018.00145https://doi.org/10.1080/15299730802624585
ACEs and ABI: �A Trauma-Informed Approach Disclosures��The
presenter has no financial conflicts of interest to
disclose.Learning ObjectivesOverviewCase Example of ABI and ACEs:
AnaPre-ABI Medical and Developmental HistoryPre-ABI Family
HistoryPre-ABI Social HistoryABI Treatment CoursePost-ABIPost-ABI,
Cont’dSome questions to consider:Stress, ACEs &
TraumaStressSlide Number 15Trauma��-“injury”— to our mind, body,
and spirit�Slide Number 17Who Does Trauma Affect?Post-Traumatic
Stress DisorderPost-Traumatic Stress Disorder Post-Traumatic Stress
DisorderForgotten or hidden trauma?Understanding TraumaTrauma and
the BrainTrauma Physiology Trauma Physiology, Cont’d Hormonal
ChangesHormonal Changes - CortisolChronic/excess Stress Influences
the Onset and Course of Virtually All IllnessThe Polyvagal
TheorySlide Number 31Slide Number 32Slide Number 33“Tend and
Befriend” Modifies Fight/Flight/Freeze ResponsesSlide Number
35Childhood or Developmental Trauma Slide Number 37�Adverse
Childhood Experiences Study�(ACES)ACE – List of
StressorsExperiential ActivitySlide Number 41Experiential
ActivitySlide Number 43ACE – Key FindingsACE – Key FindingsACE
score ≥6 associated with:�DemographicsSlide Number 48Expanded list
of ACEs may include:Mechanisms still being elucidated:Shared
Neurophysiological MechanismsSlide Number 52Mitigating
Influences�PCEs – Positive Childhood Experiences �PCE Study –
Results/RelevanceSlide Number 56Slide Number 57Slide Number
58Shame?Trauma-Informed Care Practical Applications�History
TakingHow to inquire?Slide Number 62Slide Number 63Slide Number
64Historical TraumaHistorical TraumaSlide Number 67Is ABI
considered an ACE?Common Causes of ABICommon Causes of
TBIConsequences of ABIsConsequences of ABI, Cont’dABI during
developmentEarly Assessment and Intervention ACEs and ABIPrior ACEs
impacts recovery from TBIPersons with prior ACEs increases risk for
TBISlide Number 78Purpose:Materials and methods:Results:Conclusion
IMPLICATIONS FOR REHABILITATION�Slide Number 84Trauma-Informed
CareTrauma-Informed CareTrauma-Informed CareSlide Number 88Healing
Centered EngagementSlide Number 90Caregiver FactorsSlide Number
92Overview of caregiver stressHigh impactRole changesFactors
influencing level of caregiver stressCaregiver characteristics
(Blake 2008)Positive Effects?An Integrative Approach to
Assessment& TreatmentWhat is Integrative Psychiatry?Traditional
Interventions to support ABIBuilding Blocks of WholenessTherapeutic
Approaches to Traumatic StressNutrition and TBINutrition and
ABINutrition and TBISlide Number 107Mind-Body Medicine…A quick
overview of the science…Slide Number 110Caring for Other, Self,
& �“Co-Regulation”�The Science of Connection:
OxytocinBiofeedback - BiosquaresAutogenics &
BiofeedbackWilderness & Trauma ScienceLessons from the
WildSlide Number 117Mind-Body Medicine TechniquesExpanding Evidence
for Individual ModalitiesSlide Number 120Mind-Body Skills
GroupMind-Body Skills Group Mind-Body Skills GroupsLots of Free
Websites and AppsSlide Number 125Slide Number 126Integrated,
Biopsychosocial CareSocial Determinants of HealthExamples of
socioeconomic determinantsExamples of physical
determinantsResources that enhance quality of life can have a
significant influence on population health outcomes. ResourcesWith
special Thanks to:Questions?BibliographyBibliography,
Cont’dBibliography, Cont’dBibliography, Cont’dBibliography,
Cont’dBibliography, Cont’dBibliography, Cont’dBibliography,
Cont’dBibliography, Cont’dBibliography, Cont’dBibliography,
Cont’dBibliography, Cont’dBibliography, Cont’dBibliography,
Cont’dBibliography, Cont’dBibliography, Cont’d