Embed Size (px)
Citation preview

CurrentConceptsReview
Acetabular Fractures in the ElderlyEvaluation and Management
Derek Butterwick, MD, FRCSC, Steve Papp, MD, MSc, FRCSC, Wade Gofton, MD, MEd, FRCSC, Allan Liew, MD, FRCSC,and Paul E. Beaule, MD, FRCSC
Investigation performed at the Division of Orthopedic Surgery, The Ottawa Hospital, University of Ottawa, Ottawa, Ontario, Canada
� Acetabular fracture patterns in the elderly, with increased involvement of the anterior column, quadrilateral platecomminution,medialization of the femoral head, andmarginal impaction, differ from those noted among a youngercohort.
� Poor prognostic factors for open reduction and internal fixation (ORIF) are posterior wall comminution, marginalimpaction of the acetabulum, a femoral head impaction fracture, a so-called gull sign, and hip dislocation.
� The rate of conversion to total hip arthroplasty following formal ORIF has been reported to be 22% at a mean oftwenty-nine months.
� Total hip replacement after an acetabular fracture generally yields good clinical results; however, in the acutesetting, it must be combined with proper stable fracture fixation.
Epidemiology and Mechanism of InjuryWith an aging population, the prevalence and burden of allosteopenic fractures, especially hip fractures, continue to be aconcern1-3. Specifically, in patients over the age of sixty, therehas been a 2.4-fold increase in the incidence of acetabularfractures over the past quarter of a century4, and geriatric pa-tients are the fastest growing subgroup of patients with ace-tabular fractures5. The mechanism of injury in this age cohortdiffers substantially in comparison with that in youngeradults. Ferguson et al. found that while low-energy falls from astanding height accounted for 50% (117) of 235 acetabularfractures in patients over sixty years of age, high-energymechanisms accounted for 82% (884) of 1072 fractures inyoung adults4. Additionally, only 30% (seventy) of 235 olderpatients with an acetabular fracture had associated injuries,
likely because of decreased involvement in motor vehiclecollisions4.
The anterior column-posterior hemitransverse fracturepattern is the classic osteopenic acetabular fracture as it displaysa number of features commonly seen in geriatric acetabularfractures6,7 (Figs. 1-A and 1-B). In patients with normal bonequality who are involved in high-energy trauma, fracture pat-terns are typical of those described by the Letournel classifi-cation8,9. However, osteopenic patients who fall on their sideexperience an impact through the greater trochanter, whichresults in an anteromedial force fracturing and displacing theanterior column and quadrilateral plate. The femoral head thenmedializes with the anterior column and impacts the postero-medial portion of the roof 4,10. At times, the femoral head canbe impacted by the intact acetabulum. This mechanism results
Disclosure: None of the authors received payments or services, either directly or indirectly (i.e., via his or her institution), from a third party in support ofany aspect of this work. One or more of the authors, or his or her institution, has had a financial relationship, in the thirty-six months prior to submissionof this work, with an entity in the biomedical arena that could be perceived to influence or have the potential to influence what is written in this work. Noauthor has had any other relationships, or has engaged in any other activities, that could be perceived to influence or have the potential to influence whatis written in this work. The complete Disclosures of Potential Conflicts of Interest submitted by authors are always provided with the online version ofthe article.
Peer Review: This article was reviewed by the Editor-in-Chief and one Deputy Editor, and it underwent blinded review by two or more outside experts. The Deputy Editorreviewed each revision of the article, and it underwent a final review by the Editor-in-Chief prior to publication. Final corrections and clarifications occurred during one ormore exchanges between the author(s) and copyeditors.
758
COPYRIGHT � 2015 BY THE JOURNAL OF BONE AND JOINT SURGERY, INCORPORATED
J Bone Joint Surg Am. 2015;97:758-68 d http://dx.doi.org/10.2106/JBJS.N.01037

in the classic features common to geriatric acetabular frac-tures, which include anterior column displacement, quadri-lateral plate involvement, medialization of the femoral head,and superomedial roof impaction, which create the so-calledgull sign on an anteroposterior pelvic radiograph4.
Radiographic Evaluation and Fracture ClassificationRadiographic evaluation begins with an anteroposterior pelvicradiograph followed by obturator and iliac oblique Judet ra-diographs (Figs. 1-A through 1-E). Fractures are then classifiedaccording to the Letournel classification of acetabular fracturesto assist in treatment planning9,11. The fracture can be furtherinvestigated with computed tomography (CT) scans and three-
dimensional reconstructions to gain a better understanding ofthe personality of the fracture and assess articular displace-ment12. Occult acetabular fractures following a low-energy fallcan occur and may result in a poor outcome if missed13. Ifradiographs are equivocal in an elderly patient with hip painfollowing a traumatic injury, a magnetic resonance imagingscan is warranted to rule out both an occult proximal femoralfracture and an acetabular fracture14-16.
Recent systematic reviews17 and epidemiological studies4
have revealed that the associated both-column variant is themost frequent fracture pattern (23% to 26%) in this agegroup. Fractures involving the anterior column are the secondmost common, with anterior column-posterior hemitransverse
Fig. 1-A
Fig. 1-B
Figs. 1-A through 1-E A patient with an anterior column-posterior hemitransverse fracture of the left hip. Figs. 1-A and 1-B Preoperative anteroposterior
pelvic radiograph (Fig. 1-A) demonstrating the fracture with a so-called gull sign, representing superomedial dome impaction (large black arrow) and
quadrilateral plate displacement (thin white arrow), and a three-dimensional reconstruction (Fig. 1-B) showing oblique views, with a white arrow indicating
the plate displacement.
759
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 97-A d NUMBER 9 d MAY 6, 2015ACETABULAR FRACTURES IN THE ELDERLY

Fig. 1-C Fig. 1-D
Fig. 1-E
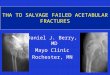
Figs. 1-C, 1-D, and 1-E The reduction and fixation of the fracture. Fig. 1-C The superomedial dome fragment is reduced via a bone tamp through an
ilioinguinal approach. Fig. 1-D The quadrilateral plate is reduced via an offset clamp. Fig. 1-E Anterior column plating and periarticular screw fixation permit
an acceptable radiographic result.
760
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 97-A d NUMBER 9 d MAY 6, 2015ACETABULAR FRACTURES IN THE ELDERLY

fractures representing 15% to 19% and isolated anterior col-umn injuries accounting for 11% to 19%. Of note, with pos-teriorly directed forces, isolated posterior wall fractures (8% to13%) are relatively common and are often associated withmarginal impaction (38%) and fracture comminution (44%).Isolated posterior column fractures (0.4% to 2%) are quite rareas these fractures generally occur in more robust bone. How-ever, when they do occur, they are associated with posteriorwall injuries (8% to 13%).
Radiographic signs associated with a poor outcome areposterior wall comminution, marginal impaction, the so-calledgull sign representing superomedial roof impaction, hip dis-location, impaction injuries to the femoral head, femoral heador neck fractures, and preexisting arthritic changes4,18-20 (TableI). Anglen et al. described the gull sign, which refers to a specifictype of marginal impaction of osteopenic bone resulting insuperomedial dome impaction from medialization of thefemoral head20. In their series, all fractures with this radio-graphic finding experienced inadequate reduction or earlyloss of reduction, medial subluxation of the femoral head,and medial and/or superior joint narrowing, with a 100%rate of failure of open reduction and internal fixation (ORIF).These findings were confirmed by Laflamme et al. in a series
of twenty-one patients, in which six patients with the gullsign had a poor reduction and progressed early to total hiparthroplasty21. However, in a larger study, Carroll et al.found no association between the gull sign and the need forsubsequent arthroplasty, stating that the failure rate waslargely related to the overall quality of the reduction andfixation22.
Treatment OptionsBefore treatment options are considered, a full history andphysical examination should be completed with a focus on thepatient’s associated injuries, medical history, ambulatory sta-tus, functional demands, living situation, and history of ar-thritic hip pain. Patients with an acetabular fracture should betreated as any other older patient with a fragility fracture; thevitamin-D level along with other factors related to osteoporosisshould be evaluated and a follow-up dual x-ray absorptiometryscan scheduled with appropriate referral to a clinician com-fortable in the evaluation and treatment of low bone density.Factors affecting the survival of the native hip should also beconsidered when choosing treatment options. In their seriesof 816 acetabular fractures followed over twenty-two years,Tannast et al. revealed that an age of greater than forty years,
Fig. 2-A
Figs. 2-A and 2-B An eighty-eight-year-old man with a both-column fracture pattern of the left hip who was managed with toe-touch weight-bearing for eight
weeks. Fig 2-A Anteroposterior radiograph made after the injury demonstrating secondary congruence.
761
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 97-A d NUMBER 9 d MAY 6, 2015ACETABULAR FRACTURES IN THE ELDERLY

anterior dislocation, posterior wall involvement, femoral headcartilage impaction fractures, marginal impaction, acetabularimpaction, and initial articular displacement of >2 cm werecorrelated with a future need for total hip arthroplasty23.
Nonoperative TreatmentHistorically, the nonoperative management of geriatric ace-tabular fractures has yielded poor results24. In the past, re-ductions were attempted via lateral trochanteric or longitudinalskeletal traction and prolonged bed rest. In a study of thirty-two displaced fractures managed nonoperatively, only 56%(eighteen) of the fractures were reduced and 44% (fourteenfractures) had a poor clinical outcome25. In a review of the casesof twenty-five patients over sixty-five years old who had anacetabular fracture that was managed nonoperatively, Spencerreported that 30% had poor results associated with severe painon walking or with incapacitation26. However, in specific situ-ations, nonoperative management may be indicated.
Nonoperative management is indicated in both-columnfracture patterns that exhibit so-called secondary congruence.In the both-column fracture, all fracture fragments are separatefrom the intact ilium, allowing the femoral head to act as atemplate such that each osteochondral fragment may settlearound the femoral head and achieve a congruent reduction27.Letournel originally reported very good to excellent results
in eleven of thirteen fractures with secondary congruence at 4.3years9. Most recently, Gansslen et al. reviewed the cases of thirty-five patients of all ages with both-column fractures who requirednonoperative treatment and found that 88% healed with sec-ondary congruence28. Overall, 80% had no to slight pain and 77%had good to excellent functional results on the basis of the Merled’Aubigne scoring system. In an elderly, low-demand patient,secondary congruence may provide acceptable functional out-comes (Figs. 2-A and 2-B).
Although indications specific to the geriatric populationdo not exist, literature on acetabular fractures in adults hasshown that nonoperative management is indicated in fracturesthat simultaneously meet all of the following criteria: <2mm ofdisplacement, an intact roof arc angle of 45�, superior 10 mmof the subchondral ring intact on CT, posterior wall fracturesinvolving <20% of the posterior wall, hip joint stability andcongruity, and an absence of the poor prognostic factors listedearlier24,29. Lastly, in patients who aremedically unfit for surgeryor functionally incapacitated, nonoperative management maybe a necessity.
Our nonoperative management protocol consists of ashort period of bed rest for pain control followed by earlymobilization with toe-touch weight-bearing for six weeks withphysiotherapy supervision depending on fall risk. Prophylaxisagainst deep vein thrombosis should be used during this
Fig. 2-B
Anteroposterior radiograph made six months after the injury showing acceptable radiographic results.
762
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 97-A d NUMBER 9 d MAY 6, 2015ACETABULAR FRACTURES IN THE ELDERLY

period, and fall prevention measures should be instituted viaallied health-care workers. The patient is seen at two, six, andtwelve weeks for pelvic radiographs to monitor for displace-ment. Bed rest is specifically contraindicated for these patients,given the morbidity and mortality associated with prolongedbed rest30. On the rare occurrence that the patient is too un-comfortable to mobilize, we recommend surgical stabilizationof the fracture to allow early mobilization.
Operative ManagementWhile it was previously suggested by Tile31 that attempts atosteosynthesis of geriatric acetabular fractures be abandonedbecause of poor bone quality, Letournel reported that 76%(forty-four) of fifty-eight patients over sixty years old withacetabular fractures treated by ORIF had good to excellentoutcomes32. Matta reported that achieving a reduction with<3 mm of intra-articular incongruity was key to obtaining agood clinical result in all acetabular fractures33. However, nu-merous authors have shown a limited ability to achieve anacceptable reduction in these patients in comparison with ayounger cohort. Both Matta and Miller et al. were only able toachieve anatomic reduction in 44% (thirteen) of twenty-ninepatients over sixty years old and in 58% (twenty-six) of forty-five patients over fifty-five years old, respectively33,34. Beforedeciding on treatment, one should consider whether an ac-ceptable reduction can be achieved and whether bone quality issufficient for the implants to maintain articular reduction.
Choice of Operative ApproachWith the exception of most transverse and T-shaped patterns,any fracture pattern involving the anterior column may beapproached via an ilioinguinal approach or the intrapelvic Stoppaapproach. Fractures involving the posterior wall or isolated pos-terior column necessitate a Kocher-Langenbeck approach9. Ingeriatric fractures involving the anterior column and displace-ment of the quadrilateral plate, the use of the Stoppa approach35-37
provides direct access and visualization of these fragments forreduction and fixation. For surgeons who prefer the ilioinguinalapproach, dissection can be limited to the lateral two windows tominimize blood loss and operative time, with similar outcomes incomparison with the traditional three windows38. When an acute
total hip arthroplasty is combined with ORIF, an ilioinguinal orStoppa approach may be utilized for fracture fixation followed byrepositioning and total hip arthroplasty via a Kocher-Langenbeckapproach39. Alternatively, surgeons who are comfortable with an-terior total hip arthroplasty may prefer the Levine anterior ap-proach in fractures without posterior wall comminution (Fig. 3)10.
ORIFFormal ORIFThe reduction sequence generally begins with disimpaction ofthe medialized femoral head via lateral traction using a Schanzpin in the proximal part of the femur, allowing lateralization ofthe femoral head back under the acetabular dome. Via thelateral window of the ilioinguinal approach, reduction and lagscrew and/or plate fixation of high anterior column fracturescan be completed. Deformity correction often requires internalrotation of the anterior column, and antiglide plate techniquescan be very useful in achieving and maintaining the reductionwithout blocking the reduction of the medial articular frag-ments or quadrilateral plate. The impacted roof segments canthen be disimpacted via a bone tamp placed through a corticalwindow on the inner table during an ilioinguinal approach.Alternatively, the Stoppa approach can be used to hinge open
TABLE I Poor Prognostic Factors for ORIF of GeriatricAcetabular Fractures*
Gull sign
Femoral head impaction fracture
Marginal impaction
Hip dislocation
Preexisting osteoarthritis
Femoral head and neck fractures
Posterior wall comminution
*ORIF = open reduction and internal fixation.
Fig. 3
The Levine approach with an incision along the iliac crest to the anterior
superior iliac spine and extending distally over the Smith-Petersen interval.
(Reproduced, with permission, from: Beaule PE, Griffin DB, Matta JM. The
Levine anterior approach for total hip replacement as the treatment for an
acute acetabular fracture. J Orthop Trauma. 2004 Oct;18[9]:623-9.)
763
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 97-A d NUMBER 9 d MAY 6, 2015ACETABULAR FRACTURES IN THE ELDERLY

the quadrilateral plate and directly reduce the impacted artic-ular fragments12. Last, the quadrilateral plate can be reducedusing offset pelvic clamps or ball-spike pushers with a spikeddisc attachment to avoid penetrating the thin cortex in thislocation (Figs. 1-C, 1-D, and 1-E).
Achieving rigid fixation of the often fragile quadrilateralplate can be the most difficult part of the procedure5. Attemptsat buttressing the quadrilateral plate through the ilioinguinalapproach via a spring plate or T-plate placed under a pelvicreconstruction along the pelvic brim have resulted in late dis-placement5. A biomechanical anterior column-posterior hemi-transverse fracture model using a cadaveric pelvis showed thatthe addition of three long periarticular screws to standard re-construction plating along the pelvic brim provided increasedresistance to displacement of the quadrilateral plate, while use ofan H plate, which hangs over the pelvic brim down the quad-rilateral plate, did not6. We favor direct buttressing of thequadrilateral plate through the Stoppa approach. Laflammeet al. described a technique for direct reduction of the frag-ment whereby the quadrilateral plate fragment was mobilized,reduction of the impacted dome fragment was achievedunder direct visualization, and subchondral raft screws wereplaced above the dome40. In a series of twenty-one elderly
patients with quadrilateral plate displacement and protru-sion, Laflamme et al. outlined the use of a contoured in-frapectineal pelvic reconstruction plate placed through theStoppa window with two screws just anterior to the sacroiliacjoint and two screws into the superior pubic ramus21. With thisconfiguration, substantial loss of reduction was only seen intwo patients.
Percutaneous Reduction and FixationIn order to minimize the risks of postoperative infection andblood loss and to offer potentially quicker recovery, some haveadvocated percutaneous fixation41. It should be noted that thistechnique requires considerable expertise and comfort withfluoroscopic anatomy of the pelvis, and it would likely only beapplicable for acetabular trauma surgeons making the transi-tion from open to percutaneous techniques. In the elderlypopulation, this technique may be used to allow sufficientstability to facilitate early mobilization, and if arthritic pro-gression occurs following consolidation, it allows for a routinetotal hip arthroplasty. Percutaneous fixation of acetabular frac-tures has been popularized by the work of Starr et al. on thedevelopment of the techniques for column fixation using largecannulated 6.5 or 7.3-mm screws42. In their review of eighty
TABLE II Outcomes of ORIF and Acute Total Hip Arthroplasty for the Treatment of Geriatric Acetabular Fractures*
StudyPatientAge (yr)
No. ofFractures
Mean Durationof Follow-up
Mean FunctionalScores (points)
Conversion toTotal Hip
ArthroplastyRates of Death/Complications
ORIF
Carroll et al.22 (2010) >55 84 5 yr 20.6 on MFA;28.3 afterconversion toTHA
30.95% at 28 mo –/40%
Archdeacon et al.44 (2013) >70 39 34 mo 16 on Merled’Aubignesystem
19% 20% at 20 mo/–
Miller et al.34 (2010) >55 45 72.4 mo 46 on SF-36PCS; 50 onSF-36 MCS
28.9% at 31.5 mo NA
Anglen et al.20 (2003) >60 48 37 mo 37.26 on SF-36PCS; 57.38 onSF-36 MCS
17% at 7.5 mo 21%/–
Laflamme et al.21 (2011) >55 21 4.2 yr 86.2 on HHS 10% NA
Acute THA and ORIF
Mouhsine et al.46 (2002) >65 12 2 yr NA NA 0
Mears and Velyvis19 (2002) >50 48 8.1 yr 89 on HHS NA 0/9.5%
Herscovici et al.47 (2010) >60 22 29.4 mo 74 on HHS NA –/59%
Chakravarty et al.48 (2013) >57 19 22 mo NA NA 26% at 1 yr/42%
Rickman et al.39 (2014) >63 24 24 mo NA NA 14% at 1 yr/8%
Boraiah et al.55 (2009) >55 18 3.9 yr 88 on HHS NA –/11%
Lin et al.56 (2014) >60 33 5.6 yr 17 on OHS NA –/15%
*ORIF = open reduction and internal fixation, MFA = Musculoskeletal Functional Assessment, THA = total hip arthroplasty, SF-36 = Short Form-36,PCS = Physical Component Score, MCS = Mental Component Score, NA = not available, HHS = Harris hip score, and OHS = Oxford hip score.
764
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 97-A d NUMBER 9 d MAY 6, 2015ACETABULAR FRACTURES IN THE ELDERLY

patients over the age of sixty, they performed surgery on dis-placed unstable acetabular fractures, with 56% (forty-five) of theeighty fractures being displaced both-column or anterior column-posterior hemitransverse fractures. Twenty-five percent (twenty)of the eighty fractures underwent closed reduction with per-cutaneous use of Cobb elevators or ball-spike pushers usingfluoroscopic guidance. Seventy-five percent (sixty fractures)required mini-open access to the quadrilateral plate via a small3-cm portion of the lateral window along the iliac crest. Of theseventy-five patients available for follow-up at a mean of 3.9years, nineteen (25%) had conversion to total hip arthroplasty ata mean of 1.41 years postoperatively. Loss of reduction withmedialization of the femoral had occurred in 6% (five) of theeighty patients41. In a follow-up study that reviewed the samepatient series, Gary et al. commented on the functional outcomeof percutaneous fixation43. Of the forty-three patients availablefor follow-up, thirty-five provided Short Musculoskeletal Func-tional Assessment (SMFA) scores at a mean of 6.8 years post-operatively. No significant difference in the SMFA scores wasfound between those who retained their native hip and thepopulation norms for patients over sixty years old. Of the thirty-six patients, eleven (31%) had a subsequent total hip arthroplasty.In their conclusion, they noted that functional scores were notsignificantly better than those in other series of formal ORIF43.
Although the outcomes of the above case series appearcomparable with those after formal ORIF, the literature sup-porting this comparison is sparse. Specific contraindications tothis technique include posterior wall fractures with hip joint in-stability and lack of expertise with percutaneous column fixation.Although Starr et al. utilized their technique for all displacedacetabular fractures42, we favor using percutaneous techniques tostabilize the columns in minimally displaced fractures in patientswho are too uncomfortable to begin our earlymobilization and/ortoe-touch weight-bearing protocol.
Postoperative ManagementPatients should be treated with prophylaxis against deep veinthrombosis during the postoperative course. Protected weight-bearing is maintained for three months until fracture consolida-tion occurs; however, patients may self-limit during this period5,44.
Outcomes of ORIFIn a 2014 systematic review of eight studies on acetabularfractures in patients over fifty-five years old, similar failurerates, as measured by conversion to total hip arthroplasty, werenoted, with 22% of the fractures treated with formal ORIF and25% of those treated with percutaneous fixation having con-version to total hip arthroplasty17. An acceptable reduction of<3 mm was found in 86% of the fractures treated with formalORIF; however, an anatomic reduction was only achieved in45%. The mean blood loss was significantly different at 891 mLin the ORIF group and 70 mL in the percutaneous fixationgroup (p < 0.001). Of note, the mortality rate in the percuta-neous group was 31% compared with 15% in the ORIF group;however, the percutaneous group was significantly older at 74.4years versus 69.5 years (p < 0.001), imparting potential bias.
Nonfatal complications were similar at 39%. TheHarris hip scoreaveraged 87.9 points in the group treated with formal ORIF17.
Acute Total Hip ArthroplastyThe indications for acute total hip arthroplasty have not beenfully developed, but generally include the poor prognosticfactors listed above. The majority of studies on acute totalhip arthroplasty have cited indications such as severe non-reconstructible comminution related to poor bone density,femoral head lesions, impaction fracture of >40% of the dome,femoral head and/or neck fractures, and preexisting severedegenerative arthritis19.
Surgical goals when this fracture is approached include theachievement of rigid stabilization of the fracture such that anacetabular component can be inserted with good initial stabilityto allow fracture site healing and long-term stability of thecomponent. Achieving these goals involves overcoming manytechnical challenges, and one should be careful not to assumethat a total hip arthroplasty is a simpler solution to a complexfracture pattern as it can be more difficult than open ORIF.
Several techniques of fracture reduction and stabilization(cables, formal ORIF, or percutaneous ORIF) can be used priorto performing the total hip replacement. During reduction, thegoal is not to achieve anatomic reduction, but to reduce thecolumns such that they will provide stability to the acetabularcomponent. The use of anterior column and iliac wing fixationcombined with braided cerclage cabling of the acetabulum andquadrilateral plate to prevent protrusio was popularized byMears et al. and Mouhsine et al. in the late 1990s and early2000s19,45,46. “The Combined Procedure” has since become apopular method of fixation in which the acetabulum is stabi-lized using formal ORIF techniques, followed by implantationof an acetabular component47. During this technique, bone lossmay occur from posterior wall fracture comminution, whichmay hinder the ability to achieve a rim fit with a press-fitcomponent. In these situations, the osteotomized native fem-oral head is used as a structural graft to provide primary sta-bility of the component similar to a figure-7-shaped graft19.Alternatively, with the popularization of percutaneous stabili-zation, large cannulated screws can be used in the place offormal ORIF48. Efforts should be made to utilize a single inci-sion for both procedures to reduce operative time and bloodloss. Surgeons who are comfortable with the anterior total hiparthroplasty technique may use the Levine modification ofthe Smith-Petersen approach in the setting of isolated ante-rior column or associated anterior column-posterior hemi-transverse fracture10.
In situations in which rigid fixation of the acetabularcomponent cannot be achieved with ORIF of the columns,antiprotrusio cages can be used to stabilize fractures by virtueof the screws that attach the cage to the intact ilium, bridgingthe fracture and providing a stable environment for cup in-sertion. This technique can be used for all acetabular fractures,with the exception of the both-column type of fracture sincethere is no intact ilium to anchor the cage. In this technique,the articular surface is left unreduced; the articular cartilage of
765
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 97-A d NUMBER 9 d MAY 6, 2015ACETABULAR FRACTURES IN THE ELDERLY

the acetabulum is carefully removed using reamers or curets,with the native femoral head used as morselized graft; the cageis implanted using numerous screws; and finally a polyethylenebearing is cemented in place (Figs. 4-A and 4-B)49. Full weight-bearing is not begun until fracture union at six weeks.
In the largest reported series, to our knowledge, on acutetotal hip arthroplasty, Mears and Velyvis reported on fifty-sevenpatients with a mean follow-up period of 8.1 years19. Superioranterior column fragments were reduced and fixed with per-cutaneous lag screws through the anterior inferior iliac spine,while the remainder of the acetabulum and the displacedquadrilateral plate were stabilized with a cabling technique.Press-fit acetabular components were used, and patients weremobilized at six weeks. The mean Harris hip score was 89points (range, 69 to 100 points). Although early migration of<3 mm was noted, there were no cases of late aseptic loosen-ing19. Similarly, a trabecular metal cup-cage construct may beused to provide stability in appropriate fracture patterns50.
In a systematic review comparing studies on the outcomeof patients managed with acute total hip arthroplasty and studiesinvolving patients who had ORIF, it was noted that operativetimes were shorter, blood loss was greater, and mortality was notsignificantly different between the two groups17. The mean ShortForm-36 score was better for acute total hip arthroplasty (57.9
versus 48.5 points; p < 0.001); however, the mean Harris hipscore was better for the ORIF group (87.9 versus 74.0 points; p <0.001)17. A summary of the available literature is given in Table II.
Delayed Total Hip ArthroplastyDelayed total hip arthroplasty is offered in the setting of post-traumatic arthritis following failure of ORIF or nonoperativetreatment. Total hip arthroplasty in this setting involves a numberof obstacles and should be approached as a revision arthroplasty.These obstacles include scarring, heterotopic bone, retainedhardware, acetabular deformity, acetabular nonunion, potentialquiescent infection, and osteonecrosis of the femoral head51.
Historically, the issues with arthroplasty in this settinghave revolved around fixation of the acetabular component.Romness and Lewallen reported on fifty-five total hip arthro-plasties performed with cement and noted a 50% rate of ra-diographic acetabular loosening and a 15% rate of componentrevision52. Weber et al. described sixty-three patients with failureafter ORIF who had conversion to total hip arthroplasty53. Of theforty-one prostheses inserted with cement, fifteen (37%) went onto loosen and nine required revision. By comparison, none of thepress-fit components loosened53. Contemporary literature hasbeen more supportive of the press-fit acetabular revision type ofcomponents with multiple screw options. Bellabarba et al.
Fig. 4-A
Figs. 4-A and 4-B A seventy-two-year-old man with a protrusio type of acetabular fracture on the right side resulting from a low-energy mechanism of injury.
Fig. 4-A Preoperative anteroposterior radiograph.
766
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 97-A d NUMBER 9 d MAY 6, 2015ACETABULAR FRACTURES IN THE ELDERLY

reported on thirty patients with posttraumatic osteoarthritis trea-ted with cementless acetabular components and noted a Kaplan-Meier ten-year survival rate of 97%54. In their series, fifteen patientshad a previous failed ORIF, and fifteen had failed nonoperativetreatment. They noted that those with previous ORIF had signif-icantly longer operating-room times (p < 0.001), more blood loss,and higher transfusion rates; however, given the restored pelvicanatomy, there was a decreased need for bone-grafting54.
Comparison of delayed total hip arthroplasty after ace-tabular fracture and primary total hip arthroplasty has yieldedvarying results. In their series, Bellabarba et al. compared theirpatients with a consecutive series of patients who had primarytotal hip arthroplasty 54. Component survival based on revisionor radiographic loosening was similar between the groups at97% and 99% at a mean follow-up of thirty-six months (range,twenty-four to 140 months)54.
OverviewAcetabular fractures in the elderly are becoming increasinglycommon and require advanced surgical skills for management.ORIF can provide acceptable outcomes when a concentric, con-gruent joint reduction is obtained. However, there remains a 22%conversion rate to total hip arthroplasty at a mean of twenty-nine
months17. For patients with poor prognostic factors, primarytreatment of the injury with acute total hip arthroplasty followingstabilization of the fracture provides excellent outcomes. Cautionshould be employed when approaching delayed total hip arthro-plasty as this procedure can be substantially more complex incomparisonwith primary total hip arthroplasty. In general, futureresearch efforts should focus specifically on the low-energy, os-teopenic fracture patterns rather than chronologic age to removethe existing heterogeneity of fracture patterns in the literature. n
Derek Butterwick, MD, FRCSCSteve Papp, MD, MSc, FRCSCWade Gofton, MD, MEd, FRCSCAllan Liew, MD, FRCSCPaul E. Beaule, MD, FRCSCDivision of Orthopedic Surgery,The Ottawa Hospital,University of Ottawa,501 Smyth Road, Ottawa,ON K1H 8L6, Canada.E-mail address for S. Papp: [email protected]
Fig. 4-B
Anteroposterior radiograph made after treatment with anterior column fixation and an acute total hip arthroplasty using a titanium cage through a Levine
anterior approach.
767
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 97-A d NUMBER 9 d MAY 6, 2015ACETABULAR FRACTURES IN THE ELDERLY

References
1. Johnell O, Kanis JA. An estimate of the worldwide prevalence and disability as-sociated with osteoporotic fractures. Osteoporos Int. 2006 Dec;17(12):1726-33.Epub 2006 Sep 16.2. Johnell O, Kanis JA. An estimate of the worldwide prevalence, mortality anddisability associated with hip fracture. Osteoporos Int. 2004 Nov;15(11):897-902.Epub 2004 May 4.3. Brauer CA, Coca-Perraillon M, Cutler DM, Rosen AB. Incidence andmortality of hipfractures in the United States. JAMA. 2009 Oct 14;302(14):1573-9.4. Ferguson TA, Patel R, Bhandari M, Matta JM. Fractures of the acetabulum inpatients aged 60 years and older: an epidemiological and radiological study. J BoneJoint Surg Br. 2010 Feb;92(2):250-7.5. Mears DC. Surgical treatment of acetabular fractures in elderly patients withosteoporotic bone. J Am Acad Orthop Surg. 1999 Mar-Apr;7(2):128-41.6. Culemann U, Holstein JH, Kohler D, Tzioupis CC, Pizanis A, Tosounidis G,Burkhardt M, Pohlemann T. Different stabilisation techniques for typical acetabularfractures in the elderly—a biomechanical assessment. Injury. 2010 Apr;41(4):405-10. Epub 2009 Dec 24.7. HessmannMH,Nijs S, RommensPM. [Acetabular fractures in the elderly. Results of asophisticated treatment concept]. Unfallchirurg. 2002 Oct;105(10):893-900. German.8. Pagenkopf E, Grose A, Partal G, Helfet DL. Acetabular fractures in the elderly:treatment recommendations. HSS J. 2006 Sep;2(2):161-71.9. Letournel E. Fractures of the acetabulum. Berlin: Springer; 1993.10. Beaule PE, Griffin DB, Matta JM. The Levine anterior approach for total hipreplacement as the treatment for an acute acetabular fracture. J Orthop Trauma.2004 Oct;18(9):623-9.11. Beaule PE, Dorey FJ, Matta JM. Letournel classification for acetabular fractures.Assessment of interobserver and intraobserver reliability. J Bone Joint Surg Am.2003 Sep;85(9):1704-9.12. Borrelli J Jr, Goldfarb C, Catalano L, Evanoff BA. Assessment of articular fragmentdisplacement in acetabular fractures: a comparison of computerized tomography andplain radiographs. J Orthop Trauma. 2002 Aug;16(7):449-56; discussion 456-7.13. Tornkvist H, Schatzker J. Acetabular fractures in the elderly: an easily misseddiagnosis. J Orthop Trauma. 1993;7(3):233-5.14. Iwata T, Nozawa S, Dohjima T, Yamamoto T, Ishimaru D, Tsugita M, Maeda M,Shimizu K. The value of T1-weighted coronal MRI scans in diagnosing occult fractureof the hip. J Bone Joint Surg Br. 2012 Jul;94(7):969-73.15. Quinn SF, McCarthy JL. Prospective evaluation of patients with suspected hipfracture and indeterminate radiographs: use of T1-weighted MR images. Radiology.1993 May;187(2):469-71.16. Lubovsky O, Liebergall M, Mattan Y, Weil Y, Mosheiff R. Early diagnosis of occulthip fractures MRI versus CT scan. Injury. 2005 Jun;36(6):788-92. Epub 2005 Apr 7.17. Daurka JS, Pastides PS, Lewis A, Rickman M, Bircher MD. Acetabular fracturesin patients aged >55 years: a systematic review of the literature. Bone Joint J. 2014Feb;96-B(2):157-63.18. Mears DC, Velyvis JH, Chang CP. Displaced acetabular fractures managed op-eratively: indicators of outcome. Clin Orthop Relat Res. 2003 Feb;407:173-86.19. Mears DC, Velyvis JH. Acute total hip arthroplasty for selected displaced acetab-ular fractures: two to twelve-year results. J Bone Joint Surg Am. 2002 Jan;84(1):1-9.20. Anglen JO, Burd TA, Hendricks KJ, Harrison P. The “gull sign”: a harbinger offailure for internal fixation of geriatric acetabular fractures. J Orthop Trauma. 2003Oct;17(9):625-34.21. Laflamme GY, Hebert-Davies J, Rouleau D, Benoit B, Leduc S. Internal fixationof osteopenic acetabular fractures involving the quadrilateral plate. Injury. 2011Oct;42(10):1130-4. Epub 2010 Dec 14.22. Carroll EA, Huber FG, Goldman AT, Virkus WW, Pagenkopf E, Lorich DG, HelfetDL. Treatment of acetabular fractures in an older population. J Orthop Trauma. 2010Oct;24(10):637-44.23. Tannast M, Najibi S, Matta JM. Two to twenty-year survivorship of the hip in 810patients with operatively treated acetabular fractures. J Bone Joint Surg Am. 2012Sep 5;94(17):1559-67.24. Matta JM, Anderson LM, Epstein HC, Hendricks P. Fractures of the acetabulum.A retrospective analysis. Clin Orthop Relat Res. 1986 Apr;205:230-40.25. Sen RK, Veerappa LA. Long-term outcome of conservatively managed displacedacetabular fractures. J Trauma. 2009 Jul;67(1):155-9.26. Spencer RF. Acetabular fractures in older patients. J Bone Joint Surg Br. 1989Nov;71(5):774-6.27. Tornetta P 3rd. Displaced acetabular fractures: indications for operative andnonoperative management. J Am Acad Orthop Surg. 2001 Jan-Feb;9(1):18-28.28. Gansslen A, Hildebrand F, Krettek C. Conservative treatment of acetabular bothcolumn fractures: does the concept of secondary congruence work? Acta Chir OrthopTraumatol Cech. 2012;79(5):411-5.29. Olson SA, Matta JM. The computerized tomography subchondral arc: a newmethod of assessing acetabular articular continuity after fracture (a preliminaryreport). J Orthop Trauma. 1993;7(5):402-13.
30. Jain R, Basinski A, Kreder HJ. Nonoperative treatment of hip fractures. IntOrthop. 2003;27(1):11-7. Epub 2002 Nov 12.31. Tile M. Fractures of the pelvis and acetabulum. 2nd ed. Baltimore: Williams &Wilkins; 1995.32. Letournel E. The treatment of acetabular fractures through the ilioinguinal ap-proach. Clin Orthop Relat Res. 1993 Jul;292:62-76.33. Matta JM. Fractures of the acetabulum: accuracy of reduction and clinical re-sults in patients managed operatively within three weeks after the injury. J Bone JointSurg Am. 1996 Nov;78(11):1632-45.34. Miller AN, Prasarn ML, Lorich DG, Helfet DL. The radiological evaluation ofacetabular fractures in the elderly. J Bone Joint Surg Br. 2010 Apr;92(4):560-4.35. Cole JD, Bolhofner BR. Acetabular fracture fixation via a modified Stoppa limitedintrapelvic approach. Description of operative technique and preliminary treatmentresults. Clin Orthop Relat Res. 1994 Aug;305:112-23.36. Sagi HC, Afsari A, Dziadosz D. The anterior intra-pelvic (modified Rives-Stoppa)approach for fixation of acetabular fractures. J Orthop Trauma. 2010 May;24(5):263-70.37. Archdeacon MT, Kazemi N, Guy P, Sagi HC. The modified Stoppa approach foracetabular fracture. J Am Acad Orthop Surg. 2011 Mar;19(3):170-5.38. Jeffcoat DM, Carroll EA, Huber FG, Goldman AT, Miller AN, Lorich DG, Helfet DL.Operative treatment of acetabular fractures in an older population through a limitedilioinguinal approach. J Orthop Trauma. 2012 May;26(5):284-9.39. Rickman M, Young J, Trompeter A, Pearce R, Hamilton M. Managing acetabularfractures in the elderly with fixation and primary arthroplasty: aiming for earlyweightbearing. Clin Orthop Relat Res. 2014 Nov;472(11):3375-82.40. Laflamme GY, Hebert-Davies J. Direct reduction technique for superomedialdome impaction in geriatric acetabular fractures. J Orthop Trauma. 2014 Feb;28(2):e39-43.41. Gary JL, Lefaivre KA, Gerold F, Hay MT, Reinert CM, Starr AJ. Survivorship of thenative hip joint after percutaneous repair of acetabular fractures in the elderly. Injury.2011 Oct;42(10):1144-51. Epub 2010 Sep 20.42. Starr AJ, Reinert CM, Jones AL. Percutaneous fixation of the columns of theacetabulum: a new technique. J Orthop Trauma. 1998 Jan;12(1):51-8.43. Gary JL, VanHal M, Gibbons SD, Reinert CM, Starr AJ. Functional outcomes inelderly patients with acetabular fractures treated with minimally invasive reductionand percutaneous fixation. J Orthop Trauma. 2012 May;26(5):278-83.44. ArchdeaconMT, Kazemi N, CollingeC, Budde B, Schnell S. Treatment of protrusiofractures of the acetabulum in patients 70 years and older. J Orthop Trauma. 2013May;27(5):256-61.45. Mears DC, Shirahama M. Stabilization of an acetabular fracture with cables foracute total hip arthroplasty. J Arthroplasty. 1998 Jan;13(1):104-7.46. Mouhsine E, Garofalo R, Borens O, Fischer JF, Crevoisier X, Pelet S, Blanc CH,Leyvraz PF. Acute total hip arthroplasty for acetabular fractures in the elderly: 11patients followed for 2 years. Acta Orthop Scand. 2002 Dec;73(6):615-8.47. Herscovici D Jr, Lindvall E, Bolhofner B, Scaduto JM. The combined hip proce-dure: open reduction internal fixation combined with total hip arthroplasty for themanagement of acetabular fractures in the elderly. J Orthop Trauma. 2010 May;24(5):291-6.48. Chakravarty R, Toossi N, Katsman A, Cerynik DL, Harding SP, Johanson NA.Percutaneous column fixation and total hip arthroplasty for the treatment of acuteacetabular fracture in the elderly. J Arthroplasty. 2014 Apr;29(4):817-21. Epub 2013Sep 24.49. Enocson A, Blomfeldt R. Acetabular fractures in the elderly treated with a pri-mary Burch-Schneider reinforcement ring, autologous bone graft, and a total hiparthroplasty: a prospective study with a 4-year follow-up. J Orthop Trauma. 2014Jun;28(6):330-7.50. Chana-Rodrıguez F, Villanueva-Martınez M, Rojo-Manaute J, Sanz-Ruız P,Vaquero-Martın J. Cup-cage construct for acute fractures of the acetabulum,re-defining indications. Injury. 2012 Dec;43(Suppl 2):S28-32.51. Sierra RJ, Mabry TM, Sems SA, Berry DJ. Acetabular fractures: the role of totalhip replacement. Bone Joint J. 2013 Nov;95-B(11)(Suppl A):11-6.52. Romness DW, Lewallen DG. Total hip arthroplasty after fracture of the acetab-ulum. Long-term results. J Bone Joint Surg Br. 1990 Sep;72(5):761-4.53. Weber M, Berry DJ, Harmsen WS. Total hip arthroplasty after operative treat-ment of an acetabular fracture. J Bone Joint Surg Am. 1998 Sep;80(9):1295-305.54. Bellabarba C, Berger RA, Bentley CD, Quigley LR, Jacobs JJ, Rosenberg AG,Sheinkop MB, Galante JO. Cementless acetabular reconstruction after acetabularfracture. J Bone Joint Surg Am. 2001 Jun;83(6):868-76.55. Boraiah S, Ragsdale M, Achor T, Zelicof S, Asprinio DE. Open reduction internalfixation and primary total hip arthroplasty of selected acetabular fractures. J OrthopTrauma. 2009 Apr;23(4):243-8.56. Lin C, Caron J, Schmidt A, Torchia M, Templeman D. Functional outcomes aftertotal hip arthroplasty for the acute management of acetabular fractures: 1 to 14 yearfollow up. J Orthop Trauma. 2014 Jun 26. [Epub ahead of print].
768
THE JOURNAL OF BONE & JOINT SURGERY d J B J S .ORG
VOLUME 97-A d NUMBER 9 d MAY 6, 2015ACETABULAR FRACTURES IN THE ELDERLY