Embed Size (px)
Citation preview

Anaesthesia in ACHD Dr Amit Ranjan
Consultant Cardiac anaesthetist and cardiac intensive care
Bristol Heart Institute

Introduction
CHD is most common birth defects, 1% of newly born .
Improvement and new surgical technique- CHD pt live longer, and pose
significant challenge .
Perioperative care is challenging and need to be evidence based.
Thorough knowledge of pathology and physiological changes is key of
successful management of ACHD.

Physiologic Classification Congenital
Heart Disease
Acyanotic CHD
• With Left-to-Right Shunt
• Without Left-to-Right Shunt
Cyanotic CHD
• Ductal-dependent Pulmonary Blood Flow
• Ductal-dependent Systemic Blood Flow
• Mixing Lesions

Acyanotic CHD
1. With L-to-R shunt
• Physiology - Volume overload in at least 1 cardiac chamber • Increase
Pulmonary Blood Flow can lead to PHTN
exp..ASD, VSD, PDA, PAPVR
2. Without L-to-R shunt
• Physiology- Increase pressure load • Limited CO/blood flow • Can lead to
significant cardiac hypertrophy
Exp.. Valve disease , Coarctation of Aorta

Cyanotic CHD
Right-to-Left shunt
• Venous admixture is added to the systemic circulation
• Ductal-dependent PBF
• Tetralogy of Fallot
• Pulmonary Atresia
• Tricuspid Atresia
• Single Ventricle
• Ductal-dependent SBF
• Critical Coarctation of Aorta
• Critical Aortic Stenosis
• Hypoplastic Left Heart Syndrome
• Mixing Lesions
• AVSD
• Double Outlet Right Ventricle
• TAPVR
• Transposition of the Great Arteries
• Truncus Arteriosus

Adult Congenital Heart Disease Most common congenital disorder of newborns
• 1% of live births
• Advances in cardiovascular medicine and surgery
85-95% survive to adulthood
15-25% survival of patients prior to treatment availability

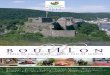
Long term Survival by complexity of
CHD
95%
Simple
90 %
Moderate
80%
Severe
ASD Anamolous Pulmonary
venous drainage
Single ventricle palliation
VSD Atriaventicular canal
defect
TGA
PFO Coarctation of aorta Truncus arteriosus
PDA TOF Tricuspid atresia
Mild PS VSD with assoc Pulmonary atresia

Long term sequelae – Cardiac
• Pulmonary hypertension
• Ventricular dysfunction
• Dysrhythmias and conduction defects
• Residual shunts - Cyanosis
• Valvular lesions- Stenosis, regurgitation
• Hypertension
• Aneurysms

Long term sequelae – Non cardiac
Secondary erythrocytosis
• Cholelithiasis
• Nephrolithiasis
• Neurodevelopment
abnormalities
• CNS disease
• Seizure
• CVA (thromboembolism)
• Hearing/vision loss
• Chronic lung disease
• Hepatic dysfunction, Cirrhosis
• Renal impairment
• Coagulopathy
• Cancers

ACHD management issues:
Changing Age prevalence of CHD
Which hospital for ACHD patients?
Which anaesthetist for which ACHD patient ?

Changing age prevalence of CHD
Increasing survival in CHD has changed age distribution of CHD patients.
One of the most important improvements was achieved by Fontan and
Baudet, pioneers in the field of single ventricle palliation.
Numbers of ACHD now surpasses those of children with CHD. More than a
third of these ACHD patients are currently at least 45years old.

Which hospital for ACHD
Several recommendations and guidelines – though level of evidence is low.
Any non cardiac surgical procedure in CHD pt carries a much higher risk
than non –CHD grp of patients.
Severe/complex CHD grp mortality increase by 2 folds compared to
control, however, with minor/simple CHD no such increase in mortality.
Despite missing high level evidence, its recommended that patient with
complex CHD should be treated by specialised centres, even if surgical risks
of non-cardiac procedures may be rated as low.

Which anaesthetist for which ACHD
In 2008 ACC/AHA recommended that all general anaesthesia and
sedation in ACHD with moderate to complex CHD should be performed in
regional ACHD centre.
Enough evidence and studies done to show that, if surgical procedure
done in mod./complex CHD grown up in non-cardiac centre or
noncardiac anaesthetists- morbidity and mortality is high.
More cardiac arrests in CHD patients were reported during non cardiac
surgery in the genral operating room (54%) than during cardiac surgery
(26%) and cardiac catherization (17%).

Anaesthetic Management
3 grp of ACHD
1. Uncorrected CHD patients
2. Patients with previous palliative surgery
3. Patients with previous corrective surgery .
Anaesthetic management in ACHD patients may change completely
depending on type of repair, age at repair, associated defects with specific
long term risk factors and complications.

Preoperative Risk assessment for
anaesthesia
Individual risk of ACHD patients depends on 4 aspect:
1. Underlying nature of CHD
2. Individual course of CHD
3. Aware of substantial CHD associated noncardiac morbidity
4. Type of cardiac/noncardiac surgical procedure.

Heart Failure
Leading cause of death in ACHD
Evaluation of HF in ACHD is more tricky – rely on physical status and echo
- Biomarker like NT-proBNP – useful tool . NTproBNP >33.3pmol/l is strongly
associated with cardiovascular events and death or HF.
In CHD pt, NTproBNP levels <15.2 pmol/l , the cumulative proportion of death
and HF was below 1%.

Arrythmias and Anticoagulation
Supraventricular tachycardia is more than ventricular arrythmias
ACC/AHA guidelines in 2016 for Mx of arrythmias in ACHD
Anticoagulation – AF
scoring system CHADS2 – not predictive for thromboembolic risk in ACHD
ACHD pts aged below 55 yrs revealed a 9-12 times higher age-sex
standardized incidence rate of ischaemic stroke.

More complex CHD – more high risk of thromboembolic events, Khairy et al.
perioperative anticoagulation has to be evaluated by a MDT, carefully
opposing risks of thromboembolic complications vs haemorrhage.
Recent evidence, Bouillon et al, suggest that for non CHD patients , bridging
therapy with heparin in AF pt., is associated with more risk of bleeding and a
similar risk arterial thromboembolism compared with no bridging therapy.
-------whether this can be transferred to ACHD pt., we need further studies.

Anaesthetic Technique
Regional Anaesthesia :
Look for bony deformity, able to lie flat, anticoagulation .
Physiological changes.
- General anaesthesia :
No anaesthetic technique is prohibited in ACHD patients. However, a
profound understanding of anaesthesia induced physiological changes and
anticipation of consequences in abnormal circulation in each individual ACHD
case is crucial.

Fontan Population
Major long term problems in Fontan patients are supraventricular
arrythmias, heart failure , Fontan specific problems like protein-losing
enteropathy, pulmonary arteriovenous fistulae, as well as liver disease
including liver cirrhosis and hepatocellular carcinoma.
During GA – high risk of haemodynamic instability due to positive pressure
ventilation. (Passive lung perfusion – increase in intrathoracic pressure –
impaired transpulmonary pressure gradient – low pulmonary flow – Low CO)
Fontan hearts often reeal an impaired ventricular systolic contractile
function and a chronotropic incompetence as wellas pre-load
dependence, which is essential for intraoperative anaesthetic
management.
Tachycardia, bradycardia, hypovolemia, and positive pressure ventilation
are therefore undesirable in patients with Fontan circulation.

Shunts & Cyanosis in CHD
Haemodynamic point of views, 3 types of shunt
1. Intracardiac ( ASD, VSD)
2. Vascular shunt ( systemic to pulmonary shunt)
3. Complex shunt ( truncus arteriosus, TAPVD etc)
Most Left – Rt shunt , causing increase PBF, and if longstanding PulmHT, Rt sided heart issues.
Shunt reversal can happen during anaesthesia – systemic hypopersion – acidosis – further decrease in SVR.
Anaesthetist need to be aware of it and treat appropriately to prevent haemodynamic collapse.

Pregnancy and congenital heart
disease
Increasing number of women with complex CHD reaching child bearing
age
Women with Fontan circulation hve reached childbearing age
Anaesthesia techniques for delivery are predominantly neuraxial
catheters(86%) whereas general anaesthesia is an exception.
Most complications in this population were post partum haemorrhage and
arrythmias .
Heart failure is the most common complication during pregnancy with two
peaks – 23-30wks and around delivery .

Cardiac disease in pregnancy risk
score
Predictors of cardiovascular events Point
Prior cardiac even (Heart failure, TIA,
MI prior to surgery) or arrythmias
1
NYHA functional class at baseline > II
or Cyanosis
1
Left heart obstruction (mitral valve
area <2.0, aortic valve area <1.5, and
LV outflow tract gradient >30mmHg)
1
Reduced systolic ventricular function
( EF <40%)
1
zero point <5% risk of cardiac
complications, 1 point – 27% risk , 2 or
more >75% risk

Red flags for Anaesthesia
Cyanosis
Poor exercise tolerance
Limited mobility/ wheel chair bound
Cardiac studies shows poor EF, high pulm HTN, poor RV
Complex CHD e.g Fontan’s circulation
Allergy to common anaesthetic drugs

Conclusion
Any surgical procedure in ACHD patients carries a greater risk than in the
normal population
Growing population of ACHD – clinicians need to take care in wide range
of settings
Risk evaluation and perioperative management of CHD – associated
cardiac and noncardiac morbidity is challenging and calls for a
multidisciplinary team approach.

Questions….

Thank you ..