Embed Size (px)
Citation preview
Achieving Acute Success and Durable Results with Complete Total Occlusion?
Christopher J. Kwolek, MD FACSChristopher J. Kwolek, MD FACSHarvard Medical SchoolHarvard Medical School
Division of Vascular and Endovascular SurgeryDivision of Vascular and Endovascular SurgeryMassachusetts General HospitalMassachusetts General Hospital
Background•Peripheral arterial occlusive disease (PAOD) is associated with substantial morbidity and health care expediture
•Operative series have consistently demonstrated 5 year limb salvage rates of 80% or greater
–Complications may occur in up to 25% patients after peripheral arterial bypass surgery
•Morbidity may compromise functional outcomes as less than 50% patients report a return to “normal” by 6 months postoperatively
Background• Increasing application of endovascular
therapy to all territories of the arterial tree
• Percutaneous endovascular infrainguinal interventions (PVI) have been proposed as first line therapy for PAOD
• PVI : primary patency rates 12-90%, but secondary interventions are non-surgical
• Enthusiasm for broadening PVI indications has continued to increase!
Claudication?Limb
Salvage?
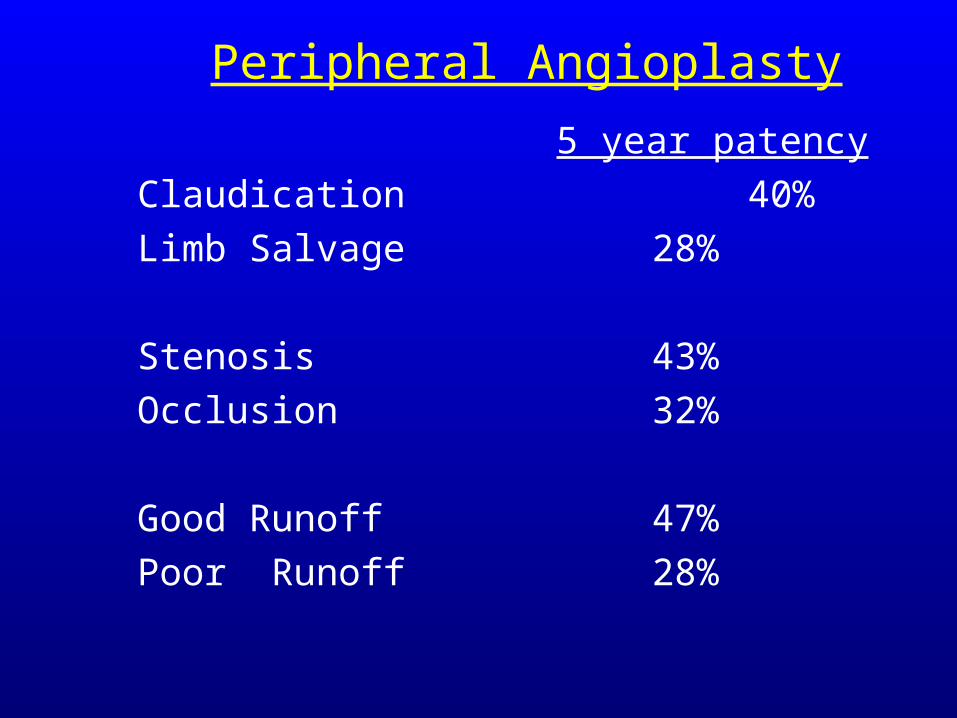
Peripheral Angioplasty
5 year patency
Claudication 40%
Limb Salvage 28%
Stenosis 43%
Occlusion 32%
Good Runoff 47%
Poor Runoff 28%
THE FUTURE DEFINED
INFRAINGUINAL DISEASE
• SFA occlusions - Traditional wisdom: The variety of endovascular interventions has produced poor results:
PTA vs. PTA/Stent Trial
• 221 patients, < 7cm SFA lesion• Angiographic failure at one year 40%• Patency @ 4 years 50%
(Becquemin et al. SVS, June ‘02)
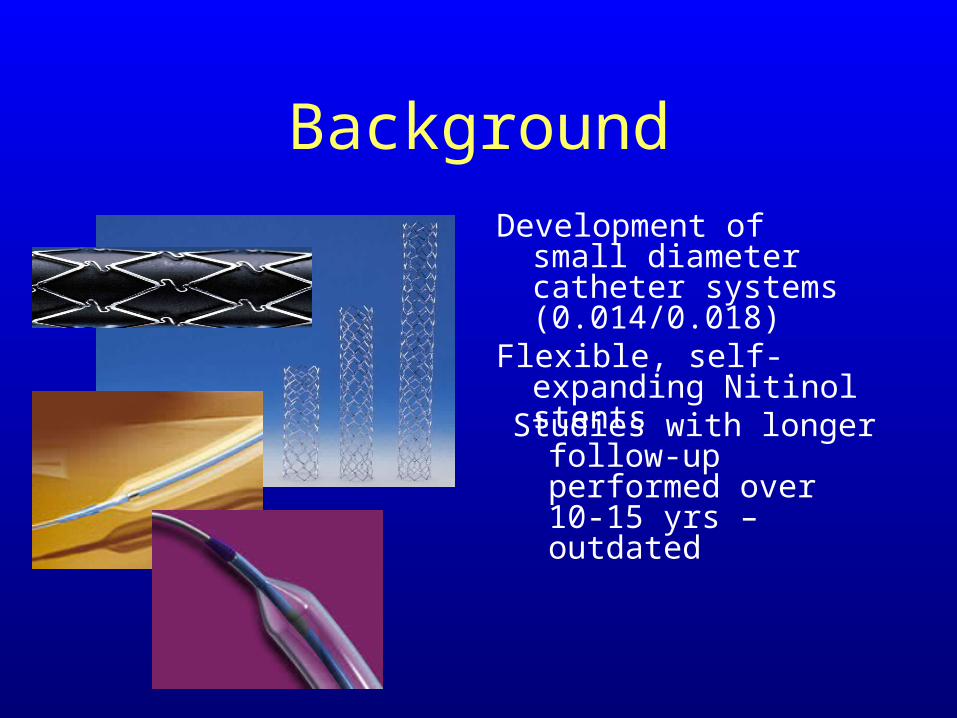
BackgroundDevelopment of small diameter
catheter systems (0.014/0.018)
Flexible, self-expanding Nitinol stents
Studies with longer follow-up performed over 10-15 yrs – outdated
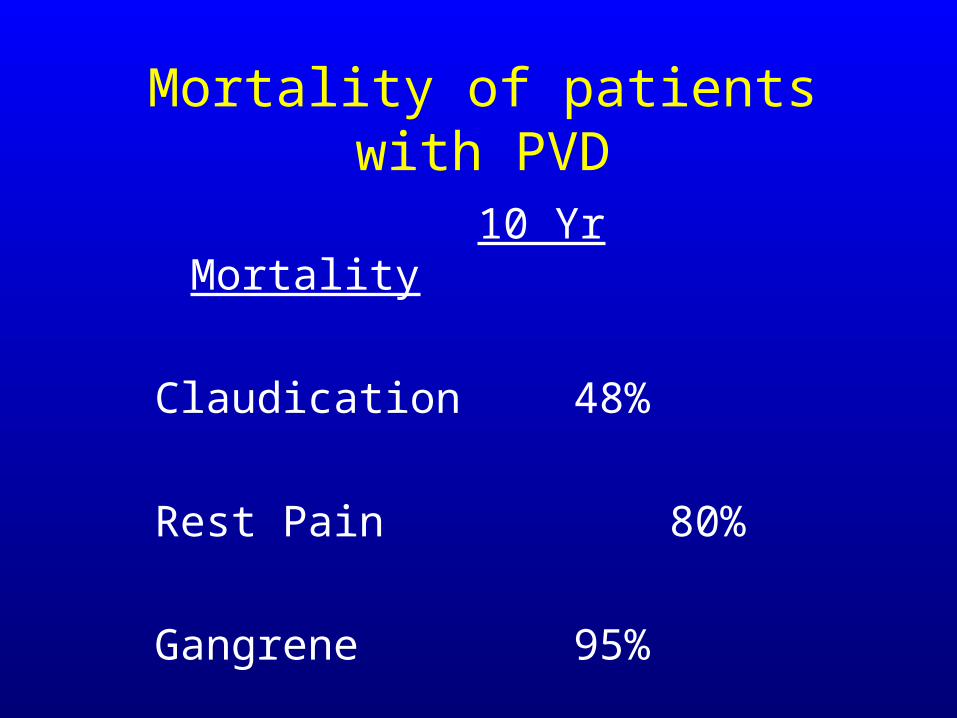
Mortality of patients with PVD
10 Yr Mortality
Claudication 48%
Rest Pain 80%
Gangrene 95%
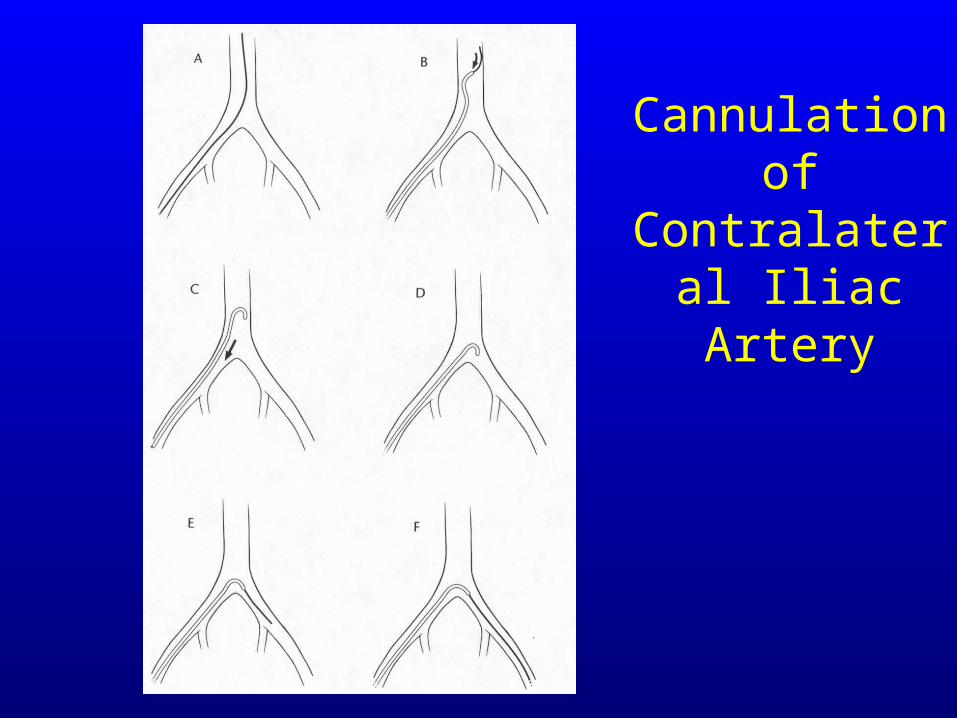
Cannulation of Contralateral Iliac Artery
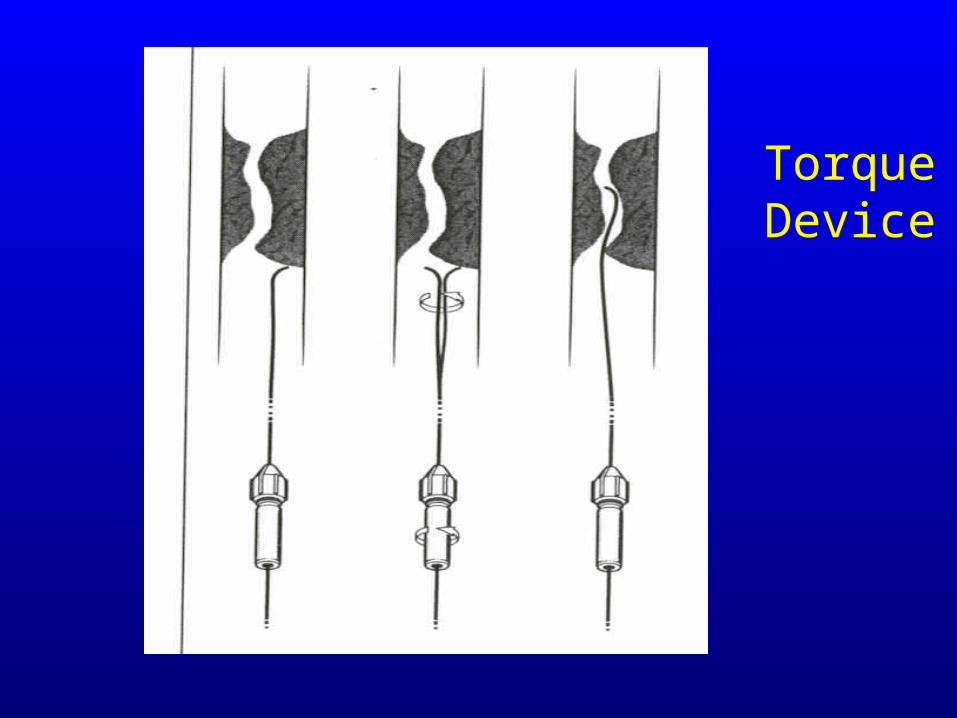
Torque Device
Technique
• Contralateral access
• Placement of a working sheath 6Fr Raabe or Balkan in the CFA or SFA
• Use of an .035” angled/straight glidewire with an angled or straight 4Fr/5FR catheter
• Try to stay intraluminal but frequently end up subintimal using the “loop” of the distal wire to advance
• REENTRY
• Retrograde popliteal/tibial approach
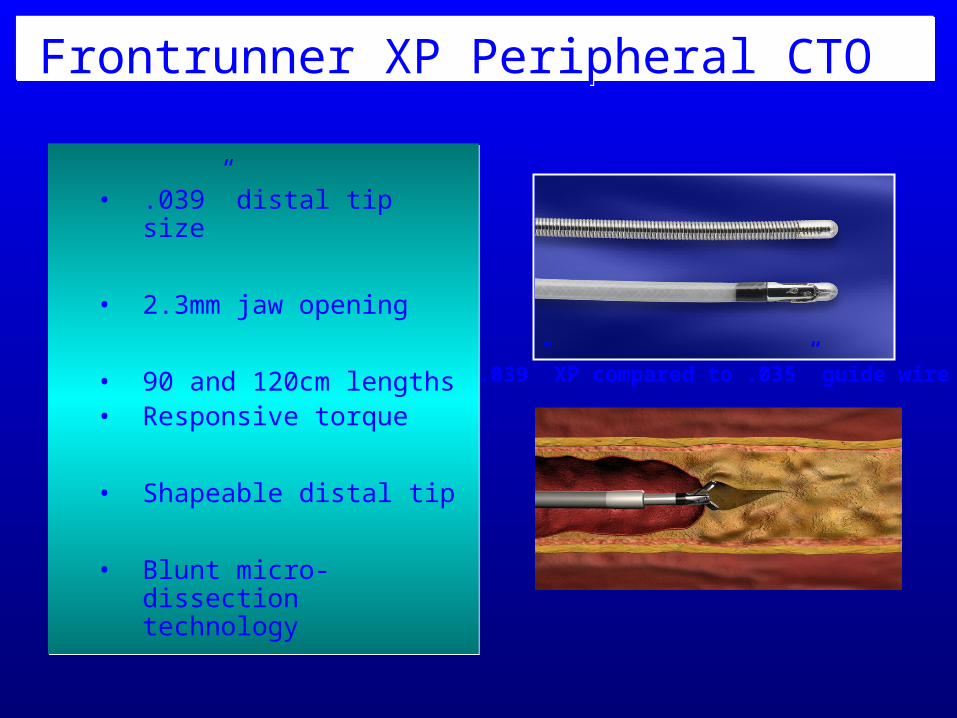
Frontrunner XP Peripheral CTO Frontrunner XP Peripheral CTO
• .039” distal tip size
• 2.3mm jaw opening
• 90 and 120cm lengths• Responsive torque
• Shapeable distal tip
• Blunt micro-dissection technology
• .039” distal tip size
• 2.3mm jaw opening
• 90 and 120cm lengths• Responsive torque
• Shapeable distal tip
• Blunt micro-dissection technology
.039” XP compared to .035” guide wire
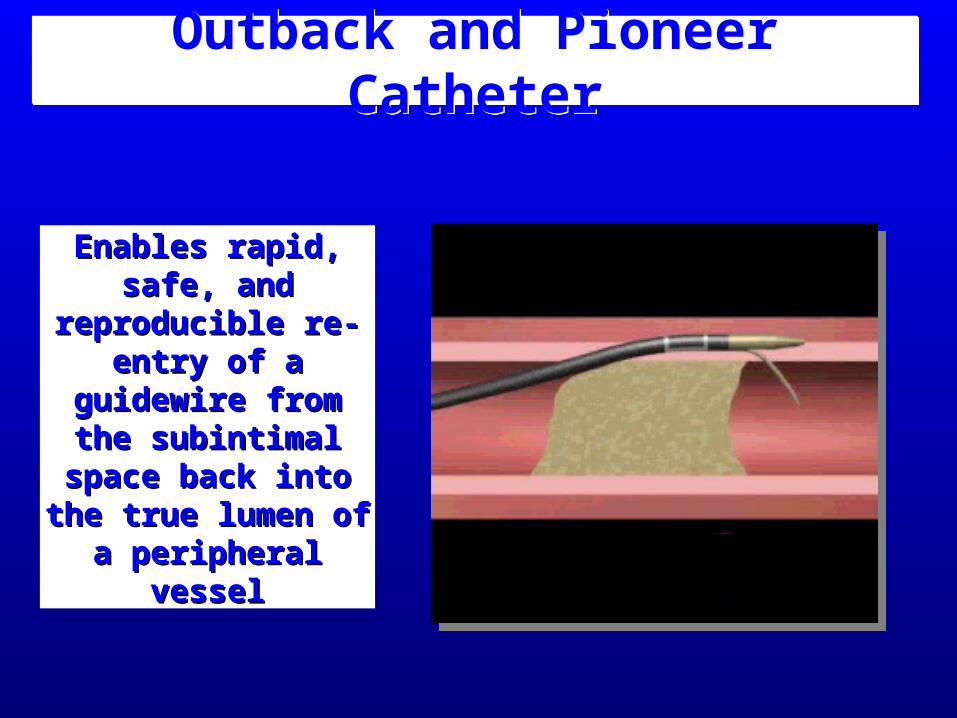
Outback and Pioneer CatheterOutback and Pioneer Catheter
Enables rapid, safe, and Enables rapid, safe, and reproducible re-entry of reproducible re-entry of
a guidewire from the a guidewire from the subintimal space back subintimal space back
into the true lumen of a into the true lumen of a peripheral vesselperipheral vessel
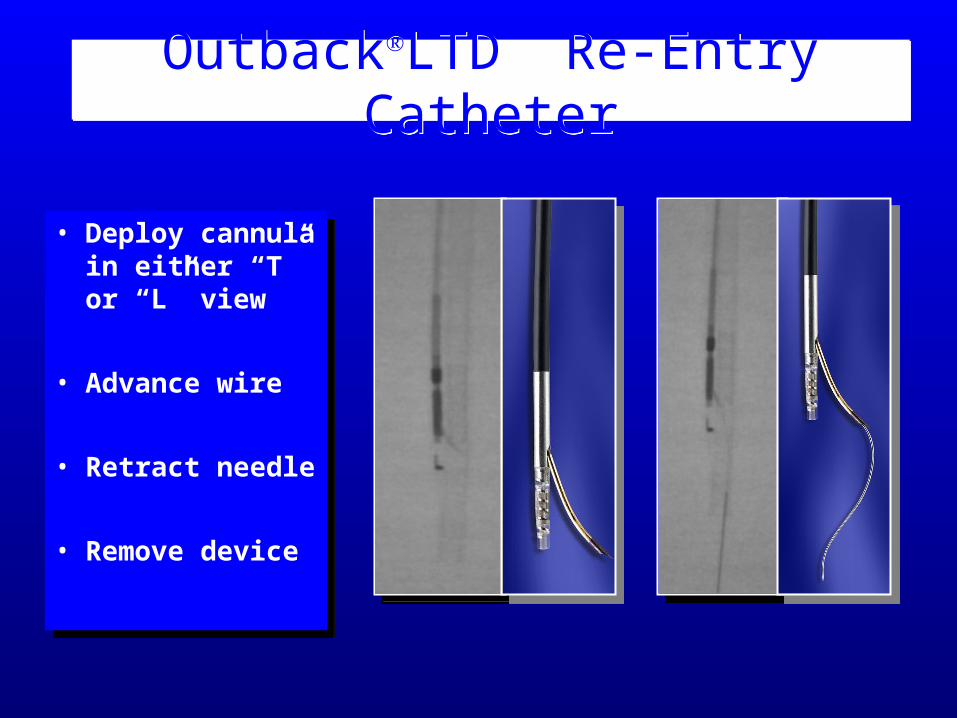
OutbackLTD Re-Entry CatheterOutbackLTD Re-Entry Catheter
• Deploy cannula in either “T” or “L” view
• Advance wire
• Retract needle
• Remove device
• Deploy cannula in either “T” or “L” view
• Advance wire
• Retract needle
• Remove device
Technique
• Once intraluminal access is regained will often switch to a low profile balloon .018” saavy or .014” coronary balloons
• Sequentially dilate up to 5 or 6 mm
• Self-expanding nitinol stents for significant recoil, dissection with flow limiting lesion
• Plavix load and then continue for at least 6 weeks then switch to ASA alone
• Flexed views of the leg
MGH Results
1) Mid-term results of femoropopliteal PTA
2) Contemporary series of patients
3) Influence of clinical variables on patency and limb salvage rates
Methods
Retrospective record review – 1/02 – 7/04Native femoropopliteal diseaseChronic LE ischemiaExclusion criteria:
Acute critical limb ischemiaFunctionally unsalvageable limbThreatened bypass graftMechanical thrombectomy/ thrombolysis
MethodsDemographic/ operative dataClinical presentation (Rutherford classification)
1-3 = Claudication 4 = Rest Pain5-6 = Tissue Loss
Lesion Anatomy (TASC classification) A = single stenosis < 3cm
B = single stenosis/occlusion 3-5cm or multiple <3cmC = single stenosis/occlusion >5cm or multiple 3-5cmD = Complete SFA/POP occlusion
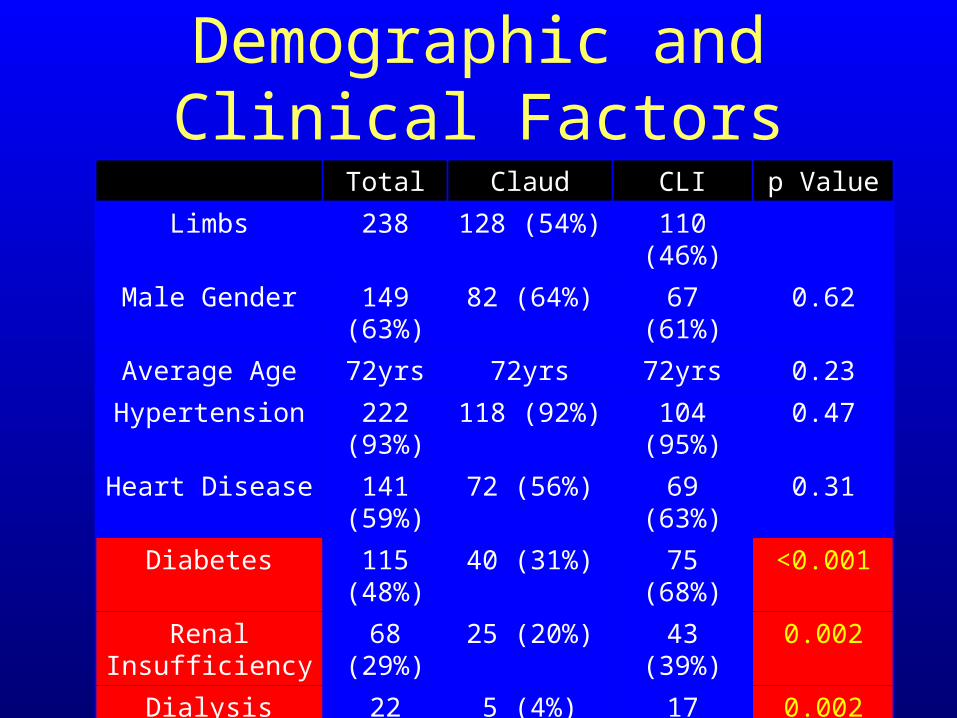
Demographic and Clinical FactorsTotal Claud CLI p Value
Limbs 238 128 (54%) 110 (46%)
Male Gender 149 (63%) 82 (64%) 67 (61%) 0.62
Average Age 72yrs 72yrs 72yrs 0.23
Hypertension 222 (93%) 118 (92%) 104 (95%) 0.47
Heart Disease 141 (59%) 72 (56%) 69 (63%) 0.31
Diabetes 115 (48%) 40 (31%) 75 (68%) <0.001
Renal Insufficiency 68 (29%) 25 (20%) 43 (39%) 0.002
Dialysis 22 (9%) 5 (4%) 17 (15%) 0.002
Current Smoker 32 (13%) 18 (14%) 14 (13%) 0.76
Previous Smoker 163 (68%) 91 (71%) 72 (65%) 0.35
Hyperlipidemia 163 (68%) 89 (70%) 74 (67%) 0.71
CHF 44 (18%) 15 (12%) 29 (23%) 0.004
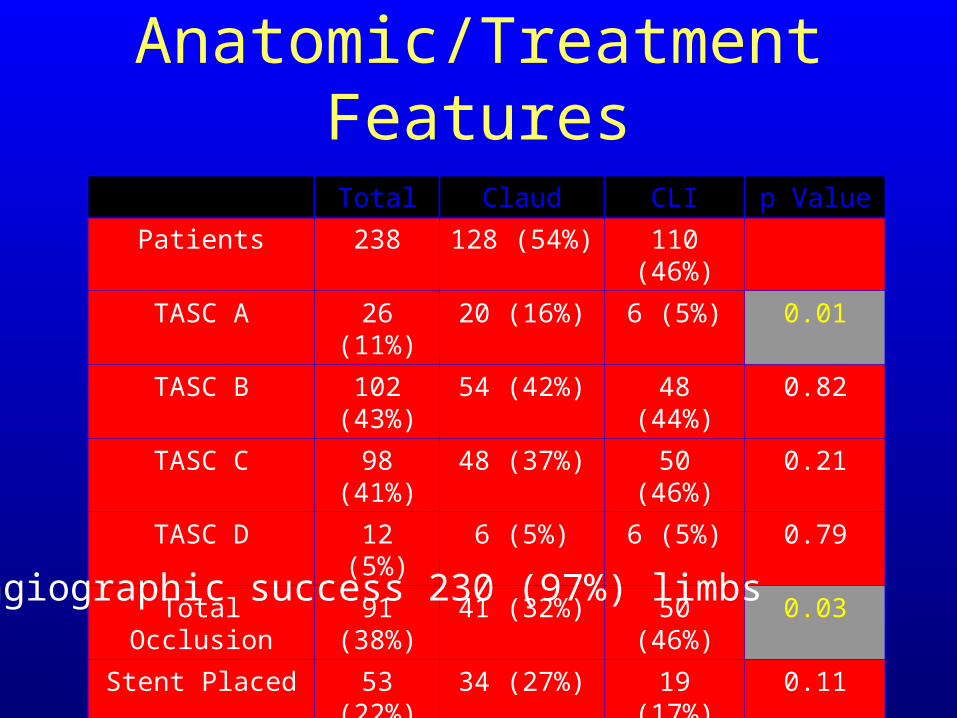
Anatomic/Treatment Features
Total Claud CLI p Value
Patients 238 128 (54%) 110 (46%)
TASC A 26 (11%) 20 (16%) 6 (5%) 0.01
TASC B 102 (43%) 54 (42%) 48 (44%) 0.82
TASC C 98 (41%) 48 (37%) 50 (46%) 0.21
TASC D 12 (5%) 6 (5%) 6 (5%) 0.79
Total Occlusion 91 (38%) 41 (32%) 50 (46%) 0.03
Stent Placed 53 (22%) 34 (27%) 19 (17%) 0.11
Angiographic success 230 (97%) limbs
Complications
No deaths related to PTA
6 Significant complications2 groin hematomas requiring transfusion1 thromboembolus – thrombolysis1 intubation from pulmonary edema1 SFA rupture – FP bypass1 device malfunction – FP bypass
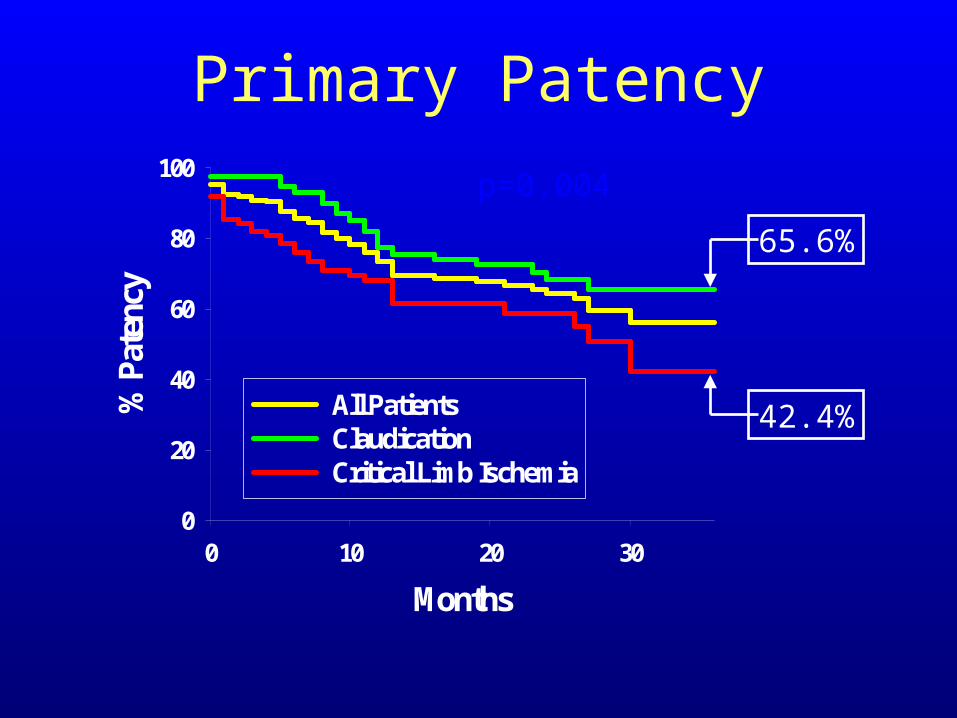
Months
0 10 20 30
% P
aten
cy
0
20
40
60
80
100
All PatientsClaudicationCritical Limb Ischemia
p=0.004
Primary Patency
42.4%
65.6%
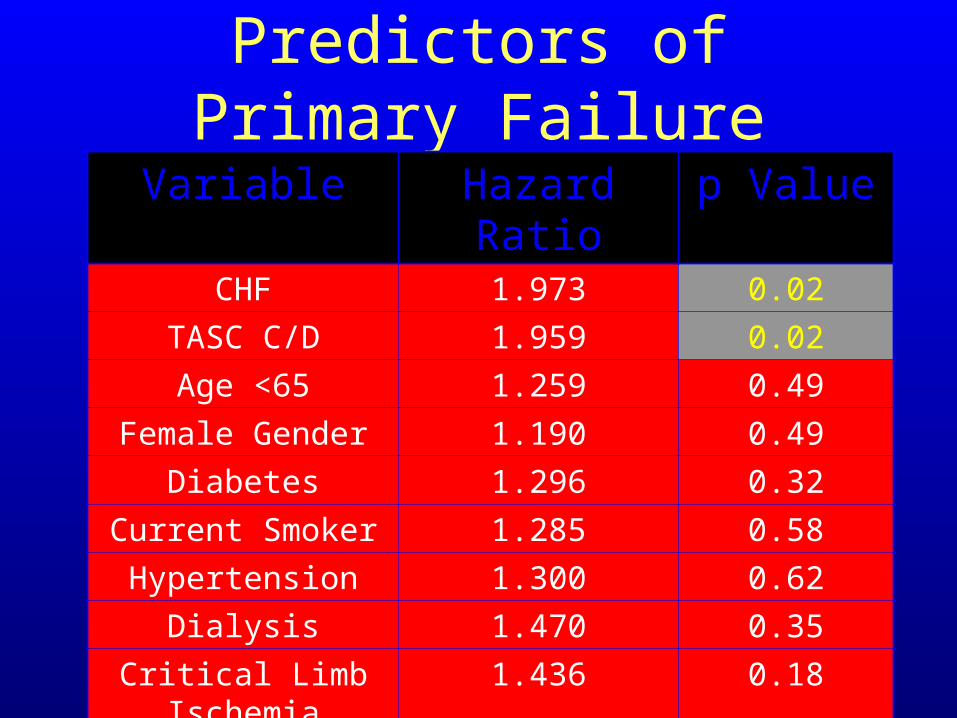
Predictors of Primary Failure
Variable Hazard Ratio p ValueCHF 1.973 0.02
TASC C/D 1.959 0.02Age <65 1.259 0.49
Female Gender 1.190 0.49Diabetes 1.296 0.32
Current Smoker 1.285 0.58Hypertension 1.300 0.62
Dialysis 1.470 0.35Critical Limb Ischemia 1.436 0.18
Occluded Lesion 1.344 0.29
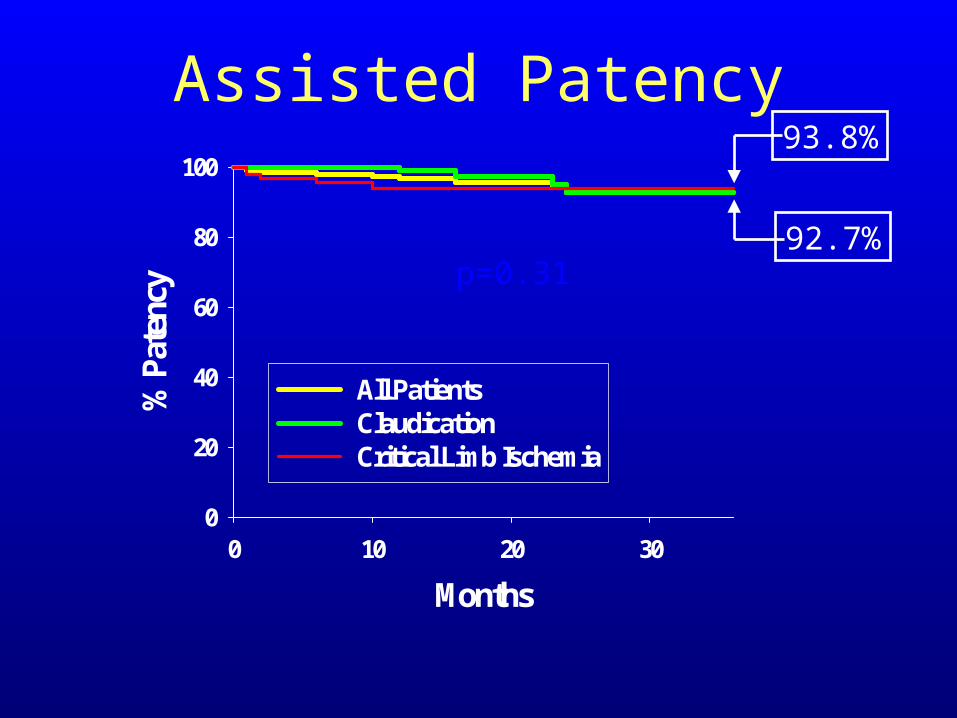
Months
0 10 20 30
% P
aten
cy
0
20
40
60
80
100
All PatientsClaudicationCritical Limb Ischemia
p=0.31
93.8%Assisted Patency
92.7%
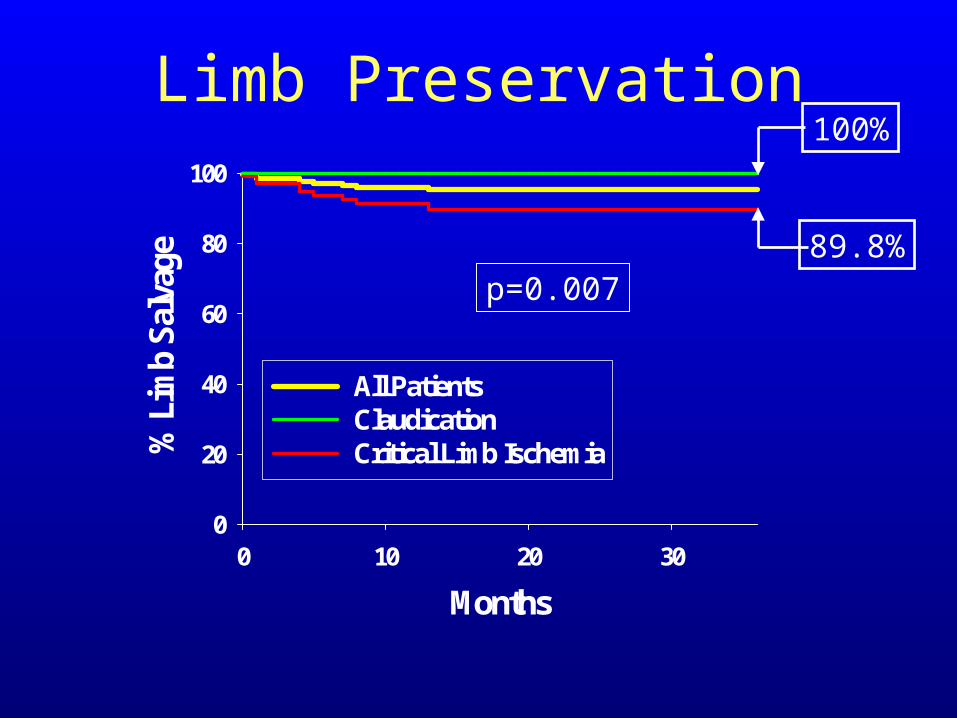
Months
0 10 20 30
% L
imb
Salv
age
0
20
40
60
80
100
All PatientsClaudicationCritical Limb Ischemia
p=0.007
100%
89.8%
Limb Preservation
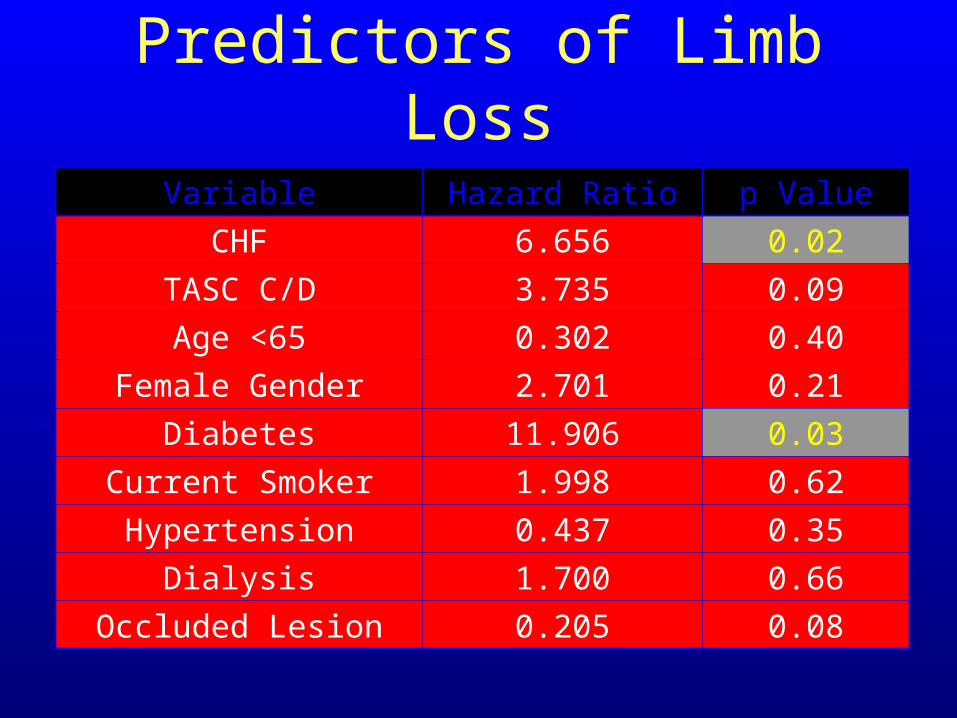
Predictors of Limb Loss
Variable Hazard Ratio p ValueCHF 6.656 0.02
TASC C/D 3.735 0.09Age <65 0.302 0.40
Female Gender 2.701 0.21Diabetes 11.906 0.03
Current Smoker 1.998 0.62Hypertension 0.437 0.35
Dialysis 1.700 0.66Occluded Lesion 0.205 0.08
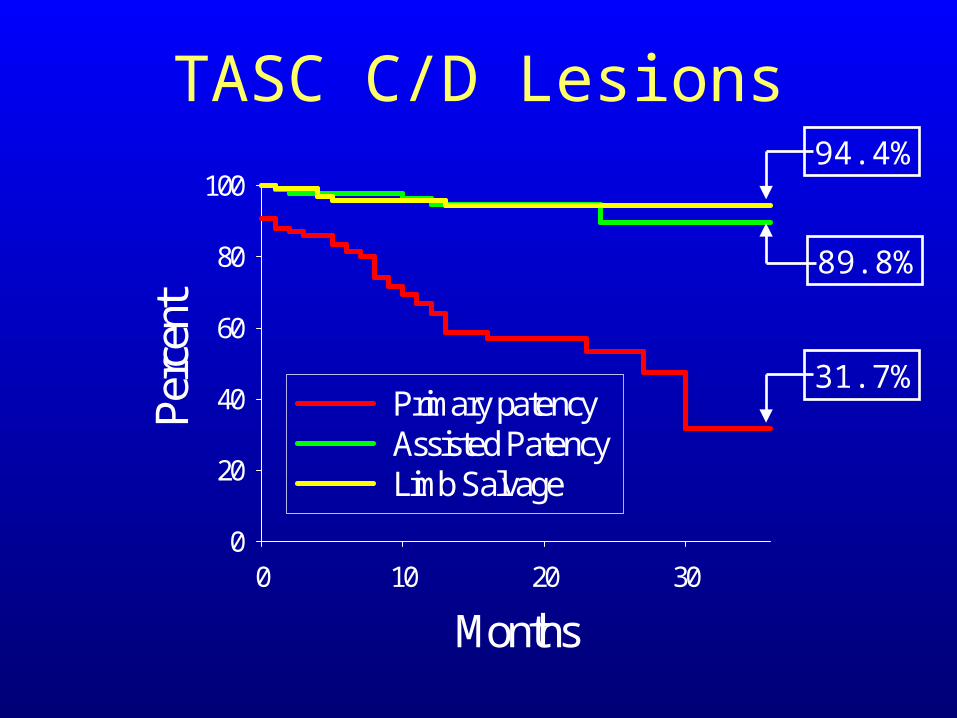
Months0 10 20 30
Perc
ent
0
20
40
60
80
100
Primary patencyAssisted Patency Limb Salvage
TASC C/D Lesions94.4%
31.7%
89.8%
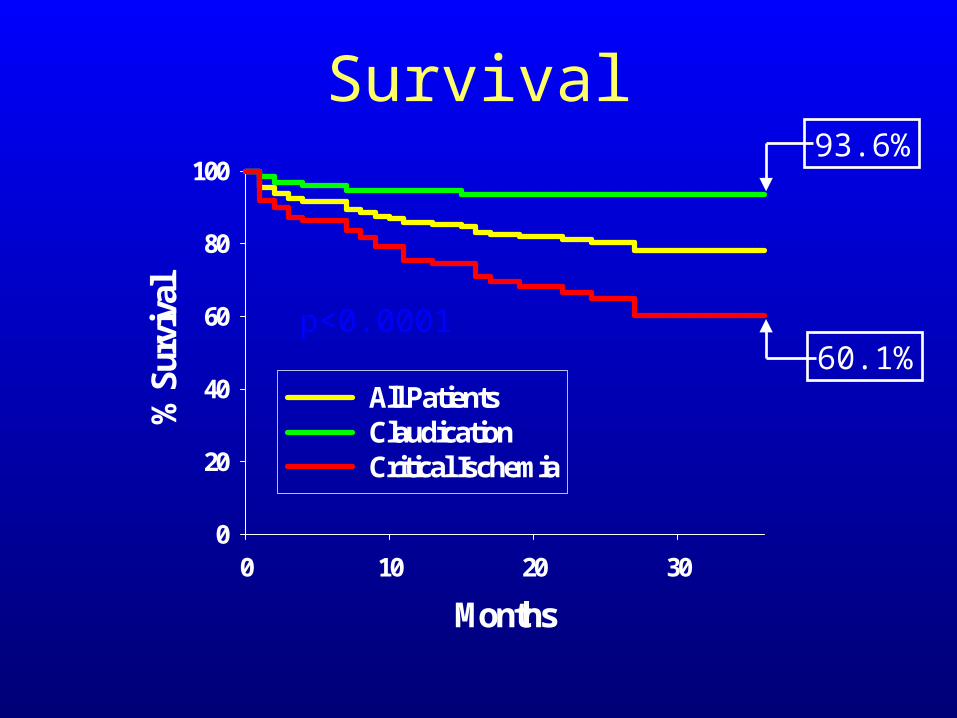
Months
0 10 20 30
% S
urvi
val
0
20
40
60
80
100
All PatientsClaudicationCritical Ischemia
p<0.0001
93.6%
60.1%
Survival
PTA of the femoropopliteal arterial segment can be performed with 97% technical success and a low peri-procedure morbidity
Three year primary patency is 54%, assisted patency is 92% and limb salvage is 89% in CLI
Summary
Predictors of primary patency failure include CHF and TASC C/D lesions
Predictors of assisted patency failure include age < 65 yrs, CHF and TASC C/D lesions
Predictors of limb loss include Diabetes and CHF
Summary
Conclusions
Although primary patency rates remain low, excellent assisted patency and limb salvage can be achieved with close follow-up
PTA should be considered as initial therapy regardless of Rutherford classification





























