Embed Size (px)
Citation preview

Acid
appl
Jia Jun Zhu, BDS
aResearch postgraduate student, PaebClinical Assistant Professor, PaediacAssociate Professor, Dental MateriadProfessor Emeritus and Honorary P
Zhu et al
etching of human enamel in clinical
ications: A systematic review
, MDS,a Alexander T. H. Tang, BDS, Odont Dr,b
Jukka P. Matinlinna, BSc, MSc, PhD,c andUrban Hägg, DDS, Odont Drd
Faculty of Dentistry, the University of Hong Kong, Hong Kong SAR;Faculty of Health Sciences, University of Copenhagen, Copenhagen,Denmark
Statement of problem. The laboratory-based enamel acid-etching doctrine with 30% to 50% phosphoric acid for 60 secondsto generate the maximum amount of Type 1 and/or Type 2 etch pattern has been established for more than 30 years.However, this recommendation may not be clinically relevant.
Purpose. The purpose of this systematic review was to compare clinically accepted protocols of enamel acid etching with thelaboratory protocol.
Material and methods. Studies were identified by searching 4 electronic databases: Medline, CINAHL Plus, Embase, andCochrane Library. The final search was run on November 8, 2012. All clinical studies published in English that investigatedenamel acid pretreatment methods on human permanent teeth were included. Additional publications were obtained fromthe reference lists of the included studies. The clinical evidence of all included studies was tabulated.
Results. Initially, 4543 publications were retrieved from the databases. A total of 4508 articles were excluded, including 2285duplicates, 1805 publications according to exclusion criteria by their titles and abstracts, 368 laboratory articles, 49 reviews,and 1 pilot study. Only 1 study was added from reference lists of the included studies. Finally, 36 clinical publications wereincluded. The included clinical studies provided different levels of clinical evidence on the efficacy of acid-etching protocols toenable successful enamel adhesion.
Conclusions. Clinical protocols of enamel acid etching differ from the laboratory-generated doctrine, which may implythat maximization of the Type 1 and/or Type 2 etch pattern is not important in the clinical acid etching of human enamel.(J Prosthet Dent 2014;-:---)
Clinical Implications
Clinical protocols of enamel acid etching varied from the ideallaboratory protocol to maximize Type 1 or 2 enamel etch patterns.However, all protocols demonstrated clinically successful enameladhesion. The laboratory-based acid-etching doctrine may not beclinically relevant.
The lack of long-term adhesion withhuman teeth was the main shortcomingof dental restorative materials before1955, when Buonocore1 reported theetching of enamel surfaces intraorallywith 85% phosphoric acid followed by
diatric Detric Dentisls Sciencerofessor, P
the placement of acrylic resin. Thismethod significantly increased theduration of resin adhesion to enamel.This study is considered to be thefoundation of lasting enamel adhesion.In the 1970s, the examination of
ntistry and Orthodontics, Faculty of Dentistry,try and Orthodontics, Faculty of Dentistry, the, Faculty of Dentistry, the University of Hong Kaediatric Dentistry and Orthodontics, Faculty
enamel surfaces after acid etchingunder scanning electron microscopyshowed 3 types of etch patterns.2
Type 1 (preferential dissolution ofenamel prism cores) and Type 2 (pref-erential dissolution of enamel prism
the University of Hong Kong.University of Hong Kong.ong.of Dentistry, the University of Hong Kong.
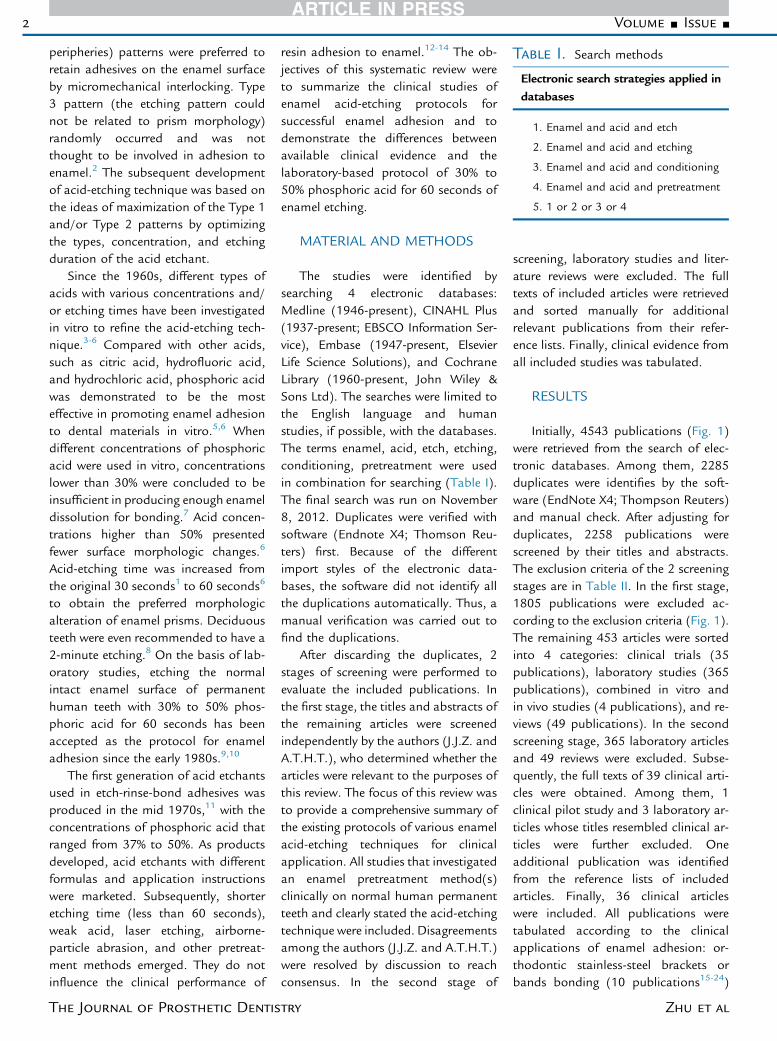
Table I. Search methods
Electronic search strategies applied indatabases
1. Enamel and acid and etch
2. Enamel and acid and etching
3. Enamel and acid and conditioning
4. Enamel and acid and pretreatment
5. 1 or 2 or 3 or 4
2 Volume - Issue -
peripheries) patterns were preferred toretain adhesives on the enamel surfaceby micromechanical interlocking. Type3 pattern (the etching pattern couldnot be related to prism morphology)randomly occurred and was notthought to be involved in adhesion toenamel.2 The subsequent developmentof acid-etching technique was based onthe ideas of maximization of the Type 1and/or Type 2 patterns by optimizingthe types, concentration, and etchingduration of the acid etchant.
Since the 1960s, different types ofacids with various concentrations and/or etching times have been investigatedin vitro to refine the acid-etching tech-nique.3-6 Compared with other acids,such as citric acid, hydrofluoric acid,and hydrochloric acid, phosphoric acidwas demonstrated to be the mosteffective in promoting enamel adhesionto dental materials in vitro.5,6 Whendifferent concentrations of phosphoricacid were used in vitro, concentrationslower than 30% were concluded to beinsufficient in producing enough enameldissolution for bonding.7 Acid concen-trations higher than 50% presentedfewer surface morphologic changes.6
Acid-etching time was increased fromthe original 30 seconds1 to 60 seconds6
to obtain the preferred morphologicalteration of enamel prisms. Deciduousteeth were even recommended to have a2-minute etching.8 On the basis of lab-oratory studies, etching the normalintact enamel surface of permanenthuman teeth with 30% to 50% phos-phoric acid for 60 seconds has beenaccepted as the protocol for enameladhesion since the early 1980s.9,10
The first generation of acid etchantsused in etch-rinse-bond adhesives wasproduced in the mid 1970s,11 with theconcentrations of phosphoric acid thatranged from 37% to 50%. As productsdeveloped, acid etchants with differentformulas and application instructionswere marketed. Subsequently, shorteretching time (less than 60 seconds),weak acid, laser etching, airborne-particle abrasion, and other pretreat-ment methods emerged. They do notinfluence the clinical performance of
The Journal of Prosthetic Dentis
resin adhesion to enamel.12-14 The ob-jectives of this systematic review wereto summarize the clinical studies ofenamel acid-etching protocols forsuccessful enamel adhesion and todemonstrate the differences betweenavailable clinical evidence and thelaboratory-based protocol of 30% to50% phosphoric acid for 60 seconds ofenamel etching.
MATERIAL AND METHODS
The studies were identified bysearching 4 electronic databases:Medline (1946-present), CINAHL Plus(1937-present; EBSCO Information Ser-vice), Embase (1947-present, ElsevierLife Science Solutions), and CochraneLibrary (1960-present, John Wiley &Sons Ltd). The searches were limited tothe English language and humanstudies, if possible, with the databases.The terms enamel, acid, etch, etching,conditioning, pretreatment were usedin combination for searching (Table I).The final search was run on November8, 2012. Duplicates were verified withsoftware (Endnote X4; Thomson Reu-ters) first. Because of the differentimport styles of the electronic data-bases, the software did not identify allthe duplications automatically. Thus, amanual verification was carried out tofind the duplications.
After discarding the duplicates, 2stages of screening were performed toevaluate the included publications. Inthe first stage, the titles and abstracts ofthe remaining articles were screenedindependently by the authors (J.J.Z. andA.T.H.T.), who determined whether thearticles were relevant to the purposes ofthis review. The focus of this review wasto provide a comprehensive summary ofthe existing protocols of various enamelacid-etching techniques for clinicalapplication. All studies that investigatedan enamel pretreatment method(s)clinically on normal human permanentteeth and clearly stated the acid-etchingtechnique were included. Disagreementsamong the authors (J.J.Z. and A.T.H.T.)were resolved by discussion to reachconsensus. In the second stage of
try
screening, laboratory studies and liter-ature reviews were excluded. The fulltexts of included articles were retrievedand sorted manually for additionalrelevant publications from their refer-ence lists. Finally, clinical evidence fromall included studies was tabulated.
RESULTS
Initially, 4543 publications (Fig. 1)were retrieved from the search of elec-tronic databases. Among them, 2285duplicates were identifies by the soft-ware (EndNote X4; Thompson Reuters)and manual check. After adjusting forduplicates, 2258 publications werescreened by their titles and abstracts.The exclusion criteria of the 2 screeningstages are in Table II. In the first stage,1805 publications were excluded ac-cording to the exclusion criteria (Fig. 1).The remaining 453 articles were sortedinto 4 categories: clinical trials (35publications), laboratory studies (365publications), combined in vitro andin vivo studies (4 publications), and re-views (49 publications). In the secondscreening stage, 365 laboratory articlesand 49 reviews were excluded. Subse-quently, the full texts of 39 clinical arti-cles were obtained. Among them, 1clinical pilot study and 3 laboratory ar-ticles whose titles resembled clinical ar-ticles were further excluded. Oneadditional publication was identifiedfrom the reference lists of includedarticles. Finally, 36 clinical articleswere included. All publications weretabulated according to the clinicalapplications of enamel adhesion: or-thodontic stainless-steel brackets orbands bonding (10 publications15-24)
Zhu et al
ScreeningStage
1
ScreeningStage
2
Medline (Pubmed): 2036 (results coverage: 1955 to 2011)CINAHL Plus (EBSCO): 125 (results coverage: 1995 to 2010)EMBASE (OvidSP): 1910 (results coverage: 1965 to 2011)Cochrane Library: 472 (results coverage: 1972 to 2011)
References retrieved by electronic search strategies: 4543
Included articles without duplication: 2258
Duplicates: 2285
Duplications with Medline database: 2284
Duplications with EMBASE database: 1
CINAHL Plus (EBSCO): 112EMBASE (OvidSP): 1771Cochrane Library: 401
Cochrane Library: 1
Included articles eligible for full-text screen based on reviewing their titles and abstracts: 453
• Clinical articles: 35• Laboratory articles: 365• Both in vitro and in vivo articles: 4• Review: 49
Excluded articles basedon exclusion criteria: 414
• Laboratory articles: 365• Review: 49
Included clinical articles eligible for full-text screening: 39
Excluded full-text articles: 4
• laboratory studies: 3• pilot study: 1
Additional article identified from
reference lists of included articles: 1
Clinical articles included in this review: 36
Excluded articles based on titles and abstracts: 1805
• Not relevant to topic: 347Bacterial adhesion: 15Dental education: 1Dentifrice and prophylaxis paste: 13Enamel loss: 24Enamel surface contamination: 43Enamel erosion/ re- or de-mineralization phenomenon: 53Endodontic studies (root caries, pulp reaction, etc.): 42Health care of workers: 1Histology of enamel: 45Measurement methods: 18Orthodontic studies (impacted teeth treatment, etc.): 6Periodontal studies (enamel matrix derivative, etc.): 33Prosthodontic studies (esthetic restoration, etc.): 20Rinse/drying methods in dental bonding procedure: 5Statistics: 1Storage methods of experimental specimens: 7Systemic diseases: 8Traumatic dental injury: 12
• Not written in English: 2• Conference reports: 9• Letters: 4• Research protocols: 1• Short communication: 4• Fluoride studies: 181• Antibacterial agents: 22• Specimens: 300
Animal teeth: 15Abnormal enamel of human permanent teeth: 56Biological apatite or enamel powder: 7Bleached teeth: 36Deciduous teeth: 44Dentine: 133Enamel and dentine (not reported separately): 9
• Other surface treatment methods: 72Air abrasion: 13Crystal growth methods: 13Ion-etching: 1Mechanical preparation (bur-cutting): 9Laser: 32Ozone gas: 4
• Bonding systems: 425Bonding primer: 3Bonding resin adhesives and bonding technique: 362Cements: 60
• Adhesive materials based bonding: 436Amalgam: 13Ceramic and metal materials: 143Restorative resin composite materials (fillings): 192Vanish and sealants: 88
• Acid etching method not specified: 2
1 Flow diagram of study selection.
- 2014 3
Zhu et al
Table II. Screening methods
Exclusion criteria for 2 screening stages 1 and 2
Screening stage 1
1. Not directly relevant to the topic of enamel acid etching
2. Not written in English
3. Conference reports
4. Letters
5. Research protocols
6. Short communications
7. Fluoride studies
8. Antibacterial studies
9. Specimens other than normal enamel of human permanent teeth
10. Other surface treatment methods
11. Evaluation and/or review of bonding systems
12. Evaluation and/or review of adhesive materials
13. Acid-etching method not specified
Screening stage 2
1. Laboratory studies
2. Review
3. Pilot study
4 Volume - Issue -
(Table III), composite resin restorations(16publications25-40) (Table IV), pit andfissure sealing (4 publications12-14,41)(Table V), and acid etching followed byno bonding procedure (6 publica-tions42-47) (Table VI). To review thedevelopment of human enamel acid-etching protocols, studies and their in-formation were tabulated in chronolog-ical order; the years of publicationranged from 1974 to 2012.
One included publication consistedof 2 parts of a clinical study design.15
Thus, in total, 37 clinical studies wererepresented in the 36 included articles.From the included studies, informationwas extracted as follows: characteristicsof specimen, sample size, and studydesign; protocols of acid etching(including acid types, concentrations ofacid, and etching time) and bondingsystems used; and assessment methods,length of follow-up, and outcomes.All included studies were classifiedinto 2 types: randomized controlledtrials (RCT) and case series. Thirtystudies claimed to be RCTs, of which 7studies applied split-mouth design. Thesplit-mouth design is considered as a
The Journal of Prosthetic Dentis
special type of RCT at the field level, inwhich different treatments are assignedrandomly to sites. However, the limi-tations of this experimental design areobvious. If a disease is not symmetri-cally distributed over the intraindividualexamination sites, then the split-mouthdesign loses its efficiency.48 Further-more, the carry-across oral environmentand the planning of professional sta-tistic analysis also should be consideredwhen designing a split-mouth experi-ment.49 Only after such factors are wellcontrolled can the split-mouth designbe regarded as an RCT. Not all thesplit-mouth studies in this systematicreview properly evaluated these factors,thus they could not be classified asRCTs.
In the other 23 RCTs, which usedparallel-group design, none had asample size that exceeded 90 partici-pants. Because at least 2 groups wereset in each parallel-group designedstudy, no group sample exceeded 45participants. Although sufficient sam-ple size should be estimated by properstatistical power analyses, as a rule ofthumb, a group sample of fewer than
try
50 participants is likely to cause thesmall-study effect, which decreasesthe precision of unknown parameterestimation.50 Therefore, none of theremaining 23 studies were properlydesigned as RCTs. Because all theincluded clinical trials failed to qualifyas RCTs, meta-analysis was inappro-priate, and, subsequently, only asystematic review was possible. Theextracted information was summarizedin the following aspects.
Seventeen studies (Tables IV and VI)used subsurface enamel, such as cariousclass II, III, V cavities, and noncariouscervical abrasive cavities, for acid etching,whereas the other 20 studies (Tables III,V, VI) used intact enamel surfaces. Thetooth type of experimental teeth alsovaried. The sample sizes of both etchedenamel surfaces and enrolled patientsare given in Tables III to VI. Threestudies26,34,36 did not report the popu-lation of participants. Among the other34 studies, only 1 case-series studyinvolved more than 100 participants.15
Acid pretreatment methods weresorted by acid type, acid concentration,and etching time. Each study appliedat least 1 kind of acid-etching proce-dure. Altogether, 57 different acidpretreatment methods were used. Theprotocols of acid etching are summa-rized in Table VII. Phosphoric acidwas commonly investigated. However,oxalic acid and maleic acid with orwithout itaconic acid were occasionallystudied. The predominant concentra-tion of phosphoric acid used was 30% to40%. Studies on higher or lower con-centrations were not common. Phos-phoric acid, 30% to 40%, was used, withetching times that ranged from 15 to120 seconds. Other concentrations ofphosphoric acid were not investigated interms of etching time. In total, 16 resinadhesive systems and 2 kinds of cementswere used in 27 studies, which hadbonding procedures (Tables III and IV).Bonding systems were coded, and theirdetails are provided in the keys toTables III and IV. The follow-up periodvaried from immediately,43-45,47 to a fewminutes26,42 to 8 years33 after acidetching.
Zhu et al
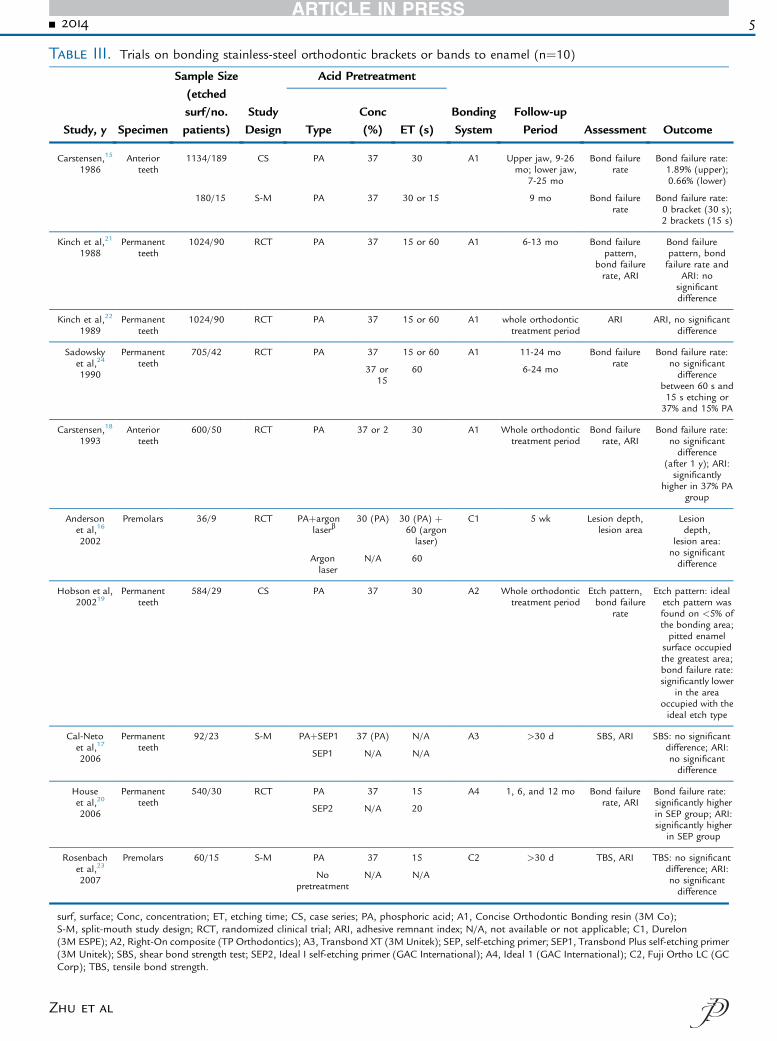
Table III. Trials on bonding stainless-steel orthodontic brackets or bands to enamel (n¼10)
Study, y Specimen
Sample Size(etchedsurf/no.patients)
StudyDesign
Acid Pretreatment
BondingSystem
Follow-upPeriod Assessment OutcomeType
Conc(%) ET (s)
Carstensen,15
1986Anterior
teeth1134/189 CS PA 37 30 A1 Upper jaw, 9-26
mo; lower jaw,7-25 mo
Bond failurerate
Bond failure rate:1.89% (upper);0.66% (lower)
180/15 S-M PA 37 30 or 15 9 mo Bond failurerate
Bond failure rate:0 bracket (30 s);2 brackets (15 s)
Kinch et al,21
1988Permanent
teeth1024/90 RCT PA 37 15 or 60 A1 6-13 mo Bond failure
pattern,bond failurerate, ARI
Bond failurepattern, bondfailure rate and
ARI: nosignificantdifference
Kinch et al,22
1989Permanent
teeth1024/90 RCT PA 37 15 or 60 A1 whole orthodontic
treatment periodARI ARI, no significant
difference
Sadowskyet al,24
1990
Permanentteeth
705/42 RCT PA 37 15 or 60 A1 11-24 mo Bond failurerate
Bond failure rate:no significantdifference
between 60 s and15 s etching or37% and 15% PA
37 or15
60 6-24 mo
Carstensen,18
1993Anterior
teeth600/50 RCT PA 37 or 2 30 A1 Whole orthodontic
treatment periodBond failure
rate, ARIBond failure rate:
no significantdifference
(after 1 y); ARI:significantly
higher in 37% PAgroup
Andersonet al,16
2002
Premolars 36/9 RCT PAþargonlaserb
30 (PA) 30 (PA) þ60 (argonlaser)
C1 5 wk Lesion depth,lesion area
Lesiondepth,
lesion area:no significantdifferenceArgon
laserN/A 60
Hobson et al,200219
Permanentteeth
584/29 CS PA 37 30 A2 Whole orthodontictreatment period
Etch pattern,bond failure
rate
Etch pattern: idealetch pattern wasfound on <5% ofthe bonding area;pitted enamel
surface occupiedthe greatest area;bond failure rate:significantly lower
in the areaoccupied with theideal etch type
Cal-Netoet al,17
2006
Permanentteeth
92/23 S-M PAþSEP1 37 (PA) N/A A3 >30 d SBS, ARI SBS: no significantdifference; ARI:no significantdifference
SEP1 N/A N/A
Houseet al,20
2006
Permanentteeth
540/30 RCT PA 37 15 A4 1, 6, and 12 mo Bond failurerate, ARI
Bond failure rate:significantly higherin SEP group; ARI:significantly higher
in SEP group
SEP2 N/A 20
Rosenbachet al,23
2007
Premolars 60/15 S-M PA 37 15 C2 >30 d TBS, ARI TBS: no significantdifference; ARI:no significantdifference
Nopretreatment
N/A N/A
surf, surface; Conc, concentration; ET, etching time; CS, case series; PA, phosphoric acid; A1, Concise Orthodontic Bonding resin (3M Co);S-M, split-mouth study design; RCT, randomized clinical trial; ARI, adhesive remnant index; N/A, not available or not applicable; C1, Durelon(3M ESPE); A2, Right-On composite (TP Orthodontics); A3, Transbond XT (3M Unitek); SEP, self-etching primer; SEP1, Transbond Plus self-etching primer(3M Unitek); SBS, shear bond strength test; SEP2, Ideal I self-etching primer (GAC International); A4, Ideal 1 (GAC International); C2, Fuji Ortho LC (GCCorp); TBS, tensile bond strength.
- 2014 5
Zhu et al
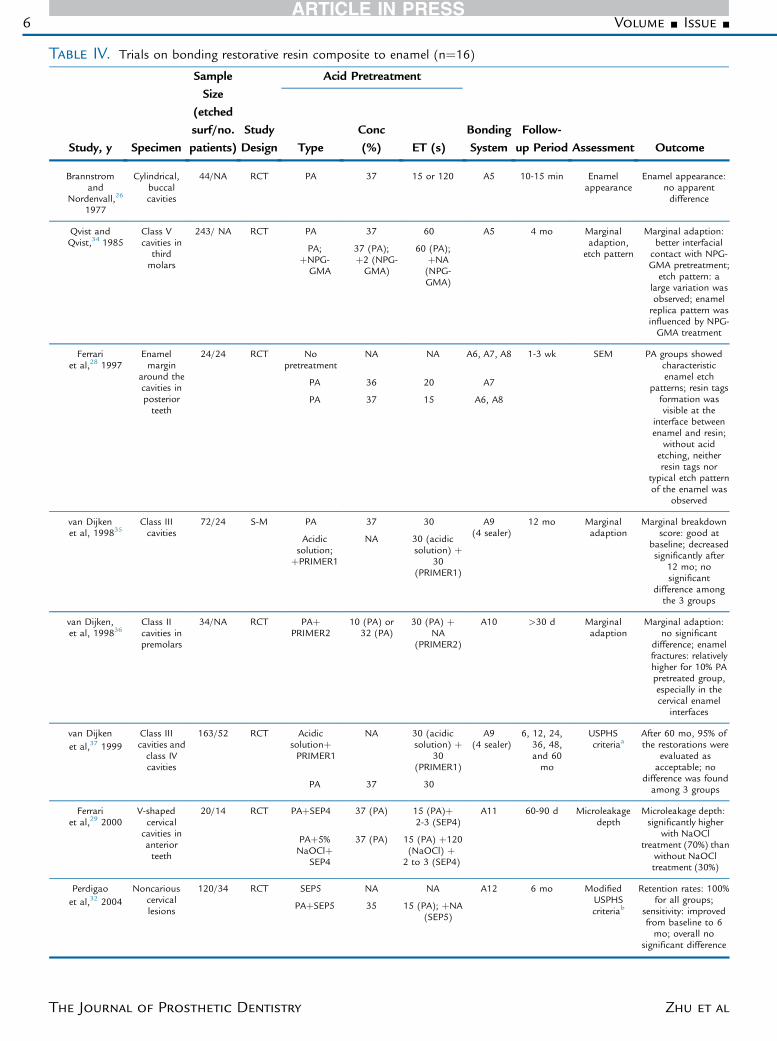
Table IV. Trials on bonding restorative resin composite to enamel (n¼16)
Study, y Specimen
SampleSize
(etchedsurf/no.patients)
StudyDesign
Acid Pretreatment
BondingSystem
Follow-up Period Assessment OutcomeType
Conc(%) ET (s)
Brannstromand
Nordenvall,26
1977
Cylindrical,buccalcavities
44/NA RCT PA 37 15 or 120 A5 10-15 min Enamelappearance
Enamel appearance:no apparentdifference
Qvist andQvist,34 1985
Class Vcavities in
thirdmolars
243/ NA RCT PA 37 60 A5 4 mo Marginaladaption,
etch pattern
Marginal adaption:better interfacial
contact with NPG-GMA pretreatment;etch pattern: a
large variation wasobserved; enamelreplica pattern wasinfluenced by NPG-GMA treatment
PA;þNPG-GMA
37 (PA);þ2 (NPG-GMA)
60 (PA);þNA(NPG-GMA)
Ferrariet al,28 1997
Enamelmargin
around thecavities inposteriorteeth
24/24 RCT Nopretreatment
NA NA A6, A7, A8 1-3 wk SEM PA groups showedcharacteristicenamel etch
patterns; resin tagsformation wasvisible at the
interface betweenenamel and resin;
without acidetching, neitherresin tags nor
typical etch patternof the enamel was
observed
PA 36 20 A7
PA 37 15 A6, A8
van Dijkenet al, 199835
Class IIIcavities
72/24 S-M PA 37 30 A9(4 sealer)
12 mo Marginaladaption
Marginal breakdownscore: good at
baseline; decreasedsignificantly after
12 mo; nosignificant
difference amongthe 3 groups
Acidicsolution;
þPRIMER1
NA 30 (acidicsolution) þ
30(PRIMER1)
van Dijken,et al, 199836
Class IIcavities inpremolars
34/NA RCT PAþPRIMER2
10 (PA) or32 (PA)
30 (PA) þNA
(PRIMER2)
A10 >30 d Marginaladaption
Marginal adaption:no significant
difference; enamelfractures: relativelyhigher for 10% PApretreated group,especially in thecervical enamel
interfaces
van Dijkenet al,37 1999
Class IIIcavities andclass IVcavities
163/52 RCT AcidicsolutionþPRIMER1
NA 30 (acidicsolution) þ
30(PRIMER1)
A9(4 sealer)
6, 12, 24,36, 48,and 60mo
USPHScriteriaa
After 60 mo, 95% ofthe restorations were
evaluated asacceptable; no
difference was foundamong 3 groupsPA 37 30
Ferrariet al,29 2000
V-shapedcervical
cavities inanteriorteeth
20/14 RCT PAþSEP4 37 (PA) 15 (PA)þ2-3 (SEP4)
A11 60-90 d Microleakagedepth
Microleakage depth:significantly higher
with NaOCltreatment (70%) than
without NaOCltreatment (30%)
PAþ5%NaOClþ
SEP4
37 (PA) 15 (PA) þ120(NaOCl) þ
2 to 3 (SEP4)
Perdigaoet al,32 2004
Noncariouscervicallesions
120/34 RCT SEP5 NA NA A12 6 mo ModifiedUSPHScriteriab
Retention rates: 100%for all groups;
sensitivity: improvedfrom baseline to 6mo; overall no
significant difference
PAþSEP5 35 15 (PA); þNA(SEP5)
6 Volume - Issue -
The Journal of Prosthetic Dentistry Zhu et al
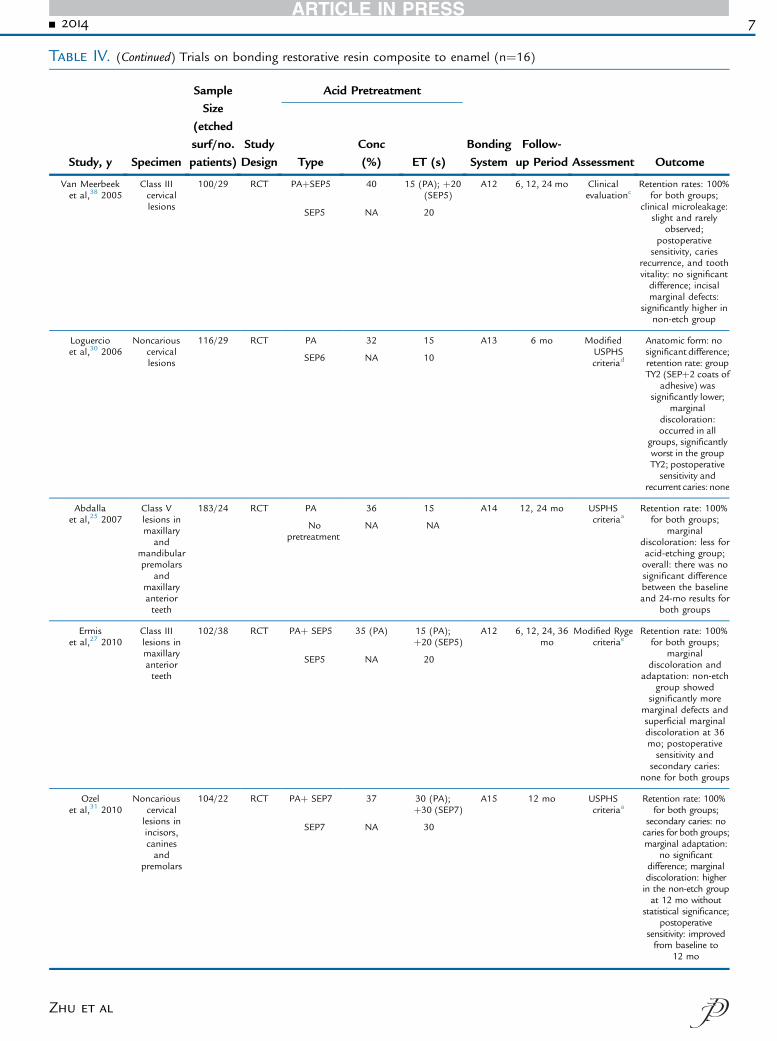
Table IV. (Continued) Trials on bonding restorative resin composite to enamel (n¼16)
Study, y Specimen
SampleSize
(etchedsurf/no.patients)
StudyDesign
Acid Pretreatment
BondingSystem
Follow-up Period Assessment OutcomeType
Conc(%) ET (s)
Van Meerbeeket al,38 2005
Class IIIcervicallesions
100/29 RCT PAþSEP5 40 15 (PA); þ20(SEP5)
A12 6, 12, 24 mo Clinicalevaluationc
Retention rates: 100%for both groups;
clinical microleakage:slight and rarely
observed;postoperative
sensitivity, cariesrecurrence, and toothvitality: no significantdifference; incisalmarginal defects:
significantly higher innon-etch group
SEP5 NA 20
Loguercioet al,30 2006
Noncariouscervicallesions
116/29 RCT PA 32 15 A13 6 mo ModifiedUSPHScriteriad
Anatomic form: nosignificant difference;retention rate: groupTY2 (SEPþ2 coats of
adhesive) wassignificantly lower;
marginaldiscoloration:occurred in all
groups, significantlyworst in the groupTY2; postoperativesensitivity and
recurrent caries: none
SEP6 NA 10
Abdallaet al,25 2007
Class Vlesions inmaxillary
andmandibularpremolars
andmaxillaryanteriorteeth
183/24 RCT PA 36 15 A14 12, 24 mo USPHScriteriaa
Retention rate: 100%for both groups;
marginaldiscoloration: less foracid-etching group;overall: there was nosignificant differencebetween the baselineand 24-mo results for
both groups
Nopretreatment
NA NA
Ermiset al,27 2010
Class IIIlesions inmaxillaryanteriorteeth
102/38 RCT PAþ SEP5 35 (PA) 15 (PA);þ20 (SEP5)
A12 6, 12, 24, 36mo
Modified Rygecriteriae
Retention rate: 100%for both groups;
marginaldiscoloration and
adaptation: non-etchgroup showed
significantly moremarginal defects andsuperficial marginaldiscoloration at 36mo; postoperativesensitivity and
secondary caries:none for both groups
SEP5 NA 20
Ozelet al,31 2010
Noncariouscervicallesions inincisors,caninesand
premolars
104/22 RCT PAþ SEP7 37 30 (PA);þ30 (SEP7)
A15 12 mo USPHScriteriaa
Retention rate: 100%for both groups;
secondary caries: nocaries for both groups;marginal adaptation:
no significantdifference; marginaldiscoloration: higherin the non-etch groupat 12 mo without
statistical significance;postoperative
sensitivity: improvedfrom baseline to
12 mo
SEP7 NA 30
- 2014 7
Zhu et al
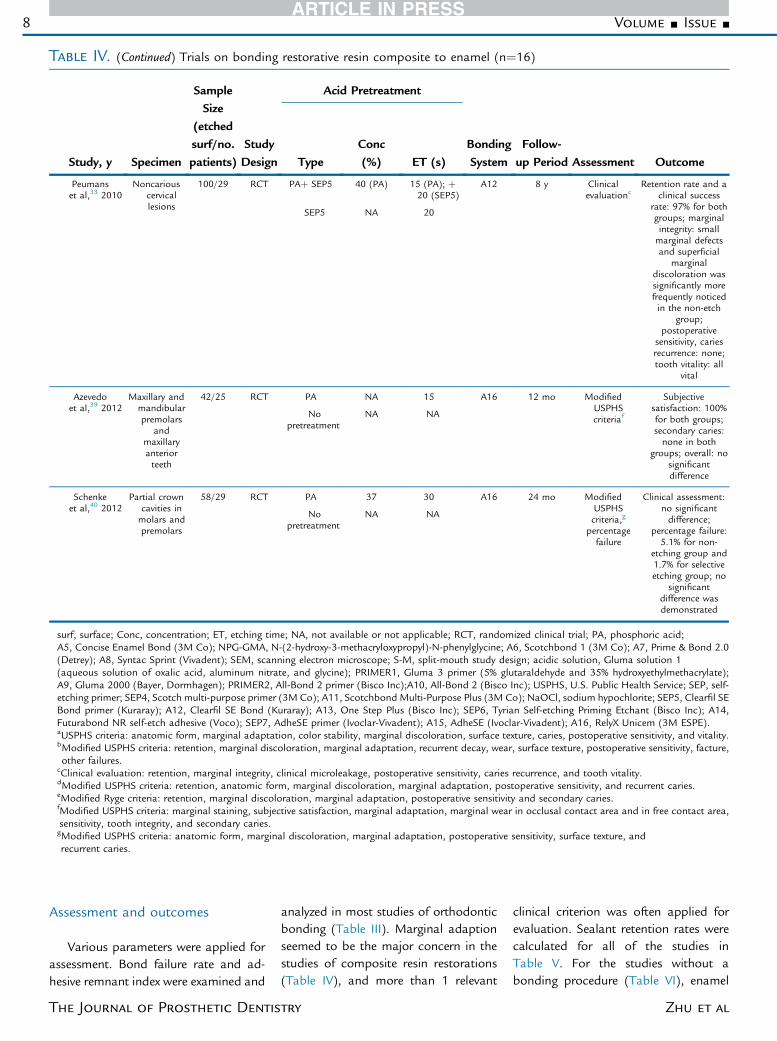
Table IV. (Continued) Trials on bonding restorative resin composite to enamel (n¼16)
Study, y Specimen
SampleSize
(etchedsurf/no.patients)
StudyDesign
Acid Pretreatment
BondingSystem
Follow-up Period Assessment OutcomeType
Conc(%) ET (s)
Peumanset al,33 2010
Noncariouscervicallesions
100/29 RCT PAþ SEP5 40 (PA) 15 (PA); þ20 (SEP5)
A12 8 y Clinicalevaluationc
Retention rate and aclinical success
rate: 97% for bothgroups; marginalintegrity: smallmarginal defectsand superficial
marginaldiscoloration wassignificantly morefrequently noticedin the non-etch
group;postoperative
sensitivity, cariesrecurrence: none;tooth vitality: all
vital
SEP5 NA 20
Azevedoet al,39 2012
Maxillary andmandibularpremolars
andmaxillaryanteriorteeth
42/25 RCT PA NA 15 A16 12 mo ModifiedUSPHScriteriaf
Subjectivesatisfaction: 100%for both groups;secondary caries:none in both
groups; overall: nosignificantdifference
Nopretreatment
NA NA
Schenkeet al,40 2012
Partial crowncavities inmolars andpremolars
58/29 RCT PA 37 30 A16 24 mo ModifiedUSPHScriteria,g
percentagefailure
Clinical assessment:no significantdifference;
percentage failure:5.1% for non-
etching group and1.7% for selectiveetching group; no
significantdifference wasdemonstrated
Nopretreatment
NA NA
surf, surface; Conc, concentration; ET, etching time; NA, not available or not applicable; RCT, randomized clinical trial; PA, phosphoric acid;A5, Concise Enamel Bond (3M Co); NPG-GMA, N-(2-hydroxy-3-methacryloxypropyl)-N-phenylglycine; A6, Scotchbond 1 (3M Co); A7, Prime & Bond 2.0(Detrey); A8, Syntac Sprint (Vivadent); SEM, scanning electron microscope; S-M, split-mouth study design; acidic solution, Gluma solution 1(aqueous solution of oxalic acid, aluminum nitrate, and glycine); PRIMER1, Gluma 3 primer (5% glutaraldehyde and 35% hydroxyethylmethacrylate);A9, Gluma 2000 (Bayer, Dormhagen); PRIMER2, All-Bond 2 primer (Bisco Inc);A10, All-Bond 2 (Bisco Inc); USPHS, U.S. Public Health Service; SEP, self-etching primer; SEP4, Scotch multi-purpose primer (3M Co); A11, Scotchbond Multi-Purpose Plus (3M Co); NaOCl, sodium hypochlorite; SEP5, Clearfil SEBond primer (Kuraray); A12, Clearfil SE Bond (Kuraray); A13, One Step Plus (Bisco Inc); SEP6, Tyrian Self-etching Priming Etchant (Bisco Inc); A14,Futurabond NR self-etch adhesive (Voco); SEP7, AdheSE primer (Ivoclar-Vivadent); A15, AdheSE (Ivoclar-Vivadent); A16, RelyX Unicem (3M ESPE).aUSPHS criteria: anatomic form, marginal adaptation, color stability, marginal discoloration, surface texture, caries, postoperative sensitivity, and vitality.bModified USPHS criteria: retention, marginal discoloration, marginal adaptation, recurrent decay, wear, surface texture, postoperative sensitivity, facture,other failures.
cClinical evaluation: retention, marginal integrity, clinical microleakage, postoperative sensitivity, caries recurrence, and tooth vitality.dModified USPHS criteria: retention, anatomic form, marginal discoloration, marginal adaptation, postoperative sensitivity, and recurrent caries.eModified Ryge criteria: retention, marginal discoloration, marginal adaptation, postoperative sensitivity and secondary caries.fModified USPHS criteria: marginal staining, subjective satisfaction, marginal adaptation, marginal wear in occlusal contact area and in free contact area,sensitivity, tooth integrity, and secondary caries.gModified USPHS criteria: anatomic form, marginal discoloration, marginal adaptation, postoperative sensitivity, surface texture, andrecurrent caries.
8 Volume - Issue -
Assessment and outcomes
Various parameters were applied forassessment. Bond failure rate and ad-hesive remnant index were examined and
The Journal of Prosthetic Dentis
analyzed in most studies of orthodonticbonding (Table III). Marginal adaptionseemed to be the major concern in thestudies of composite resin restorations(Table IV), and more than 1 relevant
try
clinical criterion was often applied forevaluation. Sealant retention rates werecalculated for all of the studies inTable V. For the studies without abonding procedure (Table VI), enamel
Zhu et al
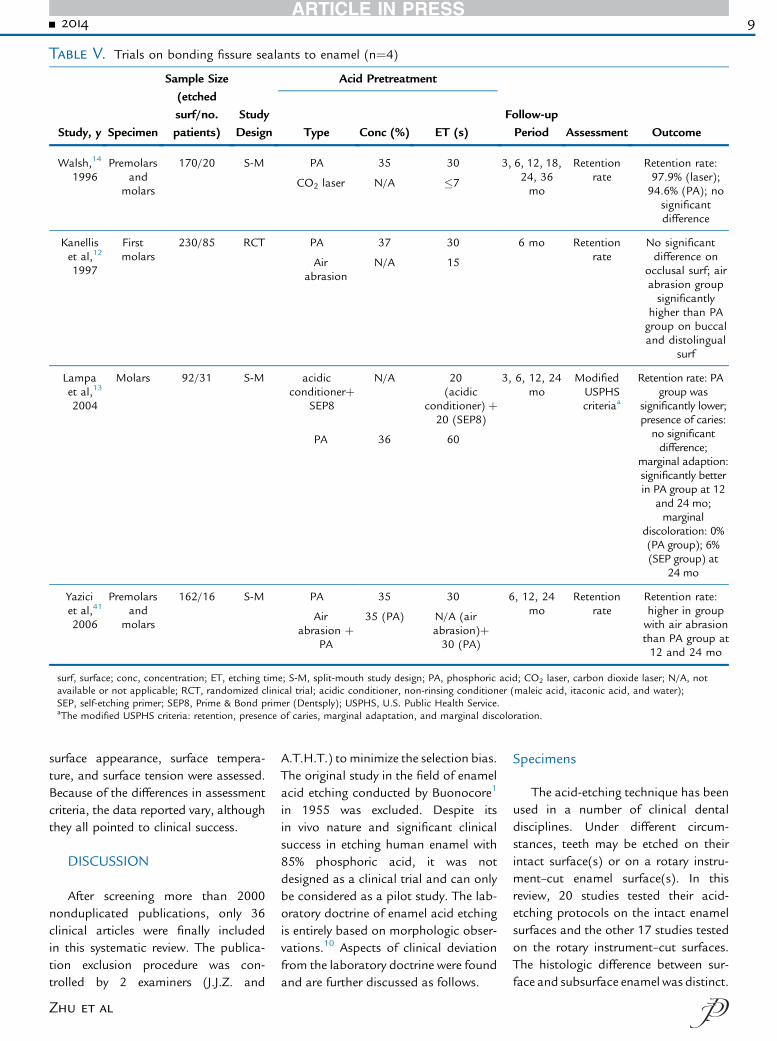
Table V. Trials on bonding fissure sealants to enamel (n¼4)
Study, y Specimen
Sample Size(etchedsurf/no.patients)
StudyDesign
Acid Pretreatment
Follow-upPeriod Assessment OutcomeType Conc (%) ET (s)
Walsh,14
1996Premolars
andmolars
170/20 S-M PA 35 30 3, 6, 12, 18,24, 36mo
Retentionrate
Retention rate:97.9% (laser);94.6% (PA); no
significantdifference
CO2 laser N/A �7
Kanelliset al,12
1997
Firstmolars
230/85 RCT PA 37 30 6 mo Retentionrate
No significantdifference on
occlusal surf; airabrasion groupsignificantly
higher than PAgroup on buccaland distolingual
surf
Airabrasion
N/A 15
Lampaet al,13
2004
Molars 92/31 S-M acidicconditionerþ
SEP8
N/A 20(acidic
conditioner) þ20 (SEP8)
3, 6, 12, 24mo
ModifiedUSPHScriteriaa
Retention rate: PAgroup was
significantly lower;presence of caries:no significantdifference;
marginal adaption:significantly betterin PA group at 12
and 24 mo;marginal
discoloration: 0%(PA group); 6%(SEP group) at
24 mo
PA 36 60
Yaziciet al,41
2006
Premolarsand
molars
162/16 S-M PA 35 30 6, 12, 24mo
Retentionrate
Retention rate:higher in groupwith air abrasionthan PA group at12 and 24 mo
Airabrasion þ
PA
35 (PA) N/A (airabrasion)þ30 (PA)
surf, surface; conc, concentration; ET, etching time; S-M, split-mouth study design; PA, phosphoric acid; CO2 laser, carbon dioxide laser; N/A, notavailable or not applicable; RCT, randomized clinical trial; acidic conditioner, non-rinsing conditioner (maleic acid, itaconic acid, and water);SEP, self-etching primer; SEP8, Prime & Bond primer (Dentsply); USPHS, U.S. Public Health Service.aThe modified USPHS criteria: retention, presence of caries, marginal adaptation, and marginal discoloration.
- 2014 9
surface appearance, surface tempera-ture, and surface tension were assessed.Because of the differences in assessmentcriteria, the data reported vary, althoughthey all pointed to clinical success.
DISCUSSION
After screening more than 2000nonduplicated publications, only 36clinical articles were finally includedin this systematic review. The publica-tion exclusion procedure was con-trolled by 2 examiners (J.J.Z. and
Zhu et al
A.T.H.T.) to minimize the selection bias.The original study in the field of enamelacid etching conducted by Buonocore1
in 1955 was excluded. Despite itsin vivo nature and significant clinicalsuccess in etching human enamel with85% phosphoric acid, it was notdesigned as a clinical trial and can onlybe considered as a pilot study. The lab-oratory doctrine of enamel acid etchingis entirely based on morphologic obser-vations.10 Aspects of clinical deviationfrom the laboratory doctrine were foundand are further discussed as follows.
Specimens
The acid-etching technique has beenused in a number of clinical dentaldisciplines. Under different circum-stances, teeth may be etched on theirintact surface(s) or on a rotary instru-ment–cut enamel surface(s). In thisreview, 20 studies tested their acid-etching protocols on the intact enamelsurfaces and the other 17 studies testedon the rotary instrument–cut surfaces.The histologic difference between sur-face and subsurface enamel was distinct.
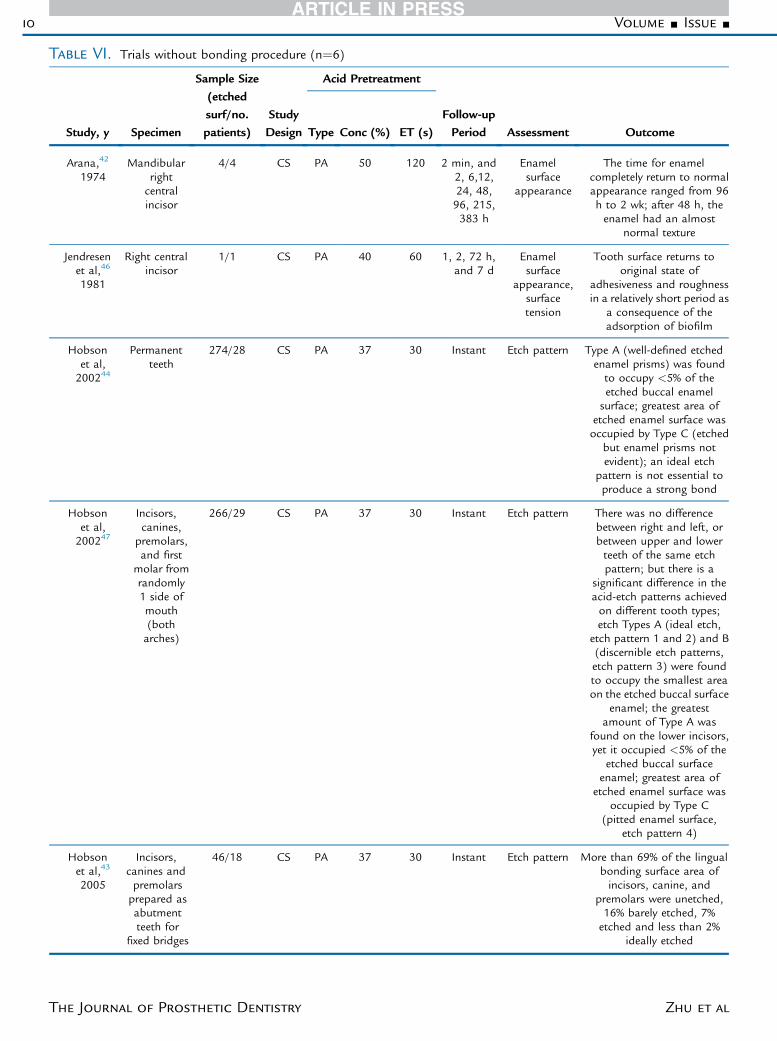
Table VI. Trials without bonding procedure (n¼6)
Study, y Specimen
Sample Size(etchedsurf/no.patients)
StudyDesign
Acid Pretreatment
Follow-upPeriod Assessment OutcomeType Conc (%) ET (s)
Arana,42
1974Mandibular
rightcentralincisor
4/4 CS PA 50 120 2 min, and2, 6,12,24, 48,96, 215,383 h
Enamelsurface
appearance
The time for enamelcompletely return to normalappearance ranged from 96h to 2 wk; after 48 h, theenamel had an almost
normal texture
Jendresenet al,46
1981
Right centralincisor
1/1 CS PA 40 60 1, 2, 72 h,and 7 d
Enamelsurface
appearance,surfacetension
Tooth surface returns tooriginal state of
adhesiveness and roughnessin a relatively short period as
a consequence of theadsorption of biofilm
Hobsonet al,200244
Permanentteeth
274/28 CS PA 37 30 Instant Etch pattern Type A (well-defined etchedenamel prisms) was foundto occupy <5% of theetched buccal enamelsurface; greatest area of
etched enamel surface wasoccupied by Type C (etched
but enamel prisms notevident); an ideal etch
pattern is not essential toproduce a strong bond
Hobsonet al,200247
Incisors,canines,
premolars,and first
molar fromrandomly1 side ofmouth(botharches)
266/29 CS PA 37 30 Instant Etch pattern There was no differencebetween right and left, orbetween upper and lowerteeth of the same etchpattern; but there is a
significant difference in theacid-etch patterns achievedon different tooth types;etch Types A (ideal etch,
etch pattern 1 and 2) and B(discernible etch patterns,etch pattern 3) were foundto occupy the smallest areaon the etched buccal surface
enamel; the greatestamount of Type A was
found on the lower incisors,yet it occupied <5% of the
etched buccal surfaceenamel; greatest area of
etched enamel surface wasoccupied by Type C
(pitted enamel surface,etch pattern 4)
Hobsonet al,43
2005
Incisors,canines andpremolarsprepared asabutmentteeth for
fixed bridges
46/18 CS PA 37 30 Instant Etch pattern More than 69% of the lingualbonding surface area ofincisors, canine, and
premolars were unetched,16% barely etched, 7%etched and less than 2%
ideally etched
10 Volume - Issue -
The Journal of Prosthetic Dentistry Zhu et al
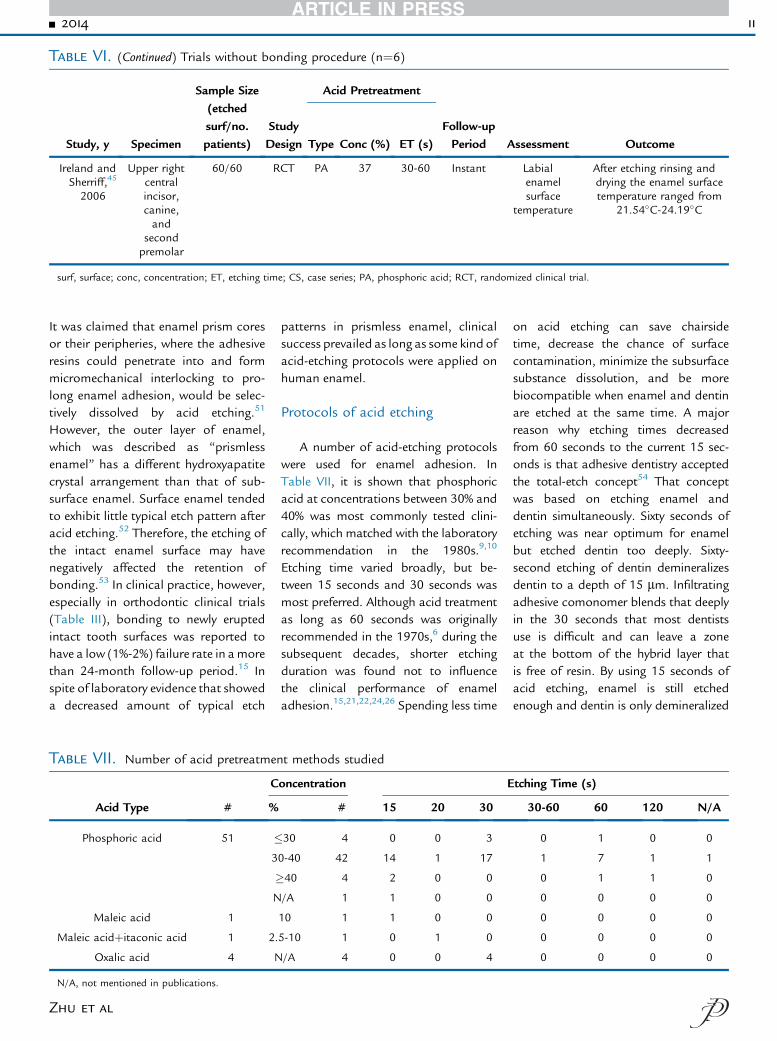
Table VI. (Continued) Trials without bonding procedure (n¼6)
Study, y Specimen
Sample Size(etchedsurf/no.patients)
StudyDesign
Acid Pretreatment
Follow-upPeriod Assessment OutcomeType Conc (%) ET (s)
Ireland andSherriff,45
2006
Upper rightcentralincisor,canine,and
secondpremolar
60/60 RCT PA 37 30-60 Instant Labialenamelsurface
temperature
After etching rinsing anddrying the enamel surfacetemperature ranged from
21.54�C-24.19�C
surf, surface; conc, concentration; ET, etching time; CS, case series; PA, phosphoric acid; RCT, randomized clinical trial.
- 2014 11
It was claimed that enamel prism coresor their peripheries, where the adhesiveresins could penetrate into and formmicromechanical interlocking to pro-long enamel adhesion, would be selec-tively dissolved by acid etching.51
However, the outer layer of enamel,which was described as “prismlessenamel” has a different hydroxyapatitecrystal arrangement than that of sub-surface enamel. Surface enamel tendedto exhibit little typical etch pattern afteracid etching.52 Therefore, the etching ofthe intact enamel surface may havenegatively affected the retention ofbonding.53 In clinical practice, however,especially in orthodontic clinical trials(Table III), bonding to newly eruptedintact tooth surfaces was reported tohave a low (1%-2%) failure rate in amorethan 24-month follow-up period.15 Inspite of laboratory evidence that showeda decreased amount of typical etch
Table VII. Number of acid pretreatmen
Acid Type #
C
%
Phosphoric acid 51 �3
�N
Maleic acid 1
Maleic acidþitaconic acid 1 2.
Oxalic acid 4 N
N/A, not mentioned in publications.
Zhu et al
patterns in prismless enamel, clinicalsuccess prevailed as long as some kind ofacid-etching protocols were applied onhuman enamel.
Protocols of acid etching
A number of acid-etching protocolswere used for enamel adhesion. InTable VII, it is shown that phosphoricacid at concentrations between 30% and40% was most commonly tested clini-cally, which matched with the laboratoryrecommendation in the 1980s.9,10
Etching time varied broadly, but be-tween 15 seconds and 30 seconds wasmost preferred. Although acid treatmentas long as 60 seconds was originallyrecommended in the 1970s,6 during thesubsequent decades, shorter etchingduration was found not to influencethe clinical performance of enameladhesion.15,21,22,24,26 Spending less time
t methods studied
oncentration E
# 15 20 30
30 4 0 0 3
0-40 42 14 1 17
40 4 2 0 0
/A 1 1 0 0
10 1 1 0 0
5-10 1 0 1 0
/A 4 0 0 4
on acid etching can save chairsidetime, decrease the chance of surfacecontamination, minimize the subsurfacesubstance dissolution, and be morebiocompatible when enamel and dentinare etched at the same time. A majorreason why etching times decreasedfrom 60 seconds to the current 15 sec-onds is that adhesive dentistry acceptedthe total-etch concept54 That conceptwas based on etching enamel anddentin simultaneously. Sixty seconds ofetching was near optimum for enamelbut etched dentin too deeply. Sixty-second etching of dentin demineralizesdentin to a depth of 15 mm. Infiltratingadhesive comonomer blends that deeplyin the 30 seconds that most dentistsuse is difficult and can leave a zoneat the bottom of the hybrid layer thatis free of resin. By using 15 seconds ofacid etching, enamel is still etchedenough and dentin is only demineralized
tching Time (s)
30-60 60 120 N/A
0 1 0 0
1 7 1 1
0 1 1 0
0 0 0 0
0 0 0 0
0 0 0 0
0 0 0 0
12 Volume - Issue -
5 to 8 mm, which makes it easier to infil-trate. With all these clinical advantages,an etching time of 15 or 30 secondshasbecome theprevailingmethodof acidetching in recent years (Tables III to VI).Besides the most commonly used phos-phoric acid-etching protocols, a lowerconcentration of phosphoric acid18,24
or weaker acids combined with adhesiveprimer35,37 have also been studied clini-cally and have produced satisfactoryclinical results. Self-etching tech-nique17,31,32 and laser etching12,16 alsoproduced comparable clinical bonding.
Bonding systems
The publication years of includedarticles ranged from 1974 to 2012,which covered the major period of thedevelopment of enamel bonding tech-niques. Generations of resin bondingsystems can be traced to these studies.The first generation of resin bondingmaterials was based on the “etch-rinse-bond” technique in 3 separate steps.Self-etch techniques without a separateetching step then were developed andseemed more convenient for clinicaluse. In addition to bonding resin sys-tems, 2 types of cements were used inthe included studies for orthodonticbonding. The enamel adhesion mecha-nisms of composite resins and cementsare different. For resin adhesives, the“tag-like” penetration of liquid resinsinto acid-etched enamel is thought toprovide the major mechanical retentionforce between bonding materials andenamel. This micromechanical inter-locking mechanism has been estab-lished for more than 40 years.51
However, for cements, the mechanismof enamel adhesion may be a result ofthe chemical reaction between carbox-ylic groups in cement materials andphosphate-calcium ions in the enamelsubstrate.55 The interaction forms anionic bond.55 Therefore, the assump-tion that there is no need to etch theenamel surface before using cementsfor adhesion is logical. However,research evidence has shown that theenhancement of cement adhesion byacid etching is inconsistent.23,56
The Journal of Prosthetic Dentis
Follow-up period
The length of follow-up depends onthe experimental purpose and methods.In clinical studies, long-term follow-upis desirable because it can give realisticinformation about the success of thetreatment. In this systematic review, thelongest follow-up period was 8 years.Other clinical trials followed up partic-ipants for months to years except forsome studies that assessed the surfaceappearance or surface temperature af-ter quite a short term. Because the acid-etched enamel surface is dynamic innature and may recover after the expo-sure to the oral environment, thefollow-up period cannot be too long.Hence, the short-term or even instantassessments in these studies fulfilled theobjectives.
Assessment
Because of the differences in clinicalapplication, assessments and thus thedata collected varied. Some contro-versies inevitably exist. Direct compari-son of the clinical performance of aself-etch bonding technique and anetch-rinse-bond technique20,25,30 orevaluation of the effect of an additionalacid-etching step in a self-etch bond-ing system may not be scientificallyadequate.17,27,31,32,38
In spite of the variations mentionedabove, enamel adhesion in clinical ap-plications was consistently successful,which may be explained on the basis ofthe results from 5 recent morphologicstudies19,34,43,44,47 included in this re-view, which showed a large variationin the morphology of enamel surfacesafter acid etching. These studies re-ported that “ideal etch patterns” wererarely produced. Generalized rough-ened enamel surfaces occupied themajority of the etched enamel area. Inthe 1970s, the characteristic etch pat-terns produced by acid on an enamelsurface were classified into 3 types,2 inwhich Type 1 and Type 2 etch patternswere called “the ideal etch patterns”and were reported to occur predomi-nantly in vitro.2,57 These patterns were
try
considered to play a critical role in themicromechanical interlocking mecha-nism of enamel adhesion. However, theclinical studies in this review showedcontradictory results that cast doubt onthe concept of the micromechanicalinterlocking mechanism of enameladhesion.
On the basis of existing clinicalevidence, some consensus in outcomescan be summarized. Shorter acid-etching time, a lower concentrationof phosphoric acid, and other etchingmethods may all achieve a clinicalbonding effect comparable with 30%to 50% phosphoric acid etching for60 seconds. The “ideal etch pattern”only occupied a small proportion ofthe etched enamel area. The clinicallysuccessful acid-etching protocols onenamel do not seem to require pre-dominantly enamel prism cores or per-iprismatic etching but may involveetching of the total enamel surface todepths that are not easily identified byscanning electron microscopy studies.
CONCLUSIONS
1. Only 36 clinical publications wereselected from 2258 nonduplicatedpublications about human enamel acidetching. These publications providedlevels of evidence of efficacy from caseseries to controlled clinical trials ofacid-etching protocols in lastingenamel adhesion.
2. Clinically accepted acid-etchingprotocols differed from the laboratoryrecommendation of 30% to 50% phos-phoric acid for 60 seconds.
3. Weaker acids, self-etching prim-ers, laser, and phosphoric acid of lowerconcentration all achieve clinical re-sults comparable with the laboratory-generated doctrine of 30% to 50%phosphoric acid for 60 seconds.
4. An etching time of less than 60seconds (30 seconds, 15 seconds, oreven shorter) can produce similar clin-ical results for enamel adhesion.
5. Clinical morphologic studiesshowed that the “ideal etch pattern”for micromechanical interlocking only
Zhu et al
- 2014 13
occupied a small proportion of theetched enamel area.
6. Successful clinical protocols ofenamel acid etching varied from theideal laboratory protocol to maximizethe Type 1 or 2 enamel etch patterns.The maximization of the “ideal etchpattern” as advocated in the laboratorydoctrine may not be clinically relevant.
REFERENCES
1. Buonocore MG. A simple method ofincreasing the adhesion of acrylic fillingmaterials to enamel surfaces. J Dent Res1955;34:849-53.
2. Silverstone LM, Saxton CA, Dogon IL,Fejerskov O. Variation in the pattern of acidetching of human dental enamel examined byscanning electron microscopy. Caries Res1975;9:373-87.
3. Poole DF, Johnson NW. The effects ofdifferent demineralizing agents on humanenamel surfaces studied by scanning electronmicroscopy. Arch Oral Biol 1967;12:1621-34.
4. Mulholland RD, DeShazer DO. The effect ofacidic pretreatment solutions on the directbonding of orthodontic brackets to enamel.Angle Orthod 1968;38:236-43.
5. Gwinnett AJ. Histologic changes in humanenamel following treatment with acidic ad-hesive conditioning agents. Arch Oral Biol1971;16:731-8.
6. Silverstone LM. Fissure sealants. Laboratorystudies. Caries Res 1974;8:2-26.
7. Chow LC, Brown WE. Phosphoric acid con-ditioning of teeth for pit and fissure sealants.J Dent Res 1973;52:1158.
8. Silverstone LM. The effect of phosphoric acidon human deciduous enamel surfacesin vitro. J Int Assoc Dent Child 1976;7:11-5.
9. Buonocore MG. Retrospections on bonding.Dent Clin North Am 1981;25:241-55.
10. Silverstone LM. Fissure sealants: the enamel-resin interface. J Public Health Dent 1983;43:205-15.
11. Dennison JB, Craig RG. Characterization ofenamel surfaces prepared with commercialand experimental etchants. J Am Dent Assoc1978;97:799-805.
12. Kanellis MJ, Warren JJ, Levy SM. Comparisonof air abrasion versus acid etch sealanttechniques: six-month retention. Pediatr Dent1997;19:258-61.
13. Lampa E, Brechter A, van Dijken JW. Effect ofa nonrinse conditioner on the durability of apolyacid-modified resin composite fissuresealant. J Dent Child 2004;71:152-7.
14. Walsh LJ. Split-mouth study of sealantretention with carbon dioxide laser versusacid etch conditioning. Aust Dent J 1996;41:124-7.
15. Carstensen W. Clinical results after directbonding of brackets using shorter etchingtimes. Am J Orthod Dentofacial Orthop1986;89:70-2.
Zhu et al
16. Anderson AM, Kao E, Gladwin M, Benli O,Ngan P. The effects of argon laser irradiationon enamel decalcification: an in vivo study.Am J Orthod Dentofacial Orthop 2002;122:251-9.
17. Cal-Neto JP, Miguel JA, Zanella E. Effect of aself-etching primer on shear bond strength ofadhesive precoated brackets in vivo. AngleOrthod 2006;76:127-31.
18. Carstensen W. Clinical effects of reduction ofacid concentration on direct bonding ofbrackets. Angle Orthod 1993;63:221-4.
19. Hobson RS, McCabe JF, Rugg-Gunn AJ. Therelationship between acid-etch patterns andbond survival in vivo. Am J Orthod Dento-facial Orthop 2002;121:502-9.
20. House K, Ireland AJ, Sherriff M. An investi-gation into the use of a single componentself-etching primer adhesive system for or-thodontic bonding: a randomized controlledclinical trial. J Orthod 2006;33:38-44.
21. Kinch AP, Taylor H, Warltier R, Oliver RG,Newcombe RG. A clinical trial comparing thefailure rates of directly bonded brackets usingetch times of 15 or 60 seconds. Am J OrthodDentofacial Orthop 1988;94:476-83.
22. Kinch AP, Taylor H, Warltier R, Oliver RG,Newcombe RG. A clinical study of amount ofadhesive remaining on enamel afterdebonding, comparing etch times of 15 and60 seconds. Am J Orthod Dentofacial Orthop1989;95:415-21.
23. Rosenbach G, Cal-Neto JP, Oliveira SR,Chevitarese O, Almeida MA. Effect of enameletching on tensile bond strength of bracketsbonded in vivo with a resin-reinforced glassionomer cement. AngleOrthod2007;77:113-6.
24. Sadowsky PL, Retief DH, Cox PR, Hernandez-Orsini R, Rape WG, Bradley EL. Effects ofetchant concentration and duration on theretention of orthodontic brackets: an in vivostudy. Am J Orthod Dentofacial Orthop1990;98:417-21.
25. Abdalla AI, Garcia-Godoy F. Clinical perfor-mance of a self-etch adhesive in Class V res-torations made with and without acidetching. J Dent 2007;35:558-63.
26. Brannstrom M, Nordenvall KJ. The effect ofacid etching on enamel, dentin, and the innersurface of the resin restoration: a scanningelectron microscopic investigation. J DentRes 1977;56:917-23.
27. Ermis RB, Temel UB, Cellik EU, Kam O.Clinical performance of a two-step self-etchadhesive with additional enamel etching inClass III cavities. Oper Dent 2010;35:147-55.
28. Ferrari M, Goracci G, Garcia-Godoy F.Bonding mechanism of three “one-bottle”systems to conditioned and unconditionedenamel and dentin. Am J Dent 1997;10:224-30.
29. Ferrari M, Mason PN, Vichi A, Davidson CL.Role of hybridization on marginal leakageand bond strength. Am J Dent 2000;13:329-36.
30. Loguercio AD, Costenaro A, Silveira AP,Ribeiro NR, Rossi TR, Reis A. A six-monthclinical study of a self-etching and an etch-and-rinse adhesive applied as recommendedand after doubling the number of adhesivecoats. J Adhes Dent 2006;8:255-61.
31. Ozel E, Say EC, Yurdaguven H, Soyman M.One-year clinical evaluation of a two-stepself-etch adhesive with and withoutadditional enamel etching technique incervical lesions. Aust Dent J 2010;55:156-61.
32. Perdigao J, Anauate-Netto C, Carmo AR,Lewgoy HR, Cordeiro HJ, Dutra-Correa M,et al. Influence of acid etching and enamelbeveling on the 6-month clinical performanceof a self-etch dentin adhesive. CompendContin Educ Dent 2004;25:33-44.
33. Peumans M, De Munck J, Van Landuyt KL,Poitevin A, Lambrechts P, Van Meerbeek B.Eight-year clinical evaluation of a 2-step self-etch adhesive with and without selectiveenamel etching. Dent Mater 2010;26:1176-84.
34. Qvist V, Qvist J. Replica patterns on com-posite restorations performed in vivo withdifferent acid-etch restorative procedures.Scand J Dent Res 1985;93:360-70.
35. van Dijken JW, Horstedt P. The effect ofpretreatment with an oxalic acid solution onmarginal adaptation to enamel in vivo.J Prosthet Dent 1998;80:75-80.
36. van Dijken JW, Horstedt P, Waern R.Directed polymerization shrinkage versus ahorizontal incremental filling technique:interfacial adaptation in vivo in Class II cav-ities. Am J Dent 1998;11:165-72.
37. van Dijken JW, Olofsson AL, Holm C. Fiveyear evaluation of class III composite resinrestorations in cavities pre-treated with anoxalic- or a phosphoric acid conditioner.J Oral Rehabil 1999;26:364-71.
38. Van Meerbeek B, Kanumilli P, De Munck J,Van Landuyt K, Lambrechts P, Peumans M.A randomized controlled study evaluating theeffectiveness of a two-step self-etch adhesivewith and without selective phosphoric-acidetching of enamel. Dent Mater 2005;21:375-83.
39. Azevedo CG, De Goes MF, Ambrosano GM,Chan DC. 1-Year clinical study of indirectresin composite restorations luted with aself-adhesive resin cement: effect of enameletching. Braz Dent J 2012;23:97-103.
40. Schenke F, Federlin M, Hiller KA, Moder D,Schmalz G. Controlled, prospective, ran-domized, clinical evaluation of partialceramic crowns inserted with RelyX Unicemwith or without selective enamel etching.Results after 2 years. Clin Oral Investig2012;16:451-61.
41. Yazici AR, Kiremitci A, Celik C, Ozgunaltay G,Dayangac B. A two-year clinical evaluation ofpit and fissure sealants placed with andwithout air abrasion pretreatment in teen-agers. J Am Dent Assoc 2006;137:1401-5.
42. Arana EM. Clinical observations of enamelafter acid-etch procedure. J Am Dent Assoc1974;89:1102-6.
43. Hobson RS, Crotty T, Thomason JM,Jepson NJ. A quantitative study of enamel acidetch patterns on surfaces used for retention ofresin-bonded fixed prostheses. Eur J Prostho-dont Restor Dent 2005;13:123-8.
44. Hobson RS, McCabe JF. Relationship betweenenamel etch characteristics and resin-enamelbond strength. Br Dent J 2002;192:463-8.

14 Volume - Issue -
45. Ireland AJ, Sherriff M. An investigation intothe use of an anaerobic adhesive with twocommercially available orthodontic brackets.Dent Mater 2006;22:112-8.
46. Jendresen MD, Glantz PO, Baier RE, Eick JD.Microtopography and clinical adhesivenessof an acid etched tooth surface. An in-vivostudy. Acta Odontol Scand 1981;39:47-53.
47. Hobson RS, Rugg-Gunn AJ, Booth TA. Acid-etch patterns on the buccal surface of humanpermanent teeth. Arch Oral Biol 2002;47:407-12.
48. Hujoel PP, Loesche WJ. Efficiency of split-mouth designs. J Clin Periodontol 1990;17:722-8.
49. Lesaffre E, Philstrom B, Needleman I,Worthington H. The design and analysis ofsplit-mouth studies: what statisticians andclinicians should know. Stat Med 2009;28:3470-82.
50. Richy F, Ethgen O, Bruyere O, Deceulaer F,Reginster J. From sample size to effect-size:small study effect investigation. Int J Epi-demiol 2004;1:1-8.
The Journal of Prosthetic Dentis
51. Gwinnett AJ, Matsui A. A study of enameladhesives. The physical relationship betweenenamel and adhesive. Arch Oral Biol1967;12:1615-20.
52. Gwinnett AJ. Human prismless enamel andits influence on sealant penetration. ArchOral Biol 1973;18:441-4.
53. Sheykholeslam Z, Buonocore MG. Bondingof resins to phosphoric acid-etched enamelsurfaces of permanent and deciduous teeth.J Dent Res 1972;51:1572-6.
54. Inokoshi S, Iwaku M, Fusayama T. Pulpalresponse to a new adhesive restorative resin.J Dent Res 1982;61:1014-9.
55. Yoshida Y, Van Meerbeek B, Nakayama Y,Snauwaert J, Hellemans L, Lambrechts P,et al. Evidence of chemical bonding atbiomaterial-hard tissue interfaces. J Dent Res2000;79:709-14.
56. Markovic D, Petrovic B, Peric T, Miletic I,Andjelkovic S. The impact of fissure depthand enamel conditioning protocols on glass-ionomer and resin-based fissure sealantpenetration. J Adhes Dent 2011;13:171-8.
try
57. Tyler JE. A scanning electron microscope studyof factors influencing etch patterns of humanenamel. Arch Oral Biol 1976;21:765-9.
Corresponding author:Dr Alexander T. H. TangFaculty of DentistryThe University of Hong Kong34 Hospital RoadHONG KONG SARE-mail: [email protected]
AcknowledgmentThe authors thank Mr Shadow Yeung, Faculty ofDentistry, the University of Hong Kong for histechnical support.
Copyright ª 2014 by the Editorial Council forThe Journal of Prosthetic Dentistry.
Zhu et al