Embed Size (px)
Citation preview
Results of Randomized Trial of a New H1N1 LAIV Strain in US Children
Raburn Mallory, MD Senior Director Clinical DevelopmentMedImmune/AstraZeneca
February 21, 2018
Improved LAIV strain selection identified a new H1N1 strain that is more immunogenic in children• LAIV is not recommended in the US as H1N1 vaccine strains used in 2013-2014 and 2015-2016 had
reduced effectiveness
• A broad-based scientific investigation determined that H1N1 LAIV strains used in those seasons replicate less well compared to older more effective LAIV strains
• Assays measuring replicative fitness were incorporated into strain selection for 2017-2018 and a new H1N1 strain (A/Slovenia) selected
• A clinical trial was conducted in US children to determine if new A/Slovenia strain was more immunogenic compared to previous A/Bolivia strain used in 2015-2016
• In the study, the new A/Slovenia H1N1 strain induced antibody responses that were significantly higher than those seen with the A/Bolivia strain Immune responses were similar to those seen with a highly effective pre-pandemic LAIV H1N1 strain
• Clinical study results validate improved strain selection process
• New strain selection process applied to all future LAIV strains and data reviewed by FDA/EMA annually
2 LAIV = Live attenuated influenza vaccine
Pediatric shedding and immunogenicity study design
Days 1-27 Days 28-56
Dose 1200 subjects 2 to < 4 years randomized Baseline immunogenicity assessed
Dose 2Immunogenicity Assessed
Day 56Immunogenicity Assessed
Shedding: Days 2, 3, 4, 5 and 7
Shedding: Days 30, 32 and 34
LAIV3 = Trivalent live attenuated influenza vaccine; LAIV4 = Quadrivalent live attenuated influenza vaccine
Arm 1: LAIV3 2015-2016 (A/Bolivia) Arm 2: LAIV4 2015-2016 (A/Bolivia) Arm 3: LAIV4 2017-2018 (A/Slovenia)

Vaccine type/subtype Arm 1: LAIV3 2015-2016
Arm 2: LAIV4 2015-2016
Arm 3:LAIV4 2017-2018
A/H1N1 A/Bolivia A/Bolivia A/Slovenia
A/H3N2 A/Switzerland A/Switzerland A/New Caledonia/14
B/Yamagata lineage B/Phuket B/Phuket B/Phuket
B/Victoria lineage -- B/Brisbane B/Brisbane
4
Vaccine strains by study arm
The two quadrivalent arms (Arms 2 and 3) represent the commercial vaccine that was distributed in those seasons
Primary endpoint:• The proportion of subjects with strain-specific HAI antibody seroconversion (≥ 4-fold increase)
through Days 28 and 56 Response rate for A/H1N1 strains in LAIV4 formulations was pre-specified for significance testing*
Secondary Endpoints: • Immunogenicity Neutralizing antibody seroconversion rates (≥ 4-fold increase from baseline) Nasal Immunoglobulin A (IgA) (≥ 2-fold increase from baseline; ≥ 4-fold shown) The proportion of subjects with any antibody response (≥ 4-fold increase in HAI antibodies,
neutralizing antibodies or IgA antibodies)
• Shedding of vaccine virus
• Safety
Study endpoints
5 HAI = Hemagglutination inhibition * Testing pre-specified in Statistical Analysis Plan for study
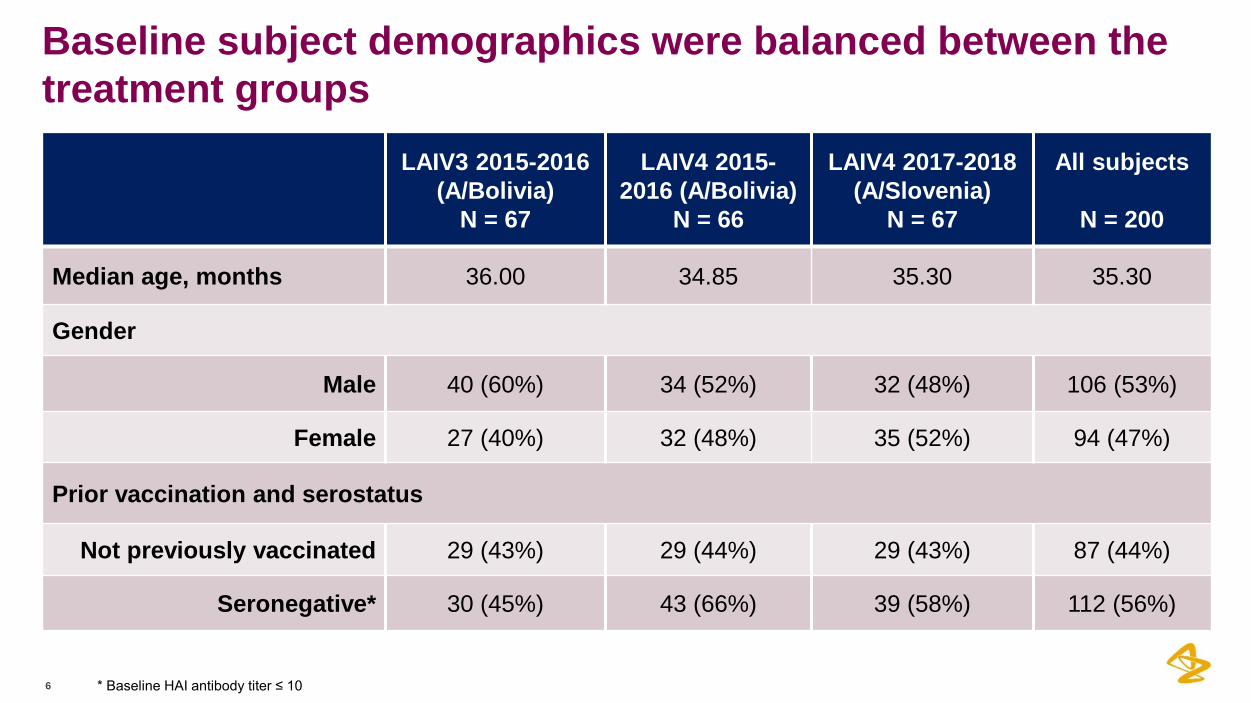
Baseline subject demographics were balanced between the treatment groups
6
LAIV3 2015-2016 (A/Bolivia)
N = 67
LAIV4 2015-2016 (A/Bolivia)
N = 66
LAIV4 2017-2018 (A/Slovenia)
N = 67
All subjects
N = 200
Median age, months 36.00 34.85 35.30 35.30
Gender
Male 40 (60%) 34 (52%) 32 (48%) 106 (53%)
Female 27 (40%) 32 (48%) 35 (52%) 94 (47%)
Prior vaccination and serostatus
Not previously vaccinated 29 (43%) 29 (44%) 29 (43%) 87 (44%)
Seronegative* 30 (45%) 43 (66%) 39 (58%) 112 (56%)
* Baseline HAI antibody titer ≤ 10
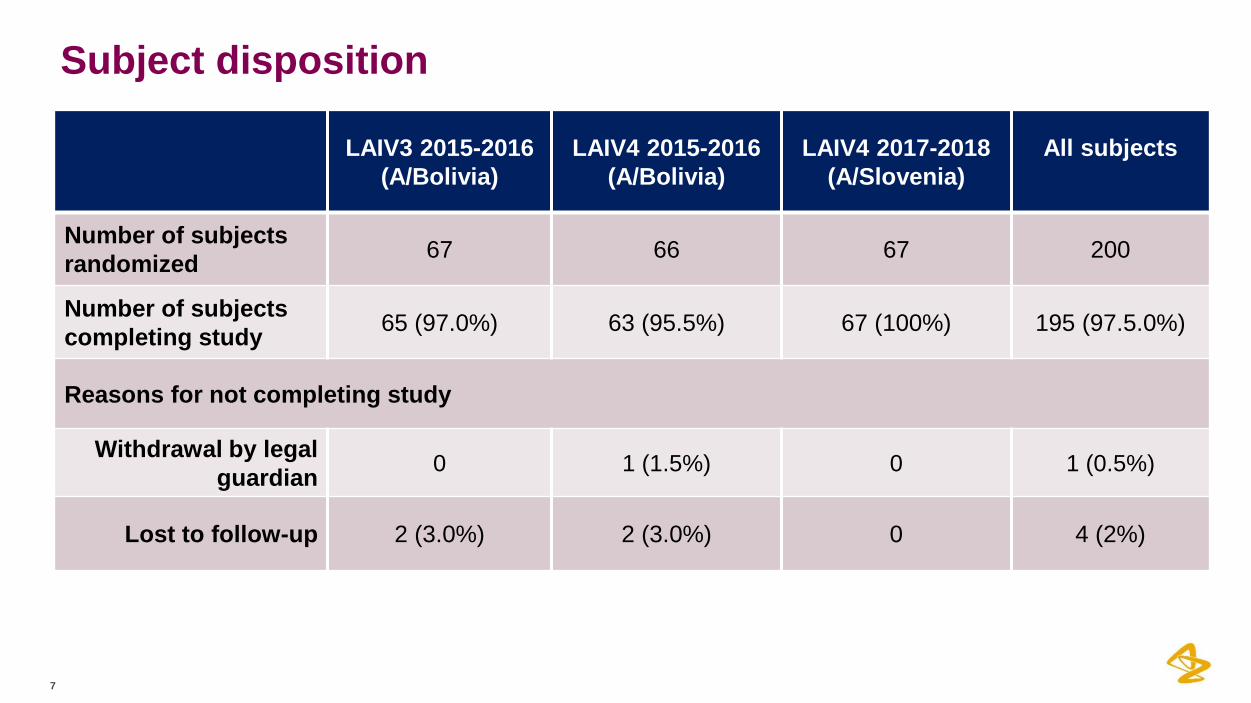
Subject disposition
7
LAIV3 2015-2016 (A/Bolivia)
LAIV4 2015-2016 (A/Bolivia)
LAIV4 2017-2018 (A/Slovenia)
All subjects
Number of subjects randomized 67 66 67 200
Number of subjects completing study 65 (97.0%) 63 (95.5%) 67 (100%) 195 (97.5.0%)
Reasons for not completing study
Withdrawal by legal guardian 0 1 (1.5%) 0 1 (0.5%)
Lost to follow-up 2 (3.0%) 2 (3.0%) 0 4 (2%)
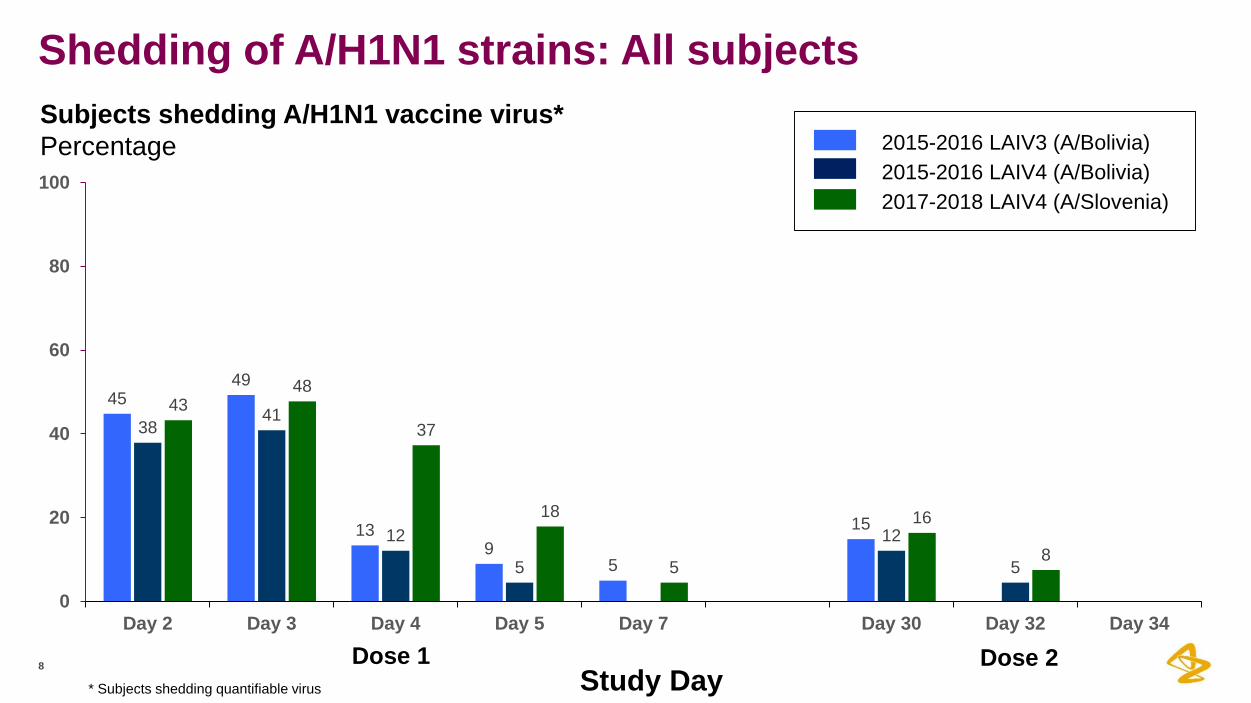
Shedding of A/H1N1 strains: All subjects
8
4549
139
5
15
3841
12
5
12
5
4348
37
18
5
16
8
0
20
40
60
80
100
Day 2 Day 3 Day 4 Day 5 Day 7 Day 30 Day 32 Day 34
Study Day
2015-2016 LAIV3 (A/Bolivia)2015-2016 LAIV4 (A/Bolivia)2017-2018 LAIV4 (A/Slovenia)
Dose 1 Dose 2
Subjects shedding A/H1N1 vaccine virus*Percentage
* Subjects shedding quantifiable virus
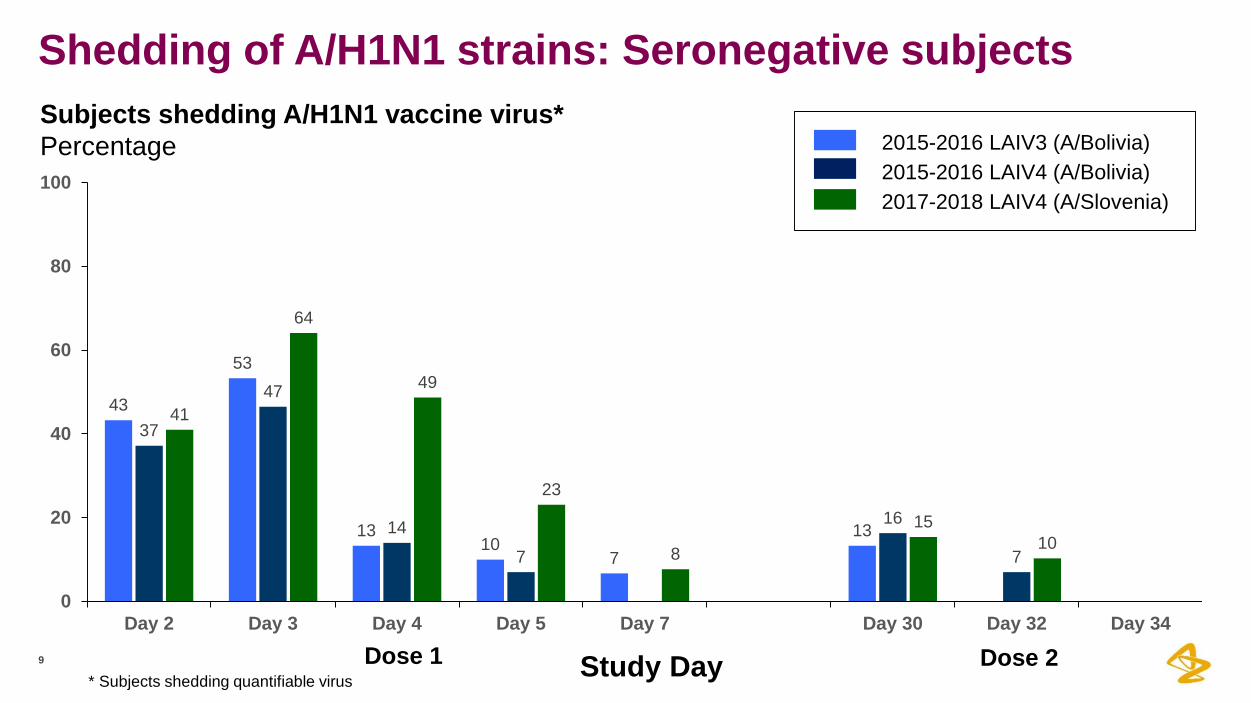
Shedding of A/H1N1 strains: Seronegative subjects
9
43
53
1310
713
37
47
147
16
7
41
64
49
23
8
1510
0
20
40
60
80
100
Day 2 Day 3 Day 4 Day 5 Day 7 Day 30 Day 32 Day 34
Study Day
2015-2016 LAIV3 (A/Bolivia)2015-2016 LAIV4 (A/Bolivia)2017-2018 LAIV4 (A/Slovenia)
Dose 1 Dose 2
Subjects shedding A/H1N1 vaccine virus*Percentage
* Subjects shedding quantifiable virus

Study Primary Endpoint: A/H1N1 HAI antibody seroconversion rates after Dose 1 and 2
10 Dose 1
p = 0.006*
1
0
10
20
30
40
50
60
70
80
90
00
10
19.2
5.4 8.6
23.4
38.9
0
10
20
30
40
50
60
70
80
90
100
All subjects Seronegative subjects
2015-2016 LAIV3 (A/Bolivia)2015-2016 LAIV4 (A/Bolivia)2017-2018 LAIV4 (A/Slovenia)
p = < 0.001*
Dose 2
23.7
48
12.518.4
45.2
75
All subjects Seronegative subjects
Subjects seroconvertingPercentage
* A/H1N1 HAI antibody responses in LAIV4 formulations for all subjects assessed for statistical significance per Statistical Analysis Plan
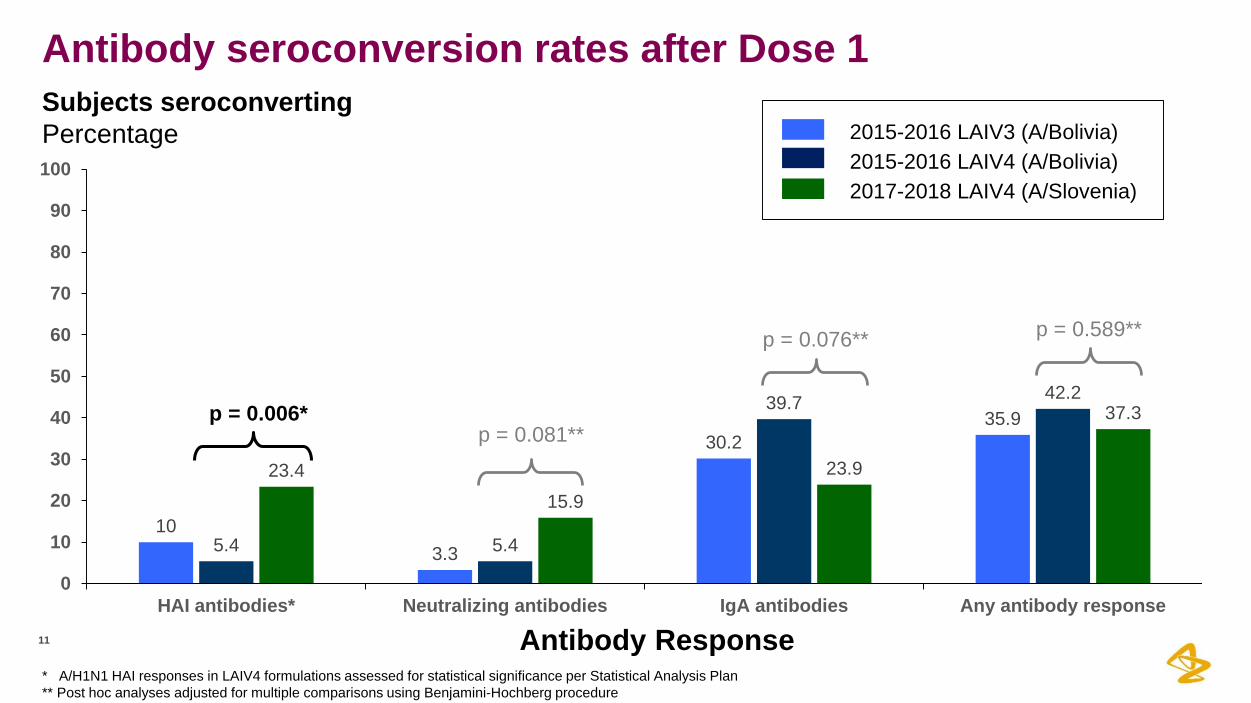
Antibody seroconversion rates after Dose 1
11
103.3
30.235.9
5.4 5.4
39.7 42.2
23.415.9
23.9
37.3
0
10
20
30
40
50
60
70
80
90
100
HAI antibodies* Neutralizing antibodies IgA antibodies Any antibody response
Antibody Response
2015-2016 LAIV3 (A/Bolivia)2015-2016 LAIV4 (A/Bolivia)2017-2018 LAIV4 (A/Slovenia)
p = 0.006*p = 0.081**
p = 0.076** p = 0.589**
Subjects seroconvertingPercentage
* A/H1N1 HAI responses in LAIV4 formulations assessed for statistical significance per Statistical Analysis Plan ** Post hoc analyses adjusted for multiple comparisons using Benjamini-Hochberg procedure
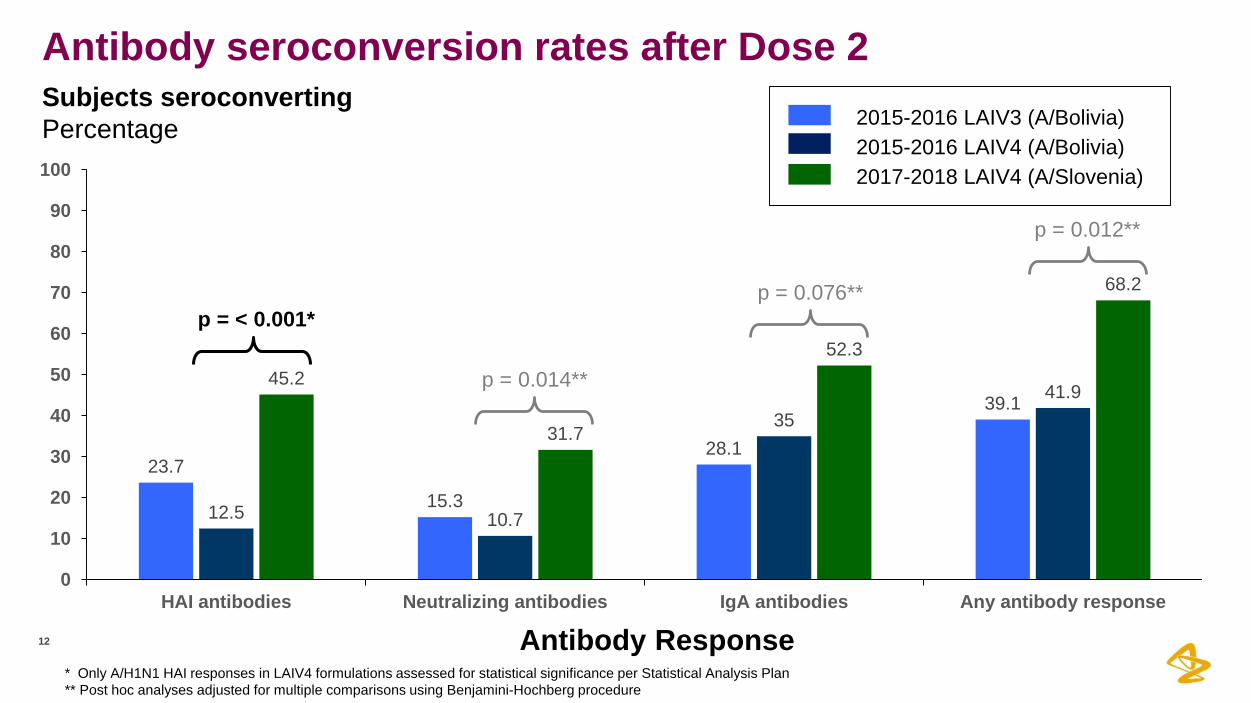
Antibody seroconversion rates after Dose 2
12
23.7
15.3
28.1
39.1
12.5 10.7
3541.9
45.2
31.7
52.3
68.2
0
10
20
30
40
50
60
70
80
90
100
HAI antibodies Neutralizing antibodies IgA antibodies Any antibody response
2015-2016 LAIV3 (A/Bolivia)2015-2016 LAIV4 (A/Bolivia)2017-2018 LAIV4 (A/Slovenia)
Antibody Response
p = < 0.001*
p = 0.014**
p = 0.076**
p = 0.012**
Subjects seroconvertingPercentage
* Only A/H1N1 HAI responses in LAIV4 formulations assessed for statistical significance per Statistical Analysis Plan** Post hoc analyses adjusted for multiple comparisons using Benjamini-Hochberg procedure
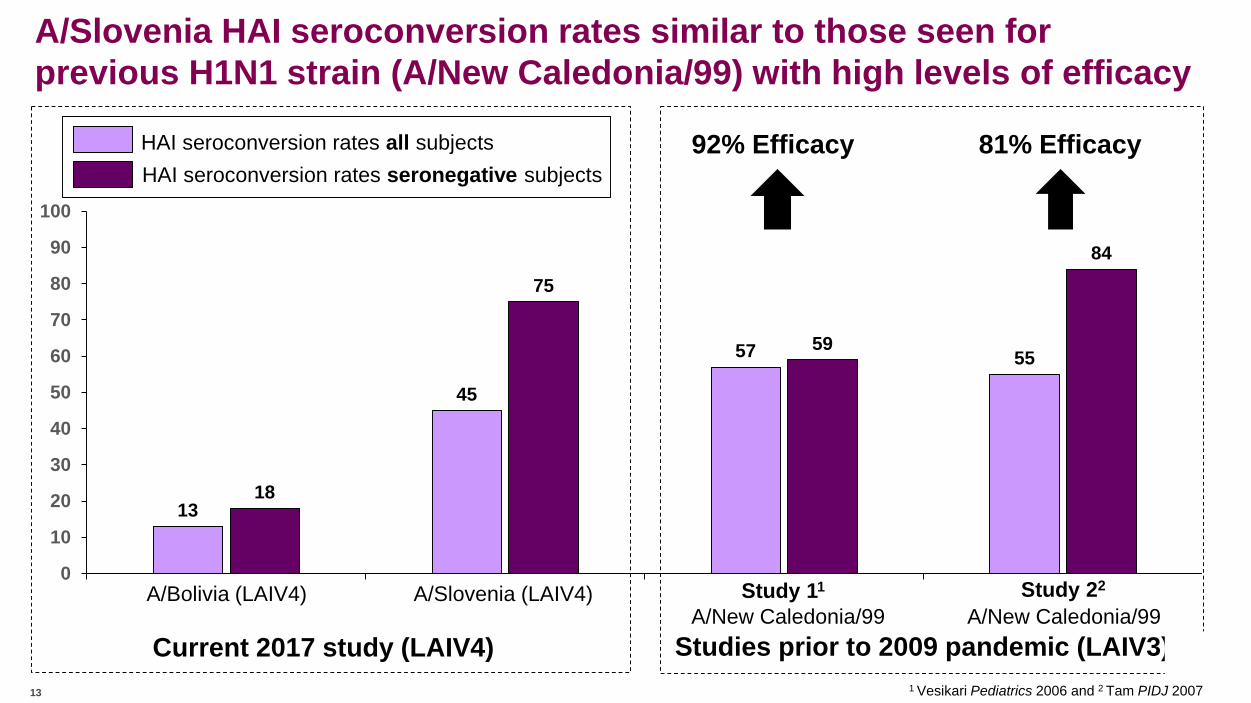
A/Slovenia HAI seroconversion rates similar to those seen for previous H1N1 strain (A/New Caledonia/99) with high levels of efficacy
13
45
18
75
0
10
20
30
40
50
60
70
80
90
100
HAI seroconversion rates all subjectsHAI seroconversion rates seronegative subjects
A/Bolivia (LAIV4) A/Slovenia (LAIV4)
Current 2017 study (LAIV4)
57 5559
84
A/New Caledonia/99Study 11
A/New Caledonia/99Study 22
92% Efficacy 81% Efficacy
Studies prior to 2009 pandemic (LAIV3)1 Vesikari Pediatrics 2006 and 2 Tam PIDJ 200713
A/H1N1 strain summary
14
•
•
•
The A/Slovenia strain was shed by a higher proportion of children from Day 4 through Day 7, after Dose 1 of the vaccine
The study met its primary endpoint: HAI seroconversion rates were significantly higher for the A/Slovenia strain than for the A/Bolivia strain
Similar results seen for neutralizing antibodies and for nasal IgA
A/Slovenia HAI seroconversion rates were similar to those seen in children the same age vaccinated with a highly efficacious pre-pandemic H1N1strain
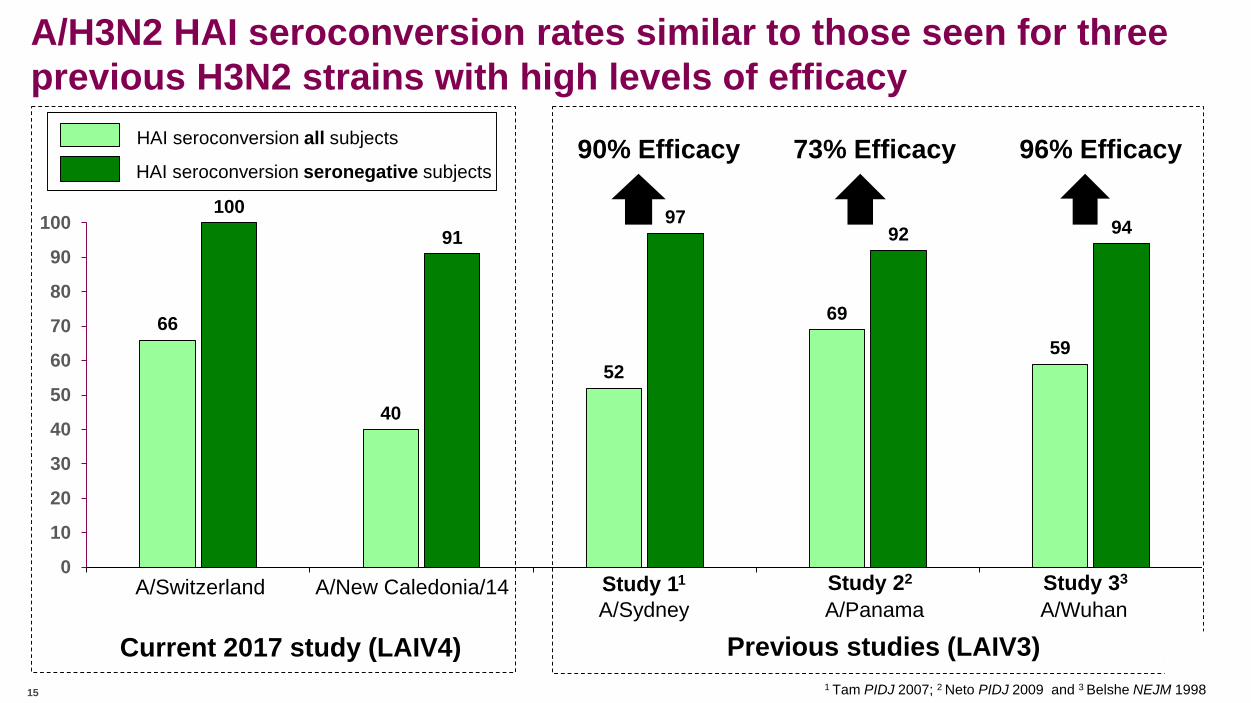
A/H3N2 HAI seroconversion rates similar to those seen for three previous H3N2 strains with high levels of efficacy
15
66
40
10091
0
10
20
30
40
50
60
70
80
90
100
A/New Caledonia/14A/Switzerland
Current 2017 study (LAIV4)
HAI seroconversion all subjects
HAI seroconversion seronegative subjects
52
69
59
9792 94
A/SydneyStudy 11
A/PanamaStudy 22
A/WuhanStudy 33
90% Efficacy 73% Efficacy 96% Efficacy
Previous studies (LAIV3)1 Tam PIDJ 2007; 2 Neto PIDJ 2009 and 3 Belshe NEJM 1998
Key changes made in the way LAIV strains are selected annually
16
•
Human nasal epithelial cell culture now used to assess the replicative fitness of new LAIV strainsPrevious strains were assessed for fitness in MDCK (dog kidney) cells and eggsFor post-pandemic H1N1 strains results were not predictive of human nasal cell replication
•
•
TCID50 assay added to quantify new LAIV strainsFFA measures infectivity of vaccine viruses through expression of antigen on the cell surface TCID50 measures spread of vaccine virus between cells following multiple rounds of replicationFor post-pandemic H1N1 strains TCID50 values were up to 3 logs lower than FFA resultsAs a result, post-pandemic H1N1 strains with reduced effectiveness may not have sustained intranasal replication to the level needed for optimal effectiveness
All future strains now only selected if they have high levels of replication in human nasal epithelial cells and when the FFA and TCID50 assays give similar results*
* TCID50 and FFA results to be submitted and reviewed by FDA and EMA as part of annual strain change process
Summary
• A broad-based scientific investigation determined that H1N1 LAIV strains used in 2013-2014 and 2015-2016 had reduced replicative fitness compared to older more effective vaccine strains
• New assays measuring how well strains replicate were incorporated into strain selection for 2017-2018 and a new H1N1 strain (A/Slovenia) was selected
• In a randomized trial in US children, the new A/Slovenia strain induced antibody responses that were significantly higher than those seen with the 2015-16 H1N1 strain Immune responses similar to those seen with a highly effective pre-pandemic LAIV H1N1 strain
• Clinical study results validate improved strain selection process
• New strain selection process applied to all future LAIV strains and data reviewed by FDA/EMA on an annual basis
• LAIV is an important vaccine option for providers, patients, and parents in the US and other countries where it continues to be recommended
17 LAIV = Live attenuated influenza vaccine
Thank you!
Safety data
19
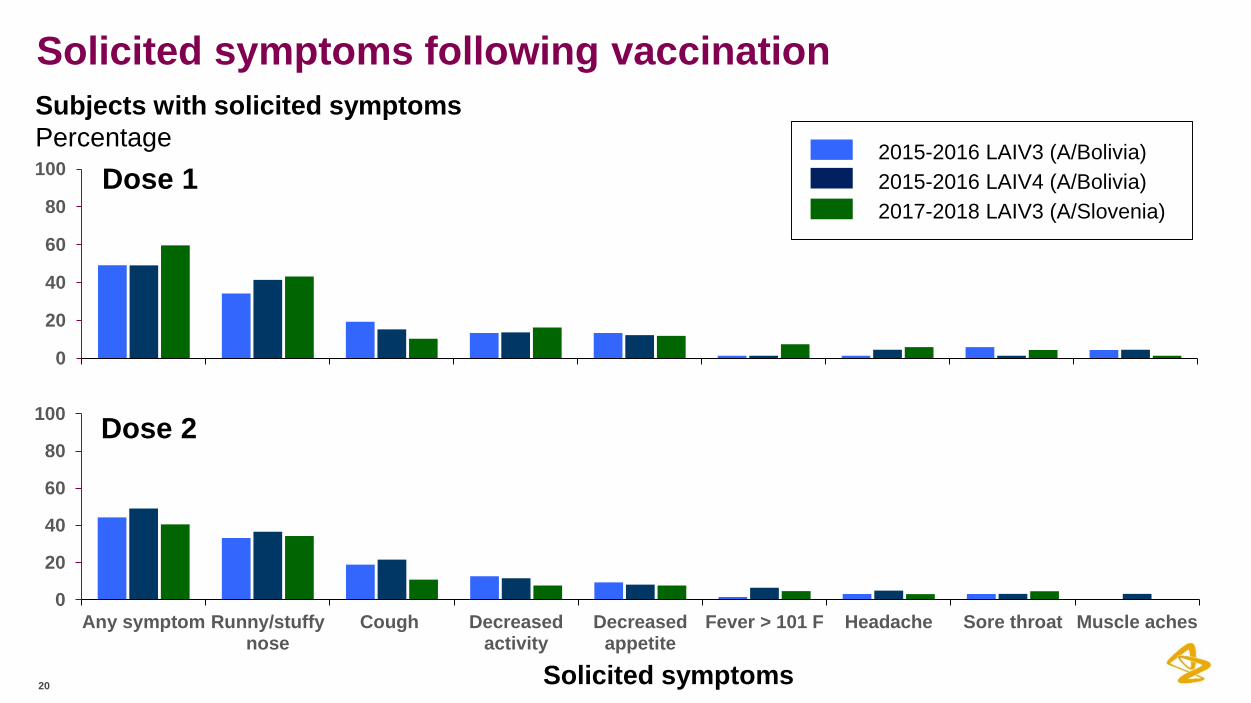
Solicited symptoms following vaccination
20
0
20
40
60
80
100
Any symptom Runny/stuffynose
Cough Decreasedactivity
Decreasedappetite
Fever > 101 F Headache Sore throat Muscle aches
Solicited symptoms
2015-2016 LAIV3 (A/Bolivia)2015-2016 LAIV4 (A/Bolivia)2017-2018 LAIV3 (A/Slovenia)
0
20
40
60
80
100 Dose 1
Dose 2
Subjects with solicited symptomsPercentage

Adverse events occurred at similar rates across the arms
21
LAIV3 2015-2016 (A/Bolivia)
N = 67
LAIV4 2015-2016 (A/Bolivia)
N = 66
LAIV4 2017-2018 (A/Slovenia)
N = 67
All subjects
N = 200
At least one event 29 (43.3%) 31 (47.0%) 34 (50.7%) 94 (47.0%)
At least one related event
5 ( 7.5%) 2 ( 3.0%) 3 ( 4.5%) 10 ( 5.0%)
At least one ≥ Grade 3 event
0 0 1 ( 1.5%) 1 ( 0.5%)
Death 0 0 0 0
At least one serious event
0 0 0 0
Grade 3 event was strep throat: this occurred in a male subject 16 days after the second dose of vaccine and was considered not related to vaccination

H1N1 data
22

23
23
0 .0
1 .0
2 .0
3 .0
4 .0
5 .0
6 .0
7 .0
8 .0
S tu d y d a y
Lo
g1
0 v
ira
l c
op
ies
/mL
D a y 3D a y 2 D a y 4 D a y 5 D a y 7
Q /L A IV 2 0 1 7 -1 8Q /L A IV 2 0 1 5 -1 6T r i/L A IV 2 0 1 5 -1 62015-2016 LAIV3 (A/Bolivia)
2015-2016 LAIV4 (A/Bolivia)2017-2018 LAIV4 (A/Slovenia)
Limit of quantification
Viral titers of shed A/H1N1 strains after Dose 1*
* Subjects with viral titers above limit of detection
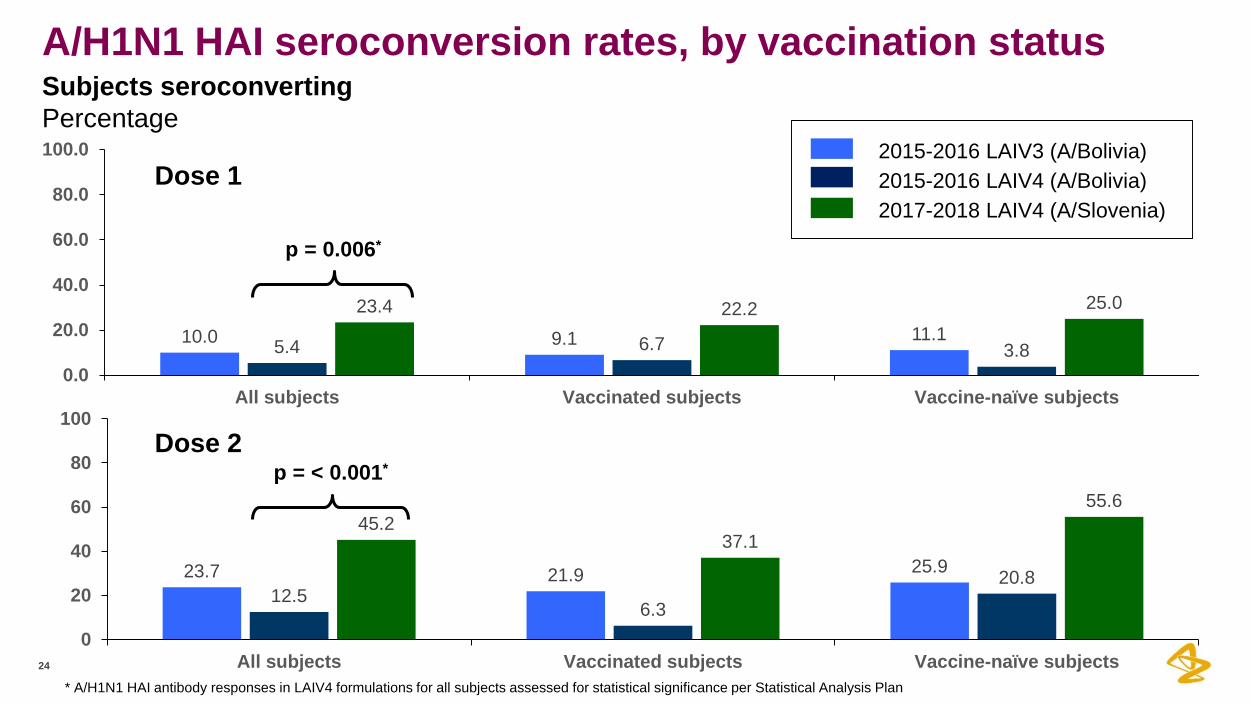
A/H1N1 HAI seroconversion rates, by vaccination status
24
Dose 12015-2016 LAIV3 (A/Bolivia)2015-2016 LAIV4 (A/Bolivia)2017-2018 LAIV4 (A/Slovenia)
p = 0.006*
p = < 0.001*Dose 2
23.7 21.9 25.912.5
6.3
20.8
45.237.1
55.6
0
20
40
60
80
100
All subjects Vaccinated subjects Vaccine-naïve subjects
10.0 9.1 11.15.4 6.7 3.8
23.4 22.2 25.0
0.0
20.0
40.0
60.0
80.0
100.0
All subjects Vaccinated subjects Vaccine-naïve subjects
Subjects seroconvertingPercentage
* A/H1N1 HAI antibody responses in LAIV4 formulations for all subjects assessed for statistical significance per Statistical Analysis Plan
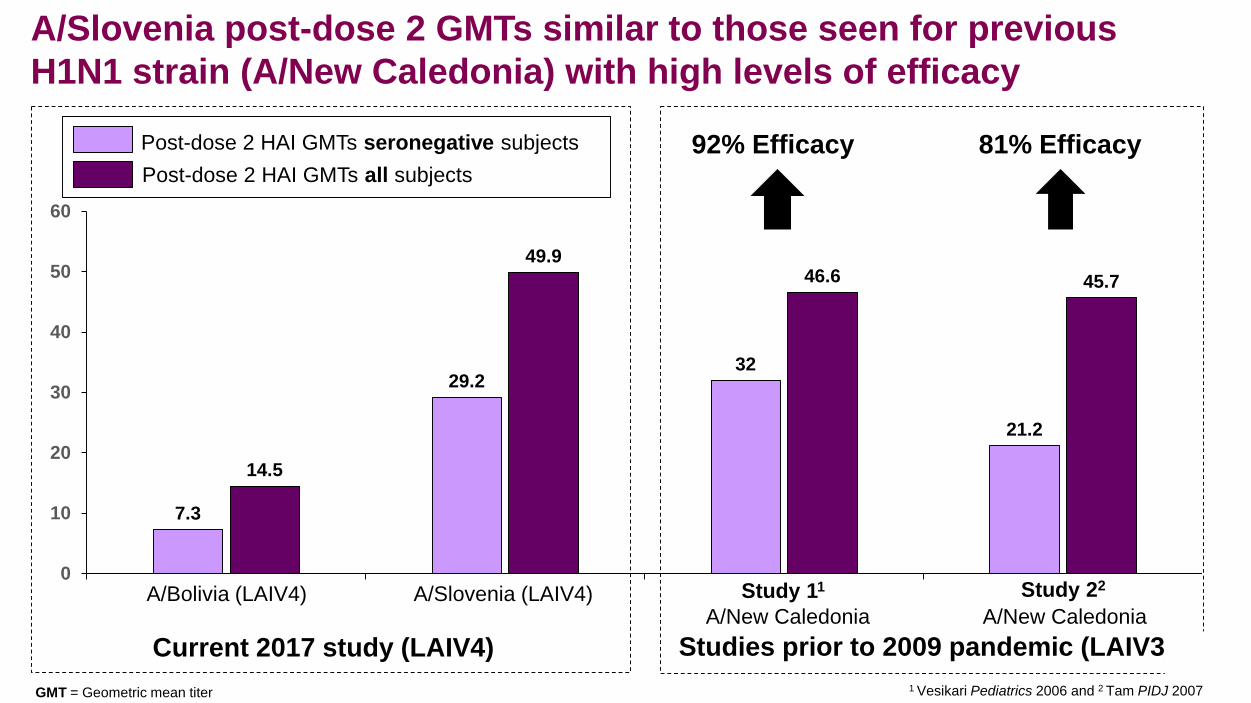
A/Slovenia post-dose 2 GMTs similar to those seen for previous H1N1 strain (A/New Caledonia) with high levels of efficacy
7.3
29.2
14.5
49.9
0
10
20
30
40
50
60
Post-dose 2 HAI GMTs seronegative subjectsPost-dose 2 HAI GMTs all subjects
A/Bolivia (LAIV4) A/Slovenia (LAIV4)
Current 2017 study (LAIV4)
32
21.2
46.6 45.7
A/New CaledoniaStudy 11
A/New CaledoniaStudy 22
92% Efficacy 81% Efficacy
Studies prior to 2009 pandemic (LAIV3)1 Vesikari Pediatrics 2006 and 2 Tam PIDJ 2007GMT = Geometric mean titer
H3N2 data
26
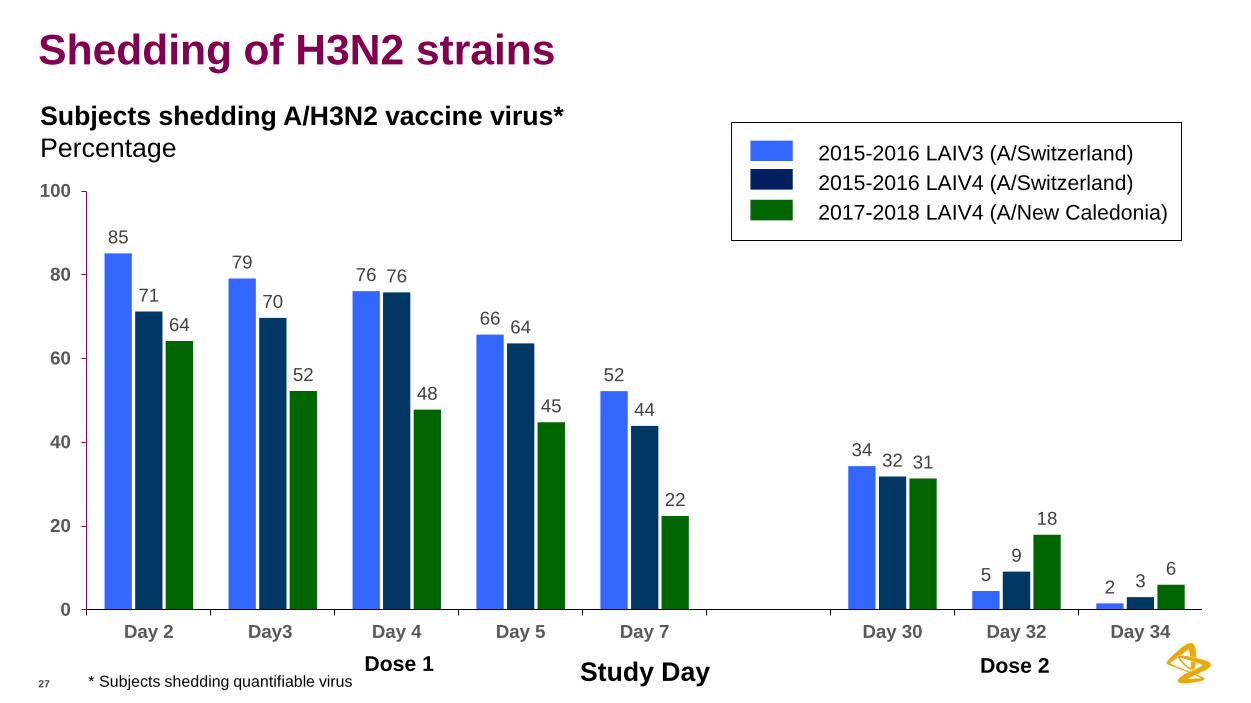
Shedding of H3N2 strains
27
8579 76
66
52
34
5 2
71 7076
64
44
32
93
64
5248 45
22
31
18
6
0
20
40
60
80
100
Day 2 Day3 Day 4 Day 5 Day 7 Day 30 Day 32 Day 34
Study DayDose 1 Dose 2 * Subjects shedding quantifiable virus
2015-2016 LAIV3 (A/Switzerland)2015-2016 LAIV4 (A/Switzerland)2017-2018 LAIV4 (A/New Caledonia)
Subjects shedding A/H3N2 vaccine virus*Percentage
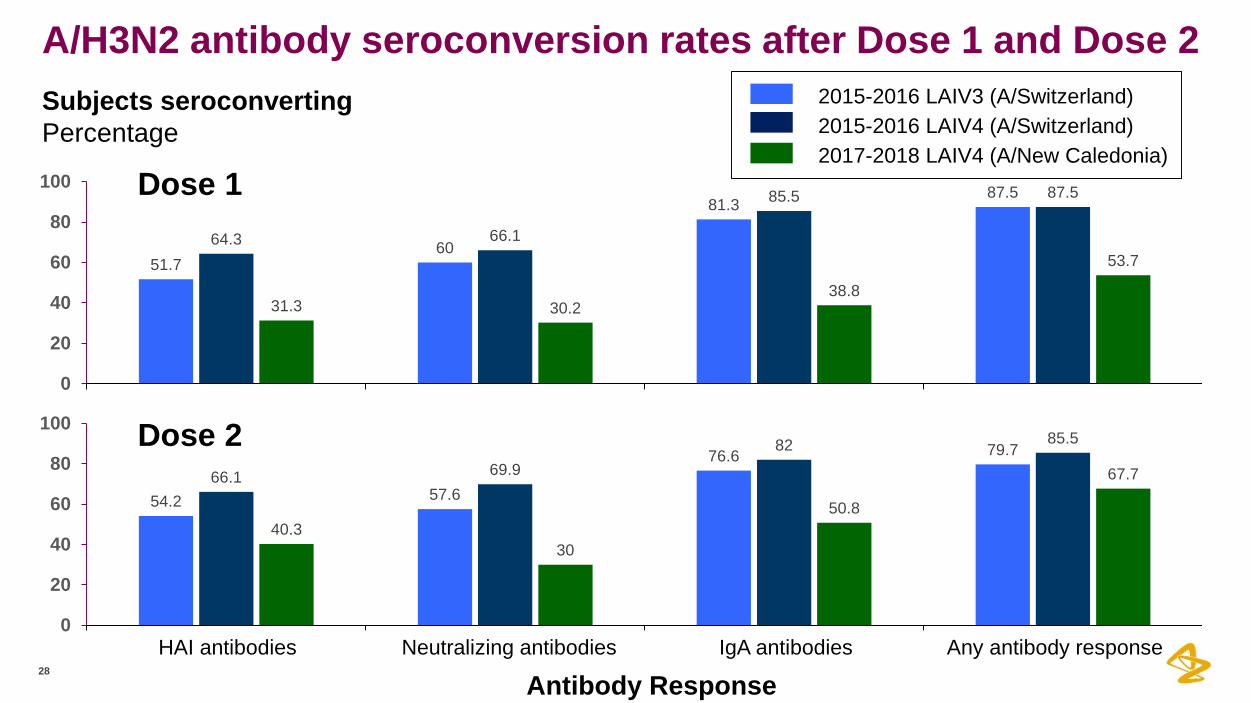
A/H3N2 antibody seroconversion rates after Dose 1 and Dose 2
28
54.2 57.6
76.6 79.7
66.1 69.982 85.5
40.330
50.8
67.7
0
20
40
60
80
100
2015-2016 LAIV3 (A/Switzerland)2015-2016 LAIV4 (A/Switzerland)2017-2018 LAIV4 (A/New Caledonia)
Antibody Response
51.760
81.387.5
64.3 66.1
85.5 87.5
31.3 30.238.8
53.7
0
20
40
60
80
100
HAI antibodies Neutralizing antibodies IgA antibodies Any antibody respons
Dose 1
Dose 2
e
Subjects seroconvertingPercentage

A/H3N2 post-dose 2 GMTs similar to those seen for three previous H3N2 strains with high levels of efficacy
29
293
127
385
170
0
50
100
150
200
250
300
350
400
A/New CaledoniaA/Switzerland
Current 2017 study (LAIV4)
Post Dose 2 HAI GMTs all subjects
Post Dose 2 HAI GMTs seronegative subjects
34
202
5644
211
73
90% Efficacy 73% Efficacy 96% Efficacy
Previous studies (LAIV3)A/SydneyStudy 11
A/PanamaStudy 22
A/WuhanStudy 33
1 Tam PIDJ 2007; 2 Neto PIDJ 2009 and 3 Belshe NEJM 1998GMT = Geometric mean titer
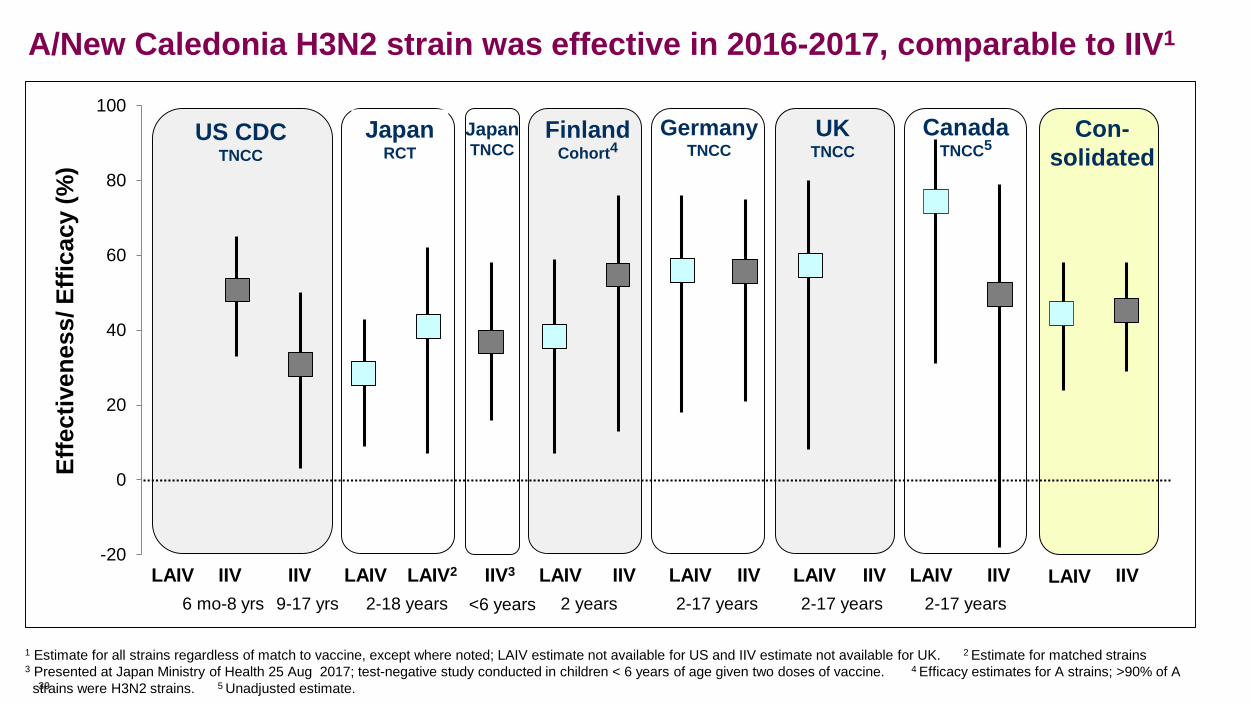
-20
0
20
40
60
80
100
Effe
ctiv
enes
s/ E
ffica
cy (%
)
6 mo-8 yrs 2-18 years 2 years 2-17 years 2-17 yearsLAIV IIV IIV
UK TNCC
LAIV LAIV2 LAIV LAIV LAIV LAIVIIV3 IIV IIV IIV IIV9-17 yrs 2-17 years
US CDC TNCC
Germany TNCC
Canada TNCC5
Con-solidated
LAIV IIV
Japan TNCC
Finland Cohort4
Japan RCT
<6 years
A/New Caledonia H3N2 strain was effective in 2016-2017, comparable to IIV1
1 Estimate for all strains regardless of match to vaccine, except where noted; LAIV estimate not available for US and IIV estimate not available for UK. 2 Estimate for matched strains 3 Presented at Japan Ministry of Health 25 Aug 2017; test-negative study conducted in children < 6 years of age given two doses of vaccine. 4 Efficacy estimates for A strains; >90% of As30trains were H3N2 strains. 5 Unadjusted estimate.

B strain data
31
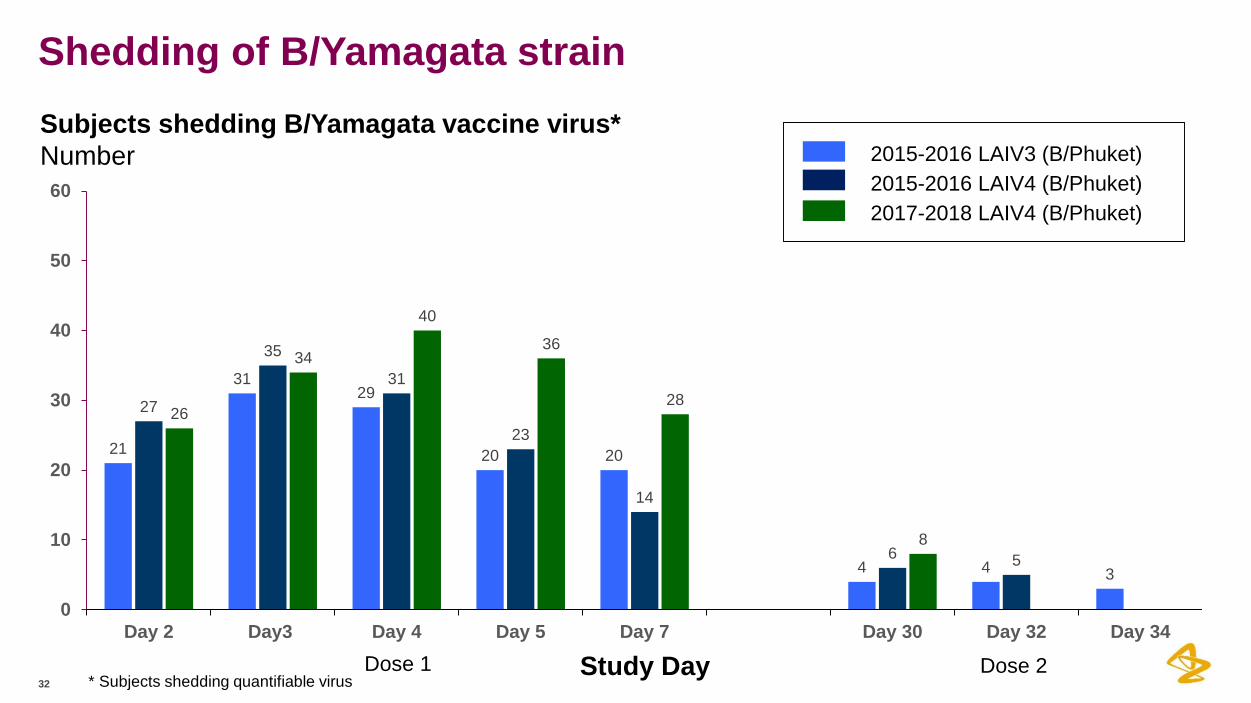
Shedding of B/Yamagata strain
32
21
3129
20 20
4 4 3
27
35
31
23
14
6 5
26
34
40
36
28
8
0
10
20
30
40
50
60
Day 2 Day3 Day 4 Day 5 Day 7 Day 30 Day 32 Da
Study DayDose 1 Dose 2
2015-2016 LAIV3 (B/Phuket)2015-2016 LAIV4 (B/Phuket)2017-2018 LAIV4 (B/Phuket)
y 34
Subjects shedding B/Yamagata vaccine virus*Number
* Subjects shedding quantifiable virus
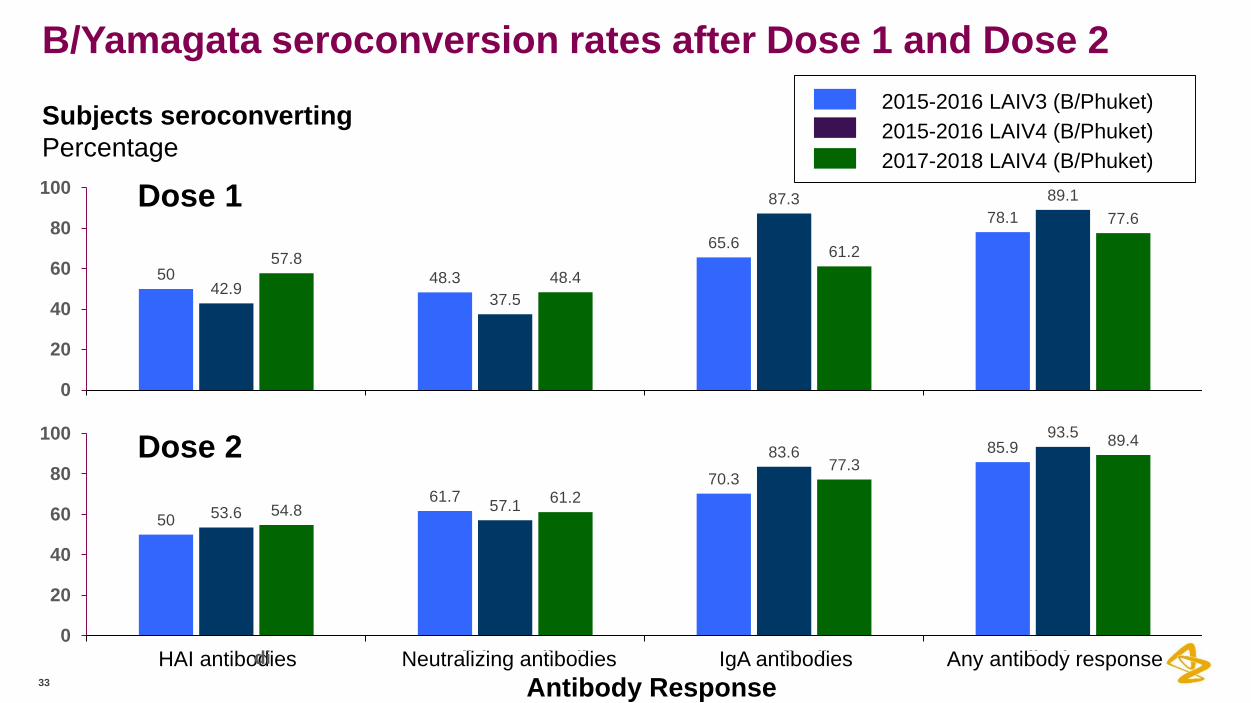
B/Yamagata seroconversion rates after Dose 1 and Dose 2
33
Dose 1
Dose 2
50 48.3
65.678.1
42.937.5
87.3 89.1
57.848.4
61.2
77.6
0
20
40
60
80
100
5061.7
70.3
85.9
53.6 57.1
83.693.5
54.861.2
77.389.4
0
20
40
60
80
100
2015-2016 LAIV3 (B/Phuket)2015-2016 LAIV4 (B/Phuket)2017-2018 LAIV4 (B/Phuket)
Subjects seroconvertingPercentage
Antibody ResponseHAI antibodidi es Neutralizing antibodies IgA antibodies Any antibody responseN t li i tib di I A tib di A tib d
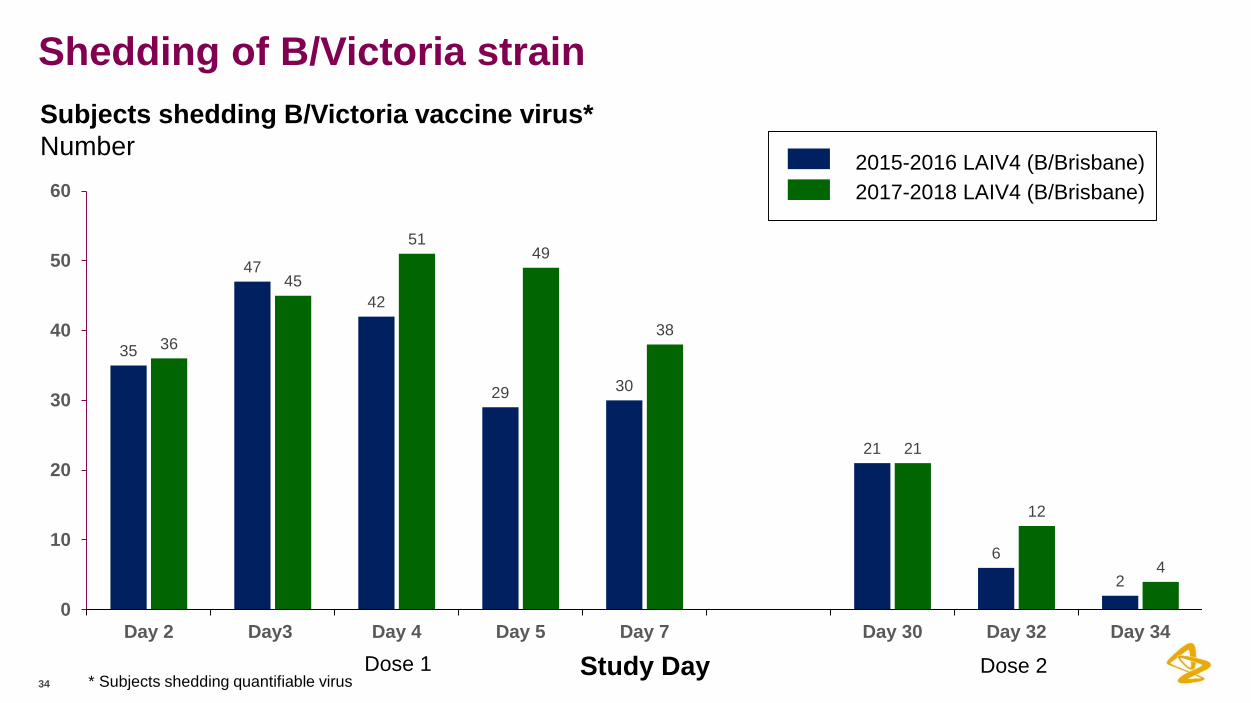
Shedding of B/Victoria strain
34
35
47
42
29 30
21
6
2
36
45
5149
38
21
12
4
0
10
20
30
40
50
60
Day 2 Day3 Day 4 Day 5 Day 7 Day 30 Day 32 Day 34
Study DayDose 1 Dose 2
2017-2018 LAIV4 (B/Brisbane)2015-2016 LAIV4 (B/Brisbane)
Subjects shedding B/Victoria vaccine virus*Number
* Subjects shedding quantifiable virus
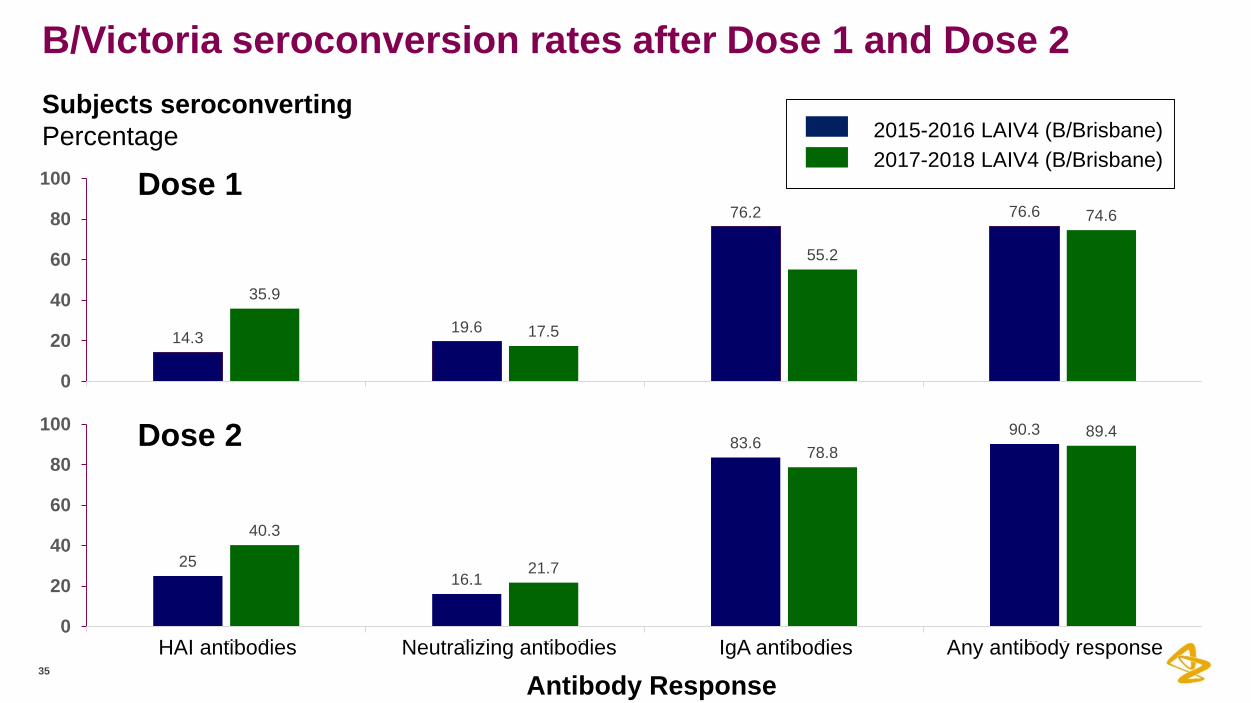
B/Victoria seroconversion rates after Dose 1 and Dose 2
35
Subjects seroconvertingPercentage
Antibody ResponseHAI antibodies Neutralizing antibodies IgA antibodies Any antibody response
Dose 1
Dose 2
14.3 19.6
76.2 76.6
35.9
17.5
55.2
74.6
0
20
40
60
80
100
2516.1
83.690.3
40.3
21.7
78.889.4
0
20
40
60
80
100
2017-2018 LAIV4 (B/Brisbane)2015-2016 LAIV4 (B/Brisbane)
HAI tib di N t li i tib di I A tib di A tib d

Root cause investigation
36
LAIV effectiveness investigation: Root Causes• Likely root cause = Reduced replicative fitness of H1N1pdm09 LAIV strains
• No support for the following as likely root causes:
Pre-existing immunity from prior vaccination
Quadrivalent-specific vaccine virus interference
Vaccine virus temperature stability and heat exposure during shipping
Manufacturing
Stability at 2-8 ⁰C
37

Unlikely Root Cause:Pre-existing immunity among vaccinated children
38
LAIV3 demonstrated low to no vaccine effectiveness against post-pandemic strains in 2010-2011 season 1,2
Given observations of reduced effectiveness with LAIV3, quadrivalent-specific interference considered an unlikely root cause of the reduced VE
Interference could be a contributing factor to the low effectiveness in context of reduced replicative fitness of post-pandemic LAIV strains
However, A/Slovenia strain in the quadrivalent formulation was more immunogenic than the A/Bolivia strain in the trivalent or quadrivalent formulations
Immunogenicity of A/Slovenia was similar to a highly effective pre-pandemic strain in the trivalent formulation
1. Chung JR, Flannery B, Thompson MG, et. al. Pediatrics 2016, 2. Helmeke et al. PLoS One. 2015., 3. Victor J, Lewis K, Diallo A, et. al. Lancet Glob Health. 2016.

Unlikely Root Cause:Vaccine virus interference from quadrivalent formulation
39
• LAIV3 demonstrated low to no vaccine effectiveness against post-pandemic strains in 2010-2011 season 1,2
• Given observations of reduced effectiveness with LAIV3, quadrivalent-specific interference considered an unlikely root cause of the reduced VE
• Interference could be a contributing factor to the low effectiveness in context of reduced replicative fitness of post-pandemic LAIV strains
• However, A/Slovenia strain in the quadrivalent formulation was more immunogenic than the A/Bolivia strain in the trivalent or quadrivalent formulations
• Immunogenicity of A/Slovenia was similar to a highly effective pre-pandemic strain in the trivalent formulation
1. Chung JR, Flannery B, Thompson MG, et. al. Pediatrics 2016, 2. Helmeke et al. PLoS One. 2015., 3. Victor J, Lewis K, Diallo A, et. al. Lancet Glob Health. 2016.





























