Embed Size (px)
Citation preview
1
ACO 2013 Collaborative: Reflecting on Progress, Preparing for the Future
ACO 2013 Collaborative: Reflecting on Progress, Preparing for the Future
MEETING SUMMARYApril 15-17, 2013 • San Francisco, California
SM
American Medical Group Association
2
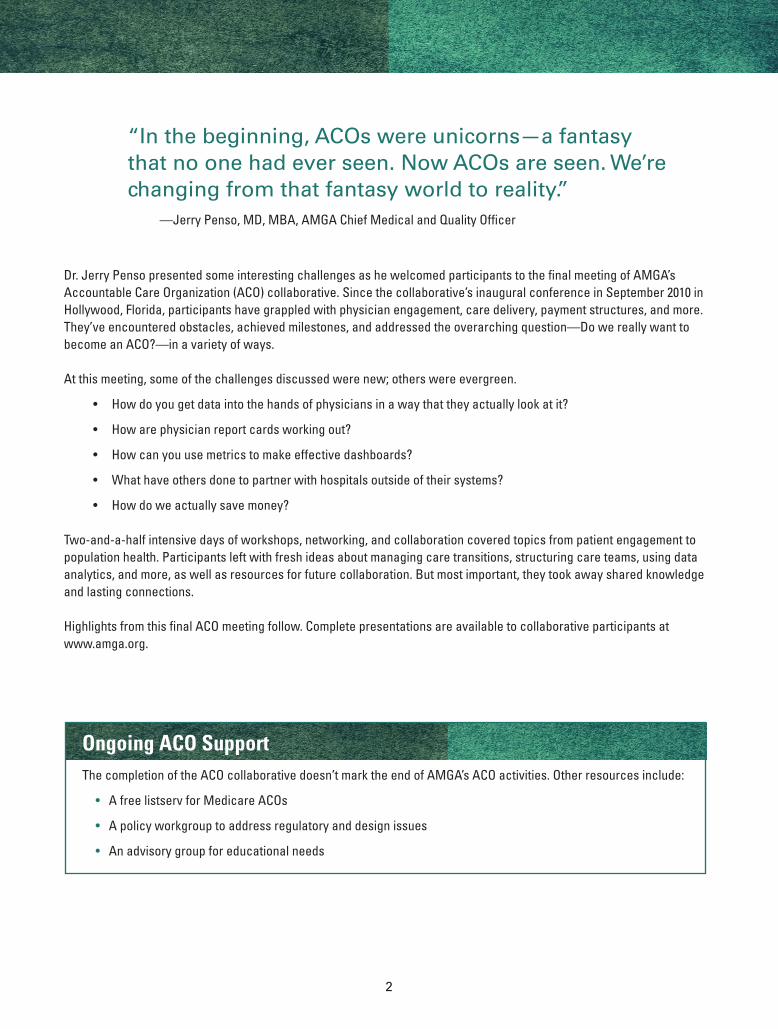
Dr. Jerry Penso presented some interesting challenges as he welcomed participants to the final meeting of AMGA’s Accountable Care Organization (ACO) collaborative. Since the collaborative’s inaugural conference in September 2010 in Hollywood, Florida, participants have grappled with physician engagement, care delivery, payment structures, and more. They’ve encountered obstacles, achieved milestones, and addressed the overarching question—Do we really want to become an ACO?—in a variety of ways.
At this meeting, some of the challenges discussed were new; others were evergreen.
• Howdoyougetdataintothehandsofphysiciansinawaythattheyactuallylookatit?
• Howarephysicianreportcardsworkingout?
• Howcanyouusemetricstomakeeffectivedashboards?
• Whathaveothersdonetopartnerwithhospitalsoutsideoftheirsystems?
• Howdoweactuallysavemoney?
Two-and-a-halfintensivedaysofworkshops,networking,andcollaborationcoveredtopicsfrompatientengagementtopopulation health. Participants left with fresh ideas about managing care transitions, structuring care teams, using data analytics,andmore,aswellasresourcesforfuturecollaboration.Butmostimportant,theytookawaysharedknowledgeand lasting connections.
Highlights from this final ACO meeting follow. Complete presentations are available to collaborative participants at www.amga.org.
Ongoing ACO SupportThecompletionoftheACOcollaborativedoesn’tmarktheendofAMGA’sACOactivities.Otherresourcesinclude:
• A free listserv for Medicare ACOs
•Apolicyworkgrouptoaddressregulatoryanddesignissues
• An advisory group for educational needs
“In the beginning, ACOs were unicorns—a fantasy that no one had ever seen. Now ACOs are seen. We’re changing from that fantasy world to reality.” —Jerry Penso, MD, MBA, AMGA Chief Medical and Quality Officer
3
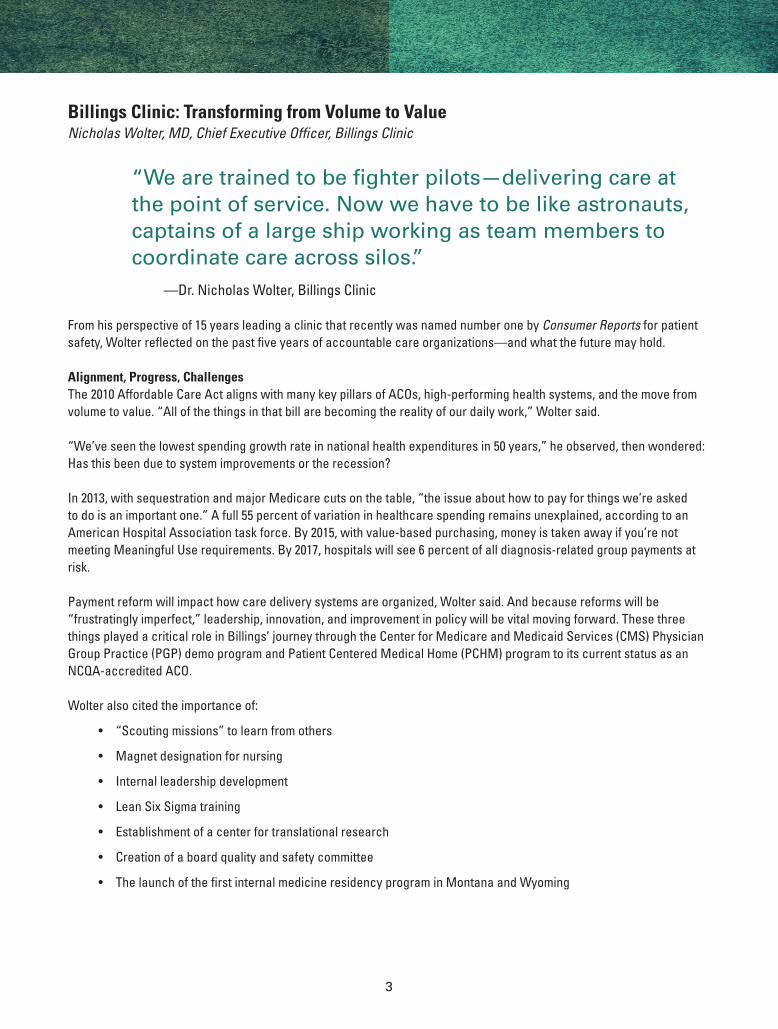
Billings Clinic: Transforming from Volume to ValueNicholas Wolter, MD, Chief Executive Officer, Billings Clinic
“We are trained to be fighter pilots—delivering care at the point of service. Now we have to be like astronauts, captains of a large ship working as team members to coordinate care across silos.”
—Dr.NicholasWolter,BillingsClinic
From his perspective of 15 years leading a clinic that recently was named number one by Consumer Reports for patient safety,Wolterreflectedonthepastfiveyearsofaccountablecareorganizations—andwhatthefuturemayhold.
Alignment, Progress, ChallengesThe2010AffordableCareActalignswithmanykeypillarsofACOs,high-performinghealthsystems,andthemovefromvolumetovalue.“Allofthethingsinthatbillarebecomingtherealityofourdailywork,”Woltersaid.
“We’veseenthelowestspendinggrowthrateinnationalhealthexpendituresin50years,”heobserved,thenwondered:Has this been due to system improvements or the recession?
In2013,withsequestrationandmajorMedicarecutsonthetable,“theissueabouthowtopayforthingswe’reaskedtodoisanimportantone.”Afull55percentofvariationinhealthcarespendingremainsunexplained,accordingtoanAmericanHospitalAssociationtaskforce.By2015,withvalue-basedpurchasing,moneyistakenawayifyou’renotmeeting Meaningful Use requirements. By 2017, hospitals will see 6 percent of all diagnosis-related group payments at risk.
Paymentreformwillimpacthowcaredeliverysystemsareorganized,Woltersaid.Andbecausereformswillbe“frustratinglyimperfect,”leadership,innovation,andimprovementinpolicywillbevitalmovingforward.Thesethreethings played a critical role in Billings’ journey through the Center for Medicare and Medicaid Services (CMS) Physician Group Practice (PGP) demo program and Patient Centered Medical Home (PCHM) program to its current status as an NCQA-accredited ACO.
Wolteralsocitedtheimportanceof:
• “Scoutingmissions”tolearnfromothers
• Magnetdesignationfornursing
• Internalleadershipdevelopment
• LeanSixSigmatraining
• Establishmentofacenterfortranslationalresearch
• Creationofaboardqualityandsafetycommittee
• ThelaunchofthefirstinternalmedicineresidencyprograminMontanaandWyoming
4
Highlights from the Billings JourneyOverthepastfiveyears,BillingsClinichasachievedseveralsuccessfulmilestones:
• ActivitiesasaPGPdemositehelpedreducepsychiatrichospitalizations,chronicconditionmanagement,ERvisits,andcaremanagementnavigationforcomplexpatients.
• Electronichealthrecords(EHRs)installedsystem-widehelpedimprovequalityscores.
• BundledpaymentsandadesignedComprehensiveCancerCenterProgrambroughttheclinicresearchdollarsandotherwise unavailable protocols.
• TheBillingsCultureofQualityandSafetyinitiativedecreasedsomecategoriesofsafetyeventstozero.
• Hospitaladmissionsdecreasedby20percent.
• Theclinicrealized$22millioninbenefitssince2009.
The clinic addressed gaps and leveraged opportunities through enhancing its physician leadership, improving its cost accounting, implementing decision support tools, and coordinating care across its nine clinics. Key strategies were “hardwired”intotactics,rolesandresponsibilities,andabalancedscorecard—andgroundedinasteadfastcommitmenttoculture.Forinstance,Billingsused“bestinnation”languageinitsvisionstatement,broughtinaretiredDisneyemployeetoconsult on service improvement, put an emphasis on internal recognition and physician and engagement, and committed its cornerstone principles in writing.
“Itusedtobe‘Ijustcameheretopracticemedicine.’Nowdoctorssay‘Iusedtothinkthiswascrazy,butnowIbelievethis.’It’sveryinternallymotivated,”saidWolter.
Charting the Right Path Movingforward,BillingsaimstocontinueasanaccreditedACOandworktowardevenmoremilestones:reducepreventableharmby50percent(andultimatelytozero),putinabusinessintelligencesystemtomeasureandtrackcosts,andusesepsistreatmentandend-of-lifecaretoreducetheobserved-to-expectedmortalityratio—tonamejustafew.
ForothermedicalgroupsconsideringanACOpathway,Wolterobservedthat:
• The PCMH program may help improve care delivery and cost management through things such as patient registries,chronicdiseasemonitoring,andperformancereportsbacktoproviders.
• The Physician Quality Reporting System will be an “interesting experience” for small and free-standing medical groups,asthesystemputsafairamountofpaymentatriskfordoctorsandissuesa1.5-2percentpenaltyfornotreporting.
• Medicare Shared Savings will be challenged by attribution and threshold requirements.“We’vedecidedtoparticipateintheprojectsowecanlearnhowtogetbetter,”Woltersaid.“Butit’sclearlyanissuewhenyoudon’tlikelyhaveachancetosharesavings.”
• Bundled payments will provide opportunities for learning. “In many studies, the variation in spending is bigger in post-acutecarethaninin-patientstays.Whatareothergoodorganizationsdoing?Howcanwetacklecoststhatareabovebenchmarks?”
5
Questions for the FutureWhichtypeofACOwillbemorelikelytosucceed—MedicareAdvantageorcommercialACOpartnerships?WhataboutprogramslikePACEthatfocusonhigh-risk,high-costpatients?WhathappensiftheAffordableCareActisrepealedormodified, or if the economy improves substantially?
Asthesequestionsplayout,Wolteradvisedparticipantsto:
• Letphysicianslead
• Createnewpartnerships—especiallywithhospitals,whichhavebeen“makingmorebydoingmore”fordecades
• Developskillsaroundthescienceofhealthcaredeliveryandastrategyforpatientengagement
• Becomemoreinvolvedinthedevelopmentofinnovativepolicy
“There’snotanactiveagendaaboutimprovingtheunderlyingfee-for-servicesystem,andthat’sabigproblem,”saidWolter.“Ifwedon’tstartthinkingofnewthingsanddealingwithunderlyingfee-for-servicepaymentstructure,wemayfindthesenewthingsnotworkingouttoowell.”
Collaborative ThinkingParticipant questions ranged from specific operations to overarching culture.
Q: How does Billings Clinic, which serves such a huge geographic area, use telemedicine? A: Theorganizationstartedinmentalhealthandis“aggressively”expandinginclinicalareassuchascardiologyfollow-up.FromadministrativetaskstointeractingwithpatientsintheirhomesviaSkypeandFacetime,“Ithinkthere’salotofpromisethere,”saidWolter.
Q. What kind of staff does Billings devote to performance and QA improvement?A:Theclinicengagesnurses,rightupthroughthechiefnursingofficer,anddoessomeworkinHR,suchassurveysandPascal metrics. Doctors tapped from more than 40 medical departments are compensated for their time with stipends. In termsofintegration,departmentchairssupportbothhospitalworkandclinicalwork.
Q: Are there any shortcuts for developing culture?A:AccordingtoWolter,“Ittakesthreegenerationsofleadershipforallthesechangestobereallydeeplyrooted.It’snotlikelythatafour-yearACOprojectwillgetyouwhereyouwanttogo,althoughmanyofthethingswe’reworkingonarethingsweneedtobedoing.Onethingiscertain:Unlessyouhavepersistenceandcornerstonesthatwillwithstandtime,it’slikelyyouwon’tgetthere.”
6
Park Nicollet Health Services: Dispatches from an Accountable Care Pioneer Sam VanNorman, MBA, Co-Chair, Office of Population Health, and Director, Business Intelligence, and Meg Cox, Director, Population Health/Medicare, Park Nicollet
AnintegratedcaresystembasedinSt.LouisPark,Minnesota,ParkNicolletHealthServiceswasoneof32healthsystemschosen nationwide to participate in the Pioneer ACO program. As a Pioneer ACO, the organization dealt with aligning teams totasks,managingdata,andgrapplingwiththetransitionfrompay-for-reportingtopay-for-performance(requirementsagroupofPioneerACOsrecentlyaskedCMStoreconsider).VanNormanandCoxdiscussedchallengesfacedandlessonslearned along the way as a Pioneer ACO and as a PGP demo participant.
Taming the Data BeastCollaborating with the CMS, which doesn’t always provide concrete information or reliable help, can be a lot of hard work,VanNormanandCoxpointedout.Participantsneedenoughmanpower,stamina,andtimetomakeorganization-widechangesandreportspeedilyonmountainsofdata.Beforemakingsuchanenormousdatatrackingandreportingcommitment,it’shelpfultoask:
• Dowehaveenoughemployeeswhoarewellsuitedtothiswork?
• Whatpre-workshouldwedo,suchasbuildingreportingsystemsordatawarehouses?
• Howmucheffortcanwedevotetoourpay-for-reportingmeasures?
• Howmucheffortcanwedevotetoourpay-for-performancemeasures?
• Arewesurewewanttodothis?
Delegate, Automate, and Keep MovingParkNicolletdecideditsclinicalreportingandanalysisteamwasbestsuitedfortheworkofmanagingchronicdiseaseregistries, core measures, Minnesota community measures, and pay-for- performance quality reporting. Staff in business intelligence, IT, care delivery, and population health were placed nearby to support the team and develop collegial cross-functionality—a crucial element for ACO success.
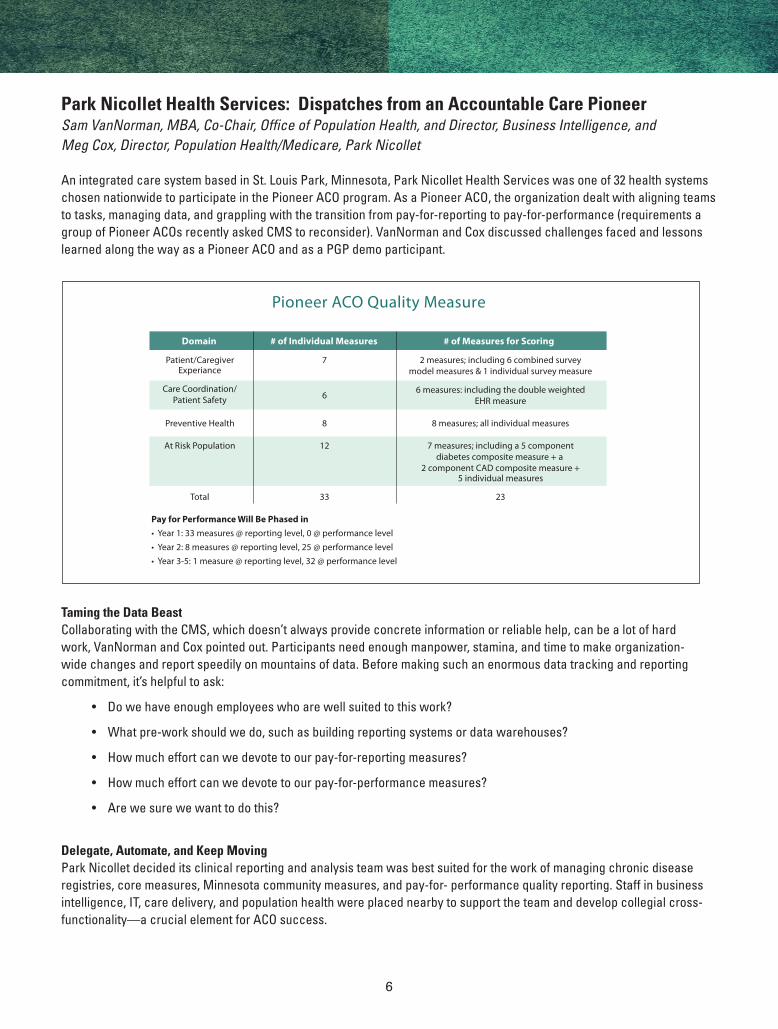
Pioneer ACO Quality Measure
Domain # of Individual Measures # of Measures for Scoring
Patient/CaregiverExperiance
Preventive Health
At Risk Population
Care Coordination/Patient Safety
7
8
12
6
2 measures; including 6 combined surveymodel measures & 1 individual survey measure
8 measures; all individual measures
7 measures; including a 5 componentdiabetes composite measure + a
2 component CAD composite measure +5 individual measures
6 measures: including the double weightedEHR measure
Total 33 23
Pay for Performance Will Be Phased in• Year 1: 33 measures @ reporting level, 0 @ performance level• Year 2: 8 measures @ reporting level, 25 @ performance level• Year 3-5: 1 measure @ reporting level, 32 @ performance level
7
Automating as much abstraction as possible as early as possible made a huge difference, even if it meant correcting some fileslaterbyhand.Sincecollectingandanalyzingdataisatime-intensive,machine-assistedmanualprocess—andlikelyalwayswillbe,VanNormanandCoxadded—theystartedtheprocessimmediatelyandfoundwaystomotivatestafftopersist.Tomaximizeefficiency,theyassignedoneemployeespecialisttoeachspecificdataset.
Ultimately,VanNormansays,ACOparticipantsmustbecomfortablewith“prettygooddata.”Therateofgrowthfororganizationscanbesofast,there’sonlytimeforgeneralindicators,notpeer-reviewedresearchorconcretefindings.“Wehavetoallowourselvestosay‘weknowthisisdirectionallycorrect—it’sgettingbiggerorsmaller,’andhavethatbeenoughforusrightnow,”saidVanNorman
Strengthening OperationsAswithdatareporting,providersshouldaskkeyquestionsbeforeundertakingaqualityimprovementinitiative:
• Dowehavethetechnicalskillsandresourcestoidentifyopportunities?
• Dowehaveenoughdisciplinetoinnovate?
• Dowehaveenoughdisciplinetokickbadhabits?
• Willweimprovequalityforallourpatientsorusetestpopulationsfirst?
• Whatwillsuccesslooklike?
• Arewesurewewanttodothis?
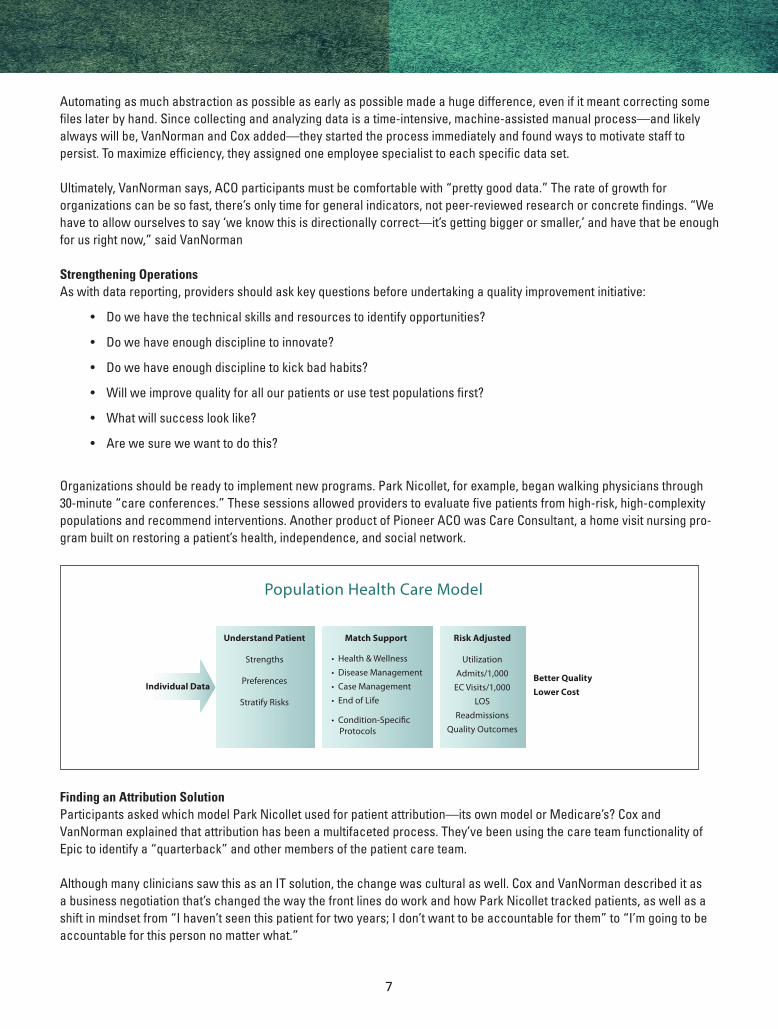
Organizationsshouldbereadytoimplementnewprograms.ParkNicollet,forexample,beganwalkingphysiciansthrough30-minute“careconferences.”Thesesessionsallowedproviderstoevaluatefivepatientsfromhigh-risk,high-complexitypopulations and recommend interventions. Another product of Pioneer ACO was Care Consultant, a home visit nursing pro-grambuiltonrestoringapatient’shealth,independence,andsocialnetwork.
Finding an Attribution SolutionParticipantsaskedwhichmodelParkNicolletusedforpatientattribution—itsownmodelorMedicare’s?CoxandVanNormanexplainedthatattributionhasbeenamultifacetedprocess.They’vebeenusingthecareteamfunctionalityofEpictoidentifya“quarterback”andothermembersofthepatientcareteam.
AlthoughmanyclinicianssawthisasanITsolution,thechangewasculturalaswell.CoxandVanNormandescribeditasabusinessnegotiationthat’schangedthewaythefrontlinesdoworkandhowParkNicollettrackedpatients,aswellasashiftinmindsetfrom“Ihaven’tseenthispatientfortwoyears;Idon’twanttobeaccountableforthem”to“I’mgoingtobeaccountableforthispersonnomatterwhat.”
Population Health Care Model
Match Support
• Health & Wellness• Disease Management• Case Management• End of Life
• Condition-Speci�c Protocols
Understand Patient
Strengths
Preferences
Stratify Risks
Individual DataBetter QualityLower Cost
Risk Adjusted
UtilizationAdmits/1,000
EC Visits/1,000LOS
ReadmissionsQuality Outcomes
8
Putting the ACO Experience into PerspectiveParkNicolletalsoparticipatedintheCMSPGPdemonstrationproject,thefirstpay-for-performanceinitiativeundertheMedicareprogram.Despitefrustrationsinareassuchasqualityreportingandsharedsavings,CoxandVanNormansaidthatthePGPandPioneerACOprogramsdeliveredvaluebyenablingParkNicollettoimplementclinicalimprovementinitiatives,create a foundation for quality improvement, grow capabilities in data management, and address important questions in the care delivery process.
“ACOisprobablynottheendoftheroadorthepaymentmethodwe’llstickwithforever,”saidCox.“Butbecomingaccountableforqualityandcostsissomethingwearelikelytostickwith.”
“The perverse incentives are starting to go away, we’re starting to align our healthcare in a way I haven’t seen since I’ve beeninhealthcare,”saidVanNorman.
9
Mastering the Rules of Patient Engagement Angie Hochhalter, PhD, Research Scientist, Scott & White Healthcare
“The distinction between improving health outcomes and improving healthcare is having the people we’re serving involved in the decisions.”
—AngieHochhalter,PhD,Scott&WhiteHealthcare
Improving patient engagement is a growing priority in today’s healthcare environment, and for many, it’s a difficult challenge. Hochhalter discussed common issues and helpful strategies for building active partnerships among clinicians, patients and families.
Cornerstone Behaviors
AccordingtotheCenterfortheAdvancementofHealth’sEngagementBehaviorFramework,toreceiveoptimal care,patientsmustknowhowto:
• Findgoodcare
• Participateintreatment
• Communicatewithproviders
• Seekhealthknowledge
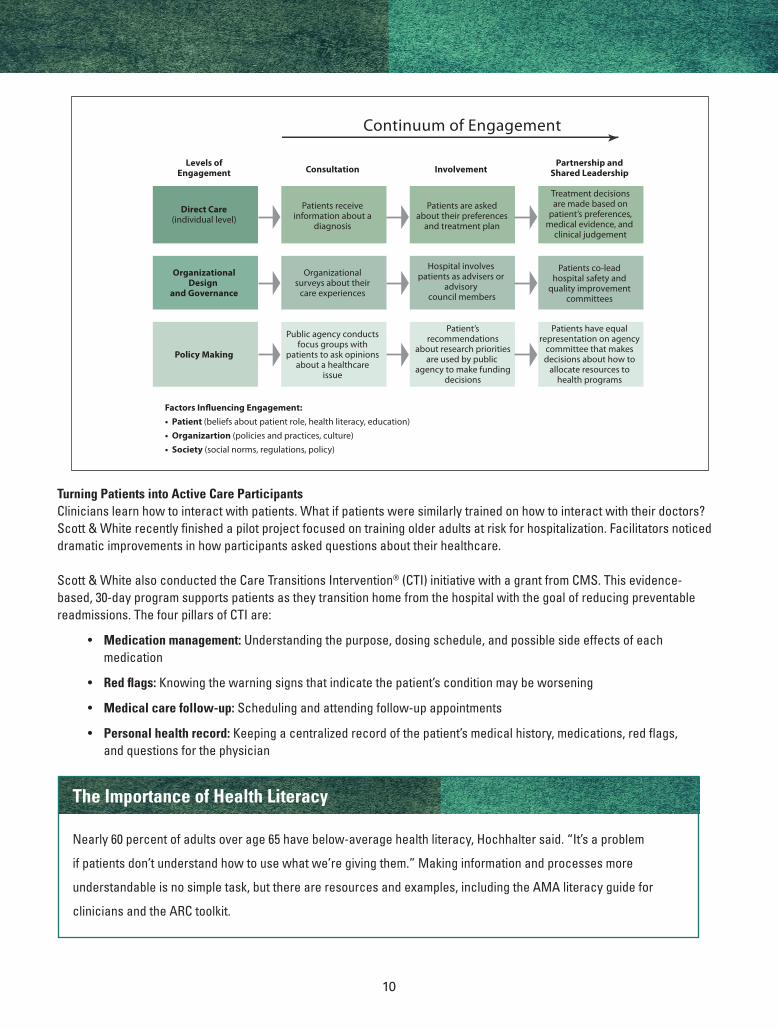
Understanding Patient Motivation Forahealthsystem,patientengagementoccursatthreeprimarylevels:directcare,organizationdesignandgovernance,andpolicymaking.Ateverypoint,engagementisinfluencedbysuchfactorsaspatientbeliefsabouthisorherrole,healthliteracyand education; an organization’s culture, policies and practices; and societal norms and regulations.
Patients are driven by different motivations, said Hochhalter. One size does not fit all, and the healthcare community needs to respond accordingly when trying to encourage patients to adopt these behaviors.
Hochhalter outlined the three major drivers of behavior that affect engagement for patients (as well as the clinicians who treatthem):
• Autonomy: The degree to which an individual has a say and is involved in decisions; the more autonomy people have, themorelikelytheywillbetotalkwithdoctorsandacceptservices
• Competence: Boththeabilitytoobtaincare/gettoappointmentsandtheperceivedabilitytomakechanges.
• Relatedness:Relationshipswithhealthcareproviders,thecommunity,andfamily,aswellastheinfluenceofothers
10
Continuum of Engagement
Direct Care(individual level)
OrganizationalDesign
and Governance
Levels ofEngagement
Patients receiveinformation about a
diagnosis
Organizationalsurveys about their
care experiences
Consultation
Factors In�uencing Engagement:• Patient (beliefs about patient role, health literacy, education)• Organizartion (policies and practices, culture)• Society (social norms, regulations, policy)
Patients are askedabout their preferences
and treatment plan
Hospital involves patients as advisers or
advisory council members
Involvement
Treatment decisionsare made based on
patient’s preferences,medical evidence, and
clinical judgement
Patients co-leadhospital safety and
quality improvementcommittees
Partnership andShared Leadership
Policy Making
Public agency conductsfocus groups with
patients to ask opinionsabout a healthcare
issue
Patient’srecommendations
about research prioritiesare used by public
agency to make fundingdecisions
Patients have equalrepresentation on agency
committee that makesdecisions about how to
allocate resources tohealth programs
The Importance of Health Literacy
Nearly 60 percent of adults over age 65 have below-average health literacy, Hochhalter said. “It’s a problem
ifpatientsdon’tunderstandhowtousewhatwe’regivingthem.”Makinginformationandprocessesmore
understandableisnosimpletask,butthereareresourcesandexamples,includingtheAMAliteracyguidefor
cliniciansandtheARCtoolkit.
Turning Patients into Active Care ParticipantsClinicianslearnhowtointeractwithpatients.Whatifpatientsweresimilarlytrainedonhowtointeractwiththeirdoctors?Scott&Whiterecentlyfinishedapilotprojectfocusedontrainingolderadultsatriskforhospitalization.Facilitatorsnoticeddramaticimprovementsinhowparticipantsaskedquestionsabouttheirhealthcare.
Scott&WhitealsoconductedtheCareTransitionsIntervention® (CTI) initiative with a grant from CMS. This evidence- based, 30-day program supports patients as they transition home from the hospital with the goal of reducing preventable readmissions.ThefourpillarsofCTIare:
• Medication management: Understanding the purpose, dosing schedule, and possible side effects of each medication
• Red flags: Knowing the warning signs that indicate the patient’s condition may be worsening
• Medical care follow-up: Scheduling and attending follow-up appointments
• Personal health record:Keepingacentralizedrecordofthepatient’smedicalhistory,medications,redflags, and questions for the physician
11
The intervention consists of a visit to the hospital room, one home visit, and two follow-up phone calls from a CTI coach. Only 28 percent of eligible cases enrolled, which Hochhalter attributed to the fact that many people don’t want home visits, especially after just leaving the hospital.
Don’t Forget to Track and Measure
Whoparticipated?Howweretheyengaged?Didphonecallsworkbetterthanpersonalvisits?Measurement
isvitaltoanyengagementinitiative.“Youcannotdoonethingandreacheveryone,”saidHochhalter.“Soyou
needtoconsistentlydeterminewhoacceptswhatyouoffer,whodoesn’tandwhy.”
To Incentivize or Not to Incentivize
Linkingincentivestoengagementisgainingpopularity.ButHochhalter,aself-described“incentivescynic,”believes
incentivesmaydomoreharmbypromotingextrinsicversusintrinsicmotivation.Whileincentivesworkwellforone-
time behavior, data shows they can negatively impact long-term motivation for both patients and physicians.
Reaching Out in New WaysManypeoplejustdon’ttrustthehealthcaresystem.ForthesekindsofpatientsScott&Whiteteamswithcommunitygroups.TheseincludetheNationalAgingServicesNetwork,whichoffershealthpromotionandself-managementclasses.
Scott&Whiteusescrowdsourcingtogetfeedbackonhospitalspendinginitiatives.Membersofthecommunityareinvitedto submit and vote for ideas online. Program leaders provide regular updates and maintain a dialogue with respondents. By submittingtheirideas,participantscanearnpointstoredeemforhealthycookingclass,lunchwithScott&White’sCEO,and other rewards.
12
Open Session: Priority Issues, “Crowdsourced” Answers
ThroughouttheACOCollaborative,peerexchangehasplayedanessentialroleinidentifyingareasofconcern,advancingbest practices, and delivering value. In this spirit, Penso facilitated an open session that gave participants the opportunity to air top challenges and find out what their peers were doing to address them in their own health systems. An audience poll identifiedtwopriorityareasfordiscussion:savingmoneyandsharingdatawithphysicians—whatdatashouldyouprovideandwhatshouldyouexpectphysicianstodowithit?
Collaborative thinking on saving money
• Focusonhealthcaremanagement,especiallyre-admissions
• Managethe“frequentflyers”(high-costpatients)
• Integratepartnerslikesocialworkersandskillednursingfacilitiesintocaredelivery
• Incorporatementalhealthintocare
• Whenworkingwithhospitals,honeinononeopportunityforsavings,e.g.,post-acutecare
• Lookforopportunitieswithpayers
• Leveragepastsuccessestoattractfuturepartners
Collaborative thinking on sharing data with physicians
• Beforesharingdata,firstbuildthegroundworkoftrust
• Makesuretheyfeelthattheirclinicalexpertiseisrespected
• Havetwo-wayconversationsabouttheirgoalsandtheresourcestheyneed
• Askforfeedbackwhenyouofferfeedback
• Beabletoshowthemwhat’sbehindthedata
• Workwiththemandmedicalsocietiestopickthemetricstotrack
• Makepatienttrackingasystem-widejob
• Understandandaccommodatefortheircultureofskepticism
13
CEO PerspectivesSpencer Berthelsen, MD, Chairman and Managing Director, Kelsey-Seybold Clinic; Stacey Hrountas, CEO, Sharp Rees-Stealy Medical Centers; Richard Fish, CEO, Brown & Toland Physicians
In this panel, leaders of three award-winning healthcare systems discussed their challenges and successes across a range oftopics,includingleadership,caredelivery,riskmanagement,IT,andpayerandpartnerrelationships.Thethreediversegroupsincluded:
• Kelsey-SeyboldClinic,amultispecialtyfor-profitpracticewith370physiciansacross20locationsintheHoustonarea
• SharpRees-StealyMedicalCenters,thelargesthealthcaresystemandprivateemployerinSanDiego
• Brown&Toland,amultispecialty,clinicallyintegratedindependentpracticeassociation(IPA)with500primarycarephysicians and 1,000 specialists across the Bay Area, as well as multiple hospital partners
Leadership Starts with EngagementKelsey-Seyboldisworkingtogetcurrentphysiciansinvestedintheprocessandhiringdoctorswhofitwillwiththegrouppractice culture. Its leaders are well compensated for time devoted to governance, and the very active and engaged operating board meets frequently and wields real control—contributing to all important or controversial clinical decisions. Berthelsendescribedhownewphysiciansmustbereadyforan“elbow-to-elbow”practiceandaproductivity-basedcompensation system.
Sharp-ReesStealylauncheditsACOinJanuaryof2012asacollaborativeeffort,leveragingtheAnthemACOmethodology.They created an interdisciplinary subcommittee structure and a governing body that included a consumer advocate and patientrepresentative.Hrountasnotedthattheprocessgoteasierovertime:“Wehadtopullandtughospitalsatfirst,butthentheywereeagertobeoncommittees.”
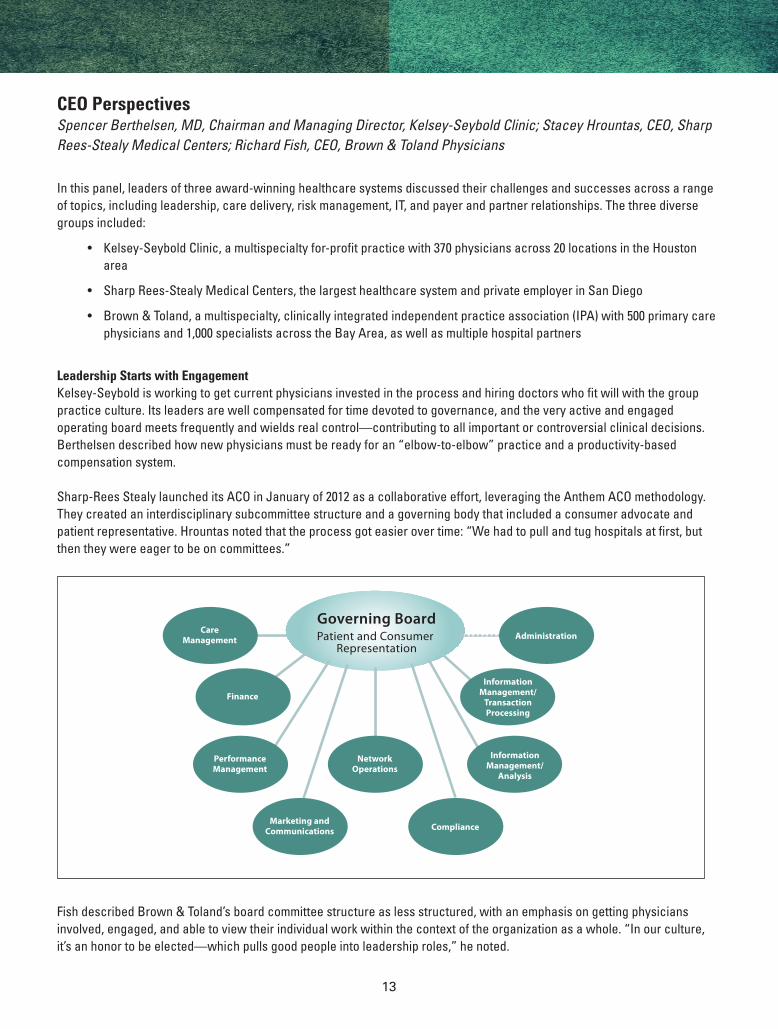
Fish described Brown & Toland’s board committee structure as less structured, with an emphasis on getting physicians involved,engaged,andabletoviewtheirindividualworkwithinthecontextoftheorganizationasawhole.“Inourculture,it’sanhonortobeelected—whichpullsgoodpeopleintoleadershiproles,”henoted.
Governing BoardPatient and Consumer
Representation
Expected Impact Time to Impact
CareManagement Administration
Finance
InformationManagement/
TransactionProcessing
PerformanceManagement
InformationManagement/
Analysis
NetworkOperations
Marketing andCommunications Compliance
14
Multiple Aspects of Care DeliveryHrountascommentedonhowSharp-ReesStealyengagedpatientsintheprocessviawebsites,hotlines,andothercommunicationsandlookedforefficiencieseverywhere—fromusingpharmacystudentstostreamlinetherefillprocess to dabbling in telemedicine.
Fish discussed how Brown & Toland applied medical management programs initially developed for HMOs and fee-for-service patientpopulationstowardTripleAimgoals:
• Improvingthepatientexperience
• Improvingthehealthofthepatientpopulation
• Reducingthecostofcarebyimprovingqualityandefficiency
Berthelsen touched on how important brand image has been to Kelsey-Seybold—a multi-year investment that communicates theorganization’scommitmenttocarethroughdetailslikeanidentifiablesetofbuildings.
The Tactical and Cultural Aspects of Risk ManagementHrountasnotedthatSharp-ReesStealyhasbeendoingrisk-basedcontractsforseveraldecades,describingitasaculturewith years of evolution and 25 years under population-based payments.
AccordingtoBerthelsen,thewillingnesstoacceptandmanagetotalcostriskhasbeenakeystrategyatKelsey-Seybold:“Webehaveandoperateasifwewereatriskfor100percent.”
Brown&Tolandhasbeentakingresponsibilityforalltheproductsitsupportsbyputtinginmorecasemanagersand addressingtheneedsofmoderate-tohigh-riskpatientsburdenedbyacuteillness,chronicconditions,age,orself-caredeficits.
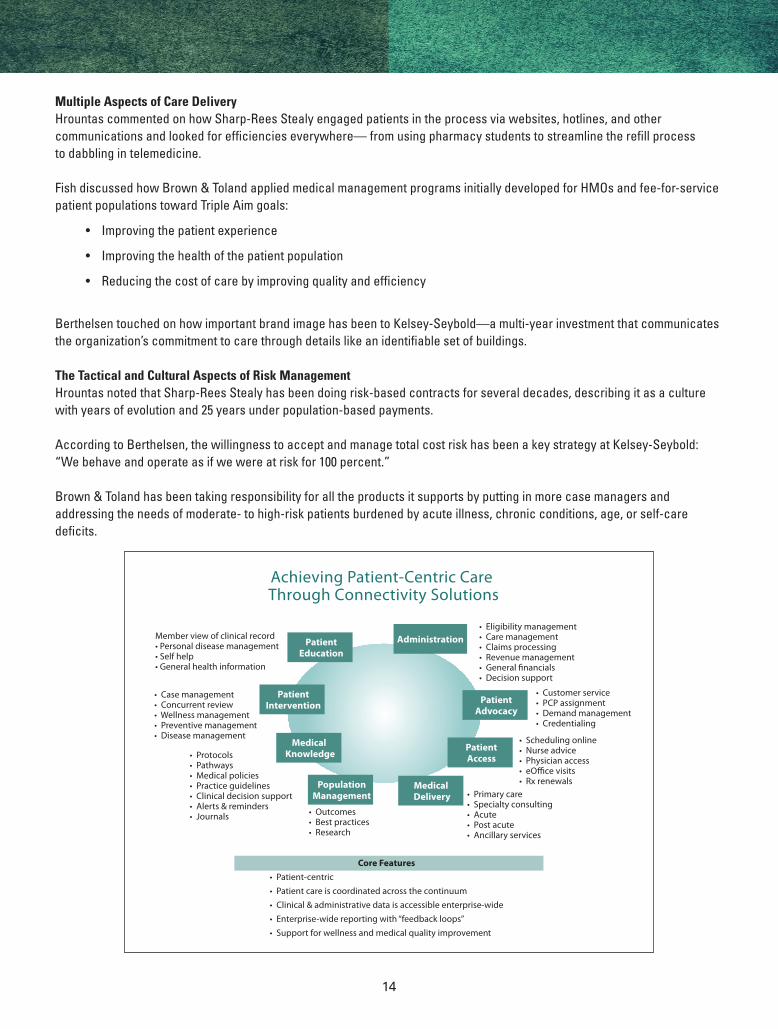
Achieving Patient-Centric Care Through Connectivity Solutions
Expected Impact Time to ImpactMember view of clinical record• Personal disease management• Self help• General health information
• Eligibility management• Care management• Claims processing• Revenue management• General financials• Decision support
• Customer service• PCP assignment• Demand management• Credentialing
• Scheduling online• Nurse advice• Physician access• eO�ce visits• Rx renewals
• Primary care• Specialty consulting• Acute• Post acute• Ancillary services
• Outcomes• Best practices• Research
• Case management• Concurrent review• Wellness management• Preventive management• Disease management
• Protocols• Pathways• Medical policies• Practice guidelines• Clinical decision support• Alerts & reminders• Journals
Core Features• Patient-centric• Patient care is coordinated across the continuum• Clinical & administrative data is accessible enterprise-wide• Enterprise-wide reporting with “feedback loops”• Support for wellness and medical quality improvement
PatientEducation
Administration
PatientAdvocacy
PatientAccess
Medical Delivery
PatientIntervention
Medical Knowledge
PopulationManagement
15
Technology’s Vital RoleKelsey-Seyboldhasmade$38millioninITinvestmentsoverfiveyearstomonitordollarsflowingthroughthesystem. Sharp-ReesStealyusedITresourcestoguidetheACO’simplementationplan.Forinstance,a2011claimsanalysisidentifiedkeyopportunitiesforimprovement—skillednursingbeddayswere42percenthigherthanbenchmarksandjust3.5percentofbeneficiaries were generating 21 percent of Part A paid claims.
Fish reported how Brown & Toland’s more distributed model lends itself to technology platforms and e-tools for integrating caremanagement,clinicalcareprograms,andfinancialincentiveprogramsforitsnetworkphysicians.
Partner and Provider RelationshipsAtKelsey-Seybold,Berthelsencited,“averydisciplinedapproachtocontractingwithpayersthatrequiresknowingyourvalueanddelta,leveragingthatdeltaintodollarsandaverycourageousboard.”
Fish related how Brown & Toland started out as a clinically integrated IPA to support physicians, with PPOs contracting acrossthenetwork.Theywereuniqueinthecountryatthetime,anditwashardworkingwithpayers.Today,theorganizationlists partnerships with Cigna, Aetna, and Blue Shield/City and County of San Francisco among its accountable care initiatives. Prioritiesincludeputtingclaimsandclinicaldatatoworktowardpatientcareandworkingtokeeprateincreasesincheck.
“Inorderforustoplaywithyou,youhavetodevelopproductsthatcreateincentivesforpatientstowanttogotoanACO,”said Hrountas.
Collaborative ThinkingQ: For complex, high-risk patients, what interventions lowered the cost of care?A: According to Berthelsen, Kelsey-Seybold has leveraged palliative care, pharmacy management, and home care and emphasizedgettingpatientsintothesystemandtotherightdoctor.“It’shardworkeveryday.It’salsoaboutavoidingcatastrophes,avoidingsurgeryiftheywon’tdowell,andtryingtoavoidmakingthingsworse.”
Fishrespondedthatinhisexperience,gettingpatientstobemoreinterestedintheirownhealthmanagementandmakingthoseeffortsscalablehasbeencrucial.HedescribedhowRNssupportedtheselessstablepopulationsinthepast.TodayoneRNoverseesateamof10healthcoaches—allfocusedonearlierinterventions.
16
Perspectives on Care Coordination Frederick Bloom, MD, MMM, Chief, Care Continuum, Geisinger Health System; Julie Day, MD, Quality Medical Director, University of Utah Community Clinics; Betty Shephard, RN, BSN, MBA, Lead Vice President of Care Management, Davita HealthCare Partners
Threehealthsystemsatdifferentphasesofthecarecoordinationprocessdiscussedactionstaken,resultsachieved,andlessons learned.
Geisinger Health System: A Mature Program Geisinger made case management an early focus and an important part of the overall PCMH model. Bloom cited primary care design, team-based delivery of care, medical neighborhood, quality outcomes, and value-based reimbursements as the corecomponentsoftheGeisingermodel—allwithanemphasisonROI.
Geisingerredesignedworkflowto:
• Eliminateworkwithoutaddedvalue
• Automatetasksthatcouldbedonebyacomputeroroutsideoftheoffice
• Delegateofficevisittaskstotrainednon-physicianstaffwhenpossible
• IncorporatenewworkflowsintotheproviderpracticewithremindersandEHRtools
• UseEHRtoolstoengageandmotivatethepatientwhenpossible
ByMarch2012,Geisingerhadachieveda7percentreductionincosts―balancedbyadditionalexpensesforcasemanagersandinfrastructure―thatrepresentedapproximately$2insavingsforeach$1invested.Analysisalsoidentifiedthepreventionof140strokesand165casesofretinopathy.
BloomattributedGeisinger’ssuccessto:
• Activated,engagedprovidersandcasemanagerstrainedinfulldiseasemanagement,includingtransitions,escalations, telemonitoring, and pharmacy management
• Professionalsworkingatthetopoftheirlicenses
• Afocusonpost-dischargetransitions
• Casemanagersembeddedattheprimarycaresitetosupportproactivecare
• Closefollow-upwithpatientswithcomplexconditions
• Useofinteractivevoicerecognitiontoolstoengagelow-riskpatients
• Relationshipswithcommunitypartnerslikenursinghomesandhomehealthagencies
17
University of Utah Health Clinics: The Creation and Development StageInJanuary2013,UUHC’sfullcapitationcontractstartedandthesystemassumedriskfor43,000Medicaidlivesand7,000employees.Itwas“awake-up,”Daysaid.
UUHC’scurrentmodelisfocusedontransitionsmanagement,medicationreconciliation,andhigh-riskpatients.Keyactivitieshaveincluded:
• Trainingcasemanagersheavilyinmotivationalinterviewingandbehavioralchange
• Establishingbaselinesandtrackingimprovementsinareasrangingfromdepressiontoqualityoflife
• Investingintransitionsmanagement,suchasstaffinga“transitionnavigator”tosupportfollow-throughfor complexcases.
According to Day, providing patients with support when they’re being discharged from the hospital has reduced noncomplianceby50percent.“Onephonecallcanbethematteroflifeordeath.”
Moving forward, UUHC aims to reduce emergency room visits, preventable hospitalizations, and hospital readmissions while improving quality scores and total cost of care savings.
Davita HealthCare Partners: Undergoing Continual ReinventionDavitahasrevitalizeditscoordinatedcareprogramthrough:
• Accountability:Eachteammemberisaccountabletoaspecificpopulation.
• Scalability:Thesystemflexiblyadaptstomeetmarketneedsandadaptableforallproducts:HMO,PPO,DualEligible,andACO.
• Affordability:Teammembersworkatthetopoftheirlicenses.
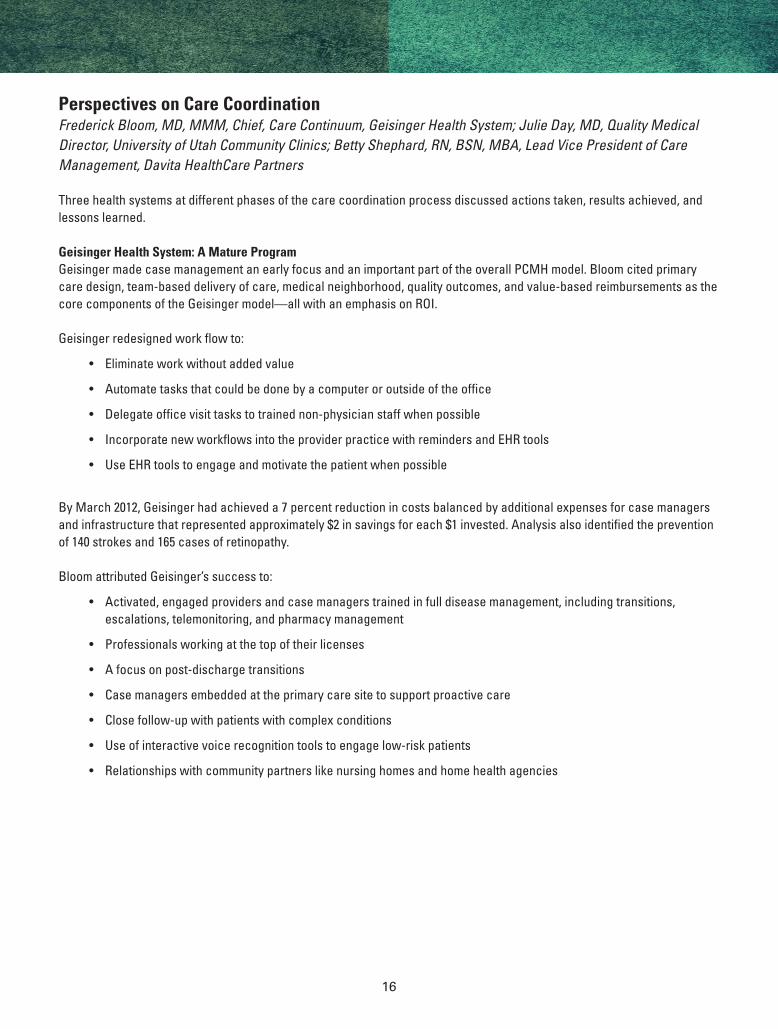
E�ective Redesign and Care CoordinationDelivers Rapid Impact
Activity Expected Impact Time to Impact
Transitions of Care Management
Case Management for Other High-Risk Patients
Pharmacy management
Case Management for High-Risk Patientswith Target Conditions: DM, HF, COPD
Reduce Readmissions
Reduce Primary Admissions & ED
Increase Generic Use
Reduce Primary Admissions & ED
3 Months
6-12 Months
6-12 Months
3-6 Months
Short-term e�ects
Nursing Home Management
High End Imaging
More E�cient Specialists andAncillary Providers
Reduce Readmissions / Primary Admissions
Reduce Unnecessary Testing
Decrease Cost per Episode of Care
12-18 Months
12-18 Months
12-18 Months
Mid-term e�ects
Interventions for Low-Risk Chronic DiseasePatients: Disease Registries;
Chronic Disease Care Optimization
Preventive Care; Screening; Lifestyle Change; Wellness
Improved Control; Avoid Complications
Earlier Identi�cation & Treatment;Decrease Incidence of Chronic Diseases
2-5 years
2-5 + Years
Mid-term e�ects
18
Basedonexperiencessofar,whatwouldShephardtellotherhealthcaresystemsinsimilarcircumstances?Relyon expertsforbuildingareasofexpertise;don’ttrytodevelopthingsonyourown.Conductalotofcasereviews.CapitalizeonITtools—exception-basedmonitoringviainteractivevoiceresponse(IVR)tools,forinstance.Andrecognizethatteamworkdoesn’tjusthappen.Trainallmembersofyourteam.Web-basedseminarscanbeeffectiveifyoudon’thavetheresourcesfor in-person training.
Astheprogrammovesforward,Davitaisfocusingon:
• Nurseandcliniciantraining
• Moreeffectivelymatchinginterventionstopatients
• Leveragingtechnologytoreduceface-to-facevisits,monitorloweracuitypatientsandtrainstaff
Collaborative Thinking Q: When one care manager is working with 150 patients, how long should patients stay in care management? A:Bloomnotedthatit’simportanttomakesurethatpatientsfalloffofacaseloadastheygraduate/stabilizeandare re-activatediftheyfallintotrouble.HisteamfollowsCOPDandCHFpatientslong-termwithcheck-inslikemonthlyphonecalls.Providerscanusenon-medicalstaff,ratherthanRNs,forsomephonecallsandadministrativetasks.DaynotedthatUUHChasbeenusingIVRsforsomeofitsfollow-up.
Q: How do you manage case managers? Do you have systems to track their work? A:AnRNoverseescasemanagersatUUHC.AtGeisinger,caremanagersareemployedbythehealthplan,andEpicEMRisusedfordocumentation.DavitausesAllScriptstotrackencountersandrunreports,“soweunderstandwho’stouchingpatientsandwho’shavinganimpact.”
Q: How do you prepare practices for embedded care managers?A:Bloomsaiditcantakeupto12monthsforapracticetoreallygetusedtoacaremanager.“Youhaveawinwhenthecasemanagermakeseveryone’sdaygobetter.”
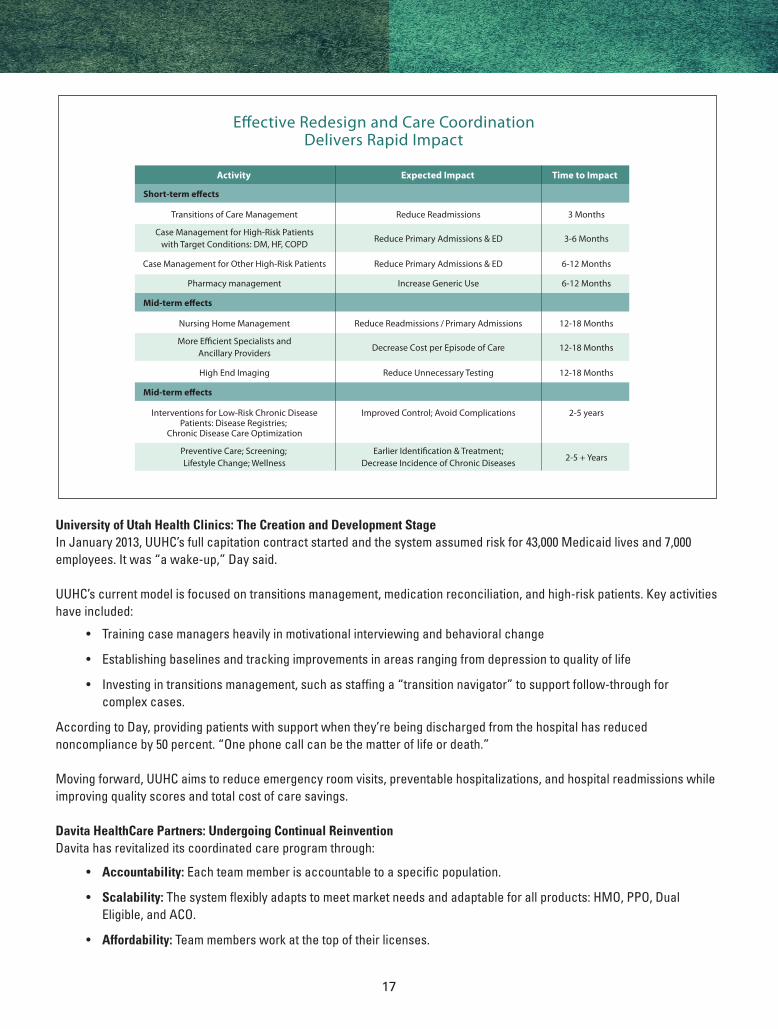
New Care Delivery Team
• Leverage PCP
• Improve e�ciencies
• Maximize team performance
• Create team alignment
• Deliver patient- focused care
PCP
Patient
SocialWorker
CareManager
Care TeamSupervisor
PatientCoach
Care TeamMember
19
Breakout Sessions: Perspectives from the FieldFromgettingstartedtotacklingreadmissionstointegratinghealthcoachesintocareteams,leadersofthesethreesessionssharedfirsthandlessonsfromtheirACOexperiences.
Triad HealthCare NetworkSteve Neorr, VP/Executive Director, Cone Health; William Hensel, MD, Operating Committee
JustasitsNorthCarolinacommunityadaptedtoprofoundchangesinthetextileindustrydecadesbefore,TriadHealthcarehasbeenadaptingtoprofoundchangesinthemedicalcommunity.AccordingtoHensel,“Wehavenotbeenonthecuttingedgeofchangeinourorganizationuntilthelastcoupleofyears.”
Andtheorganizationhasexperiencedtransformativechangeeversince.Itbeganwiththecreationofa20-member,physician-led steering committee in fall 2010, engaged independent and employed physicians with Cone Health over the nexteightmonths,andofficiallybecametheclinicallyintegratedTriadHealthcareNetworkin2011.
Workhasinvolved:
• Developing a structure:“Weneededtogetprimarycareandspecialiststoworktogether.Wedidn’twantprivatepracticeandemployeddoctorsbuttingheads,”saidHensell.Butmostimportantly,theyneededtodecidewhomtoinvite to the table in terms of collecting data and dividing money.
• Engaging physicians:Howdoyougetdoctorstothis“newreligionofvalue-basedreform”—especiallymembersofthepreviousgroup’smedicalexecutivecommittee?Gettheminvolvedthroughleadershipinitiativeslikeaqualitycommittee.
• Transforming the delivery of care: A multifaceted mission, efforts here included creating a care management team to support physician practices, redesigning the care process, achieving PCMH recognition, and deploying IT systems for population management.
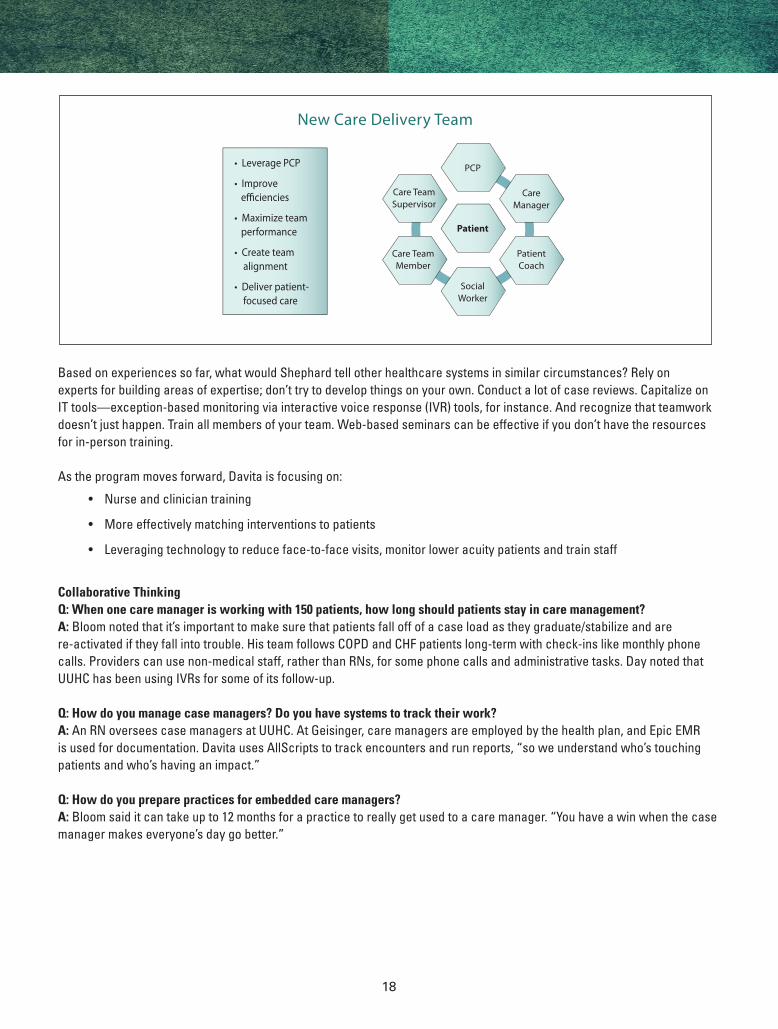
“Wehadtodecidewithlimitedresourceswheretofocusourefforts,”saidNeorr,addingthatITresourcesdriveeverything.
Triad HealthCare NetworkThe challenge of aggregating data in a community
EMPI
LabCorp
Quest
Solastas
GSORadiology/Canopy
EMREMR
Wellogic HIE(Amazon Cloud)
Primary CareProviders
EPIC
Hospitals
Claims System
Payers(CMS to begin with)
CINA Edge Serverat Practice
Specialist Providers& Providers not in
CINA
HIECDR Portal
CT
Optum Care Suite
(Hosted at Optum)
IP II
THN Server(CINA Datamart)
AggregateClinical
CDR
PracticeCDR
ClaimsCDR
PracticeCare Mgr
User
Providerswith no
EMR
ADT & Clinicals
HL7.CSV /MLLP. SFTP.WS
Clinicals /ProceduresODBC / SQL
Direct
POC ReportFop Mgmt
Performance
Clinicals: Encounter, Vitals Problems, Meds, Alergies,
Immunization, Procedures,Social History,Family History
RiskStrati�cation
DB Replication
User AccessPopulation
Reports
Payer Data(Future)
CSV / SFTP
EMFIADT, SUI,
ORU, ORMHL7/MLLP ADT
(AD1-AD8)HL7/MLLP
IncrementalClinical Data
(Care PlanPDF)
(POC RecordsPDF)
Claims DataCSV / SFTP
CliniciansCSV / SFTP
EMPICSV / SFTP
Provider Portal
EMREMR Lite
THNCare Mgr
User
THNQuality
HL7/MLLP
HL7/WS
HL7/MLLP
HL7/MLLP

20
Summit Health SolutionsRobert Kolock, MD, Medical Director
SummitstarteditsACOjourneyinJuly2012withcarecoordinationasacentralfocus.OnekeyinitiativewastheSummitTransitionandReadmissionProgram,whichinitiallyfocusedonCOPDandheartfailurepatients.Hospitalssentdailyfeedsof patient lists and treatment plans to care coordinators, who reached out to patients with information about post-discharge medicationusage,follow-upappointments,andself-care.Eightypercentwerecontactedwithintwodaysofleavingthehospital.
“Tacklingreadmissionfirstmakessense—yougetthebiggestbangforyourbuck,”saidKolock.“Hospitalsshouldbepartnersonthis,sincethey’relosingmoneyaswelliftheycan’tgettheirnumbersdown.”
Forothercaremanagementapproachesandtactics,participantssharedideasandexamplesfromtheirownhealthsystems,including:
• Embeddingcaremanagersinclinics,suchasRNs,MAs,socialworkers,andhealtheducators
• Trainingcommunityhealthworkerstoserveashealthcoachesinareassuchashomevisitsandhelpingunderserved populations navigate the system
• EngagingMAs,LPNs,andparamedicsfortakingpatientshomeandconductingassessments
• Tappingpharmacistsandpharmacystudentstohelpwithmedication-relatedrecommendationsandtasksasappropriate
Toward PCMH Value-Based Model
Old Fee for ServiceModel
Volume-BasedModel
Patient-CenteredPhysician-
Directed Care (Medical
Home)
Value-BasedModel
DataAnalysis
& Sharing
CareCoordination
Patient Education
MedicalNeighborhood
Care Management
Physician/Patient
21
Mercy ClinicsDavid Swieskowski, MD, MBA, CEO, Mercy ACO; Senior Vice President and Chief Accountable Care Officer, Mercy Medical Center, Des Moines
MercyMedicalCenter’s$1.7millioninvestmentinhealthcoachesrepresentsoneofitsbiggestexpenditures—andpotentially most versatile resources. Staffed at a ratio of 1 for every 2,000 ACO patients, these professionals are responsiblefor:
• Interviewingpatientsabouttheirmotivationsand goals
• Coordinatingcare
• Servingasanaccesspointforpatientsandfamilies (via phone and e-mail)
• Connectingpatientstocommunityresources
• Distributingdecisionaids
• Supportingpatientself-managementactivities
• Closingthelooponreferralsandtransitions
• Managinghigh-riskpatientcases
• Servingasapointpersonfortheintroduction of new care processes
• Reviewingpopulationdataforinterventionopportunities
Participants had many questions about the program.
Q. How do you know what your health coaches are doing?A.Mercyisputtinginsoftwaretotrackandmanagetheseactivities.It’spartofanoverallefforttoputcaremanagementprotocols into an electronic format so it can be standardized and capture information such as language preferences and community resources.
Q: Every clinic wants coaches, yet no department wants them on its budget. Where do you put them?A: Eachclinichiresitsownhealthcoach.Tolowerresistance,Mercywasabletodemonstratethathealthcoacheshavethepotential to generate ancillary revenue far greater than their salaries.
Q: Are coaches incentivized?A: All Mercy employees are incentivized under the same program of shared metrics.
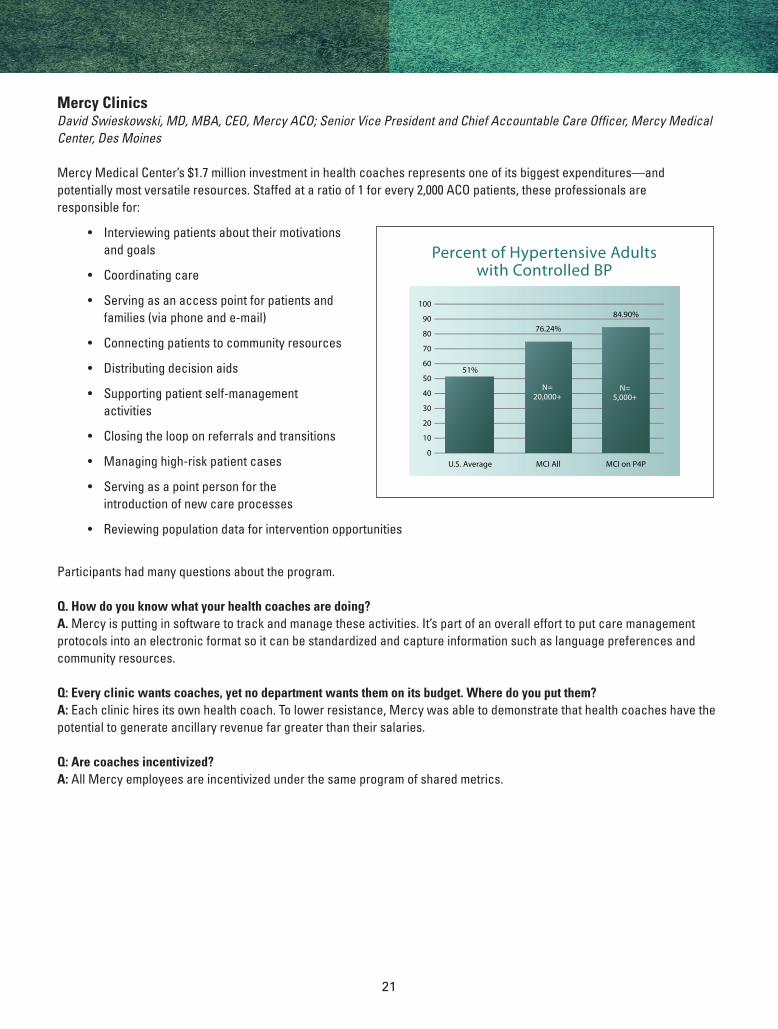
N=5,000+
N=20,000+
Percent of Hypertensive Adultswith Controlled BP
U.S. Average
51%
MCI All
76.24%
MCI on P4P
84.90%
22
Insights from Other Collaboratives: PACT and the Dartmouth-Brookings ACO Learning NetworkJoe Damore, Vice President, Engagement and Delivery, Premier Healthcare Alliance; Greg Kotzbauer, Project Manager, Health Policy and ACO, The Dartmouth Institute
Hosted by Premier Healthcare Alliance, the PACT Population Health Collaborative helps members navigate the shift toward populationhealthinpublicandprivatemarkets.Thisincludespopulationhealthassessmenttoolstouseinareaslikereadinessandbundledpayment.Whenitcomestimeformemberstoimplementprograms,PACTprovidestemplatestoreduce time and effort and metrics to assist with performance improvement.
Membersmeetinsummitsandideaexchanges.Organizationsoffertheirownspecializedon-sitetrainingsessions.Andateamofcontentexperts,frompayernegotiationtocaremanagement,isavailabletomembersanytime.Foruppermemberlevels,sharedlearningshoneinonspecificissueslikediabeticcaremanagementandnewrevenueopportunitiesinsmallergroup settings.
TheDartmouth-BrookingsACOLearningNetworkprovidesbestpracticesandtoolsformedicalgroupsplanningandimplementing accountable care reforms. Its purpose, according to Kotzbauer, is to translate strategy into operational goals andhavingaplanformovingforward.“Wespecializeinaskingquestions,”saidKotzbauer.“Andtoavoidpushinganysortofagenda,ourmember-drivennetworksimplybringslike-mindedpeopletogethertomovetowardacommongoal.”
Monthlycalls,informalworkgroups,andconferencesconnectmemberswithoutsideexperts.Thenetworkalsoworkswithhealthsystemstobuildbasictools.Theseincludeaself-assessmentthathelpsusersmeasureproficiencylevelsforkeyclinical transformations and then identify methods for improving them.
DamoreandKotzbauersharedobservationsandinsightsgainedthroughtheircollaboratives’work.
Achieving Cost SavingsCost savings is on everyone’s mind, Damore said. How can we do these reforms and save money?
Basedonwhathe’sseeninthePACTcollaborative,Damoresuggestedfocusingon:
• High-riskpopulations,especiallytothetop1to2percent
• Chronicdisease,includingasthma,diabetes,andchronicdepression.
• ByfocusingonPCMHandreplacingmoreexpensivelocationswithlesscostlyones,healthsystemscanreducecare management costs by up to 8 percent
• Bettertransitionsofcare—forinstance,bettermanagementofthedischargeprocess
• Reformingpharmaceuticalcostsandusage
Opportunity also can be found in intensive care. One PACT participant hosted a special site visit for peers that highlighted its sixyearsofICUoutpatientexperience.Theorganizationshareditslessonslearnedandimpressiveresults,whichincludeda12 percent reduction in costs, dramatic quality improvements, and increased patient satisfaction.
Managing Population Health Populationhealthstartswithknowingyourpatientpopulationanditsneeds,saidKotzbauer.Doyouhavetherightleadership,staff,andcommunityprogramsinplace?Whataboutyourprocessesandtools?Andhowdotheseprocessesandtoolsinfluenceinteractionsanddecisions?
23
According to Damore, who has conducted many of PACT’s assessments in the area of population health, organizations need arobustprimarycarenetwork—forattributionandmanyotherreasons.APCMHalsocanbehelpful.Othercrucialelementstopopulationhealthmanagementinclude:
• Transitionsthatarephysician-ledandprofessionallymanaged
• Caremanagementprograms(centralizedordecentralized)
• Chronicdiseasemanagement,especiallyforthe“bigsix”conditions
• Populationhealthanalytics,includinghistoricclaimsandpredictivemodeling
• Aclinicallyintegratednetworkforsharedsavings
• Alignedpayerarrangements
Alsoimportant,“Getpatientstounderstandthattheyhaveskininthegame,thathealthcareisnotjustaboutustakingcareofyou,”Kotzbauersaid.“Providepatientswiththetoolssotheyaremoreempowered.”
Navigating Medicare Shared SavingsTheCMSMedicareSharedSavingsprogramisonewayahealthsystemcanbecomeanACO.PACTfieldexpertstookasmallgroupofparticipantsinterestedinthismodelthrougha10-weekprocessthatinvolvedimplementationsupportandone-on-onedevelopmentandguidance.Regularmeetingsinvolvedsharingbestpractices,contractingtemplates,sharedsavings models, public policy considerations, and more.
How do we get specialists engaged? Should we try building incentives for certain specialty areas? How do we embed care managers and navigators into practices and patient-centered medical homes?
PACTparticipantsfacedthesequestions,aswellaschallengesintheareasof:
• Beneficiarynotificationandcommunication
• Newphysicianrecruitment
• Physicianengagementandeducation
• Timelyandaccuratecollectionsofclaimsdata
• Implementationofpopulationanalytics
Many Models, Common Needs“Systems are dipping their toes into value-based delivery—and some systems are doing this without calling themselves ACOs,”Kotzbauersaid.
Whateverthemodel,“weneedtoidentifyhoweverythingcomestogether,inordertoprovidepatientswithnomoreandnolessthanwhattheyneed,”saidKotzbauer.“Understandtheimportanceofpatientexperienceandcliniciansatisfaction,andassignpatientstotherightproviders.”
24
The Anceta Collaborative: Leveraging Data for Operations, Patients, and PopulationsJohn Cuddeback, MD, PhD, CMIO, Anceta
Data-drivencollaborationisthepremisebehindAMGA’sAncetadatawarehousecollaborative.Throughworkingwithdetailed,disease-specificmodels,participantsareabletobenchmarktheiroperationsandidentifyopportunitiesforimprovement.Ancetahelpsparticipantsgaindata-driveninsightinto:
• Thequalityandcostoftheircaredelivery
• Interventionsforhigh-risk,high-costpatientgroups
• Referralpatterns
• Operationalefficiencies
New DevelopmentsOptumInsight’searly2013acquisitionofHumedicamakesAncetatheonlysystemintheindustrycapableofintegratingclinicalandadministrativedata—anddelivering“applestoapples”comparisonsacrossits25health-systemparticipants.AMGAisexpandingthescopeoftheAncetacollaborativetoincludesevendiseasemodels,populationmanagement,andadashboard.
Shared ChallengesAncetaparticipantsworktogethertosharebestpracticesandfindwaystoachievefavorableoutcomesatthelowestcosts.Currentchallengesinclude:
• Integratingoperationswhentwoorganizationswithdifferentsystemsmerge
• Decidingwhethertogowith“bestofbreed”or“monolithic”technology
• Supportinganintegratedcaredeliveryprocessacrossareassuchasambulatorycare,acutecare,andcommunityresources
• Attributingpatientsacrossorganizationsandcareteams
• Reportingtoexternalpartners
• Gettingacompletepictureofthetotalcostofcare,includingclaimsforservicesfromotherproviders
Analyzing CostsThrough technology and shared learning, Anceta is helping participants find answers. In the area of cost accounting, users canlookatexpensesperunit,comparecostsagainstutilizationandgeta“realcost”viewoftheworld.Itenablesmodel-ingforbundledandothercontracts,statisticalriskadjustments,andthecreationofresourceprofiles,whichcanbeusedtocreate standardized costs.
Allocating ResourcesForintegratingcaredelivery,Ancetacanbeusedtoguideresourceallocation—particularlyinopportunityareaslikeprimaryandambulatorycare—andmapprocessflow.Who’stherightpersontotalktoapatient?What’sthebestnextstepin the process?
Whendeliveringpatientcareitself,youneedtolookatoutcomemetricsaswellasprocessmetrics,Cuddebackadvised—thingslikeapatient’sfunctionalstatusandmentalhealthstatus.Inonementalhealthusecase,hesaid,doctorswereabletoidentifyseveredepressionasakeyfactorinpatienthealth,eventhoughitwasn’tpartoftheiroriginaldiscussiondialogue.
25
Insight without the WaitModeling and analytics tools also give medical groups the ability to focus in on correlations and variations without having to wait for the outcomes of controlled studies. Providers can analyze readmissions data to predict future emergency room visitsforcongestiveheartfailurepatients.OrtheycanbreakoutacohortinapharmacystudybydrugclassorBMI—forinstance, to test the relationship between insulin treatment and weight gain.
“Itchallengestherationalespeoplehaveintheirheadsforthingslikedrugchoice,”saidCuddeback.
Support for Population HealthAspopulationhealthbecomesagrowingfocusforACOs,Cuddebackanticipatesagrowingdemandforintermediate-levelpopulationmanagement—theprocessesforextractingandloadingdatawhenanalyzingitatthepatientandpopulationlevels.
Whatprocessesworkbestforgettingdatainandoutofsystems?Howcantheseprocessesbemosteffectivelyimplemented? Anceta participants will grapple with these and other questions.
Meanwhile,needalsoexistsforviewingprocessexecutionandimprovements.Thisincludes:
• Providerperformancereports
• Patientregistryforoutreachandcarecoordination
• Comparativedatalinkingprocesstooutcomes
For information about the Anceta collaborative, visit www.anceta.com/join.htm.
“A window has opened for providers of care to take the initiative to prove that lower cost and higher quality are not only compatible, but strongly linked. But the window will not stay open for long if results are not forthcoming. American healthcare providers face an opportunity and a test — now.”
—DonaldBerwick,MD,MPP,CMSAdministrator2010-2011
26
AbbVieCarolO’Brien,Esq.,Director,PublicPolicy
Austin Diagnostic ClinicGhassanSalman,MD,MPH,FACP,ChiefExecutiveOfficer
Billings ClinicNicholasWolter,MD,ChiefExecutiveOfficer,BillingsClinic
Brown & Toland PhysiciansRichardFish,ChiefExecutiveOfficer
Daiichi-Sankyo, Inc.VinilChokshi,OrganizedCareMangaerEyadMatar,RegionalAccountManagerPeteOlsen,AreaDirector,WestRegion–ValueSelling
The Dartmouth InstituteGreg Kotzbauer, Project Manager, Health Policy and ACO
Geisinger Health SystemFrederickJ.BloomJr.,MD,MMM,Chief,CareContinuum
HealthCare PartnersBettyShephard,RN,BSN,MBA,LeadVicePresidentofCare
Management
Kelsey-Seybold ClinicSpencer Berthelsen, MD, Chairman and Managing Director
Mankato Clinic, Ltd.LaurieDahl,DirectorofClinicalOperationsRandyFarrow,ChiefExecutiveOfficerJulie Gerndt, MD, Chief Medical OfficerSteveHatkin,ChiefFinancialOfficer
Mercy ClinicsDavidSwieskowski,MD,MBA,ChiefExecutiveOfficer,Mercy
ACO;SeniorVicePresidentandChiefAccountableCareOfficer, Mercy Medical Center, Des Moines
Ohio Health GroupStephen Cardamone, DO, MS, Chief Clinical Integration OfficerLouImbrogno,ChiefExecutiveOfficer
Ortho-McNeilLarryWestfall,PharmD,NationalDirector,StrategicAlliances
Park Nicollet Health ServicesMeganCox,Director,PioneerACOandMedicareProducts,
Office of Population HealthSamVanNorman,MBA,CPHQ,Co-Chair,OfficeofPopulation
Health, and Director, Business Intelligence
The PolyClinicPhilLillich,RN,BSN,MBA,ManagerCareManagement
Services
Premier Healthcare AllianceJoeDamore,FACHE,VicePresident,EngagementandDelivery
Scott and White HealthcareAngieHochhalter,PhD,ResearchScientist,SystemQuality&
Safety
Sharp Rees-Stealy Medical CentersStaceyHrountas,ChiefExecutiveOfficer
Summit Health SolutionsRobertKolock,MD,MedicalDirector
Triad HealthCare Network / Cone HealthWilliamHensel,MD,Physician,OperatingCommitteeMemberSteveNeorr,ExecutiveDirector/VicePresident
Union Associated PhysiciansHans Andreason, MD, Chair of the Board
University of Utah Community ClinicsJulie Day, MD, Quality Medical DirectorAnnieSheetsMervis,MSW,QualityManagerSusan Terry, MD, FACP, Medical DirectorVickiWilson,DirectoroftheUniversityofUtahHealthPlan
From AMGAJohnCuddeback,MD,PhD,ChiefMedicalInformaticsOfficer,
AncetaDanielle Casanova, Director, Quality InitiativesJoyce Jones, Quality Program CoordinatorSamuelLin,MD.,PhD,MBA,ConsultantforMedicalAffairsJerry Penso, MD, MBA, Chief Medical and Quality Officer
Collaborative Member Participants
27
ONE PRINCE STREET, ALEXANDRIA, VIRGINIA 22314-3318
TEL: (703) 838-0033 FAX: (703) 548-1890 WWW.AMGA.ORG
© 2013 American Medical Group Association.All rights reserved
AMGA ACO Initiative Sponsors