Embed Size (px)
Citation preview
Acquired and Primary
Immunodeficiencies
Cheryl Pikora MD, PhDUniv of Mass Medical School
Outline
Brief overview of causes of acquired immunodeficiencies
Brief discussion of the components of innate and adaptive immunity
Clinical presentations of primary immunodeficiencies
Discussion of pediatric HIV prevention, diagnosis and treatment
Acquired immunodeficiencies
Chemotherapy Breakdown in integumentary barriers Altered microbial colonization Enhanced susceptibility to infection
Neutrophils* T lymphocytes* B lymphocytes* NK cells Peripheral blood monocytes* Fixed-tissue macrophages
Acquired immunodeficiencies
Immunosuppressive drugs Corticosteroids Anti-rejection agents Monoclonal antibodies
Immunomodulatory infections HIV TB Malaria EBV, CMV
Primary Immunodeficiencies: Genetic
Neutrophil function defect
Complement deficiency
B cell deficiency
Specific immunoglobulin deficiency
T cell deficiencies (SCID)
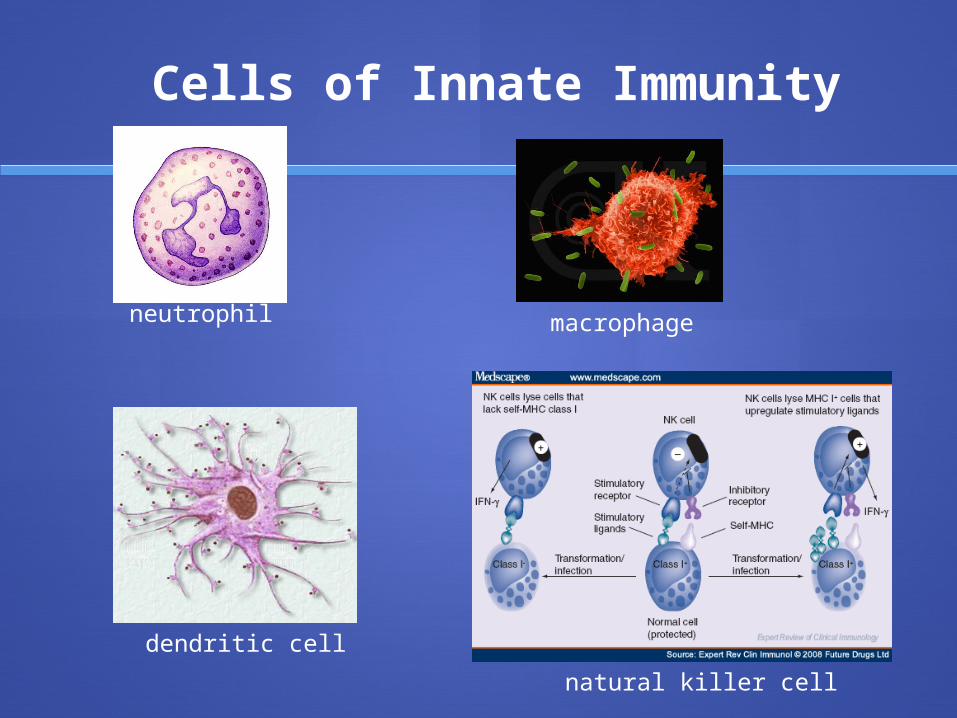
Cells of Innate Immunity
neutrophil macrophage
dendritic cell
natural killer cell
Bacterial and fungal infection: first line of defense: neutrophil
Phagocytosis and secretion of mediators of inflammation:
macrophages
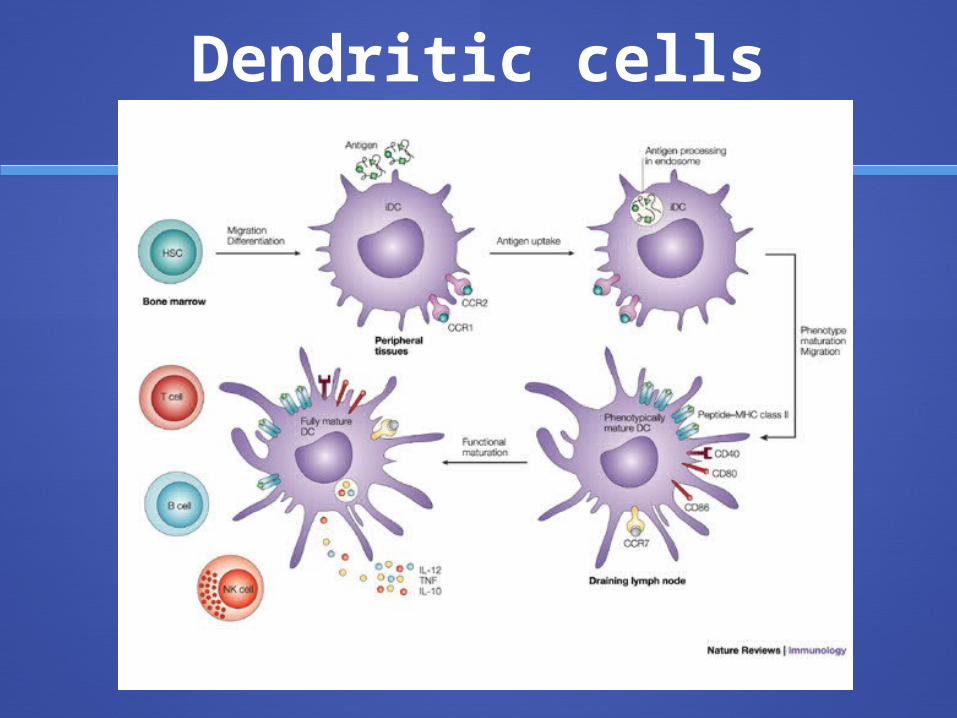
Dendritic cells
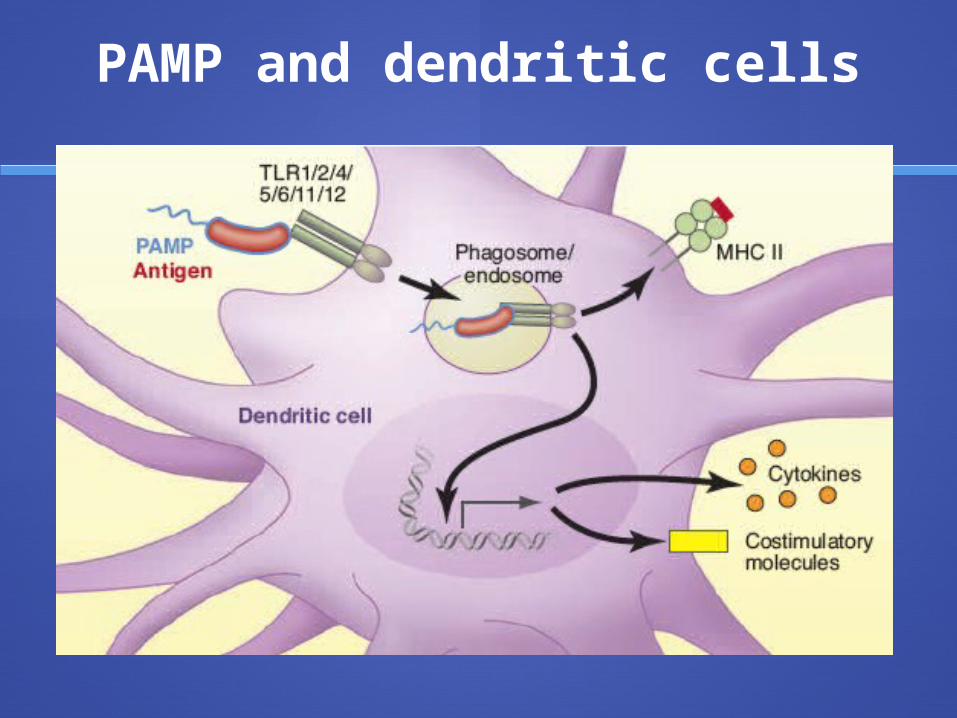
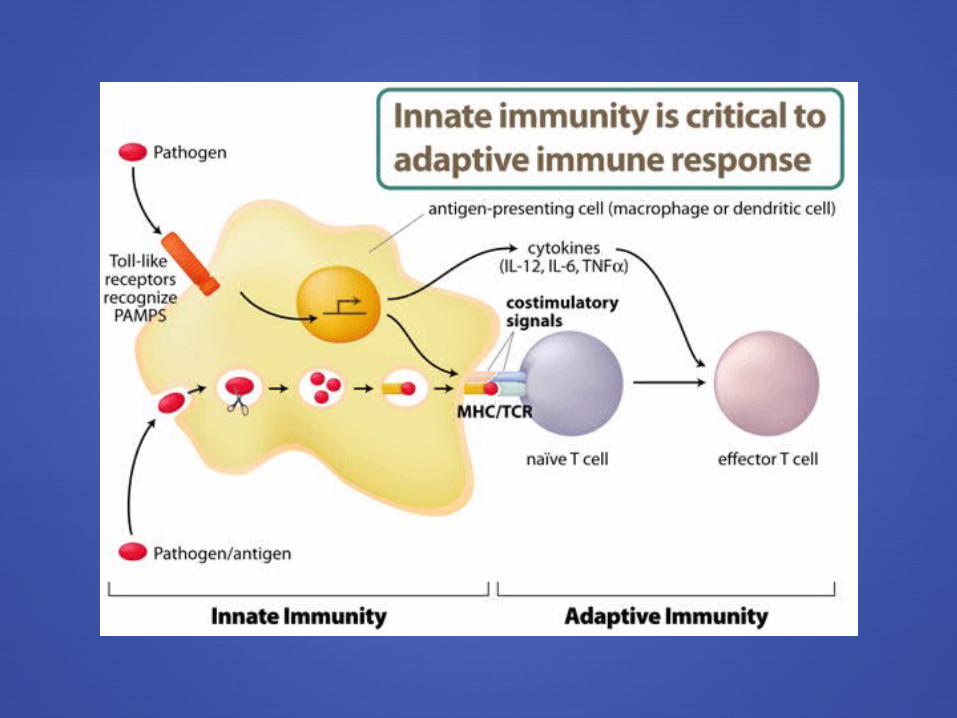
PAMP and dendritic cells
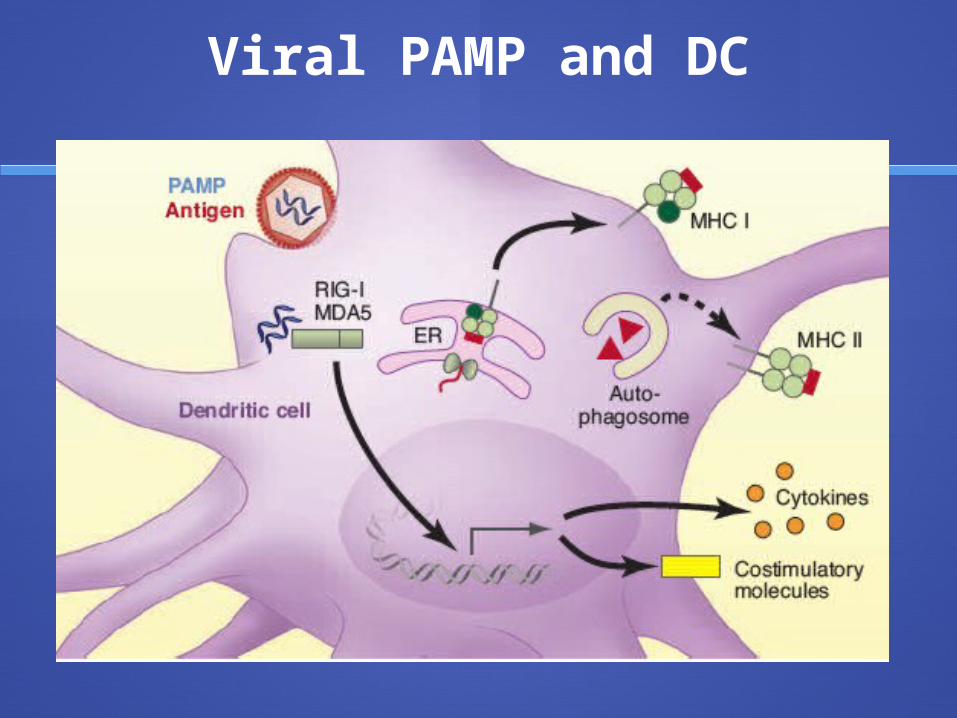
Viral PAMP and DC
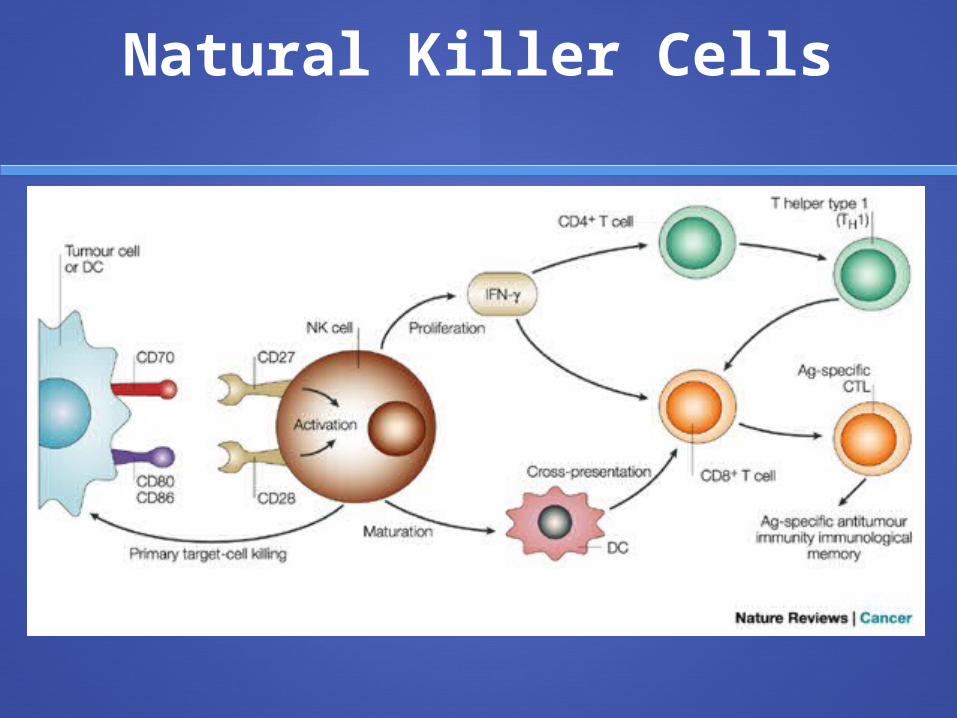
Natural Killer Cells
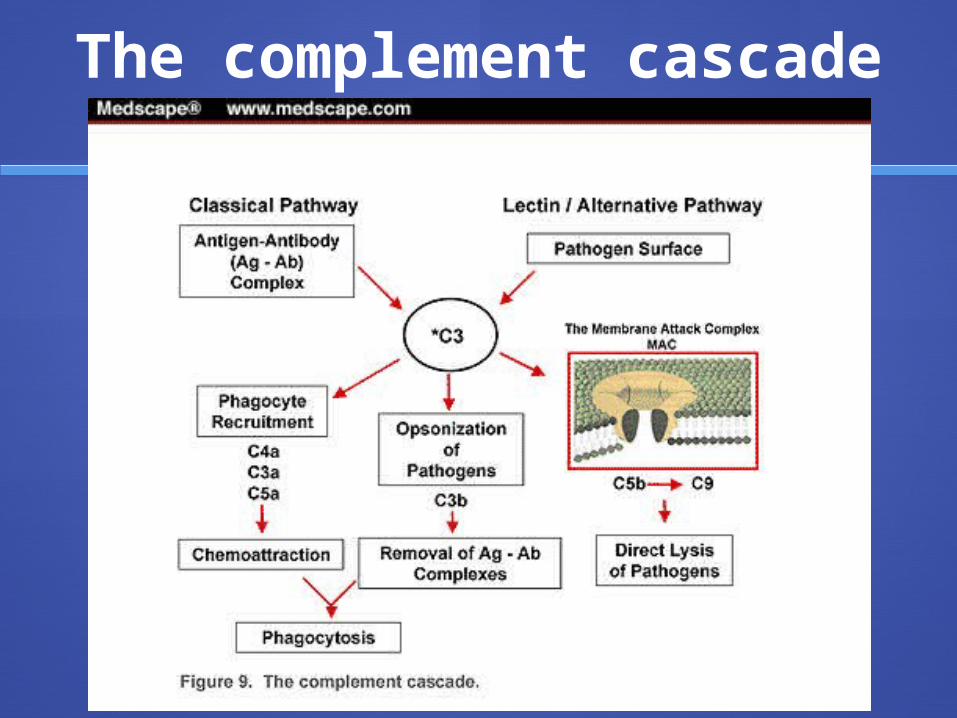
The complement cascade
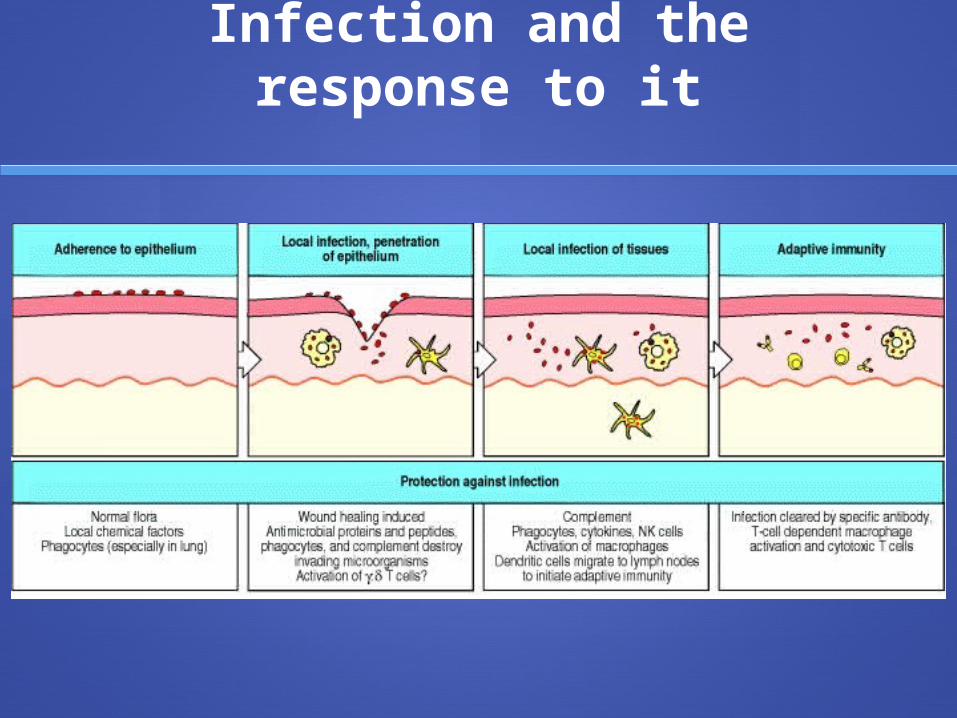
Infection and the response to it
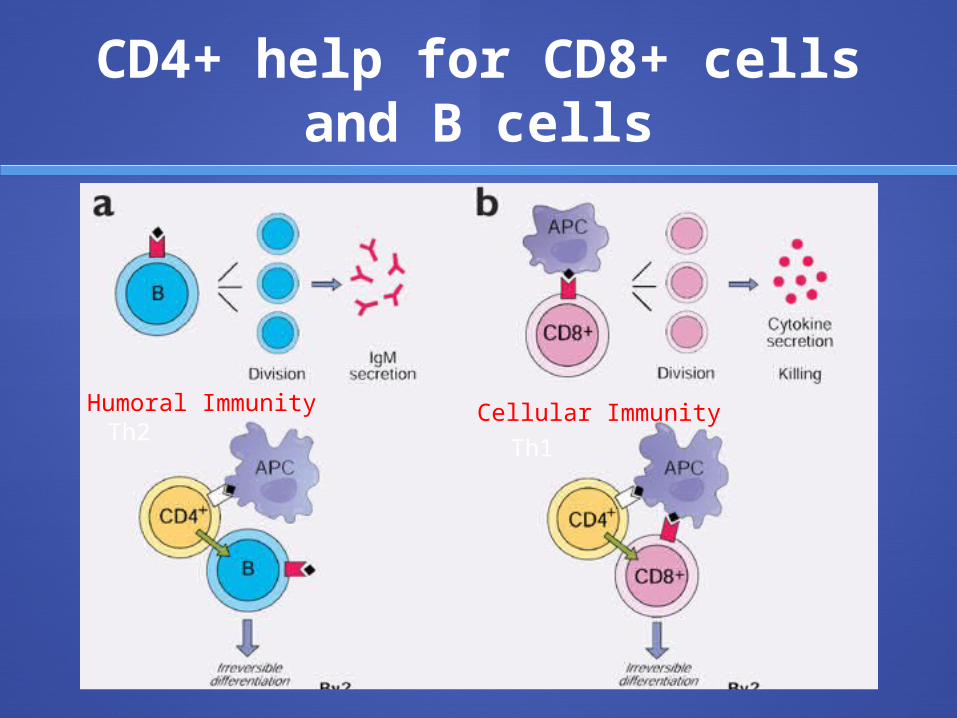
CD4+ help for CD8+ cells and B cells
Th2Th1
Humoral Immunity Cellular Immunity
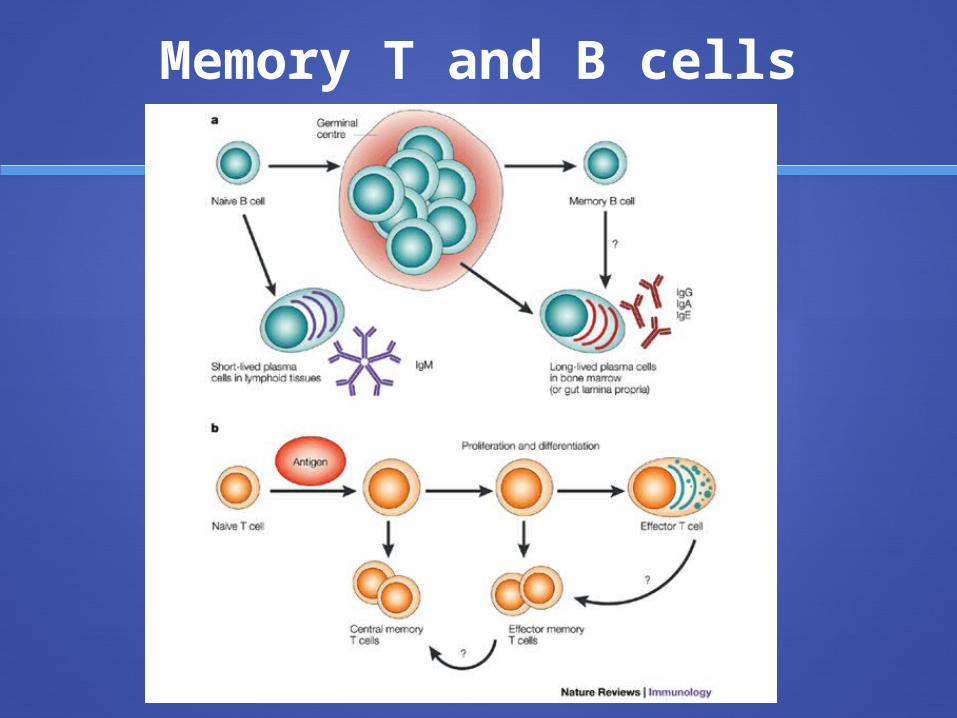
Memory T and B cells
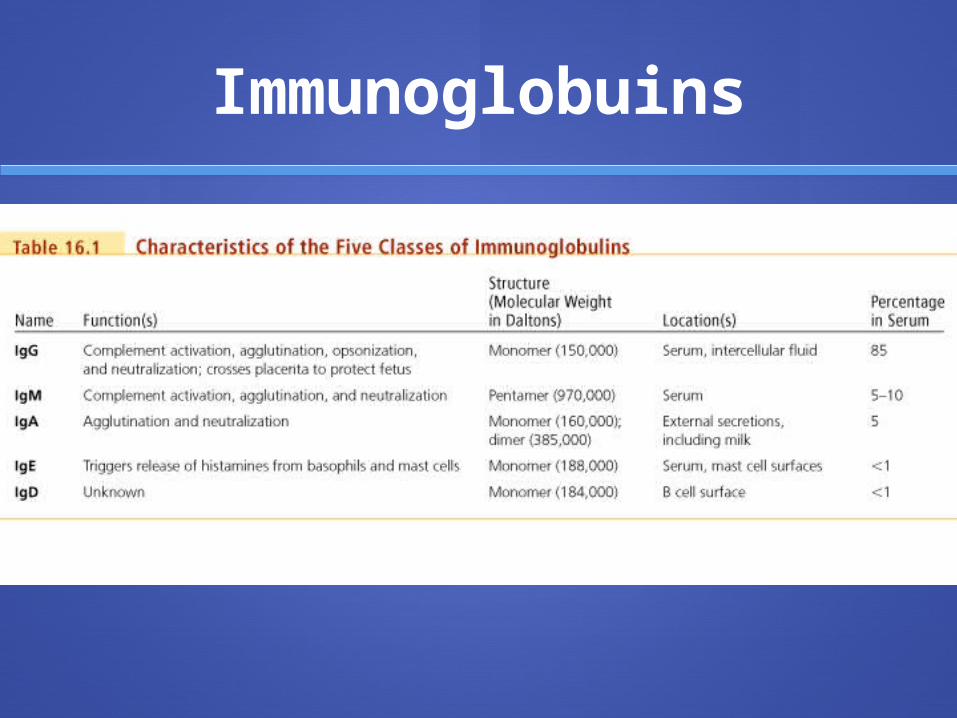
Immunoglobuins
Humoral vs. Cellular Mediated Immunity (CMI)
Humoral: Extracellular
pathogens
CMI Intracellular
pathogens
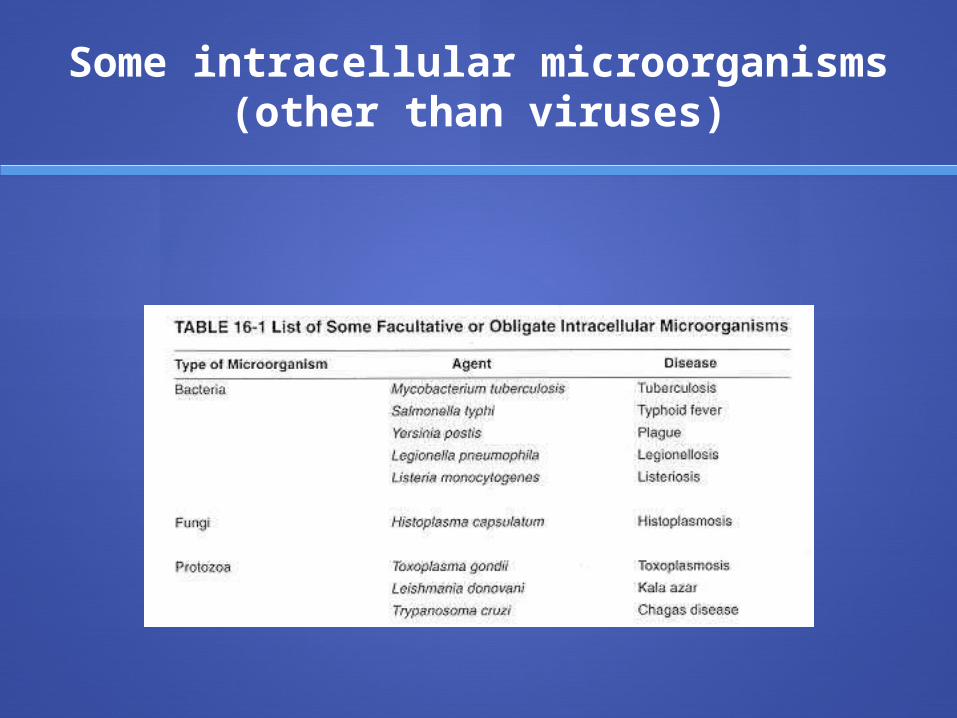
Some intracellular microorganisms (other than viruses)
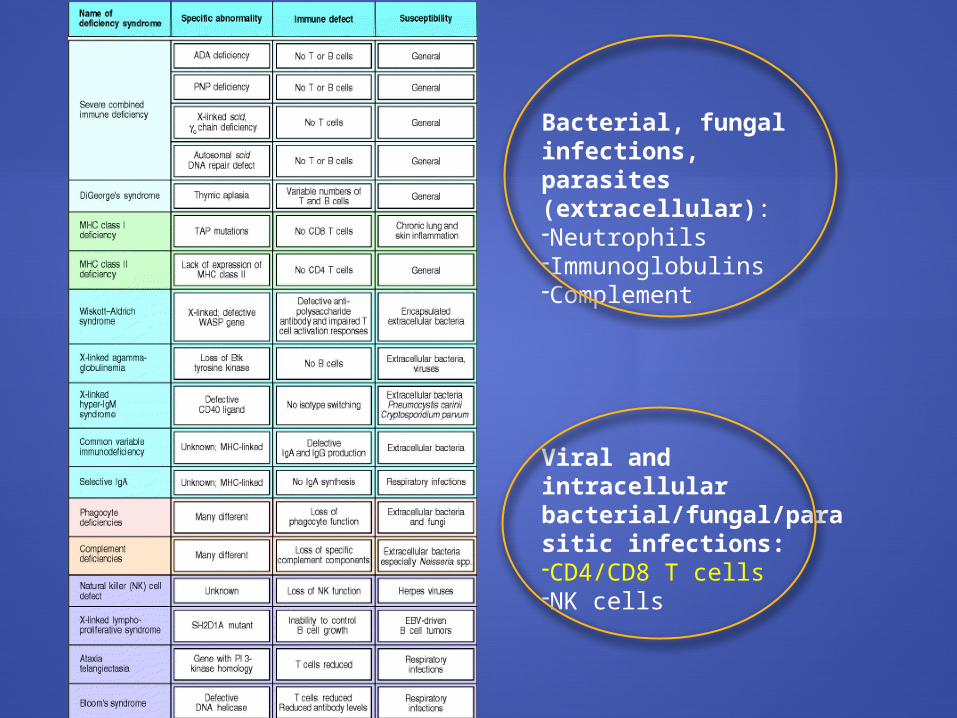
Bacterial, fungal infections,parasites (extracellular):-Neutrophils-Immunoglobulins-Complement
Viral and intracellular bacterial/fungal/parasitic infections:-CD4/CD8 T cells-NK cells
Pediatric HIV infection
HIV/AIDS Statistics in Liberia
Adult prevalence of HIV/AIDS in Liberia estimated to be 5.2%.1
The prevalence rate of HIV in Greater Monrovia is estimated to be 9.5%1
UNICEF has not received reporting on incidence or prevalence of HIV/AIDS in the pediatric population of Liberia.2
1The Basic Package of Health and Social Welfare Services, Republic of Liberia, Ministry of Health and Social Welfare.2http://www.unicef.org/infobycountry/liberia.html
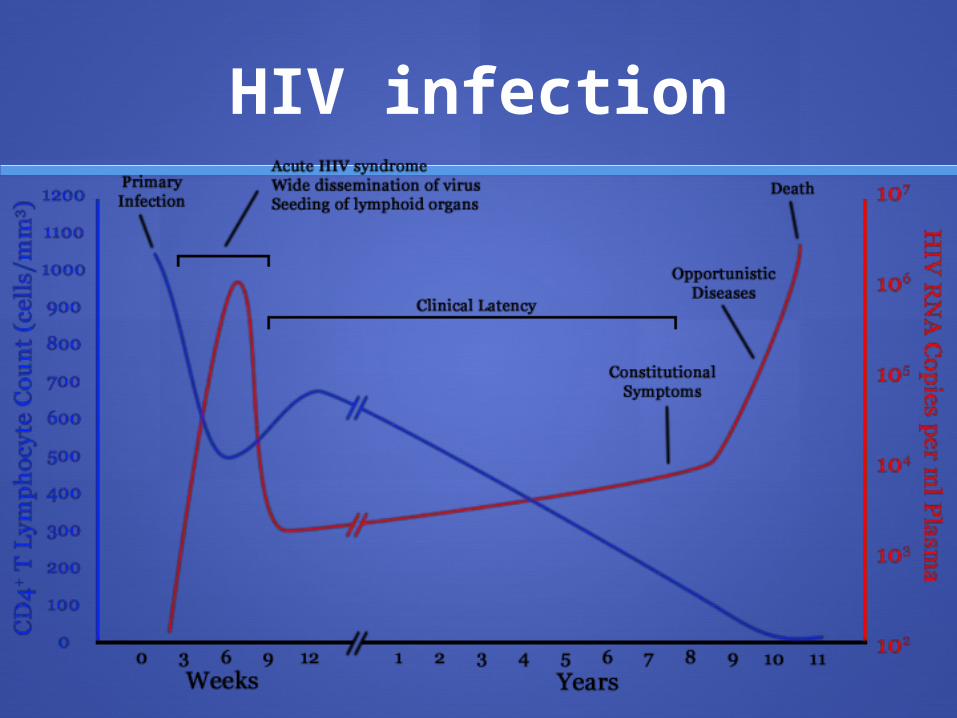
HIV infection
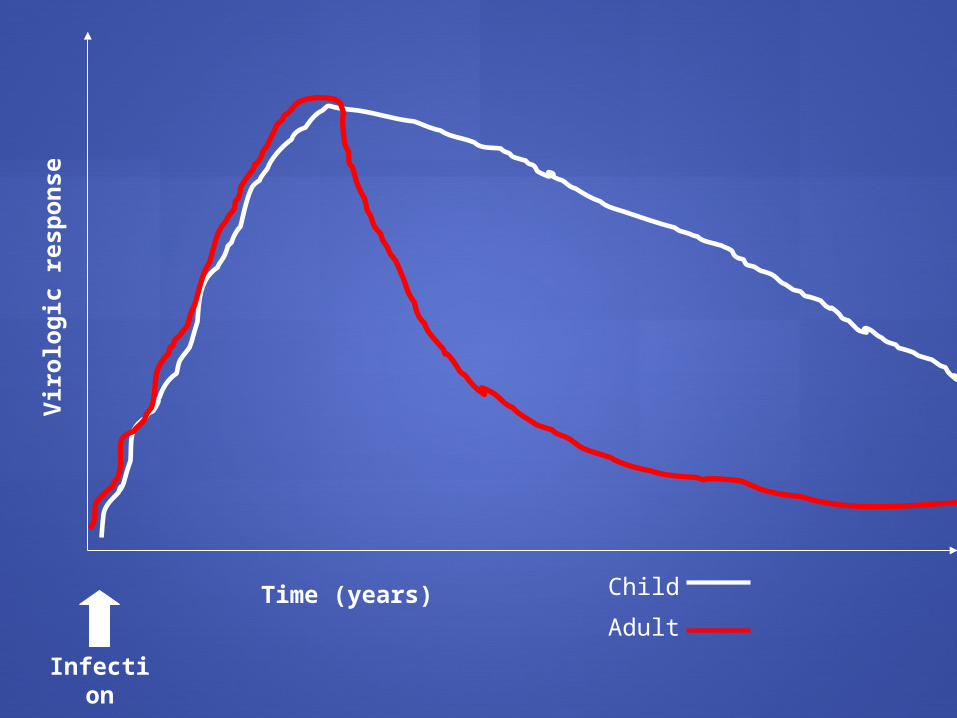
Time (years)
Vir
olo
gic
resp
on
se
Child
Adult
Infection
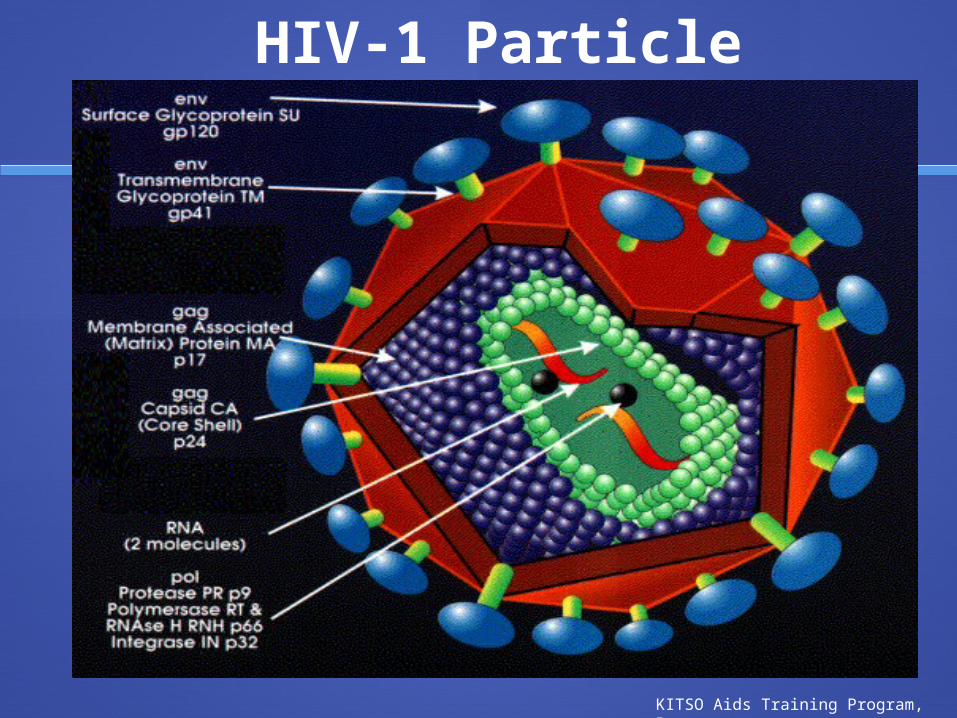
HIV-1 Particle
KITSO Aids Training Program, Botswana
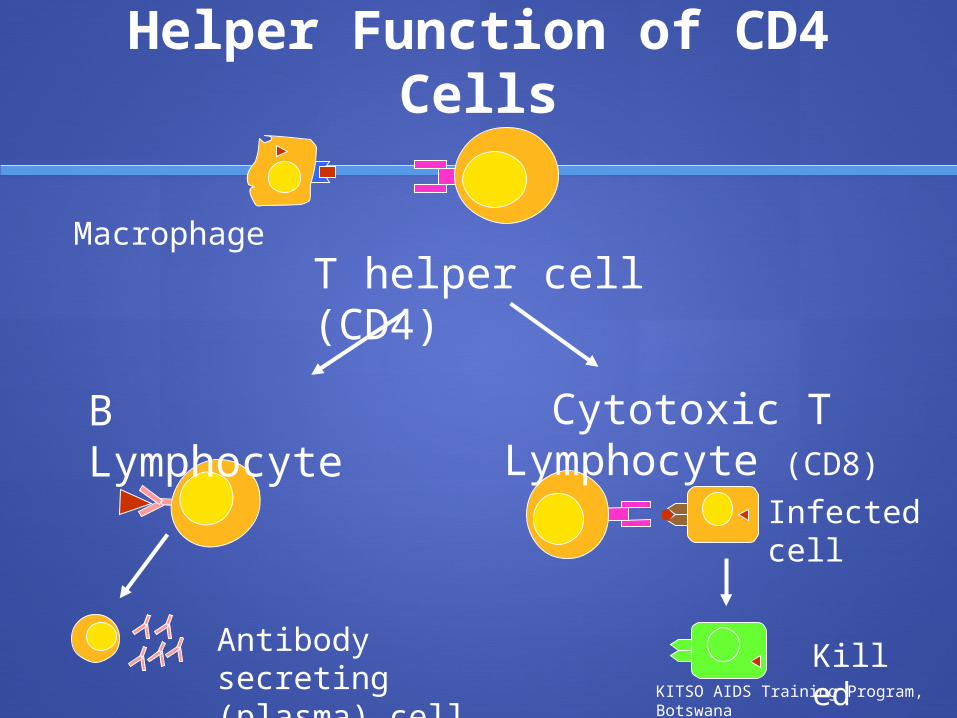
Helper Function of CD4 Cells
B Lymphocyte
T helper cell (CD4)Macrophage
Antibody secreting (plasma) cell
Infected cell
Cytotoxic T Lymphocyte (CD8)
KilledKITSO AIDS Training Program, Botswana
Immune abnormalities
Hypergammaglobulinemia
Increased CD8+ cells
Decreased CD4+ cells
Decrease in CD4:CD8 ratio < 1
Immune activation (chronic)
HIV may be transmitted to the infant during pregnancy, at the time of delivery, and through breastfeeding; most transmission is thought to take place during delivery
For a mother known to be HIV-infected prenatally, the additional risk of transmission of HIV to her infant through breastfeeding has been estimated at 14%
The risk is as high as 29% for mothers who acquire HIV post-natally
Transmission
Mother-to-Child Transmission of HIV
ARV Therapy and MTCT
• Prevention of prenatal transmission• Women first diagnosed with HIV
infection during pregnancy• HIV-infected women on ART who
become pregnant
High maternal viral load: >5-10,000 copies/ml (e.g., at time of seroconversion and during late HIV disease: CD4 cell counts <100 cells/mm)
Recurrent STDs Malaria interferes with placental
functions and eases viral transmission across the placenta
Vitamin A deficiency Preterm delivery
Factors Which May Increase the Risk of Transmission
Vaginal delivery Duration of rupture of membranes is
longer than 4 hours Placental disruption Invasive procedures during delivery
(e.g., vacuum extraction, episiotomy, use of forceps, fetal scalp monitoring)
Mechanical nasal suction after delivery Breastfeeding and especially mixed
feeding
Factors Which May Increase the Risk of Transmission, continued
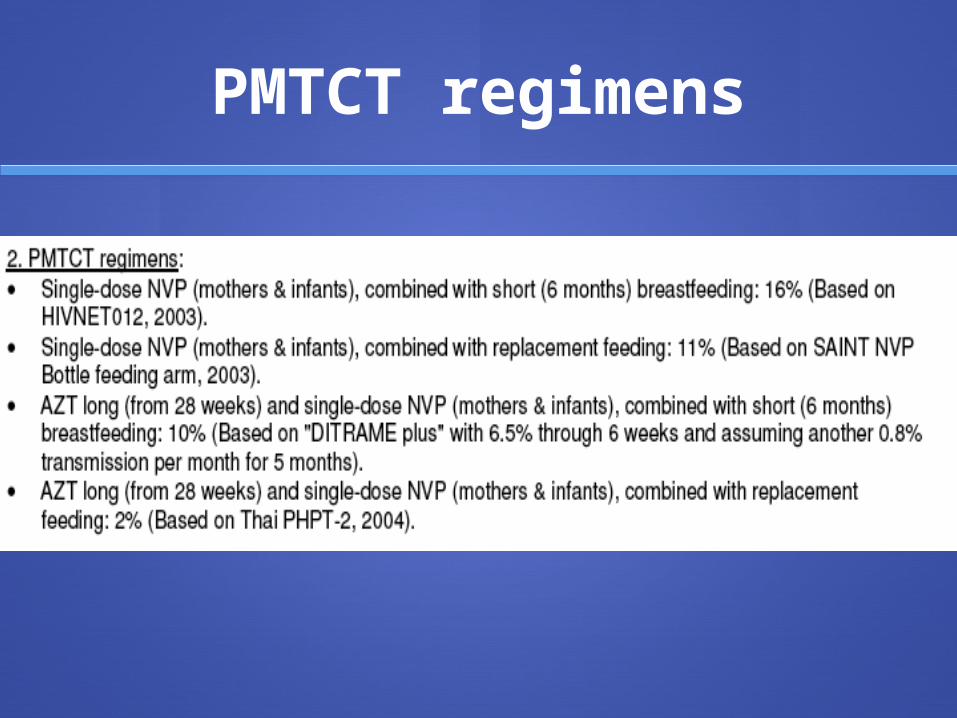
PMTCT regimens
Breastfeeding Formula
HIV Mortality
Breastfeeding and MTCT
Pediatric HIV Infection –Common Clinical Presentations Infectious Diseases
Respiratory Illness (PCP, Tuberculosis) Diarrheal Diseases Oral Candidiasis Herpes Zoster
Lymphadenopathy, Hepatomegaly, Parotitis
Persistent fever
Growth failure: Kwashiorkor, Marasmus
Developmental Delay or Regression
Malignancies: Lymphoma, Kaposi’s sarcoma
Diarrheal Illness
Similar prevalence of stool pathogens between HIV infected and uninfected children.
Worse outcomes in HIV infected children.
KITSO AIDS Training, Botswana
Respiratory Illness
Death from respiratory tract infections: PCP: Most common pathogen in HIV-infected
children below six-months of age
Acute pyogenic pneumonia and tuberculosis common in HIV-infected and uninfected children.
KITSO AIDS Training, Botswana
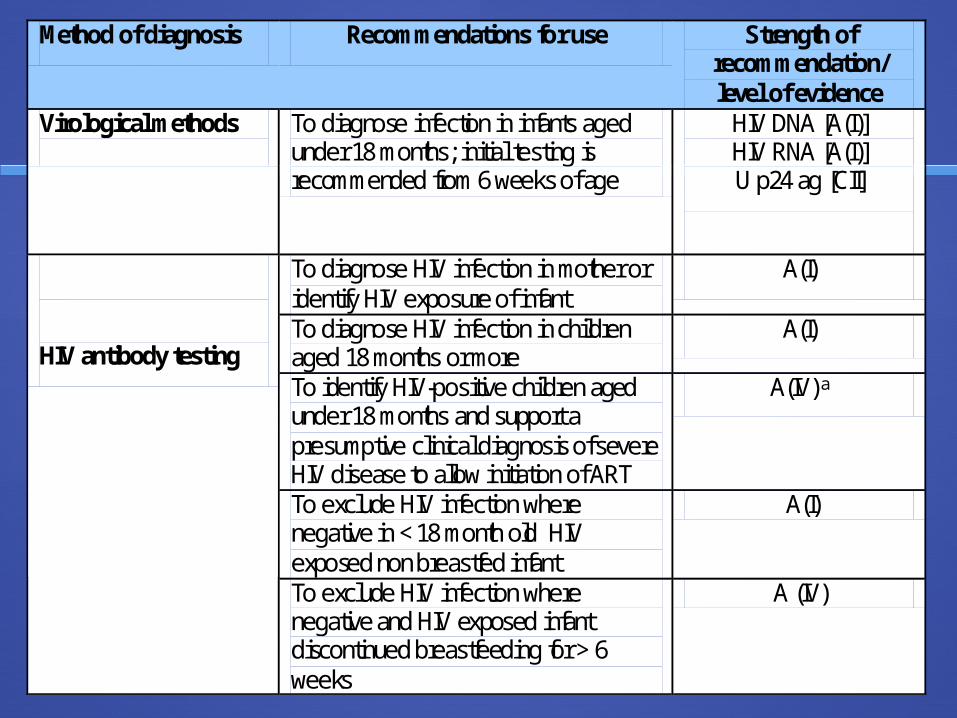
Method of diagnosis Recommendations for use Strength of recommendation/ level of evidence
Virological methods
To diagnose infection in infants aged under 18 months; initial testing is recommended from 6 weeks of age
HIV DNA [A(I)] HIV RNA [A(I)] U p24 ag [CII]
To diagnose HIV infection in mother or identify HIV exposure of infant
A(I)
To diagnose HIV infection in children aged 18 months or more
A(I)
To identify HIV-positive children aged under 18 months and support a presumptive clinical diagnosis of severe HIV disease to allow initiation of ART
A(IV) a
To exclude HIV infection where negative in < 18 month old HIV exposed non breastfed infant
A(I)
HIV antibody testing
To exclude HIV infection where negative and HIV exposed infant discontinued breastfeeding for > 6 weeks
A (IV)
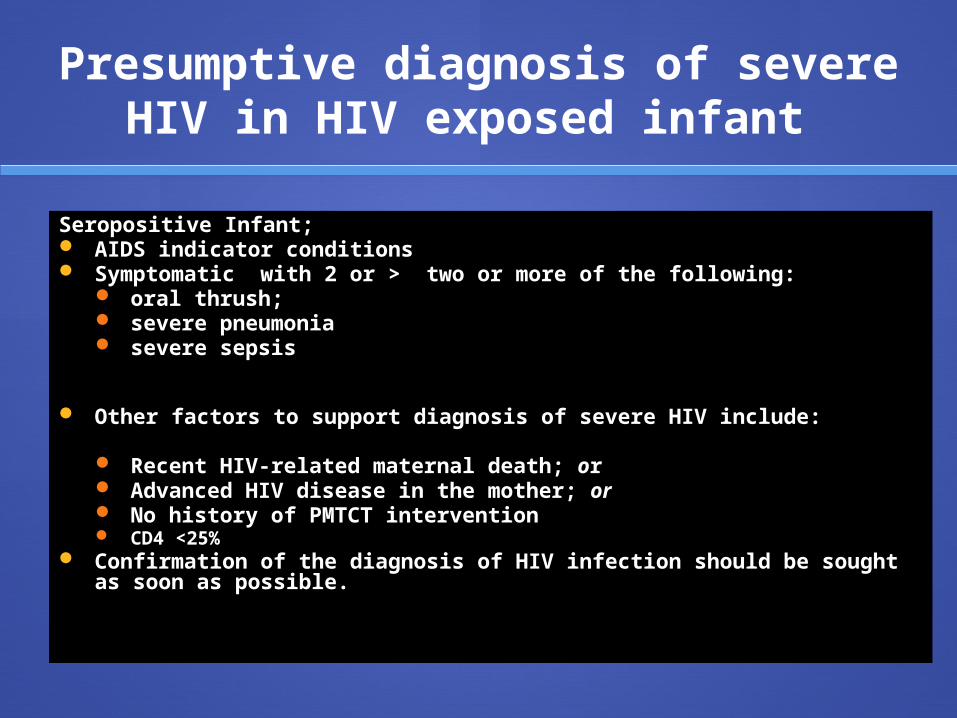
Presumptive diagnosis of severe HIV in HIV exposed infant
Seropositive Infant; AIDS indicator conditions Symptomatic with 2 or > two or more of the following:
oral thrush; severe pneumonia severe sepsis
Other factors to support diagnosis of severe HIV include:
Recent HIV-related maternal death; or Advanced HIV disease in the mother; or No history of PMTCT intervention CD4 <25%
Confirmation of the diagnosis of HIV infection should be sought as soon as possible.
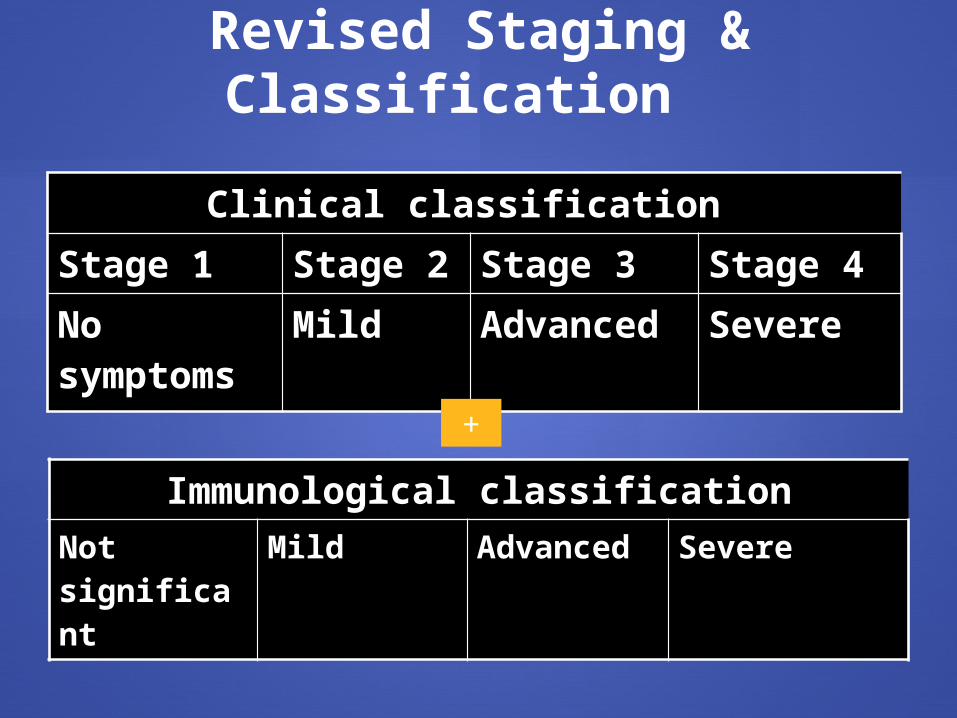
Revised Staging & Classification
Clinical classification
Stage 1 Stage 2 Stage 3 Stage 4No symptoms
Mild Advanced Severe
Immunological classificationNot significant
Mild Advanced Severe
+
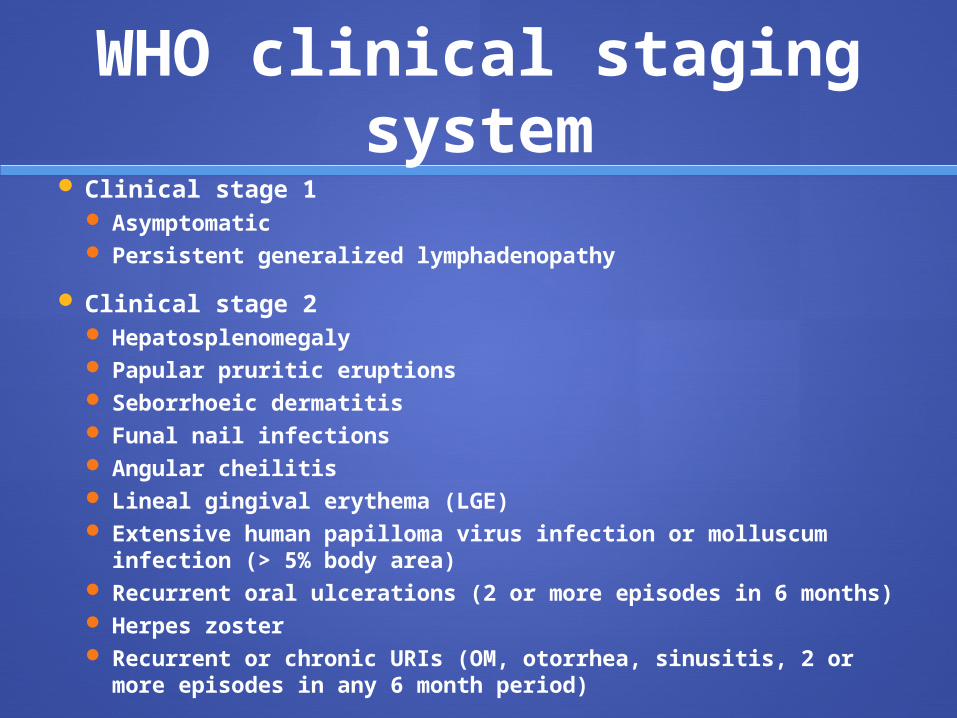
WHO clinical staging system
Clinical stage 1 Asymptomatic Persistent generalized lymphadenopathy
Clinical stage 2 Hepatosplenomegaly Papular pruritic eruptions Seborrhoeic dermatitis Funal nail infections Angular cheilitis Lineal gingival erythema (LGE) Extensive human papilloma virus infection or molluscum
infection (> 5% body area) Recurrent oral ulcerations (2 or more episodes in 6 months) Herpes zoster Recurrent or chronic URIs (OM, otorrhea, sinusitis, 2 or
more episodes in any 6 month period)
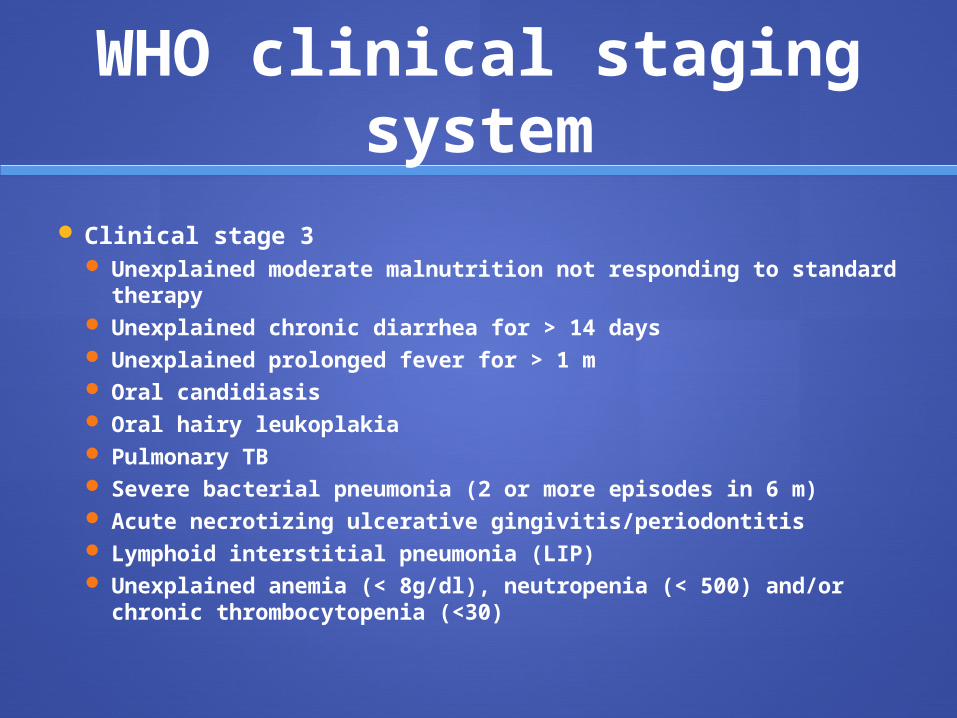
WHO clinical staging system
Clinical stage 3 Unexplained moderate malnutrition not responding to
standard therapy Unexplained chronic diarrhea for > 14 days Unexplained prolonged fever for > 1 m Oral candidiasis Oral hairy leukoplakia Pulmonary TB Severe bacterial pneumonia (2 or more episodes in 6 m) Acute necrotizing ulcerative gingivitis/periodontitis Lymphoid interstitial pneumonia (LIP) Unexplained anemia (< 8g/dl), neutropenia (< 500) and/or
chronic thrombocytopenia (<30)
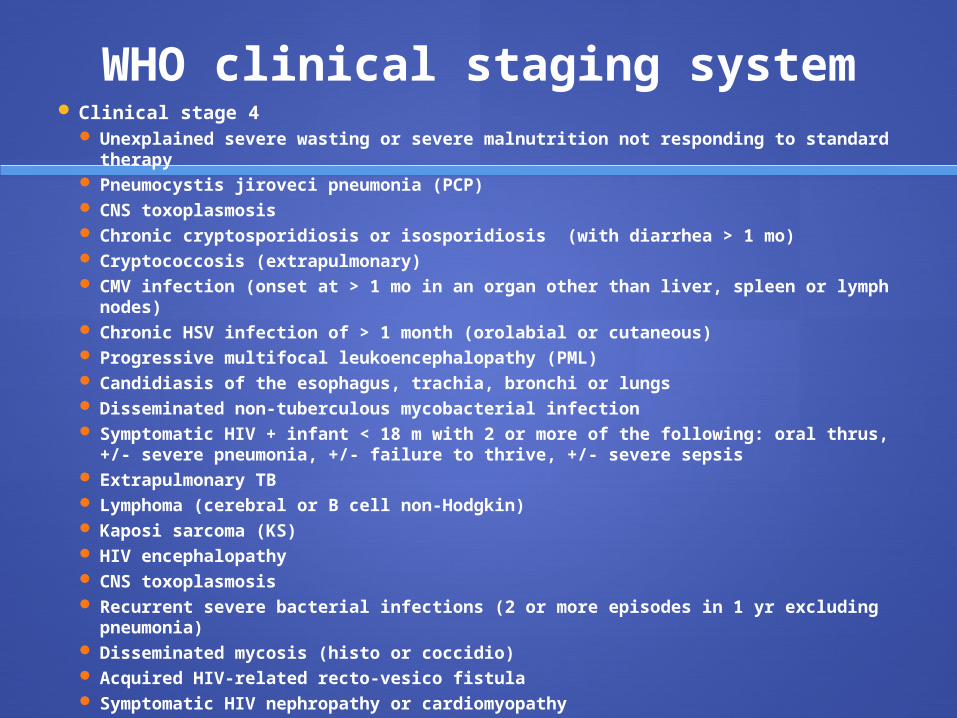
WHO clinical staging system Clinical stage 4
Unexplained severe wasting or severe malnutrition not responding to standard therapy
Pneumocystis jiroveci pneumonia (PCP) CNS toxoplasmosis Chronic cryptosporidiosis or isosporidiosis (with diarrhea > 1 mo) Cryptococcosis (extrapulmonary) CMV infection (onset at > 1 mo in an organ other than liver, spleen or lymph
nodes) Chronic HSV infection of > 1 month (orolabial or cutaneous) Progressive multifocal leukoencephalopathy (PML) Candidiasis of the esophagus, trachia, bronchi or lungs Disseminated non-tuberculous mycobacterial infection Symptomatic HIV + infant < 18 m with 2 or more of the following: oral thrus,
+/- severe pneumonia, +/- failure to thrive, +/- severe sepsis Extrapulmonary TB Lymphoma (cerebral or B cell non-Hodgkin) Kaposi sarcoma (KS) HIV encephalopathy CNS toxoplasmosis Recurrent severe bacterial infections (2 or more episodes in 1 yr excluding
pneumonia) Disseminated mycosis (histo or coccidio) Acquired HIV-related recto-vesico fistula Symptomatic HIV nephropathy or cardiomyopathy
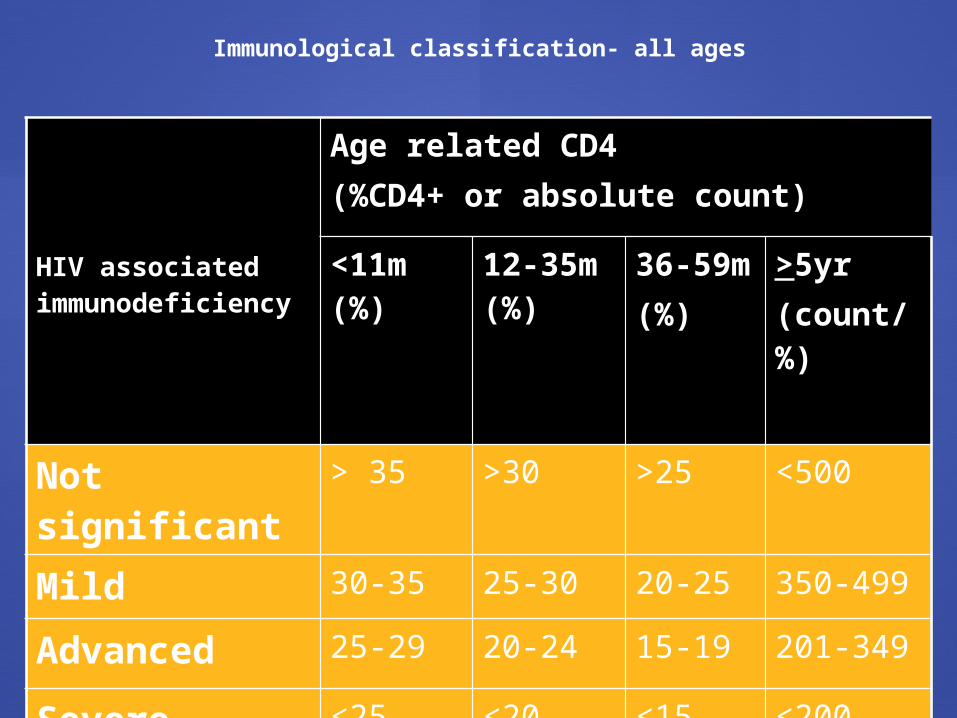
Immunological classification- all ages
HIV associated immunodeficiency
Age related CD4(%CD4+ or absolute count)
<11m (%)
12-35m (%)
36-59m(%)
>5yr(count/%)
Not significant > 35 >30 >25 <500
Mild 30-35 25-30 20-25 350-499
Advanced 25-29 20-24 15-19 201-349
Severe <25 <20 <15 <200
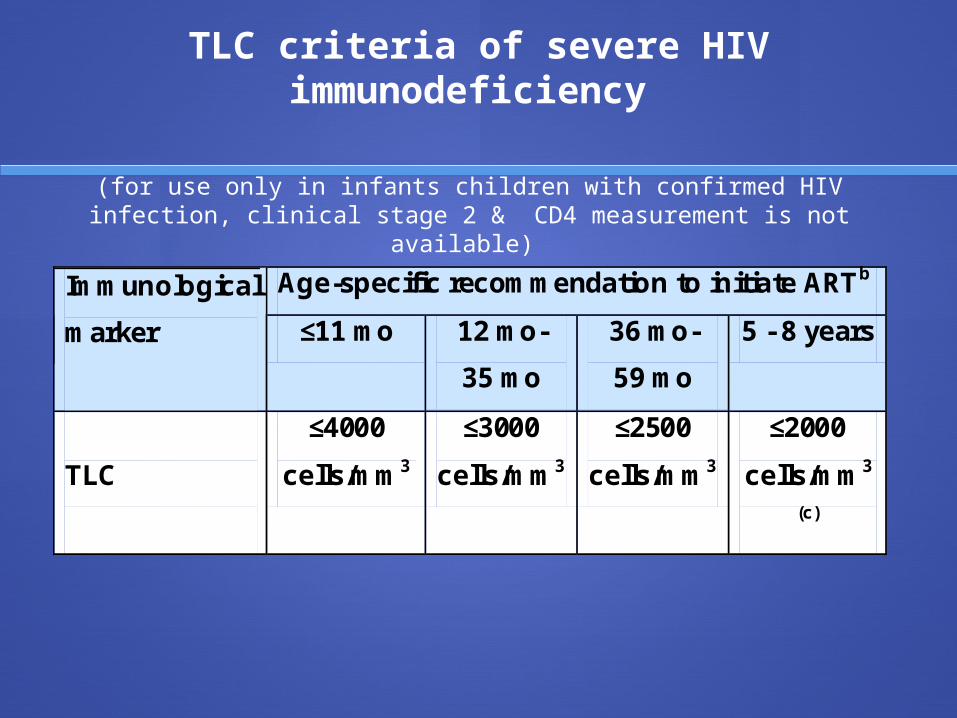
TLC criteria of severe HIV immunodeficiency
Age-specific recommendation to initiate ARTb Immunological
marker
≤11 mo 12 mo-
35 mo
36 mo-
59 mo
5 - 8 years
TLC
≤4000
cells/mm3
≤3000
cells/mm3
≤2500
cells/mm3
≤2000
cells/mm3
(c)
(for use only in infants children with confirmed HIV infection, clinical stage 2 & CD4 measurement is not available)
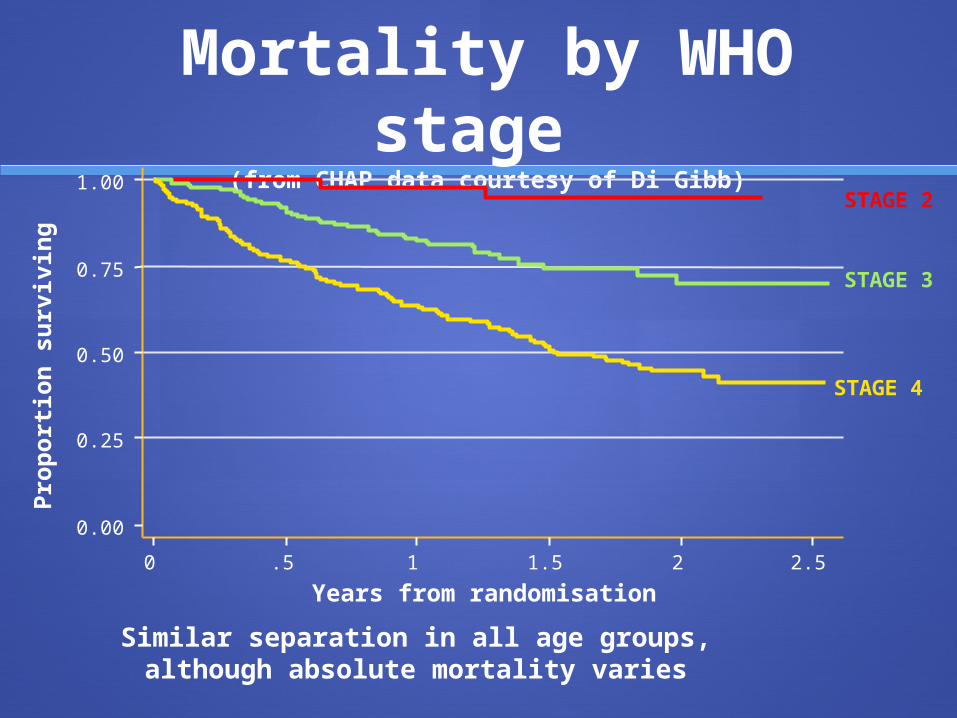
Mortality by WHO stage
(from CHAP data courtesy of Di Gibb)
0.00
0.25
0.50
0.75
1.00
0 .5 1 1.5 2 2.5
Years from randomisation
STAGE 2
STAGE 3
STAGE 4
Pro
port
ion
su
rviv
ing
Similar separation in all age groups, although absolute mortality varies
Goals of Treatment
Clinical: Prolong life, improve quality of life.
Virologic: Achieve maximal suppression of viral load Viral load should drop by at least 1.0 after 3
months of treatment Viral load should be less than 400 after 6 months
of treatment
Immunologic: Reverse immune system damage.
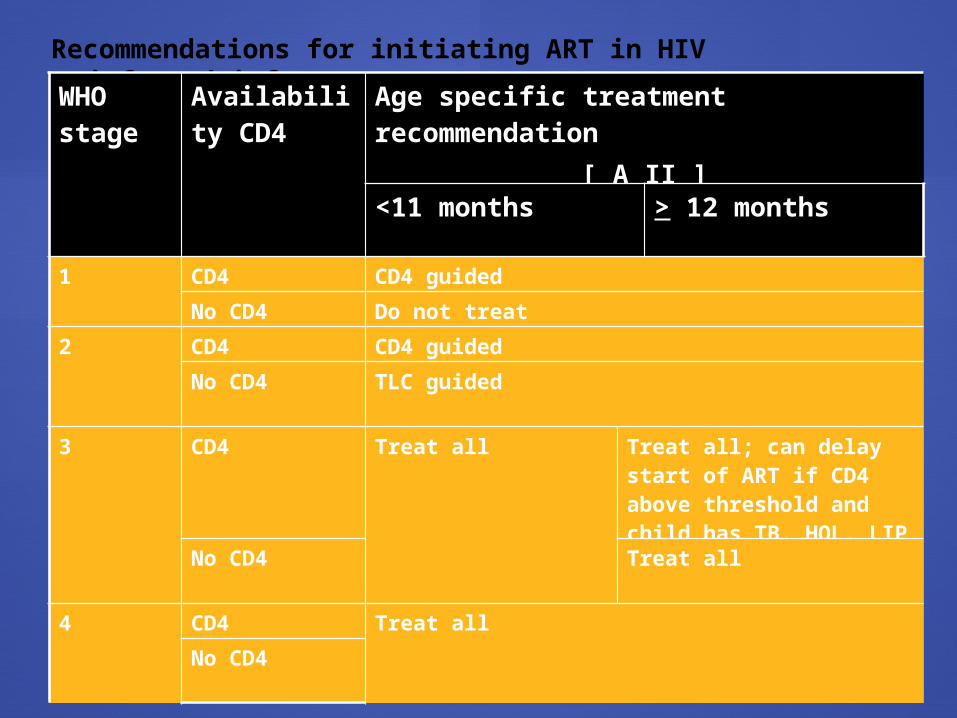
Recommendations for initiating ART in HIV
infected infantsWHO stage
Availability CD4
Age specific treatment recommendation
[ A II ]
<11 months > 12 months
1 CD4 CD4 guided
No CD4 Do not treat
2 CD4 CD4 guided
No CD4 TLC guided
3 CD4 Treat all Treat all; can delay start of ART if CD4 above threshold and child has TB, HOL, LIP
No CD4 Treat all
4 CD4 Treat all
No CD4
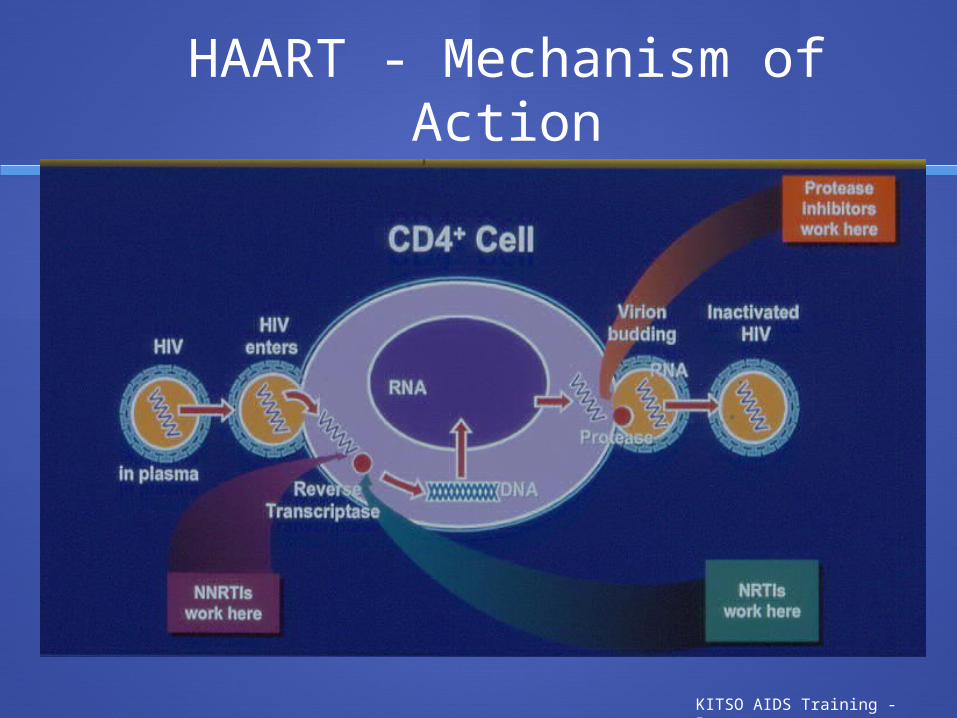
HAART - Mechanism of Action
KITSO AIDS Training - Botswana
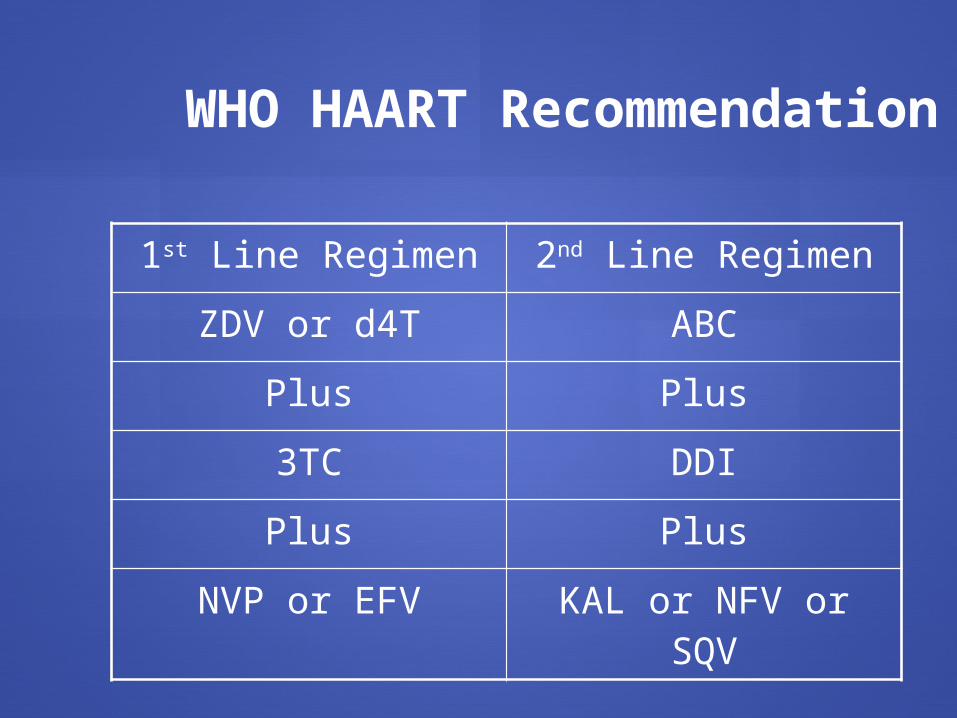
1st Line Regimen 2nd Line Regimen
ZDV or d4T ABC
Plus Plus
3TC DDI
Plus Plus
NVP or EFV KAL or NFV or SQV
WHO HAART Recommendation
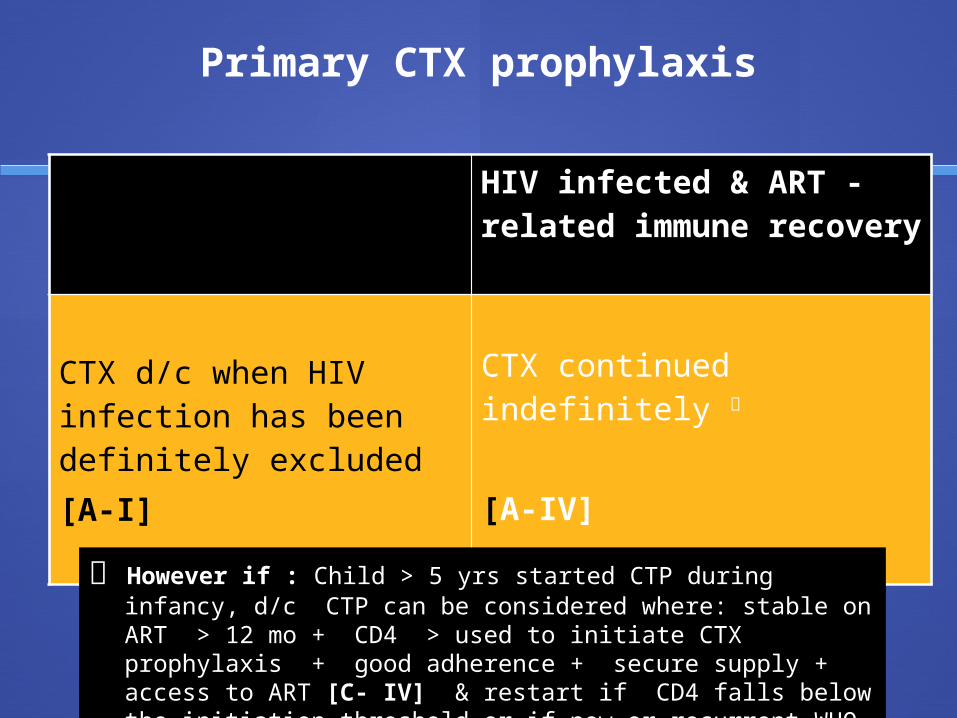
Primary CTX prophylaxis
HIV-exposed infants & children confirmed HIV uninfected
HIV infected & ART - related immune recovery
CTX d/c when HIV infection has been definitely excluded [A-I]
CTX continued indefinitely
[A-IV]
However if : Child > 5 yrs started CTP during infancy, d/c CTP can be considered where: stable on ART > 12 mo + CD4 > used to initiate CTX prophylaxis + good adherence + secure supply + access to ART [C- IV] & restart if CD4 falls below the initiation threshold or if new or recurrent WHO 2, 3 or 4 conditions occur [A- IV]
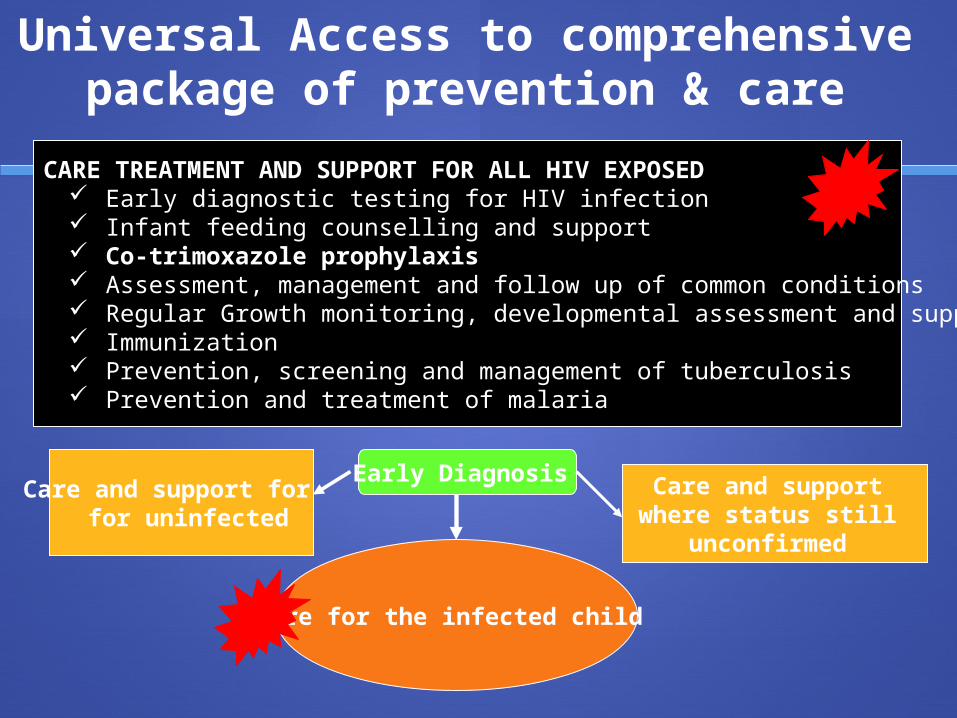
Universal Access to comprehensive package of prevention & care
CARE TREATMENT AND SUPPORT FOR ALL HIV EXPOSED Early diagnostic testing for HIV infection Infant feeding counselling and support Co-trimoxazole prophylaxis Assessment, management and follow up of common conditions Regular Growth monitoring, developmental assessment and support Immunization Prevention, screening and management of tuberculosis Prevention and treatment of malaria
Care and support for for uninfected
Care and support where status still
unconfirmed
Care for the infected child
Early Diagnosis
Thank you for your attention!
Any questions?



![Music Therapy For Acquired Brain Injury - Temple · PDF file[Intervention Review] Music therapy for acquired brain injury Joke Bradt1, Wendy L Magee2, Cheryl Dileo3, Barbara L Wheeler4,](https://img.pdfslide.net/doc/110x75/5a7a08327f8b9adf228ca12b/music-therapy-for-acquired-brain-injury-temple-intervention-review-music-therapy.jpg)