Embed Size (px)
Citation preview
Case Report
Dermatology 2001;203:60–62
Acquired Hair Fragility in Pili anulati: CausalRelationship with Androgenetic Alopecia
Günther F.L. Hofbauera Dionysios Tsambaosc Max A. Spycherb Ralph M. Trüeba
aDepartment of Dermatology, University Hospital, and bDepartment of Pathology, University of Zürich, Switzerland;cDepartment of Dermatology, University of Patras, Greece
Received: September 25, 2000Accepted: March 2, 2001
Ralph M. Trüeb, MDDepartment of Dermatology, University HospitalGloriastrasse 31CH–8091 Zürich (Switzerland)Tel. +41 1 255 25 92, Fax +41 1 255 44 03, E-Mail [email protected]
ABCFax + 41 61 306 12 34E-Mail [email protected]
© 2001 S. Karger AG, Basel1018–8665/01/2031–0060$17.50/0
Accessible online at:www.karger.com/journals/drm
Key WordsPili anulati W Increased hair fragility W
Secondary trichorrhexis nodosa W
Androgenetic alopecia
AbstractPili anulati are defined by characteristic al-ternating light and dark banding in the hairshaft, due to air-filled spaces between themacrofibrillar units of the hair cortex, andare regarded as a congenital hair shaft dis-order without increased hair fragility. Twocases of pili anulati are presented, in whichfragility of hair developed in a causal rela-tionship with the onset of androgeneticalopecia. Accordingly, trichorrhexis-nodo-sa-like hair fracturing was exclusively lim-ited to the androgenetic region. In general,secondary trichorrhexis nodosa is an unspe-cific finding related to excess stress of hairin relation to its fragility. With onset of hairthinning due to androgenetic alopecia, pro-gressive reduction of hair shaft diametermay cause increased fragility in pili anulati.In this case, hair shaft fracturing occurswithin the area of androgenetic alopecia andcolocalizes with the air-filled cavities of pilianulati.
Copyright © 2001 S. Karger AG, Basel
Anomalies of the hair shaft are distin-guished into those with and those withoutincreased hair fragility. Pili anulati are gen-erally classified as a hair shaft disorder with-out increased hair fragility. We report 2 casesof increased hair shaft fragility in pili anulatiacquired in a causal relationship with thedevelopment of androgenetic alopecia.
Case Reports
Case 1A 24-year-old woman presented with a
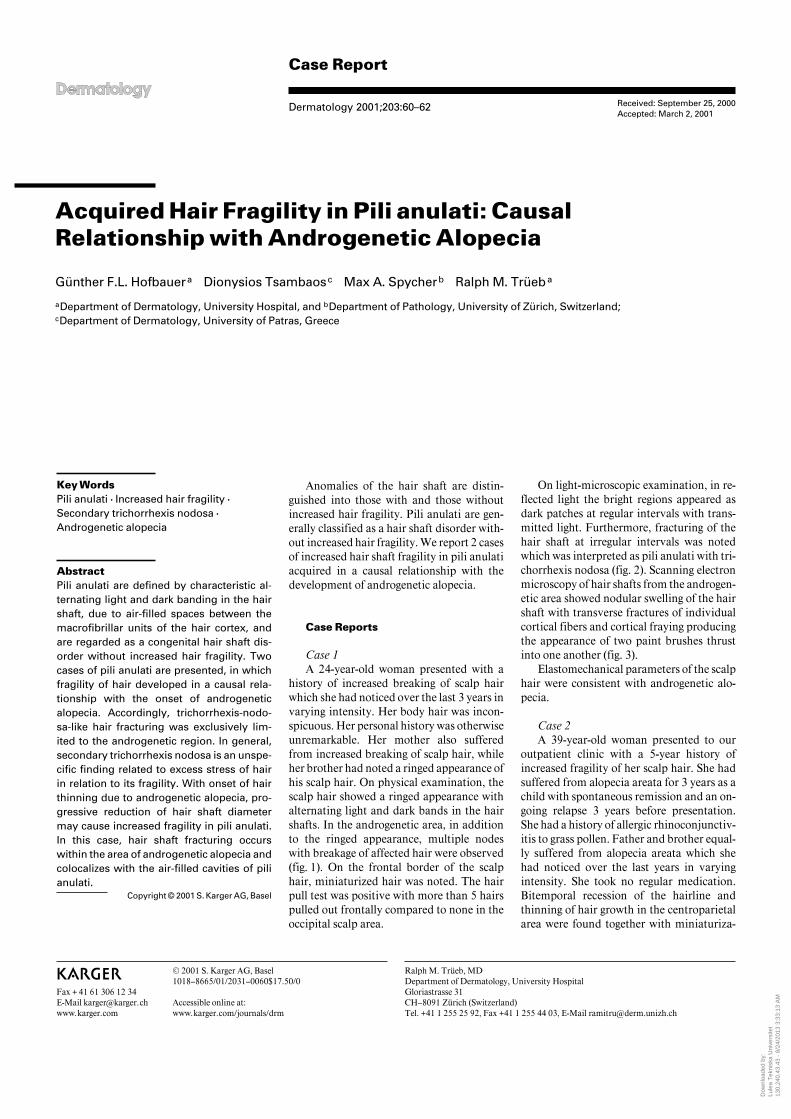
history of increased breaking of scalp hairwhich she had noticed over the last 3 years invarying intensity. Her body hair was incon-spicuous. Her personal history was otherwiseunremarkable. Her mother also sufferedfrom increased breaking of scalp hair, whileher brother had noted a ringed appearance ofhis scalp hair. On physical examination, thescalp hair showed a ringed appearance withalternating light and dark bands in the hairshafts. In the androgenetic area, in additionto the ringed appearance, multiple nodeswith breakage of affected hair were observed(fig. 1). On the frontal border of the scalphair, miniaturized hair was noted. The hairpull test was positive with more than 5 hairspulled out frontally compared to none in theoccipital scalp area.
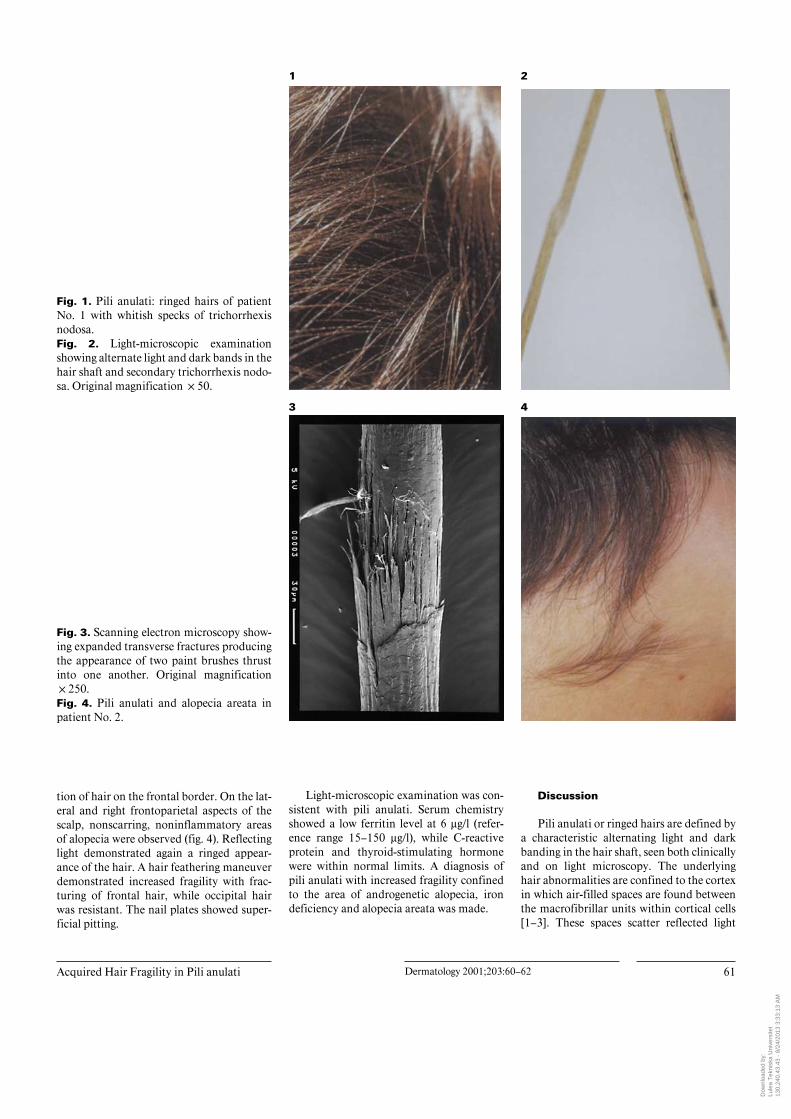
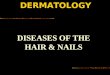
On light-microscopic examination, in re-flected light the bright regions appeared asdark patches at regular intervals with trans-mitted light. Furthermore, fracturing of thehair shaft at irregular intervals was notedwhich was interpreted as pili anulati with tri-chorrhexis nodosa (fig. 2). Scanning electronmicroscopy of hair shafts from the androgen-etic area showed nodular swelling of the hairshaft with transverse fractures of individualcortical fibers and cortical fraying producingthe appearance of two paint brushes thrustinto one another (fig. 3).
Elastomechanical parameters of the scalphair were consistent with androgenetic alo-pecia.
Case 2A 39-year-old woman presented to our
outpatient clinic with a 5-year history ofincreased fragility of her scalp hair. She hadsuffered from alopecia areata for 3 years as achild with spontaneous remission and an on-going relapse 3 years before presentation.She had a history of allergic rhinoconjunctiv-itis to grass pollen. Father and brother equal-ly suffered from alopecia areata which shehad noticed over the last years in varyingintensity. She took no regular medication.Bitemporal recession of the hairline andthinning of hair growth in the centroparietalarea were found together with miniaturiza-
Dow
nloa
ded
by:
Lule
a T
ekni
ska
Uni
vers
itet
13
0.24
0.43
.43
- 8/
24/2
013
3:33
:13
AM
Acquired Hair Fragility in Pili anulati Dermatology 2001;203:60–62 61
Fig. 1. Pili anulati: ringed hairs of patientNo. 1 with whitish specks of trichorrhexisnodosa.Fig. 2. Light-microscopic examinationshowing alternate light and dark bands in thehair shaft and secondary trichorrhexis nodo-sa. Original magnification !50.
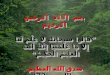
Fig. 3. Scanning electron microscopy show-ing expanded transverse fractures producingthe appearance of two paint brushes thrustinto one another. Original magnification!250.Fig. 4. Pili anulati and alopecia areata inpatient No. 2.
tion of hair on the frontal border. On the lat-eral and right frontoparietal aspects of thescalp, nonscarring, noninflammatory areasof alopecia were observed (fig. 4). Reflectinglight demonstrated again a ringed appear-ance of the hair. A hair feathering maneuverdemonstrated increased fragility with frac-turing of frontal hair, while occipital hairwas resistant. The nail plates showed super-ficial pitting.
Light-microscopic examination was con-sistent with pili anulati. Serum chemistryshowed a low ferritin level at 6 Ìg/l (refer-ence range 15–150 Ìg/l), while C-reactiveprotein and thyroid-stimulating hormonewere within normal limits. A diagnosis ofpili anulati with increased fragility confinedto the area of androgenetic alopecia, irondeficiency and alopecia areata was made.
Discussion
Pili anulati or ringed hairs are defined bya characteristic alternating light and darkbanding in the hair shaft, seen both clinicallyand on light microscopy. The underlyinghair abnormalities are confined to the cortexin which air-filled spaces are found betweenthe macrofibrillar units within cortical cells[1–3]. These spaces scatter reflected light
1 2
3 4
Dow
nloa
ded
by:
Lule
a T
ekni
ska
Uni
vers
itet
13
0.24
0.43
.43
- 8/
24/2
013
3:33
:13
AM

62 Dermatology 2001;203:60–62 Hofbauer/Tsambaos/Spycher/Trüeb
producing the typical clinical appearance ofringed hair. There is usually no increasedfragility of the hair shaft, and mechanicalparameters of pili anulati have been unre-markable [4, 5], but when fracturing followsexcessive mechanical or chemical trauma, ittends to occur within the bands.
In both presented cases pili anulati werefound in connection with acquired hair fra-gility confined to the area of androgeneticalopecia, as manifested by localized second-ary trichorrhexis nodosa and a pathologichair feathering test in this region. Acquiredtrichorrhexis nodosa is caused by externalstress to the hair shaft, usually secondary tophysicochemical trauma that is mostly asso-ciated with hair cosmetic procedures. Theseinclude treatments involving heat and chem-ical handling such as permanent waves, hairstraighteners, bleaching and hair dyes, aswell as vigorous styling with brushes orcombs. However, an inherent weakness ofthe hair shaft may also contribute to itspathogenesis with a lowered threshold levelof susceptibility to trauma.
Both pili anulati and androgenetic alope-cia per se are not associated with increasedhair fragility, but the progressive reductionof hair shaft diameter due to androgeneticalopecia in combination with the abnormali-ty of pili anulati may cause hair shaft fractur-ing within the areas of hair shaft cavities fol-lowing seemingly inadequate trauma. Corre-spondingly, fractures typical of secondarytrichorrhexis nodosa colocalize both with theanatomic region of androgenetic alopeciaand with the air-filled cavities of pili anu-lati.
Elastomechanical parameters in patientNo. 1 showed changes typical of androgenet-ic alopecia. To what extent iron deficiencycontributed to weakness of hair in patientNo. 2 cannot be determined. The associationof pili anulati with alopecia areata seen inpatient No. 2 has formerly been reported. Itis thought to be coincidental [6–8].
There is no specific therapy for pili anu-lati, but it can be reasoned that in acquiredhair fragility in pili anulati with androgenet-ic alopecia, specific and early treatment of
androgenetic alopecia using appropriate sys-temic and topical therapy as described else-where [9] may be of benefit. Finally, care ofincreased hair shaft fragility aims at mini-mizing trauma: patients may profit fromshampooing gently using mild detergents incombination with cream-rinse conditioners.Also, conditioners can be used instead ofshampoos. Styling brushes with roundedprongs or wide-toothed combs should re-place hair brushes and their use should berestricted to a minimum. Ultimately, treat-ments involving heat and cosmetic proce-dures, such as permanent waves, hairstraighteners, bleaching and coloring shouldbe avoided, particularly in the androgeneticarea. This should effectively be communi-cated especially to the female patient whotends to treat thinning hair due to androgen-etic alopecia with hair cosmetic procedures.
References
1 Musso LA: Pili annulati. Aust J Dermatol1970;11:67–75.
2 Price VH, Thomas RS, Jones FT: Pili annulati:Optical and electron microscopic studies. ArchDermatol 1968;98:640–647.
3 Cady LD, Trotter M: A study of ringed hair.Arch Dermatol Syphilol (Chic) 1922;6:301–317.
4 Price VH, Thomas RS, Jones FT: MicroscopicStudies of Pili annulati. Congressus Interna-tionalis Dermatologiae XIII. Munich,Springer, 1968.
5 Dawber R: Investigations of a family with piliannulati associated with blue nevi. Trans StJohn’s Hosp Dermatol Soc 1972;58:51–58.
6 Smith SR, Kirkpatrick RC, Kerr JH, MezebichD: Alpecia areata in a patient with pili annula-ti. J Am Acad Dermatol 1995;32:816–818.
7 Iankova R, Savova Y, Tschudomirova K: Pilianulati. Dermatol Monatsschr 1989;175:658–661.
8 Moffitt DL, Lear JT, de Berker DA, PeacheyRD: Pili annulati coincident with alopeciaareata. Pediatr Dermatol 1998;15:271–273.
9 Price VH: Treatment of hair loss. N Engl J Med1999;341:964–973.
Dow
nloa
ded
by:
Lule
a T
ekni
ska
Uni
vers
itet
13
0.24
0.43
.43
- 8/
24/2
013
3:33
:13
AM


























![Frontal fibrosing alopecia: A multicenter review of 355 ... · with androgenetic alopecia [AGA]), symptoms (pruritus, trichodynia), dermoscopy (perifollicular erythema and follicular](https://img.pdfslide.net/doc/110x75/5ebdda55a09b4c70d34c1b7e/frontal-fibrosing-alopecia-a-multicenter-review-of-355-with-androgenetic-alopecia.jpg)