Embed Size (px)
Citation preview

Radiography (2009) 15, 34e39
ava i lab le a t www.sc iencedi rec t .com
journa l homepage : www.e lsev i er . com/ loca te / rad i
Act, scene, agency: The drama of medical imaging
Frederick Murphy*
Department of Medical Imaging, School of Health Science, Unitec NZ, Carrington Road, Mt Albert 92025,Auckland 92025, New Zealand
Received 13 June 2007; revised 6 July 2007; accepted 12 September 2007Available online 24 October 2007
KEYWORDSBehaviour;Dramaturgy;Perceptions;Qualitative;Space analysis;MRI
* Tel.: þ64 098154321x8103; fax: þ6E-mail address: [email protected]
1078-8174/$ - see front matter ª 200doi:10.1016/j.radi.2007.09.006
Abstract This paper investigates the use of a novel research paradigm in order to describepractice and behaviour within the context of magnetic resonance imaging (MRI) departments.Using a thematic analysis of patient and radiographer transcripts, a social model of the inter-actions that can occur is constructed from a theatrical perspective. A review of the social sci-entific literature was undertaken to identify the main concepts associated with this paradigm.Results: Radiographers and patients fitted into the roles and categories, as described by theoriginal philosophers. Behaviour and ritual were seen to be markedly different in the presenceof the patient as opposed to being in the control room. The deliberate ‘acting out’ of roles wasalso revealed in order to maintain self-identity and professional image. Patients provided aninsightful account of their experiences and demonstrated some sophisticated coping strategiesduring the scanning procedure.Conclusion: The use of this alternative qualitative method revealed some very interesting,complex rituals and behaviour patterns amongst the sample of radiographers and theirpatients.ª 2007 The College of Radiographers. Published by Elsevier Ltd. All rights reserved.
Introduction
The purpose of this paper is to explore the behaviouralcharacteristics of a sample of radiographers and patients inthe environment of a magnetic resonance imaging (MRI)department. Using data derived from patient and radiogra-pher interviews, a dramaturgical analysis provides a uniqueinsight into the social interactions and behaviours.
Since radiography emanates from a predominantlyscientific background, the majority of research output
4 098154326.c.nz
7 The College of Radiographers.
has been from a traditional quantitative culture. Further-more, qualitative inquiry within the profession has alsotended to follow a conventional framework.1 The use ofalternative research paradigms can, however, be moreinteresting, novel and important to any professional groupthat seeks to truly understand the behaviour of itsmembers.2
Dramaturgical analysis
The use of theatrical concepts in order to elucidate thesocial world is known as dramaturgy. It is the study ofmeaningful behaviour3 and is seen as a powerful instrumentand a valuable adjunct to the construction of a social reality
Published by Elsevier Ltd. All rights reserved.

Act, scene, agency 35
‘imbued with vitality and wisdom’.2 The initial theory isattributed to the social psychologist, Burke,4 but given en-hanced application and understanding in the work of Goff-man.5 Through micro-sociological analysis and by focussingon the meaning of mundane interaction, a dramaturgical ap-proach will Ausdrucken (squeeze out) understanding, andbecome liberating to patients and healthcare professional.6
Brissett and Edgley3 also reinforced the point that it is de-scriptive understanding, not explanation, that is the focusof this analysis.
Literature review
Although there is significant literature on the use ofdramaturgical analyses in social psychology and anthropo-logical studies, an understanding of the basic tenets ofthis paradigm and its associated, often tentative, links tohealthcare are not well described within the literature.Fig. 1 shows a basic framework for dramaturgy with every-day examples from Goffman’s studies. Each component isthen considered from a medical imaging perspective.
Goffman7 spoke of the drama of interactions that occurwithin the ‘total institution’ which he defined as a placewhere the subject is cut-off from significant others fora period of time and control is enabled by a few powerfulindividuals.
Although many of his studies where conducted in varioussocial settings, the parallels with a patient lying alonewithin an MRI scanner controlled by radiographers areimmediately apparent.
Institutionalisation
Where an individual is cut offfrom the significant other within aclosed system. Hospitalisation iscited as a prime example ofinstitutionalisation. A fewpowerful individuals maintaintotal control. This disempowersself.
Impression Management
Goffman also called theseanticipatory skills. By usingappearance and manner wemanage others’ impressions ofus. These are usually non –verbal expressions that signal ourintent.
Dramatu
Figure 1 The central tenets of a dramaturgical framewo
Space analysis
The process of establishing social identity is linked to whatGoffman referred to as the ‘front regions’ and the ‘backregions’, by analogy with frontstage and backstage in thetheatre.8 The frontstage is described as: a regular and fixedpart of an individuals’ performance. It is the proper settingwhere the actor must fulfil the ‘duties’ of their social roleand communicate the activities and characteristics of therole to other people in a consistent manner.9 Backstagemay be defined as a place ‘relative to a given performance,where the impression fostered by the performance is know-ingly contradicted as a matter of course’.10 While in thebackstage, workers can relax and do not have to conformto expected frontstage rules8: it is therefore an area wherethe impression fostered by the performance is intentionallycontradicted.11 A distinctive feature is the restrictive ac-cess of the audience to the ‘backstage’, although literaturespeaks of a barrier in terms of audience perceptions, veryoften a physical barrier is evident. Goffman7 characteriseswhat he calls the ‘language of backstage’ behaviour such asreciprocal first naming, profanity, shouting, hummingand whistling. This is arguably, a more truthful type ofperformance.
It would seem apparent that any area where patientsand visitors are present, such as wards, clinics8 and presum-ably X-ray rooms would be frontstage. By the same tokenstaffrooms and radiology console rooms would be back-stage. Although radiographers may not consciously thinkabout their roles as being part of a performance, each
Space Analysis
The different styles of behaviourand language used when ‘actingout’ the performance with anaudience present (front stage) oran audience absent (backstage).
Role Distance
Deliberately maintaining adistance in order to complete thedrama. This usually has anulterior motive and may beassociated with deviant behaviourby the actors.
rgy
rk (based on the work of Erving Goffman 1922e1982).

36 F. Murphy
radiological investigation can be considered to have anact, scene, and agency. When each imaging procedure isconsidered to be a well-rehearsed series of actions andinstructions carried out within a specific time frame, theparallels with a ‘drama’ start to become more apparent.
If, as suggested, the outer self is the pretending self12
then radiographers and patients ‘act out’ their roles duringthe imaging procedure.
It is, however, not just an individual performance, sinceworking closely with our colleagues, the imaging team tryto present the most appropriate image of the departmentand indeed the profession. As part of this role radiographersare expected to perform the rituals of the team and todeviate from these could reveal what Charon11 calls the‘dark secrets’ of the team.
Impression management
The roles that are performed are designed to create a scenethrough what Goffman calls ‘impression management’ orour presentation to the audience. Typically this is front-stage behaviour, and in order to preserve this peopledevelop ‘anticipatory skills’ to cope with the demands ofthe unfolding drama. One facet of this would be ‘responsecries’, whereby a person indicates their displeasure orawkwardness in a situation in a covert fashion, hoping thatthe significant other will pick up on it. By doing this they arenot disturbing the flow of the drama. Patients moving in thescanner or trying to attract the attention of the radiogra-pher might be a type of response cry.
Role distance
Role distance is a situation when an individual is consciously‘playing with a role’, they have knowingly established an‘inner-distance’ between themselves and the role playing.3
This establishes a role that may be void of meaning andwith concealed purpose. According to Goffman7 they havenow two choices; to change the direction in which theencounter is developing, or to cease playing the role alto-gether. If social reality is dramatically created, it will prob-ably also be dramatically malleable.7 Like stage actors,social actors enact roles, assume characters, and playthrough scenes when engaged in interaction with oneanother. Both require the necessary props (medical tech-nology), dialect (medical terminology), and costumes (uni-forms and gowns) to produce a ‘shared experience andsense of reality’.11
Dramaturgical studies
Inspired by the early works of Goffman, Emerson wrote Be-haviour in Private Places: Sustaining Definitions of Realityin Gynecological examinations.13 This is a fascinating ac-count of the true patient experience and a compulsoryread for sonographers. Upon initial reading of the drama-turgical literature, few other studies have any obviouslink with radiology. However, one seminal dramaturgicalaccount that can be associated to medical imaging is thework of Davis14 who wrote a paper entitled: The Cabdriverand his Fare: Facets of a Fleeting Relationship. In this studythe interactions between the passenger (institutionalised)
and the car driver (actor) were analysed from the perspec-tive of a drama.
It has been a concern of Bowman15 that radiographersalso have a ‘fleeting relationship’ with patients; in factReeves16 goes further in describing radiographers as ‘hitand run carers’, for the same reason. Although radiogra-phers’ do not, as would be expected, fit into Davis’s14 de-scription of cabdrivers daily routines, the situation is nottoo dissimilar in the following respect:
The .day consists of a long series of brief contacts withunrelated persons of whom [he] has no foreknowledge,just as they [passengers or patients] have none of him,and whom he is not likely to encounter again.3
It is appreciated that radiographers may know somepatients who will have been scanned before, and mayreturn, but generally the statement could be applied to therole of the radiographer. The patient will have beenreferred for a radiological examination by a ‘named physi-cian’, to whom they will return for the results. From thisperspective the production of the image is seen as ‘a meansto an end’, like the identity of the cabdriver, and theindividuals in the white uniform are, as Goffman7 cate-gories them, as ‘‘non-persons.’’
Just as the identity and ‘self’ of the person who takesa passenger from point A to point B is unimportant sincearriving safely and within a time frame is the only realaim,14 getting a clear diagnosis in a safe environment is theimportant factor for the patient, and not the identity and‘self’ of the radiographer. The role of the radiographer,or more precisely the sonographer in Cussins’ study,17 wasseen as being important in directing the procedure andgiving support; in this respect Cussins derived the term ofontological (reality and existence) choreographers (perfor-mance directors) for the sonographers in his anthropologi-cal research.
Dramaturgical studies in healthcare
Related work in medicine and nursing has focussed on theinteractions in theatre, not the metaphorical theatre in thiscase, but the hospital operating theatre.6,8,18 They all rec-ognise the frontstage behaviour before the patient is givenanaesthetic as opposed to the backstage behaviour after-wards. Here again the patient is totally institutionalisedand some of the basic tenets of dramaturgy are apparent.Holmes6 considered it to be a very exciting and novel ap-proach to the study of nursing. Although acknowledged,he does avoid the many criticisms levelled at Goffman, es-pecially with regard to the cynical view of relationships.Holmes concluded his thoughts by stating that dramaturgi-cal analysis provides fresh insight into practice and rela-tionships. Meanwhile, Tanner and Timmons,8 also nurses,concentrated only on a space analysis which producedsome interesting, if somewhat controversial, findings.
Method
As part of a much larger study,19 radiographers and patientswere interviewed about their role in the MRI scanning pro-cedure. Following ethical approval, a convenience sample

Act, scene, agency 37
of 22 patients and eight radiographers were interviewed.The transcripts were then studied using a thematic analysisas described by Burnard,20 and following immersion in thedata dramaturgical concepts were extrapolated.
In line with most qualitative studies, rigour was main-tained through reflection and reflexivity.21
Interviews, rather than observations, were the chosenmethod of data collection since the actions and behaviourof the patients could not be seen within the confines ofa scanner. In order to construct the true reality of thepatient experience it was essential to obtain the emic(inside) perspective. Conversely, radiographer interviewswere chosen to provide ‘shadowed data’22 on the range ofexperiences and the domain of the phenomena beyond thesingle participant’s personal experience. Although partici-pant observations may have revealed additional data onthe radiographers’ roles, ethical restrictions on gainingfrequent access to a very busy unit prevented this at thetime of the study.
Results and discussion
Many dramaturgical themes were derived from the data.The frontstage (MR room) and backstage (control room)locations were readily identified by both patients andradiographers. Whilst the physical barrier made this moreapparent, the behaviour and language were also markedlydifferent. The language and terminology of backstage werea regular feature of the radiographers working perfor-mance. Although patients were unaware of the backstagelanguage, they did note a small amount of ‘unprofessionalbehaviour’ such as radiographers drinking coffee and havingtheir feet up. They recognised that these were rituals thatwould never be exhibited on frontstage. It was interestingto note that if radiographers had had scans elsewhere, theywere more critical of their colleagues behaviour. It isthought that this was the case because they were fullyaware of the script and the unfolding drama, i.e. they knewwhat to look for.
Space analysis
There were many examples of backstage performanceparticularly evident in the radiographer transcripts. Theyincluded examples of communicating with the patient inthe scan room (frontstage) in a professional manner andthen going into the control room and speaking about thepatient in disparaging terms.
As far as frontstage performance was concerned, thevast majority of patients recognised the high professionalstandards that were evident in the MR room and radiogra-phers felt compelled to present a good image of themselvesand the department.
Rituals and dark secrets
A couple of examples of the imaging team protectinga ‘dark secret’11 were evident, in one case the radiogra-phers were knowledgeable of the patient’s condition butpretended not to know, or in another situation, informingthe patient that the scanner was operating on-time when
they all knew there were problems that may delay theexamination. Within dramaturgy these are both forms ofdeviant behaviour, which may be hidden by the sophisti-cated performance of the imaging team.
Non-persons
Some radiographers identified with the concept of ‘non-persons’ with their role. For instance, one remarked that[radiographers] are not permitted to disclose the result ofthe scan to the patient, he said, ‘I’m not allowed to speakto patients in that way, I just do my bit’. Other referencessuggested a diminished role in the medical team such as‘you are [just] a radiographer’. The most appropriateconcepts were the obvious lack of professional identity,so striking within the patient interviews, where the major-ity assumed that radiographers were nurses or doctors.According to the radiographers in this sample, this alsocontributed to poor self-definition and the belief held bymany external bodies, that the scanning process wasa simple task. As one noted, ‘it must appear to othersthat we are not doing anything other than pressing the oddbutton’. He continued using a most coincidental metaphorby saying, ‘in reality we are running the whole show’.However, the impression that radiographers only explainthe process, take the scan, and then sent the patientstraight back to the clinician, clearly showed the transientnature of the ‘hit and run carers’,16 within the patienteradiographer interaction.
The total institution
Being confined to a narrow bore of the magnet under thetotal control of the radiographers, matched perfectly withGoffman’s definition of the total institution,7 patientsspoke of the deliberate use of coping strategies such asclosing of eyes, counting, and singing which can be consid-ered to be analogous to the ‘anticipatory survival’ recog-nised by Goffman.7 This would also be another form ofself-regulated participation and impression management.
The radiological performance
The role of the radiographer was central in preparingpatients for the examination with advice, support andcoping methods, which would all be classified as anticipa-tory skills.7 This preparation typically included the wearingof the hospital gown, thus removing some patient self-image, before bringing them into a strange technologicalenvironment. Once in the frontstage, they introduced thepatient to the technology as advocated by Bowman,15 andwith the explanation, which can be assumed to have beensymbolic, since the vast majority claimed to have under-stood it, they effectively rehearsed the requirements forthe performance (positions and breathing instructions).Any isolation or objectification only occurred once theradiographer had retreated to the backstage, leaving thepatient alone to have the scan performed within a tempo-rary ‘total institution’. In the words of one patient ‘theygreet you, you get ready, you go into the room and theyare gone’. Regular communication to the frontstage was
38 F. Murphy
variable, varying from physical touch, to words of encour-agement. However, unlike other true dramaturgical studies,the patient, although on frontstage, was not in control ofthe proceedings, whilst they had a part in the interactionwith the radiographer and the scanner when necessary,the total control remained with the radiographer. This in-cluded the relaying of breathing instructions, operatingthe movements of the scanner, and giving a final count-down to the end of the performance. Radiographers are inthis role, most appropriately, meeting with the definitionof ontological choreographers.17
The dramaturgical perspective was confirmed witha theatrical metaphor from a radiographer who noted‘they [patients] do not know what goes on behind thescenes’. There is evidence when considered from thisperspective, to suggest that the role of the patient isanything but passive. The acting back and forth referred toearlier, can be viewed as a form of deliberate enactmentswhich were intended to focus the attention of the radiog-rapher onto the patient. If patients knew they were beingobserved, then the closing of eyes or verbal expressions ofdiscomfort could be seen as ‘hints’ of displeasure known as‘response cries’.7 An example was given by a patient whowanted get out of the scanner and normally kept his eyesclosed. He said:
I looked for the radiographers this time since I could seethem in the mirror.I think I might have done it for a rea-son actually.I was kind of hoping that she would get up,and then I thought if she gets up she will be coming toget me out.
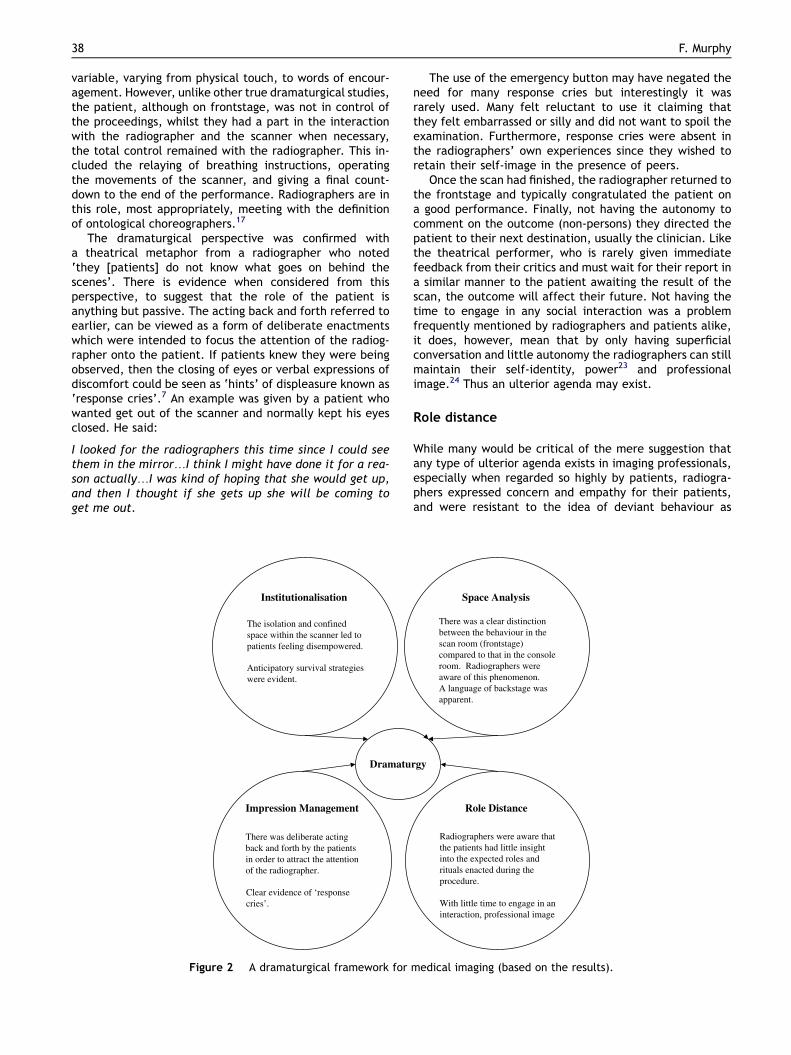
Institutionalisation
The isolation and confinedspace within the scanner led topatients feeling disempowered.
Anticipatory survival strategieswere evident.
Impression Management
There was deliberate actingback and forth by the patientsin order to attract the attentionof the radiographer.
Clear evidence of ‘responsecries’.
Dramatu
Figure 2 A dramaturgical framework for
The use of the emergency button may have negated theneed for many response cries but interestingly it wasrarely used. Many felt reluctant to use it claiming thatthey felt embarrassed or silly and did not want to spoil theexamination. Furthermore, response cries were absent inthe radiographers’ own experiences since they wished toretain their self-image in the presence of peers.
Once the scan had finished, the radiographer returned tothe frontstage and typically congratulated the patient ona good performance. Finally, not having the autonomy tocomment on the outcome (non-persons) they directed thepatient to their next destination, usually the clinician. Likethe theatrical performer, who is rarely given immediatefeedback from their critics and must wait for their report ina similar manner to the patient awaiting the result of thescan, the outcome will affect their future. Not having thetime to engage in any social interaction was a problemfrequently mentioned by radiographers and patients alike,it does, however, mean that by only having superficialconversation and little autonomy the radiographers can stillmaintain their self-identity, power23 and professionalimage.24 Thus an ulterior agenda may exist.
Role distance
While many would be critical of the mere suggestion thatany type of ulterior agenda exists in imaging professionals,especially when regarded so highly by patients, radiogra-phers expressed concern and empathy for their patients,and were resistant to the idea of deviant behaviour as
Space Analysis
There was a clear distinctionbetween the behaviour in thescan room (frontstage)compared to that in the consoleroom. Radiographers wereaware of this phenomenon.A language of backstage wasapparent.
Role Distance
Radiographers were aware thatthe patients had little insightinto the expected roles andrituals enacted during theprocedure.
With little time to engage in aninteraction, professional image
rgy
medical imaging (based on the results).

Act, scene, agency 39
undermining professional integrity. However, as Goffman,7
recognised, if social reality is dramatically created, it willalso be dramatically malleable. The deliberate ‘acting outof a role’ would then be for ulterior motives. Being awarethat the patients cannot see or hear the radiographers,may, it was suggested, facilitate elements of unprofes-sional behaviour.
The results were transposed onto the original frameworkto give a dramaturgical model for the interactions that canexist with the arena of medical imaging. This is demon-strated in Fig. 2.
Dramaturgical analysis within medical imaging
Although radiographers may not consciously think abouttheir roles as being part of a performance, each radiologicalinvestigation can be considered to have an act, scene, andagency. When each imaging procedure is considered to bea well-rehearsed series of actions and instructions carriedout within a specific time frame, the parallels with a ‘drama’start to become more apparent. Such a study is not limitedto MR departments since interactions occur in all modali-ties. The analysis provides new insight into the roles thatstaff plays according to their personalities, expectationsand role patterning within the group.25 This understandingwill also facilitate awareness of behaviour, and thereby fos-ter the ability to accept different ways of interacting.
Equally, any research that can provide insight into thetrue patient experience is invaluable to the profession.Further knowledge on how patients perceive medicalimaging procedures and radiographers’ roles can only leadto improved communication and understanding.
Conclusion
As medical imaging equipment continues to evolve ina rapidly changing technological world, radiographers mustbe increasingly aware of the social phenomena, as well asthe scientific facts that surround radiological procedures.
The physical lay-out of the scan room lends itselftowards a space analysis, where the scan room is the stagefor the performance and the control room is the backstagechoreography. Just like a theatre production, all mayappear fine and under control at the front whilst thebackstage team are dealing with all the issues.
It is only by appreciating these, and identifying ‘roles’and ‘self’, that the profession can hope to fully understandthe humanistic interactions that exist in medical imagingprocedures.19
References
1. Adams J, Smith T. Qualitative methods in radiography re-search: a proposed framework. Radiography 2003;9:193e9.
2. Massey G. The drama of social life: essays in critical drama-turgy. Dramaturgical Society, <www.tryoung.com/dramasociallife/004dramaturgicalsociety.html>; 1990 [accessed12.02.01].
3. Brissett D, Edgley C, editors. Life as theatre: a dramaturgicalsourcebook. Chicago: Aldine Publishing Company; 1975.
4. Burke K. A grammar of motives. In: Life as theatre: a dramatur-gical sourcebook. Chicago: Aldine Publishing Company; 1950.1975.
5. Goffman E. On the face work. New York: Doubleday; 1967.6. Holmes CA. The drama of nursing. J Adv Nurs 1992;17:941e50.7. Goffman E. The presentation of self in everyday life. London:
Penguin Books; 1959.8. Tanner J, Timmons S. Backstage in the theatre. J Adv Nurs
2000;32(4):975e80.9. Barnhart A. Erving Goffman: the presentation of self in everyday
life, <http://www.hewett.norfolk.sch.uk/curric/soc/goffman.htm>; 2000. p. 1e11 [accessed 06.09.2000].
10. Goffman E. Strategic interaction. University of PennsylvaniaPress; 1969.
11. Charon J. Symbolic interactionism: an introduction, an inter-pretation, an integration. 7th ed. New Jersey: Prentice Hall;2001.
12. Morrison P, Burnard P, editors. Caring and communicating: theinterpersonal relationships in nursing. London: Mac MillanEducation Limited; 1991.
13. Emerson J. Behaviour in private places: sustaining definitionsof reality in gynaecological examinations. Recent Sociology1979;2:74e97.
14. Davis F. The cabdriver and this fare: facets of a fleetingrelationship. Am J Sociol 1959 September;65:158e65.
15. Bowman S. The radiographer/patient relationship e a shortterm but vital interaction. Radiogr Today 1993;59(675):17e8.
16. Reeves PJ. Models of care for diagnostic radiography and theiruse in the education of undergraduate and postgraduatestudents. PhD thesis. Bangor: University of Wales; 1999.
17. Cussins C. Ontological choreography: agency through ob-jectification in infertility clinics. Soc Stud Sci 1996;26:575e610.
18. Mc Garvey H, Chambers M, Boore J. Development and defini-tion of the role of the operating department nurse: a review.J Adv Nurs 2000;32(5):1092e100.
19. Murphy FJ. Understanding the humanistic interaction withmedical imaging technology. PhD thesis. Bangor: University ofWales; 2003.
20. Burnard P. A method of analysing interview transcripts inqualitative research. Nurse Educ Today 1991;11:461e6.
21. Hammersley M. The dilemma of the qualitative method.London: Routledge; 1989.
22. Morse J. Critical issues in qualitative research methods.Thousand Oaks: Sage; 1994.
23. Jones L. The social context of health and health work.Hampshire: Palgrave; 1994.
24. Simon CM. Images and image: technology and the social politicsof revealing disorder in a North American hospital. MedAnthropol Q 1999;13:141e62.
25. Hays M, Weinert C. A dramaturgical analysis of shift report pat-terns with cost implications: a case study. Nurs Econ Sept/Oct2006;24(5):253e61.