Embed Size (px)
Citation preview
Acta Gastroenterológica Latinoamericana
ISSN: 0300-9033
Sociedad Argentina de Gastroenterología
Argentina
Moreno, Eduardo Antonio; Cickman, Pablo; Azar, Ricardo; Feliu, Luis; Nari, Gustavo Adrián
Intestinal intussusception in adults: Tomographic findings and report of two cases
Acta Gastroenterológica Latinoamericana, vol. 43, núm. 2, junio-enero, 2013, pp. 126-129
Sociedad Argentina de Gastroenterología
Buenos Aires, Argentina
Available in: http://www.redalyc.org/articulo.oa?id=199327532010
How to cite
Complete issue
More information about this article
Journal's homepage in redalyc.org
Scientific Information System
Network of Scientific Journals from Latin America, the Caribbean, Spain and Portugal
Non-profit academic project, developed under the open access initiative

126 Acta Gastroenterológica Latinoamericana - Vol 43 / Nº 2 / Junio 2013
♦caso clínico
Intestinal intussusception in adults: Tomographic findings and report of two cases Eduardo antonio Moreno,1 Pablo cickman,2 Ricardo azar,1 luis Feliu,1 Gustavo adrián nari 1
1 General SurgeryService, Clínica Sucre; 2 Diagnostic ImagingService,Conci-Carpinella; Córdoba, Argentina.3 General Surgery Service, Hospital Florencio Diaz, Cordoba . Argentina
Acta Gastroenterol Latinoam 2013;43:126-129
Summary
Intestinal intussusception is infrequent in adults. Unlike what happens in kids, it shows a demonstrable etiology in most cases: polyps, lipomas, hamartomas, malignancies, etc. Among diagnostic methods, CT scan is the study that yields the best results for the diagnosis, giving forth pathognomonic signs and favoring therapeutic decision-making.Two cases of intestinal intussusception in adults secondary to benign pathology are analyzed, stressing mainly the tomo-graphic findings and some considerations about therapeutic decision-making based on tomographic results.
Key words. Adult intestinal itussusception, CT findings, treatment.
Intususcepción intestinal en adultos: Hallazgos tomográficos y comunicación de dos casos
Resumen
La intususcepción intestinal en el adulto es poco frecuente. Al contrario de lo que sucede en los niños, en los adultos existe una etiología demostrable en un alto porcentaje: pólipos, li-pomas, hamartomas, enfermedad maligna, etc. Dentro de los métodos complementarios de diagnóstico, la tomografía com-putada es el estudio que presenta los mejores resultados, con signos patognomónicos y favoreciendo la toma de decisiones terapéuticas. Se presentan dos raros casos de intususcepción en adultos secundarios a patología benigna, haciendo princi-pal hincapié en los hallazgos tomográficos y en las considera-ciones terapéuticas consecuentes a los mismos.
Palabras claves. Intususcepcion intestinal del adulto, ha-llazgos tomográficos, tratamiento.
The invagination of part of the intestine into another sec-tion of intestine is known as intestinal intussusception. Most cases happen in kids and about 90% have idiopathic origin. This is the most frequent cause of acute abdomen in this age group, after appendicitis.1 The appearance of intussus-ception in adults is rare: only 1% of intestinal obstructions are due to this cause and, unlike what occurs in childhood, about 90% of cases have a demonstrable etiology.1-3
Nevertheless, in most observations in adults, the symp-toms tend to come in a chronic, overlapped manner, so that the diagnosis can be suspected in only few occasions. Abdominal pain, nausea and vomiting are usually the most frequent symptoms and, to a lesser extent, melena, anemia, gastro-intestinal bleeding, diarrhea, fever, weight loss and constipation. The causes of intussusception in adults vary according to the affected intestine section. In the colon, malignancies occur most frequently, whereas in the small intestine, benign tumors prevail (lipomas, hamartomas, leiomyomas, hemangiomas, neurofibromas, diverticula, lymphoid hyperplasia, mesenteric adenitis, trauma, celiac disease, intestinal duplication, HenochSchönleinpurpura). Melanoma metastases are the most frequent malign cause for invagination of the small intestine. Furthermore, a high rate of patients with AIDS is reporteddue to the increased number of tumors such as Kaposi’s sarcoma and infections with lymphoid affection.2-6
Even though different diagnostic methods are used, in-cluding simple abdominal X-rays, ultrasound scan and con-trast studies, CT scan (computed tomography) is the method with the best diagnosis accuracy andthe best evidenceof the pathognomonic signs typical of this pathology.4,6-14 The goal of this paperis to present two cases of ileo-ileal invagination secondary to benign polypoid lesions that were diagnosed by CT scan and to update the tomographic findings.
Case report
Case 1
A 29-year-old female seeks medical advice due to con-tinous epigastric pain irradiated to the back, set in in the last 24 hours. She refers a history of colic abdominal pain
Correspondence: Gustavo Adrián NariServicio de Cirugia, Hospital Florencio Diaz. Av 11 de Setiembre 2900 - 5000.Cordoba - ArgentinaE-mail: [email protected]
127Acta Gastroenterológica Latinoamericana - Vol 43 / Nº 2 / Junio 2013
Intestinal intussusception in adults: Tomographic findings and report of two cases Eduardo Antonio Moreno y col
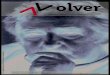
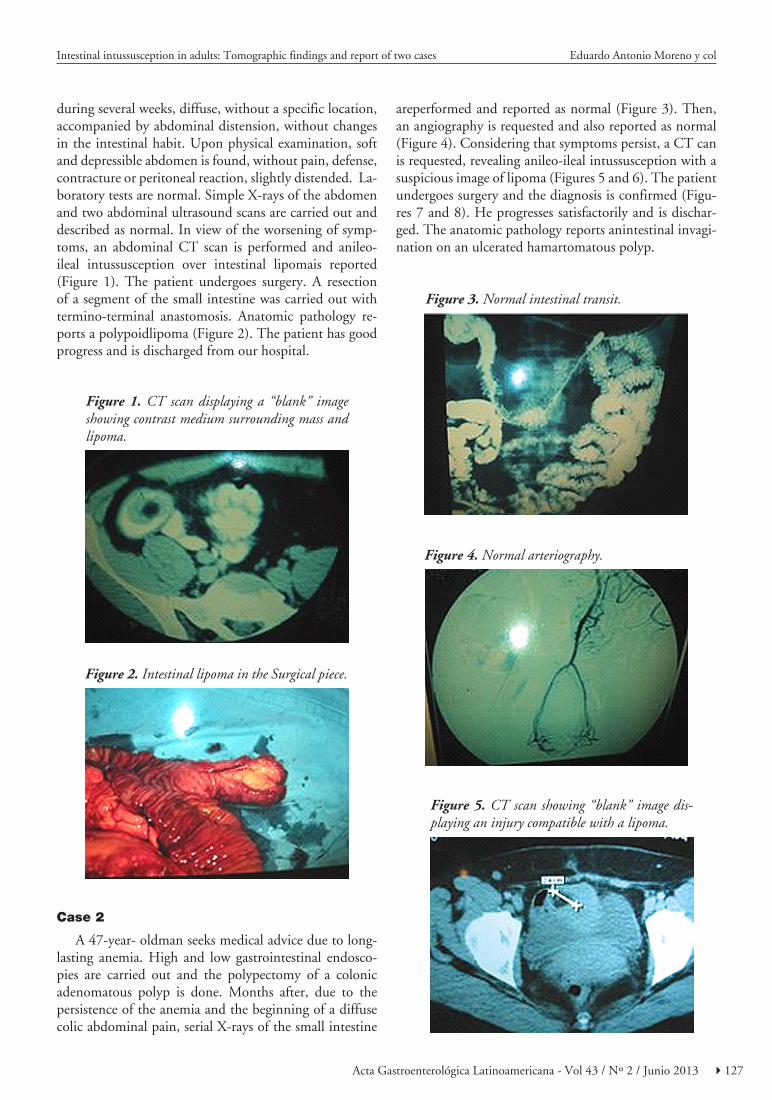
during several weeks, diffuse, without a specific location, accompanied by abdominal distension, without changes in the intestinal habit. Upon physical examination, soft and depressible abdomen is found, without pain, defense, contracture or peritoneal reaction, slightly distended. La-boratory tests are normal. Simple X-rays of the abdomen and two abdominal ultrasound scans are carried out and described as normal. In view of the worsening of symp-toms, an abdominal CT scan is performed and anileo-ileal intussusception over intestinal lipomais reported (Figure 1). The patient undergoes surgery. A resection of a segment of the small intestine was carried out with termino-terminal anastomosis. Anatomic pathology re-ports a polypoidlipoma (Figure 2). The patient has good progress and is discharged from our hospital.
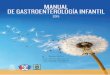
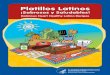
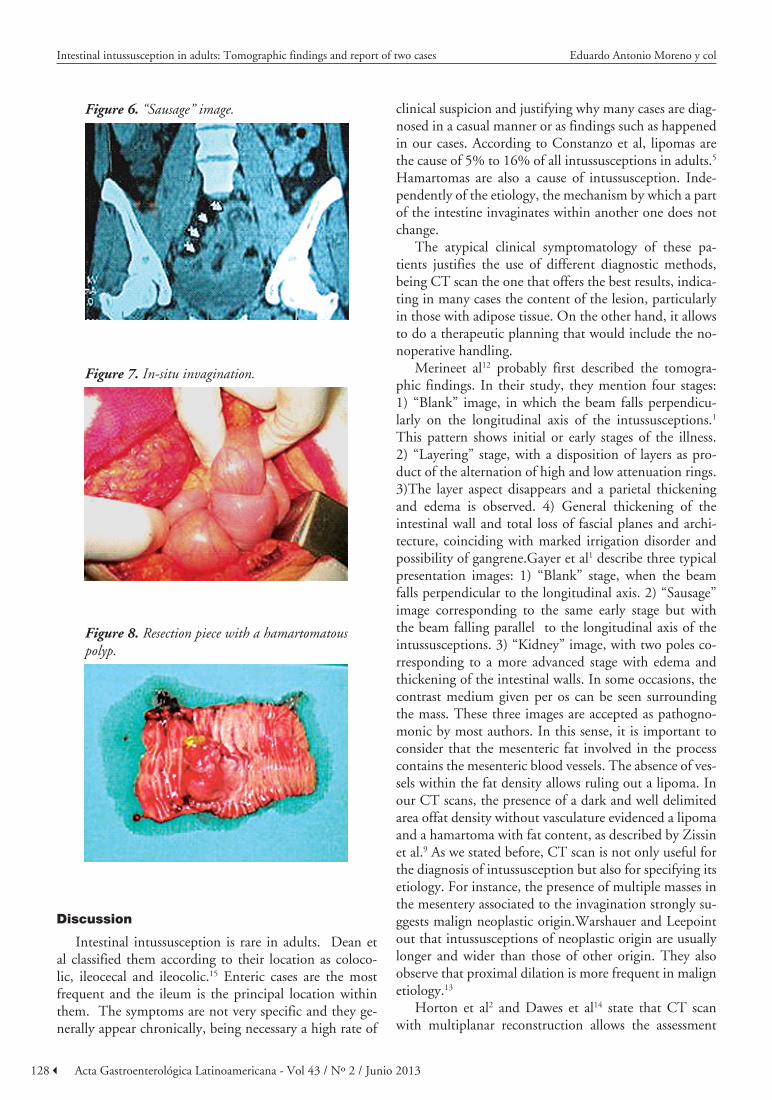
areperformed and reported as normal (Figure 3). Then, an angiography is requested and also reported as normal (Figure 4). Considering that symptoms persist, a CT can is requested, revealing anileo-ileal intussusception with a suspicious image of lipoma (Figures 5 and 6). The patient undergoes surgery and the diagnosis is confirmed (Figu-res 7 and 8). He progresses satisfactorily and is dischar-ged. The anatomic pathology reports anintestinal invagi-nation on an ulcerated hamartomatous polyp.
Figure 5. CT scan showing “blank” image dis-playing an injury compatible with a lipoma.
Figure 1. CT scan displaying a “blank” image showing contrast medium surrounding mass and lipoma.
Figure 2. Intestinal lipoma in the Surgical piece.
Case 2
A 47-year- oldman seeks medical advice due to long-lasting anemia. High and low gastrointestinal endosco-pies are carried out and the polypectomy of a colonic adenomatous polyp is done. Months after, due to the persistence of the anemia and the beginning of a diffuse colic abdominal pain, serial X-rays of the small intestine
Figure 3. Normal intestinal transit.
Figure 4. Normal arteriography.
128 Acta Gastroenterológica Latinoamericana - Vol 43 / Nº 2 / Junio 2013
Intestinal intussusception in adults: Tomographic findings and report of two cases Eduardo Antonio Moreno y col
Discussion
Intestinal intussusception is rare in adults. Dean et al classified them according to their location as coloco-lic, ileocecal and ileocolic.15 Enteric cases are the most frequent and the ileum is the principal location within them. The symptoms are not very specific and they ge-nerally appear chronically, being necessary a high rate of
clinical suspicion and justifying why many cases are diag-nosed in a casual manner or as findings such as happened in our cases. According to Constanzo et al, lipomas are the cause of 5% to 16% of all intussusceptions in adults.5 Hamartomas are also a cause of intussusception. Inde-pendently of the etiology, the mechanism by which a part of the intestine invaginates within another one does not change.
The atypical clinical symptomatology of these pa-tients justifies the use of different diagnostic methods, being CT scan the one that offers the best results, indica-ting in many cases the content of the lesion, particularly in those with adipose tissue. On the other hand, it allows to do a therapeutic planning that would include the no-noperative handling.
Merineet al12 probably first described the tomogra-phic findings. In their study, they mention four stages: 1) “Blank” image, in which the beam falls perpendicu-larly on the longitudinal axis of the intussusceptions.1 This pattern shows initial or early stages of the illness. 2) “Layering” stage, with a disposition of layers as pro-duct of the alternation of high and low attenuation rings. 3)The layer aspect disappears and a parietal thickening and edema is observed. 4) General thickening of the intestinal wall and total loss of fascial planes and archi-tecture, coinciding with marked irrigation disorder and possibility of gangrene.Gayer et al1 describe three typical presentation images: 1) “Blank” stage, when the beam falls perpendicular to the longitudinal axis. 2) “Sausage” image corresponding to the same early stage but with the beam falling parallel to the longitudinal axis of the intussusceptions. 3) “Kidney” image, with two poles co-rresponding to a more advanced stage with edema and thickening of the intestinal walls. In some occasions, the contrast medium given per os can be seen surrounding the mass. These three images are accepted as pathogno-monic by most authors. In this sense, it is important to consider that the mesenteric fat involved in the process contains the mesenteric blood vessels. The absence of ves-sels within the fat density allows ruling out a lipoma. In our CT scans, the presence of a dark and well delimited area offat density without vasculature evidenced a lipoma and a hamartoma with fat content, as described by Zissin et al.9 As we stated before, CT scan is not only useful for the diagnosis of intussusception but also for specifying its etiology. For instance, the presence of multiple masses in the mesentery associated to the invagination strongly su-ggests malign neoplastic origin.Warshauer and Leepoint out that intussusceptions of neoplastic origin are usually longer and wider than those of other origin. They also observe that proximal dilation is more frequent in malign etiology.13
Horton et al2 and Dawes et al14 state that CT scan with multiplanar reconstruction allows the assessment
Figure 6. “Sausage” image.
Figure 7. In-situ invagination.
Figure 8. Resection piece with a hamartomatous polyp.

129Acta Gastroenterológica Latinoamericana - Vol 43 / Nº 2 / Junio 2013
of ischemia, an important feature when the therapeutic approach is decided. Furthermore, CT scan is not only a diagnostic tool but also allows assuming an expectant be-havior with medical management of the intussusception. For instance, an invagination shorter than 3.5 cm would not require surgical treatment and would most likely have a spontaneous resolution, particularly in an asymptoma-tic patient. In this sense, Catalano et al7 and Rea et al10 recommend to avoid a surgical procedure when a “blank” shape is detected in the CT scan, with not or slightly di-lated proximal handles and without an apparent cause of invagination, in an asymptomatic patient. In this sense, considering that a demonstrable underlying cause of in-tussusception is found in around 90% of adult cases, the-se patients will require a surgical procedure anyway.
We conclude that intestine intussusceptions are rare in adult patients and generally the clinic picture is not typical, except when acute obstructive episodes are pre-sent. Currently, the CT scan is the best study for its diagnosis, contributing with typical and pathognomonic images,specifying the etiology and severity of the process ,and being of critical importance when a therapeutic de-cision is required.
References
1. Gayer G, Apter S, Hofmann C, Nass S, Amitai M, Zissin R, Hertz M. Intussusception in adults: CT diagnosis.ClinRadiol 1998;53:53-57.
2. Horton K, Fishman E. MDCT and 3D imaging in transient ente-roenteric intussusception: clinical observations and review of the literature. AJR Am J Roentgenol2008;191:736-742.
3. Akagi I, Miyashita M, Hashimoto M, Makino H, Nomura T, Tajiri T. Adult intussusceptions caused by an intestinal lipoma; report of a case. J Nippon Med Sch 2008,75:166-170.
4. Nincheri Kunz M, Evaristi L, Spadoni R, Cozzani R, Valle O, Bacigalupo B.Lipoma of the small intestine as a rare cause of in-testinal occlusion.Minerva Chir1994;49:859-865.
5. Constanzo A, Patrizi G, Cancrini G, Fiengo L, Toni F, So-lai F, Arcieri S, Giordano R. Double ileo-ileal and ileo-ceco-colic intussusception due to submucouslipoma: case report.G Chir2007;28:135-138.
6. Farrokh D, Saadaoui H, Hainaux B. Contribution of imaging in intestinal intussusception in the adult. Apropos of a case of ileoco-lic intussusception secondary to cecallipoma.Ann Radiol (Paris) 1996;39:213-216.
7. Catalano O. Transient small bowell intussusception: CT findings in adults. Br J Radiol 1997;70:805-808.
8. Oyen TL, Wolthuis AM, Tollens T, Aelvoet C, Vanrijkel JP. Ileo-ileal intussusception secondary to a lipoma: a literature review.ActaChirBelg 2007;07:60-63.
9. Zissin R.Enteroenteric intussusception secondary to a lipoma: CT diagnosis.EmergRadiol 2004;11:107-109.
10. Rea JD, Lockhart ME, Yarbrough DE, Leeth RR, Bledsoe SE, Clements RH. Approach to management of intussusception in adults: a new paradigm in the computed tomography era.Am Surg 2007;73:1098-1105.
11. McKay R.Ileocecal intussusception in an adult: the laparoscopic approach.JSLS 2006;10:250-253.
12. Merine D, Fishman E, Jones BB, Siegelman S. Enteroenteric In-tussusception: CT findings in nine patients. AJR Am J Roentge-nol 1987;148:1120-1132.
13. Warshauer DM, Lee JKT. Adult intussusceptions detected at CT or MR imaging: clinical–imagingcorrelation. Radiology 1999;212:853-860.
14. Dawes LC, Hunt R, Wong JK, Begg S. Multiplanar reconstruc-tion in adult intussusception: case report and literature review.AustralasRadiol 2004;48:74-76.
15. Dean DL, Ellis FH, Sauer WG. Intussusception in adults. Arch Surg1956;73:6-11.
Intestinal intussusception in adults: Tomographic findings and report of two cases Eduardo Antonio Moreno y col