Embed Size (px)
Citation preview

Active Learning
Alfred Tenore
Active Learning and the CNUCOM Curriculum

Introductory : Think – Pair – Share
Think of what you know about the meaning of active learning
Turn to a partner and discuss your knowledge
Do you have anything to share with the rest of us (class)?
Experiment : : Think – Pair – Share Experiment : : Think – Pair – Share Experiment : : Think – Pair – Share
End 0 2 1

Active Learning Active Learning and the CNUCOM Curriculum
Outline
1) Introduction
2) “Active Learning”
a) What is it ?
b) Differences between “Padagogy ” and “Andragogy ”
3) Components of Curriculum changes
a) “Teaching”
b) “Learning”
c) “Assessing”
4) Methods used in “Active Learning”
5) Introducing “Active Learning” in the NCUCOM Curriculum
Active Learning Active Learning and the CNUCOM Curriculum
Educational Objectives
Appreciate that some things of the past continue to have value
Discuss what active learning is and is not
List some characteristics that identify “adult learners”
List a variety of methods that reflect active learning
Select appropriate interactive strategies
Reflect on the need to restructure the CNUCOM curriculum
INTRODUCTION
Quotes:
Good quotes help to tell a story . . .
reflect experiences that have withstood the barrier of time
Good quotes help to tell a story . . . and enhance the credibility of what is being said.
reflect experiences that have withstood the barrier of time…… and therefore proven to be true
Great Men have said Great Things !

Great Men have said Great Things !
“Education is not the filling of a pail,
William Butler Yeats
but the lighting of a fire”.
Socrates

Reflections on the Teaching of Medicine
“On the pedagogic side, modern medicine, like all scientific teaching, is characterized by activity. The ‘student’ no longer merely watches, listens, memorizes: he does.
His own activities in the laboratory and in the clinic are the main factors in his instruction and discipline.
Since education nowadays involves both learning and learning how; the ’student’ cannot effectively know, unless he knows how.”
Abraham Flexner (1910)

HISTORY
1) Dr Franciscus de la Boe Sylvius (1614 – 1672)
3) The first to introduce the technique of bedside teaching in medical education
2) Professor of Medicine at the University of Leyden, Netherlands

STORIA
1) Dr William Osler (1849 – 1919)
2) McGill (1875); Philadelphia (1884); Johns Hopkins (1888); Oxford (1905)
(Whitman N (1990) Creative Medical Teaching U Utah Sc Med.)
3) He considered his greatest contribution to medical education the introduction of students on the wards and the elimination of the old system based on formal lectures
4) He believed that students would learn best by "doing“; therefore, clinical education must start with the patient and end with the patient
5) To study the phenomenon of disease without books is like sailing in an uncharted sea, whereas studying from books without patients is not to go at all at sea
The Agnew Clinic, Portrait of David Hayes Agnew,1889 Thomas C. Eakins (1844-1916) Oil on canvas, 74 1/2 x 130 1/2 inches The University of Pennsylvania School of Medicine, Philadelphia, PA
Originally developed by Edgar Dale in 1946
The Future of Medical Education is in Rediscovering the Past
Dale’s “Cone of Experience”
Intended as a way of describing various learning experiences
Dale’s “Cone of Experience”
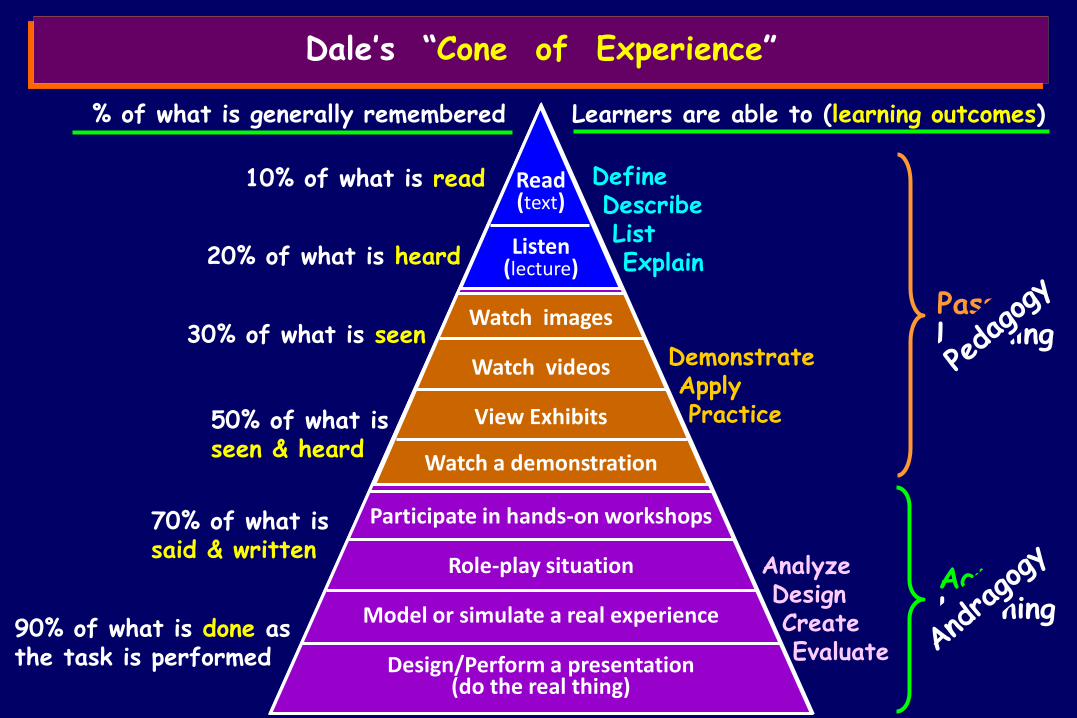
% of what is generally remembered Learners are able to (learning outcomes)
10% of what is read
20% of what is heard
Define Describe List Explain
Read (text)
Listen (lecture)
Watch images 30% of what is seen
Watch videos
View Exhibits
Watch a demonstration
50% of what is seen & heard
Demonstrate Apply Practice
Participate in hands-on workshops
Role-play situation
70% of what is said & written
Model or simulate a real experience
Design/Perform a presentation (do the real thing)
90% of what is done as the task is performed
Analyze Design Create Evaluate
Dale’s “Cone of Experience”
Passive Learning
Active Learning

Originally developed by Edgar Dale in 1946
Dale’s Cone of Experience
Intended as a way of describing various learning experiences
Theorized that learners retain more information by what they “do” as opposed to what is “heard”, “read” or “observed”
The least effective method involves learning from information presented through verbal symbols
i.e., listening to spoken words
The most effective methods involves direct, purposeful learning experiences
i.e., hands-on or field experiences
The Future of Medical Education is in Rediscovering the Past

Originally developed by Edgar Dale in 1946
Dale’s Cone of Experience
Intended as a way of describing various learning experiences
Theorized that learners retain more information by what they “do” as opposed to what is “heard”, “read” or “observed”
Today, this “learning by doing” has become known as:
“experiential learning”
“action learning”
The Future of Medical Education is in Rediscovering the Past

Adapted from Kolb
Experiential learning
Experience
Reflection Apply
Learn
Motivating the mind
Acquiring the necessary information
Utilizing the information
Incorporating in long-term memory
Reflecting on what has been learned
Great Men have said Great Things !
“What we should seek to instill in our colleagues is not so much learning as the spirit of learning”
(Woodrow Wilson)

Points to Remember !
little of the factual knowledge we convey to our pupils is actually retained
If we can convey enthusiasm for the process of learning — the thought, research, and investigation — then we have met an important educational objective
The process of how we learn as physicians eclipses and surpasses the content of any factual data
Promotes thoughtful engagement
“Active learning”
“ACTIVE LEARNING"
What is “Active Learning” ?
Encourages analytical thinking and reasoning
Fosters integration and manipulation of knowledge
Designed to analyze, synthesize, evaluate & apply information
Stimulates the learner to
process
interact
share
experiences as part of the educational process

Seek out learning activities to
“Andragogy” vs “Pedagogy”
“ACTIVE LEARNING"
Reflects what is known about how adults learn…
Enhance their own knowledge
To meet a specific need
Learn best when information is relevant and contextual
Want to apply new information

Pedagogy vs Andragogy
Differences:
Style:
Characteristics Teacher centered
1) The teacher decides what has to be taught and how
( directives & content )
The learner is totally dependant on the teacher
2) The objective of learning is to create the basis of knowledge which may be utilized in the future.
Andragogy Pedagogy Student centered

Student centered
1) The student plays a more active role in deciding what is it that he needs
Develop the competences to use immediately
Applying knowledge
2) The objective of the learning process is primarily directed to:
3) The role of the teacher is one of “facilitator” of the learning process and as a “resource” for the learner
Andragogy
Pedagogy vs Andragogy
Differences:
Style
Characteristics Teacher centered
Pedagogy

Adult learners
assume the responsibility of their own education
Student centered
Andragogy
Pedagogy vs Andragogy
Differences:
Characteristics Teacher centered
Pedagogy

WHY is “ACTIVE LEARNING“ important
Thomas, 1972
Research showed that discussion vs lecture techniques resulted in significant differences in measures of retention of information, problem solving, thinking, attitude change and motivation for further learning, in favor of discussion methods
The amount of information retained by students declines appreciably after 10 minutes
McKeachie, et al, 1987
“All genuine learning is active, not passive. It is a process of discovery in which the student is the main agent, not the teacher.”
Adler, 1982
“One must learn by doing, for though you think you know it – you have no certainty until you try..” Sophocles, 5th Cent BC
“Students learn what they care about and remember what they understand.”
Ericksen, 1984
0
10
20
30
40
50
60
70
80
90
100
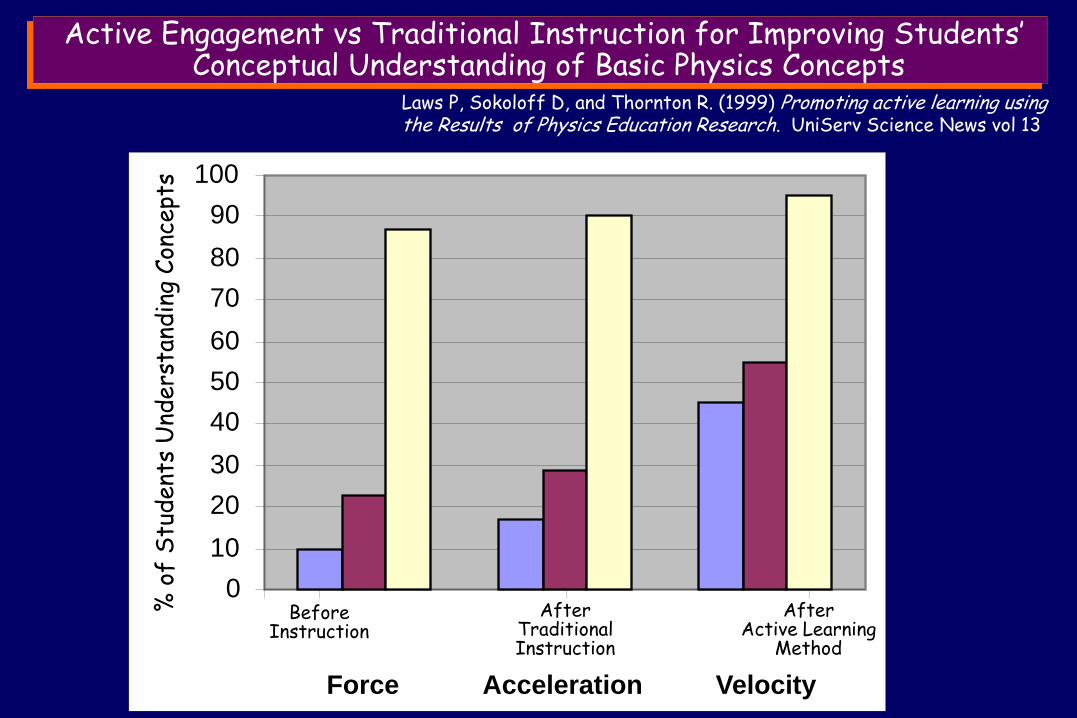
Force Acceleration Velocity
Before Instruction
After Traditional Instruction
After Active Learning
Method
% o
f S
tudent
s U
nders
tand
ing
Con
cept
s
Laws P, Sokoloff D, and Thornton R. (1999) Promoting active learning using the Results of Physics Education Research. UniServ Science News vol 13
Active Engagement vs Traditional Instruction for Improving Students’ Conceptual Understanding of Basic Physics Concepts

Can enhance academic achievement
“Active learning”
Research Results indicate:
Promote retention and application of knowledge
Enhance understanding and mastery of course content
Improve critical thinking and problem solving
Improve clinical competencies
Enhance interpersonal skills
Promote teamwork
Increase student engagement
Promote positive student attitudes
Increase course satisfaction
Encourage self-directed lifelong learning
“ACTIVE LEARNING"
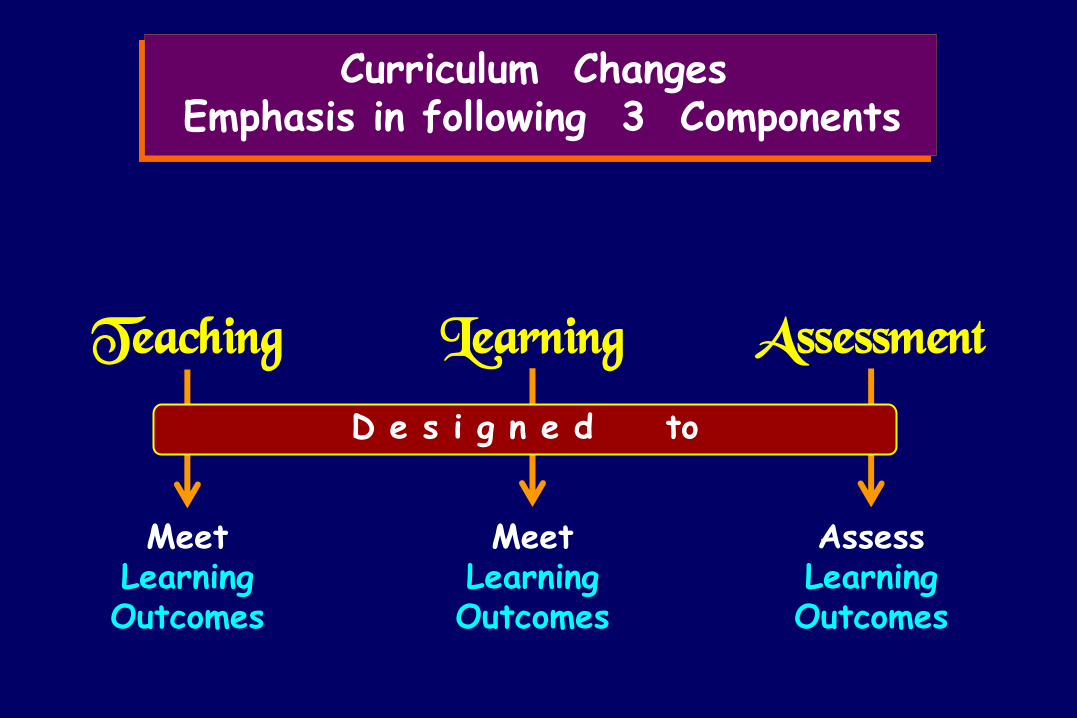
Curriculum Changes Emphasis in following 3 Components
Teaching Learning Assessment
Meet Learning Outcomes
Meet Learning Outcomes
Assess Learning Outcomes
D e s i g n e d to

Teaching
“Teachers” must have a clear idea
of what they want students to be able to do
at the end of a unit of study
Intended learning outcomes to students
so that they can share in the responsibility of
achieving them
However, Students will inevitably tend to look at the assessment
and structure their learning activities to optimize their performance
Communicate

Creating a teaching environment in which students
Are active and not spoon-fed
Driven by their curiosity and develop documented competencies
not merely the ability to regurgitate facts
Develop comprehensive skills
beyond a physical exam
Teaching

“ I never teach my pupils;
Albert Einstein
I only attempt to provide the conditions in which they can learn "
if learning
takes place inside the student’s brain
the “real” learning
can only be managed by the student
(where teachers cannot reach)
All teachers can do is to create an environment which is encouraging and supportive of students engaging in the appropriate and necessary mental activity
Learning

“Learning takes place through the active behaviour of the student :
It is what he does that he learns, not what the teacher does”
Tyler. Basic Principles of Curriculum and Instruction . (1949)
“ Nothing that is worth knowing
can be taught"
Oscar Wilde

National Training Laboratories, Bethel, Maine, USA
Correlation between “Learning Mode” and Retention Capacity
5%
10%
20%
30%
50%
70%
90%
Average Retention Capacity (2 weeks)
Confucius”, 551-479 BCE
“I hear and I forget,
I see and I remember,
I do and I understand”
Teach others
Discussion group
Practice by doing
Lecture
Demonstration
Audiovisual
Reading
The Future of Medical Education is in Rediscovering the Past
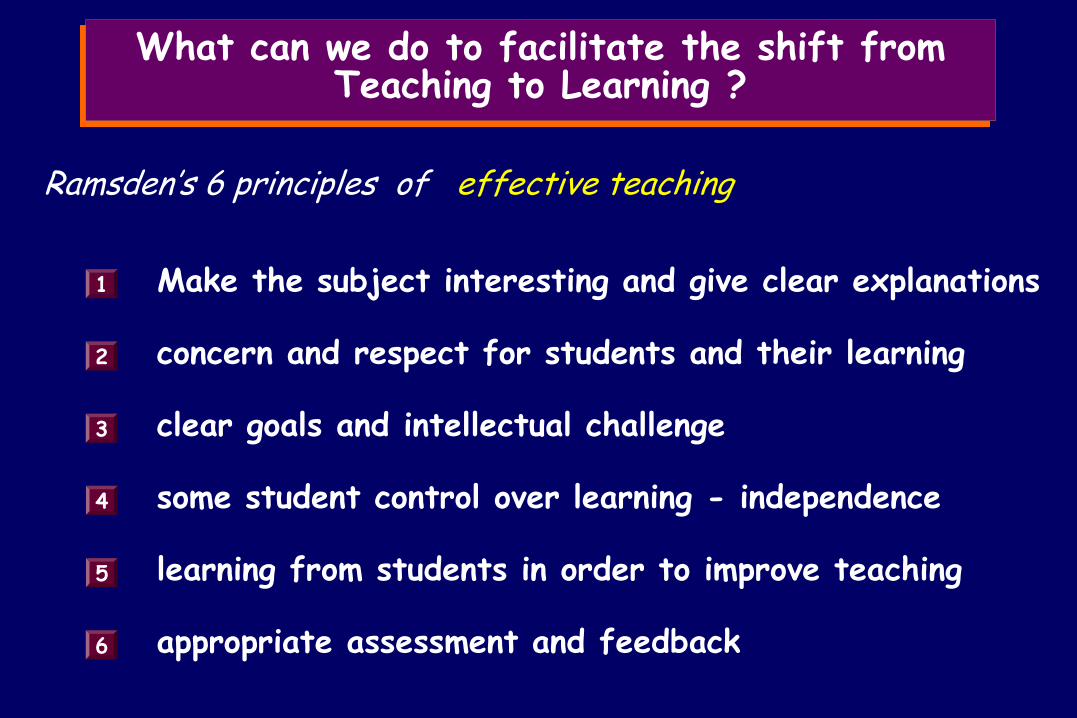
What can we do to facilitate the shift from Teaching to Learning ?
Ramsden’s 6 principles of effective teaching
Make the subject interesting and give clear explanations 1
concern and respect for students and their learning 2
appropriate assessment and feedback 6
clear goals and intellectual challenge 3
some student control over learning - independence 4
learning from students in order to improve teaching 5
Traditionally
Teachers tend to think about assessment once the learning process is over
( making an unconscious gap between student’s learning and achievement in a specific assessment task )
Constructive Alignment Assessment needs to be thought of while delineating the “Intended Learning Outcomes” and therefore, embedded in the learning activities
Assessment

Constructive Alignment J. Biggs. (2003) Teaching for Quality Learning of University . (Buckingham. Open University Press/McGraw Hill)
SOLO Taxonomy
developed by Biggs & Collins (1982)
Structure of Observed Learning Outcomes
Has become the framework for much quality assurance work in the UK and HK
Provides a specific method of implanting Outcomes Based Teaching and Learning

The “Constructive” aspect refers to what the learner does
Students Construct meaning through relative learning activities
“Meaning” is not something imparted or transmitted from teacher to learner
it is something that learners have to create for themselves
The “Alignment” aspect refers to a what the teacher does :
Set up a learning environment that:
is appropriate to achieving the observed learning outcomes
B
supports learning activities A
Constructive Alignment J. Biggs. (2003) Teaching for Quality Learning of University . (Buckingham. Open University Press/McGraw Hill)
Passive learning
Active learning
Assessment Learning
Students will structure their learning activities
to optimize their performance
drives
assessment DOES test the learning outcomes
we want students to achieve
must make
sure that
By being strategic optimizers of their assessment performance, students will actually be working to achieve the
Intended Learning Outcomes
Assessment

If we tell students that we want them to achieve something (intended learning objectives) and then assess them against assessment criteria that do not match
They will feel cheated and will become
Cynical strategic surface learners
“Alignment” is nothing more than a matter of honesty and fairness that establishes
the trust required for students to be confident that they can manage their own learning
Assessment
Snadden D. Portfolios- attempting to measure the unmeasurable? Medical Education 1999;33:478-479.
At present our assessment methods stem from the reductionist philosophy that underpins our discipline, and we are, thus, trapped by our need to compare like with like.
Think Beyond “Quantitative”
Until we can make a mental shift that allows us to include a more holistic approach to assessment, one which evaluates the development of individuals over time, , we will continue to struggle to measure the unmeasurable, and may end up measuring the irrelevant because it is easier.
“ “ ”
Assessment
Snadden D. Portfolios- attempting to measure the unmeasurable? Medical Education 1999;33:478-479.
At present our assessment methods stem from the reductionist philosophy that underpins our discipline, and we are, thus, trapped by our need to compare like with like.
Think Beyond “Quantitative”
Until we can make a mental shift that allows us to include a more holistic approach to assessment, one which evaluates the development of individuals over time, , we will continue to struggle to measure the unmeasurable, and may end up measuring the irrelevant because it is easier.
“ “ ”
Assessment
WHICH ARE NOT METHODS IN “ACTIVE LEARNING"
Traditional Classroom

METHODS IN “ACTIVE LEARNING"
Flipped Classroom
Blended learning
Case Based Learning (Clinical Case studies/Presentations)
Audience response system
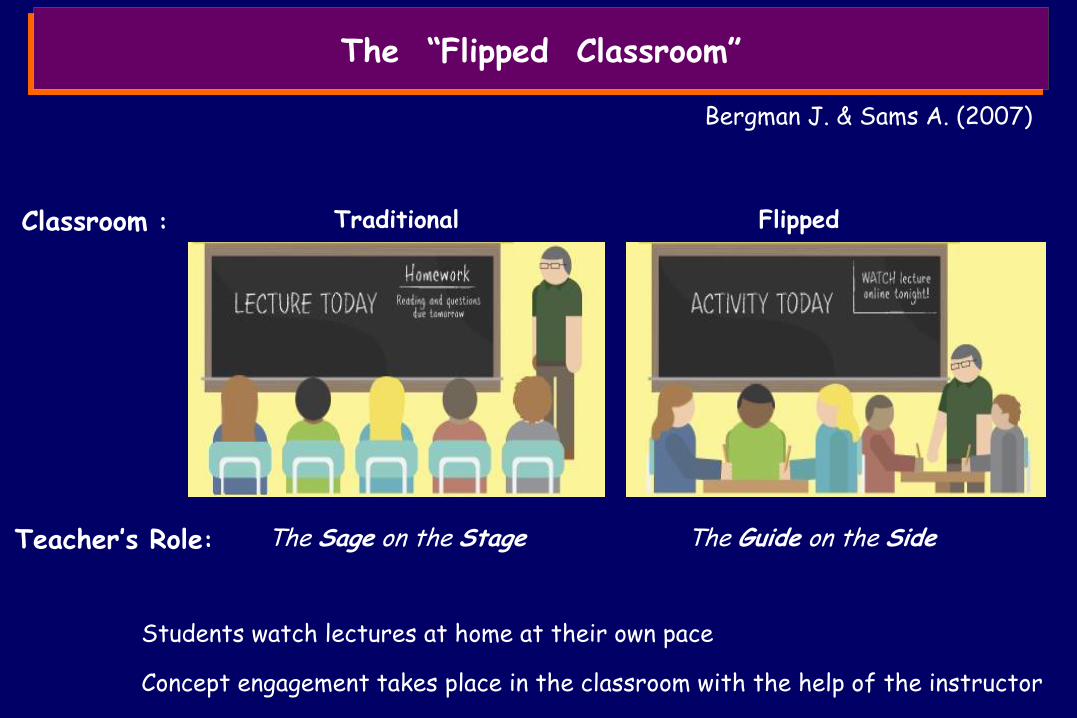
Traditional
Teacher’s Role: The Sage on the Stage The Guide on the Side
Flipped
Students watch lectures at home at their own pace
Concept engagement takes place in the classroom with the help of the instructor
Classroom :
The “Flipped Classroom”
Bergman J. & Sams A. (2007)

Poor learning outcomes
What Drove the change ?
The traditional one-size-fits all model of education often results in limited concept engagement and severe consequences
0
20
40
60
80
100
Traditional Flipped
English Math English Math
Percent of Freshmen Passing English and Math on the Basis of
the “teaching” Method Used
Technological Progress
The availability of online video and increasing student access to technology
The “Flipped Classroom”
50
81
56
87
METHODS IN “ACTIVE LEARNING"
Problem based Learning (adult learning)
Flipped Classroom
Blended learning
Case Based Learning (Clinical Case studies/Presentations)
Audience response system
Small group discussion
Student debates
Learning by teaching
Think – Pair – Share
Team based Learning Individual readiness assurance test (iRAT) :
Team readiness assurance test (tRAT) :
What can WE do !
Active Learning & The CNUCOM

“ACTIVE LEARNING“ Curriculum
1) Small group formation (ideal group from 5 to 7 students)
Three options: (considering an incoming class of 60 students) 10 groups of 6 students each (ideal situation)
8 groups of 7 to 8 students each (acceptable situation)
6 groups of 10 students each (forced situation)
2) In the classroom, the sitting is indicated according to groups
3) Before students start the first day of classes they are instructed to go over the lectures of the arguments covered the subsequent day
4) 6 MCQ are created for each 50 minute “lecture” 2 questions derived from the first 1/3 of the lecture, 2 from middle 1/3 and 2 from last 1/3
Students are instructed to write down any questions or needed clarifications that the assignment may raise

9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 – 1) Individual quiz (Individual Readiness Assurance Test):
Each student, individually takes an MCQ exam based on the assigned lectures for that particular day
The assigned lectures can vary from a minimum of 3 to a maximum of 6 /day
The amount of “home” time dedicated to assignments (based on technical facilitations) range from 1.0-1.5 to 2.5-3 hrs
Amount of time allotted for the quiz depends on the number of questions which can vary from 18 to 36
(allowing maximum 40 sec/question – the necessary time would be from 12 to 24 minutes (15 to 30 minutes)
1) Individual Quiz (iRAT)
“ACTIVE LEARNING“ Curriculum
(Speed with which lectures can be listened: 2 – 2.5 x)
Day 1 - Monday

9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 –
At the end of MC Quiz, the students are given the clinical case
Each member of the group gets a hard copy of the CP
One of the components of the group (changes with each CP) reads it out loud as the other components of the group follow the written hand-out (~ 5-10 minutes)
2) Clinical Presentation – “Xxxxxx”
1) Individual Quiz (iRAT)
2) Clinical Presentation 1) Individual quiz (individual Readiness Assurance Test):
“ACTIVE LEARNING“ Curriculum
Day 1 - Monday
9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 –
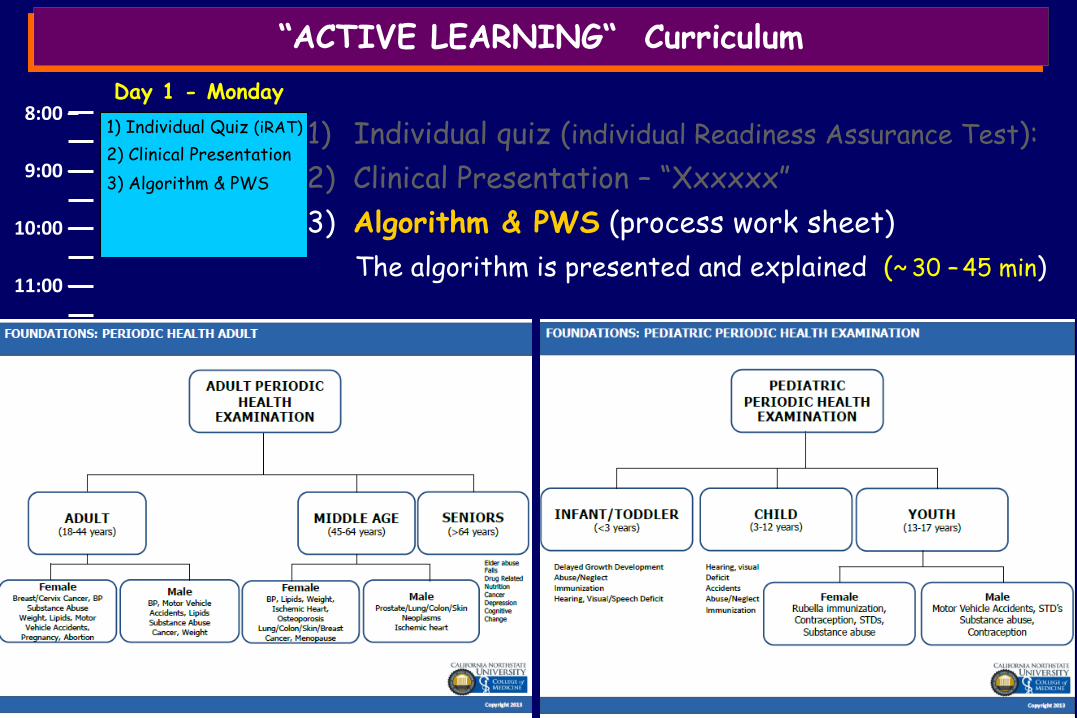
The algorithm is presented and explained (~ 30 – 45 min)
2) Clinical Presentation – “Xxxxxx”
3) Algorithm & PWS (process work sheet)
1) Individual Quiz (iRAT)
2) Clinical Presentation
3) Algorithm & PWS
1) Individual quiz (individual Readiness Assurance Test):
“ACTIVE LEARNING“ Curriculum
Day 1 - Monday

9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 –
The students as a group are given the same initial quiz (discussion occurs among the students to choose the correct answer)
The agreed upon correct answer from each group is indicated by audience response system
Course supervisor(s) goes over each question allowing students to give the reason why the chose answer is the right one or the instructor gives the explanation
2) CP – “Xxxxxx”
3) Algorithm & PWS (process work sheet)
4) Group Quiz (Team Readiness Assurance Test)
1) Individual Quiz (iRAT)
2) Clinical Presentation
3) Algorithm & PWS
4) Group Quiz (tRAT)
1) Individual quiz (individual Readiness Assurance Test):
“ACTIVE LEARNING“ Curriculum
Day 1 - Monday

9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 –
2) CP – “Xxxxxx”
3) Algorithm & PWS (process work sheet)
Course supervisor(s) goes over each question allowing students to give the reason why the chosen answer is the right one or the instructor gives the explanation
5) Discussion of answers
1) Individual Quiz (iRAT)
2) Clinical Presentation
3) Algorithm & PWS
4) Group Quiz (tRAT)
5) Discuss. Of answers
1) Individual quiz (individual Readiness Assurance Test):
4) Group Quiz (Team Readiness Assurance Test)
“ACTIVE LEARNING“ Curriculum
Day 1 - Monday

9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 – 1) Small Group Meeting -
The members of each group (working together), try to identify what are the key points presented in the clinical case and decide what information they know and/or need to better understand the problem being presented
Small Group meeting These decisions are listed on a sheet of paper (or computer) where they indicate:
a) Key points identified in the case and explanations as to why they are considered key points
b) Known information/knowledge identified in the case and explanations as to how it will help them understand the case
c) Needed information/knowledge identified in the case and explanations of how this information will help them understand the case
Students are instructed to search for needed information and write down questions or needed clarifications that the clinical case may raise
“ACTIVE LEARNING“ Curriculum
1) Individual Quiz (iRAT)
2) Clinical Presentation
3) Algorithm & PWS
4) Group Quiz (tRAT)
5) Discuss. Of answers
Day 1 - Monday

“ACTIVE LEARNING“ Curriculum

Clinical Case Work-sheet
Key Points identified Why are these considered “key points”
Known information/knowledge How will it help understand the case
Needed information/knowledge How will it help understand the case
The “paper” (computer program) is made in such a way that it can be amended as they get further into the week (in order to see their evolving line of thought)

9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 – 1) Class (FC) (minimum 1 – maximum 3 topics
First session will be composed of only 1 topic
For the first 15 minutes the questions formulated by the students are pooled by the group spokesman for that day
a) Each group will formulate from 4 to 7 questions which will be listed in order of apparent importance
b) The leader of each group is given the opportunity to ask the questions and conduct the discussion on behalf of his group
Class 1 The first 2 from each group will be asked and if time allows additional questions are asked (1/group)
This “leader” changes every day until every one has had the opportunity to lead the group (restart)
“ACTIVE LEARNING“ Curriculum
Small Group meeting
1) Individual Quiz (iRAT)
2) Clinical Presentation
3) Algorithm & PWS
4) Group Quiz (tRAT)
5) Discuss. Of answers
Day 1 - Monday
Intro to Human Body
9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
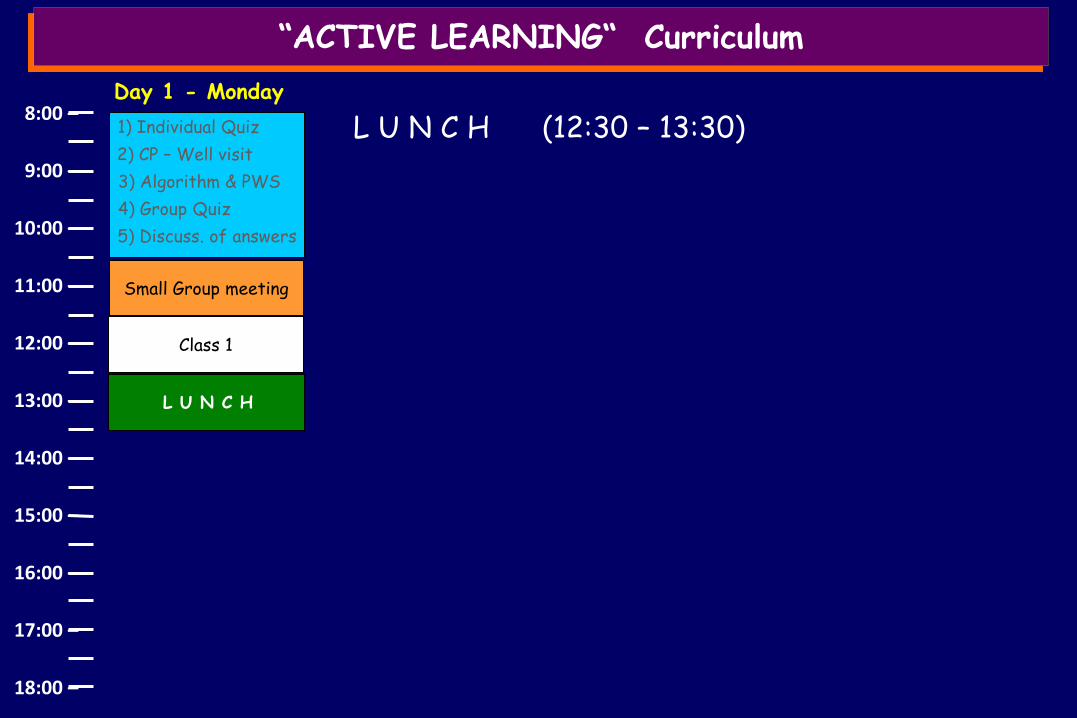
8:00 – 1) Individual Quiz
2) CP – Well visit
3) Algorithm & PWS
4) Group Quiz
L U N C H (12:30 – 13:30)
5) Discuss. of answers
Small Group meeting
Class 1
L U N C H
“ACTIVE LEARNING“ Curriculum
Day 1 - Monday

9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 – 1) Individual Quiz
2) CP – Well visit
3) Algorithm & PWS
4) Group Quiz
1) Class (FC) (minimum 1 – maximum 3 topics)
5) Discuss. of answers
Small Group meeting
Class is conducted in the same manner as the prior class
a) Additional important value:
Class – 1 Topic
More than one instructor is present simultaneously
Better integration (and discussion) of the answers to the questions posed
L U N C H
Class – 3 Topics
“ACTIVE LEARNING“ Curriculum
NB: It should be something highly desirable and actively sought to have more instructors involved simultaneously
Day 1 - Monday
Normal Cell Struct Normal Cell Growth
Gametogenesis

9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 – 1) Individual Quiz
2) CP – Well visit
3) Algorithm & PWS
4) Group Quiz
5) Discuss. of answers
Small Group meeting
Class – 1 Topic
L U N C H
Class – 3 Topics
“ACTIVE LEARNING“ Curriculum
Small Group meeting
Day 1 - Monday
1) Small Group Meeting - Students analyze what information they have been able to find from class discussions:
Source of information
Reliability of information
a) distribute individual tasks to search for additional information, citing:
b) Formulate additional (preliminary) questions regarding what they need to know in order to present them the next day in class
9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 – 1) Individual Quiz
2) Group Quiz
3) Discuss. of answers
Class – 2 Topics
L U N C H
Class – 2 Topics
“ACTIVE LEARNING“ Curriculum
Small Group meeting
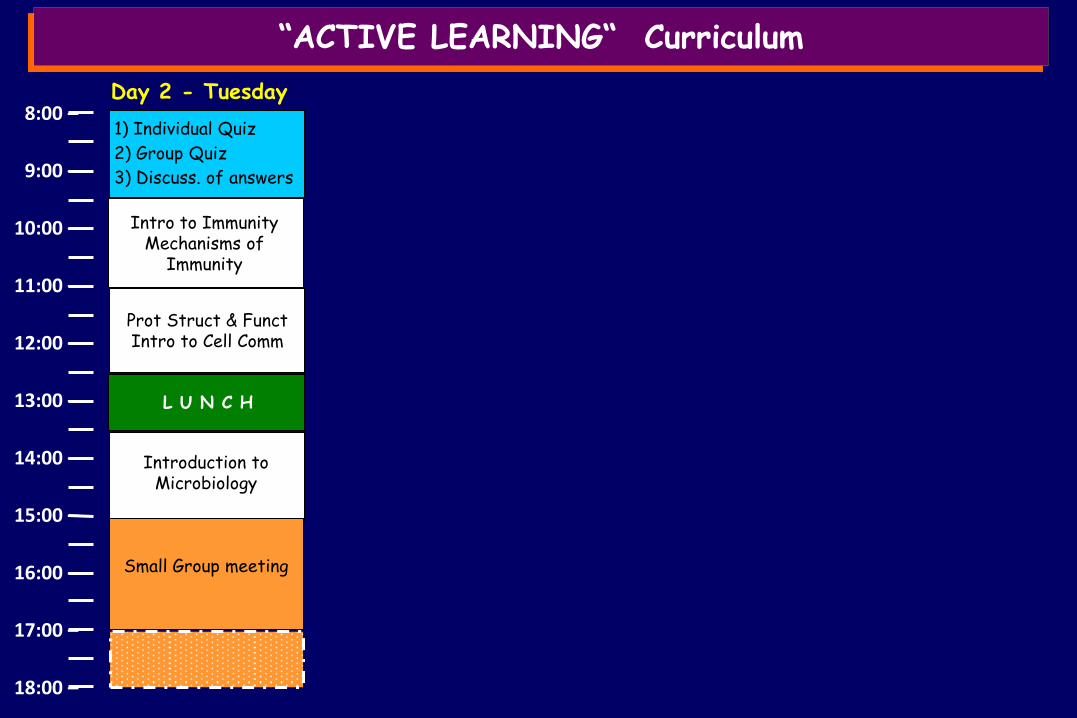
Day 2 - Tuesday
Class – 1 Topic
Intro to Immunity Mechanisms of
Immunity
Prot Struct & Funct Intro to Cell Comm
Introduction to Microbiology
9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 – 1) Individual Quiz
2) Group Quiz
3) Discuss. of answers
Class – 1 Topic
L U N C H
Class – 1 Topic
“ACTIVE LEARNING“ Curriculum
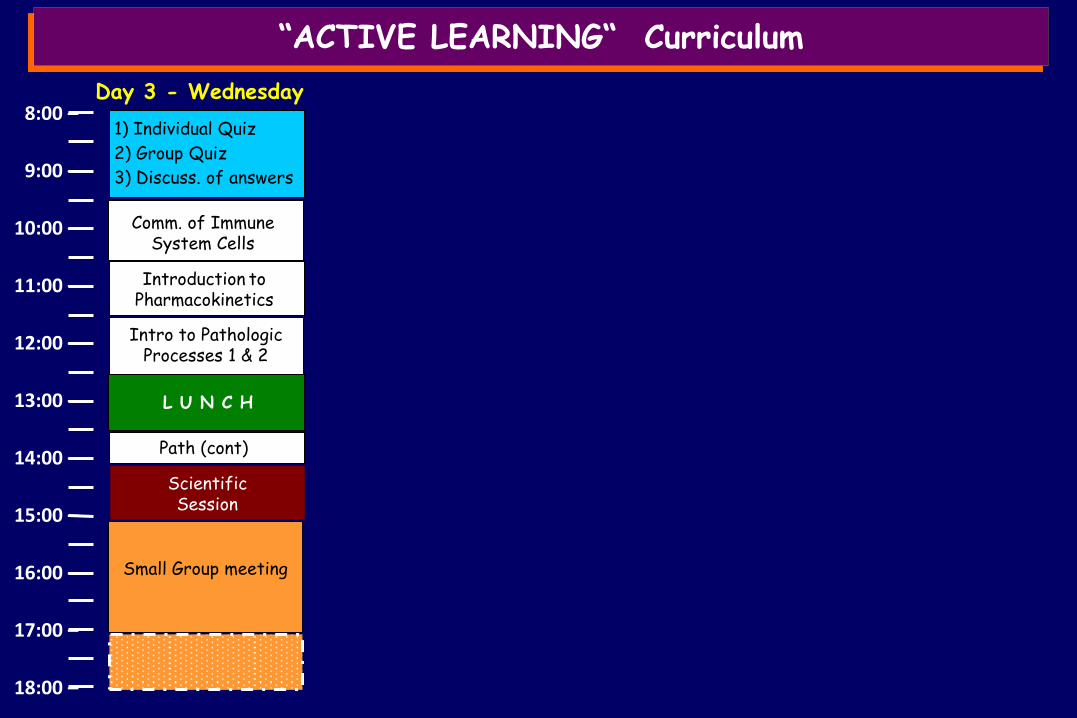
Day 3 - Wednesday
Path (cont)
Comm. of Immune System Cells
Introduction to
Pharmacokinetics
Scientific Session
Class – 1 Topic Intro to Pathologic
Processes 1 & 2
Small Group meeting

9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
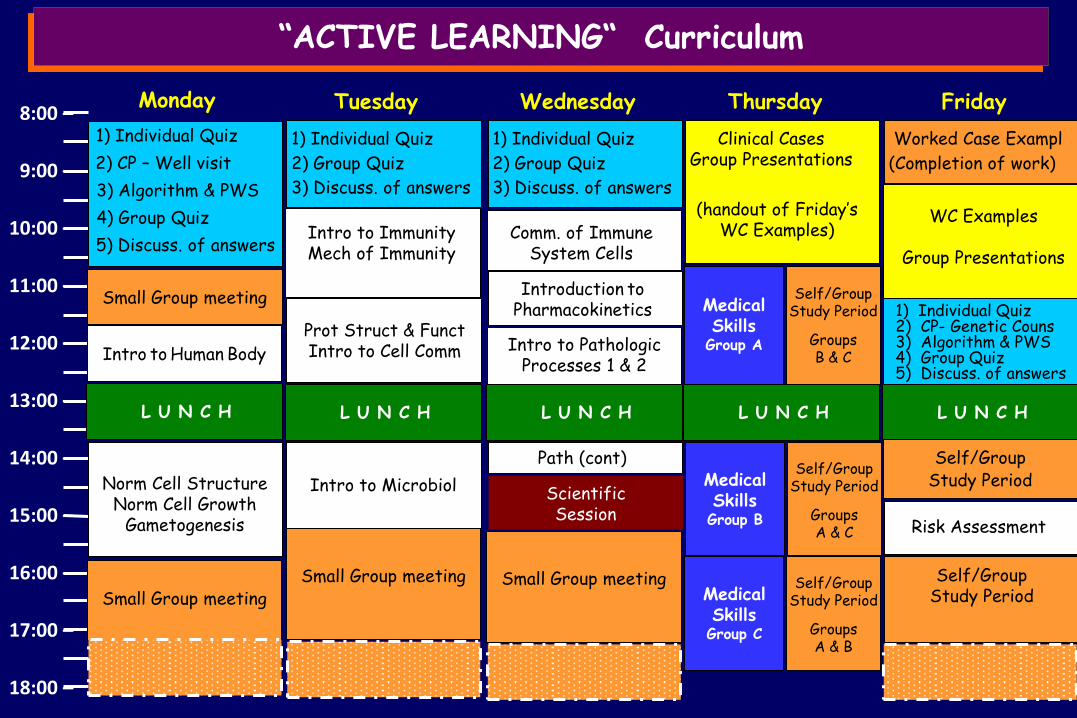
8:00 – Clinical Cases
Group Presentations
(handout of Friday’s WC Examples)
L U N C H
“ACTIVE LEARNING“ Curriculum
Day 4 - Thursday
Medical Skills
Group A
Self/Group Study Period
Groups B & C
Medical Skills
Group B
Self/Group Study Period
Groups A & C
Medical Skills
Group C
Self/Group Study Period
Groups A & B
1) Clinical Cases Presentations - Each group has 10-15 minute presentation performed by group leader* chosen (within the group) for that week
NB: At the end of the session each group is given a WC example:
* group leader changes with each Clinical case Presentation
2) Medical Skills
While Group A (20 students) are involved with Med Skills
Components of the “Class teams” pertaining to Medical Skills Groups B & C work of the WC Examples
9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
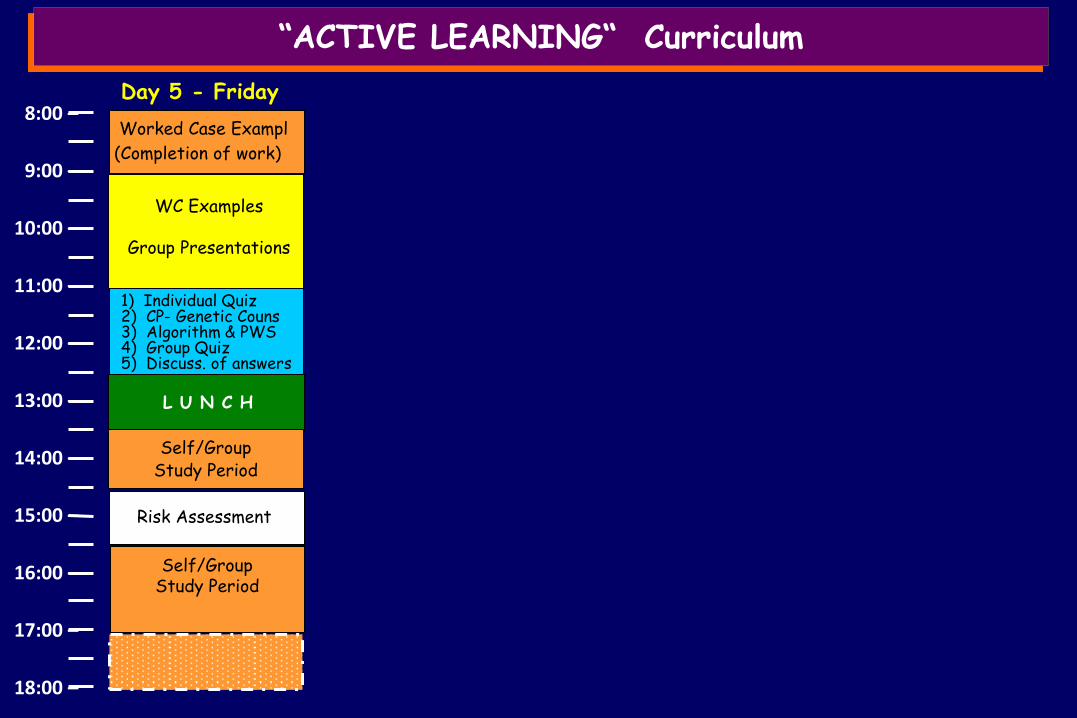
8:00 – Worked Case Exampl
(Completion of work)
WC Examples
Group Presentations
L U N C H
Class – 1 Topic
“ACTIVE LEARNING“ Curriculum
Day 5 - Friday
Risk Assessment
Self/Group Study Period
1) Individual Quiz 2) CP- Genetic Couns 3) Algorithm & PWS 4) Group Quiz 5) Discuss. of answers
Self/Group Study Period
9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 –
“ACTIVE LEARNING“ Curriculum
Worked Case Exampl
(Completion of work)
WC Examples
Group Presentations
L U N C H
Class – 1 Topic
Friday
Risk Assessment
Self/Group Study Period
1) Individual Quiz 2) CP- Genetic Couns 3) Algorithm & PWS 4) Group Quiz 5) Discuss. of answers
Self/Group Study Period
Clinical Cases Group Presentations
(handout of Friday’s WC Examples)
L U N C H
Thursday
Medical Skills
Group A
Self/Group Study Period
Groups B & C
Medical Skills Group B
Self/Group Study Period
Groups A & C
Medical Skills Group C
Self/Group Study Period
Groups A & B
1) Individual Quiz
2) Group Quiz
3) Discuss. of answers
Class – 1 Topic
L U N C H
Class – 1 Topic
Wednesday
Path (cont)
Comm. of Immune System Cells
Introduction to
Pharmacokinetics
Scientific Session
Class – 1 Topic Intro to Pathologic
Processes 1 & 2
Small Group meeting
1) Individual Quiz
2) CP – Well visit
3) Algorithm & PWS
4) Group Quiz
5) Discuss. of answers
Small Group meeting
Intro to Human Body
L U N C H
Norm Cell Structure Norm Cell Growth
Gametogenesis
Small Group meeting
Monday
1) Individual Quiz
2) Group Quiz
3) Discuss. of answers
Class – 2 Topics
L U N C H
Class – 2 Topics
Small Group meeting
Tuesday
Class – 1 Topic
Intro to Immunity Mech of Immunity
Prot Struct & Funct Intro to Cell Comm
Intro to Microbiol
9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 –
“ACTIVE LEARNING“ Curriculum
Friday Thursday
Medical Skills
Group A
Self/Group Study Period
Groups B & C
Medical Skills Group B
Self/Group Study Period
Groups A & C
Medical Skills Group C
Self/Group Study Period
Groups A & B
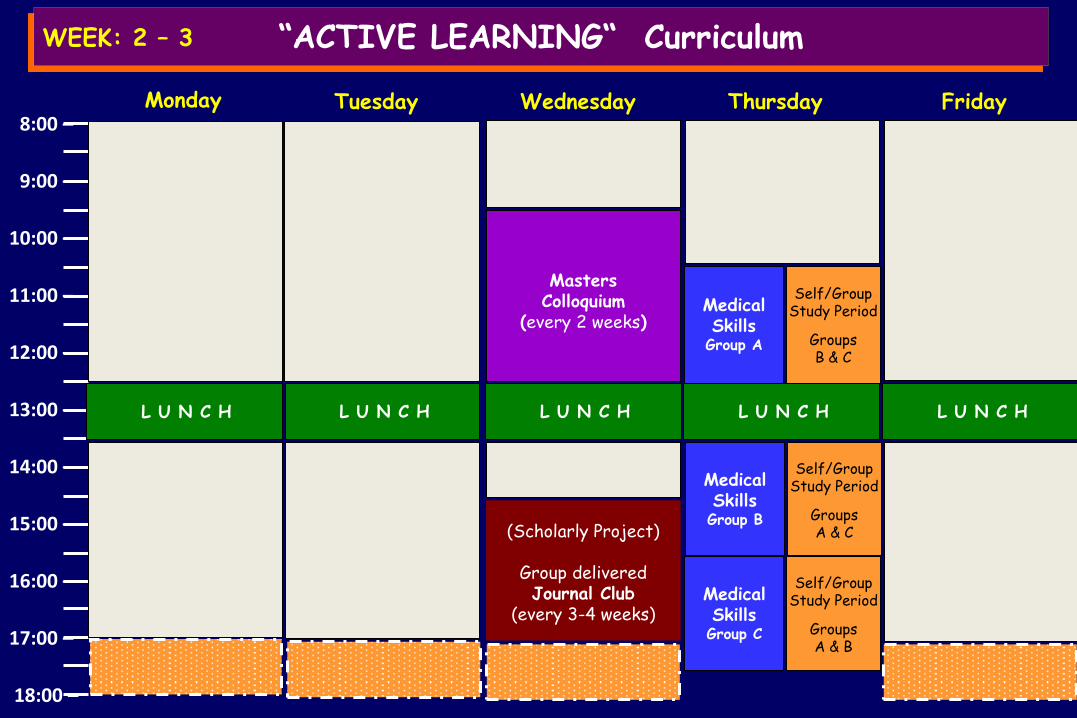
Masters Colloquium
(every 2 weeks)
Wednesday
(Scholarly Project)
Group delivered Journal Club
(every 3-4 weeks)
Monday
L U N C H L U N C H L U N C H L U N C H L U N C H
Tuesday
WEEK: 2 – 3

9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 –
“ACTIVE LEARNING“ Curriculum
Masters Colloquium
(every 2 weeks)
L U N C H
Wednesday
(Scholarly Project)
Group delivered Journal Club
(every 3-4 weeks)
L U N C H
Monday
L U N C H
Tuesday
WEEK: 2 – 3
1) Journal Club a) Teams of 5 students Team reviews an article
Introduction
Followed by general Discussion
Results Discussion How this work relates
to future and past research
Peer & Faculty assessment of presentations – (Rubric)
Each student is given a section to present
Methods
Selected article corresponds to unit being covered
Reference is made available to Class/Faculty at least one week prior to presentation
9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 –
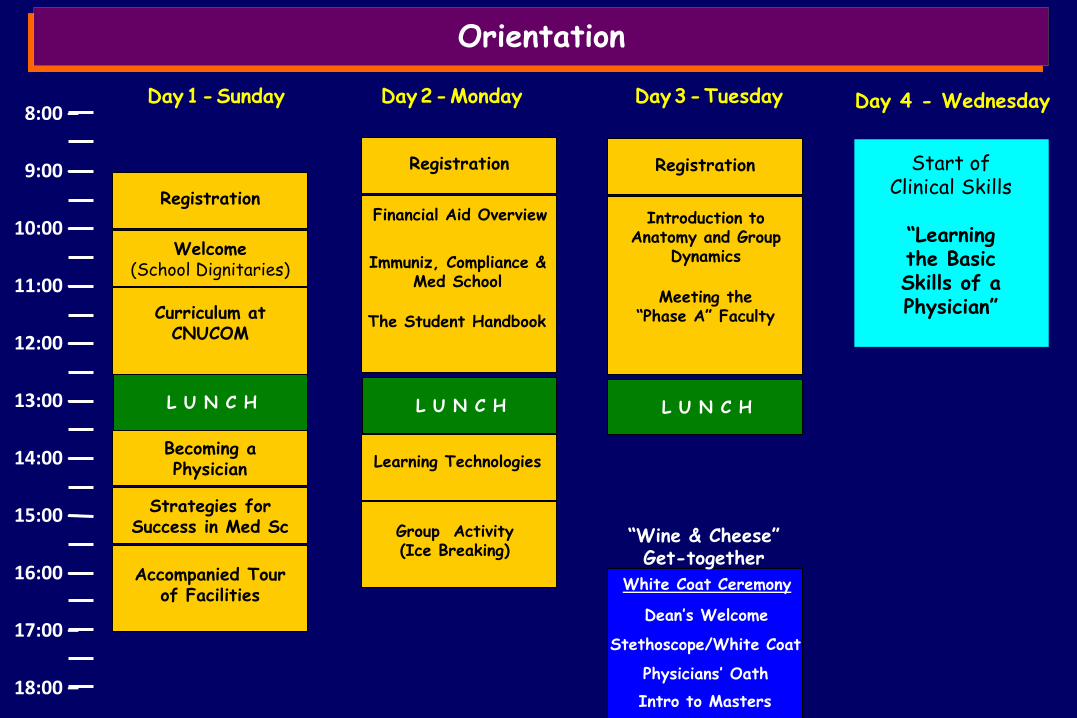
Orientation
Day 1 - Sunday
L U N C H
Registration
Welcome (School Dignitaries)
Curriculum at CNUCOM
Becoming a Physician
Strategies for Success in Med Sc
Accompanied Tour of Facilities
Day 2 - Monday
L U N C H
Registration
Financial Aid Overview
Learning Technologies
Immuniz, Compliance & Med School
The Student Handbook
Learning Technologies
Group Activity (Ice Breaking)
L U N C H
Registration
Introduction to Anatomy and Group
Dynamics
Meeting the “Phase A” Faculty
Day 3 - Tuesday
“Wine & Cheese” Get-together
White Coat Ceremony
Stethoscope/White Coat
Physicians’ Oath
Intro to Masters
Dean’s Welcome
Day 4 - Wednesday
Start of Clinical Skills
“Learning the Basic Skills of a Physician”

Introduction to Medical School – The Basic Skills of a Physician
Day 1 - Wednesday Day 2 - Thursday
Medical Skills Written Present Comprehensive Hx SOAP notes Oral Presentation
L U N C H
Vital signs (OSCE rooms) Reflexes Touch fiber Tun fork Stethosc Otoscope
Break
PE in Teams (Osce rooms) HEENT Chest/Thorax Abdomen Extremeties Neuro
Break
Continue with PE (above)
L U N C H
HIPAA Training
Break
Intro to Medical Skills Distrib of Med equip Skills partic. Consent Skills partic. Forms Needle Policy Hand disinfection
Break
Verbal & non verb com Peter Eveland Actors Intro to BLS on-line
Ethics/Professionalism Intro to Med Ethics Cadaver Respect Dr-Patient relation Dress Code
Day 3 - Friday
CP Presentation
H&P Practice SOAP notes
L U N C H
Break
BLS Test
Break
CP Presentation (contd)
H&P Practice SOAP notes
BLS Test (contd)
BLS on-line (self study) BLS on-line (self study)
9:00 –
10:00 –
11:00 –
12:00 –
13:00 –
14:00 –
15:00 –
16:00 –
17:00 –
18:00 –
8:00 –
Welcome to
CNUCOM
Light Years Ahead
in The Innovative
Delivery of Medical Education
CONCLUSIONS
Health care has a cost
but good “teaching”
is priceless !
A. Tenore
but good innovative “teaching”
is priceless !























