Embed Size (px)
Citation preview
Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Activity presentations are considered intellectual property.
• These slides may not be published or posted online without permission from VindicoMedical Education ([email protected]).
• Please be respectful of this request so we may continue to provide you with presentation materials.
Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Oral Therapy for MS Management:State of the Union
Bruce Cree, MD, PhD, MAS
Associate Professor of Clinical Neurology
Clinical Research Director
University of California San Francisco
San Francisco, CA

Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Existing and Emerging MS Therapies
Phase III completed In Phase IIIApproved therapies
2009 2010 201120051995 2000
Gilenya (Fingolimod)
Aubagio(Teriflunomide)
Extavia(IFNβ-1b)
Tysabri (natalizumab)
Betaseron(IFNβ-1b)
Copaxone(glatiramer acetate)
Avonex (IFNβ-1a)
Rebif(IFNβ-1a)
Novantrone (mitoxantrone)
Laquinimod
Approval date Estimated launch date
Cladribine
2012
*In March 2011, the FDA did not approve cladribine and requested Merck KGaA provide an improved understanding of its safety risks and overall benefit-risk profile.
Daclizumab
Ocrelizumab
Ofatumumab
Siponimod
Ampyra(4-amino pyradine)
Nuedexta (Dextromehtorphan
Quinidine)
2013
Lemtrada(alemtuzumab)
Tecfidera(Dimethyl Fumarate)
(BG-12)
Ozanimod
Oral Therapies Overview
• In theory, orally bioavailable therapies will be better tolerated than parenterally administered medications.
• In practice, adherence to treatment is dependent on more than route of administration. Frequency of treatment, common adverse events, as well as, more rare but serious adverse events influence adherence.
• A recent non-industry sponsored, single-center study using a patient reported outcome found that adherence for never missing a dose was highest for an infusible medication, followed by injectables, and then by oral therapies.
– 93.3% vs 70.8% vs 55%, P<.005, N=209
Dione C, CMSC 2015, Abstract DX19.
Fingolimod: Efficacy
• Indicated for relapsing MS, single once-daily capsule
• Proven efficacy1
– 54% relative reduction in relapses
– 30% reduction in hazard ratio for disability (3 month sustained change)
– Superior to interferon β-1a IM (TRANSFORMS Study)2
– Robust effects on lesion evolution and brain volume loss
1. Kappos K, et al. N Engl J Med. 2010;362:387-401. Reprinted with permission. 2. Cohen J, et al. N Engl J Med. 2010;362:402-415.
Fingolimod 0.5 mg vs placebo HR=0.70P=.02 in time to disability progression
Fingolimod 1.25 mg vs placebo HR=0.68P=.02 in time to disability progression
Fingolimod 1.25 mg (17%)†
90 180 270 360 450 540 630 720
5
10
15
20
25
30
Placebo (24%)
Fingolimod 0.5 mg (18%)*
Days on Study
% W
ith
3-M
on
th C
on
firm
ed
E
DS
S P
rog
ress
ion
*P=.03 vs placebo†P=.01 vs placebo
0.4
0.16 0.18
00.050.1
0.150.2
0.250.3
0.350.4
0.45
AnnualizedRelapse
Rate

Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Therapeutic Satisfaction: EPOC Study Primary Results
Change in Treatment Satisfaction Questionnaire for Medication (TSQM) Global Satisfaction Scores in Subjects Switching to Fingolimod Versus
Staying on Injectables
• LSM changes (± standard error) in TSQM Global Satisfaction scores from baseline to 6 months were significantly superior following a switch to fingolimod compared with remaining on GA (17.08 ± 1.56 vs 0.81 ± 2.89, respectively), IM IFN beta-1a (17.57 ± 1.51 vs 2.10 ± 3.22, respectively), SC IFN beta-1a (24.70 ± 1.62 vs 2.29 ± 2.96, respectively) or IFN beta-1b (22.34 ± 1.85 vs 4.45 ± 3.29, respectively); all P<.001.
Calkwood J, et al. BMC Neurology. 2014;14:220.
IFN, interferon; GA, glatiramer acetate
S1P=sphingosine-1 phosphate.
Activation Proliferation anddifferentiation
Afferent lymphatic vessel
S1PLymphatic sinus
Sinus-lining endothelium
Efferent lymphatic vesselNaïve T cell
Lymph node
S1P1 receptor
Activated T cells
Fingolimod
S1P1
downregulationSinus-lining endothelial cell
barrier enhancement
Reduced T cell egress
Fingolimod: Mechanism of Action
Horga A, et al. Expert Rev Neurother. 2008;8:699-714.
Fingolimod Suppression of Peripheral Lymphocytes
• Fingolimod diminishes peripheral lymphocyte counts by ~75%1,2
1. Mehling M, et al. Neurology. 2008;71:1261-1267.2. Kappos K, et al. N Engl J Med. 2010;362:387-401.
Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
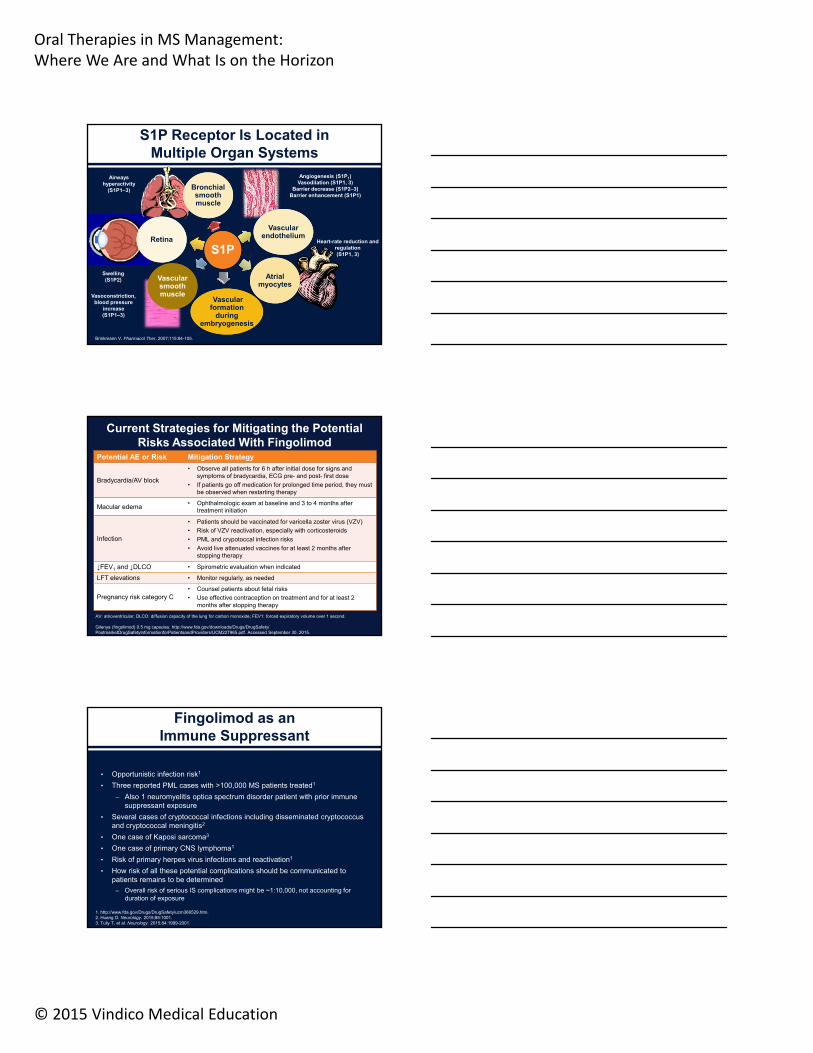
Airways hyperactivity
(S1P1–3)
Vasoconstriction, blood pressure
increase (S1P1–3)
Heart-rate reduction and regulation (S1P1, 3)
Angiogenesis (S1P1)Vasodilation (S1P1, 3)
Barrier decrease (S1P2–3)Barrier enhancement (S1P1)
S1PS1P
Bronchial smooth muscle
Bronchial smooth muscle
Vascular endothelium
Vascular endothelium
Atrial myocytes
Atrial myocytes
Vascular smooth muscle
Vascular smooth muscle
RetinaRetina
Swelling(S1P2)
Vascular formation
during embryogenesis
Vascular formation
during embryogenesis
S1P Receptor Is Located in Multiple Organ Systems
Brinkmann V. Pharmacol Ther. 2007;115:84-105.
Potential AE or Risk Mitigation Strategy
Bradycardia/AV block
• Observe all patients for 6 h after initial dose for signs and symptoms of bradycardia, ECG pre- and post- first dose
• If patients go off medication for prolonged time period, they must be observed when restarting therapy
Macular edema• Ophthalmologic exam at baseline and 3 to 4 months after
treatment initiation
Infection
• Patients should be vaccinated for varicella zoster virus (VZV)
• Risk of VZV reactivation, especially with corticosteroids
• PML and crypotoccal infection risks
• Avoid live attenuated vaccines for at least 2 months after stopping therapy
↓FEV1 and ↓DLCO • Spirometric evaluation when indicated
LFT elevations • Monitor regularly, as needed
Pregnancy risk category C• Counsel patients about fetal risks
• Use effective contraception on treatment and for at least 2 months after stopping therapy
Current Strategies for Mitigating the Potential Risks Associated With Fingolimod
AV: atrioventricular; DLCO: diffusion capacity of the lung for carbon monoxide; FEV1: forced expiratory volume over 1 second.
Gilenya (fingolimod) 0.5 mg capsules. http://www.fda.gov/downloads/Drugs/DrugSafety/ PostmarketDrugSafetyInformationforPatientsandProviders/UCM227965.pdf. Accessed September 30, 2015.
Fingolimod as an Immune Suppressant
• Opportunistic infection risk1
• Three reported PML cases with >100,000 MS patients treated1
– Also 1 neuromyelitis optica spectrum disorder patient with prior immune suppressant exposure
• Several cases of cryptococcal infections including disseminated cryptococcus and cryptococcal meningitis2
• One case of Kaposi sarcoma3
• One case of primary CNS lymphoma1
• Risk of primary herpes virus infections and reactivation1
• How risk of all these potential complications should be communicated to patients remains to be determined
– Overall risk of serious IS complications might be ~1:10,000, not accounting for duration of exposure
1. http://www.fda.gov/Drugs/DrugSafety/ucm366529.htm. 2. Huang D. Neurology. 2015;85:1001.3. Tully T, et al. Neurology. 2015;84:1999-2001.

Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Teriflunomide
• Indicated for relapsing MS1
• Antimetabolite, inhibits dihydro-orotate dehydrogenase thereby inhibiting de novo DNA synthesis in proliferating lymphocytes
• Proven efficacy2
– 32% relative reduction in relapses (14 mg)
– 30% reduction in hazard ratio for disability
• Single once-daily pill
• Generally, well-tolerated, but with boxed warnings
• No known PML risk
1. http://products.sanofi.us/aubagio/aubagio.pdf 2. O’Connor P, et al. N Engl J Med. 2011;365:1293-1303.
Evaluating Treatment Satisfaction:TSQM in the TENERE Phase 3 trial of Teriflunomide vs IFNβ-1a
Vermersch P, et al. Mult Scler. 2014;20:705-716.
0
20
40
60
80
100
120
Effectiveness Side effects Convenience Global satisfaction
Teri 7 mg Teri 14 mg IFN-b
P=.02
NS
P<.0001P<.0001
P=.02
N=324
Teriflunomide: Targeting Activated Lymphocyte Proliferation
• Teriflunomide selectively and reversibly inhibits mitochondrial dihydro-orotate dehydrogenase (DHODH), impairing the proliferation of activated lymphocytes while sparing resting and slowly dividing cells*1,2
• Pyrimidine salvage pathway is not affected by teriflunomide1
1. Gold R, et al. Acta Neurol Scand. 2011;124:75-84. 2. Warnke C, et al. Neuropsychiatr Dis Treat. 2009;5:333-340.
Stimulated lymphocyte
PYRIMIDINE DEMAND
Resting and slowly dividing lymphocytes
De novo pyrimidine synthesis pathway: DHODH
SALVAGE PATHWAY
* The exact mechanism by which teriflunomide exerts its therapeutic effect in MS is not fully understood
Homeostaticproliferationpreserved
Inhibition of activelyproliferating lymphocytes
X
Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
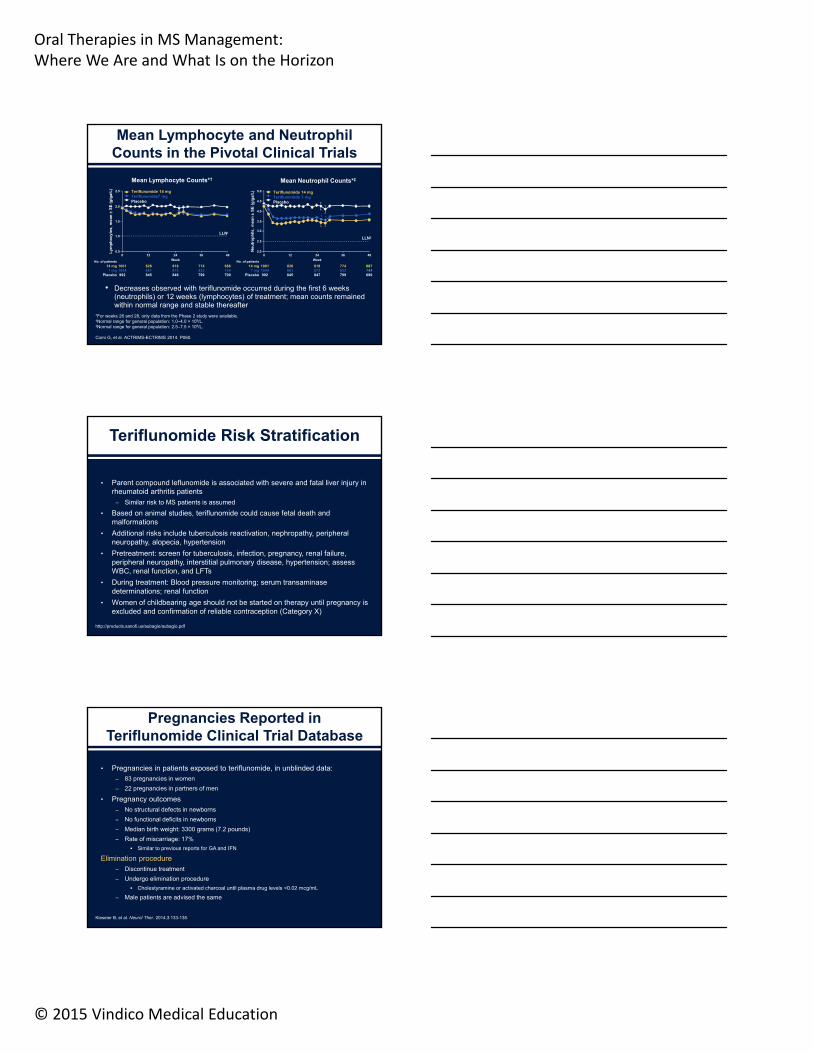
Mean Lymphocyte and Neutrophil Counts in the Pivotal Clinical Trials
Comi G, et al. ACTRIMS-ECTRIMS 2014. P060.
Mean Lymphocyte Counts*† Mean Neutrophil Counts*‡
• Decreases observed with teriflunomide occurred during the first 6 weeks (neutrophils) or 12 weeks (lymphocytes) of treatment; mean counts remained within normal range and stable thereafter
*For weeks 26 and 28, only data from the Phase 2 study were available.†Normal range for general population: 1.0–4.0 × 109/L. ‡Normal range for general population: 2.5–7.5 × 109/L.
No. of patients
14 mg7 mg
Placebo
10011044992
826861845
818873848
774833799
688744700
No. of patients
14 mg7 mg
Placebo
10011044992
826861845
818872847
774833799
687744699
Ly
mp
ho
cyte
s, m
ean
S
E (
gig
a/L
)
0 12 24 36 48
Week
0.5
1.0
1.5
2.0
2.5 Teriflunomide 14 mgTeriflunomide7 mgPlacebo
Neu
tro
ph
ils,
mea
n
SE
(g
iga/
L)
0 12 24 36 48
Week
2.0
2.5
3.5
4.0
5.0
3.0
4.5
Teriflunomide 14 mgTeriflunomide 7 mgPlacebo
LLN†
LLN‡
Teriflunomide Risk Stratification
• Parent compound leflunomide is associated with severe and fatal liver injury in rheumatoid arthritis patients
– Similar risk to MS patients is assumed
• Based on animal studies, teriflunomide could cause fetal death and malformations
• Additional risks include tuberculosis reactivation, nephropathy, peripheral neuropathy, alopecia, hypertension
• Pretreatment: screen for tuberculosis, infection, pregnancy, renal failure, peripheral neuropathy, interstitial pulmonary disease, hypertension; assess WBC, renal function, and LFTs
• During treatment: Blood pressure monitoring; serum transaminase determinations; renal function
• Women of childbearing age should not be started on therapy until pregnancy is excluded and confirmation of reliable contraception (Category X)
http://products.sanofi.us/aubagio/aubagio.pdf
http://products.sanofi.us/aubagio/aubagio.pdf
Pregnancies Reported in Teriflunomide Clinical Trial Database
• Pregnancies in patients exposed to teriflunomide, in unblinded data:– 83 pregnancies in women
– 22 pregnancies in partners of men
• Pregnancy outcomes– No structural defects in newborns
– No functional deficits in newborns
– Median birth weight: 3300 grams (7.2 pounds)
– Rate of miscarriage: 17%
Similar to previous reports for GA and IFN
Elimination procedure – Discontinue treatment
– Undergo elimination procedure
Cholestyramine or activated charcoal until plasma drug levels <0.02 mcg/mL
– Male patients are advised the same
Kieseier B, et al. Neurol Ther. 2014;3:133-138.

Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Dimethyl Fumarate
• Indicated for relapsing MS1
• Mechanism unclear, may induce anti-oxidative genes through Keap1 inhibition that allows Nrf2 to translocate to nucleus and induce antioxidative response
• Proven efficacy2
– 53% relative reduction in relapses
– 38% reduction in hazard ratio for disability (3 month sustained change in EDSS)
• Twice daily capsule
• Generally well tolerated
• Risk of PML in setting of chronic lymphopenia and hypothetical risk of RCC based on dimethyl fumarate used for psoriasis3
1. http://www.tecfidera.com/pdfs/full-prescribing-information.pdf
2. Gold R, et al. N Engl J Med. 2012;367:1098-1107.
3. Sheremata W, et al. Expert Opin Drug Saf. 2015;14(1):161-170.
DMF and its Metabolite, MMF, “Inhibit the Inhibitor”
Adapted from Brück W, et al. JAMA Neurol. 2013;70:1315-1324.
Keap1
Gene Transcription
GSTA2NQO1HO-1
MMF
MMF Keap1CYTOPLASM
NUCLEUS
Dimethyl Fumarate
• Nrf2 is reported to have antiproliferative and immunomodulatory activity.1-3
• DMF 56% and multiple ethyl fumarates promotes development of anti-inflammatory type II DC.4
• DMF may also exert effects through other pathways.
– For example, flushing induced by DMF has been attributed to activation of the nicotinic acid receptor, HCA2.5
The protective effect of DMF is mediated, in part, by HCA2.6
1. Williams MA, et al. J Immunol. 2008;181(7):4545-4559. 2. Rockwell CE, et al. J Immunol. 2012;188(4):1630-1637.3. Lehmann JC, et al. J Invest Dermatol. 2007;127(4):835-845.4. Ghoreschi K, et al. J Exp Med. 2011;208(11):2291-2303.5. Tang H, et al. Biochem Biophys Res Commun. 2009;378(3):662-667. 6. Chen H, et al. J Clin Invest. 2014;124(5):2188-2192.

Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
PML in a Patient Without Severe Lymphocytopenia Receiving Dimethyl Fumarate
Nieuwkamp DJ, et al. N Engl J Med. 2015;372(15):1474-1476. Reprinted with permission.
CD8 Lymphocytes Are Disproportionately Suppressed With DMF Treatment
• Lymphocyte counts go down over time with each of the subsets, whether you look at CD3, CD19, CD56 NK cells, or CD4 or CD8 cells
• The level of CD8 lymphopenia is relatively low
• The CD4/CD8 ratio is reversed over time
Spencer CM, et al. Neurol Neuroimmunol Neuroinflamm. 2015;2(3):e76.
Risk Mitigation With DMF
• GI symptoms and flushing are common• May cause lymphopenia: recent complete blood cell count (<6 months)
before starting treatment and every 6 months thereafter or as clinically indicated
• Liver function tests at baseline• Administration with food may decrease flushing
– Co-treatment with aspirin can reduce flushing• Withholding treatment should be considered in patients with severe
infections• Check JCV serology?
– 1 case of PML reported in MS patients treated with DMF, several other cases associated with DMF in psoriasis patients
• Will checking lymphocyte subsets help mitigate risk of potential opportunistic infections?
Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Is Tiered Treatment Still Applicable?
• Oral therapies have changed the way relapsing MS is managed
• Oral treatment options are likely to be better tolerated compared to auto-injectable medications
• Some oral DMTs may be more effective than injectable therapies inreducing relapses
– Fingolimod was compared to interferon β-1a IM and showed superior efficacy1
– Dimethyl fumarate was compared to glatiramer acetate and showed apparent superior efficacy (post-hoc analysis)2
• Oral therapies may be associated with greater therapeutic satisfaction
• Whether adherence is improved remains to be established
• Each oral therapy has a unique risk/benefit ratio
• Is therapeutic satisfaction (and potentially greater efficacy) worth theadded risk?
1. Cohen JA, et al. N Engl J Med. 2010;362:402-415.
2. Fox RJ, et al. N Engl J Med. 2012;367:1087-1097.
Emerging Oral Agents for MS Management
Amit Bar-Or, MD, FRCPC
Professor, Neuroimmunology
Montreal Neurological Institute McGill University
Montreal, Quebec, Canada
Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Objectives
• Clinical review of oral agents in late-stage development for MS therapy:– Ponesimod – Phase 2; OPTIMUM
– Ozanimod (RPC1063) – RADIANCE/SUNBEAM
– Siponimod/BAF312 – BOLD; EXPAND
– (MT-1303 – MOMENTUM)
– Laquinimod – CONCERTO, ARPEGGIO
Objectives
• Clinical review of oral agents in late-stage development for MS therapy:– Ponesimod – Phase 2; OPTIMUM
– Ozanimod (RPC1063) – RADIANCE/SUNBEAM
– Siponimod/BAF312 – BOLD; EXPAND
– (MT-1303 – MOMENTUM)
– Laquinimod – CONCERTO, ARPEGGIO
Ponesimod
• Profile suitable for once-daily oral dosing
• Selective S1P1 receptor modulator
• Lymphocyte reduction is rapid, dose-dependent, reversible
• Penetrates into brain and spinal cord
Olsson T, et al. J Neurol Neurosurg Psychiatry. 2014;85(11):1198-1208.
Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Randomization
40 mg o.d. ponesimod (N=119)
Placebo (N=121)
20 mg o.d. ponesimod (N=116)
10 mg o.d. ponesimod (N=108)
Follow-upTreatment 24 weeks
Baseline
Follow-upScreening
ExtensionCore
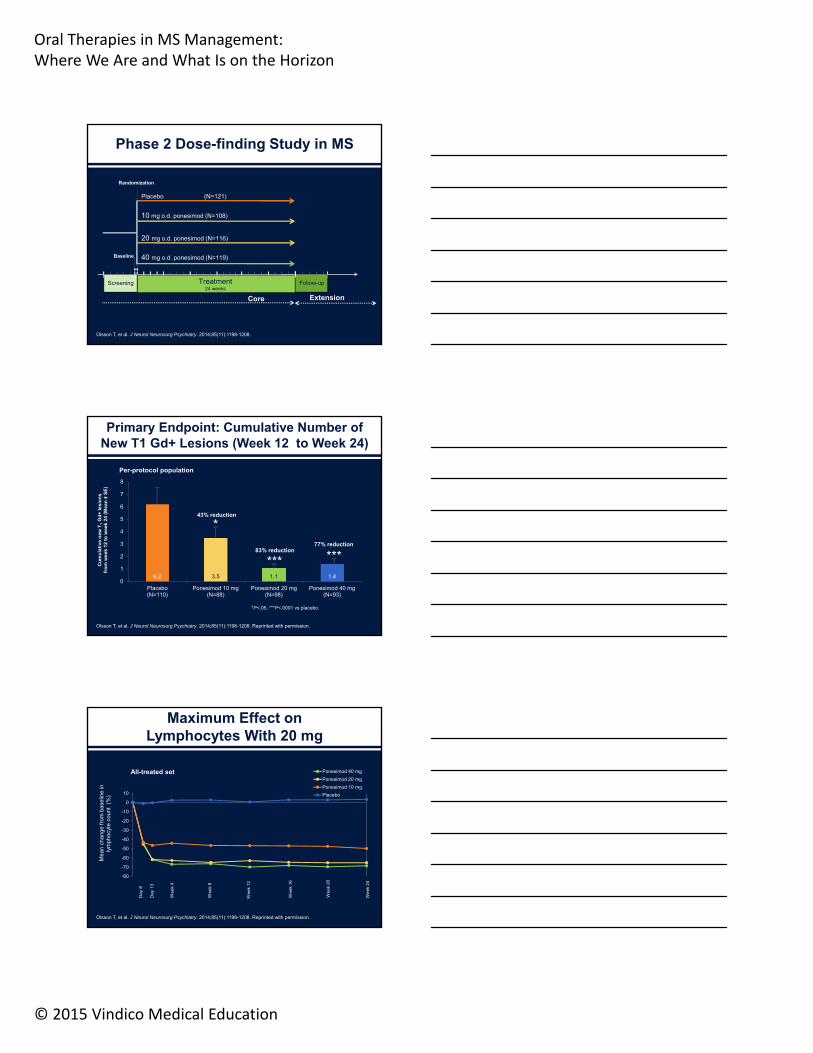
Phase 2 Dose-finding Study in MS
Olsson T, et al. J Neurol Neurosurg Psychiatry. 2014;85(11):1198-1208.
6.2 3.5 1.1 1.40
1
2
3
4
5
6
7
8
Placebo(N=110)
Ponesimod 10 mg(N=88)
Ponesimod 20 mg(N=98)
Ponesimod 40 mg(N=93)
Cu
mu
lati
ve n
ew T
1G
d+
lesi
on
sfr
om
wee
k 12
to
wee
k 24
(M
ean
±S
E)
*P<.05, ***P<.0001 vs placebo
******
Per-protocol population
*43% reduction
83% reduction77% reduction
Primary Endpoint: Cumulative Number of New T1 Gd+ Lesions (Week 12 to Week 24)
Olsson T, et al. J Neurol Neurosurg Psychiatry. 2014;85(11):1198-1208. Reprinted with permission.
Mea
n ch
ange
from
bas
elin
e in
lym
phoc
yte
coun
t (%
)
-80
-70
-60
-50
-40
-30
-20
-10
0
10
Ponesimod 40 mg
Ponesimod 20 mg
Ponesimod 10 mg
Placebo
All-treated set
Day
8
Day
13
We
ek 4
We
ek 8
We
ek 1
2
Wee
k 16
Wee
k 20
Wee
k 24
Maximum Effect on Lymphocytes With 20 mg
Olsson T, et al. J Neurol Neurosurg Psychiatry. 2014;85(11):1198-1208. Reprinted with permission.

Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
40 mg ponesimod
20 mg ponesimod
10 mg ponesimod
Treatment 24 weeks
Randomization
Treatment Period 1 Up to 96 weeks
40 mg ponesimod
20 mg ponesimod
10 mg ponesimod
ExtensionCore
Placebo
Randomization
End of Treatment
Follow-up
Treatment Period 2 Up to 432 weeks
10 mg ponesimod
20 mg ponesimod
10 mg ponesimod
20 mg ponesimod
Ongoing Phase 2 Extension Study in MS1,2
1. Freedman M, et al. AAN 2013 (P01.156). 2. Pozzilli C, et al. ECTRIMS 2013 (P995).
Ponesimod Phase 3 Study Ongoing
OPTIMUM: Oral Ponesimod versus Teriflunomide in RMS
• A multicenter, randomized, double-blind, parallel-group, active-controlled, superiority study
• 200 centers in North America, Latin America, Eastern and Western Europe, Pacific
• 1100 patients randomized 1:1 ratio to either ponesimod 20 mg or teriflunomide 14 mg
• New dose up-titration scheme implemented
• Enrollment ongoing
ClinicalTrials.gov Identifier: NCT02425644
Objectives
• Clinical review of oral agents in late-stage development for MS therapy:– Ponesimod – Phase 2; OPTIMUM
– Ozanimod (RPC1063) – RADIANCE/SUNBEAM
– Siponimod/BAF312 – BOLD; EXPAND
– (MT-1303 – MOMENTUM)
– Laquinimod – CONCERTO, ARPEGGIO

Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Phase 2
1 mg RPC1063
1 mg RPC1063
0.5 mg RPC1063
0.5 mg RPC1063
Blinded Safety-Extension
Phase 3
IFN -1a 30 g IM (N=400)
Interim analysis of Phase 2 (Nov 2013) gated initiation of
Phase 3 (Dec 2013)
RADIANCE Phase 2/3 Trial Overview
Cohen J, et al. Program and abstracts of the 2014 Joint ACTRIMS/ECTRIMS Meeting; September 10-13, 2014; Boston, Massachusetts. Abstract LB1.1. Used with permission.
Patient Disposition
Randomized (N=258)
Placebo (N=88)RPC1063 0.5 mg
(N=87) RPC1063 1 mg (N=83)
Discontinued 3 (3.4%)
Adverse event 0
Lost to follow-up 1 (1.1%)
Protocol violation 0
Consent withdrawn 2 (2.3%)
Discontinued 2 (2.3%)
Adverse event 0
Lost to follow-up 0
Protocol violation 1 (1.1%)
Consent withdrawn 1 (1.1%)
Discontinued 1 (1.2%)
Adverse event 0
Lost to follow-up 0
Protocol violation 0
Consent withdrawn 1 (1.1%)
Completed 85 (96.6%) Completed 85 (97.7%) Completed 82 (98.8%)
• Very high rate of study compliance and completion (252 of 258)
• Favorable tolerability with 249 of 252 completers entering the extension
Cohen J, et al. Program and abstracts of the 2014 Joint ACTRIMS/ECTRIMS Meeting; September 10-13, 2014; Boston, Massachusetts. Abstract LB1.1. Used with permission.
Effects of Ozanimod on GdE Lesions
Primary Endpoint: Total Cumulative Number of GdE Lesions (Weeks 12 to 24)
Secondary Endpoint: Number of GdE Lesions at Week 24
Cohen J, et al. Program and abstracts of the 2014 Joint ACTRIMS/ECTRIMS Meeting; September 10-13, 2014; Boston, Massachusetts. Abstract LB1.1. Used with permission.
GdE: Gadolinium-enhancing
Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
SafetySafety: Ozanimod Adverse
Events (AEs) of Special Interest
• Likely due to S1P pharmacology (eg, fingolimod)
• No notable cardiac, pulmonary, ophthalmologic, infectious, or malignancy TEAEs
• 3 TEAEs of elevated liver enzymes ( ≥3x ULN) without clinical signs issues
– All were isolated ALT elevations, without AST or Bilirubin elevations
– None ≥5x ULN
– Transient elevations despite continued treatment
• Thorough QT Study: Therapeutic dose-titration and supra-therapeutic dosing (N=62); Placebo (N=62)
– No effect on QTc or other CV parameters
Cohen J, et al. Program and abstracts of the 2014 Joint ACTRIMS/ECTRIMS Meeting; September 10-13, 2014; Boston, Massachusetts. Abstract LB1.1.
Adverse Events of Special Interest (AESI)
AEs reported in fingolimod’s label, most related to S1P pharmacology
• S1P1R: Bradycardia (symptomatic or HR<35 bpm), first dose AV block
• S1P3R: Hypertension, cardiac conduction abnormalities (QT prolongation, long-term AV conduction delays)
• S1P1R: Hepatic: confirmed ALT or AST ≥3x ULN
• S1P3R: Pulmonary function: decline in FEV1 or FVC <50% predicted
• S1P1R: Ophthalmologic: new onset or significantly worse macular edema (not explained by an alternative cause)
• Immunomodulation: Malignancy and infection: serious & opportunistic infections
Fingolimod prescribing information. http://www.accessdata.fda.gov/drugsatfda_docs/label/2015/022527s019lbl.pdf
Objectives
• Clinical review of oral agents in late-stage development for MS therapy:– Ponesimod – Phase 2; OPTIMUM
– Ozanimod (RPC1063) – RADIANCE/SUNBEAM
– Siponimod/BAF312 – BOLD; EXPAND
– (MT-1303 – MOMENTUM)
– Laquinimod – CONCERTO, ARPEGGIO
Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
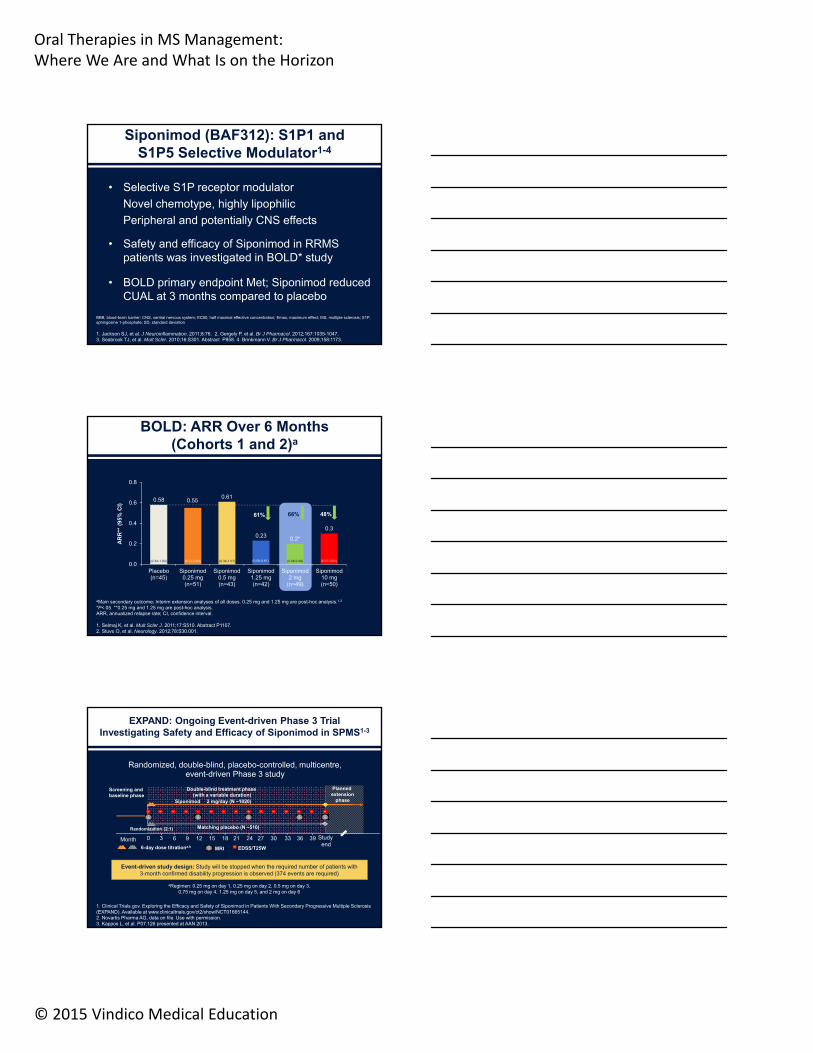
• Selective S1P receptor modulator
Novel chemotype, highly lipophilic
Peripheral and potentially CNS effects
• Safety and efficacy of Siponimod in RRMS patients was investigated in BOLD* study
• BOLD primary endpoint Met; Siponimod reduced CUAL at 3 months compared to placebo
Siponimod (BAF312): S1P1 and S1P5 Selective Modulator1-4
BBB, blood-brain barrier; CNS, central nervous system; EC50, half maximal effective concentration; Emax, maximum effect; MS, multiple sclerosis; S1P, sphingosine 1-phosphate; SD, standard deviation
1. Jackson SJ, et al. J Neuroinflammation. 2011;8:76. 2. Gergely P, et al. Br J Pharmacol. 2012;167:1035-1047. 3. Seabrook TJ, et al. Mult Scler. 2010;16:S301. Abstract P858. 4. Brinkmann V. Br J Pharmacol. 2009;158:1173.
0.58 0.550.61
0.23 0.2*
0.3
0.0
0.2
0.4
0.6
0.8
Placebo(n=45)
Siponimod0.25 mg(n=51)
Siponimod0.5 mg(n=43)
Siponimod1.25 mg(n=42)
Siponimod2 mg
(n=49)
Siponimod10 mg(n=50)
AR
R**
(95
% C
I)
(0.34-1.00) (0.32-0.93) (0.34-1.07) (0.08-0.61) (0.08-0.48) (0.15-0.61)
61% 66% 48%
BOLD: ARR Over 6 Months(Cohorts 1 and 2)a
aMain secondary outcome; Interim extension analyses of all doses. 0.25 mg and 1.25 mg are post-hoc analysis.1,2
*P<.05. **0.25 mg and 1.25 mg are post-hoc analysis.ARR, annualized relapse rate; CI, confidence interval.
1. Selmaj K, et al. Mult Scler J. 2011;17:S510. Abstract P1107. 2. Stuve O, et al. Neurology. 2012;78:S30.001.
Randomized, double-blind, placebo-controlled, multicentre, event-driven Phase 3 study
Event-driven study design: Study will be stopped when the required number of patients with 3-month confirmed disability progression is observed (374 events are required)
Studyend
Double-blind treatment phase (with a variable duration)
Planned extension
phase
Screening and baseline phase
Matching placebo (N ~510)
2 mg/day (N ~1020)
6-day dose titrationa,b
Siponimod
362412
MRI EDSS/T25W
15 18 21 279630 30 33 39
Randomization (2:1)
Month
aRegimen: 0.25 mg on day 1, 0.25 mg on day 2, 0.5 mg on day 3, 0.75 mg on day 4, 1.25 mg on day 5, and 2 mg on day 6
EXPAND: Ongoing Event-driven Phase 3 Trial Investigating Safety and Efficacy of Siponimod in SPMS1-3
1. Clinical Trials.gov. Exploring the Efficacy and Safety of Siponimod in Patients With Secondary Progressive Multiple Sclerosis (EXPAND). Available at www.clinicaltrials.gov/ct2/show/NCT01665144.2. Novartis Pharma AG, data on file. Use with permission. 3. Kappos L, et al. P07.126 presented at AAN 2013.
Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
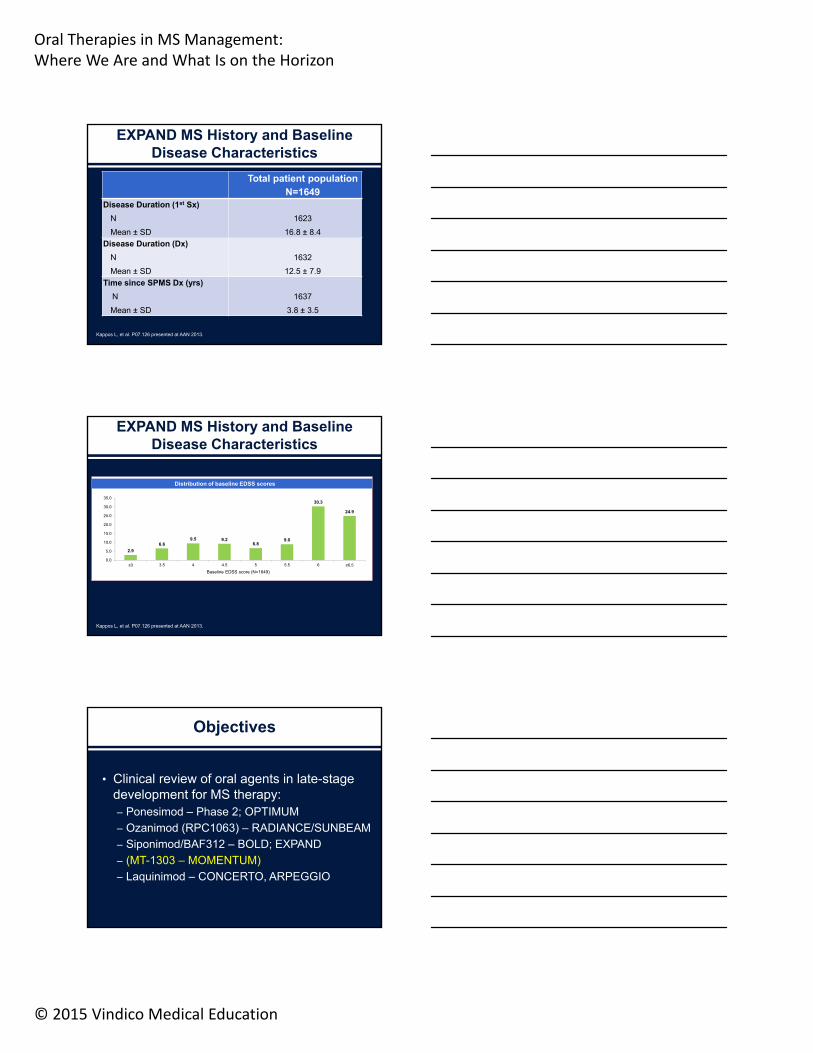
Total patient populationN=1649
Disease Duration (1st Sx)
N
Mean ± SD
1623
16.8 ± 8.4
Disease Duration (Dx)
N
Mean ± SD
1632
12.5 ± 7.9
Time since SPMS Dx (yrs)
N
Mean ± SD
1637
3.8 ± 3.5
EXPAND MS History and Baseline Disease Characteristics
Kappos L, et al. P07.126 presented at AAN 2013.
EXPAND MS History and Baseline Disease Characteristics
Kappos L, et al. P07.126 presented at AAN 2013.
2.9
6.69.5 9.2
6.89.0
30.3
24.9
0.0
5.0
10.0
15.0
20.0
25.0
30.0
35.0
≤3 3.5 4 4.5 5 5.5 6 ≥6.5
Baseline EDSS score (N=1649)
Distribution of baseline EDSS scores
Objectives
• Clinical review of oral agents in late-stage development for MS therapy:– Ponesimod – Phase 2; OPTIMUM
– Ozanimod (RPC1063) – RADIANCE/SUNBEAM
– Siponimod/BAF312 – BOLD; EXPAND
– (MT-1303 – MOMENTUM)
– Laquinimod – CONCERTO, ARPEGGIO

Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
Results of MOMENTUM, a randomized, double-blind, placebo-controlled, Phase 2 trial with
MT-1303, a novel selective sphingosine 1-phosphate receptor 1 (S1P1) modulator, in
relapsing-remitting MS
Ludwig Kappos, Douglas Arnold, Amit Bar-Or, John Camm, Tobias Derfuss, Bernd Kieseier, Till Sprenger, Kristin Greenough, Pingping Ni, Tomohiko Harada and the
MOMENTUM [email protected]
Late Breaking News Presentation, Saturday,October 10, 2015
Objectives
• Clinical review of oral agents in late-stage development for MS therapy:– Ponesimod – Phase 2; OPTIMUM
– Ozanimod (RPC1063) – RADIANCE/SUNBEAM
– Siponimod/BAF312 – BOLD; EXPAND
– (MT-1303 – MOMENTUM)
– Laquinimod – CONCERTO, ARPEGGIO
Laquinimod: Results From RRMS That Provide a Rationale for PPMS Study1,2
0
5%
10%
15%
25%
27%
4.8%
7.6%
Placebo
Laquinimod 0.6 mg
20%
18.9%
22.1%
39%
Relapse-free (n=1220) Relapsing (n=770)
prop
ortio
n of
pat
ient
s ex
peri
enci
ng 3
-mon
th C
DP
1. Comi G, et al. AAN 2014: P3.195. 2. Sorman MP, et al. Neurology. 2010 27;75(4):302-309.Reprinted with permission.
CDP: confirmed disability progression

Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education
A multinational, multicenter, randomized, double-blind, parallel-group, placebo-controlled study followed by an active treatment period, to evaluate the efficacy, safety, and tolerability of 2 doses of oral administration of laquinimod (0.6 or 1.2 mg/day) in subjects with relapsing remitting multiple sclerosis (RRMS).
CONCERTO Design
Primary endpoint: 3 months confirmed disability progression
Secondary endpoints: BA and time to first relapse
Exploratory endpoints: Include cognitive (Symbol Digital Modalities Test), MRI, and quality of life measures
Vollmer T, et al. ECTRIMS 2013:P1054. Used with permission.
= EDSS, T25FW, 9HPT, SDMT, MSWS
= MRI Brain and C-spine
4Week 80 12 24 36 48 Every 12 weeks
Completion visit
Screening
LAQ 1.5 mg/dayLAQ 1.5 mg/day
Placebo dailyPlacebo daily
LAQ 0.6 mg/dayLAQ 0.6 mg/day
Part A(Core)
Part B(Data Analysis)
= OCT, BICAMS= LCVA
1:1:1 Randomization1:1:1 Randomization
ARPEGGIO Design
Giovannoni G, et al. AAN 2015:P7.210. Used with permission.
Objectives
• Clinical review of oral agents in late-stage development for MS therapy:– Ponesimod – Phase 2; OPTIMUM
– Ozanimod (RPC1063) – RADIANCE/SUNBEAM
– Siponimod/BAF312 – BOLD; EXPAND
– (MT-1303 – MOMENTUM)
– Laquinimod – CONCERTO, ARPEGGIO

Oral Therapies in MS Management:Where We Are and What Is on the Horizon
© 2015 Vindico Medical Education