Embed Size (px)
Citation preview

Acute & Chronic Headache
presenting to A&E & AMU
Royal College of Physicians, London 24th October 2016
Dr Brendan Davies
Midlands Regional Headache Clinic
& Department of Neurology
Royal Stoke University Hospital
University Hospital of North Midlands

Outline
• The Epidemiology of Acute & Chronic Headache
– “Is there a problem?
– The problem of “Just do a brain scan” !!
– Do we know what we are looking for?
• Its all in the History ?
– Video Cases & Interactive
• Final Thoughts.......

Acute & Chronic Headache scope -
It depends where you sit & where you look !!
Population Headache Epidemiology Incidence
• SAH 8-12 per 100, 0000
• Dissection 3-5 per 100,000
• Brain Tumour 10-12 per 100,000 – Only 50-60% ever have headache
& Prevalence
• Migraine 6-18 per 100
• Cluster HA 1 per 1,000
“Acute” Headache Referrals
to secondary care
1-2% of all presentations to A & E
– Self-presentation
– GP referral
Medical admissions to an Acute Neurology Service
Carroll & Zajicek. (2004) JNNP; 75: 406-409
Primary symptom = Headache 24%
Subarachnoid haemorrhage 1%
CNS infection (meningitis/encephalitis) 2.5%
Primary headache 13%
Head injury 0.2%
Other 7.3%
Chronic Headache Epidemiology – Both primary & Secondary !!
Prevalence
• All forms Primary CDH 2-4% population
• Chronic Migraine 2% population
• Medication overuse HA 1% population
• Others
• CSF Pressure related - IIH & SIH
• Post-Traumatic

Why don`t we just do a scan - that
will reassure us and the patient?

• 19,6000 people; 16 studies
• Mean age 11-63 years old
• Prevalence of any incidental brain
finding = 2.7%
No. Needed to scan = 37
• Any Neoplastic finding = 0.7%
(95% CI 0.47-0.98)
No. Needed to scan = 143
• Any Non-Neoplastic finding = 2.0%
(95% CI 1.1-3.1%)
No. Needed to scan = 50
• Higher resolution scan = ↑ prevalence

Why do patients with headache present
to the Emergency Department?
• New severe headache especially if progressive..!
– unlike anything they have had before
– “First and Worst “
• Associated features that are concerning
– for example: Severity, persistence, altered mental state, fever,
focal neurological symptoms and / or signs
• At the end of their tether with new onset, persistent or
recurrent headaches that are unresponsive to treatment
Personal observations & Adapted from Edmeads J. Headache. 1990;30:537-540.

Headache presenting
to the ED in UK
• Locker et al. Headache 2006;46:954-961
(Northern General Hospital, Sheffield)
• Prospective observational study - Alert adult patients
• UK Emergency department - 14 month period
– 3 month follow-up
• 91,509 ED attendances - 0.85% were for headache
– 42% due to 2° cause
– 55% Primary Headaches
• Migraine > Cluster > NOS ??? (TN & TTH)
– 22% recurrent headaches 126
– 18% headache + associated features 101
• Remit of ED is to exclude serious Secondary
headache?
– No good data on Chronic headache presentations
Serious pathological cause 13.4%

“Red Flags”
Clinically important headache
patterns to recognise in A&E
• Acute “Thunderclap Headache” (TCH)
• “Acute” Headache PLUS*”
• New “Progressive (Worsening)” Headache PLUS*
PLUS* Equates to:
– persisting focal neurological signs
– +/or ↓ed GCS or altered mental state-behaviour
– Fever
– Seizures & “SNOOP – TO”

CASE • 48 yrs male Rt handed – No prior history of Headache
PHx Hypertension FHx – Uncle had “Brain haemorrhage”
02.30 Dec 2011
– Woken suddenly Excruciating Holocranial pain
– Volunteered “Worst ever pain he had experienced”
– Vomited, Photophobic after about an 1 hour – stoical so waited until morning
09.30 - Saw Out of Hours GP - Assessed & Examined. No abnormal signs
– Told he was fine and told if gets worse call Ambulance to go to A&E
– Told it was a migraine – sent home by on call GP emergency clinic
2 days later – Sent by own GP to On-Call Acute Neurology Service via A&E
– Persistent Headache, double vision
– Exam showed = Right eye Ptosis, Mdriasis & Rt. Complete Opthalmoplegia
Differential Diagnosis ??

Diagnosis?

Q1. What do you think is the diagnosis?
1. Acute Severe Migraine with aura variant
2. Basilar Type Migraine
3. Acute Subarachnoid Haemorrhage
4. Acute Cluster Headache
5. Reversible Cerebral Vasoconstriction Syndrome (RCVS)
6. Acute Maxillary Sinusitis
7. Pituitary Apoplexy
8. Other?

Pituitary Apoplexy on CT & MRI

“Thunderclap” headache
• Thunderclap Headache (ICHD Beta III - 2013) – High-intensity headache of abrupt onset
– Peak in < 1 minute
• No reliable way of differentiating between primary and secondary thunderclap headache
• ⅓ presentations to the ED with thunderclap headaches are due to a potentially life threatening / disabling neurological condition

“Radiology says No”
Thanks to Dr S Weatherby, Plymouth for the slide

Sensitivity of CT to detect radiological evidence of
SAH decreases over time (Van Gijn, 1982 Kassel, 1990 van der Wee,1995 Sames, 1996 )
– In the 1st 12 hours 98-100%
– Within 24 hours 92-95%
– Within 48 hours 86%
– At 5 days 58%
– At 7 days 50%
– After 2 weeks 30%
– After 3 weeks Almost nil
Neuromythology - “the CT can wait?”
CT
sensitivity
decreases
over time
Utilising 3rd-5th generation CT scanners & neuroradiologist
Investigations: early brain CT (ASAP)
High initial sensitivity (decreases with time)

Potentially overlooked SAH
• A - subarachnoid blood in
anterior interhemispheric
cistern & both Sylvian fissures
from AcoM anneurysm SAH
• B - Disappearance of cisternal
blood on
repeat CT scan after 2 days
• Early Hydrocephalus due to SAH
Patterns of SAH on CT brain imaging

• Prospective study; Modern 3rd generation scanners, Neuroradiologist
• 3,132 patients with suspected acute SAH (Canada) – 11 A&E depts.
– >80% worst headache ever
– CT then LP for xanthochromia (not Spectrophotometry !)
• 953 patients scanned < 6 hours – No CT – ve , LP +ve SAH
• All 121 patients with SAH identified - 100% PPV & NPV with
specificity 100%.
• Advised Caution over 6 hours !!
Controversial Study – Advocates no need for LP if
CT okay within 6 hours of HA onset

Recent UHNM “Suspected SAH & Acute Headache”
CSF & Xanthochromia Testing Audit when CT Normal
• 6 month review of Xanthochromia results - 95 requests
– 61 cases via Acute Neurology Unit
– NO Positive CSF Xanthochromia results....... !!
– 9 of 65 (15%) Other non-SAH - Secondary Headaches
• 4 of 61 had Viral meningitis*
• 2 of 61 - IIH* 1 of 61 with CVST*
– CSF Analysis necessary to make HA diagnosis in ≈ 10%
• Other Primary Headaches >19.6% (ICHD-3 beta 2013 criteria)
• 10 of 61 - Primary Thunderclap Headache
• 1 of 61 - Primary Coital (Orgasmic) headache
• 1 of 61 - Primary Exertional Headache

• Thunderclap headache (TCH) alone in 75%
– Usually recurrent (> 90%) – days to weeks
• Cerebral vasoconstriction on angiography
– Multi-focal & segmental
– Reversible within 3 months
1st week 2nd week
10
0
3rd week
HA
Se
ve
rity
“Recurrent Thunderclap Headache - RCVS?

• Transient or persistent focal symptoms – Visual>unilateral sensory > aphasia> motor weakness
– “TIA like” or “migrainous aura” like
• Early complications: < 1 week from recurrent TCH onset
– Intra-cerebral haemorrhage & cortical SAH
– PRES - posterior reversible leucoencephalopathy syndrome
– Seizures (rare)
• Late complications: > 1 week from recurrent TCH onset
– TIA & ischaemic stroke
RCVS – symptoms & time course Ducros et al (2007), Brain; 130: 3091; Calabrese et al (2007), Ann Intern Med; 146: 34

Brain & angiographic findings in RCVS Ducros et al, 2007
• A & B = small cortical SAH
• C = occipital intracerebral haemorrhage
• D = sequelae of bilateral occipital infarcts and left frontal-parietal infarct
• E & F = acute PRES on FLAIR and resolution of PRES 1 month later

Prospective 12 month study study – 34 patients
– Dutch Acute Neurology service
– Acute TCH > 6 hrs duration; Severity >8/10
– consecutive CT –ve & LP –ve TCH patients
– 5 had recurrent TCH over a week (2 of 5 had RCVS)
• Overall - 8% had RCVS on 3T MRI & MRA (3 of 34)
– 2:1 female: male ratio
– 2 associated with vasoactive substances ingestion
• 82% - Idiopathic TCH (28 of 34)

“Thunderclap Headache” (TCH) “So If it’s not a SAH what else commonly needs consideration?”
• Intracranial infection
– Meningitis
• Vascular disease
– Subarachnoid haemorrhage (10-25%)
– Cervical artery dissection (10+%)
– Cerebral venous sinus thrombosis
(2-10%)
– Pituitary Apoplexy
– Ischaemic & Hemorrhagic stroke
– Reversible cerebral vasoconstriction syndrome (8%)
• CSF pressure related
– Spontaneous intracranial hypotension (10-15%)
– Third ventricle colloid cyst
• Metabolic
– Acute hypertensive crisis
– Phaeochromocytoma
• Miscellaneous
– Retroclival haematoma
– Sphenoid Sinusitis
• Primary headaches**
– Primary (idiopathic) thunderclap headache
– Exploding head syndrome • Not a pain disorder
• A perceptual disorder

With thanks to patient for consent

Q2. What do you think is the diagnosis?
1. Migraine (with visual) aura in a known migraine sufferer
2. Giant Cell Arteritis
3. Acute Subarachnoid Haemorrhage
4. Basilar Type Migraine
5. Posterior Circulation TIA
6. Acute Dissection
7. Acute Optic Neuritis
8. Other?

Acute Cervical Arterial dissection Thunderclap Headache onset presentation in 10-20% NB Associated Neck Pain
Carotid Dissection • Unilateral headache/face pain
+/- • Ipsilateral Horners syndrome
• Contralateral TIA / stroke
• Ipsilateral cranial nerve palsies – X, XII >> than VII, II
Vertebral dissection • Acute Headache &
Posterior circulation TIA / Stroke
• *Very Rare as “Isolated headache” – 2-8% of cases
He
ad
ach
e In
ten
sity

Cervical Arterial Dissection - Appropriate Investigation
• MRI Brain & Neck & MRA (Carotids & vertebral)
Crescent shaped intramural haematoma & vessel occlusion identifies
ischaemic brain tissue > clearly
• CT Brain & CTA of cervical vessels
Tapering lumen, vessel occlusion
• Carotid ultrasound not sensitive enough
Vertebral artery
dissection
Carotid artery
dissection

• Anti-platelet therapy vs. Warfarin for 3 months
• Treatment < 7 days post Extra-cranial dissection
– Stroke/TIA = 234
– Painful Horner’s syndrome, Headache = 24
• Overall 2% Stroke risk < 3 months i.e. Very low ....
– None in “TIA/Stroke” presentations
– None in late presenters

Chronic Headache Cases
Its all in the history !!

Chronic Daily headache
How to Approach diagnosis
Primary Headache
disorders
Secondary
Headache disorders
Paroxysmal Headache
Attack Duration < 4 hours +/or
Discrete episodes
Long lasting Headache
Daily or near daily headache
Duration > 4 hours per day
Chronic Migraine
New Daily
Persistent
headache
Hemicrania
Continua
Adapted from Silberstein et al., Neurology (1996) 47: 871-
With or without medication overuse
Chronic
Tension Type
Headache

52 yrs male, self employed – no prior headache
• 8/52 Hx - New onset daily headache at DGH
• Onset with presumed upper respiratory tract infection
– Constant holocranial throbbing, nausea & neck pain
• Headache free on awakening & started <1/2 hour after
waking
• Headache improved with bedrest each day
Examination: GCS 15 & Apyrexial,
C/o Severe HA & Neck pain and wanting to lie down
No menningism or systemic toxicity
No focal Neurological signs or Papiloedema
•

Q3. Headache Diagnosis?
1. Acute Bacterial or Viral Meningitis
2. Brain tumour
3. Idiopathic Intracranial Hypertension
4. Cerebral Venous Sinus Thrombosis
5. Chronic Migraine
6. Giant Cell Arteritis
7. Spontaneous Intracranial Hypotension
8. A Chronic daily headache –”Tell him to stop whinging !”
9. Other?

Investigations & Initial Management
CT Brain - Bilateral chronic subdural collections
– Effaced Cerebral sulci & No shift
– Lt 8mm, Rt 7mm thickness
• ER
What would you do now?

Q4. What would you do now?
1. Do nothing – send him home with GP Follow-up
2. Do nothing – Reassure & watch & wait & rescan as OPD
3. Start Amitriptyline - Reassure & watch & wait
4. Phone Neurosurgery & ask for transfer +/or advice
5. Phone Neurology & ask for advice + / or transfer
6. Take a more detailed history
7. I don’t know.......

• Management @ DGH:
– Referred & Transferred to local Neurosurgery Unit
• Neurosurgical Centre Management:
– Bilateral Burr hole drainage
– 24 hour Post OP CT:

Day 1 & 2 - Post Op
“Ohh ….Dr !! - My headache is worse”
• 1st week post-op – ↑ severe HA
– Increased Orthostatic HA & Neck pain
– Vomiting & variable impaired hearing
– Decreased conscious level & obtundation
• Neurosurgery Senior Re-review
– Revisited the history & Investigations !!
– MRI with Contrast ordered – “SEEPS +ve”

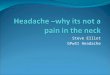
The 5 characteristic Brain MRI abnormalities
of Spontaneous Intracranial Hypotension
(Shievinik WI. JAMA 2006; 295; 2286-2296)
“SEEPS”
S Subdural fluid collections
E Enhancement of (Pachy) meninges
E Engorgement of veins
P Pituitary hyperaemia / posterior fossa crowding
S Sagging of brain

Brain MRI & Gd-DTPA contrast
Bilateral SDH & diffuse
Pachymeningeal dural enhancement

• History – Orthostatic HA & Bilateral atraumatic SDH
– No trauma, No ETOH XS, Normal clotting
– Not hypermobile, No LP prior to NDPH onset
Subsequent Management:
• Supine bedrest
• L3-4 Lumbar Epidural Blood Patch - 40ml
– 90% HA resolution < 24 hrs
– HA resolution by 1 week – Still Asymptomatic at 6/12
Final Diagnosis
SIH - exacerbated by Burr Hole drainage

Spontaneous Intracranial Hypotension (SIH) New onset persistent Orthostatic headache

25% of non-geriatric Patients with Bilateral atraumatic
subdural had evidence of a CSF leak

Diagnostics in Suspected SIH
• TCH onset in 10-15%
• May be onset event – Trauma? Cough? Valsalva?
• CT Brain often Normal !!
• CSF Pressure < 60mm H20 ? (but can be normal!)
– Normal glucose but may - WCC, Protein, RBC
• Gd-DTPA is investigation
of 1st choice
– Diffuse linear Non-nodular
Pachymeningeal enhancement

How do Chronic Daily Headache disorders start ?
Time
Evolving CDH
Time
NDPH
Headache Free before
daily headache
De novo (Acute?)
headache onset
Hea
da
che
sev
erit
y

“SNOOP - TO” Red flags for secondary headache
•Systemic symptoms (fever, weight loss)
– or Secondary risk factors (systemic disease, cancer, HIV )
•Neurologic symptoms +/or abnormal signs
– (confusion, impaired alertness or consciousness, focal signs)
•Onset:
– sudden, abrupt, or split-second or worsening & progressive
•Older:
– new-onset and progressive headache, especially in middle age, >50 years (giant cell arteritis)
•Previous headache history:
– first headache or different (significant change in attack frequency, severity, or clinical features)
•Triggered headache
By Valsalva activity, exertion, or sexual intercourse
•Orthostatic
–Reliable worsening with erect compared to supine posture
Adapted from Silberstein SD et al. Wolff’s Headache and Other Head Pain. 2001:6-26.

Even when “Radiology says YES” Important Acute SecondaryHeadaches
where Brain CT scan can be normal
• Subarachnoid Haemorrhage
• Meningoencephalitis
• Cerebral Venous Sinus Thrombosis
• Carotid & Vertebral Arterial dissection
• RCVS
• Temporal Arteritis
• Malignant Hypertension
• Head Injury, IIH
& CSF Hypovolaemia (SIH)
History, History,
History !!!..........

6th Keele Biennial Headache Teaching Course
University of Keele
Staffordshire
Application forms - [email protected]
www.bash.org.uk June 29th-Sat 1st July 2017