Embed Size (px)
Citation preview

Acute Arterial Occlusion
Junainah D. Benito

What is Acute Arterial Occlusion?• Results in the sudden cessation of blood flow
to an organ or body part

Causes of Acute Arterial OcclusionEmbolus Thrombosis Trauma
Cardiac source Vascular grafts Blunt Atrial fibrillation Atherosclerosis Penetrating Myocardial infarction Thrombosis of aneurysm Iatrogenic Endocarditis Entrapment syndrome Valvular disease Hypercoagulable state Atrial myxoma Low flow state Prosthetic valvesArterial source Aneurysm Atherosclerotic plaqueParadoxical embolus

Symptoms• Arms or legs:
– Cold arm or leg – Decreased or no pulse in an arm or leg – Fingers or hands feel cool – Lack of movement in the arm or leg – Muscle pain in the affected area – Muscle spasm in the affected area – Numbness and tingling in the arm or leg – Pale color of the arm or leg (pallor) – Weakness of an arm or leg

Symptoms• Later symptoms:
– Blisters of the skin fed by the affected artery – Shedding (sloughing) of skin – Skin erosion (ulcer) – Tissue death (necrosis; skin is dark and damaged)

Symptoms• Organ:
– Pain in the part of the body that is involved – Temporarily decreased organ function

Treatment Options• Endovascular Therapy
– Peripheral Transluminal Angioplasty– Peripheral Stenting– Atherectomy– Thrombolytic Therapy– Embolic or foreign body retrieval
• Surgery– Bypass grafts– Fasciotomy– Amputation– Endarterectomy

Considerations for Endovascular and Surgical Therapy
• Location and length of the occlusion• Etiology (Embolus vs thrombus)• Duration of ischemia• Native artery or graft• Patient-related risks• Intervention-related risks• Contraindications to thrombolysis

Lower Extremity Acute Ischemia2007 Inter-Society Consensus for the
Management of Peripheral Arterial Disease (TASC II)• Acute limb ischemia is defined as a sudden decrease
in limb perfusion that causes a potential threat to limb viability (manifested by ischemic rest pain, ischemic ulcers, and/or gangrene) in patients who present within two weeks of the acute event
• Patients with similar manifestations who present later than two weeks are considered to have critical limb ischemia, which is by definition chronic

Lower Extremity Acute Ischemia• Clinical Evaluation
– History & PE– Five P’s:
• Pain• Pulselessness• Pallor• Paresthesias• Paralysis• Poikilothermia or “perishing cold” (6th “P”)

Lower Extremity Acute Ischemia• Classification:
– Viable limbs – Threatened limbs – Nonviable extremities

Lower Extremity Acute Ischemia
Category DescriptionCapillaryReturn
MuscleParalysis
SensoryLoss
Doppler SignalsArterial Venous
I Viable Not immediately threatened
Intact None None Audible Audible
IIa Marginally Threatened
Salvageable if treated
Intact/slow None Partial Inaudible Audible
IIb Immediately Threatened
Salvageable if treated as emergency
Slow/absent Partial Partial Inaudible Audible
III Irreversible Primary amputation frequently required
Absent Complete Complete Inaudible Inaudible

Lower Extremity Acute Ischemia• Diagnostic Tests
– Arteriography• Embolus: Sharp cutoff with a rounded reverse
meniscus sign.– Intraluminal filling defect if the vessel is not
completely occluded. –Presence of otherwise normal vessels, the
absence of collateral circulation, and the presence of multiple filling defects.

Lower Extremity Acute Ischemia• Diagnostic Tests
– Arteriography• Arterial thrombosis: Sharp or tapered, but not
rounded, cutoff.–Diffuse atherosclerosis with well developed
collateral circulation is generally present.

Lower Extremity Acute Ischemia• Treatment
– Thrombolytic therapy– Surgical revascularization

Lower Extremity Acute Ischemia• Treatment: Thrombolytic therapy
Diagnosis of AAO
10,000 units of IV heparin
continuous heparin infusion
surgery or thrombolytic therapy

Lower Extremity Acute Ischemia• Treatment: Surgery
– Patients with threatened extremities: emergent surgical revascularization Embolectomy Intraoperative completion arteriogram Intraoperative thrombolytic therapy Fasciotomy

Lower Extremity Acute Ischemia• Treatment: Surgery
– Patients with viable extremities: Intraarterial thrombolysis

Lower Extremity Acute Ischemia• Treatment: Surgery
– Patients with viable extremities: Intraarterial thrombolysis

Lower Extremity Acute Ischemia• Treatment: Surgery
– Patients with nonviable extremities: prompt amputation.
– Delays in amputation can result in Infection Myoglobinuria acute renal failure Hyperkalemia


Treatment PathwayAcute Arterial
Occlusion(thromboembolism)
Heparin unlesscontraindicated
Class Iviable
Treat as per
chronicLimb
ischemia
Class IIaMarginallythreatenedClose monitorin
gUrgent
angiography
Class IIbImmediately threatened
Urgent thromboembolect
omy
Class IIINot viable
AmputationAfter
demarcation

Complications of Revascularization• Reperfusion syndrome
– Hypotension– Hyperkalemia– Myoglobinuria– Renal failure
• Compartment syndrome• Ischemic neuropathy• Muscle necrosis• Recurrent thrombosis

Reperfusion Syndrome• Is the paradoxical and complex phenomenon of
exacerbation of cellular dysfunction and increase in cell death after the restoration of blood flow to previously ischemic tissues.
• Massive wash out of lactate, potassium, myoglobin, with resultant systemic acidosis, hyperkalemia, myoglobinuria and free radicals releasing.
• Simultaneously, the acutely revascularized limb develops massive edema, hemoconcentration and hypovolemia with subsequent impairment of the renal function

Reperfusion Syndrome• There are two components which follows extremity
ischemia: – Local response, which follows reperfusion, consists
of limb swelling with its potential for aggravating tissue injury
– Systemic response, which results in multiple organ failure and death.

Reperfusion Syndrome• Treatment
– Fasciotomy– Anticoagulation– Amputation

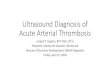
Compartment Syndrome• It is an acute medical problem following injury,
surgery or in most cases repetitive and extensive muscle use, in which increased pressure within a confined space (fascial compartment) in the body impairs blood supply.
• Most commonly seen in the anterior compartment and posterior compartment of the leg.
• Irreversible nerve damage & muscle death

Compartment Syndrome

Compartment Syndrome• Causes
– Tibial or forearm fractures– Ischemic-reperfusion following injury– Hemorrhage– Vascular puncture– Intravenous drug injection– Casts– Prolonged limb compression– Crush injuries– Burns

Compartment Syndrome• Clinical manifestations
– Excessive pain in the compartment– Pain on passive stretching of the compartment– Sensory loss– Numbness in the web space between 1st & 2nd toes– Skin changes

Compartment Syndrome• Treatment:
– Fasciotomy

THANK YOU!