Embed Size (px)
Citation preview

Acute Assessment and
Treatment of Asthma
Melanie Clements
Consultant Paediatrician
Feb 2014

Asthma is one of the most common
long term conditions in the UK, affecting
5.4 million people, of which 1.1 million are
children. Asthma is the most common
long-term medical condition for children.
Caring for people who experience
an asthma attack costs 3.5 times
more
than caring for those whose asthma
is well managed.
Most patients can achieve
effective control of their asthma in
partnership with primary care.
Many children with asthma have
poor control of their condition,
often as a consequence of poor
compliance with therapy. This may
lead to exacerbations of the
condition and hospital
admissions.
On average 3 people per day or
1 person every 8 hours dies
from
asthma in the UK
There were 80,000 emergency
hospital admissions for asthma in
the UK in 2008-09. Of these, 30,000
were children under 14;
An estimated 75% of hospital
admissions for asthma and as many
as 90% of the deaths from asthma
are preventable.
Paediatric asthma represents
4% of primary care activity

Getting the Basics Right
“We come together; Inhaler + Plan = 1
http://changeday.nhs.uk/campaign?select=2863

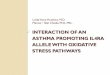
The Evidence Base

Variation in care

0
50
100
150
200
250SD
R p
er
10
0,0
00
Austria
Finland
France
Germany
Greece
Italy
Netherlands
Portugal
Spain
Sweden
United Kingdom
Deaths in children 0-14 years
0
10
20
30
40
50
60
2005-2007 2006-2008 2007-2009 2008-2010
Ingrid Wolfe, Lancet, Mar
2013

0
5
10
15
20
25
30
0
0.05
0.1
0.15
0.2
0.25
0.3
Sweden Portugal Finland Italy Austria Germany Spain UnitedKingdom
Pe
rce
nta
ge w
he
eze
10
ye
ar S
DR
pe
r 1
00
00
0 (
0-1
4 y
ear
s)
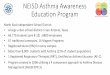
Mortality
6-7 age group
13-14 agegroup
Asthma mortality and children with wheeze
Ingrid Wolfe, Lancet, Mar
2013

Stories

Do we need assessment and treatment tools?
http://www.ted.com/talks/atul_gawande_how_do_we_heal_medicine.html

What’s
normal?

The journey so far
Children and young people emergency and urgent care pathway
Parents/CarersSelf HelpInternet
Digital TVPharmacistNHS Direct
ProfessionalsHealth Visitors
CommunityChildren’s Nurses
Social Services
A&E Children’s A&E
Urgent Care Centre
Ambulance
GP PracticeOut of Hours Service
MIMI Unit*Walk in Centre
Children’s Assessment
Unit
Ward
Children’s Critical
Care
Community Care
HomeCAMHS**
Dedicated children’s environment and play facilitiesChildren and young people’s trained workforce
Child protection systemsSystem wide information
CYP and Family Involvement
* Minor illness, Minor Injury Unit
** Child and Adolescent Mental Health Service
Self Referral
Referral from the community
Open AccessSelf referral
Children, Young People and Families
Commissioners

Acute Assessment

Acute Treatment

Discharge & FU

Under 2yrs

Respiratory Distress
• Recession
• Head bobbing
• Anxious demeanour
• Flared nostrils
• Grunting
• Stridor or wheezing
• Exhaustion
• Tachypnoea
• Use accessory muscles
• Hyper expanded
• Poor tidal Volume
• Abdominal breathing
• Prolonged expiration

Asthma Management Plan

Children age 5-12 yrs

2008/12 Guidelines - Diagnosis
Recurrent respiratory symptoms:
> than 1 of: • cough • wheezing • difficulty breathing • chest tightness

Asthma in children
Differential Diagnosis: •Upper, lower & non-respiratory causes: •Rhinnitis, secretions •ENT
• Foreign body, • vocal cord dysfunction, • vascular rings • laryngeal webs, • tracheomalacia, or stenosis
• Bronchiolitis •Cystic Fibrosis
Bush A. Diagnosis of asthma in children under five. Prim Care Respir J. 2007;16:7–15.

Asthma More Likely
Frequent/Recurrent
Night & Early morning
Exercise
Triggers
Intercurrent symptoms
Atopy/eczema
Family history
Wheeze
Responds to treatment

Asthma Less Likely
Symptoms with colds only
No interval symptoms
Isolated cough or moist cough
Dizzy, light-headed, tingling
Repeat normal examination of chest when symptomatic
Normal PEF with symptoms
No response to treatment

Poor treatment response
23

Reasons for poor asthma control
• Wrong diagnosis
• Poor inhaler technique
• Smoking
• Rhinitis
• Non adherence
• Variation in treatment response
• Under treatment
• Exposure to allergen



https://spottingthesickchild.com/?

Case 1: 8yr old F DoD: 2002
• Severe asthma
• Multiple previous hospital admissions
• Medication: flixotide, salmeterol, salbutamol, prednisolone (BTS step 4)
• Good compliance / Good inhaler technique
• No asthma management plan
• Atopic child: eczema (severe in the past), ?dog allergy

• Fatal attack:
• Seen by GP 16hrs prior to death, diagnosis: croup (in retrospect: asthma), no treatment given.
• Seen by GP in community hospital 4 hrs prior to death, given nebs and Prednisolone, not admitted
Presented to hospital with respiratory arrest

Case 2: 9yrs old F DoD: 2004
• Mild/moderate asthma
• Medication: inhaled steroids, salmeterol prn (not salbutamol) (BTS step 2-3)
• Poor compliance
• No previous hospital admissions
• Atopic: eczema, allergy to animals
• Autistic, learning difficulties

• Fatal attack: • Wheezy all day at school, • Playing with guinea pig in friend’s bedroom prior to attack,
• Sudden deterioration, • Parents declined ambulance, died on route to hospital