Embed Size (px)
Citation preview

4 8 6 Clinical and laboratory observations The Journal of Pediatrics March 1992
R E F E R E N C E S
1. Bloom JN, Palestine AG. The diagnosis of cytomegalovirus retinitis. Ann Intern Med 1988;109:963-9.
2. Holland GN, Sidikaro Y, Kreiger AE, et al. Treatment of cy- tomegalovirus retinopathy with ganciclovir. Ophthalmology 1987;94:815-23.
3. Jacobson MA, O'Donnell J J, Brodie HR, Wofsy C, Mills J. Randomized prospective trial of ganciclovir maintenance ther- apy for cytomegalovirus retinitis. J Med Virol 1988;25:339-49.
4. Buhles WC, Mastre B J, Tinker A J, et al. Ganciclovir treat- ment of life- or sight-threatening cytomegalovirus infection: experience in 314 immunocompromised patients. Rev Infect Dis 1988;10:$495-506.
5. Fanning MM, Read SE, Benson M, et al. Foscarnet therapy of cytomegalovirus retinitis in AIDS. J Acquir Immun Defic Syndr 1990;3:472-9.
6. Jacobson MA, O'Donnell J J, Mills JF. Foscarnet treatment of cytomegalovirus retinitis in patients with the acquired immu- nodeficiency syndrome. Antimicrob Agents Chemother 1989; 33:736-41.
7. Lehoang P, Girard B, Robinet M, et al. Foscarnet in the treat- ment of cytomegalovirus retinitis in the acquired immune de- ficiency syndrome. Ophthalmology 1989;96:865-74.
8. Walmsley S, Chew E, Read SE, et al. Treatment of cytome- galovirus retinitis with trisodium phosphonoformate hexahy- drate (foscarnet). J Infect Dis 1988;157:569-72.
9. Freitas VR, Fraser-Smith E, Matthews T. Increased efficacy of ganciclovir in combination with foscarnet against cytome- galovirus and herpes simplex virus type 2 in vitro and in vivo. Antiviral Res 1989;12:205-12.
10. Manischewitz JF, Quinnan GV, Lane HC, Wittek AE. Syn- ergistic effect of ganciclovir and foscarnet on cytomegalovirus replication in vitro. Antimicrob Agents Chemother 1990;34: 373-5.
11. Butler KM, Husson RN, Balis FM, et al. Dideoxyinosine in children with symptomatic human immunodeficiency virus in- fection. N Engl J Med 1991;324:137-44.
12. Millar AB, Miller RF, Patou G, Mindel A, Marsh R, Semple SJG. Treatment of cytomegalovirus retinitis with zidovudine and ganciclovir in patients with AIDS: outcome and toxicity. Genitourin Med 1990;66:156-8.
13. Hochster H, Dieterich D, Bozzette S, et al. Toxicity of combined ganciclovir and zidovudine for cytomegalovirus disease associated with AIDS. Ann Intern Med 1990;113: 111-7.
14. Drew WL. Cytomegalovirus infections in patients with AIDS. J Infect Dis 1988;158:449-56.
15. Gross JG, Bozzette SA, Mathews WC, et al. Longitudinal study of cytomegalovirus retinitis in acquired immune defi- ciency syndrome. Ophthalmology 1990;97:681-6.
16. Erice A, Chou S, Biron KK, Stanat S, Balfour HH Jr, Jordan MC. Progressive disease due to ganciclovir-resistant eytome- galovirus in immunocompromised patients. N Engl J Med 1989;320:289-93.
17. Jacobson MA, O'Donnell J J, Rousell R, Dionian B, Mills J. Failure of adjunctive cytomegalovirus intravenous immune globulin to improve efficacy of ganciclovir in patients with ac- quired immunodeficiency syndrome and cytomegalovirus re- tinitis: a phase 1 study. Antimicrob Agents Chemother 1990; 34:176-8.
Acute bronchodilator response to a combination of beta-adrenergic and anticholinergic agents in patients with cystic fibrosis
Ignacio Sanchez, MD, Jessica Holbrow, RRT, and Victor Chernick, MD
From the Department of Pediatrics, University of Manitoba, Section of Pediatric Respirology, Children's Hospital, Winnipeg, Manitoba, Canada
Patients with cystic fibrosis had a better acute bronchodilator response to albuterol and ipratropium bromide than to either drug alone. Further studies of long-term eff icacy and safety seem justified. (J PEDIATR 1992;420"486-8)
Supported by the Children's Hospital of Winnipeg, Research Foundation, Inc. Dr. Sanchez is a Fellow of the Manitoba Lung Association. Submitted for publication Aug. 29, 1991; accepted Oct. 21, 1991. Reprint requests: Victor Chernick, MD, Department of Pediatrics, University of Manitoba, P216-770 Bannatyne Ave., Winnipeg, Manitoba R3E 0W3, Canada. 9/26/34492
The use of/3-adrenergic bronchodilator therapy in patients
with cystic fibrosis is controversial because various studies
have shown that these medications may have different
effects on expiratory airflow, ranging from a positive
response to no response or even an adverse response} -7 In
addition, studies of inhaled anticholinergic bronchodilators
in patients with CF are limited and even more controver-
Volume 120 Clinical and laboratory observations 4 8 7 Number 3
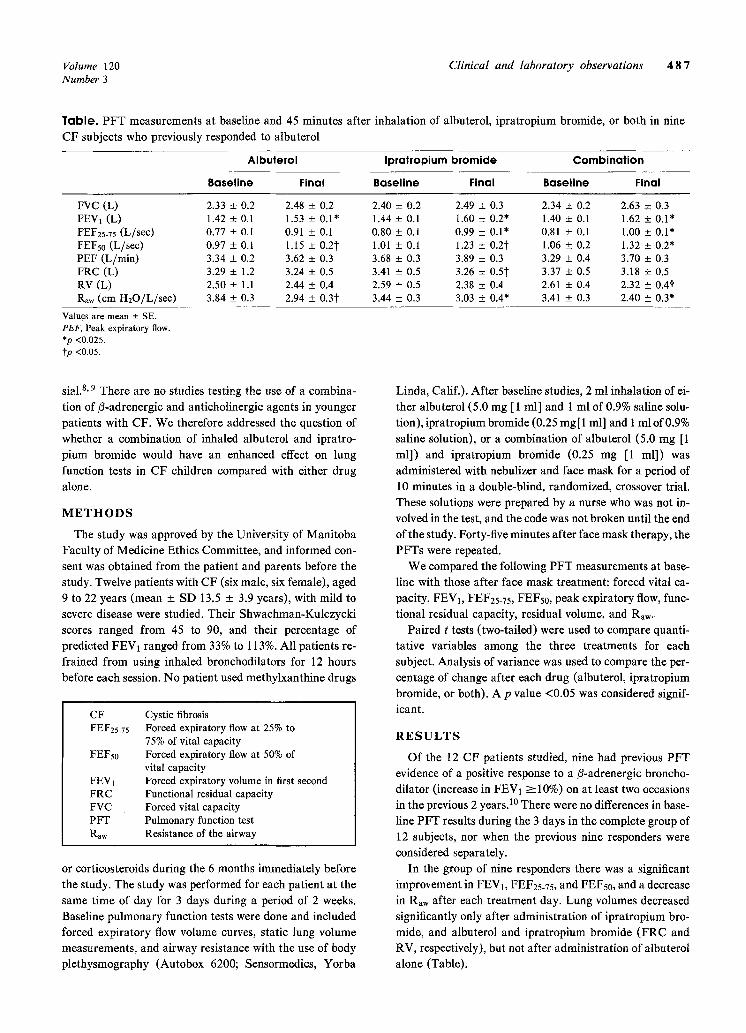
Table. P F T measurements at baseline and 45 minutes after inhalation of albuterol, ipratropium bromide, or both in nine
CF subjects who previously responded to albuterol
Albuterol Ipratropium bromide Combination
Baseline Final Baseline Final Baseline Final
FVC (L) 2.33 _+ 0.2 2.48 + 0.2 2.40 + 0.2 2.49 + 0.3 2.34 + 0.2 2.63 + 0.3 FEV1 (L) 1.42 +_ 0.l 1.53 _+ 0.1" 1.44 _+ 0.1 1.60 + 0.2* 1.40 _+ 0.1 1.62 +_ 0.1" FEF25.75 (L/see) 0.77 _+ 0.1 0.91 ___ 0.1 0.80 + 0.1 0.99 __+ 0.1" 0.81 + 0.1 1.00 + 0.1" FEFs0 (L/see) 0.97 + 0.1 1.15 + 0.2t 1.01 + 0.1 1.23 _ 0.2t 1.06 _+ 0.2 1.32 + 0.2* PEF (L/min) 3.34 + 0.2 3.62 +_ 0.3 3.68 + 0.3 3.89 _+ 0.3 3.29 + 0.4 3.70 + 0.3 FRC (L) 3.29 _ 1.2 3.24 + 0.5 3.41 + 0.5 3.26 + 0.5~ 3.37 + 0.5 3.18 + 0.5 RV (L) 2.50 + 1.1 2.44 _+ 0.4 2.59 +_ 0.5 2.38 _+ 0.4 2.61 + 0.4 2.32 +__ 0.4"~ Ra,~ (cm H20/L/sec) 3.84 _+ 0.3 2.94 + 0.3t 3.44 _ 0.3 3.03 + 0.4* 3.41 + 0.3 2.40 +__ 0.3*
Values are mean _+ SE. PEF, Peak expiratory flow. *p <0.025. ~p <0.05.
sial.S, 9 There are no studies testing the use of a combina-
tion of/3-adrenergic and anticholinergic agents in younger
patients with CF. We therefore addressed the question of
whether a combination of inhaled albuterol and ipratro-
pium bromide would have an enhanced effect on lung
function tests in CF children compared with either drug
alone.
M E T H O D S
The study was approved by the University of Manitoba
Faculty of Medicine Ethics Committee, and informed con-
sent was obtained from the patient and parents before the
study. Twelve patients with CF (six male, six female), aged
9 to 22 years (mean +_ SD 13.5 + 3.9 years), with mild to
severe disease were studied. Their Shwachman-Kulczycki
scores ranged from 45 to 90, and their percentage of
predicted FEV1 ranged from 33% to 113%. All patients re-
frained from using inhaled bronchodilators for 12 hours
before each session. No patient used methylxanthine drugs
CF FEF25-75
FEFso
FEV1 FRC FVC PFT
Raw
Cystic fibrosis Forced expiratory flow at 25% to 75% of vital capacity Forced expiratory flow at 50% of vital capacity Forced expiratory volume in first second Functional residual capacity Forced vital capacity Pulmonary function test Resistance of the airway
or corticosteroids during the 6 months immediately before
the study. The study was performed for each patient at the
same t ime of day for 3 days during a period of 2 weeks.
Baseline pulmonary function tests were done and included
forced expiratory flow volume curves, static lung volume
measurements, and airway resistance with the use of body
plethysmography (Autobox 6200; Sensormedics, Yorba
Linda, Calif.). Af ter baseline studies, 2 ml inhalation of ei-
ther albuterol (5.0 mg [ 1 ml] and 1 ml of 0.9% saline solu-
tion), ipratropium bromide (0.25 rag[ 1 ml] and 1 ml of 0.9%
saline solution), or a combination of albuterol (5.0 mg [1
ml]) and ipratropium bromide (0.25 mg [1 ml]) was
administered with nebulizer and face mask for a period of
10 minutes in a double-blind, randomized, crossover trial.
These solutions were prepared by a nurse who was not in-
volved in the test, and the code was not broken until the end
of the study. Forty-five minutes after face mask therapy, the
PFTs were repeated.
We compared the following PFT measurements at base-
line with those after face mask treatment: forced vital ca-
pacity, FEVI, FEF25.75, FEFs0, peak expiratory flow, func-
tional residual capacity, residual volume, and Raw.
Paired t tests (two-tailed) were used to compare quanti-
tative variables among the three treatments for each
subject. Analysis of variance was used to compare the per-
centage of change after each drug (atbuterol, ipratropium
bromide, or both). A p value <0.05 was considered signif-
icant.
R E S U L T S
O f the 12 CF patients studied, nine had previous PFT
evidence of a positive response to a ~-adrenergic broncho-
dilator (increase in FEV1 >--10%) on at least two occasions
in the previous 2 years. 1~ There were no differences in base-
line PFT results during the 3 days in the complete group of
12 subjects, nor when the previous nine responders were
considered separately.
In the group of nine responders there was a significant
improvement in FEVb FEF25.75, and FEFs0, and a decrease
in Raw after each treatment day. Lung volumes decreased
significantly only after administration of ipratropium bro-
mide, and albuterol and ipratropium bromide ( F R C and
RV, respectively), but not after administration of aibuterol
alone (Table).
4 8 8 Clinical and laboratory observations The Journal of Pediatrics March 1992
Although after t reatment with either drug alone the P F T
values also showed significant improvement, the greatest
percentage of increase in FEV1 (17%), FEF25-75 (26%), and
FEFs0 (25%), and the greatest percentage of decrease in
F R C ( -7%) , RV ( -9%) , and Raw ( -32%), occurred after
a combination of albuterol and ipratropium bromide was
administered. The combination significantly improved
FEVI and decreased RV and Raw in comparison with either
drug alone (p <0.025). There was no significant correlation
between age, baseline PFT measurements, or Shwachman-
Kulczycki scores and the response to/3-adrenergic or anti-
cholinergic bronchodilators.
In the three patients who did not previously respond to
albuterol, there was no significant difference in PFTs after
any of the three inhalations. Thus, in 75% of patients stud-
ied, there was a significantly better response to a combina-
tion of drugs than to either drug alone.
D I S C U S S I O N
The question of whether bronehodilators are efficacious
in CF has been discussed by several authors. 46 Recently
Pattishall 7 showed in a longitudinal and cross-sectional
study that 40% of patients had a positive response to inhaled
adrenergic agents; however, there was a lack of consistent
response. In our series, 9 of 12 patients did have a positive
response to albuterol (salbutamol) at least once in the 2
years before the study, and those patients responded to both
drugs alone and in combination during the trial. On the
other hand, 3 of 12 patients had not previously responded
and also did not have a significant change during the trial.
Several previous studies have assessed the change in FEV1
after/3-agonist and anticholinergic therapy in patients with
CF,9, 11 but only one study tested the effect of both drugs in
combination in adults with CF. 12 In that study there was a
12.5% improvement in FEV1 after metaproterenol treat-
ment and a 17.1% increase after ipratropium. 12 We found
on average a 7% increase in FEVI after albuterol treatment
and a 10% improvement after ipratropium. When these two
drugs were used in combination, Weintraub and Eschen-
bacher lz found a 16.6% increase in FEVb similar to our
finding.
Our patients were younger than those of Weintraub and
Eschenbacher. 12 It is possible that both the prevalence and
the extent of bronchial reactivity increases with age in CF.
In our patients the mean baseline FEV1 was about 60% of
the predicted value on the 3 protocol days, compared with
44% in the patients studied by Weintraub and Eschenbach-
er. 12 In our study the interval between baseline PFT mea-
surements and those after treatment was chosen to be 45
minutes to take into account the maximal ipratropium ef-
fect; in most previous studies the waiting time was only 30
minutes.9, 12 It is unclear whether the use of an inhaler so-
lution contributed to a response different from that obtained
with a metered dose inhaler, but this is another difference
between our findings and those of other studies. 1, 9, 12
Our study had two major limitations. The first is the small
sample size; a larger patient population should be studied.
Second, we have described only the acute response to bron-
chodilator therapy; further studies are needed to assess
long-term efficacy and safety.
We conclude that muscarinic pathways appear to be im-
portant in the pathogenesis of expiratory airflow obstruction
in some patients with CF and suggest that PFTs be done
after albuterol and ipratropium bromide are used by those
patients who respond significantly to albuterol, to evaluate
whether they would benefit from combined bronchodilator
therapy. Further studies are needed to evaluate the long-
term effects of such therapy.
We are grateful to Anne Rempel, RN, for recruiting the patients, and to Robert Tate for performing the statistical analyses.
R E F E R E N C E S
1. Tobin M J, Maguire O, Reen D, Tempany E, Fitzgerald MX. Atopy and bronchial reactivity in older patients with cystic fi- brosis. Thorax 1980;35:807-13.
2. Svenonius E, Arborelius M Jr, Kentto R, Kornifalt R, Lind- berg T. Lung function in cystic fibrosis. Respiration 1980; 40:226-32.
3. Eggleston PA, Rosenstein B J, Stackhouse CM, Mellits D, Baumgardner RA. A controlled trial of long-term broncho- dilator therapy in cystic fibrosis. Chest 1991;99:1088-92.
4. Landau LI, Phelan PD. The variable effect of a bronchodilat- ing agent on pulmonary function in cystic fibrosis. J PEDIATR 1973;82:863-8.
5. Shapiro GG, Bamman J, Kanarek P, Bierman CW. The par- adoxical effect of adrenergic and methylxanthine drugs in cys- tic fibrosis. Pediatrics 1976;58:740-3.
6. Zach MS, Oberwaldner B, Forche G, Polgar G. Bronchodila- tors increase airway instability in cystic fibrosis. Am Rev Respir Dis 1985;131:537-43.
7. Pattishall EN. Longitudinal response of pulmonary fiinction to bronchodilators in cystic fibrosis. Pediatr Pulmonol 1990; 9:80-5.
8. Larsen GL, Barron R J, Cotton EK, Brooks JG. A comparative study of inhaled atropine sulfate and isoproterenol hydro- chloride in cystic fibrosis. Am Rev Respir Dis 1979;119: 399-407.
9. Kattan M, Mansell A, Levison H, Corey M, Krastins IRB. Response to aerosol salbutamol, SCH 1000 and placebo in cystic fibrosis. Thorax 1980;35:531-5.
10. Bibi H, Montgomery M, Pasterkamp H, Chernick V. Rela- tionship between response to inhaled salbutamol and meth- acholine bronchial provocation in children with suspected asthma. Pediatr Pulmonol 1991; 10:244-8.
11. Wiebicke W, Poynter A, Montgomery M, Pagtakhan R. The effect of ipratropium bromide on lung function in patients with cystic fibrosis. Pneumologie 1990;44:277-8. Weintraub S J, Eschenbacher WL. The inhaled bronchodila- tors ipratropium bromide and metaproterenol in adults with CF. Chest 1989;95:861-4.
12.