Embed Size (px)
DESCRIPTION
pathophysiology and management of acute coronary syndrome and heart failure based on malaysia guideline.
Citation preview

Syuraih Abdullah b. Abu Kassim 45244 Muhd. Haziq Qaiyum b. Roslan 45226Bahiyah bt. Abdul Jabar 45245Wan Nur Umirah bt. Wan Rusmi 45247Muhd. Nu’man bin Jeman 45233Rachel Wong Jing Ting 33462
IDA 6 SEMINARACUTE CORONARY SYNDROME & HEART FAILURE
Epidemiology

Acute Coronary Syndrome
• Acute coronary syndrome (ACS) is the leading cause of death not only in Malaysia but also globally.• Estimated incidence =141/100,000 population per year• 10% mortality rate for patients who were admitted to hospital with
STEMI in 2006-2008. - The National Cardiovascular Disease (NCVD) ACS Registry -
• Thrombolysis (for STEMI only) reduced in-hospital and 30-day mortality by nearly 50%.

Heart Failure• Estimated incidence = 3-20 per 1000 population.• Coronary Artery Disease & Hypertension accounting for almost 70%
of all cases.• The prognosis remains poor. • One year mortality rate = 5% to 52% depending on the severity and
the presence of co-morbidity. • In a study, about 40% of individuals with HF died within a year of
initial diagnosis. • About 25% of patients are readmitted within 30 days for acute
decompensation. (major health and economic burden)

Case Study
Patient’s profile• Name : Mr. C• Age : 37 years old• Occupation : Army ranger• Home address : Kuching• Social : Active smoker
History of Presenting Illness• Previously well. Had no history of being diagnosed with any kind of illnesses.
September 2014:- Had sudden onset of central chest discomfort while resting and smoking cigarette at the army mess.- The chest discomfort was described as dull in nature and radiates to the left arm and his jaw.- Associated with sweating.- Lasted for about 20 minutes.- Went to hospital Ipoh by himself. - Given treatment. Chest pain resolved.- ECG was inconclusive. Some blood tests done.- Was told that troponin was “positive”.- Admitted for 6 days . Refused coronary angiogram even though advised.- Reason being he was still able to exercise and run as usual after the event of chest discomfort.
13th December 2014:- Was on a mission at the Thai-Malaysian Border in the jungle.- Had finished his medications for the past 2 weeks but did not replenish his supply from the hospital.- Woke up suddenly at 8am with sudden onset of chest pain, similar with the previous one but more severe.- Associated with shortness of breath, diaphoresis and nausea.- Took some sublingual GTN but only improved slightly.- Evacuated from the area via a helicopter. Subsequently admitted to Hospital Sultanah Bahiyah in Alor Setar.- Not given thrombolysis because it was a late presentation.- Coronary angiogram and PCI was done with a DES to the LAD. (15/12/2015)- Discharged well after admission for 1 week.

Late December, 2014 (*just around 2 weeks after PCI done):- Started to have some mild shortness of breath on exertion but chose to ignore the symptom.
Between late Feb and March, 2015:- Stationed at Sematan, 100km from Kuching.- Started to have pedal edema and reduced effort tolerance.
30th March – 6th April, 2015 :- Bilateral pedal edema up to thigh, mild orthopnea and NYHA III.- Discharged after given diuretics and had good urine output.- Started on warfarin after ECHO noted LV thrombus.
9th April – 29th April, 2015:- Worsening of pedal edema.- Appeared jaundice.- Claimed as compliant to medications but not to fluid restrictions.- Had no fever, no sputum and no dysuria to suggest any infection.- Had no malaena to suggest any upper GI bleeding.- Had reduced urine output but had no uraemic symptoms.
Family History:- Mother has diabetes mellitus, hypertension and dyslipidemia.- All of his mother’s male siblings have ischaemic heart disease.- One had CABG. 2 had sudden death at an early age.
Social History:- An army ranger.- Smokes 2 packs per day for the past 19 years. Stopped in December, 2014.- Married. Has 3 children. 11 year-old daughter, 7 year-old and 1 year-old son.

Medications :Rate control:
Carvedilol - 3.125mg bd Ivabradine - 5mg bd
Digoxin - 0.125mg od
Diuretics:Frusemide - 40mg bd
Spironolactone - 12.5mg bd
Anti-coagulant:Warfarin - 2mg od
Anti-dyslipidaemic:Atorvastatin - 40mg
noct
Anti-platelet:Aspirin - 75mg bd Clopidogrel - 75mg
od
Anti-hypertensive:Perindopril - 2mg od
Proton-pump inhibitor: Pantoprazole – 40mg bd
Clinical Examination:- Raised JVP, pedal edema up to the knees.- Displace apex beat. Soft systolic murmur at apical area .
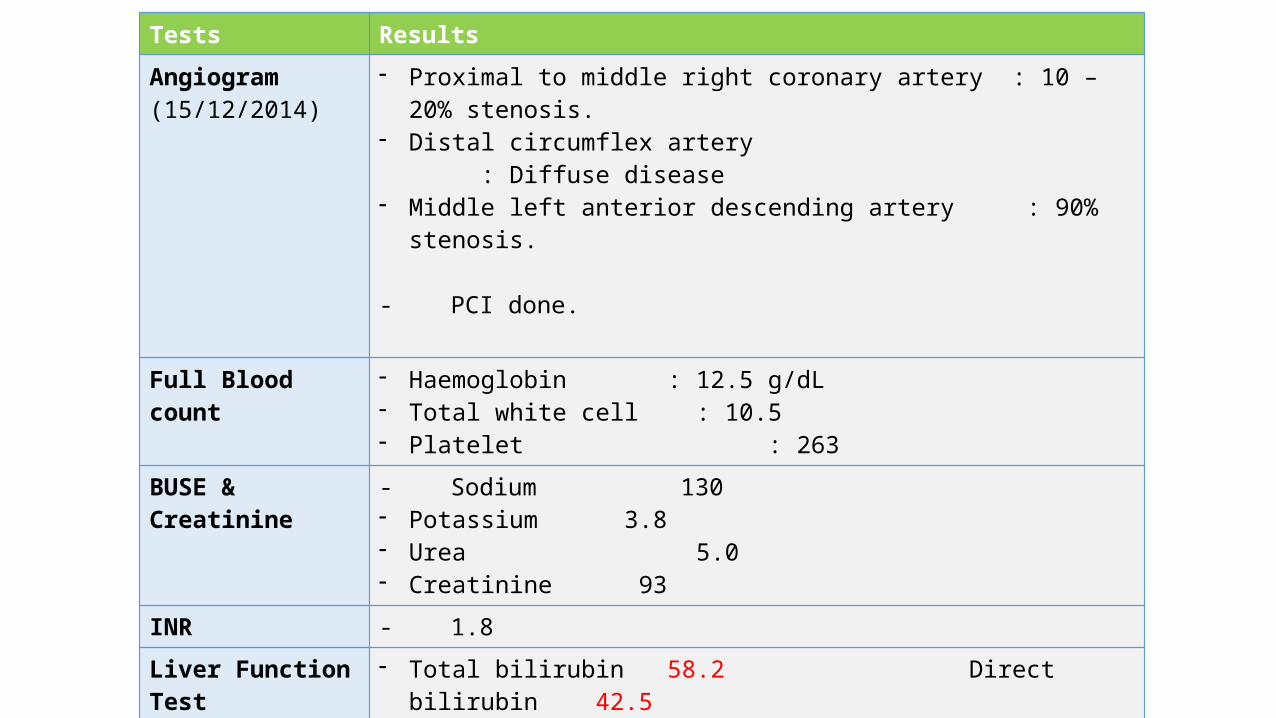
Tests ResultsAngiogram (15/12/2014)
- Proximal to middle right coronary artery : 10 – 20% stenosis.- Distal circumflex artery : Diffuse disease- Middle left anterior descending artery : 90% stenosis.
- PCI done.
Full Blood count - Haemoglobin : 12.5 g/dL- Total white cell : 10.5- Platelet : 263
BUSE & Creatinine - Sodium 130- Potassium 3.8- Urea 5.0- Creatinine 93
INR - 1.8Liver Function Test - Total bilirubin 58.2 Direct bilirubin 42.5
- AST 243- ALT 200- Protein 74- Albumin 22- Globulin 52- ALP 246

Sept.
Mid Dec.
Late Dec. Feb-March-April
Mid-Late, April
First heart attack
Onset of HF
symptomsWorsening of HF symptoms
Right heart failure + renal sx
Secondheart attack
20152014
Medication only Stenting
done
HF medications ???
???
Summary• A 37-year-old male, army, active smoker, with history of being
diagnosed with ischaemic heart disease, on medications and stenting done 5 months ago, complicated with heart failure and on medications, currently presenting with worsening of pedal edema, and jaundice. Physical examination also revealed pedal edema up till knee level and jaundice plus raised JVP, displaced apex beat and soft systolic murmur at the apical area.

What are the issues?• Why did the patient develop heart failure despite PCI was done?• Why he needs warfarin?• What are the precipitating and perpetuating factors that pose high
risks in this patient?• What are the next options that this patient has for treatment?
Acute Coronary Syndrome

• RCA and its branches supplies the RA, RV & inferoposterior aspects of the LV.
• RCA supplies the SA node in ≈ 60% of individuals and the AV node in ≈ 90% of individuals.• Sinus bradycardia and AV
nodal block.
Occlusion:- RCA Right-sided and
inferior infarct.- LAD, CX Left-sided
infarct

ACS
Myocardial infarction
NSTEMI
STEMIUnstable angina

Etiology of ACS
Atherosclerotic plaque ***
Coronary artery
dissection
Coronary emboli
Coronary arteritis
Coronary spasm

Excess LDL accumulates in intima
Macrophage ingest the cholesterol
Macrophage becomes lipid laden foam cells
Foam cells die and release fatty content
Lipid pool formation
Smooth muscle cells (SMC) moves to intima from media (chemotatic cytokines from foam cells)
SMC proliferates, produces collagen and elastin, thus form fibrous cap

Stimulated by LDL and atherogenic cytokines, SMC produces matrix metalloproteinases (MMP)
MMP degrades the fibrous cap
Lower SMC:lipid ratio, increasing lipids and cellular debris in lipid core, higher plaque vulnerability
Plaque rupture
Activation of platelet aggregation, coagulation pathway and vasoconstriction
Partial or total occlusion of coronal artery
Ischemia of cardiac muscles leads to myonecrosis

Risk factorsNON MODIFIABLE MODIFIABLEAge (55 years old) Smoking
Gender (Male > Female) HypertensionFamily history of coronary heart
diseaseDiabetes mellitus
Obesity Dyslipidemia

Symptoms Signs
Chest pain Diaphoresis Nausea & vomiting Hypotension
SweatingShortness of breath
PalpitationSyncope
Atypical chest pain
Symptoms and Signs

How to diagnose?
Investigations
ECG EchocardiogramCardiac Markers
Angiogram MRI

Electrocardiogram (ECG)UNSTABLE ANGINA MYOCARDIAL INFARCTION
NSTEMI STEMI
ST depression
T wave inversion
ST depression
T wave inversion
Loss of R wave
Absent Q waves
ST elevation
Diminution of R wave
Q wave
T wave inversion

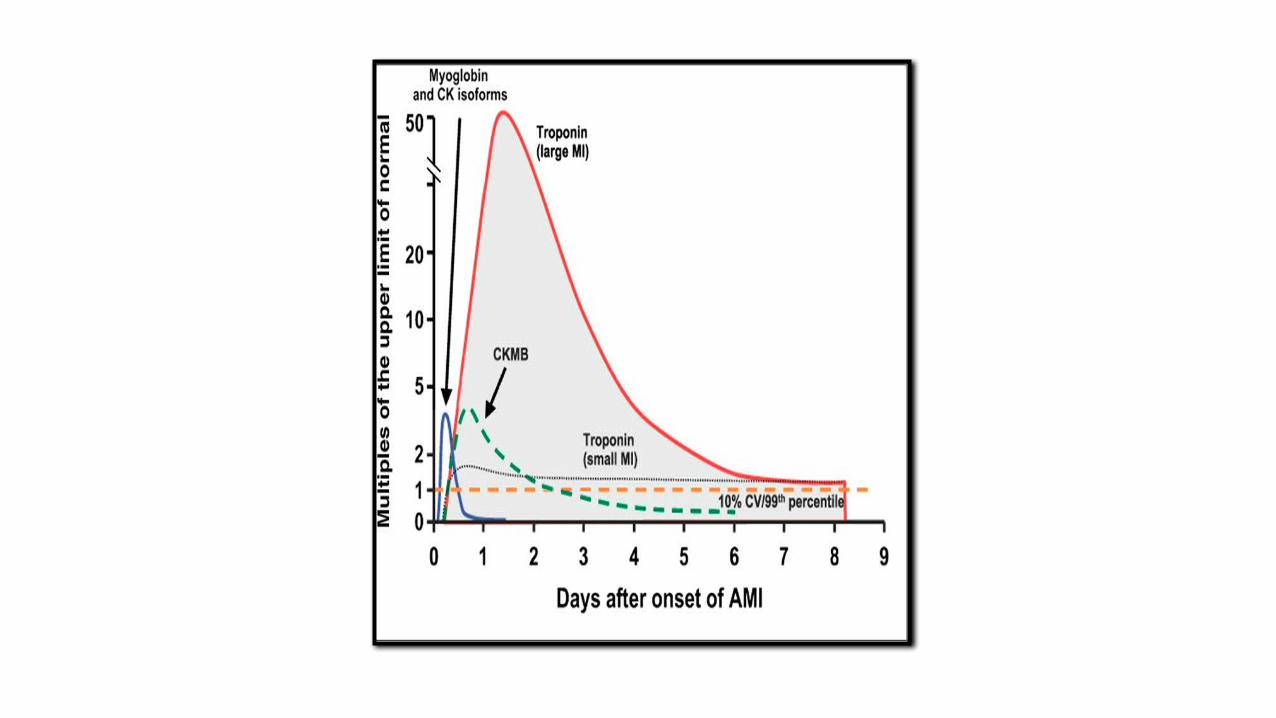
Cardiac markersCARDIAC ENZYMES
Rise Peak Falls
Creatinine Kinase (CKMB)
4-6 hours 12 hours 48-72 hours
Troponin T & I 3-4 hours 18-36 hours After 2 weeks


Echocardiography: Assess ventricular function & complication• Findings: Left ventricle thrombus
Angiogram: Blockage of the vessels
• Findings:• Proximal to middle right coronary artery : 10 to 20% stenosis.• Distal circumflex artery : Diffuse disease• Middle left anterior descending artery : 90% stenosis.

Cardiac MRI
• Define cardiac anatomy• Quantify right & left ventricular function• Assess myocardial perfusion• Quantify blood flow• Assess myocardial scar & viability

EARLY HOSPITAL CARE
Arrived at hospital
Test for cardiac biomarkers
ECG
Medications:-B blocker-Nitroglycerin-Morphine-Aspirin

Outline Treatment of Acute Coronary Syndromes
ST-Elevation(STEMI)
Emergent PCI availablewithin 90 min?
FibrinolyticTherapy(e.g., tPA)
Non-ST-Elevation(UA and NSTEMI)
Risk Assessment(e.g., TIMI Score)
Primary PCI ConservativeStrategy(Proceed to cardiac cathonly if recurrent anginaor predischargestress test is markedlypositive)
InvasiveStrategy(Cardiac cathleading toPCI or CABG)
No Yes Low High

Coronary Artery Bypass Graft Surgery (CABG)
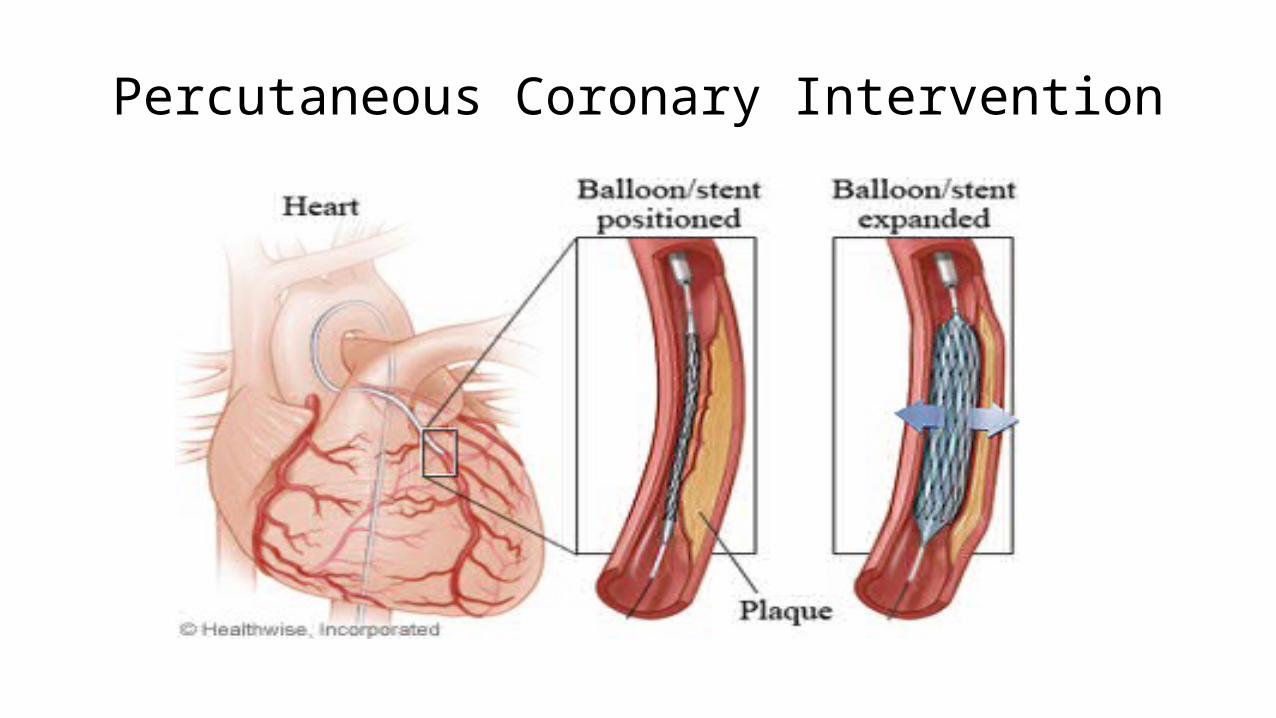
Percutaneous Coronary Intervention



INDICATIONS OF PCI:-Have frequent or severe angina that is not responding to medicine and lifestyle changes.
-Have evidence of severely reduced blood flow (ischemia) to an area of heart muscle caused by one or more narrowed coronary arteries.
-Have a narrowed or blocked artery that is likely to be treated successfully with angioplasty.
-Are in good enough health to have the procedure.

Back to our case:• Fibrinolytic therapy: was not given due to late presentation
• PCI and stenting: done after 2 days from the onset of symptoms
DELAY IN TREATMENT!
COMPLICATION OF ACS
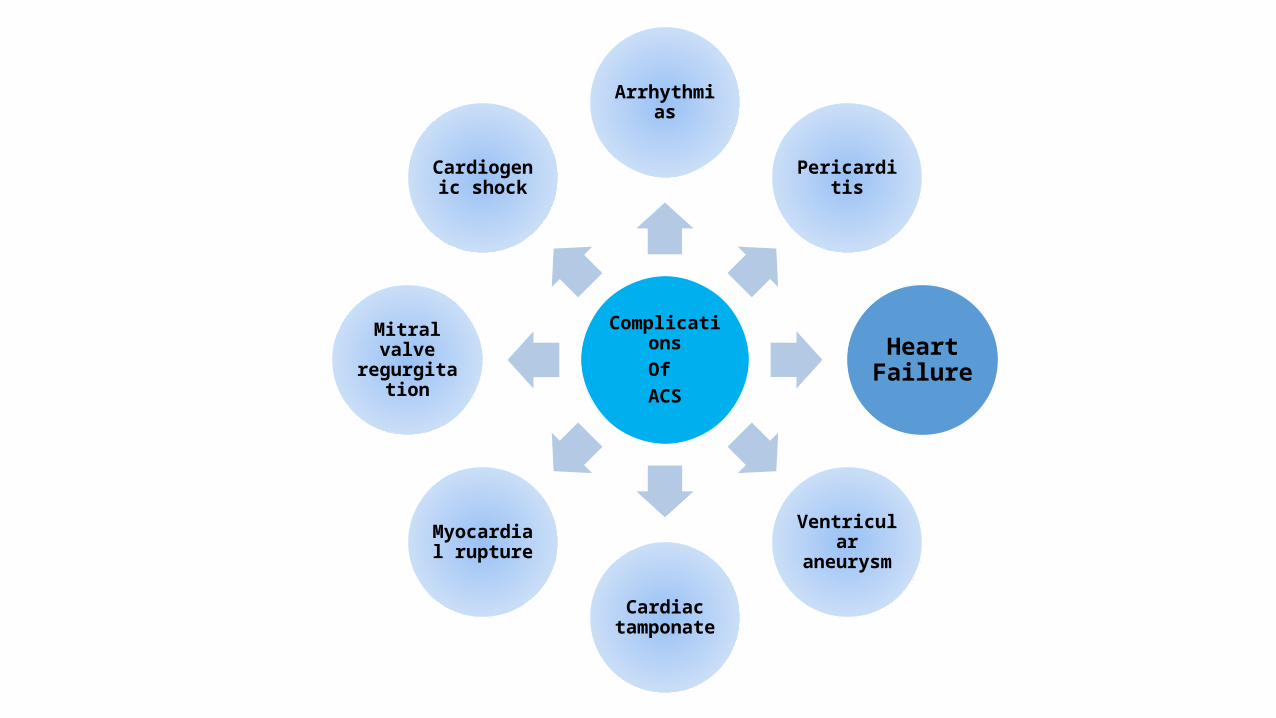
ComplicationsOf ACS
Arrhythmias
Pericarditis
Heart Failure
Ventricular aneurysm
Cardiac tamponate
Myocardial rupture
Mitral valve regurgitation
Cardiogenic shock

Heart FailureHF is an abnormality of cardiac structure or function
leading to an impairment of ventricular filling or ejection of blood. It is a clinical syndrome in which patients have
typical symptoms and signs.
Management of Heart Failure 3rdEd CPG 2014


Classifications
Right, Left, biventricular
Systolic, Diastolic
High Output Failure
Acute, ChronicPractical purpose
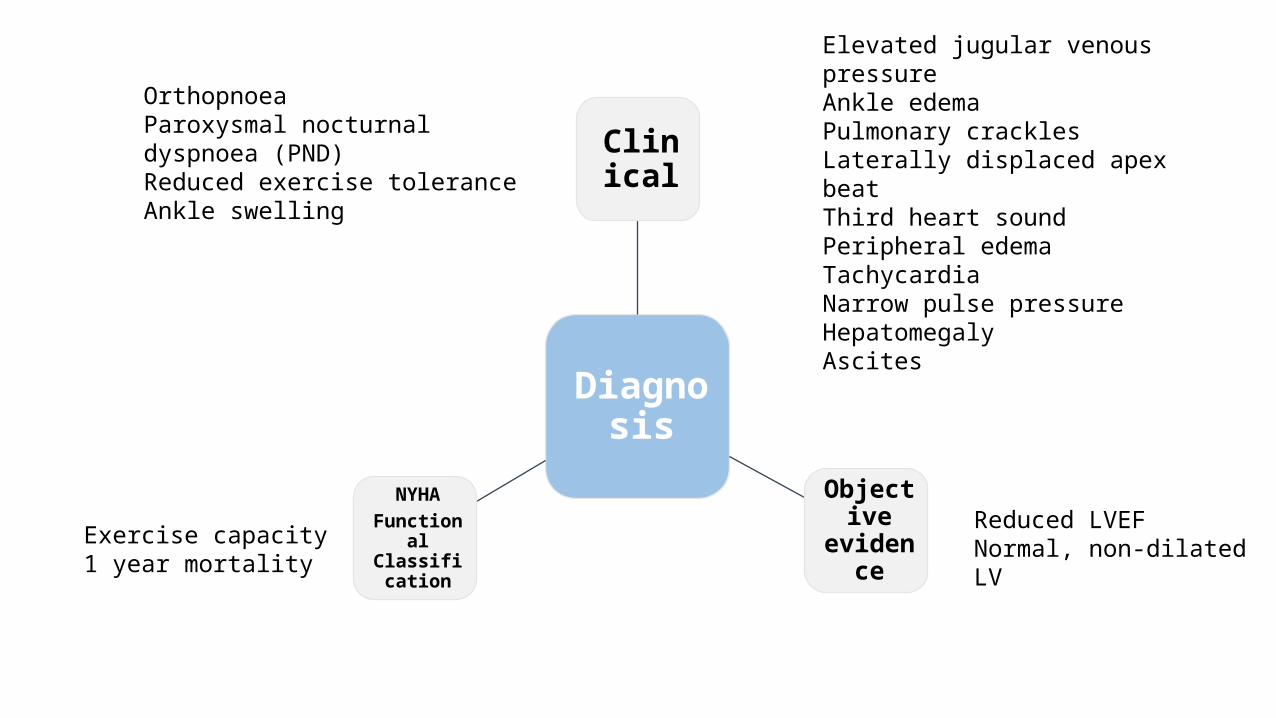
Diagnosis
Clinical
Objective
evidence
NYHAFunctional
Classification
OrthopnoeaParoxysmal nocturnal dyspnoea (PND)Reduced exercise tolerance Ankle swelling
Elevated jugular venous pressure Ankle edema Pulmonary crackles Laterally displaced apex beatThird heart soundPeripheral edemaTachycardia Narrow pulse pressureHepatomegalyAscites
Exercise capacity1 year mortality
Reduced LVEFNormal, non-dilated LV

The New York Heart Association Functional Classification
Class 1 Year mortality
CLASS I No limitation. Ordinary physical activity does not cause undue fatique, dyspnoea or palpitation.
5 - 10%
CLASS II Slight limitation of physical activity. Such patients are comfortable at rest. Ordinary physical activity results in fatique, palpitation, dyspnoea or angina.
10 - 15%
CLASS III Marked limitation of physical activity. Although patients are comfortable at rest, less than ordinary activity will lead to symptoms.
15 - 20%
CLASS IV Inability to carry on any physical activity without discomfort. Symptoms of congestive failure is present at rest. With any physical activity, increased discomfort is experienced.
20 - 50%
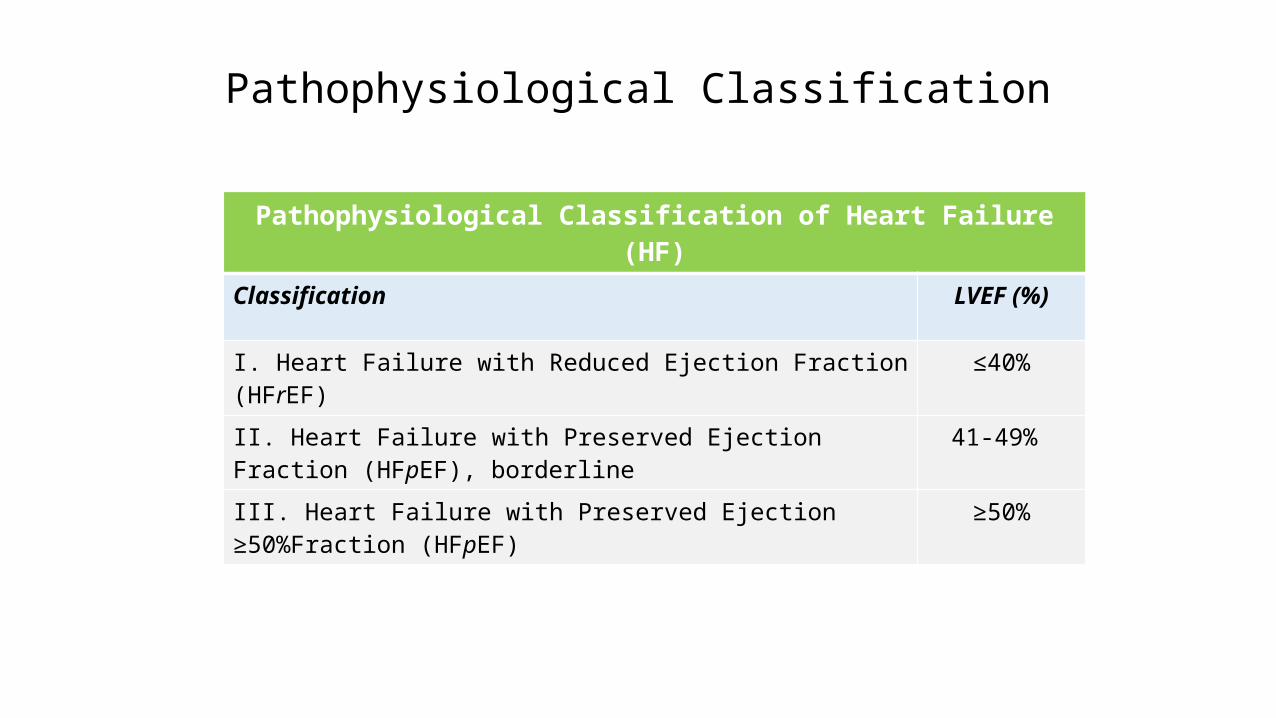
Pathophysiological Classification
Pathophysiological Classification of Heart Failure (HF)
Classification LVEF (%)
I. Heart Failure with Reduced Ejection Fraction (HFrEF) ≤40%
II. Heart Failure with Preserved Ejection Fraction (HFpEF), borderline 41-49%
III. Heart Failure with Preserved Ejection ≥50%Fraction (HFpEF) ≥50%

Factors Contributing to Decompensation in a Patient with stable HF• Non compliance to medications• Dietary indiscretion especially salt and fluid intake• Inappropriate medications e.g. NSAIDS and COX-2 inhibitors• Alcohol consumption
Patient factors
• Superimposed myocardial ischaemia or infarction (often asymptomatic)• Uncontrolled hypertension• Arrhythmias• Pulmonary embolism• Secondary mitral or tricuspid regurgitation
Cardiac causes
• Superimposed infections• Anemia• Thyroid disease• Electrolyte disturbances• Worsening renal disease
Systemic condition
s

53
Investigations for Heart Failure
Investigations
Confirm diagnosis
Underlying causes
Assess severity

55

1) Electrocardiography (ECG)
• heart rate • heart rhythm • QRS morphology • QRS duration
• QRS voltage • evidence of ischaemia
• LV hypertrophy• arrhythmias

57
2) Chest Radiograph
ABCDE•Alveolar oedema (bat’s wings)•kerley B lines (interstitial oedema)•Cardiomegaly•Dilated prominent upper lobe vesselsEffusion (pleural)

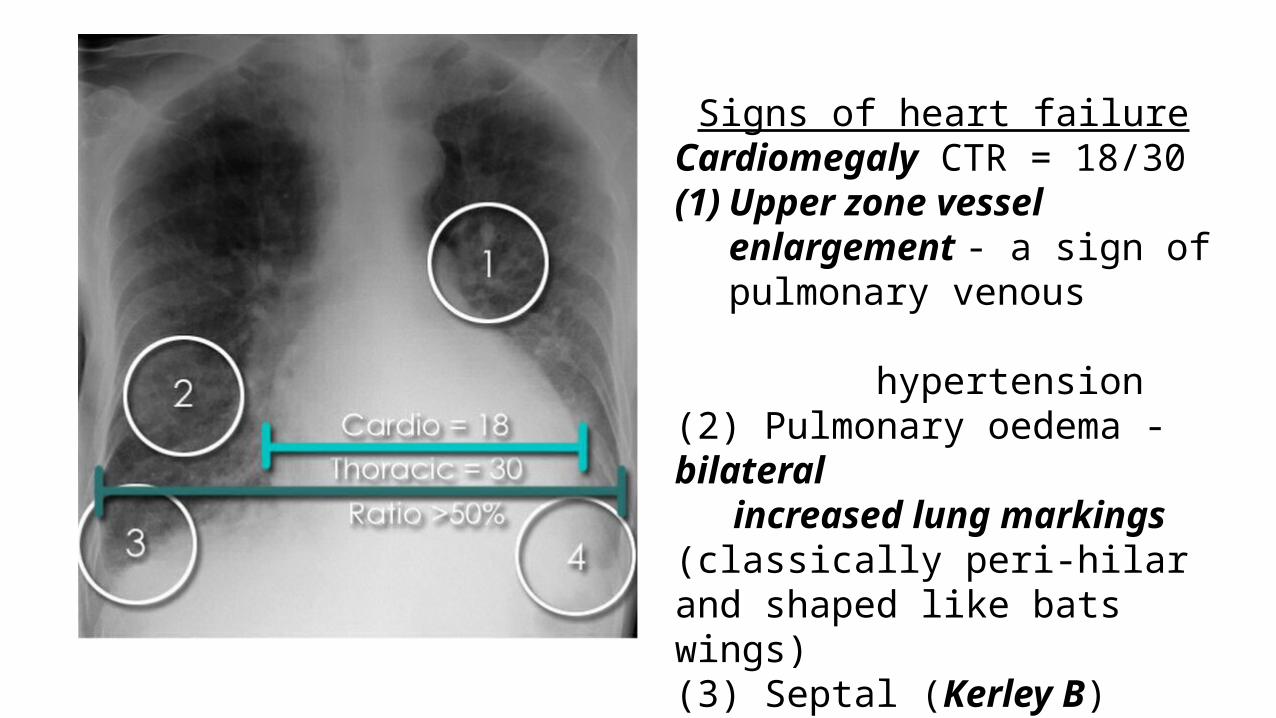
Signs of heart failureCardiomegaly CTR = 18/30(1) Upper zone vessel enlargement
- a sign of pulmonary venous
hypertension(2) Pulmonary oedema - bilateral increased lung markings (classically peri-hilar and shaped like bats wings)(3) Septal (Kerley B) lines(4) Pleural effusions

Septal lines (Kerley B lines)• Costophrenic angle• Horizontal lines reaching the
lung edge

61
3) Echocardiography• To identify structural abnormalities and assess systolic and diastolic function

62
4) B type natriuretic peptide (BNP) assay and N terminal pro BNP (NT- pro BNP)
• Hormones secreted by ventricles in response to wall stress. • Emergency setting, as a “rule out” test - acute heart failure• Levels increase with age, reduced in obesity. • Level correlate with severity of heart failure

Blood tests• Full blood count: anemia, infection• Renal profile: deteriorating renal function• Liver function test: elevated liver enzymes• Thyroid function test: thyrotoxicosis• D-dimer: risk for thrombosis• Cardiac markers: myocardial infarction• Arterial blood gas: hypoxia, pulmonary diseases
Test for myocardial ischaemia and/ or viability• Cardiac MRI: Assess myocardial perfusion and viability, infiltrative cardiomyopathy, congenital, anatomy vessels,
gold standard for RV function • Stress Echocardiography: examine viability in impaired LV function• Myocardial perfusion scanning: SPECT (single photon emitting CT): detect inducible ischaemia and hibernating
myocardium• Exercise (stress) ECG
• Underlying CAD may be diagnosed• Prognostic aid-following myocardial infarction• Distinguish between CAD and pulmonary causes

Invasive• Coronary angiography- assess extent and severity of
stenoses, thrombus and calcification, PCI and CABG planning

Others • Urinalysis
• Proteinuria, Glycosuria• 24 hour Holter monitoring
• Detects arrhythmias• Lung function tests
• FVC and FEV1 reduced in HF• Reversibility testing may be useful to decide use of beta blocker

66
Management
67
Acute Decompensation of Chronic Heart Failure• Principles of management:• Rapid recognition of the condition• Stabilization of haemodynamics• Improvement in clinical symptoms and signs• Identification and treatment of the
• Underlying cause• Precipitating / aggravating factors
68
Initial managementSit patient upright
Maintain oxygenation• 5 to 6 liters/ minute• keep SaO2>95%• mechanical ventilation is indicated if hypercapnia co-exist or oxygenation is
inadequate• Non-invasive positive pressure ventilation (NIPPV) if patient alert & coorperative
• correct severe metabolic acidosis (pH<7.2) to prevent negative inotropic and pro-arrhythmic effects

69
Insert IV cannula:• Frusemide
• I.V frusemide 40 mg- 100 mg depend on the severity of the clinical condition (renal function)
• Nitrate• Morphine sulphate
• I.V Morphine 2.5- 5 mg• Reduces pulmonary venous congestion and sympathetic drive
Further treatment based on systolic pressure:SBP ≥ 100 mmHg SBP ≤ 100 mmHg
• Frusemide• Inotropes (dopamine, dobutamine)• Vasodilators
• Noradrenaline• Dopamine• Intubation and mechanical ventilation• Correct acidosis• Invasive haemodynamic monitoring• Intra-aortic balloon counterpulsation
(IABP)

70

71
Chronic Heart Failure Management
Non Pharmacological
Pharmacological
Device Therapy Surgery
Heart Transplantation

72
Non- Pharmacological
Low salt and low fat diet
Ideal Body Weight
Smoking and Alcohol Cessation
Exercise
73
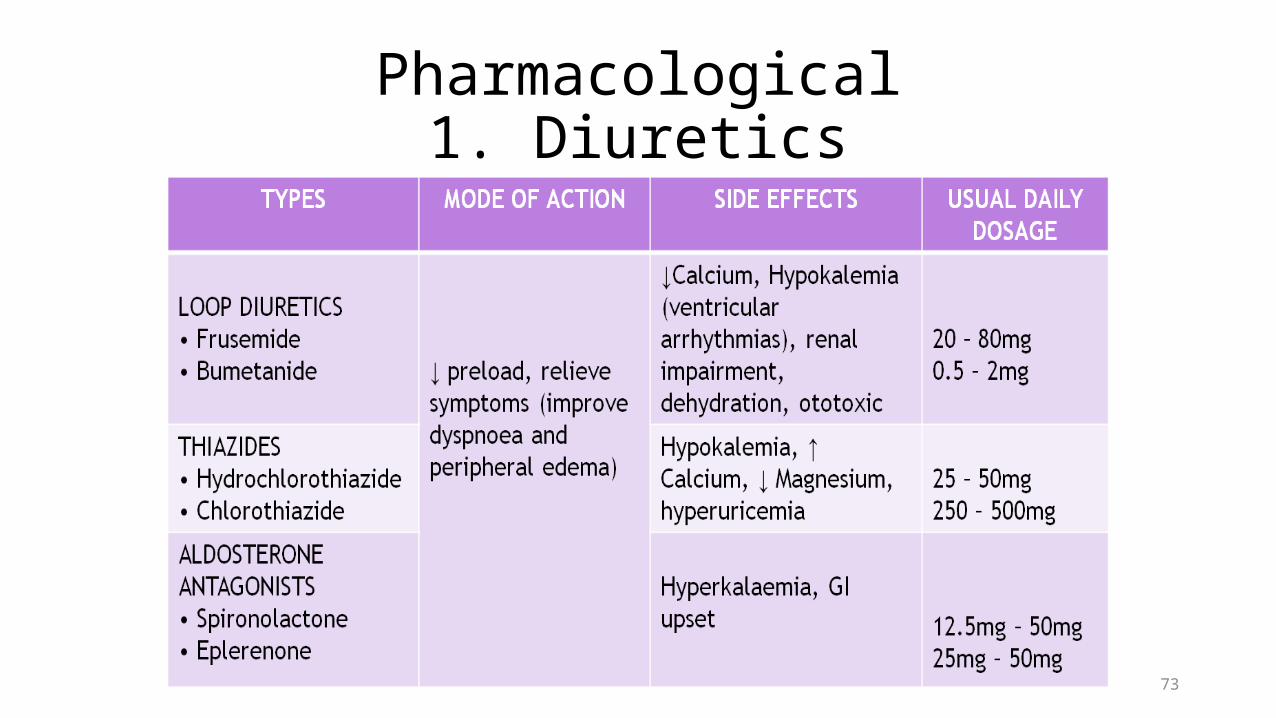
Pharmacological1. Diuretics

74
2. Vasodilators

75
3. Inotropic agents

4. Anticoagulants Types: Warfarin / Heparin Indications: atrial fibrillation, intracardiac thrombus (except for
organized mural thrombus), past history of thromboembolic episode(s)
Side effects: ↑bleeding
5. Antiarrhythmic agents Type: Amiodarone Side effects: Photosensitivity, hepatitis, lung fibrosis

77
Device Therapy • Cardiac Resynchronisation Therapy (CRT)

78
• Implantable Cardioverter Defibrillator (ICD)
• Combined Biventricular Pacing with ICD Capabilities

79
Parachute

80

81
Surgery• Revascularisation Procedures• PCI• Coronary artery bypass surgery (CABG)
• Valve surgery• LV Reduction Surgery • Patients with a large discrete LV
aneurysm
• LV Assist Devices• For patients awaiting for heart
transplantation

82

83
Heart Transplantation• Treatment of refractory end stage HF but it is limited
by lack of donor organs





