Embed Size (px)
Citation preview

KERCKHOFF
KLINIK
Acute Coronary Syndrome
Update
Christian W. Hamm
Medical Clinic I
University Hospital Giessen
& Kerckhoff Heart and Thorax Center
Germany

KERCKHOFF KLINIKUNIVERSITÄTSKLINIKUM GIESSEN
Conflict of Interest – Disclosure
Christian W. Hamm
Affiliation/Financial Relationship Company
1. Honoraria for lectures Abbott, AstraZeneca ,Bayer, Berlin Chemie,
Boehringer Ingelheim, MSD, BMS,
BRAHMS, Daiichi Sankyo, Essex, GSK,
Medtronic, Lilly, SanofiAventis,
Correvio, Pfizer, Roche, The
Med. Comp., Boston Scientific, Gilead
2. Honoraria for advisory AstraZeneca, Bayer, BRAHMS, Median,
board activities Boehringer Ingelheim, Medtronic, SHS
3. Participation in AstraZeneca, MSD, Boston Scientific, GSK
clinical trials Takeda, Terumo, The Med. Comp., Gilead
4. Financial shares and options: no

Chest Pain
Acute Coronary Syndrome
persistent
ST-elevation
ST/T -
abnormalities
normal or
undetermined
ECG
STEMI NSTEMIUnstable
Angina
troponin
rise/fall
troponin
normal
Admission
Working
diagnosis
ECG
Bio-chemistry
Diagnosis
Hamm et al: European Heart Journal (2011) 32:2999–3054

www.escardio.org/guidelines European Heart Journal 2012 - doi:10.1093/eurheartj/ehs215
European Heart Journal
doi:10.1093/eurheartj/ehs215
ESC Guidelines for the management of acute myocardial
infarction in patients presenting with ST-segment
elevationThe Task Force on the management of ST-segment elevation acute myocardial
infarction of the European Society of Cardiology
Authors/Task Force Members: Ph. Gabriel Steg (Chairperson) (France)*, Stefan K. James (Chairperson) (Sweden)*, Dan Atar
(Norway), Luigi P. Badano (Italy), Carina Blomstrom Lundqvist (Sweden), Michael A. Borger (Germany), Carlo Di Mario (United
Kingdom), Kenneth Dickstein (Norway), Gregory Ducrocq (France), Francisco Fernandez-Aviles (Spain), Anthony H. Gershlick (United
Kingdom), Pantaleo Giannuzzi (Italy), Sigrun Halvorsen (Norway), Kurt Huber (Austria), Peter Juni (Switzerland), Adnan Kastrati
(Germany), Juhani Knuuti (Finland), Mattie J. Lenzen (Netherlands), Kenneth W. Mahaffey (USA), Marco Valgimigli (Italy), Arnoud van't
Hof (Netherlands), Petr Widimsky (Czech Republic), Doron Zahger (Israel)
ESC Committee for Practice Guidelines (CPG): Jeroen J. Bax (Chairman) (Netherlands), Helmut Baumgartner (Germany), Claudio
Ceconi (Italy), Veronica Dean (France), Christi Deaton (UK), Robert Fagard (Belgium), Christian Funck-Brentano (France), David Hasdai
(Israel), Arno Hoes (Netherlands), Paulus Kirchhof (Germany/UK), Juhani Knuuti (Finland), Philippe Kolh (Belgium), Theresa McDonagh
(UK), Cyril Moulin (France), Bogdan A. Popescu (Romania), Željko Reiner (Croatia), Udo Sechtem (Germany), Per Anton Sirnes
(Norway), Michal Tendera (Poland), Adam Torbicki (Poland), Alec Vahanian (France), Stephan Windecker (Switzerland)
Document Reviewers: David Hasdai (CPG Review Coordinator) (Israel), Felicity Astin (UK), Karin Åström-Olsson (Sweden), Andrzej
Budaj (Poland), Peter Clemmensen (Denmark), Jean-Philippe Collet (France), Keith A. Fox (UK), Ahmet Fuat (UK), Olivija Gustiene
(Lithuania), Christian W. Hamm (Germany), Petr Kala (Czech Replublic), Patrizio Lancellotti (Belgium), Aldo Pietro Maggioni (Italy), Béla
Merkely (Hungary), Franz-Josef Neumann (Germany), Massimo F. Piepoli (Italy), Frans Van de Werf (Belgium), Freek Verheugt
(Netherlands), Lars Wallentin (Sweden)

European Heart Journal
Advance Access published August 26, 2011

www.escardio.org/guidelinesEuropean Heart Journal
doi:10.1093/eurheartj/ehu278

KERCKHOFF
KLINIKWhat is new 2014 ?
• STEMI-Upstream bivalirudin: EUROMAX
• STEMI-Upstream ticagrelor: ATLANTIC
• NSTEMI-Upfront prasugrel: ACCOAST
• Rule out: CT new scanner

Troponin & CK elevated Troponins elevated or not
Adapted from Michael Davies
ACS without ST- Elevation
NSTEMI / Unstable A.p.
ACS with ST-
Elevation STEMI

ESC Revascularisation Guideline 2014

www.escardio.org/guidelines
Anticoagulation in primary PCI
Bivalirudin (with use of GP IIb/IIIa blocker
restricted to bailout) is recommended over
unfractionated heparin and a GP IIb/IIIa blocker.

1-Year All-Cause Mortality
Stone et al, New Engl J Med 2008
Mo
rta
lity
(%
)
0
1
2
3
4
5
Time in Months
0 1 2 3 4 5 6 7 8 9 10 11 12
Bivalirudin alone (n=1800)
Heparin + GPIIb/IIIa (n=1802) 4.8%
3.4%
Diff [95%CI] =
-1.5% [-2.8,-0.1]
HR [95%CI] =
0.69 [0.50, 0.97]
P=0.029
3.1%
2.1%
Δ = 1.0%
P=0.049
Δ = 1.4%

2218 patients with STEMI with symptom onset >20 min and ≤12h
Randomized in ambulance or non-PCI hospital
Intent for primary PCI
UFH/LMWH ± GPIPer standard practice
Bivalirudin(0.75 mg/kg bolus, 1.75 mg/kg/h infusion)
+ prolonged optional infusion (PCI dose or 0.25 mg/kg/h)
(provisional GPI only)
Aspirin + P2Y12 inhibitor
(any) as soon as possibleR
1:1
Primary endpoint: 30-day death or non-CABG related major bleeding
Key Secondary endpoint: Death, Re-infarction or non-CABG major bleeding at 30 days
Clinical FU at 30 days and 1 year
EUROMAX Trial Design
Steg et al. New Engl. J. Med. 2013

0,0
2,0
4,0
6,0
8,0
10,0
0 5 10 15 20 25 30
Days from Randomization Date
Eve
nt
Rate
Bivalirudin 1089 1038 1024 1020 1007 988 791
Heparins with optional GPI
1109 1024 1003 998 984 958 765
Bivalirudin
Heparins with optional GPI 8.4%
Log-rank p = 0.002
Patients at risk:
Primary Endpoint:Death or Major Bleed, 30 day
5.1%

0,0
2,0
4,0
6,0
8,0
0 5 10 15 20 25 30
2.7%
Log-rank p < 0.001
Non–CABG-related major bleed, 30 day
Days from Randomization Date
Bivalirudin 1089 1040 1025 1022 1010 991 794
Heparins with optional GPI
1109 1030 1009 1005 990 964 773
Patients at risk:
Eve
nt
Ra
te
6.1%
Bivalirudin
Heparins with optional GPI

0,0
1,0
2,0
3,0
4,0
0 5 10 15 20 25 30
Cardiac
Non-cardiac
Log-rank p = 0.46
Log-rank p = 0.10
3.0%
Cardiac and Non-Cardiac Death, 30-day
Days from Randomization Date
Bivalirudin 1089 1057 1048 1044 1039 1036 1034
Heparins with optional GPI
1109 1062 1061 1056 1050 1043 1037
Patients at risk:
Bivalirudin
Heparins with optional GPI
2.4%
0.1%
0.5%
Eve
nt
Ra
te

Outcomes, 30 daysBivalirudin(N=1089)
Heparins with optional GPI
(N=1109)
Relative risk [95% CI]
P Value
Reinfarction 19 (1.7) 10 (0.9) 1.93 (0.90–4.14) 0.08
Q-wave 3 (0.3) 2 (0.2) 1.53 (0.26–9.12) 0.68
Non-Q-wave 16 (1.5) 8 (0.7) 2.04 (0.88–4.74) 0.09
Stent thrombosis (ARC definition) 17 (1.6) 6 (0.5) 2.89 (1.14–7.29) 0.02
Definite 17 (1.6) 6 (0.5) 2.89 (1.14–7.29) 0.02
Probable 0 (0) 0 (0) – n/a
Acute (≤24 hours) 12 (1.1) 2 (0.2) 6.11 (1.37–27.24) 0.007
Subacute (>24 hours to 30 days) 5 (0.5) 4 (0.4) 1.27 (0.34–4.73) 0.75
Ischemia-driven revascularization 24 (2.2) 17 (1.5) 1.44 (0.78–2.66) 0.25
Reinfarction, ischemia-driven revascularization or stent thrombosis
29 (2.7) 21 (1.9) 1.41 (0.81–2.45) 0.23
Any stroke 6 (0.6) 11 (1.0) 0.56 (0.21–1.50) 0.24
Ischemic 6 (0.6) 9 (0.8) 0.68 (0.24–1.9) 0.46
Hemorrhagic 0 2 (0.2) Not applicable 0.50
Acquired thrombocytopenia 7 (0.7) 14 (1.4) 0.50 (0.20–1.24) 0.13
n/a: not applicable.

MACE and Individual CV Outcomes
Unfractionated Heparin versus Bivalirudinin Patients Undergoing PCI
Cavender, Sabatine. Lancet 2014
16 RCTs with 33,958 patients

www.escardio.org/guidelinesEuropean Heart Journal
doi:10.1093/eurheartj/ehu278
Antithrombotic therapy in
STEMI patients undergoing primary PCI

In-hospital new oral P2Y12 antagonistsPrimary PCI of STEMI
Montalescot G, et al. Lancet 2009;373:723–31 Steg PG, et al. Circulation. 2010;122:2131-41
0%
5%
10%
15%
0 2 4 6 8 10 12
Primary efficacy EP
N=7544p=0.07
Time (Months)
Cu
mu
lati
ve in
cid
ence
(%
)
ClopidogrelTicagrelor
0%
5%
10%
15%
0 50 100 150 200 250 300 350 400 450
Time (Days)
Pro
po
rtio
n o
f p
atie
nts
(%
)
9,5
12,4
10,0
HR=0.79 (0.65–0.97) NNT=41
p=0.02
RRR=21%
p=0.002
RRR=32%
6,5
ClopidogrelPrasugrel
Primary efficacy EP
TRITON PLATO

Clopidogrel Prasugrel Ticagrelor
Class Thienopyridine Thienopyridine Triazolopyrimidine
Binding Irreversible Irreversible Reversible
ActivationProdrug, limited
by metabolisationProdrug, not limited
by metabolisationActive drug
Nonresponders Yes No No
Onset of Effect 2–4 h 30 min 30 min
Duration of Effect 3–10 days 5–10 days 3–4 days
Withdrawal BeforeMajor Surgery
5 days 7 days 5 days
Adapted from Hamm CW, et al. Eur Heart J. 2011;32:2999–3054. www.escardio.org/guidelines. 21

ESC Revascularisation Guideline 2014
?

Administration of Ticagrelor in the cath Lab or in the Ambulance for New ST elevation myocardial Infarction to
open the Coronary artery
G. Montalescot, COI are available at www.action-coeur.org
G. Montalescot, A.W. van’t Hof, F. Lapostolle, J Silvain, J.F. Lassen, L. Bolognese, W.J. Cantor, A. Cequier, M. Chettibi, S.G. Goodman, C.J. Hammett, K. Huber, M. Janzon,
B. Merkely, R.F. Storey, U. Zeymer, O. Stibbe, P. Ecollan, W.M.J.M. Heutz, E. Swahn,J.P. Collet, F.F. Willems, C. Baradat, M. Licour, A. Tsatsaris, E. Vicaut, C.W. Hamm,
for the ATLANTIC investigators

Pre-Hospital
In-Hospital
Design
STE –ACS planned for PCISymptoms of acute MI >30 min but <6 hours
Ticagrelor
180mg loading
dose
RANDOMIZE 1:1
DOUBLE BLIND
•Written informed consent in mobile care unit•New persistent ST-segment elevation ≥ 1 mm in two or more contiguous ECG leads
Loading dose
placebo
Loading dose
placebo
Ticagrelor
180mg loading
dose
Primary Objectives:
TIMI flow grade 3 of MI culprit vessel at initial angiography or
≥70% ST-segment elevation resolution pre-PCI
Tic
ag
relo
r9
0m
g/b
id
30d
N ~ 1870
99.201,011

73 min 31 min 14 min
90 min 63 min
28 min
159 min
Median timesto pre- and in-hospital steps
Onset of Symptoms
EKGPre-hospital LD1 LD2
EKGPre-PCI Angiography PCI
Randomization

1st Co-primary endpointNo ST-segment resolution (≥70%)
86,8%
42,5%
87,6%
47,5%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre-PCI Post-PCI
Pre-hospitalIn-hospital
pat
ien
ts (
%)
p = NS
p = 0.055 (NS)

2nd Co-primary endpointNo TIMI 3 flow in infarct-related artery
82,6%
17,8%
83,1%
19,6%
0%
10%
20%
30%
40%
50%
60%
70%
80%
90%
100%
Pre-PCI Post-PCI
Pre-hospitalIn-hospital
pat
ien
ts (
%)
p = NS
p = NS

0%
1%
2%
3%
4%
5%
6%
7%
0 4 8 12 16 20 24 28 32
Ticagrelor in-hospital
Ticagrelor pre-hospital
30
Eve
nt
rate
(K
M %
)
Major adverse CV events up to 30 days
Ticagrelor pre-hospital : 41/906 (4.5%) Ticagrelor in-hospital 42/952 (4.4%)OR : 1.03 (95% CI 0,66, 1.0) ; p = 0.9056
MACE: death, MI, stent thrombosis, stroke or urgent revascularization
Days

Clinical endpoints at 30 days
Values are %Odds ratio
(95% CI)p-value
Death (all-cause)1.68
(0.94, 3.01) 0.08
MI0.73
(0.28, 1.94) 0.53
Stroke2.11
(0.39, 11.53) 0.39
TIANot
estimableUrgent coronary revascularization
0.66 (0.21, 2.01) 0.46
Bail-out GP IIb/IIIa inhibitors0.80
(0.59, 1.10) 0.17

Definite stent thrombosis up to 30 days
0%
1%
2%
0 2 4 6 8 10 12 14 16 18 20 22 24 26 28 30
Ticagrelor pre-hospital
Ticagrelor in-hospital
Eve
nt
rate
(K
M %
)
Time (days)
Ticagrelor pre-hospital 2/906 (0.2%) versusTicagrelor in-hospital 11/952 (1.2%)OR 0.19 (95% CI 0.04, 0.86), P=0.0225
P=0.0225
30days

Non-CABG-related bleeding events (PLATO definitions) - Safety population
1,8%
0,9%
2,6%
1,2%0,8%
2,0%1,6%
0,9%
2,5%
1,2%
0,5%
1,7%
0%
5%
10%
Major Minor Composite ofmajor and minor
Major Minor Composite ofmajor and minor
Pre-hospitalIn-hospital
Within 48h of first dose After 48h up to 30 days
p = NS p = NS p = NS p = NS p = NS p = NS
pat
ien
ts (
%)

Global time effect of ticagrelor Evolution of VASP-PRI (%) in all patients (median value)
p=0.19 (T1 vs T2)
p<0.0001* (T1 vs T3)
p<0.0001* (T1 vs T4)
p<0.0001* (T1 vs T5)
T1(Pre-PCI)
T2(End of PCI)
+37’
T3(H1 Post-PCI)
+1h 52’
T4(H6 Post-PCI)
+6h 52’
T5(Before MD)
+13h 18’
LD1 LD2Wilcoxon test with Bonferroni correction p value significant if <0.01
Platelet Function Substudy
0 120 240 360 480 600 720 840 9600
10
20
30
40
50
60
70
80
90
100
VA
SP-P
RI %
Time (min from T1)
• T1 - when catheterization starts (pre PCI)
• T2 - after PCI (end of procedure)
• T3 - 1 h post-PCI
• T4 - 6 h post-PCI
• T5 - 12 h post-PCI before the first maintenance dose

Ticagrelor pre-hospital vs. in-hospital for VASP-PRI
Pre Hospital (Pre-treatment)In Hospital (CathLab) p=NS p=NS p=NS
p=NS
p=NS
T1(PrePCI)
+67’
T2(End of PCI)
+1h44’
T3(H1 Post PCI)
+2h59’
T4(H6 PostPCI)
+8h59’
T5(Before MD)
+14h25’
LD1 LD2
0
20
40
60
80
100
Pre-PCI TIMI Flow and ST resolution
Post-PCI ST resolution
Primary objective
% V
ASP
-P
RI

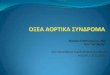
Absence of ST-segment resolution by patient characteristics
Characteristic Total patients Endpoint rate P ValueAge Pre-hospital In-hospital OR (95% CI) (Int.)
<65 years 1014 85.9% 87.3% 0.887 (0.618, 1.272) 0.6207≥65 years 584 88.6% 88.2% 1.037 (0.625, 1.724)<75 years 1348 86.7% 86.8% 0.994 (0.726, 1.362) 0.2940≥75 years 250 87.6% 92.0% 0.617 (0.269, 1.418)
SexMale 1288 87.0% 87.7% 0.945 (0.680, 1.312) 0.8292
Female 310 85.9% 87.5% 0.871 (0.451, 1.684)
DiabetesYes 212 88.3% 88.1% 1.015 (0.438, 2.353) 0.8319No 1386 86.6% 87.5% 0.922 (0.673, 1.261)
Location of MIAnterior 831 89.0% 87.3% 1.183 (0.775, 1.808) 0.1320
Non-anterior 767 84.7% 88.0% 0.750 (0.495, 1.136)TIMI risk score
0–2 971 86.0% 87.6% 0.867 (0.597, 1.256) 0.71293–6 599 88.3% 87.4% 1.081 (0.661, 1.767)>6 28 86.7% 92.3% 0.542 (0.043, 6.757)
Highest Killip Classifiation pre-PCII 1458 86.1% 88.2% 0.833 (0.612, 1.133) 0.1049
>I 82 93.5% 83.3% 2.865 (0.664, 12.236)
Prior ASA useYes 476 88.8% 87.1% 1.178 (0.670, 2.075) 0.3455No 1122 86.1% 87.9% 0.856 (0.604, 1.214)
GPIIb/IIIa inhibitor use before angiographyYes 117 85.2% 83.9% 1.106 (0.405, 3.021) 0.7281No 1481 87.0% 87.9% 0.918 (0.675, 1.248)
Morphine use for index event/PCI
Yes 800 90.8% 86.8% 1.493 (0.954, 2.331) 0.0050No 798 82.8% 88.4% 0.632 (0.423, 0.943)
Pre-hospital better In-hospital better10.5 2
Odds ratio(95% CI)

KERCKHOFF
KLINIK

KERCKHOFF
KLINIK

KERCKHOFF KLINIKUNIVERSITÄTSKLINIKUM GIESSEN
Conclusions
• Pre-hospital ticagrelor administration before pPCI in patients with
ongoing STEMI is safe.
• Ticagrelor does not improve pre-PCI coronary reperfusion.
• It may, however, reduce the risk of post-PCI stent thrombosis.
• Role of morphine?
Ticagrelor prehospital may be given, particularly
when long delay to pPCI is expected

Troponin & CK elevated Troponins elevated or not
Adapted from Michael Davies
ACS without ST- Elevation
NSTEMI / Unstable A.p.
ACS with ST-
Elevation STEMI

Fibrinogen
Thrombocyte
GP IIb/IIIa
--
ClopidogrelPrasugrelTicagrelorCangrelor
Aspirin
-GP IIb/IIIa Inhibitors
COXADP
Thrombocyte
Activation
AggregationIV
Oral
Anti-Platelet Therapy
-
PAR-1
Vorapaxar

www.escardio.org/guidelines
Recommendations for oralantiplatelet agents (1)
Recommendations Class Level
Aspirin should be given to all patients without contraindications at an initial loading dose of 150-300 mg, and at a maintenance dose of 75-100 mg dailylong-term regardless of treatment strategy.
I A
A P2Y12 inhibitor should be added to aspirin as soon as possible and maintained
over 12 months, unless there are contraindications such as excessive risk of
bleeding.
I A
A proton pump inhibitor (preferably not omeprazole) in combination with DAPT is recommended in patients with a history of gastrointestinal haemorrhage or peptic ulcer, and appropriate for patients with multiple other risk factors (H. elicobacter pylori infection, age ≥ 65 years, concurrent use of anticoagulants or steroids).
I A
Prolonged or permanent withdrawal of P2Y12 inhibitors within 12 months after
the index event is discouraged unless clinically indicated.I C
Ticagrelor (180 mg loading dose, 90 mg twice daily) is recommended for all patients at moderate-to-high risk of ischaemic events (e.g. elevated troponins), regardless of initial treatment strategy and including those pre-treated withclopidogrel (which should be discontinued when ticagrelor is commenced).
I B
Prasugrel (60 mg loading dose, 10 mg daily dose) is recommended for
P2Y12-inhibitor-naïve patients (especially diabetics) in whom coronary anatomy
is known and who are proceeding to PCI unless there is a high risk of life-
threatening bleeding or other contraindications.
I B
European Heart Journal (2011) 32:2999–3054doi:10.1093/eurheartj/ehr236
TRITON-TIMI
38
Prasugrel (60 mg loading dose, 10 mg daily dose)
is recommended for P2Y12-inhibitor-naïve patients
(especially diabetics) in whom coronary anatomy
is known and who are proceeding to PCI unless there is
a high risk of life-threatening bleeding or other
contraindications.
82723011/13

82723011/13

Days From First Dose
0 5 10 15 20 25 30
En
dp
oin
t (%
)
0
5
10
15
1996
2037
1788
1821
1775
1809
1769
1802
1762
1797
1752
1791
CV Death, MI, Stroke, UR, GPIIb/IIIa Bailout
1621
1616
No. at Risk, Primary
Efficacy End Point:
No pre-treatment
Pre-treatment
Pre-treatment10.810.0
Pre-treatment
Hazard Ratio, 0.997 (95% 0.83, 1.20)P=0.98P=0.81
(95% 0.84, 1.25) Hazard Ratio, 1.02
No Pre-treatment10.8
9.8No Pre-treatment
1° Efficacy End Point @ 7 + 30 days
(All Patients)
82723011/13

All TIMI (CABG or non-CABG) Major Bleeding
(All Treated patients)
Days From First Dose
0 5 10 15 20 25 30
En
dp
oin
t (%
)
0
1
2
3
4
5
All TIMI Major Bleeding
Pre-treatment2.9
Pre-treatment2.6
No Pre-treatment1.5
No Pre-treatment1.4
19962037
19471972
13281339
12971310
12881299
12841297
12631280
No. at Risk, All TIMI Major Bleeding:No pre-treatmentPre-treatment
Hazard Ratio, 1.97 (95% 1.26, 3.08)P=0.002
Hazard Ratio, 1.90(95% 1.19, 3.02) P=0.006
82723011/13

www.escardio.org/guidelinesEuropean Heart Journal
doi:10.1093/eurheartj/ehu278
Antithrombotic therapy in
NSTE-ACS patients undergoing PCI

Rapid rule-out of ACS with high-sensitivity troponin.

www.escardio.org/guidelines
Recommendations for diagnosisand risk stratification
Recommendations Class Level
Blood has to be drawn promptly for troponin (cardiac troponin T or I)
measurement.The result should be available within 60 min.The test should be
repeated 6-9 h after initial assessment if the first measurement is not conclusive.
Repeat testing after 12-24 h is advised if the clinical condition is still suggestive
of ACS.
I A
A rapid rule-out protocol (0 and 3 h) is recommended when highly sensitive
troponin tests are available.I B
An echocardiogram is recommended for all patients to evaluate regional and
global LV function and to rule in or rule out differential diagnoses.I C
Coronary angiography is indicated in patients in whom the extent of CAD or
the culprit lesion has to be determined.I C
Coronary CT angiography should be considered as an alternative to invasive
angiography to exclude ACS when there is a low to intermediate likelihood of
CAD and when troponin and ECG are inconclusive.IIa B
In patients without recurrence of pain, normal ECG findings, negative troponins
tests, and a low risk score, a non-invasive stress test for inducible ischaemia is
recommended before deciding on an invasive strategy.I A
European Heart Journal (2011) 32:2999–3054doi:10.1093/eurheartj/ehr236
A rapid rule-out protocol (0 and 3 h) is recommended
when highly sensitive troponin tests are available.

KERCKHOFF
KLINIK
T. Reichlin, Arch Intern Med. 2012
Hs-Troponin Elevation on Admission

www.escardio.org/guidelines
Recommendations for diagnosisand risk stratification (2)
Recommendations Class Level
Blood has to be drawn promptly for troponin (cardiac troponin T or I)
measurement.The result should be available within 60 min.The test should be
repeated 6-9 h after initial assessment if the first measurement is not conclusive.
Repeat testing after 12-24 h is advised if the clinical condition is still suggestive
of ACS.
I A
A rapid rule-out protocol (0 and 3 h) is recommended when highly sensitive
troponin tests are available.I B
An echocardiogram is recommended for all patients to evaluate regional and
global LV function and to rule in or rule out differential diagnoses.I C
Coronary angiography is indicated in patients in whom the extent of CAD or
the culprit lesion has to be determined.I C
Coronary CT angiography should be considered as an alternative to invasive
angiography to exclude ACS when there is a low to intermediate likelihood of
CAD and when troponin and ECG are inconclusive.IIa B
In patients without recurrence of pain, normal ECG findings, negative troponins
tests, and a low risk score, a non-invasive stress test for inducible ischaemia is
recommended before deciding on an invasive strategy.I A
European Heart Journal (2011) 32:2999–3054doi:10.1093/eurheartj/ehr236
Coronary CT angiography should be considered as an
alternative to invasive angiography to exclude ACS
when there is a low to intermediate likelihood of CAD
and when troponin and ECG are inconclusive.

KERCKHOFF
KLINIK

KERCKHOFF
KLINIK
Length of Stay in the Hospital and Proportion of Patients Discharged.
Hoffmann U et al. N Engl J Med 2012;367:299-308.

KERCKHOFF
KLINIK
New: Somatom Force

Somatom Force
CHANGE AS COMPARED MAIN ADVANTAGETO „FLASH“
Faster Rotation (=> 65 ms temporal resolution)
New Detector (=> 2 x 192 slices, faster coverage, lower noise)
New Tube (=> 70 kV at high mAs)
Collimators (=> dose for sequential scan)
New Iterative Reconstruction (=> more natural look)
Courtesy of Stephan Achenbach

Clinical Results
Courtesy of Stephan Achenbach

SOMATOM FORCE: SEVERE DISEASE
Courtesy of Stephan Achenbach

SOMATOM FORCE: Clinical Results
DLP 19
=> Effective Dose 0.3 mSvCourtesy of Stephan Achenbach

SOMATOM FORCE: IMAGE QUALITY - STENTS
Courtesy of Stephan Achenbach

Rapid rule-out of ACS with high-sensitivity troponin.
CT

KERCKHOFF
KLINIK
Thank you !
KERCKHOFF
KLINIK

www.escardio.org/guidelines
Recommendations for oralantiplatelet agents (1)
Recommendations Class Level
Aspirin should be given to all patients without contraindications at an initial loading dose of 150-300 mg, and at a maintenance dose of 75-100 mg dailylong-term regardless of treatment strategy.
I A
A P2Y12 inhibitor should be added to aspirin as soon as possible and maintained
over 12 months, unless there are contraindications such as excessive risk of
bleeding.
I A
A proton pump inhibitor (preferably not omeprazole) in combination with DAPT is recommended in patients with a history of gastrointestinal haemorrhage or peptic ulcer, and appropriate for patients with multiple other risk factors (H. elicobacter pylori infection, age ≥ 65 years, concurrent use of anticoagulants or steroids).
I A
Prolonged or permanent withdrawal of P2Y12 inhibitors within 12 months after
the index event is discouraged unless clinically indicated.I C
Ticagrelor (180 mg loading dose, 90 mg twice daily) is recommended for all patients at moderate-to-high risk of ischaemic events (e.g. elevated troponins), regardless of initial treatment strategy and including those pre-treated withclopidogrel (which should be discontinued when ticagrelor is commenced).
I B
Prasugrel (60 mg loading dose, 10 mg daily dose) is recommended for
P2Y12-inhibitor-naïve patients (especially diabetics) in whom coronary anatomy
is known and who are proceeding to PCI unless there is a high risk of life-
threatening bleeding or other contraindications.
I B
Ticagrelor (180 mg loading dose, 90 mg twice daily) is recommended for all patients at moderate-to-high risk of ischaemic events (e.g. elevated troponins), regardless
of initial treatment strategy and including those pre-treated with clopidogrel (which should be discontinued
when ticagrelor is commenced).
European Heart Journal (2011) 32:2999–3054doi:10.1093/eurheartj/ehr236
PLATO

www.escardio.org/guidelines
Recommendations for oralantiplatelet agents (2)
Recommendations Class Level
Clopidogrel (300 mg loading dose, 75 mg daily dose) is recommended for patients who cannot receive ticagrelor or prasugrel.
I A
A 600 mg loading dose of clopidogrel (or a supplementary 300 mg dose at PCI following an initial 300 mg loading dose) is recommended for patients scheduled for an invasive strategy when ticagrelor or prasugrel is not an option.
I B
A higher maintenance dose of clopidogrel 150 mg daily should be considered for the first 7 days in patients managed with PCI and without increased risk of bleeding.
IIa B
Increasing the maintenance dose of clopidogrel based on platelet function testing is not advised as routine, but may be considered in selected cases.
IIb B
Genotyping and/or platelet function testing may be considered in selected cases when clopidogrel is used.
IIb B
In patients pre-treated with P2Y12 inhibitors who need to undergo non-emergent major surgery (including CABG), postponing surgery at least for 5 days after cessation of ticagrelor or clopidogrel, and 7 days for prasugrel, if clinicallyfeasible and unless the patient is at high risk of ischaemic events should be considered.
IIa C
Ticagrelor or clopidogrel should be considered to be (re-)started after CABG surgery as soon as considered safe.
IIa B
The combination of aspirin with an NSAID (selective COX-2 inhibitors and non-selective NSAID) is not recommended.
III C
European Heart Journal (2011) 32:2999–3054doi:10.1093/eurheartj/ehr236

Recommendations for oral Antiplatelet Agents 2

www.escardio.org/guidelines
Decision-making algorithm in ACS
Evaluation
• Quality of chest pain.
• Symptom-orientated
physical examination.
• Short history for the
likelihood of CAD.
• Electrocardiogram
(ST elevation?).
STEMI reperfusion
ACS
possible
1. Clinical Evaluation 2. Diagnosis/Risk Assessment 3. Coronary angiography
No CAD
early
< 24 h
< 72 h
urgent
< 120 min
no/elective
Validation
• Response to antianginal treatment.
• Biochemistry/troponin.
• ECG.
• Echocardiogram.
• Calculated risk score (GRACE).
• Risk criteria.
• Optional: CT, MRI, scintigraphy.

www.escardio.org/guidelines
Recommendation for initial diagnosis
Echocardiography may assist in making the
diagnosis in uncertain cases but should not
delay transfer for angiography.