Embed Size (px)
Citation preview

Acute Effects of Transluminal Angioplastyin Three Experimental Models of
AtherosclerosisDavid P. Faxon, Vance J. Weber, Christian Haudenschild,
Susan B. Gottsman, Wanda A. McGovern, and Thomas J. Ryan
Transluminal angioplasty has shown promise as a nonoperative treatment ofatherosclerotic obstruction. Despite its Increasing clinical use and potential Impor-tance, little Is known of its mechanism and acute effects. To evaluate transluminalangioplasty, three rabbit models of experimental atherosclerosis were developed:Group 1 (n = 20) = high cholesterol diet plus balloon de-endothellalization; Group 2A(n = 12) = high cholesterol diet plus an Indwelling catheter; Group 2B (n = 10) =normal diet plus an indwelling catheter. After 6 weeks or 8 weeks, distinct angio-graphlc and pathological lesions In the iliac artery were evident in all groups. Group 1showed predominant foam cell lesions, while Group 2 showed eccentric mixed fi-brous and foam cell or only fibrous lesions. Significant anglographic stenosis waspresent in 78% of the animals. Angioplasty of the highest grade lilac stenosis resultedIn at least a 20% reduction In luminal diameter narrowing In 26 of 37 animals (70%).Hlstopathologlcal examination 1 day following angloplasty In 17 animals showed twopatterns. In Group 1 animals, neointimal fracture and dissection were evident, while inGroup 2 animals thinning and stretching of the nonatherosclerotic portion of thevessel walls could be demonstrated. This study demonstrates that the New Zealandrabbit can be used to produce a spectrum of morphologically distinct atheroscleroticlesions that lend themselves to the study of transluminal angloplasty. The immediateconsequences of angloplasty, which appear to depend upon the underlying hlsto-pathology and widening of the narrowed lumen, are frequently concurrent with intlmalfracture, dissection, or thinning of the nonatherosclerotic portion of the vessel wall.(Arteriosclerosis 2: 125-133, March/April 1982)
The development and clinical utilization of translu-minal angioplasty has provided a nonsurgical
treatment of atherosclerotic obstruction. In 1964,Dotter and Judkins1 described a method for enlarg-ing the lumen of stenotic peripheral vessels using apercutaneous catheter system. The development ofa unique double balloon catheter system in 1973 hasallowed successful nonsurgical treatment of periph-eral, renal, coronary, and cerebral vascular diseasein selected patients.2 The results of peripheral percu-taneous dilatation have been encouraging with aninitial success rate of 80% and a patency rate of 73%after 2 years.3 The use of transluminal angioplasty in
From the Evans Memorial Department of Clinical Research andDepartment of Medicine, University Hospital, Boston UniversityMedical Center, Boston, Massachusetts.
This work was supported in part by NIH Grant 1 ROLNL27512-01.Address for reprints: David P. Faxon, M.D., Department of Car-
diology, University Hospital, 75 East Newton Street, Boston,Massachusetts 02118.
Received September 21, 1981; revision accepted January 8,1982.
the treatment of coronary artery obstruction hasbeen most encouraging, since this disease com-prises a major health problem worldwide.4 Initial re-ports from a national registry sponsored by the Na-tional Institutes of Health have indicated an initialsuccess of 63% with a low mortality and excellentlong term symptomatic relief of angina in the first1500 patients reported.5
Despite the early promise of this treatment, little isknown about its mechanism of action, long-term con-sequences, and whether a lasting amelioration ofobstructive atherosclerosis will be possible. It wasinitially postulated that the enlargement of the vascu-lar lumen was due to compression of the atheroscle-rotic plaque.3 However, other possibilities includeredistribution of the atheroma, embolization of ather-osclerotic debris, stretching or aneurysm formation,and localized fracture or dissection of the plaque.This experimental animal study was undertaken todevelop an animal model that would be suitable forthe study of transluminal angioplasty and to evaluatethe possible mechanism of its immediate effects.
125
by guest on May 7, 2018
http://atvb.ahajournals.org/D
ownloaded from

126 ARTERIOSCLEROSIS VOL 2, No 2, MARCH/APRIL 1982
Methods
Aortic and left iliac atherosclerosis was developedin 42 New Zealand white male rabbits each weighing3 kg. Three distinct methods combining vascular in-jury with cholesterol feeding provided a spectrum ofatherosclerotic disease. Group 1 rabbits (n = 20)were anesthetized with pentothal. After surgical ex-posure of the left femoral artery, aortic and left iliacendothelial debridement was performed by the tech-nique described by Baumgartner.6 In this technique,a 3F Fogarty balloon catheter is passed to 30 cm andinflated until gentle contact with the vascular wall isachieved. De-endothelialization is accomplished bygradually pulling the catheter down the aorta andiliac vessels. To assure adequate de-endothelializa-tion, the Fogarty balloon was passed twice to 30 cm.All animals were then placed on a 2% cholesteroldiet composed of rabbit chow supplemented with10% peanut oil for 6 weeks. On this diet, serum cho-lesterol levels were found to be in the range of 1000to 1200 mg%.
Group 2 animals (n = 22) had atherosclerotic le-sions produced by the surgical placement of a 20 cmP50 polyethylene catheter into the left femoral arteryand advanced into the aorta to approximately theupper abdominal level as described by Moore.7 Theend of the catheter was sutured in place and allowedto remain in the artery for 8 weeks. Previous pilotstudies had indicated that an 8-week period wasnecessary to develop atherosclerosis with thismethod. Twelve animals were placed on a 2% cho-lesterol diet and the remainder on normal rabbitchow.
After 6 or 8 weeks, during which atherosclerosiswas allowed to develop, all animals underwent ab-dominal arteriography in the following manner: surgi-cal exposure of the right and left femoral artery wasperformed and the indwelling catheter in Group 2animals removed. In no animal was this removaltraumatic. A 4F or 5F Cournand or Goodale Lubincatheter was introduced into the right femoral arteryand passed retrograde to a position 1 to 2 cm abovethe aortic bifurcation, just below the renal arteries asverified by fluoroscopy. Renograffin 76 (3 cc) wasinjected over 3 seconds, and angiographic imageswere recorded on 35 mm film using a Philips 6-inchimage intensifier with a resolution of 3.8 line pairs/mm. A 2.5 or 3.0 mm Gruntzig intraoperative translu-minal angioplasty catheter was then placed retro-grade under fluoroscopic guidance through the sur-gically exposed left femoral artery. With use of avideo recording of the angiogram, the dilatation cath-eter was positioned at the point of highest grade iliacstenosis and inflated three times to 5 atmospheresfor 30 seconds. The catheter size and inflation pres-sure was chosen to carefully approximate clinicaluse. After removal of the catheter, a repeat angio-gram was performed. During each angiogram, carewas taken to position the image intensifier at thesame height and a 1 cm grid was positioned at thelevel of the spine in order to provide correction for
magnification error. The pre- and postdilatation cine-angiograms were then compared to estimate anychange in the narrowest segment that underwentdilatation. Percent stenosis was estimated in eachanimal by using the proximal nondilated but dis-eased segment in the left iliac artery as the controlsegment. In addition, the size of the dilated segmentand adjacent nondilated segment was calculatedusing the grid to correct for magnification.
A change in vessel size of 20% could readily beresolved using this technique and was felt to be sig-nificant. Each angiogram was read independently bytwo angiographers, and discrepancies resolved by asubsequent simultaneous reading.
One day following angiography, 17 animals (six inGroup 1, and 11 in Group 2) were sacrificed by pen-tothol anesthesia during which a 10% solution offormalin was infused via the aorta at a pressure of 80mm Hg for 15 minutes as previously described.8 Theaorta and iliac vessels were surgically removed andplaced in formalin. Sections of the abdominal aortaand control right iliac as well as serial 1 cm sectionsof the left iliac artery were obtained. This allowedexamination by light microscopy of at least two sec-tions through the dilated area. Sections stained withhematoxylin and eosin and Verhoff Von Giesen elas-tin were viewed by at least two investigators, and aconsensus reading was made as to the histologicalfindings. The remaining animals were followed todetermine the longer term effects of angioplasty andwere sacrificed at 2 or 4 weeks after angioplasty.Details of this longer term study are the subject of alater repSrt.
Results
Atherosclerotic Model
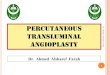
Three morphologically distinct atherosclerotic le-sions were produced by the combination of vascularinjury and variations of cholesterol feedings, asshown in table 1. All animals, those sacrificed at 24hours and at 2 or 4 weeks postangioplasty, wereincluded in this analysis. Group 1 animals (n = 20)demonstrated concentric foam cell lesions charac-terized by marked intimal thickening and filled withlipid-laden cells and a fibrous cap. In addition, intra-cellular lipid was frequently noted in the media. Onlyrarely was significant fibrosis noted in this group ofanimals. A representative example of this type oflesion is seen in figure 1.
Table 1. Hlstopathology of Experimental Models
Model Foam Mixed Fibrous
Group 1 (n = 20) 16 4 0Group 2A (n = 12) 1 9 2Group 2B (n = 10) 0 2 8
by guest on May 7, 2018
http://atvb.ahajournals.org/D
ownloaded from
EXPERIMENTAL ANGIOPLASTY Faxon et al. 127
Figure 1 . Portion of a concentric lesion in a rabbit of Group 1 showing predominantly foam cells and a thin luminal fibrouscap. The foam cells in the thickened intima appear similar to those in the media. The internal elastic lamina is intact andstraightened, x 185
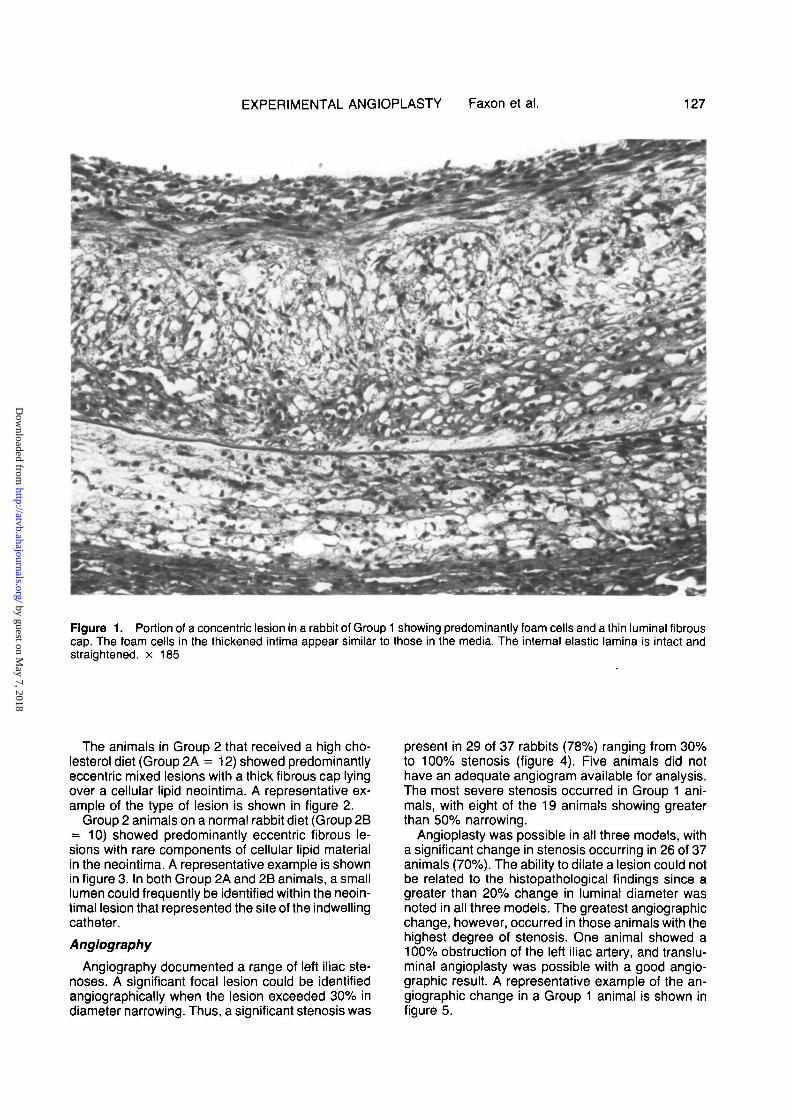
The animals in Group 2 that received a high cho-lesterol diet (Group 2A = 12) showed predominantlyeccentric mixed lesions with a thick fibrous cap lyingover a cellular lipid neointima. A representative ex-ample of the type of lesion is shown in figure 2.
Group 2 animals on a normal rabbit diet (Group 2B= 10) showed predominantly eccentric fibrous le-sions with rare components of cellular lipid materialin the neointima. A representative example is shownin figure 3. In both Group 2A and 2B animals, a smalllumen could frequently be identified within the neoin-timal lesion that represented the site of the indwellingcatheter.
Anglography
Angiography documented a range of left iliac ste-noses. A significant focal lesion could be identifiedangiographically when the lesion exceeded 30% indiameter narrowing. Thus, a significant stenosis was
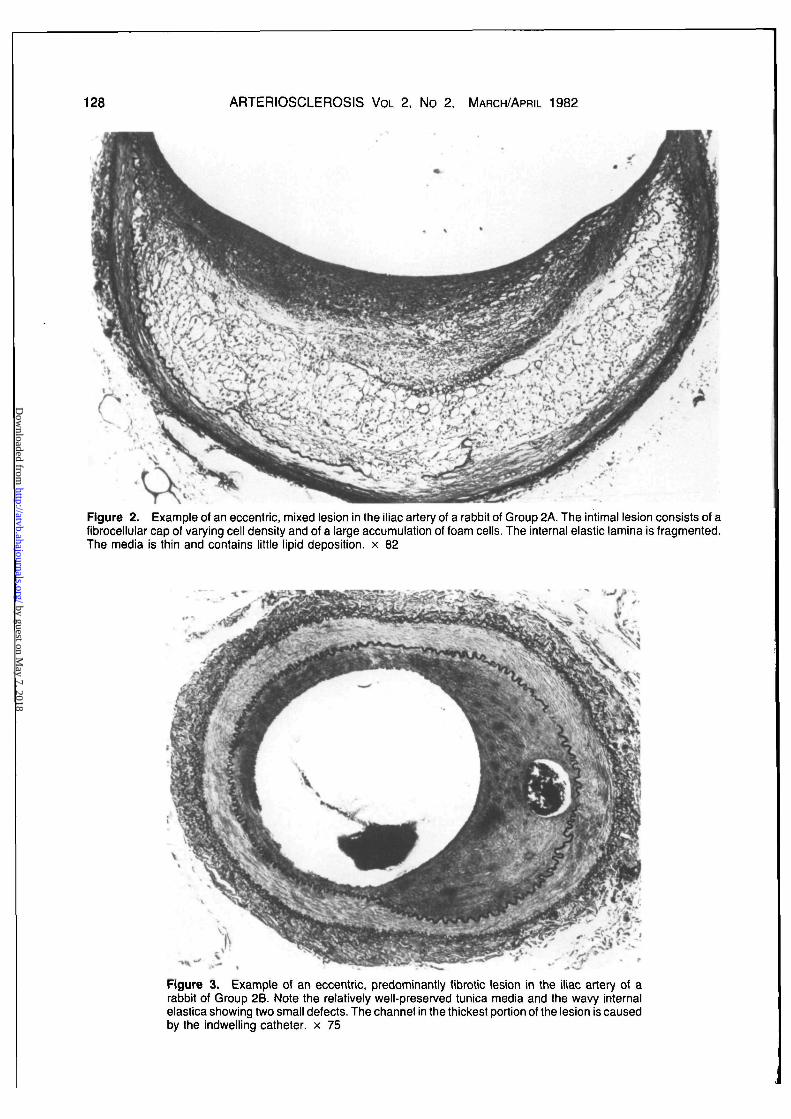
present in 29 of 37 rabbits (78%) ranging from 30%to 100% stenosis (figure 4). Five animals did nothave an adequate angiogram available for analysis.The most severe stenosis occurred in Group 1 ani-mals, with eight of the 19 animals showing greaterthan 50% narrowing.
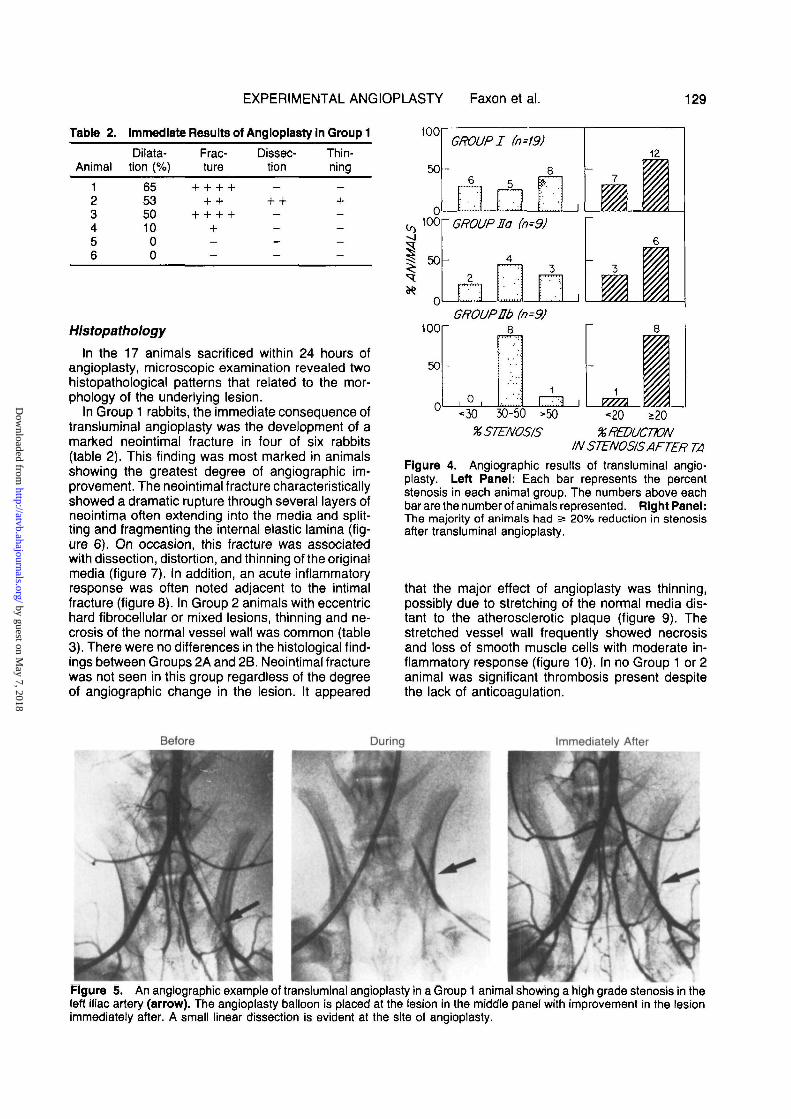
Angioplasty was possible in all three models, witha significant change in stenosis occurring in 26 of 37animals (70%). The ability to dilate a lesion could notbe related to the histopathological findings since agreater than 20% change in luminal diameter wasnoted in all three models. The greatest angiographicchange, however, occurred in those animals with thehighest degree of stenosis. One animal showed a100% obstruction of the left iliac artery, and translu-minal angioplasty was possible with a good angio-graphic result. A representative example of the an-giographic change in a Group 1 animal is shown infigure 5.
by guest on May 7, 2018
http://atvb.ahajournals.org/D
ownloaded from
128 ARTERIOSCLEROSIS VOL 2. No 2. MARCH/APRIL 1982
Figure 2. Example of an eccentric, mixed lesion in the iliac artery of a rabbit of Group 2A. The intimal lesion consists of afibrocellular cap of varying cell density and of a large accumulation of foam cells. The internal elastic lamina is fragmented.The media is thin and contains little lipid deposition, x 82
Figure 3. Example of an eccentric, predominantly fibrotic lesion in the iliac artery of arabbit of Group 2B. Note the relatively well-preserved tunica media and the wavy internalelastica showing two small defects. The channel in the thickest portion of the lesion is causedby the indwelling catheter, x 75
by guest on May 7, 2018
http://atvb.ahajournals.org/D
ownloaded from
EXPERIMENTAL ANGIOPLASTY Faxon et al. 129
Table 2. Immediate Results of Angioplasty In Group 1
AnimalDilata-
tion (%)Frac-ture
Dissec-tion
Thin-ning
123.456
6553501000
Hlstopathology
In the 17 animals sacrificed within 24 hours ofangioplasty, microscopic examination revealed twohistopathological patterns that related to the mor-phology of the underlying lesion.
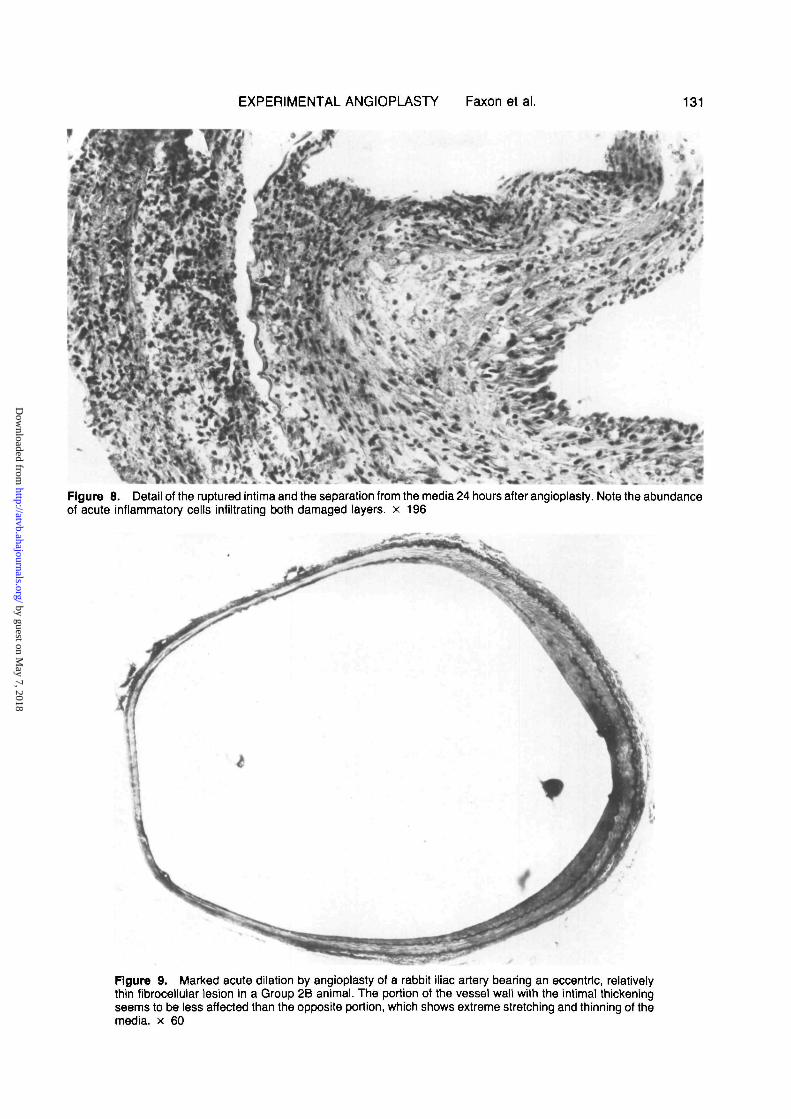
In Group 1 rabbits, the immediate consequence oftransluminal angioplasty was the development of amarked neointimal fracture in four of six rabbits(table 2). This finding was most marked in animalsshowing the greatest degree of angiographic im-provement. The neointimal fracture characteristicallyshowed a dramatic rupture through several layers ofneointima often extending into the media and split-ting and fragmenting the internal elastic lamina (fig-ure 6). On occasion, this fracture was associatedwith dissection, distortion, and thinning of the originalmedia (figure 7). In addition, an acute inflammatoryresponse was often noted adjacent to the intimalfracture (figure 8). In Group 2 animals with eccentrichard fibrocellular or mixed lesions, thinning and ne-crosis of the normal vessel wall was common (table3). There were no differences in the histological find-ings between Groups 2A and 2B. Neointimal fracturewas not seen in this group regardless of the degreeof angiographic change in the lesion. It appeared
too
50
Co 1 0 0
50
GROUP I (n=19)
GROUP Ea (n=9)
12
GROUP Eb100
50 -
8
1
HZI I1
V777X
8n" <30 30-50 >50 <20 >20
% STENOSIS % REDUCTIONIN STENOSIS AFTER TA
Figure 4. Angiographic results of transluminal angio-plasty. Left Panel: Each bar represents the percentstenosis in each animal group. The numbers above eachbar are the number of animals represented. Right Panel:The majority of animals had 2= 20% reduction in stenosisafter transluminal angioplasty.
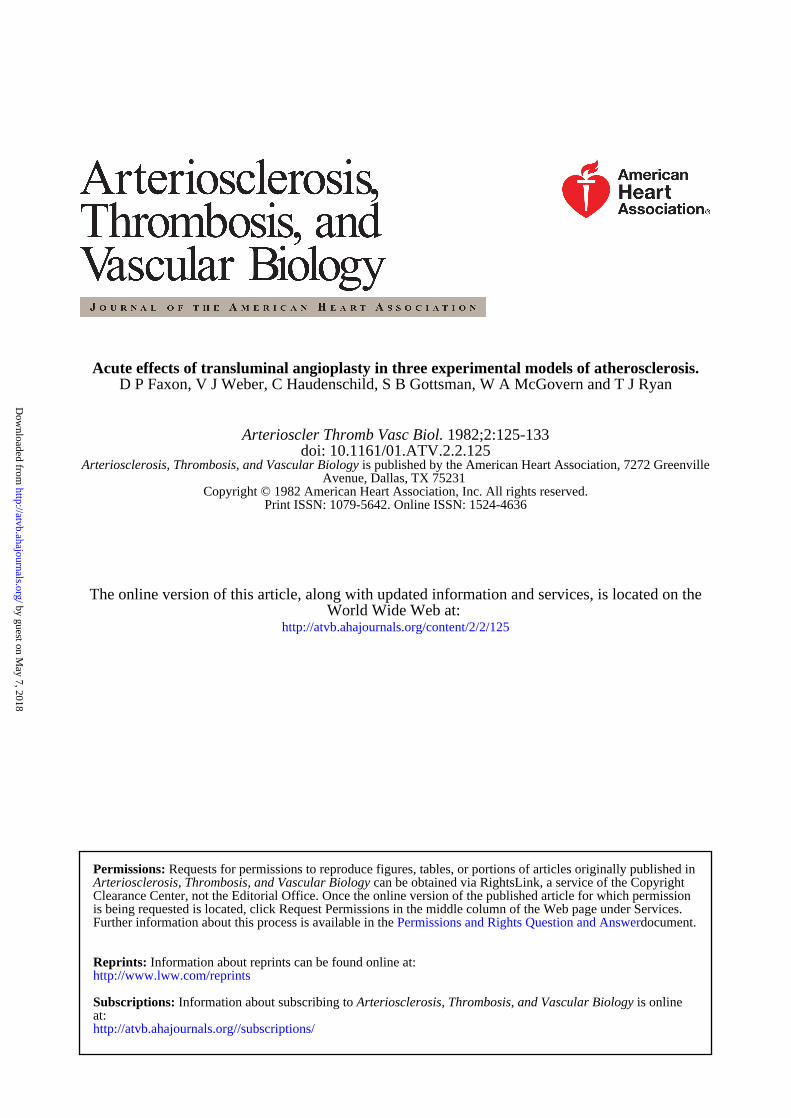
that the major effect of angioplasty was thinning,possibly due to stretching of the normal media dis-tant to the atherosclerotic plaque (figure 9). Thestretched vessel wall frequently showed necrosisand loss of smooth muscle cells with moderate in-flammatory response (figure 10). In no Group 1 or 2animal was significant thrombosis present despitethe lack of anticoagulation.
Before During Immediately After
Figure 5. An angiographic example of translumlnal angioplasty in a Group 1 animal showing a high grade stenosis in theleft Iliac artery (arrow). The angioplasty balloon is placed at the lesion in the middle panel with improvement in the lesionimmediately after. A small linear dissection is evident at the site of angioplasty.
by guest on May 7, 2018
http://atvb.ahajournals.org/D
ownloaded from

130 ARTERIOSCLEROSIS VOL 2, No 2, MARCH/APRIL 1982
Figure 6. Acute effect of the angioplasty on an iliac artery with a mixed intimal lesion. Thethickened intima is ruptured and is separated from the media along the intemal elastic laminaover a large portion of the circumference, x 60
Figure 7. Acute angioplasty effect on a rabbit iliac artery which was virtually occluded by a lesion. The angioplasty balloonhas cleaved the thickened intima from the media, opening up a new lumen with aneurysmal dilations and overstretching ofportions of the media. The intimal lesion containing many foam cells appears not to be compressed, x 40
by guest on May 7, 2018
http://atvb.ahajournals.org/D
ownloaded from
EXPERIMENTAL ANGIOPLASTY Faxon et al.
Figure 8. Detail of the ruptured intima and the separation from the media 24 hours after angioplasty. Note the abundanceof acute inflammatory cells infiltrating both damaged layers, x 196
Figure 9. Marked acute dilation by angioplasty of a rabbit iliac artery bearing an eccentric, relativelythin fibroceiiuiar lesion in a Group 2B animal. The portion of the vessel wall with the intimal thickeningseems to be less affected than the opposite portion, which shows extreme stretching and thinning of themedia, x 60
by guest on May 7, 2018
http://atvb.ahajournals.org/D
ownloaded from

132 ARTERIOSCLEROSIS VOL 2, No 2, MARCH/APRIL 1982
Table 3. Immediate Results of Angioplasty InGroups 2A and 2B
Animal
123456789
1011
Dilata-tion (%)
100584543403522191900
Frac-ture
—--———_———-
Dissec-tion
+ +---——————-
Thin-ning
++ +++
+ + +++
+ 4-+—-
Discussion
This study demonstrates that the New Zealandrabbit can be used to produce a spectrum of morpho-logically distinct lesions that lend themselves to thestudy of transluminal angioplasty. Experimental ath-erosclerosis created in this animal model varies fromhuman atherosclerosis in that fibrosis, necrosis, ex-tracellular lipid, and calcium are frequently absent. Incontrast, the lesions created in the rabbit containabundant lipid-laden foam cells with little extracellu-lar cholesterol. However, Block et al.9 have suggest-ed that the rabbit is a desirable animal model for thestudy of balloon angioplasty due to the rapid devel-opment of atherosclerosis, ease of handling, and rel-
ative low cost. In addition, the iliac vessels are similarin size and character to human coronary vessels andfrequently develop concentric lesions of a highenough degree to be suitable for angioplasty. Rec-ognizing the limitations of any one animal model ofatherosclerosis, we have demonstrated that by usingtwo methods of intimai injury, three histopathologi-cally distinct types of atherosclerotic plaques can becreated. This diversity provides a useful model forthe study of angioplasty.
In this study, more than 75% of the animals devel-oped significant angiographic obstruction and angio-plasty could be accomplished irrespective of thehistopathological findings. Clinical experience hassuggested that fibrous lesions may be less amena-ble to angioplasty than soft lipid lesions.4 Althoughwe are unable to comment on concentric fibrous le-sions, the ability to dilate did not appear to relate tothe degree of neointimal fibrosis. It is possible thathuman lesions with more necrosis, fibrosis, and cal-cium respond differently to transluminal angioplasty.
The mechanism by which transluminal angio-plasty reduces luminal narrowing in humans remainslargely undefined. Earlier clinical and pathologicalstudies have suggested that redistribution or com-pression of the intramural lipid within the plaquemight occur; however, there is little experimental evi-dence to support this hypothesis. Castaneda-Zunigaet al.10 suggested that aneurysmal dilatation of theatherosclerotic vessel occurs following balloon an-gioplasty. Studying human autopsy iliac and femoralarteries as well as normal dog peripheral vessels,
Figure 10. Detail of the overstretched nonatherosclerotic media opposite an eccentric intimai thickening 24 hours afterangioplasty. Endothelial cells are absent, medial smooth muscle cells are necrotic, and the media is thin and containspolymorphonuclear leukocytes in its luminal portion, x 230
by guest on May 7, 2018
http://atvb.ahajournals.org/D
ownloaded from

EXPERIMENTAL ANGIOPLASTY Faxon et al. 133
the authors showed that angioplasty results in abulging at the site of dilatation, which could be pre-vented by placing the vessel within a constrictingglass tube. The findings of the present study wouldsupport the concept that when eccentric, fibrotic le-sions are present, balloon dilatation results instretching of the nonatherosclerotic media and aneu-rysm formation. Pasternak et al.11 demonstratedthat, in a normal canine coronary artery, angioplastycauses loss of endothelium with stimulation of plate-let adhesion and thrombosis formation. Althoughheparin and aspirin were ineffective in reducing theplatelet adhesion, dextran was effective. In subse-quent experiments in rabbits, these authors demon-strated that angioplasty of the aorta and iliac vesselsfrequently caused desquamation of the endotheliumand splitting of atheroma.9 The present study ex-tends these preliminary observations and demon-strates that marked intimal damage with fracturethrough the neointima is common in the foam celllesions typical of this model. This fracture frequentlyextends into the media with disruption of the internalelastic lamina. In addition, dissection, as well as thin-ning of the media, occurs with a significant acuteinflammatory response often adjacent to the fractureplane. We have also demonstrated that in eccentricfibrocellular lesions thinning and stretching of themedia occurs and neointimal fracture is distinctly ab-sent. Thus, the histopathological lesion determinesthe immediate microscopic findings after angio-plasty. It is noteworthy that no evidence of significantthrombosis occurred following angioplasty. Althoughwe did not specifically examine the specimens fordesquamation and platelet adhesion, it seems likelythat this did occur. Perhaps the improvement in ves-sel flow and spontaneous thrombolysis preventedthrombotic complication.
Since no animal model of atherosclerosis exactlyrepresents human atherosclerosis, direct extrapola-tion of these findings to patients is subject to criti-cism. However, the degree and type of histologicalfindings in this study are consistent with human au-topsy studies. Freudenberg et al.12 demonstratedthat vascular dissection frequently occurred in au-topsy human hearts during postmortem angioplasty.However, Lee et al.13 reported that only minimal dis-ruption of the arterial wall could be documented in 12human cadaver hearts that underwent angioplasty.Pathological material obtained from three patientswho died within 3 days of successful percutaneoustransluminal angioplasty has shown significant frac-tures of the atheroma extending into the media.14
The histological findings in these patients are identi-cal to that noted in our Group 1 animals.
The results of this study demonstrate that the NewZealand rabbit can be used to produce a spectrum ofmorphologically distinct atherosclerotic lesions thatcan be assessed by angiography and that lend them-
selves to the study of transluminal angioplasty. Inaddition to the appropriate size and degree of steno-sis, angioplasty can be accomplished in the majorityof animals. This study provides evidence that, de-pending on the nature of the stenosing lesion, eithermarked intimal fracture and dissection, or thinning ofthe vessel wall, can occur as a consequence of suc-cessful angioplasty. Although these findings docu-ment the injurious nature of angioplasty, it is possiblethat these acute changes could result in long-termpatency. In addition, despite marked histologicalfindings, angiography documented no instance ofperforation or sudden occlusion of the vessel. Fur-ther investigation of the long-term consequence oftransluminal angioplasty and methods of improvingthe success of this procedure in this animal modelshould provide valuable information applicable to hu-man angioplasty.
References1. Dotter CT, Judklns MP. Transluminal treatment of athero-
sclerotic obstruction: Description of a new technique and apreliminary report of its application. Circulation 1964;30:654
2. Gruntzlg AR. Die perkutane Rekanalisation chronischer ar-terieller Verschlusse (Dotter-Prinzip) mit einem doppellumin-gen Dilatationskatheter Fortschr Rontgenstr 1976;124:80
3. Zertler E, Gruntzlg AR, Schoop W, eds. Percutaneous vas-cular recanalization. Heidelberg: Springer, 1978
4. Gruntzlg AR, Sennlng A, Selgenthaler WE. Non-operativedilation of coronary artery stenosis. Percutaneous translu-minal coronary angioplasty. N Engl J Med 1979;301:61
5. Proceedings of the workshop on percutaneous translu-minal coronary angioplasty. DHEW publication PHS NIH80-2030 Washington, DC: National Institutes of Health, 1980
6. Baumgartner HR. The role of blood flow in platelet adhesion,fibrin deposition, and formation of mural thrombi. MicrovascRes1973;5:167
7. Moore S. Ttiromboatherosclerosis in normolipemic rabbits. Aresult of continued endothelial damage. Lab Invest 1973;29:478
8. Haudenschlld CC, Baumgartner AR, Studer A. Signifi-cance of fixation procedure for preservation of arteries. Ex-perientJa 197228:828
9. Block PC, Baughman KL, Pasternak RC, Fallon JT. Trans-luminal angioplasty: Correlation of morphologic and angle-graphic findings In an experimental model. Circulation 1978;61:778
10. Castaneda-Zunlga WR, Formanek A, Tadavarthy M, et al.Trie mechanism of balloon angioplasty. Diagn Radiol 1980;135:565-571
11. Pasternak RC, Baughman KL, Fallon JT, Block PC. Scan-ning electron microscopy after coronary transluminal angio-plasty of normal canine coronary arteries. Am J Cardiol1980;45:591-598
12. Freudenberg H, Llchten PR, Engel HJ. Transluminal angio-plasty of the coronary arteries — an analysis of the mostimportant complications by a post mortal study in the humanheart (ger) Z Kardiol 1981;70 (1):39-44
13. Lee G, Ikeda RM, Joye JA, Bogren HG, DeMarla AN, Ma-son DT. Evaluation of transluminal angioplasty of chronicartery stenosis. Circulation 1980;61:77-83
14. Block PC, Myler RK, Stertzer S, Fallon JT. Morphologyafter transluminal angioplasty in human beings. N Engl J Med1981:305:382-385
Index Terms: angioplasty • atherosclerosis • animal model
by guest on May 7, 2018
http://atvb.ahajournals.org/D
ownloaded from
D P Faxon, V J Weber, C Haudenschild, S B Gottsman, W A McGovern and T J RyanAcute effects of transluminal angioplasty in three experimental models of atherosclerosis.
Print ISSN: 1079-5642. Online ISSN: 1524-4636 Copyright © 1982 American Heart Association, Inc. All rights reserved.
Avenue, Dallas, TX 75231is published by the American Heart Association, 7272 GreenvilleArteriosclerosis, Thrombosis, and Vascular Biology
doi: 10.1161/01.ATV.2.2.1251982;2:125-133Arterioscler Thromb Vasc Biol.
http://atvb.ahajournals.org/content/2/2/125World Wide Web at:
The online version of this article, along with updated information and services, is located on the
http://atvb.ahajournals.org//subscriptions/
at: is onlineArteriosclerosis, Thrombosis, and Vascular Biology Information about subscribing to Subscriptions:
http://www.lww.com/reprints
Information about reprints can be found online at: Reprints:
document.Permissions and Rights Question and AnswerFurther information about this process is available in theis being requested is located, click Request Permissions in the middle column of the Web page under Services.Clearance Center, not the Editorial Office. Once the online version of the published article for which permission
can be obtained via RightsLink, a service of the CopyrightArteriosclerosis, Thrombosis, and Vascular Biology Requests for permissions to reproduce figures, tables, or portions of articles originally published inPermissions:
by guest on May 7, 2018
http://atvb.ahajournals.org/D
ownloaded from