Embed Size (px)
Citation preview

Acute Iron Intoxication*
A Case Treated by Chelation
G. WHELAN, M.B., V. FAZIO, M.B. and J. C. BIGGS, D.PHIL., M.B.
Sydney, Australia
I RON salts, usually regarded as harmless and of proved therapeutic value in iron de-
ficiency, can lead to death when taken in ex- cessive quantities by young children. Fatal iron poisoning accounts for a significant pro- portion of the deaths in this age group from ac- cidental ingestion of potentially lethal sub- stances.
Aldrich [I] reviewed the literature in 1958 and found that the over-all mortality was 50 per cent in reported cases of iron intoxication. Ferrous sulfate was usually implicated and the fatal doses ranged from 3 to 18 gm. Survival has been reported after ingestion of 15 gm. of ferrous sulfate [Z]. This paper describes survival after the ingestion of 20 gm. of ferrous sulfate by a female child of two years. It seems likely that prompt therapy with an iron-chelating agent (desferrioxamine) was responsible for the favourable outcome.
CASE REPORT
The patient, a girl aged two years, presented in the Casualty Department at 6:30 P.M. on August 27, 1965, after having taken 100 ferrous sulfate tablets-a total of 20 gm. These tablets had been within reach of the chid since about 2:00 P.M. that afternoon.
The mother stated that before admission the chid had vomited a large amount of blood-stained fluid from which 5 tablets were recovered. The diaper contained black watery faeces in which 10 tablets were found. There was no past history of serious disease.
On arrival in the Casualty Department, the child was pale and shocked. The pulse rate was 120 per minute and the systolic blood pressure was 85 mm. Hg. There were no other physical abnormalities.
A nasogastric tube was passed and blood-stained gastric contents were aspirated. As aspiration and lavage were difficult, the tube was withdrawn. Vomit- ing was induced by pharyngeal stimulation and saline drinks, resulting in 200 ml. of blood-stained
gastric contents. At 7:30 P.M. desferrioxamine meth- ane sulfonate (13.5 gm.) was given via a gastric tube and 500 mg. was given intramuscularly. This was followed within 30 minutes by the passage of red, watery diarrhoea and two small haematemeses.
Microscopy revealed numerous red cells but after centrifugation most of the red discolouration was found to be due to ferrioxamine. The iron concentra- tion of this faecal fluid was greater than 75 mg. per 100 ml. (by Ferritest methodt). At this stage 2 more tablets were obtained in the vomitus.
A cannula was inserted into the long saphenous vein and an infusion of 4 per cent dextrose in one-fifth normal saline solution was commenced. Desferriox- amine methane sulfonate, 3 gm., was added to 1 L. of this intravenous fluid, which was adjusted to run at 12 drops per minute. Serum collected at the time contained 1,000 fig. of iron per 100 ml. By 9:00 P.M.
the patient’s general condition had improved and at this stage her pulse rate was 120 per minute and sys- tolic blood pressure 100 mm. Hg. The red, watery diarrhoea persisted in lessening amounts until the following morning.
At 9:30 A.M. on August 28, 1965, the following in- vestigations were performed: serum iron 220 fig. per 100 ml., serum sodium 129 mEq. per L., serum potas- sium 4.2 mEq. per L., Cog-combining power 16 mm. per L., haemoglobin 13.0 gm. per cent. A blood smear showed normochromic and normocytic red cells. The white cells were present in normal numbers and the platelets were adequate.
A roentgenogram of the chest did not demonstrate any abnormalities. Plain x-ray film of the abdomen failed to show the presence of any radiopaque material in the gastrointestinal tract.
Oral administration of fluids was begun at this stage, together with sodium bicarbonate, to combat the acidosis. Intramuscular injection of desferriox- amine methane sulfonate, 250 mg. at 8 hourly inter- vals, was continued.
The patient progressed satisfactorily with no signs
t This is a tablet indicator test for iron under clinical trial by Ciba Corp., Basle, Switzerland.
* From the Department of Medicine, St. Vincent’s Hospital, Sydney, Australia. Manuscript received January 18, 1966.
626 AMERICAN JOURNAL OF MEDICINE
Acute Iron Intoxication- Whelan et al. 627
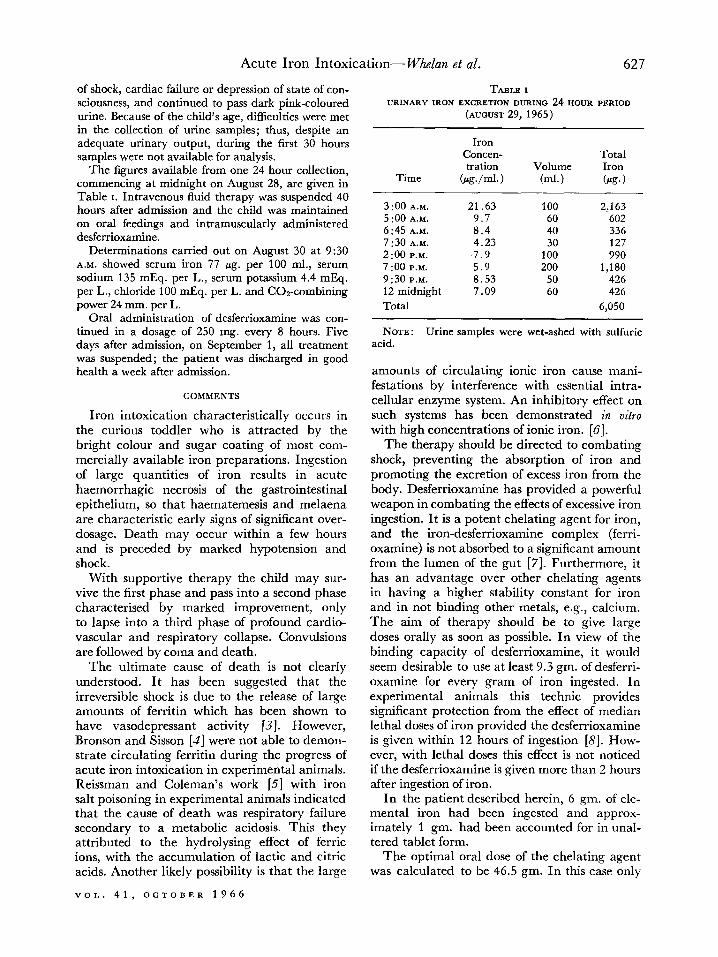
of shock, cardiac failure or depression of state of con- sciousness, and continued to pass dark pink-coloured urine. Because of the child’s age, difficulties were met in the collection of urine samples; thus, despite an adequate urinary output, during the first 30 hours samples were not available for analysis.
The figures available from one 24 hour collection, commencing at midnight on August 28, are given in Table I. Intravenous fluid therapy was suspended 40 hours after admission and the child was maintained on oral feedings and intramuscularly administered desferrioxamine.
Determinations carried out on August 30 at 9:30 A.M. showed serum iron 77 pg. per 100 ml., serum sodium 135 mEq. per L., serum potassium 4.4 mEq. per L., chloride 100 mEq. per L. and Cog-combining power 24 mm. per L.
Oral administration of desferrioxamine was con- tinued in a dosage of 250 mg. every 8 hours. Five days after admission, on September 1, all treatment was suspended; the patient was discharged in good health a week after admission.
COMMENTS
Iron intoxication characteristically occurs in the curious toddler who is attracted by the bright colour and sugar coating of most com- mercially available iron preparations. Ingestion of large quantities of iron results in acute haemorrhagic necrosis of the gastrointestinal epithelium, so that haematemesis and melaena are characteristic early signs of significant over- dosage. Death may occur within a few hours and is preceded by marked hypotension and shock.
With supportive therapy the child may sur- vive the first phase and pass into a second phase characterised by marked improvement, only to lapse into a third phase of profound cardio- vascular and respiratory collapse. Convulsions are followed by coma and death.
The ultimate cause of death is not clearly understood. It has been suggested that the irreversible shock is due to the release of large amounts of ferritin which has been shown to have vasodepressant activity [3]. However, Bronson and Sisson [4] were not able to demon- strate circulating ferritin during the progress of acute iron intoxication in experimental animals. Reissman and Coleman’s work [5] with iron salt poisoning in experimental animals indicated that the cause of death was respiratory failure secondary to a metabolic acidosis. This they attributed to the hydrolysing effect of ferric ions, with the accumulation of lactic and citric acids. Another likely possibility is that the large
VOL. 41, OCTOBER 1966
TABLE I URINARY IRON EXCRETION DURING 24 HOUR PERIOD
(AUGUST 29, 1965)
Time
Iron Concen- tration
&+/ml.) Volume
(ml.)
Total Iron (PP. )
3 :oo A.M. 21.63 100 2,163 5 :00 A.M. 9.7 60 602 6:45 A.M. 8.4 40 336 7:30 A.M. 4.23 30 127 2:oo P.M. 7.9 100 990 7 :oo P.M. 5.9 200 1,180 9:30 P.M. 8.53 50 426 12 midnight 7.09 60 426
Total 6,050
NOTE: Urine samples were wet-ashed with sulfuric acid.
amounts of circulating ionic iron cause mani- festations by interference with essential intra- cellular enzyme system. An inhibitory effect on such systems has been demonstrated in vitro with high concentrations of ionic iron. [6].
The therapy should be directed to combating shock, preventing the absorption of iron and promoting the excretion of excess iron from the body. Desferrioxamine has provided a powerful weapon in combating the effects of excessive iron ingestion. It is a potent chelating agent for iron, and the iron-desferrioxamine complex (ferri- oxamine) is not absorbed to a significant amount from the lumen of the gut [7]. Furthermore, it has an advantage over other chelating agents in having a higher stability constant for iron and in not binding other metals, e.g., calcium. The aim of therapy should be to give large doses orally as soon as possible. In view of the binding capacity of desferrioxamine, it would seem desirable to use at least 9.3 gm. of desferri- oxamine for every gram of iron ingested. In experimental animals this technic provides significant protection from the effect of median lethal doses of iron provided the desferrioxamine is given within 12 hours of ingestion [a]. How- ever, with lethal doses this effect is not noticed if the desferrioxamine is given more than 2 hours after ingestion of iron.
In the patient described herein, 6 gm. of ele- mental iron had been ingested and approx- imately 1 gm. had been accounted for in unal- tered tablet form.
The optimal oral dose of the chelating agent was calculated to be 46.5 gm. In this case only

628 Acute Iron Intoxication-WMzn et al.
13.5 gm. was given as the initial dose orally because further supplies of the drug were not available at the time. Furthermore, we had not previously given such a large dose to so young a child and very much smaller doses had been reported in the literature for the treatment of iron intoxication. On the basis of work with animals it seems unlikely that the large theo- retical requirement (46.5 gm.) would lead to toxic side effects. However, the possibility of such side effects cannot be excluded.
To combat the effects of iron undergoing absorption, desferrioxamine was given paren- terally by the intravenous route in a dose of 300 mg. per kg- body weight, over a 24 hour period. In addition, 500 mg. was given initially (intramuscularly) and 250 mg. repeated at 8 hourly intervals for four days.
If sufficient supplies of this drug had been readily available, oral therapy would have been continued at intervals after the initial dose. In this case the oral therapy was interrupted for 48 hours.
Every case of probable iron poisoning should be regarded as potentially serious and early oral chelation should be instituted.
The initial serum iron level was significantly elevated in this case but not as high as might have been expected in view of the large oral dosage. This may reflect the blocking effect of the oral chelating agent in the absorption of iron; however, the elevation of the serum iron level in such cases does not necessarily reflect the total body content of iron. Even in untreated cases the serum iron levels fall significantly dur- ing the first 36 hours due to the diffusion of iron into the tissues.
The salmon-pink discolouration of the urine and quantitative estimations of urinary iron after parenteral administration of desferriox-
amine are probably the best indices of iron over- load in such patients.
SUMMARY
A description has been given of a two year old child who ingested an ordinarily fatal dose of ferrous sulfate (20 gm.). The early oral and parenteral administration of desferrioxamine undoubtedly had a favourable influence on the ultimate outcome, which was early and com- plete recovery.
ADDENDUM
The same child was readmitted to the Cas- ualty Department on October 22, 1965, after the ingestion of 20 ml. of turpentine. Gastric lavage was carried out and there were no se- quelae.
REFERENCES
1. ALDRICH, R. A. Acute iron toxicity. In: Iron in Clinical Medicine, p. 93. Edited by Wallerstein, R. 0. and Mettier, S. R. Berkeley, California, 1958. University of California Press.
2. SPENCER, 1: 0. B. Ferrous sulphate poisoning in children. &it. M. J.. 2: 1112. 1951.
3. MAZIJR, A. and GO& E. Hepatorenal factors in circulating homeostasis. IX. The identification of the hepat& vasodepressor substance, VDM, with ferritin. J. Biol. C&-m.. 176: 771. 1948.
4. BRONSON, W. R. and S&ON, T. R. C. Studies on acute iron poisoning. Am. J. Dis. Child., 99: 18, 1960.
5. REISSMAN, K. R. and COLEMAN, T. J. Acute intes- tinal iron intoxication. II. Metabolic, respiratory and circulating effects of absorbed iron salts. Blood, 10: 46, 1955.
6. RACKER, E. and KRIMSKY, I. Inhibition of coupled phosphorylation in brain homogenates by ferrous sulphate. J. Biol. Chum., 173 : 519, 1948.
7. HWANG, Y.-F. and BROWN, E. B. Effect of desferriox- amine on iron absorption. Lancet, 1: 135, 1965.
8. MOESCHLIN, S. and SCHNIDER, U. Treatment of pri- mary and secondary haemochromatosis and acute iron. poisoning with. a new potent iron-eliminating agent (desferrioxamine-B). New En&nd J. Med., 269: 57, 1963.
AMERICAN JOURNAL OF MEDICINE