Embed Size (px)
Citation preview

Manual Therapy (2001) 6(2), 106-115© 2001 Harcourt Publishers Ltddoi:10.1054/math.2000.0386, available online at http://www.idealibrary.com on
Clinical commentry
Acute low cervical nerve root conditions: symptom presentationsand pathobiological reasoning
L. Gifford
SUMMARY. Acute low cervical nerve root conditions may be easily misdiagnosed. The perspective presented isthat their symptom presentation is not as straightforward as the classic descriptions of brachialgia would have usbelieve. This clinical commentary presents a series of observations and reasoning models that are relevant to patientsymptom presentations believed to be of cervical nerve root origin. Clinicians are urged to consider low cervicalnerve root assessment in the light of our current understanding of neural sensitivity, pain science, nerve rootbiomechanics and the presence and effect of degenerative changes. This particularly relates to thoughts aboutcervical movements and postures being able to bring forces to bear on nerve roots via compressive as well aselongation forces. © 2001 Harcourt Publishers Ltd.
'False facts are highly injurious to the progress of science forthey often endure long; but false hypotheses do little harm,as everyone takes a salutary pleasure in proving thefalseness; and when this is done, one path toward error isclosed and the road to truth is often at the same timeopened'. Charles Darwin. (In Ramachandran & Blakeslee1998 pxvi).
accepted that the material is speculative and can bechallenged, being based on carefully recorded patientreport and clinical observation and interpretation.There is plenty of scope for the observationsdescribed to be more robustly recorded and testedin an unbiased setting.
INTRODUCTION
Nerve root disorders are often difficult to evaluateand may be misdiagnosed or go unrecognised. Theearly part of this clinical commentary urges practi-tioners to consider much of the recent work on thepathophysiological mechanisms relating to peripheralnerve related pain. The second part presents adescriptive analysis of the common features of patientpain presentations which are believed to have theirorigins in low cervical nerve roots. It is intended thatclinicians may find the material useful during historytaking and the clinical reasoning of aches and painsin the neck/shoulder and upper limb regions. Muchof the material presented can be used in anappropriately modified form to help educate patientswith acute and subacute cervical nerve root problems.
The clinical descriptions relate to acute nerve rootdisorders - here defined as the first 6-12 weeks. It is
Louis Gifford, MAppSc, BSc, MCSP, SRP, Kestrel,Swanpool, Falmouth, Cornwall TR11 5BD UK.Tel: +4401326312156; Fax:+4401326211149;E-mail: [email protected];Web: www.achesandpainsonKne.com
THE SPECTRUM OF CLINICALPRESENTATIONS
It is proposed that many conditions exist on a clinicalcontinuum, or spectrum, that range from the full-blown and blatantly obvious to the more obscure andharder to detect. It is as if these obscure and oftenminor problems have one or two components offamiliarity about them but do not have the fullcompliment of features necessary to make a confidentclinical diagnosis. Maitland (1986) used the term'subclinical presentation'. Three examples that repre-sent the extremes of the nerve root clinical spectrumfollow:
1. Diagnosis — 'trapped nerve'
'I've got pain from my neck down the arm, it'sconstant agony, there's numbness and pins andneedles in the thumb and first finger, I think I'vetrapped a nerve in my neck' (even the patient has areasonable concept of the problem). Whenexamined, neck movements clearly influence
106

Manual Therapy (2001) 6(2), 106-115© 2001 Harcourt Publishers Ltddoi:10.1054/math.2000.0386, available online at http://www.idealibrary.com on
Clinical commentry
Acute low cervical nerve root conditions: symptom presentationsand pathobiological reasoning
L. Gifford
ft
SUMMARY. Acute low cervical nerve root conditions may be easily misdiagnosed. The perspective presented isthat their symptom presentation is not as straightforward as the classic descriptions of brachialgia would have usbelieve. This clinical commentary presents a series of observations and reasoning models that are relevant to patientsymptom presentations believed to be of cervical nerve root origin. Clinicians are urged to consider low cervicalnerve root assessment in the light of our current understanding of neural sensitivity, pain science, nerve rootbiomechanics and the presence and effect of degenerative changes. This particularly relates to thoughts aboutcervical movements and postures being able to bring forces to bear on nerve roots via compressive as well aselongation forces. © 2001 Harcourt Publishers Ltd.
'False facts are highly injurious to the progress of science forthey often endure long; but false hypotheses do little harm,as everyone takes a salutary pleasure in proving thefalseness; and when this is done, one path toward error isclosed and the road to truth is often at the same timeopened'. Charles Darwin. (In Ramachandran & Blakeslee1998 pxvi).
accepted that the material is speculative and can bechallenged, being based on carefully recorded patientreport and clinical observation and interpretation.There is plenty of scope for the observationsdescribed to be more robustly recorded and testedin an unbiased setting.
INTRODUCTION
Nerve root disorders are often difficult to evaluateand may be misdiagnosed or go unrecognised. Theearly part of this clinical commentary urges practi-tioners to consider much of the recent work on thepathophysiological mechanisms relating to peripheralnerve related pain. The second part presents adescriptive analysis of the common features of patientpain presentations which are believed to have theirorigins in low cervical nerve roots. It is intended thatclinicians may find the material useful during historytaking and the clinical reasoning of aches and painsin the neck/shoulder and upper limb regions. Muchof the material presented can be used in anappropriately modified form to help educate patientswith acute and subacute cervical nerve root problems.
The clinical descriptions relate to acute nerve rootdisorders - here defined as the first 6—12 weeks. It is
Louis Gifford, MAppSc, BSc, MCSP, SRP, Kestrel,Swanpool, Falmouth, Cornwall TR11 5BD UK.Tel: +4401326312156; Fax:+4401326211149;E-mail: [email protected];Web: www.achesandpainsonline.com
THE SPECTRUM OF CLINICALPRESENTATIONS
It is proposed that many conditions exist on a clinicalcontinuum, or spectrum, that range from the full-blown and blatantly obvious to the more obscure andharder to detect. It is as if these obscure and oftenminor problems have one or two components offamiliarity about them but do not have the fullcompliment of features necessary to make a confidentclinical diagnosis. Maitland (1986) used the term'subclinical presentation'. Three examples that repre-sent the extremes of the nerve root clinical spectrumfollow:
1. Diagnosis - 'trapped nerve'
Tve got pain from my neck down the arm, it'sconstant agony, there's numbness and pins andneedles in the thumb and first finger, I think I'vetrapped a nerve in my neck' (even the patient has areasonable concept of the problem). Whenexamined, neck movements clearly influence
106

Acute low cervical nerve root conditions 107
symptoms and loss of reflex and segmentallyrelated muscle strength are easy to detect.
2. Diagnosis - 'Sprained shoulder muscles'A 43 year old patient presents with a 10-day historyof vague right shoulder aching pain following aseries of vigorous tennis matches over several days.He has normal full range of neck movement andsome shoulder movements produce inconsistentsharp pains radiating from the shoulder downinto biceps. For the patient, the focus isunderstandably on the shoulder and reinforcedwhen the clinician finds positive pain responses totests that mechanically load shoulder tissues.
On closer questioning it is revealed that thepatient has had vague ('of no consequence')feelings of heaviness in the arm that last about30 sec when rising in the morning and briefsharp pains around the medial border ofscapula that he has noticed on and off forthe last 3-4 months. Vague, but rare, arm pinsand needles are also noted. Closer physicalexamination reveals a markedly reduced tricepsreflex and exacerbation of the shoulder achewhen the neck is rotated to the right and gentleright side flexion added and sustained for10-15 seconds. By 15 seconds arm paraesthesiabecomes evident. Sustained gentle pressure overthe ipsilateral C6 nerve root anteriorly on themedial aspect of the transverse process of C6increases the shoulder ache and reproduces fleetingsharp scapula pains similar to those mentioned.
3. Other Diagnoses- 'supraspinatus tendinitis' for shoulder pain
with positive static muscle tests,— 'sprained rib muscle' for medial scapula pain— 'carpal tunnel syndrome' if hand pins and
needles only— 'epicondylitis' if pain in the forearm
Closer scrutiny often reveals an atypical presentationfor the given diagnosis. For example a carpal tunnel.diagnosis where the patient reports paraesthesia inthe whole arm as well as the hand.
At this 'low' end of spectrum it is not uncommonfor patients to report symptom distributions andbehaviours that show no detectable clinical evidenceof loss of conduction but which are similar to othercases that do show such losses. Example^ above witha less dominant pain state and without any para-esthesia or loss of reflex would be a good example.Thus, the only way a component of nerve rootinvolvement can be suspected is via a balancedanalysis of physical tests that rely on symptomresponse and the fact that similar pain distributionsand pain behaviours are often associated withdetectable conduction losses in other patients. Suspi-cion of nerve root culpability is further strengthened
when the patient suffers later episodes with similarpains that do reveal conduction abnormalities. It isnot uncommon for conditions like those listed aboveto develop into a classic nerve root problem.
NERVE INJURY AND SENSITIVITY
Normal nerve roots are generally considered to bemechanically insensitive with the exception of thedorsal root ganglion area (Howe et al. 1977; Kuslichet al. 1991). However, nerve fibre axons (Devor &Seltzer 1999) and nerve fibre terminals withinperipheral nerve sheaths (Bove & Light 1997) mayupregulate their sensitivity in response to changes intheir local environment. This may be a result of directmechanical insults, changes in circulatory perfusionor the inward diffusion of irritative inflammatorychemicals from damaged or disordered adjacent softtissues like the disc and facet joints (Olmarker et al.1993, Byrod et al. 1995; Clatworthy et al. 1995;Tracey & Walker 1995).
It is feasible for nerve roots to be physically injuredby extreme spinal movements, or by less extrememovements in the presence of degenerative changesthat compromise the normal foraminal or spinalcanal dimensions. Hence, disc protrusions and extru-sions, vertebral approximation, osteophytes, facetenlargements, synovial cysts, and enlarged osteoliga-mentous structures like the uncovertebral joints,may all play a part in increasing the vulnerability ofnerve roots to adverse postural or movement relatedforces. From studies of the lumbar spine it is clearthat the likelihood of roots being mechanicallycompromised by normal end range movementsincreases with increasing degenerative change (Pen-ning & Wilmink 1981; Penning 1992). In two neckcadaver studies, extension and ipsilateral rotationwere found to be the most root compromisingmovements (Yoo et al. 1992; Farmer & Wisneski1994). Clinicians are urged to consider injuring forcesin relation to movements that tend to compress orelongate nerve roots.
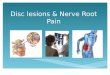
Nerve roots may become sensitised by changes incirculatory perfusion. Anything that diminishes space 'in the foramen is likely to alter normal circulatorypressure gradients and hence the normal circulatoryflow through the nerve root. Space occupyingmaterial may be transient, e.g. oedema or extrudeddisc material (Maigne & Deligne 1994), or morepermanent, e.g. osteophytes. Significant sensitisingof the nerve may be achieved via compression offoraminal venous plexi, which as a result produces aback pressure and circulatory stasis within the nerve(e.g. Olmarker et al. 1989). Ongoing circulatory stasismay lead to ischaemia and the potential forintraneural oedema, inflammation and fibrosis (re-viewed in Butler 1991; Gifford 1997a) (see Fig. 1).
2001 Harcourt Publishers Ltd Manual Therapy (2001) 6(2), 106-115

108 Manual Therapy
Mechanical factors(may be slow or fast)
Compression of....
Relatively insensitiveimmediately?
Local vascular system-particularlythe extradural and nerve root venous
plexi.
But, if enough force/damage, signsof altered conduction occur, e.g. diminishedreflexes, paraesthesia, numbness, weakness
Immediate response
Antigenic /irritativesubstances
e.g. leaked nuclear material from disc
Alteration in intraneural physiologye.g. oedema, inflammation, fibrosis, nerve fibre damage and dysfunction and
the development of ectopic impulse generating sites.
Pain/symptoms?
Fig. 1—Mechanisms of root injury that can lead to symptoms.
The potential for circulatory distress to cause nervefibre injury, degeneration and upregulation of sensi-tivity is evident. This knowledge highlights the likelydetrimental effects of prolonged immobility, espe-cially in postures that compress or elongate the nerveroots. It also draws attention to the fact that directphysical compression of a nerve root is not necessaryfor it to be injured and alter its sensitivity state. Thus,discs do not necessarily have to directly pinch orcompress nerve tissue to produce pathologicalchanges or sensitivity changes to the nerve.
Recent revelations about the capacity of axonsto become pathophysiologically sensitised and activeself-generators of impulses, goes a long way to helpexplain the way in which pain behaves clinically.Injured or degenerate/regenerating axons withinnerve trunks or nerve roots can become sitesdemonstrating enhanced sensitivity as well as sourcesof ongoing and self-sustaining barrages of impulsesthat have the potential to cause long lasting and highintensity pains (Wall & Devor 1983, Devor & Seltzer1999). These zones of abnormal impulse generationon axons are referred to as ectopic impulse generatingsites (Devor 1996, Devor & Seltzer 1999), sinceimpulses are normally generated at nerve fibreterminals.
Clinically, it may be worth analysing sensitivitystates in the following ways (see Gifford 1997a & b):
• Increased mechanosensitivity. Here pressure and/or stretch on a nerve produces immediatesymptoms (Devor & Seltzer 1999). Clinically, thismeans a more or less instantaneous increase insymptoms when nerves are either elongated — thinkof movements 'away from side of pain andcomponents of neural tension/neurodynamic test-ing; or, when nerves are compressed - think ofmanoeuvres that tend to compress nerve, likecervical extension and movements towards thepainful side. Note however that ectopic impulsegenerating sites may not always react in parallelwith changes in the force applied to them (Devor& Seltzer 1999). Clinically, this may translate intosudden bursts of pain which instantly go, even ifthe pressure of the test is maintained or a testmovement repeated, or symptoms continuing onafter the stimulus is removed.
• Increased ischaemosensitivity (Gifford 1997b).Here, reasoning suggests that sustained com-pression or stretch of a nerve will compromiseneural circulatory perfusion leading to ischaemia.Ischaemia, for example, via a lowering in local pH
Manual Therapy (2001) 6(2), 106-115 2001 Harcourt Publishers Ltd

Acute low cervical nerve root conditions 109
(Issberner et al. 1996; Steen et al. 1996), may thengive rise to a steadily increasing barrage ofimpulses from an ectopic impulse generating site,or sensitised region of nerve. A common exampleis the progressive increase in distal paraesthesiaprovoked by holding the elbow in a flexed position,or crossing the legs for a long time. A nervedemonstrating clinical ischaemosensitivity woulddevelop symptoms over time, but far more quicklyand intensely than normal. Phalens' test for carpaltunnel syndrome is a classic example where theonset of symptoms in the wrist flexion positionmay take only a few seconds to come on and thensteadily builds up (see Durkan 1991). The sametype of response is obtained in many acute nerveroot disorders when test positions are sustained(see example 2 above).
• Increased adrenosensitivity. Sensitised nociceptors,dorsal horn cells and ectopic impulse generatingsites on axons have all been shown to be capableof becoming sensitive to adrenaline and noradr-enaline (Koltzenburg 1996; Devor & Seltzer 1999).This is thought to be the principle pathophysio-logical mechanism that underpins sympatheticallymaintained pain precipitated by nerve injury(overviewed in Janig & Stanton-Hicks 1996;Gifford 1997b; Gifford & Butler 1997; Gifford1998c; Devor & Seltzer 1999; Scadding 1999).Clinically this link of adrenaline-like substances toincreases in neural impulse generation helps turnour attention towards the potential influences ofanxiety and stress, via a peripheral mechanism, onthe behaviour of pain.
As noted above, ectopic generating sites can, oftheir own accord, generate ongoing or intermittentbarrages of impulses spontaneously - when they aretermed 'ectopic pacemaker sites'. Clinically this mayrepresent ongoing pain which waxes and wanes forno apparent reason or pain that mysteriously appearsand disappears. Both are very common scenarios foracute nerve root pains and a source of much concernfor the mystified patient.
Ectopic impulse generating sites are also knownto be capable of becoming sensitive to many chemicalmediators that includes inflammatory chemicals(Devor & Seltzer 1994; 1996; 1999). An injured nerveroot that contains nerve fibres which have developedectopic impulse generating capability may well besurrounded by inflammatory chemicals derived fromnearby tissues that have been injured or arepathological. The inflammatogenic potential of nu-clear fluid that has leaked out of the disc via radialfissures is a useful example (e.g. McCarron et al.1987; Olmarker et al. 1995; Saal 1995). Inflammatorychemicals that derive from adjacent pathological orinjured soft tissues may not only play a part in givingrise to ectopic impulse generators but may also be
involved in stimulating and maintaining their activ-ity. A major consideration is that pain behaviour isnot necessarily mechanically patterned and the causeof the pain may not always be the result of directmechanical insult.
In summary, this section highlights the need forclinicians to integrate known neural pathophysiologyinto reasoning in order to better explain the variablenature of peripheral nerve related pain behaviour.Relying solely on mechanical explanations to explainpain and its behaviour are likely to be inadequate.Inflammatory/metabolic sensitivity, ischaemosensi-tivity, adrenosensitivity plus central and higher centreprocessing also need to be considered.
SYMPTOM PRESENTATION
1. Distribution of symptoms
Even in a classic nerve root disorder, symptoms areusually distributed in a vague way - not in neatdermatoma patterns and packages that most litera-ture on nerve root pain would have us believe. Thepatient usually indicates the area of symptoms in ageneral and imprecise way. The very nature of thepain is often one of being hard for the patient toaccurately localise. It is pleasing for clinical realitythat non-dermatomal and widespread distributions ofsymptoms have now been quantified by direct rootstimulation in patients with cervical radicular pain(Slipman et al. 1998).
In acute low cervical root irritation, common areasof distribution are: the lower neck spreading laterallytowards the point of the shoulder; the medial border ofscapula; the whole of the scapula; the anterior neck tothe upper pectoral area; down the back or front of thearm (the patient often grips the triceps/biceps toindicate the pain area); the lateral or medial forearmand into the hand. Symptoms are often more intense atparticular sites and these are not necessarily proximal.For example, deep forearm ache that is particularlyintense over the lateral elbow. It is not uncommon forsome patients to use the term tennis elbow to helpdescribe their symptoms. Another common area ofintense pain is located deeply along the medial borderof the scapula, or over the upper scapula area.
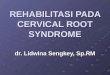
Importantly, the area of symptom distribution isvery variable, can be very patchy and is often hard tolocalise to a particular nerve root distribution (e.g.Fig. 2). When a patient describes their symptoms, it isimportant to be content with what is described andworry less about a textbook dermatome or preciseroot level that one might wish the pain to fit. A reviewof Slipman et al. (1998) confirms this.
Other areas of symptoms that further challengedermatomal pattern thinking include:
• Patients with C6 or C7 nerve root deficit havingpain in the axilla area frequently radiating down
2001 Harcourt Publishers Ltd Manual Therapy (2001) 6(2), 106-115

110 Manual Therapy
Constantbut variable Constant, intense
'toothache', deep.comes in waves
of pain
Vague pins & needlescomes/goes whole hand
Constant deepaching
Fig. 2—-Body chart of a 41 year old female policewomen. Three week history of pain in distribution shown. Diagnosed as having shoulderstrain and tennis elbow. No recollection of an injuring incident and no previous history of neck, shoulder or arm pain. One key physicalfinding was that she had a significantly reduced triceps reflex and grade 4 triceps power. She had significant forward head posture.
onto the lateral chest wall and medial upper arm.Many patients report symptoms spreadinganteriorly into the pectoral/breast area
• Axillary pain with acute low cervical nerve rootsseems very common
• Symptoms may also be reported in the anteriorneck, clavicular and pectoral area.
At the lower end of the spectrum, symptoms maybe found in any one of the above areas — alone, or incombination, and may have no symptoms at allanywhere near the neck (Fig. 2). Frequent descrip-tions include: deep intermittent aching in the bicepsor triceps region and occasional sharp shooting painsin the lateral forearm; an annoying localised burningpain or itch in a small area along the medial scapulaborder that keeps the subject awake at nightaccompanied by a disturbing heaviness and tirednessof the ipsilateral arm during the day.
Symptoms of paraesthesia may fit more consis-tently into dermatomal patterns, though frequentlydo .not (Fig. 2). Thus patients may report paraesthe-sia of the whole arm in vague patterns, or from theelbow to the hand with difficulty in describing theboundaries of its distribution. Alternatively, para-esthesia may be described in a single fingertip or oneor two fingers that are typical of the relevantdermatome. Caution is strongly advised when allot-ting a specific root-level based on paraesthesia oranaesthesia location alone. For example, it seems
common to find that a patient will complain ofnumbness/pins and needles in the thumb (classically,C6) yet be found to have a weak triceps and/ordiminished triceps reflex (C7).
The important point is that symptoms rarely fitinto neat dermatome distributions and are frequentlyin isolated areas well away from the nerve root andneck region.
2. Symptom quality
Symptom quality and behaviour may be a keydefining feature of pain that has neurogenic origins.Well known authorities on the spine insist that nerveroot pain is sharp and shooting in quality and welllocalized (Bogduk 1997; Waddell 1998). Time andagain, this does not seem to fit with the everydayclinical reality observed. Even classic 'objectivelyproven' severe acute cervical and lumbar nerve rootpresentations invariably describe their pain as anunremitting intense tooth-ache like pain. The paincan be ghastly, unrelenting and extremely wearing,even for the most stoical and uncomplaining ofpeople. Patients are desperate for help. Most patientswould do anything, take anything or have anythingdone to them to get pain relief.
Sharp shooting pains do occur, but seem to bemore common in elderly patients. Symptoms maybe 'sharp shooting' or more commonly 'knife in' or
Manual Therapy (2001) 6(2), 106-115 2001 Harcourt Publishers Ltd

Acute low cervical nerve root conditions 111
'gripping' pains, anywhere from the neck across theshoulders to down the arm. Sharp shooting pain maymanifest on its own without any ache. Like aching,the shooting pain can be ghastly, the patientclutching the area of pain and strongly wincing formany seconds until the 'after' pain gradually sub-sides. It often occurs for no apparent physical reason,hence shooting pains at rest, whatever the position,or occurring one moment with a neck movement, thenext with an arm movement. Patients are under-standably worried, even frightened by these intenseand mysterious pains. It is very easy to see whypatients often view their condition in terms of seriouspathology.
Symptoms are occasionally more bizarre. Forexample, feelings of crawling, trickling and some-times extremely uncomfortable 'gripping' sensations.A very common description of the arm is that it feels'heavy', 'leaden' or 'tired and useless' a lot of thetime. 'The kind of feeling you get when youcontinuously overwork a muscle' is a commondescription. At the less intense lower end of thespectrum words like 'annoying', 'distracting' and'irritating' are used.
While these descriptive terms are not difficult tofathom, what is, is the difficulty the patient often hasin tying the symptoms to particular things that theyhave done. An appreciation of ectopic impulsegenerating sites' capacity to develop sudden, sponta-neous or ongoing activity or be influenced by non-mechanical stimuli, helps in the understanding andexplanation of many of these types of phenomenon.
3. Symptom behaviour
Time: 24 hour behaviourAcute nerve root symptoms may be constant andunrelenting 24 hours a day, with the result that thepatient gets very little useful rest or sleep. Manypatients report pain far worse at night and yet thatthey can manage during the day when on the move ordistracted by their daily tasks. Pain at night is viewedas a marker of serious pathology and this mustalways be considered (CSAG 1994; RCGP 1996;Roberts 2000).
Less severe nerve root presentations show hugevariability over 24 hours having no particular timerelated pattern from one day to the next. However,many do report having wakeful nights. Nightsymptoms are a common feature of many peripheralneurogenic disorders, recall the persistent nightsymptoms associated with carpal tunnel syndrome.
As nerve root syndromes recover they can oftenease up significantly for a day or two, with the patientgreatly relieved, but then return with former severity,adding much to the patient's concern. It is worthwarning the patient of this likelihood so that
they know what to expect. Improvement ofteninvolves lurching from good periods to bad, but astime goes on the flare-up times get shorter and lessintense.
Symptom behaviour related to posture and movementsPatients with intense acute nerve root pains rarelyfind consistent positions of relief and if they do it isonly for a brief period of time. A key feature is thatthe patient becomes physically restless with the painand greatly appreciates an understanding of thisproblem. 'The doctor told me to take paracetomoland lie down and rest for 10 days'... 'The lastphysiotherapist insisted I sat up straight and kept myneck in perfect posture. I'm sorry I just can't keep itup, at first its better for a short time then I have tomove and get relief by bending my neck forward' -are frequent comments from patients.
Acute low cervical nerve root disorders may findshort term relief in the following ways:• Arm overhead - relief usually lasts for short
periods. Patients may be forced into this positionfrequently if they have to sit for long periods - forexample, driving the car with one hand on thewheel while the affected arm is raised with the handresting on the head. This has been called the'shoulder abduction relief sign' (Davidson et al.1981; Beatty et al. 1987; Fast et al. 1989) and hasbeen shown to significantly reduce intraforaminalpressures on the C5, C6 and C7 nerve roots in freshcadavers (Farmer & Wisneski 1994). Themechanisms these authors proposed for this are:First, the shoulder abduction may cause theintervertebral foramen to enlarge thereforereducing pressure on the sensitised nerve root (Ifyou do this your head tends to flex forwardslightly).
Second, the abducted position reduces thetension on the nerve root. While this can bechallenged by concepts of neurodynamics that usearm abduction to add neural tension, it should beappreciated that normal arm abduction allows thescapula to elevate and rotate towards the spine.Hence, the coracoid process may move severalcentimetres closer to the neck thus allowingconsiderable slack into the brachial plexus areaand nerve roots (Davidson et al. 1981). Allstandard upper limb tension tests (ULTTs) eitherprevent the scapular elevation occurring or add inscapular depression before the arm abductioncomponent is added (e.g. Butler 1991; Elvey 1994;Elvey & Hall 1997).
From this one would expect the patient to gainrelief from sustained shoulder shrugging or sittingwith plenty of pillow support along the forearm sothat the whole arm/scapular unit is raised intoelevation. Surprisingly, this does not always occursuggesting that either scapular rotation is needed as
2007 Harcourt Publishers Ltd Manual Therapy (2001) 6(2), 106-115

well, or, relief by reducing root tension or pressureis only one possible explanation behind the'shoulder abduction relief position.
• Postures and movements into flexion and awayfrom the side of pain. In a similar way to lumbarnerve root conditions, many patients with classicacute cervical nerve root disorders adopt posturesthat flex slightly and deviate away from the side ofpain. Moving towards the side of pain or intoextension is often very provocative if the nerve is inan extremely mechanosensitive state. This clinicalfinding fits with knowledge that the intervertebralforamina of the low cervical roots enlarge in flexionand movements away from the side of pain anddiminish in extension or movements towards thesymptomatic side (Ehni et al. 1990; Yoo et al.1992). Thus, movements that decrease the size ofthe foramen tend to compress and increasepressure on the roots, and movements thatincrease the foramen size tend to decreasepressure on the root (see Farmer & Wisneski1994). Interestingly, Farmer and Wisneski (1994)noted unpredictable results in their pressure changeobservations in cervical flexion. For example, C5and C7 roots demonstrated modest increases inpressure in flexion and C6 showed modestdecreases in pressure. It appears that the actualpressure exerted on the nerve root is not whollydependent on changes in foramina! sizes in flexionpositions. Proximal and distal tethering effects byvariable intraspinal and extraspinal ligamentousstructures that may tether the roots (Moses &Carman 1996); movements of dura relative to theoften angulated course of nerve roots within thespinal canal (Nathan & Feuerstein 1970); posturaleffects on circulatory supply, and the position ofthe shoulder complex and arm are the sorts ofissues that need to be considered too. Whatever thebiomechanical findings from these few cadaverstudies, in the clinic it is very common to findpatients getting relief by adopting varying anglesof, and sometimes extreme, neck flexion. It may bethat there is far more significant reduction of rootcompression in flexion in the presence of localswelling, or a disc bulge, herniation or frankprotrusion.
Many patients find that the only position that theycan get comfortable enough to get to sleep in is bylying supine and having 2 or 3 pillows wedgedbehind the neck to maintain end of range flexion.While this goes against many principles ofphysiotherapy management it can be seen as avery adaptive 'nerve saving/pain relieving' positionto adopt during the early very acute phase of thedisorder. Rapid progression to restore normalposture and range may exacerbate or maintainpain (and possibly increase neural damage/
sensitivity too) for longer than it otherwise wouldif left to 'natural', well ingrained reflex antalgicpostures that have survived the test of time.Ubiquitous antalgic postures seem to havebiological wisdom that should really dictate agraduated recovery of range and posture approachto management.
• Postures and movements towards the side of pain.It seems that there are a small percentage ofpatients with cervical nerve root disorders whoobtain relief by adopting postures deviatingtowards the side of pain. Although this appearsincompatible with thoughts of foraminalcompression it may be that some relief in roottension is achieved. In keeping with this is theclinical finding that the majority of those patientswho prefer deviation towards the side of pain tendto have very clear-cut responses to neurodynamictesting. In these cases, the neural tissue appearsto be more sensitive to stretch/elongation thanto compression. Arm postures that can beassociated include scapular elevation and the armheld into the side with the elbow flexed across theabdomen.
Patients with less obvious or more minor rootproblems often have great difficulty in identifying anyclear relieving postures or movements. Considerationof factors mentioned earlier relating to the activity ofectopic impulse-generating sites and the ischaemo-sensitivity model for delayed onset symptoms mayhelp make sense of the presentation and direct thetype of examination testing. In desperation patientsmay find quite odd positions for relief. Examplesfrom the authors patient population include: on allfours dangling the head down; a yoga shoulder stand;extreme cervical extension in prone and wedging thehead in side flexion away.
If all else fails for the patient, the most commonmethods of relief come down to protective use of thepart where the pain is felt, something which maydraw clinical attention away from proximal oftennon-symptomatic areas and towards the hurtingtissues as the primary source of the pain mechanism.It is important to bear in mind that mechanical effectson nerve roots can be altered by arm postures. Thusa patient may well find several arm postures thatprovide a degree of relief.
Even in some classic nerve root conditions, patientsmay not associate dominant distal symptoms withneck postures and movements. It is quite common tofind patients having quite normal and free neckmovements but considerable distal 'radicular' pain. Itoften takes a good examination and explanation toconvince the patient that the primary site of paingeneration is proximal and related to enhancedneural sensitivity where the nerves enter and leavethe vertebrae of the neck.
Manual Therapy (2001) 6(2), 106-115 2001 Harcourt Publishers Ltd

Acute low cervical nerve root conditions 113
The following postures and movements are fre-quently found to exacerbate the symptoms of acutecervical nerve root disorders:
• Looking up and extending the neck, sustainedpostures involving extension, repeated cervicalretraction exercises, and movements towards thepainful side.One of the most consistent aspects of acute lowcervical root syndromes is the production andprovocation of symptoms with cervical extensionmovements, exercises and postures. This clearly fitswith the decrease in foraminal dimensions reportedearlier. The presence of extruded or bulging disctissue, or any space occupying tissue or materialwill obviously enhance this effect. Clinicians needto bear in mind the age of the patient, the likelydegenerate encroachment and the actual mobilityof the low cervical segments. Loss of range of lowcervical joints may account for a dispropor-tionately low level of symptom provocation withstandard neck movements in the elderly 'stiff-necked' patient - it may be that the motionsegments just do not move enough to have anyimmediate physical impact on the sensitised nerveroots they contain.Patients often report provocation of symptomswhen performing activities like shaving, lyingsupine in bed with a single pillow, lying pronewith the head in full ipsilateral rotation, swimmingwith the head up and hair washing in neckextension under a shower. Analysis often revealssignificant and often sustained low cervicalextension and that minor alterations of posturequickly or slowly change symptoms.
All positions and activities that patients volunteeras being provocative are worth analysing withthoughts of neural compression or neural elongationeffects. For instance, patients often report being ableto lie comfortably on one side but not on the other.Analysis of the number of pillows used combinedwith thoughts about compression/elongation can beuseful. Thus a right-sided nerve root problem thatis mainly provoked by root compression postures/movements tends to be more comfortable lying on theright side if the pillows are sufficient to side flex thehead to the left. When the patient turns onto their leftside, with the same number of pillows, the neck side-flexes towards the right, compresses the roots andhence tends to exacerbate the symptoms. Patientsoften find it odd that they are more comfortable lyingon the painful side rather than off it. This type of'mechanically-based' thinking can help explain theapparent paradox.
Clinicians are urged to be aware that nerves mayrespond in a delayed manner to insult or injury(Devor 1994; Devor et al. 1994; Devor & Seltzer1999) and that this may well be from examination or
therapeutic movements. Relying on pain response tomechanical testing like repeated movements mayreduce or change the location of symptoms at thetime but cause significant flare-up or worsening in thehours or days that follow. Personal experience of thisdelayed flare-up is so frequent that any repeatedmovements are prescribed with considerable caution.Movements that tend to compress nerve roots, likerepeated extension or side flexion/rotation/side glid-ing towards the painful side appear to be mostprovocative.
• Movements away from painful sideThis response fits with the cluster of patients whopresent with symptoms relieved by posturestowards the painful side and who have positiveneural tension/neurodynamic tests, i.e. 'neuralelongation' root sensitivity.
• Flexing the neckWhile many patients report relief in flexion, if themovement is taken towards the limit of range,symptoms may be further provoked. End-rangeflexion occasionally provokes distal/arm symptomsbut more commonly produces local neck and yoke-area related discomfort. A small proportion ofpresentations have all symptoms severely broughton in flexion - these patients are usually extremelylimited in most cervical movements.
• Arm movementsPatients with arm pain of root origin frequentlyreport difficulties using the arm. Closer scrutinyusually reveals a very variable stimulus responserelationship. Again, analysis should bear in mindneck posture and the effects of arm/shoulder/scapula posture on neural tension/elongation.Increased pain as a result of carrying shoppingcan be interpreted in terms of increased neuraltension on the hyperalgesic roots. Positive painresponses to distal joint and muscle testing mayreflect a secondary hyperalgesic state rather thanany localised primary lesion (see below but also seeHasue 1993).
OTHER FACTORS TO CONSIDER
Clinicians should be far more aware that barrages ofimpulses arising from ectopic generating sites onperipheral nerves or as a result of nociceptor activityfollowing tissue injury will cause changes in thecentral nervous system processing of normal sensoryinput from normal tissues (reviewed in Zusman 1992;Gifford 1997b; Johnson 1997; Gifford 1998a; Wright1999). Barrages from ectopic impulse generating siteson sensory axons and cell bodies in peripheral nervescan be particularly unpleasant. Central nervoussystem changes result in the phenomenon of second-ary hyperalgesia whereby normal inputs from normal
2001 Harcourt Publishers Ltd Manual Therapy (2001) 6(, 106-115

114 Manual Therapy
tissues get processed in the central nervous systemin terms of pain, rather than innocuous sensations.The clinical significance of this is that many tissuesthat produce pain when physically tested by manualtechniques using physiological movements, staticmuscle tests or palpatory pressures may be relativelynormal. Thus, the central consequences of tissue/peripheral nerve injury may easily result in 'false'positive findings in examined peripheral muscles,nerves, joints, skin and any other soft tissues in areassegmentally related to the nerve, and in extreme/severecases, tissues well beyond normal segmental limits.Physically testing or pressing on a particular structureand reproducing the pain the patient complains ofdoes not therefore mean that the definitive source ofthe problem has been found (see Gifford 1997b;Gifford 1998a). All any 'positive' test response doesis reflect the sensitivity state of the tissue examinedand/or the sensitivity of the relevant processingpathways in the central nervous system. A sensitivetissue may or may not be significantly pathological.
For example, a 34 year old patient complained ofhaving a heavy tired right arm with a low grade andfairly continuous forearm aching sensation that wasstarting to disturb his sleep. His major concern was aknife like pain well localised about one third of theway down the right medial scapula border. Theproblem was about 2 weeks old and described asworsening and becoming worrying. He reportedhaving had 2 sessions of manipulative treatment forthe scapular pain. This involved 'firm' neck andthorax 'cracking' but to little effect other than afeeling of freedom of movement for several hours.The arm problem worsened about 3^4 days after hislast manipulation session. On examination the medialscapula area felt thickened and tight compared to theother side and modestly firm palpatory pressuresexacerbated the arm pain within 15 seconds or so.Was this the source of the problem? It clearly was tothe patient, but there were further striking findingsto be taken into account. The patient had no tricepsreflex on the affected side and the triceps muscle wasmarkedly weaker to the astonishment of the patient.Neck movements were normal except end range lowcervical extension which brought on a vicious 'bite' ofpain in the medial border of scapula. The patient wasunaware of this finding until tested. Anterior palpa-tion of the neck over the ipsilateral transverse processof C7 also reproduced the scapula pain and increasedthe forearm discomfort. Upper limb tension testswere unrevealing.
Taking into account results like this adjusts thefocus of attention towards low cervical nervedysfunction and altered central sensitivity andrelegates the medial scapula tenderness more to asecondary hyperalgesia status with the possibility ofsecondary changes (swelling and thickening) influ-enced via efferent neurogenic signaling (overviewed
in: Hasue 1993). In fact, in this patient, furtherpalpatory investigation revealed widespread andsignificant tenderness, or 'pain related impairments'over the lateral epicondyle of the elbow, the radialnerve in the radial groove and the belly of thesupraspinatus muscle where medial border of scapu-lar pain could again be reproduced. Skin light-touchcomparisons with the non-symptomatic forearmrevealed skin hypersensitivity too. Overpressure toglenohumeral flexion and elbow extension producedmarkedly more discomfort when compared to similarcontralateral overpressures. A cursory examination islikely to miss significant findings that might otherwiseadd to the possible nerve root origins of the problemand the appreciation of altered processing factorswithin the central nervous system. There are greatdangers, or 'reasoning errors', in assuming that justbecause a tissue palpated or tested reproduces apatients pain it has to be the 'source' of the problem.Pain distribution and pain response to testing areoften very misleading and always difficult to inter-pret, even in acute conditions like these.
Finally, it is worthwhile making an observationwith regards recovery and natural history. In theearly days some nerve root disorders seem unrelent-ing. As a clinician one feels impotent and as a patientone feels desperate. Typically, the worst period is thefirst one to two weeks but may be as long as fouror five weeks. Thereafter, and if well managed thecondition usually gradually subsides with more andmore good periods and the gradual restoration ofnormal activity. For patients, the 'good news' is thatthe symptoms do settle and most gradually settle, the'bad news' is that it can take three months or longer.Some become chronic pain . sufferers, but thispossibility is reduced if they are managed well inthe early stages (Waddell 1998; Watson 2000; Kendall& Watson 2000; Watson & Kendall 2000; Linton1999).
References
Beatty RM, Fowler RD, Hanson EJ 1987 The abducted arm as asign of ruptured cervical disk. Neurosurgery 21: 731-732
Bogduk N 1997 Clinical Anatomy of the Lumbar Spine andSacrum. Churchill Livingstone, Edinburgh
Bove GM, Light AR 1997 The Nervi Nervorum. Missing link forneuropathic pain? Pain Forum 6(3): 181-190
Butler DS 1991 Mobilisation of the Nervous System. ChurchillLivingstone, Melbourne
Byrod G, Olmarker K, Konno S, Larsson K, Takahashi K,Rydevik B 1995 A rapid transport route between the epiduralspace and the intraneural capillaries of the nerve roots. Spine20(2): 138-143
Clatworthy AL, Illich PA, Castro GA, Walters ET 1995 Role ofperi-axonal inflammation in the development of thermalhyperalgesia and guarding behavior in a rat model ofneuropathic pain. Neuroscience Letters 184: 5-8
CSAG 1994 Report of a Clinical Standards Advisory GroupCommittee on back pain. HMSO, London
Davidson RI, Dunn DJ, Metzmaker JN 1981 The shoulderabduction test in the diagnosis of radicular pain in cervicalextradural compression monoradiculopathies. Spine 6: 441-446
Manual Therapy (2001) 6(2), 106-115 © 2001 Harcourt Publishers Ltd

Acute low cervical nerve root conditions 115
Devor M 1994 The pathophysiology of damaged peripheral nerves.In: Wall PD, Melzack R (eds) Textbook of Pain. 3rd ednChurchill Livingstone, Edinburgh 79-100
Devor M 1996 Pain mechanisms and pain syndromes. In: CampbellJN (ed) Pain 1996 - An updated review. Refresher coursesyllabus IASP Press, Seattle 103-112
Devor M, Lomazov P, Matzner O 1994 Sodium channelaccumulation in injured axons as a substrate for neuropathicpain. In: Boivie J, Hansson P, Lindblom U (eds) Touch,Temperature and Pain in Health and Disease: Mechanisms andAssessments IASP Press, Seattle 207-230
Devor M, Seltzer Z 1999 Pathophysiology of damaged nerves inrelation to chronic pain. In: Wall PD, Melzack R (eds) TheTextbook of Pain. 4th edn Churchill Livingstone, Edinburgh129-164
Durkan JA 1991 A new diagnostic test for carpal tunnel syndrome.J Bone Joint Surg [Am] 73A(4): 535-538
Ehni B, Ehni G, Patterson RH 1990 Extradural spinal cord andnerve root compression from benign lesions of the cervical area.In: Youmans JR (ed) Neurological Surgery Saunders,Philadelphia 2878-2916
Elvey R, Hall T 1997 Neural tissue evaluation and treatment. In:Donatelli R (ed) Physical Therapy of the Shoulder 3rd. ednChurchill Livingstone, New York 131-152
Elvey RL 1994 The investigation of arm pain: signs of adverseresponses to the physical examination of the brachial plexusand related neural tissues. In: Boyling JD, Palastanga N (eds)
• Grieve's Modern Manual Therapy. 2nd edn ChurchillLivingstone, Edinburgh 577-585
Farmer JC, Wisneski RJ 1994 Cervical spine nerve rootcompression. An analysis of neuroforaminal pressures withvarying head and arm positions. Spine 19(16): 1850-1855
Fast A, Parikh S, Marin E 1989 The shoulder abduction reliefsign in cervical radiculopathy. Arch-Phys-Med-Rehabil 70(5):402-403
Gifford LS 1997a Neurodynamics. In: Pitt-Brooke (ed)Rehabilitation of Movement: Theoretical bases of clinicalpractice Saunders, London 159-195
Gifford LS 1997b Pain. In: Pitt-Brooke (ed) Rehabilitation ofMovement: Theoretical bases of clinical practice Saunders,London 196-232
Gifford LS 1998a Central mechanisms. In: Gifford LS (ed) TopicalIssues in Pain 1. Whiplash - science and management. Fear-avoidance beliefs and behaviour. CNS Press, Falmouth 67-80
Gifford LS 1998b The mature organism model. In: Gifford LS (ed)Topical Issues in Pain. Whiplash - science and management.Fear-avoidance beliefs and behaviour. CNS Press, Falmouth45-56
Gifford LS 1988c Output mechanisms. In: Gifford LS (ed) Topicalissues in Pain 1. Whiplash - science and management. FearAvoidance beliefs and behaviour. CNS Press, Falmouth, 81-91
Gifford LS, Butler DS 1997 The integration of pain sciences intoclinical practice. Hand Therapy 10(2): 86-95
Hasue M 1993 Pain and the nerve root. An interdisciplinaryapproach. Spine 18(14): 2053-2058
Howe JF, Loeser JD, Calvin WH 1977 Mechanosensitivity ofdorsal root ganglia and chronically injured axons: aphysiological basis for the radicular pain of nerve rootcompression. Pain 3: 25-41
Issberner U, Reeh PW, Steen, KH 1996 Pain due to tissue acidosis:a mechanism for inflammatory and ischemic myalgia?Neuroscience letters 208: 191-194
Janig W, Stanton-Hicks M 1996 Reflex Sympathetic Dystrophy:A reappraisal. IASP Press, Seattle
Johnson MI 1997 The physiology of the sensory dimensions ofclinical pain. Physiotherapy 83(10): 526-536
Kendall N, Watson P 2000 Identifying psychosocial yellow flagsand modifying management. In: Gifford LS (ed) Topical Issuesin Pain 2. Biopsychosocial assessment and management.Relationships and pain. CNS Press, Falmouth, 131-139
Koltzenburg M 1996 Afferent mechanisms mediating pain andhyperalgesia in neuralgia. In: Janig W, Stanton-Hicks M (eds)Reflex Sympathetic Dystrophy: A reappraisal IASP Press,Seattle 123-150
Kuslich SD, Ulstrom CL, Michael CJ 1991 The tissue origin oflow back pain and sciatica: a report of pain response totissue stimulation during operations on the lumbar spine using
local anesthesia. Orthopaedic Clinics of North America22(2): 181
Linton SJ 1999 Cognitive behavioural interventions for thesecondary prevention of low back pain. In: Max M (ed) Pain1999 An updated review. Refresher course syllabus IASP PressSeattle, 305-311
Maigne JV, Deligne L 1994 Computed tomographic follow-upstudy of 21 cases of non-operatively treated cervicalintervertebral soft disc herniation. Spine 19: 189-191
Maitland GD 1986 Vertebral Manipulation. Butterworth, LondonMcCarron RF, Wimpee MW, Hudgins PG, Laros GS 1987 The
inflammatory effect of nucleus pulposus: a possible element inthe pathogenesis of low back pain. Spine 12: 760-764
Moses A, Carman J 1996 Anatomy of the cervical spine:implications for the upper limb tension test. Australian Journalof Physiotherapy 42: 31-35
Nathan H, Feuerstein M 1970 Angulated course of spinal nerveroots. Journal of Neurosugery 32: 249-352
Olmarker K, Blomquist J, Stromber J, Nannmark U, Thomsen P,Rydevik B 1995 Inflammatogenie properties of nucleuspulposus. Spine 25(6): 665-669
Olmarker K, Rydevik B, Holm S, Bagge U 1989 Effects ofexperimental graded compression on blood flow in spinal nerveroots. A vital microscopic study on the porcine cauda equina.Journal of Orthopaedic Research 7: 817-823
Olmarker K, Rydevik B, Nordborg C 1993 Autologous nucleuspulposus induces neurophysiologic and histologic changes inporcine cauda equina nerve roots. Spine 18(11): 1425-1432
Penning L 1992 Functional pathology of lumbar spinal stenosis(review). Clinical Biomechanics 7(1): 3-17
Penning L, Wilmink JT 1981 Biomechanics of lumbosacral duralsac. A study of flexion-extension myelography. Spine 6(4): 398
Ramachandran VS, Blakeslee S 1998 Phantoms in the Brain.Probing the mysteries of the human mind. Quill, New York
RCGP 1996 Clinical guidelines for the management of acute lowback pain. Royal College of General Practice, London
Roberts L 2000 Flagging the danger signs of low back pain. In:Gifford L (ed) Topical Issues in Pain 2. Biopsychosocialassessment and management. Relationships and pain CNSPress, Falmouth
Saal JS 1995 The role of inflammation in lumbar pain. Spine20(16): 1821-1827
Scadding JW 1999 Complex regional pain syndrome. In: Wall PD,Melzack R (eds) The Textbook of Pain. 4th edn ChurchillLivingstone, Edinburgh 835-849
Slipman CW, Plastaras CT, Palmitier RA, Huston CW, SterenfeldEB 1998 Symptom provocation of fluoroscopically guidedcervical nerve root stimulation. Are dynatomal maps identicalto dermatomal maps? Spine 23(20): 2235-2242
Steen KH, Steen AE, Kreysel HW, Reeh PW 1996 Inflammatorymediators potentiate pain induced by experimental acidosis.Pain 66: 163-170
Tracey DJ, Walker JS 1995 Pain due to nerve damage: areinflammatory mediators involved? Inflammatory Research44: 407-411
Waddell G 1998 The Back Pain Revolution. Churchill Livingstone,Edinburgh
Wall PD, Devor M 1983 Sensory afferent impulses originate fromdorsal root ganglia and chronically injured axons: Aphysiological basis for the radicular pain of nerve rootcompression. Pain 17: 321-339
Watson P 2000 Psychosocial predictors of outcome from low backpain. In: Gifford LS (ed) Topical Issues in Pain 2.Biopsychosocial assessment and management. Relationshipsand pain. CNS Press, Falmouth, 85-109
Watson P, Kendall N 2000 Assessing psychosocial yellow flags. In:Gifford LS (ed) Topical Issues in Pain 2. Biopsychosocialassessment and management. Relationships and pain. CNSPress, Falmouth, 111-129
Wright A 1999 Recent concepts in the neurophysiology of pain.Manual Therapy 4(4): 196-202
Yoo JU, Zou D, Edward^T, Bayley J, Yuan HA 1992 Effect ofcervical spine motion on the neuroforaminal dimensions ofhuman cervical spine. Spine 17(10): 1131
Zusman M 1992 Central nervous system contribution tomechanically produced motor and sensory responses.Australian Journal of Physiotherapy 38(4): 245-255
2001 Harcourt Publishers Ltd Manual Therapy (2001) 6(2), 106-115